Integrated Care of Patients on Constant Observation in a General Hospital Setting Aaron Pinkhasov, MD
|
|
|
- Kristopher Hawkins
- 5 years ago
- Views:
Transcription
1 Integrated Care of Patients on Constant Observation in a General Hospital Setting Aaron Pinkhasov, MD Chairman, Department of Behavioral Health NYU Winthrop Hospital Associate Professor of Psychiatry and Medicine Stony Brook School of Medicine
2 In compliance with ACCME Standards for Commercial Support of CME activities I have no relevant financial relationships to disclose. Aaron Pinkhasov, MD

3 Objectives By the end of this presentation the audience will be able to: Demonstrate understanding of the role of psychiatric services in management of patients placed on constant observation in a general hospital. Recite main strategies in management of patients on constant observation. List potential benefits of management protocol.





4 Est 1831 Est 1860




5



6 Est 1896
7 591-bed university-affiliated medical center which offers sophisticated diagnostic and therapeutic care in virtually every specialty and subspecialty of medicine and surgery Primary teaching affiliate of Stony Brook School of Medicine Clinical Campus Offering 24 residency and fellowships The prevalence of psychiatric co-morbidity in our hospital - 34% The psychiatry consultation rate at the time was only 1.36%

8 $2.3mln spent on sitters alone by Winthrop Hospital in 2014
9 Constant Observation (CO) Facts CO-utilization adds substantial burden on hospital finances and personnel resources. CO-cost may range from $2 to 6 million per year, not including the cost of CO in specialized psychiatric units. Studies fail to show a reduction in adverse events despite use of CO. Harding, A. D. (2010). Observation assistants: sitter effectiveness and industry measures. Nursing Economics, 28(5), 330. Adams, J., & Kaplow, R. (2013). A sitter-reduction program in an acute health care system. Nursing Economics, 31(2), 83.[5.] Rochefort et al (2012). Patient and nurse staffing characteristics associated with high sitter use costs. Journal of advanced nursing, 68(8),
10 QI Program Development Formalized policy - psychiatric CL services for any patient on CO Hiring a psychiatric NP for management of patients on CO Early/Proactive daily evaluation of CO patients by BH team Collaboration with patient, patient s family and medical team Implementing non-pharmacological as well as pharmacological Tx
11 QI Project Development BH-CO protocol was implemented daily on all patients who had at least 12 business hours of CO except weekends & holidays. All patients were followed until at least 1 business day after CO d/c Data on length of stay (LOS), CO cost, complications (falls, elopements or inadvertent extubations) and 30-day readmissions were collected over a 6-month study period. 533 patients were studied (42pts excluded <12business hrs of CO use) 491 patients were seen by the BH team and underwent the protocol. Data was compared with a similar sequential group of all patients placed on CO during the previous year.
