Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida?
|
|
|
- Muriel Craig
- 5 years ago
- Views:
Transcription

1 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Luigi Oltrona Visconti Divisione di Cardiologia IRCCS Fondazione Policlinico S. Matteo Pavia

2
3 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 The question is : how long? Reducing or prolonging the recommended period of treatment? LOV 2015




4
5 Haemorragic risk Thrombotic risk
6 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 Definitions a) stented stable coronary disease b) acute coronary syndromes LOV 2016
7 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 a) stented stable coronary disease Considerations stent-related strategy (neither disease nor patient) clopidogrel only available (beyond clopidogrel?) duration of treatment LOV 2016
8 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 The future Trial Population Reference Tx Experimental Tx 1 E-point GLOBAL LEADERS 16,000 pts All-comers PCI (stable pts) 12 M asa+clopidogrel + 24 M asa (stable pts) 1 M asa+ticagrelor + 23 M ticagrelor 2 year death/mi TWILIGHT 9,000 pts All-comers PCI (h-risk stable) 15 M asa+ticagrelor 3 M asa+ticagrelor + 12 M ticagrelor BARC bleeding ALPHEUS 1,900 pts Stable pts PCI 30-D asa+clopidogrel 30-D asa+ticagrelor 48h ischemic episodes


9

10
11 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 DAPT administration after stenting with respect to the recommemded time Short? stent thrombosis? MACCE* reduced? bleeding Prolonged * = mortality (total, CV, non-cv), MI, stroke LOV 2016
12 Randomized Trials of DAPT Duration (DES stents) Trial Pts N Months Randomization Design % ACS 1 EP Abbreviated DAPT *Plus a 3M washout EXCELLENT 1,443 6 vs. 12 asa vs. asa + clop ISAR-SAFE 4,000 6 vs. 12* asa vs. asa + clop ITALIC 3,700 6 vs. 12 asa vs. asa + clop OPTIMIZE 3,120 3 vs. 12 asa vs. asa + clop Noninfer iority Noninfer iority Noninfer iority Noninfer iority 52 D/MI/TVR 40 D/MI/CVA/ST, Bleed 24 D/MI/CVA/Rev/MB 32 D/MI/CVA/MB RESET 2,148 3 vs. 12 asa vs. asa + clop Strategy 54 CVD/MI/ST/TVR, Bleed SECURITY 1,399 6 vs 12 asa vs. asa + clop Noninfer iority 38 CD/MI/CVA/ST, Bleed
13 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 LOV 2015 Giustino G et al JACC 2015;65:

14 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 LOV 2015 Giustino G et al JACC 2015;65:
15 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 LOV 2015 Giustino G et al JACC 2015;65:

16 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 LOV 2015 Giustino G et al JACC 2015;65:

17
18 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 Compared to 12 months of DAPT administration short unchanged unchanged reduced stent thrombosis MACCE* bleeding prolonged * = mortality (total, CV, non-cv), MI, stroke LOV 2015
19
20 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 Definitions a) stented stable coronary disease b) acute coronary syndromes LOV 2016
21 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 b) acute coronary syndromes Considerations not stent-related strategy (?) not only clopidogrel available duration of treatment LOV 2016
22 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 The question is : how long? Reducing or prolonging the recommended period of treatment? LOV 2015


23

24

25

26
 10 5 HR 0.77 P=0.0001 HR 0.80 P=0.0003 Prasugrel 9.9 (643) HR 0.81 (0.73-0.90) P=0.0004 NNT= 46 0 ITT= 13,608 LTFU = 14 (0.")
27 Primary Endpoint (%) Nuovi antiaggreganti orali : prasugrel evidenze cliniche di efficacia 15 Primary Endpoint CV Death,MI,Stroke Clopidogrel 12.1 (781) 10 5 HR 0.77 P= HR 0.80 P= Prasugrel 9.9 (643) HR 0.81 ( ) P= NNT= 46 0 ITT= 13,608 LTFU = 14 (0.1%) Days
28 K-M estimate of time to first primary efficacy event (composite of CV death, MI or stroke) Cumulative incidence (%) No. at risk Ticagrelor Clopidogrel ,333 9,291 8,628 8,521 HR 0.84 (95% CI ), p= Days after randomisation 8,460 8,362 8,219 8,124 6,743 6,743 K-M = Kaplan-Meier; HR = hazard ratio; CI = confidence interval Clopidogrel Ticagrelor 5,161 5,096 4,147 4,
 ICH in Pts")
 % Pras 6 (2.3)% (P=0.")


29 % Events 4 Clopidogrel Prasugrel Bleeding Events Safety Cohort (N=13,457) ICH in Pts w Prior Stroke/TIA (N=518) 2 1,8 2,4 1,4 0,9 0,9 1,1 Clop 0 (0) % Pras 6 (2.3)% (P=0.02) 0 TIMI Major Bleeds Life Threatening 0,1 0,4 0,3 0,3 Nonfatal Fatal ICH ARD 0.6% HR 1.32 P=0.03 NNH=167 ARD 0.5% HR 1.52 P=0.01 ARD 0.2% P=0.23 ARD 0.3% P=0.002 ARD 0% P=0.74