12 Protocol Overview 1:1 one staff member directly observes patient within an arm's length at all times. SW one staff member observes up-to four patients cohorted in the same room. Both groups of CO patients are referred to and evaluated by the BH team (psychiatric nurse practitioner (NPP) with a board-certified psychiatrist)
13 40 Primary Reasons for 1:1 Order Percentage Agitation/Confusion Suicidal Risk Pulling out IV lines/tubes Trying to get out of bed Combative behavior Elopement Risk Fall Risk Acute Psychosis/Mania
14 Primary Reasons for Safety Watch Order Agitation/Confusion Trying to get out of bed Fall Risk Pulling out IV lines/tubes Combative behavior Elopement Risk


15 Overlap of Reasons for CO Agitated and a Elopement Risk Agitated and a Fall Risk Agitated and Combative Agitated and Confused Agitated Agitated and Pulling IV's 0

16 CO Protocol Overview A comprehensive evaluation and management protocol was developed as part of this QI project
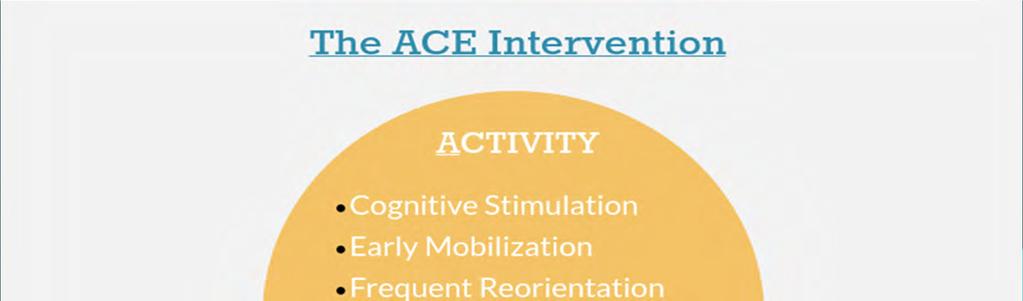
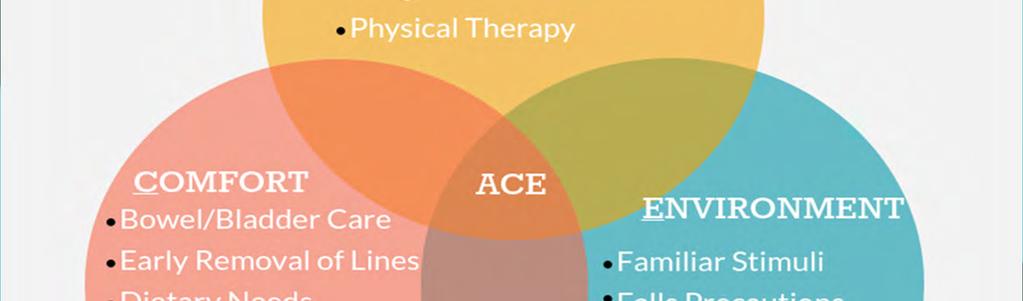
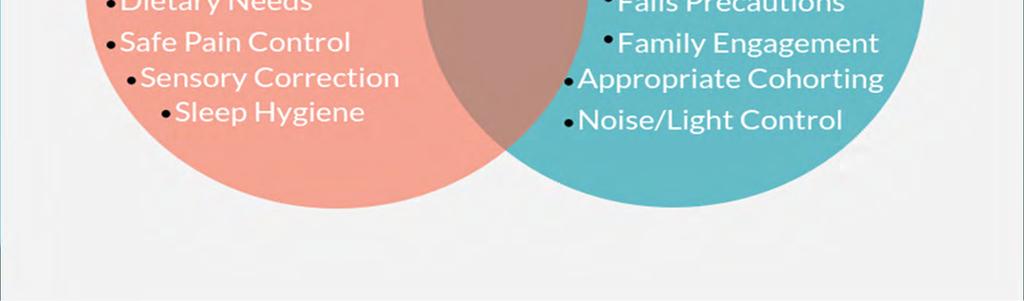
17
18 Pharmacologic Intervention Minimize the use of benzodiazepines/opiates/anticholinergic Mx Melatonin receptor agonist for sleep phase disturbances Acetaminophen PO/IV when appropriate to avoid/minimize narcotic analgesics Judicious use of low dose antipsychotics for agitation/psychosis Use of dexmedetomidine in ICU settings for agitation
19 Low Dose Antipsychotics Use in CO Protocol Generic Name Usual Dose Range (mg/day) Route Extrapyramidal symptoms QTc Prolongations Orthostatic Hypotension Haloperidol PO/IM/IV (more with IV use) + Quetiapine PO +/ Risperidone PO
20 CO Age Distribution

 Delirium (N, %) Anxiety (N, %) Depression (N, %)")
21 CO Prevalence of Psychiatric Dx Psychosis 4.9% EtoH 7.9% Bipolar/Mania 3.5% Other Substance 3.3% Depression 25.1% Dementia 52.7% Anxiety 10.6% Delirium 62.1% Dementia (N, %) Delirium (N, %) Anxiety (N, %) Depression (N, %) Bipolar/Mania (N, %) Psychosis (N, %) Alcohol Use (N, %) Other Substance (N, %)
22 HIGH PREVALENCE OF DELIRIUM (62.1%) AND DEMENTIA (52.7%) N*PATIENTS REDUCTION DISCONTINUATION NO CHANGE Benzodiazepines 130 (26.8%) 24.6% 53.1% 22.3% Opiates 116 (23.9%) 33.6% 49.1% 17.2% Anticholinergics 12 (2.5%) % 8.3% *We also found that patients diagnosed with delirium treated with nightly ramelteon were less likely given as-needed antipsychotics for agitation (60% vs 86%)



23 Constant Observation Cost Reduction $300, $271, Program Implemented $250, $238, $200, $189, $150, $100, $141, $82, $114, $109, $105, $50, $0.00 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
24 RESULTS: Average Monthly CO Cost STUDY GROUP CONTROL PERIOD $177,541 $118,847 $58,700 Monthly Difference 33.06% (p-value 0.045) $704,400 Annual Projected Savings
25 RESULTS Median Length of Stay STUDY GROUP CONTROL PERIOD 6 days 7 days 15% REDUCTION
26 Results: Complications ADVERSE EVENTS CONTROL PERIOD STUDY RESULTS FALLS 63 2 INADVERTENT EXTUBATIONS 10 0 ELOPEMENTS 3 1 READMISSION 20 of 553 patients (3.6%) 10 of 491 patients (2.0%)



27





28 Resistance from staff or family members towards discontinuation of co Delay in disposition due to non availability of beds and insurance issues Patients who remain difficult to redirect BARRIERS Patients who are an imminent danger to self and others, and need psychiatric hospitalization Patients with severe cognitive decline
29 CASE ILLUSTRATION A 72 yo female with history of Alzheimer s dementia x 2 yrs bib dtr because she found her house in disarray. She has been forgetful and paranoid towards neighbors for some time. Admitted for low Hb (7.8) and need for GI work up. Placed on 1:1 for agitation and poor c/w care. Other lab s WNL. PMHx: Migraine, OA Home Meds: Advil PRN; Aricept 5mg qd MSE: Pt. alert and oriented to person and place only. Word finding difficulties. Mild paranoia. No a/v hallucinations and/or s/h ideas. Poor I/J. MMSE 19/30 Diagnosis: Dementia with behavioral disturbances Recommendations: Increase Aricept to 10mg qhs Namenda 5mg qd Risperdal 0.5mg q12hrs Frequent reassurance, reorientation and redirection Discontinue 1:1 and place patient on q30 checks for safety Results of Interventions: Pt. had uneventful night. Dtr was encouraged to accompany pt and facilitated c/w Upper Endoscopy. Pt was stabilized and placed to NH.
30 CASE ILLUSTRATION Female in early 90s with history of age related memory loss admitted s/p fall and R- Hip Fx, had ORIF,POD-2; became very confused and disorganized post op. Relatively independent prior to fall. Placed on 1:1 for agitation and fall risk. She was up all night and given Benadryl 50mg x 1 stat. No PPHx. PMHx: mild HTN and OA. Meds included Methadone,Oxycodone,Tramadol 50mg TID, Ativan PRN, Dilaudid PRN MSE: Elderly woman, lethargic, disoriented. Trying to get out of bed. Responding to internal stimuli (reaching for imaginary objects). Diagnosis: Dementia with superimposed delirium Recommendations: d/c Methadone,Tramadol,Oxycodone,Ativan and Dilaudid Tylenol 1g IV q 8hrs Rozerem 8mg qhs and keep awake during daytime Quetiapine 25 mg PO qhs Frequent reorientation and redirection Adequate PO hydration and assistance with ADLs Remove Foley Results of Interventions: Became alert and cooperative with PT next day, then 1:1 was changed to q30 checks. D/C to Sub-acute Rehab day after.
31 MANAGEMENT OF PATIENTS WITH COGNITIVE DECLINE Frequent reorientation and redirection of confused patients. Use of bed checks and safety alarms to prevent them from getting out of bed without assistance. Use of hand mittens to prevent them from pulling out lines and tubes. Ordering q30 checks for patients with fall risk. Use of low dose anti-psychotics like Haldol for management of dementia with behavioral disturbances. Encouraging frequent family visits to provide patients with a familiar environment.