30 K-M estimated rate (% per year) Non-CABG and CABG-related major bleeding NS 7.9 Ticagrelor Clopidogrel p= NS p= Non-CABG PLATO major bleeding Non-CABG TIMI major bleeding CABG PLATO major bleeding CABG TIMI major bleeding
31 CURE Safety Bleeding complications Clopidogrel + Standard therapy standard therapy alone including including ASA (%) ASA (%) Major * life-threatening non-life-threatening ** Transfusion *** The CURE Investigators. N Eng J Med August 2001 Data on file *p=0.001; **p=0.002; ***p=0.02
32 Palmerini T et al EurHJ 2017;38:
33 Randomized Trials of DAPT Duration (DES stents) Trial Pts N Months Randomization Design % ACS 1 EP Abbreviated DAPT *Plus a 3M washout EXCELLENT 1,443 6 vs. 12 asa vs. asa + clop ISAR-SAFE 4,000 6 vs. 12* asa vs. asa + clop ITALIC 3,700 6 vs. 12 asa vs. asa + clop OPTIMIZE 3,120 3 vs. 12 asa vs. asa + clop Noninfer iority Noninfer iority Noninfer iority Noninfer iority 52 D/MI/TVR 40 D/MI/CVA/ST, Bleed 24 D/MI/CVA/Rev/MB 32 D/MI/CVA/MB RESET 2,148 3 vs. 12 asa vs. asa + clop Strategy 54 CVD/MI/ST/TVR, Bleed SECURITY 1,399 6 vs 12 asa vs. asa + clop Noninfer iority 38 CD/MI/CVA/ST, Bleed
34 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 Optimal duration of antiplatelet treatment after DES (or ACS) What to do? LOV 2015



35 Il progetto SCA e Diabete : dal documento di consenso al Registro GISE Inibitori P2Y12 alla dimissione (89% dei pazienti) STEMI NSTEMI
36 Gestione della DAPT nel primo anno dopo SCA o PCI : bastano le attuali Linee Guida? Novara 7 Giugno 2018 Optimal duration of antiplatelet treatment after DES (or ACS) Changing the perspective : treat the patient not the stent LOV 2015
37 Levine GN et al Circulation 2017;135:

38 TRACER NSTEMI pts Valgimigli M et al. EurHJ 2017; 38:

39

40
41
42


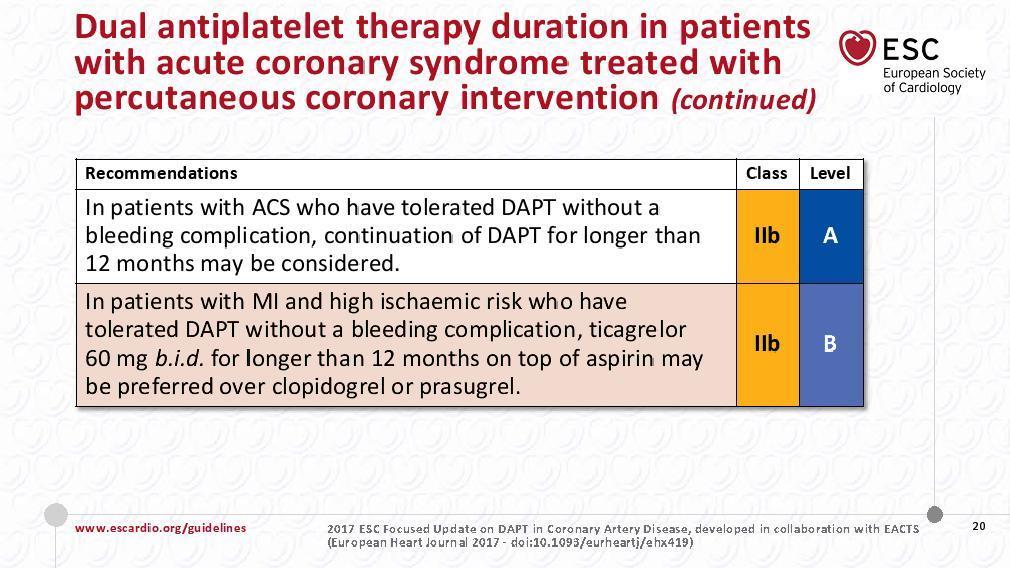
43 DAPT therapy (ACS patients) Guidelines Condition Recommandation/ Evidence Level Year Duration ESC NSTEMI STEMI I A I A months 12 months AHA/ACC NSTEMI STEMI I B I B months 12 months LOV 2017

44 STEMI ESC 2017
45 La durata della DAPT dopo SCA : dallo stent al paziente The question is : how long? Prolonging the recommended period of treatment? LOV 2017
46 Randomized Trials of DAPT Duration (DES stents) Trial Pts N Months Randomization Design 1 EP Abbreviated DAPT *Plus a 3M washout EXCELLENT 1,443 6 vs. 12 asa vs. asa + clop Noninferiority D/MI/TVR ISAR-SAFE 4,000 6 vs. 12* asa vs. asa + clop Noninferiority D/MI/CVA/ST, Bleed ITALIC 3,700 6 vs. 12 asa vs. asa + clop Noninferiority D/MI/CVA/Rev/MB OPTIMIZE 3,120 3 vs. 12 asa vs. asa + clop Noninferiority D/MI/CVA/MB RESET 2,148 3 vs. 12 asa vs. asa + clop Strategy CVD/MI/ST/TVR, Bleed SECURITY 1,399 6 vs 12 asa vs. asa + clop Noninferiority CD/MI/CVA/ST, Bleed Prolonged DAPT *Plus a 3M washout REAL/ZEST Late 2, vs. 24 asa vs. asa + clop Superiority D/MI DAPT 20, vs. 30* asa vs. asa + clop (pras) NI and Sup D/MI/CVA/ST, Bleed PRODIGY 1,800 6 vs. 24 asa vs. asa + clop Superiority D/MI/CVA ARCTIC Interr 1, vs 18 asa vs. asa + clop Superiority D/MI/CVA/TVR/ST
47