32 Suicidal Patients on Co Patients who are considered acutely suicidal kept on 1:1 observation until transfer to an inpatient psych. Unavoidable delays in disposition like 2 PC transfers of undocumented /uninsured patients and bed unavailability in inpatient facilities further increase the number of hours utilized.
33 CASE ILLUSTRATION 54 yo male with h/o Anxiety and ETOH abuse was admitted with PNA.Placed on 1:1 due to expressing suicidal ideas to RN. On evaluation stated: I just said I feel like jumping out of window to nurse, I don t mean it, I am just frustrated. No h/o prior psychiatric admissions or suicidal attempts. No signs of EtOH withdrawal. MSE: Pt Diagnosis: Adjustment d/o with depressed mood Recommendations: d/c 1:1 Ativan 1mg q6hrs PRN anxiety/alcohol withdrawal Lexapro 5mg PO qd Day after: 1:1 resumed as he was talking about jumping out of window to RN. 1:1 stopped and staff reassured Day 3: back on 1:1 I asked for it, I feel more comfortable when I have company. I like this nurse, she is cute. Pt was discharged with oral antibiotics 5 days later.
34 Interventions PHARMACOLOGICAL: These include use of various psychotropic medications broadly categorized as: Typical Antipsychotics Atypical Antipsychotics Antidepressants Melatonin Agonists Benzodiazepines Mood Stabilizers/Anticonvulsants Dementia Medications Strongly discouraging the use of benzodiazepines, sedative-hypnotics, anti-cholinergic or opiate analgesics in elderly patients who are at high risk of delirium.
Multiple Choice Questions
 Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
ARE EMERGENCY DEPARTMENTS THE BEST PLACE TO CARE FOR PSYCHIATRIC PATIENTS IN CRISIS? Objectives. Conflict of Interest
 ARE EMERGENCY DEPARTMENTS THE BEST PLACE TO CARE FOR PSYCHIATRIC PATIENTS IN CRISIS? Jeannine Loucks, MSN, RN BC PMH Elizabeth Winokur, Ph.D., RN CEN Sacred Encounters Perfect Care Healthiest Communities
ARE EMERGENCY DEPARTMENTS THE BEST PLACE TO CARE FOR PSYCHIATRIC PATIENTS IN CRISIS? Jeannine Loucks, MSN, RN BC PMH Elizabeth Winokur, Ph.D., RN CEN Sacred Encounters Perfect Care Healthiest Communities
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013
 A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
Medical and Behavioral Health: A Delicate Balance
 Medical and Behavioral Health: A Delicate Balance Mae Centeno DNP, RN, CCRN,CCNS,ACNS-BC Corporate Director Chronic Care Continuum Jeff Place MSN,MBA,RN Director BUMC Nursing Service Support 1 Background
Medical and Behavioral Health: A Delicate Balance Mae Centeno DNP, RN, CCRN,CCNS,ACNS-BC Corporate Director Chronic Care Continuum Jeff Place MSN,MBA,RN Director BUMC Nursing Service Support 1 Background
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
PRN Medications. Indications & Use. Bindu Swaroop, MD Associate Clinical Professor Department of Medicine
 PRN Medications Indications & Use Bindu Swaroop, MD Associate Clinical Professor Department of Medicine Objectives Identify which prn medications are appropriate for inclusion in admission orders Identify
PRN Medications Indications & Use Bindu Swaroop, MD Associate Clinical Professor Department of Medicine Objectives Identify which prn medications are appropriate for inclusion in admission orders Identify
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
TELEPSYCHIATRY CONSULTATION PROGRAM FOR A COMMUNITY HOSPITAL IN WASHINGTON
 TELEPSYCHIATRY CONSULTATION PROGRAM FOR A COMMUNITY HOSPITAL IN WASHINGTON CMC in Olympia is a 110-bed full-service hospital providing 24-hour emergency care in a Level IV Trauma Designated Facility. Despite
TELEPSYCHIATRY CONSULTATION PROGRAM FOR A COMMUNITY HOSPITAL IN WASHINGTON CMC in Olympia is a 110-bed full-service hospital providing 24-hour emergency care in a Level IV Trauma Designated Facility. Despite
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
There s No Place like Home
 THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Telepsychiatry In Rural Nursing Homes