48

49

50

51

52

53
54 MACE reduction greater for patients with MI (3.9% vs. 6.8% HR 0.42 p < 0.001) compared with those with no MI (4.4% vs. 5.3% HR 0.60 p = 0.08) Yeh RW, et al. J Am Coll Cardiol 2015;65:
55 La durata della DAPT dopo SCA : dallo stent al paziente Changing the perspective : treat the patient not the stent LOV 2017
")





56 MACE (%) PROSPECT: MACE (N=697) All Culprit lesion (CL) related Non culprit lesion (NCL) related Indeterminate 20.4% % % 5 2.7% Time in Years Number at risk ALL CL related NCL related Indeterminate MACE = cardiac death, cardiac arrest, MI, or rehospitalization for unstable or progressive angina

57
58 Jernberg T et al. EurHJ 2015; 36:
59 Bhatt DL et al. JAMA 2010;304: %

60 Fox KAA et al. EurHJ 2010;31: %
61 PEGASUS-TIMI 54: Study Design Patients aged 50 years with a history of spontaneous MI 1 3 years prior to enrolment AND at least one additional atherothrombosis risk factor* (N=21,162) Ticagrelor 90 mg bid + ASA mg/day Ticagrelor 60 mg bid + ASA mg/day Placebo + ASA mg/day Minimum of 12 months follow up: Every 4 months in Year 1, then semi-annually Primary efficacy endpoint: CV death, MI or stroke Primary safety endpoint: TIMI-defined major bleeding *Age 65 years, diabetes mellitus, second prior MI, multivessel CAD or chronic non-end stage renal disease bid, twice daily; CAD, coronary artery disease; TIMI, Thrombolysis in Myocardial Infarction Bonaca MP et al. Am Heart J 2014;167: Bonaca MP et al. N Engl J Med 2015;372: FOR REACTIVE MEDICAL USE ONLY 61
62 LOV 2017
63
64 PEGASUS-TIMI 54: Efficacy Endpoints Endpoint 3-year KM event rates (%) Ticagrelor Placebo HR (95% CI) P value Primary CV death, MI or stroke (1558 events) CV death (566 events) MI (898 events) Stroke (313 events) ( ) ( ) ( ) ( ) ( ) ( ) ( ) 0.01* ( ) 0.03* ( ) 0.005* ( ) 0.14* ( ) 0.03* ( ) 0.03* Ticagrelor better Placebo better Ticagrelor 90 mg bid Ticagrelor 60 mg bid Ticagrelor pooled *Indicates nominal P value; P<0.026 indicates statistical significance Bonaca MP et al. N Engl J Med 2015;372: FOR REACTIVE MEDICAL USE ONLY 64
65 PEGASUS-TIMI 54: Primary Endpoint * by Subgroup (1) Subgroup Patients Ticagrelor 90 mg 3-year KM (%) Ticagrelor 60 mg 3-year KM (%) Placebo 3-year KM (%) HR (95% CI) ticagrelor 90 mg bid vs placebo HR (95% CI) Interaction P value HR (95% CI) ticagrelor 60 mg bid vs placebo HR (95% CI) Interaction P value All patients 21, ( ) 0.84 ( ) Age at randomisation <75 years 18, ( ) 0.86 ( ) 75 years ( ) 0.77 ( ) Sex Female ( ) 0.98 ( ) Male 16, ( ) 0.79 ( ) Qualifying MI NSTEMI ( ) 0.89 ( ) STEMI 11, ( ) 0.81 ( ) Unknown ( ) 0.74 ( ) Time from qualifying MI <2 years 12, ( ) 0.77 ( ) 2 years ( ) 0.96 ( ) History of diabetes Diabetes ( ) 0.83 ( ) No diabetes 14, ( ) 0.84 ( ) *Composite of CV death, MI or stroke KM, Kaplan-Meier Ticagrelor 90 mg better Placebo better Ticagrelor 60 mg better Placebo better Bonaca MP et al. N Engl J Med 2015;372: FOR REACTIVE MEDICAL USE ONLY 65

66 Bhatt DL, et al. JACC 2016;67: Magnani G, et al. EurHJ 2015;doi /eurheartj/ehv482 Bonaca M et al. JACC 2016;67:
67
68 Number of Patients Discontinued for Bleeding Discontinuation over time for Bleeding by Randomization Group 500 Placebo Ticagrelor 60 mg twice daily Ticagrelor 90 mg twice daily 450 P<0.01 for each dose vs. placebo Median Days to Discontinuation Days From Randomization An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Bonaca M et al. JAMA Cardiol 2016;1:
69 Number of events per 10,000 patients initiated on treatment per year PEGASUS-TIMI 54: Estimates of First Efficacy and Bleeding Events Prevented and Caused Annualized from 3-year Kaplan-Meier event rates in the intention-to-treat population Irreversible harm CV death, MI or stroke CV death MI Stroke Fatal bleeding ICH TIMI major bleeding Ticagrelor 90 mg bid Ticagrelor 60 mg bid -50 Net clinical benefit is defined as the comparison of first occurrence of CV death, MI or stroke with first occurrence of TIMI major bleeding; irreversible events are defined as CV death, MI, stroke, fatal bleeding and ICH Note these are estimated events based on calculations made from the observed ARRs in the PEGASUS-TIMI 54 study and therefore should be viewed as estimates of events prevented and caused rather than specific indicators of efficacy. Also note that these analyses are based on Kaplan-Meier time to first event curves, and therefore the sum of the events for CV death, MI and stroke individually do not equal that for the composite of CV death/mi/stroke Bonaca MP et al. N Engl J Med 2015;372: , Supplementary Appendix Data on file: ATLAS approval ID 773, FOR REACTIVE MEDICAL USE ONLY 69
70 La durata della DAPT dopo SCA : dallo stent al paziente Pegasus N events/1000 patients/year Ticagrelor 90 mg 60 mg Ischemic ev. prevented Bleeding LOV 2017