 Telepsychiatry In Rural Nursing Homes Andrew Rosenzweig MD, MPH Chief Medical Officer, Forefront TeleCare Assistant Clinical Professor, Brown University cope of Problem: evere Unmet Need Over 5,000 rural/hpa
Telepsychiatry In Rural Nursing Homes Andrew Rosenzweig MD, MPH Chief Medical Officer, Forefront TeleCare Assistant Clinical Professor, Brown University cope of Problem: evere Unmet Need Over 5,000 rural/hpa
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Disclosure. Speaker Bureaus. Grant Support. Pfizer Forest Norvartis. Pan American Health Organization/WHO NIA HRSA
 Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
9/11/2012. Clare I. Hays, MD, CMD
 Clare I. Hays, MD, CMD Review regulatory background for current CMS emphasis on antipsychotics Understand the risks and (limited) benefits of antipsychotic medications Review non-pharmacologic management
Clare I. Hays, MD, CMD Review regulatory background for current CMS emphasis on antipsychotics Understand the risks and (limited) benefits of antipsychotic medications Review non-pharmacologic management
GERIATRICS 101. Victoria L. Braund, MD, FACP, CMD. Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston
 GERIATRICS 101 Victoria L. Braund, MD, FACP, CMD Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston LET S REVIEW Medicare Hospice Pain mgmt. Bowel business Delirium Sleep
GERIATRICS 101 Victoria L. Braund, MD, FACP, CMD Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston LET S REVIEW Medicare Hospice Pain mgmt. Bowel business Delirium Sleep
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Inpatient Delirium Management: A Quality Improvement Project for Hospitalized Veterans. IIndiana Nursing Summit
 Inpatient Delirium Management: A Quality Improvement Project for Hospitalized Veterans IIndiana Nursing Summit November 5, 2018 At the conclusion of this presentation, participants will be able to: Identify
Inpatient Delirium Management: A Quality Improvement Project for Hospitalized Veterans IIndiana Nursing Summit November 5, 2018 At the conclusion of this presentation, participants will be able to: Identify
Inpatient Delirium Management: A Quality Improvement Project for Hospitalized Veterans
 Inpatient Delirium Management: A Quality Improvement Project for Hospitalized Veterans IIndiana Nursing Summit November 5, 2018 Veteran Health Indiana At the conclusion of this presentation, participants
Inpatient Delirium Management: A Quality Improvement Project for Hospitalized Veterans IIndiana Nursing Summit November 5, 2018 Veteran Health Indiana At the conclusion of this presentation, participants
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Delirium and cognitive impairment in the perioperative
 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
ADULTS WITH COMPLEX BEHAVIORAL SUPPORT NEEDS. Betsey Benson, Ph.D. Vanessa Rodriguez, Ph.D., BCBA-D Nisonger Institute 2015
 ADULTS WITH COMPLEX BEHAVIORAL SUPPORT NEEDS Betsey Benson, Ph.D. Vanessa Rodriguez, Ph.D., BCBA-D Nisonger Institute 2015 Transitions School to Work or Other Guardianship Home Mental Health Physical Health
ADULTS WITH COMPLEX BEHAVIORAL SUPPORT NEEDS Betsey Benson, Ph.D. Vanessa Rodriguez, Ph.D., BCBA-D Nisonger Institute 2015 Transitions School to Work or Other Guardianship Home Mental Health Physical Health
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
QuickTime and a DV - NTSC decompressor are needed to see this picture.
 QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Residents Who Don t Sleep
 Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery. The next steps in orthogeriatrics
 Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery Dr. John Joanisse, Chantal Chabot NP The next steps in orthogeriatrics Background More than 8 years
Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery Dr. John Joanisse, Chantal Chabot NP The next steps in orthogeriatrics Background More than 8 years
Antipsychotics for Dementia Under Control or Over-Prescribed?