71 pts Charisma Prodigy Arctic-Int 323 DAPT DES-Late Pegasus
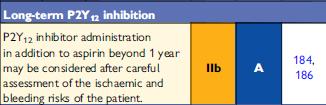
72 La durata della DAPT dopo SCA : dallo stent al paziente Who and when to treat after 12 months LOV 2017
73 La durata della DAPT dopo SCA : dallo stent al paziente Who Patients with prior MI at high risk: Diabetes mellitus Multiple prior MIs Renal dysfunction Multiple vascular disease Prior CABG PAD Not at high risk for bleeding Prior/risk of ICH Recent major Bleeding Bleeding diathesis On anticoagulation Anemia LOV 2017


74

75 The DAPT Score Variable Patient Characteristic Age Points Distribution of DAPT Scores among all randomized subjects in the DAPT Study <75-1 < 65 0 Diabetes Mellitus 1 Current Cigarette Smoker 1 Prior PCI or Prior MI 1 CHF or LVEF < 30% 2 Index Procedure Characteristic MI at Presentation 1 Vein Graft PCI 2 Stent Diameter < 3mm 1 75
76 Cumulative Incidence of GUSTO Moderate/ Severe Bleed Cumulative Incidence of ST/MI Cumulative Incidence of MACCE Continued Thienopyridine vs. Placebo DAPT Score 2 (High); N=5917 Myocardial Infarction or Stent Thrombosis 10% 8% Continued Thienopyridine Placebo Death, MI or Stroke (MACCE) 10% 8% Continued Thienopyridine Placebo 6% 4% 2.7% vs. 5.7% P< % 4% 4.9% vs. 7.6% P< % 2% 0% GUSTO Moderate/ Severe Bleeding Months After Enrollment 10% 8% 6% 4% 2% Continued Thienopyridine Placebo 1.8% vs. 1.4% P=0.26 0% Months After Enrollment 0% Months After Enrollment 76
77 Cumulative Incidence of GUSTO Moderate/ Severe Bleed Cumulative Incidence of ST/MI Cumulative Incidence of MACCE Continued Thienopyridine vs. Placebo DAPT Score <2 (Low); N=5731 Myocardial Infarction or Stent Thrombosis 10% 8% Continued Thienopyridine Placebo Death, MI, or Stroke (MACCE) 10% 8% Continued Thienopyridine Placebo 6% 6% 4% 1.7% vs. 2.3% P=0.07 4% 3.7% vs. 3.8% P=0.73 2% 2% 0% GUSTO Moderate/ Severe Bleeding Months After Enrollment 10% 8% 6% 4% 2% Continued Thienopyridine Placebo 3.0% vs. 1.4% P< % Months After Enrollment 0% Months After Enrollment 77
78 Complex PCI was defined (at least 1 of the following features) : 3 vessels treated 3 stents implanted 3 lesions treated bifurcation with 2 stents implanted total stent length >60 mm or chronic total occlusion Giustino G et al. JACC 2016;68:
79 La durata della DAPT dopo SCA : dallo stent al paziente When Continue after started for MI and re-evaluate at each visit: Recent bleeding? Are they tolerating? Are they adherent? Contraindications? (e.g. AF requiring anticoagulation) LOV 2017
80 Bonaca M et al. EurHJ 2016;37:
81 Bonaca M et al. EurHJ 2016;37:


82
 LOV")
83 La durata della DAPT dopo SCA : dallo stent al paziente Prolonging DAPT duration in ACS pts treat the patient not the stent one size may not fit all (carefully assessing the balance between thrombotic and bleeding risk) LOV 2016

84 Reed GW et al. Lancet 2017; 389:
85 Backup

86
87 Bonaca M et al. JAMA Cardiol 2016;1:
88
89 PEGASUS-TIMI 54: Safety Endpoints Endpoint Ticagrelor 90 mg bid N=6988; n (%) Ticagrelor 60 mg bid N=6958; n (%) Placebo N=6996; n (%) Ticagrelor 90 mg bid vs placebo HR (95% CI) Ticagrelor 60 mg bid vs placebo HR (95% CI) Primary safety endpoint TIMI major bleeding 127 (2.60) 115 (2.30) 54 (1.06) 2.69 ( ) P< ( ) P<0.001 Secondary safety endpoints ICH 29 (0.56) 28 (0.61) 23 (0.47) 1.44 ( ) P=0.19 Haemorrhagic stroke 4 (0.07) 8 (0.19) 9 (0.19) 0.51 ( ) P=0.26 Fatal bleeding 6 (0.11) 11 (0.25) 12 (0.26) 0.58 ( ) P=0.27 Fatal bleeding or nonfatal ICH 32 (0.63) 33 (0.71) 30 (0.60) 1.22 ( ) P= ( ) P= ( ) P= ( ) P= ( ) P=0.47 Rates are presented as 3-year Kaplan-Meier estimates n = number of patients with events, not the number of events Bonaca MP et al. N Engl J Med 2015;372: FOR REACTIVE MEDICAL USE ONLY 89
90 PEGASUS-TIMI 54: Safety Endpoints Endpoint Ticagrelor 90 mg bid N=6988; n (%) Ticagrelor 60 mg bid N=6958; n (%) Placebo N=6996; n (%) Ticagrelor 90 mg bid vs placebo HR (95% CI) Ticagrelor 60 mg bid vs placebo HR (95% CI) Secondary safety endpoints TIMI minor bleeding 66 (1.31) 55 (1.18) 18 (0.36) 4.15 ( ) P< ( ) P<0.001 Bleeding requiring transfusion Bleeding leading to study drug discontinuation 122 (2.43) 105 (2.09) 37 (0.72) 3.75 ( ) P< (7.81) 354 (6.15) 86 (1.50) 5.79 ( ) P< ( ) P< ( ) P<0.001 Rates are presented as 3-year Kaplan-Meier estimates n = number of patients with events, not the number of events Bonaca MP et al. N Engl J Med 2015;372: FOR REACTIVE MEDICAL USE ONLY 90
91 yspnea Bleeding E) Serious (SAE) 5% mild or moderate TIMI Major Med Attention TIMI Minor Minimal % mild or moderate icagrelor 0 mg BID 8 11 Ticagrelor 60 mg BID Placebo Ticagrelor 90 Ticagrelor 60 mg BID mg BID Bonaca M et al. JAMA Cardiol 2016;1:

92

 m unchanged stent thrombosis reduced")
,")
93 Optimal duration of antiplatelet treatment after ACS Compared to 12 months of DAPT administration short (3 or 6 m) > 12 (30?) m unchanged stent thrombosis reduced unchanged MACCE* reduced reduced bleeding increased * = mortality (total, CV, non-cv), MI, stroke LOV 2015
94 Jernberg T et al. EurHJ 2015; 36:
95 PEGASUS-TIMI 54: Primary Endpoint * by Subgroup (2) Subgroup Patients Ticagrelor 90 mg 3-year KM (%) Ticagrelor 60 mg 3-year KM (%) Placebo 3-year KM (%) HR (95% CI) ticagrelor 90 mg bid vs placebo HR (95% CI) Interaction P value HR (95% CI) ticagrelor 60 mg bid vs placebo HR (95% CI) Interaction P value All patients 21, ( ) 0.84 ( ) ASA dose mg ( ) 0.82 ( ) >75 mg 16, ( ) 0.85 ( ) History of PCI Prior PCI 17, ( ) 0.83 ( ) No prior PCI ( ) 0.87 ( ) Region North America ( ) 0.75 ( ) South America ( ) 0.90 ( ) Europe 12, ( ) 0.85 ( ) Asia ( ) 0.90 ( ) Ticagrelor 90 mg better Placebo better Ticagrelor 60 mg better Placebo better *Composite of CV death, MI or stroke Bonaca MP et al. N Engl J Med 2015;372: FOR REACTIVE MEDICAL USE ONLY 95
96 PEGASUS-TIMI 54: Primary Endpoint * by Subgroup (3) Subgroup Patients Ticagrelor 90 mg 3-year KM (%) Ticagrelor 60 mg 3-year KM (%) Placebo 3-year KM (%) HR (95% CI) ticagrelor 90 mg bid vs placebo HR (95% CI) Interaction P value HR (95% CI) ticagrelor 60 mg bid vs placebo HR (95% CI) Interaction P value All patients 21, ( ) 0.84 ( ) Race Caucasian 18, ( ) 0.81 ( ) Non-Caucasian ( ) 1.07 ( ) Weight < Median (81 kg) 10, ( ) 0.77 ( ) Median (81 kg) 10, ( ) 0.91 ( ) Second prior MI Second MI ( ) 0.85 ( ) No second MI 17, ( ) 0.83 ( ) Multivessel disease Multivessel 12, ( ) 0.81 ( ) disease No multivessel disease ( ) 0.88 ( ) Non-endstage renal dysfunction Renal dysfunction No renal dysfunction ( ) 0.81 ( ) 16, ( ) 0.88 ( ) *Composite of CV death, MI or stroke n = number of patients with events, not the number of events Bonaca MP et al. N Engl J Med 2015;372: Ticagrelor 90 mg better Placebo better Ticagrelor 60 mg better Placebo better FOR REACTIVE MEDICAL USE ONLY 96
97 Storey RF, et al. JACC 2016;67:
98 La doppia antiaggregazione prolungata : gli aggiornamenti dal PEGASUS robusto disegno e risultati convincenti coerenza dei risultati in numerosi sottogruppi prespecificati spalanca il focus sul paziente stabile nella fase successiva a una sindrome coronarica acuta LOV 2016
99 DAPT Duration for Complex PCI Patient-level meta-analysis of 9,577 pts from 6 PCI trials of DAPT duration Definite or probable stent thrombosis P for interaction = ,6% 0,8% 0,5% 0,5% Complex PCI Noncomplex PCI Long DAPT Short DAPT Complex PCI was defined as having at least 1 of the following features: 3 vessels treated, 3 stents implanted, 3 lesions treated, bifurcation with 2 stents implanted, total stent length >60 mm, or chronic total occlusion Giustino G et al. JACC 2016;68:
100 DAPT a lungo termine : un nuovo paradigma Il rischio residuo del paziente nella pratica clinica It s time to re-focus our attention and resources on the chronic phase after an acute coronary event LOV 2017