 Antipsychotics for Dementia Under Control or Over-Prescribed? Nathaniel Hedrick, PharmD ProCare HospiceCare, Manager of Clinical Services Learning Objectives Summarize the disease progression and most
Antipsychotics for Dementia Under Control or Over-Prescribed? Nathaniel Hedrick, PharmD ProCare HospiceCare, Manager of Clinical Services Learning Objectives Summarize the disease progression and most
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Care of the Acutely Agitated Patient. Objectives. Agitation Defined
 Care of the Acutely Agitated Patient James C. Hardy, MD Assistant Professor of Emergency Medicine Department of Emergency Medicine, UCSF Dealing with combative patients is one of the most difficult challenges
Care of the Acutely Agitated Patient James C. Hardy, MD Assistant Professor of Emergency Medicine Department of Emergency Medicine, UCSF Dealing with combative patients is one of the most difficult challenges
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Bock Associates 221 West 2 nd Street, Suite 607 Little Rock, AR 72201
 Bock Associates 221 West 2 nd Street, Suite 607 Little Rock, AR 72201 State Project Director- Bliss Beeman, RN Clinical Associate- Shelley Smith, RN Administrative Assistant- Viki DeClerk bockarkansas@gmail.com
Bock Associates 221 West 2 nd Street, Suite 607 Little Rock, AR 72201 State Project Director- Bliss Beeman, RN Clinical Associate- Shelley Smith, RN Administrative Assistant- Viki DeClerk bockarkansas@gmail.com
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Medication Management. Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015
, FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015") Medication Management Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015 1 Medication Management Objectives: 1. Principles of psycho-pharmacology
Medication Management Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015 1 Medication Management Objectives: 1. Principles of psycho-pharmacology
Delirium in Cancer: Psychopharmacologic Management
 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Mental Health Issues in Nursing Homes. I m glad you asked.
 Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
DAVE SHESKI, MD DELIRIUM
 DAVE SHESKI, MD DELIRIUM GOALS/OUTLINE What is delirium? What are the different ways in which it can present? How do you screen for and diagnose it? What causes it? How do you treat it? WHAT IS DELIRIUM?
DAVE SHESKI, MD DELIRIUM GOALS/OUTLINE What is delirium? What are the different ways in which it can present? How do you screen for and diagnose it? What causes it? How do you treat it? WHAT IS DELIRIUM?
OPMH LIASION TEAM BASINGSTOKE & WINCHESTER
 OPMH LIASION TEAM BASINGSTOKE & WINCHESTER Initial Challenges Resources Information from referrers Diagnosis: delirium or dementia Training all clinical staff about behavioural management Appropriate use
OPMH LIASION TEAM BASINGSTOKE & WINCHESTER Initial Challenges Resources Information from referrers Diagnosis: delirium or dementia Training all clinical staff about behavioural management Appropriate use
LIAISON PSYCHIATRY FOR OLDER PEOPLE
 LIAISON PSYCHIATRY FOR OLDER PEOPLE Fiona Thompson Consultant Psychiatrist Addenbrookes Hospital US LP mid 18 th Century UK after WW2 Developmental History 1948 WHO defined health as a state of complete
LIAISON PSYCHIATRY FOR OLDER PEOPLE Fiona Thompson Consultant Psychiatrist Addenbrookes Hospital US LP mid 18 th Century UK after WW2 Developmental History 1948 WHO defined health as a state of complete
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Fall Reduction in the Christus Santa Rosa ACE Unit
 Clinical Safety & Effectiveness Cohort # 7 Fall Reduction in the Christus Santa Rosa ACE Unit Educating for Quality Improvement & Patient Safety Project Milestones Milestone Date Team created January 2011
Clinical Safety & Effectiveness Cohort # 7 Fall Reduction in the Christus Santa Rosa ACE Unit Educating for Quality Improvement & Patient Safety Project Milestones Milestone Date Team created January 2011
12/17/2012. Unnecessary Drugs
 Nursing Home Social Work Webinar Series December 19, 2012 Dr. Robin P. Bonifas, PhD, MSW Arizona State University School of Social Work Importance of familiarity with psychotropic medication regulations.
Nursing Home Social Work Webinar Series December 19, 2012 Dr. Robin P. Bonifas, PhD, MSW Arizona State University School of Social Work Importance of familiarity with psychotropic medication regulations.