 Post-MI Registry 230")
101 The EYESHOT Post-MI Snapshot EYESHOT (EmploYEd antithrombotic therapies in patients with acute coronary Syndromes HOspitalized in italy) Post-MI Registry 230 centers 3 months duration

102 Number of Patients Discontinued for Dyspnea Discontinuation over time for Dyspnea by Randomization Group 500 Placebo Ticagrelor 60 mg twice daily Ticagrelor 90 mg twice daily 450 P<0.01 for each dose vs. placebo Median Days to Discontinuation Days From Randomization An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Bonaca M et al. JAMA Cardiol 2016;1:



103 Protease-activated receptor (PAR)-1 Thrombin Vorapaxar C C C C Vorapaxar is an oral, potent, and selective antagonist of PAR-1 Metabolism by CYP3A4 enzymes No meaningful renal clearance Long half-life (T1/2 > 100 hrs) XSignal Shape Change Activation Aggregation Adapted from Vu TH et al. Cell 1991;64:


104 Event Rate (%) CV Death, MI, or Stroke 12% 10% 8% 6% N = Mean f/u: 2.5 years Hazard Ratio 0.87 p < Background 1 Efficacy Evaluation Overall Population Placebo Vorapaxar 10.5% 9.3% 4% 2% GUSTO Mod/Sev at 3 yrs 4.2 v. 2.5%, HR 1.66, p< % Days since randomization Morrow et al. N Engl J Med 2012 ClinicalTrials.gov NCT c