OBJECTIVES. Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia
 Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia Amy J. Osborn, NHA, PMP Executive Director, Health Services Advisory Group (HSAG) Rick Foley, PharmD,
Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia Amy J. Osborn, NHA, PMP Executive Director, Health Services Advisory Group (HSAG) Rick Foley, PharmD,
Antipsychotic use in Dementia care. Jabbar Fazeli, MD
 Antipsychotic use in Dementia care Jabbar Fazeli, MD www.mainegeriatrics.com What changed in 2012? NY times- May 9, 2011!! Antipsychotic Drugs Called Hazardous for the Elderly - referencing the OIG audit
Antipsychotic use in Dementia care Jabbar Fazeli, MD www.mainegeriatrics.com What changed in 2012? NY times- May 9, 2011!! Antipsychotic Drugs Called Hazardous for the Elderly - referencing the OIG audit
The place for treatments of associated neuropsychiatric and other symptoms
 The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
Patient Safety - IV Opioid Use in Hospitalized Patients. October 2014
 Patient Safety - IV Opioid Use in Hospitalized Patients October 2014 Objectives List reasons that necessitated development of risk assessment State a few risk factors or medical conditions from the IV
Patient Safety - IV Opioid Use in Hospitalized Patients October 2014 Objectives List reasons that necessitated development of risk assessment State a few risk factors or medical conditions from the IV
Aging Research Day March 8, 2012
 Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist
 Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Home Care and Hospice Association of New Jersey Annual Conference 2017
 Home Care and Hospice Association of New Jersey Annual Conference 2017 I D E N T I F I C A T I O N A N D M A N A G E M E N T O F D E L I R I U M E L I Z A B E T H M A G E R - O C O N N O R A C H P N DR
Home Care and Hospice Association of New Jersey Annual Conference 2017 I D E N T I F I C A T I O N A N D M A N A G E M E N T O F D E L I R I U M E L I Z A B E T H M A G E R - O C O N N O R A C H P N DR
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Insomnia: Updates in Medical Management. Michael Newnam M.D.
 Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Clinical Management of Confusion. Mark Sherer, Ph.D. Associate Vice President for Research
 Clinical Management of Confusion Mark Sherer, Ph.D. Associate Vice President for Research Assessment of PTCS Confusion Assessment Protocol Authors: Mark Sherer, Risa Nakase-Richardson, Stuart Yablon Key
Clinical Management of Confusion Mark Sherer, Ph.D. Associate Vice President for Research Assessment of PTCS Confusion Assessment Protocol Authors: Mark Sherer, Risa Nakase-Richardson, Stuart Yablon Key
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Margaret Knight PhD, PMHCNS-BC Catherine Coakley MS, RN-BC
 Margaret Knight PhD, PMHCNS-BC Catherine Coakley MS, RN-BC By 2020, the cost of falls is estimated to be 30 billion per year. Fall Prevention: National Patient Safety Goal Focus on falls: older adults,
Margaret Knight PhD, PMHCNS-BC Catherine Coakley MS, RN-BC By 2020, the cost of falls is estimated to be 30 billion per year. Fall Prevention: National Patient Safety Goal Focus on falls: older adults,
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
4/3/2014. Disclosures Delirious about End-of-Life Delirium? Objectives. Case 1. Yes ma am, that s delirium. What are we talking about?
 Disclosures Delirious about End-of-Life Delirium? No financial or other conflicts of interest There will be off-label discussion TNMHO Convention San Antonio, Texas April 2014 Presenter: Robert A. Friedman,
Disclosures Delirious about End-of-Life Delirium? No financial or other conflicts of interest There will be off-label discussion TNMHO Convention San Antonio, Texas April 2014 Presenter: Robert A. Friedman,
3/27/2013. Objectives. Psychopharmacology at the End of Life Nicole Thurston, MD
 Psychopharmacology at the End of Life Nicole Thurston, MD Psychiatrist Mountain States Tumor Institute Objectives Describe 2 common psychiatric symptoms that can present at or near end of life. Review
Psychopharmacology at the End of Life Nicole Thurston, MD Psychiatrist Mountain States Tumor Institute Objectives Describe 2 common psychiatric symptoms that can present at or near end of life. Review
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model