105 Event Rate (%) Primary Efficacy Evaluation Prior MI Cohort 12% 10% 8% 6% CV Death, MI, or Stroke N = 17,779 Mean f/u: 2.5 years Hazard Ratio 0.80; 95% CI p < Placebo 9.7% 8.1% Vorapaxar 4% 2% 0% Vora Plac HR P-value CV Death MI <0.001 Stroke Days since Randomization
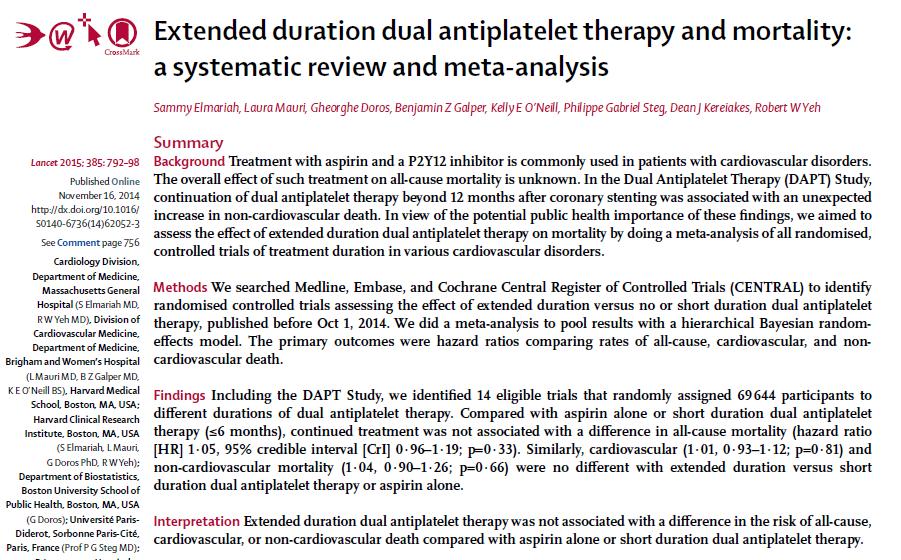
Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta
 Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta Giuseppe Musumeci SC Cardiologia Ospedale Santa Croce e Carle Cuneo
Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta Giuseppe Musumeci SC Cardiologia Ospedale Santa Croce e Carle Cuneo
Dual Antiplatelet duration in ACS: too long or too short?
 Dual Antiplatelet duration in ACS: too long or too short? Leonardo Bolognese, MD, FESC, FACC Cardiovascular Department, Arezzo, Italy Paradigm Shift the ideal duration of DAPT: a moving target Early (stent-related)
Dual Antiplatelet duration in ACS: too long or too short? Leonardo Bolognese, MD, FESC, FACC Cardiovascular Department, Arezzo, Italy Paradigm Shift the ideal duration of DAPT: a moving target Early (stent-related)
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Lo studio Pegasus: il ruolo di Ticagrelor dopo i primi 12 mesi di trattamento. C. Cavallini Perugia
 Lo studio Pegasus: il ruolo di Ticagrelor dopo i primi 12 mesi di trattamento C. Cavallini Perugia PEGASUS-TIMI 54: Aspetti qualificanti Tutti Pazienti Post-MI Tutti Pazienti stabili (>1 anno) STUDIO DI
Lo studio Pegasus: il ruolo di Ticagrelor dopo i primi 12 mesi di trattamento C. Cavallini Perugia PEGASUS-TIMI 54: Aspetti qualificanti Tutti Pazienti Post-MI Tutti Pazienti stabili (>1 anno) STUDIO DI
Antithrombotic Therapy for Long-Term Secondary Prevention Considerations for Long-Term DAPT
 Antithrombotic Therapy for Long-Term Secondary Prevention Considerations for Long-Term DAPT Marc P. Bonaca, MD, MPH Vascular Section, Cardiovascular Division Investigator TIMI Study Group Brigham and Women
Antithrombotic Therapy for Long-Term Secondary Prevention Considerations for Long-Term DAPT Marc P. Bonaca, MD, MPH Vascular Section, Cardiovascular Division Investigator TIMI Study Group Brigham and Women
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
PAR-1 Antagonist: What Do Clinical Trials Teach Us?
 Prevention of Atherothrombotic Events: What s the New Evidence? PAR-1 Antagonist: What Do Clinical Trials Teach Us? David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care Unit Senior Investigator,
Prevention of Atherothrombotic Events: What s the New Evidence? PAR-1 Antagonist: What Do Clinical Trials Teach Us? David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care Unit Senior Investigator,
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Προβληματισμοι στην χρηση αντιαιμοπεταλιακων στα οξέα ισχαιμικά σύνδρομα
 Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΚΑΙ ΟΜΩΝΥΜΟ ΕΡΓΑΣΤΗΡΙΟ ΙΑΤΡΙΚΗ ΣΧΟΛΗ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΑΘΗΝΩΝ ΙΠΠΟΚΡΑΤΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ ΑΘΗΝΩΝ Διευθυντής: Καθηγητής ΔΗΜΗΤΡΙΟΣ ΤΟΥΣΟΥΛΗΣ Προβληματισμοι στην χρηση αντιαιμοπεταλιακων
Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΚΑΙ ΟΜΩΝΥΜΟ ΕΡΓΑΣΤΗΡΙΟ ΙΑΤΡΙΚΗ ΣΧΟΛΗ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΑΘΗΝΩΝ ΙΠΠΟΚΡΑΤΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ ΑΘΗΝΩΝ Διευθυντής: Καθηγητής ΔΗΜΗΤΡΙΟΣ ΤΟΥΣΟΥΛΗΣ Προβληματισμοι στην χρηση αντιαιμοπεταλιακων
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events
 Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Disclosures. Dr. Scirica has also served as a consultant for Lexicon, Arena, Gilead, and Eisai.
 Disclosures Benjamin M. Scirica, MD, MPH, is employed by the TIMI Study Group, which has received research grants from Abbott, AstraZeneca, Amgen, Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb,
Disclosures Benjamin M. Scirica, MD, MPH, is employed by the TIMI Study Group, which has received research grants from Abbott, AstraZeneca, Amgen, Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb,
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS. Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands
 DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands RECENT DEVELOPMENTS Better anti-platelet agents: Prasugrel and Ticagrelor to replace
DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands RECENT DEVELOPMENTS Better anti-platelet agents: Prasugrel and Ticagrelor to replace
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Great debate: thrombocardiology post-compass
 The Great debate: thrombocardiology post-compass Anticoagulation should replace antiplatelets in CAD prevention - CON Jean-Philippe COLLET Jean-philippe.collet@psl.aphp.fr Sorbonne Université_Action Study
The Great debate: thrombocardiology post-compass Anticoagulation should replace antiplatelets in CAD prevention - CON Jean-Philippe COLLET Jean-philippe.collet@psl.aphp.fr Sorbonne Université_Action Study
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A new era in the treatment of peripheral artery disease (PAD)?
?") A new era in the treatment of peripheral artery disease (PAD)? Prof. Dr. Jan Beyer-Westendorf Head of Thrombosis Research, University Hospital Carl Gustav Carus, TU Dresden; Germany Senior Lecturer Thrombosis
A new era in the treatment of peripheral artery disease (PAD)? Prof. Dr. Jan Beyer-Westendorf Head of Thrombosis Research, University Hospital Carl Gustav Carus, TU Dresden; Germany Senior Lecturer Thrombosis
1. Whether the risks of stent thrombosis (ST) and major adverse cardiovascular and cerebrovascular events (MACCE) differ from BMS and DES
 and major adverse cardiovascular and cerebrovascular events (MACCE) differ from BMS and DES") 1 Comparison of Ischemic and Bleeding Events After Drug- Eluting Stents or Bare Metal Stents in Subjects Receiving Dual Antiplatelet Therapy: Results from the Randomized Dual Antiplatelet Therapy (DAPT)
1 Comparison of Ischemic and Bleeding Events After Drug- Eluting Stents or Bare Metal Stents in Subjects Receiving Dual Antiplatelet Therapy: Results from the Randomized Dual Antiplatelet Therapy (DAPT)
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון מרכז רפואי רבין
 תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Is there enough evidence for DAPT after endovascular intervention for PAOD?
 Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
P 2 Y 12 Receptor Inhibitors
 P 2 Y 12 Receptor Inhibitors Clopidogrel, Prasugrel and Ticagrelor Which Drug and for Whom? Cheol Whan Lee, MD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical
P 2 Y 12 Receptor Inhibitors Clopidogrel, Prasugrel and Ticagrelor Which Drug and for Whom? Cheol Whan Lee, MD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical
SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable?
 SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable? tielle est 2 ré Totielle est interdite. Prof. Marco Roffi Hôpitaux Universitaires de Genève Research funding
SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable? tielle est 2 ré Totielle est interdite. Prof. Marco Roffi Hôpitaux Universitaires de Genève Research funding
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Triple Therapy: A review of the evidence in acute coronary syndrome. Stephanie Kling, PharmD, BCPS Sanford Health
 Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
DAPT in CAD, Acute & Chronic CAD, antiplatelet therapy non-responders
 DAPT in CAD, Acute & Chronic CAD, antiplatelet therapy non-responders Annual Ohio ACC Conference October 14, 2017 Ernest L. Mazzaferri Jr, MD, FACC, FSCAI Disclosures No financial disclosures related to
DAPT in CAD, Acute & Chronic CAD, antiplatelet therapy non-responders Annual Ohio ACC Conference October 14, 2017 Ernest L. Mazzaferri Jr, MD, FACC, FSCAI Disclosures No financial disclosures related to
7 th Munich Vascular Conference
 7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
10 Steps to Managing Non-ST Elevation ACS
 Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
Subsequent management and therapies
 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study
 ESC, Hotline III, Paris, August, 30, 2011 PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study M. Valgimigli, MD, PhD University of Ferrara, ITALY On behalf of the
ESC, Hotline III, Paris, August, 30, 2011 PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study M. Valgimigli, MD, PhD University of Ferrara, ITALY On behalf of the
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs
 Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας. A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο
 Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο Europe* 2001 2011 Incident MI 291,100 327,700 US 2001 2011 Incident MI 405,100 485,200
Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο Europe* 2001 2011 Incident MI 291,100 327,700 US 2001 2011 Incident MI 405,100 485,200
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor
 Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Clopidogrel vs New Antiplatelet Therapy (Prasugrel) Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany
 Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany") Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
TRIAL UPDATE 1. ISAR TRIPLE SECURITY Trial. Dr Deven Patel Royal Free Hospital
 TRIAL UPDATE 1 ISAR TRIPLE SECURITY Trial Dr Deven Patel Royal Free Hospital NO CONFLICT OF INTEREST TO DECLARE ISAR TRIPLE Comparison of 6 weeks vs 6 months Triple Therapy in patients on oral anticoagulation
TRIAL UPDATE 1 ISAR TRIPLE SECURITY Trial Dr Deven Patel Royal Free Hospital NO CONFLICT OF INTEREST TO DECLARE ISAR TRIPLE Comparison of 6 weeks vs 6 months Triple Therapy in patients on oral anticoagulation
P2Y 12 blockade. To load or not to load before the cath lab?
 UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
How Long Patietns Will Be on Dual Antiplatelet Therapy?
 How Long Patietns Will Be on Dual Antiplatelet Therapy? Ron Waksman,, MD, FACC Professor of Medicine (Cardiology) Georgetown University Associate Director, Division of Cardiology, Washington Hospital Center
How Long Patietns Will Be on Dual Antiplatelet Therapy? Ron Waksman,, MD, FACC Professor of Medicine (Cardiology) Georgetown University Associate Director, Division of Cardiology, Washington Hospital Center
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Angioplastica coronarica nel paziente anziano ad alto rischio emorragico
 Attualità in Cardiologia Aprilia, Enea Hotel 22 ottobre 2011 Angioplastica coronarica nel paziente anziano ad alto rischio emorragico Fabrizio Tomai, MD, FACC, FESC Dept. of Cardiovascular Sciences - Interventional
Attualità in Cardiologia Aprilia, Enea Hotel 22 ottobre 2011 Angioplastica coronarica nel paziente anziano ad alto rischio emorragico Fabrizio Tomai, MD, FACC, FESC Dept. of Cardiovascular Sciences - Interventional
Case Challenges in ACS The Very Elderly in the Cath Lab
 Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Re- Setting our COMPASS for Secondary Prevention in Atherosclerotic Vascular Disease
 Re- Setting our COMPASS for Secondary Prevention in Atherosclerotic Vascular Disease Robert C. Welsh, MD, FRCPC Professor of Medicine, University of Alberta Zone Clinical Department Head, Cardiac Sciences
Re- Setting our COMPASS for Secondary Prevention in Atherosclerotic Vascular Disease Robert C. Welsh, MD, FRCPC Professor of Medicine, University of Alberta Zone Clinical Department Head, Cardiac Sciences
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Antiplatelet in diabetics: strong but incomplete umbrella
 Antiplatelet in diabetics: strong but incomplete umbrella Seung-Whan Lee, MD. Heart Institute, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea Global Projections for the Number
Antiplatelet in diabetics: strong but incomplete umbrella Seung-Whan Lee, MD. Heart Institute, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea Global Projections for the Number
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome'
 'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Clopidogrel Use in ACS and PCI: Clinical Trial Update
 Clopidogrel Use in ACS and PCI: Clinical Trial Update Matthew J. Price MD Director, Cardiac Catheterization Laboratory, Scripps Clinic, La Jolla, CA Assistant Professor, Scripps Translational Science Institute
Clopidogrel Use in ACS and PCI: Clinical Trial Update Matthew J. Price MD Director, Cardiac Catheterization Laboratory, Scripps Clinic, La Jolla, CA Assistant Professor, Scripps Translational Science Institute
Anti-platelet therapies and dual inhibition in practice
 Anti-platelet therapies and dual inhibition in practice Therapeutics; Sept. 25 th 2007 Craig Williams, Pharm.D. Associate Professor of Pharmacy Objectives 1. Understand the pharmacology of thienopyridine
Anti-platelet therapies and dual inhibition in practice Therapeutics; Sept. 25 th 2007 Craig Williams, Pharm.D. Associate Professor of Pharmacy Objectives 1. Understand the pharmacology of thienopyridine
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
Does COMPASS Change Practice?
 Does COMPASS Change Practice? C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division Chairman, PERFUSE Study Group Founder,
Does COMPASS Change Practice? C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division Chairman, PERFUSE Study Group Founder,
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
New insights in stent thrombosis: Platelet function monitoring. Franz-Josef Neumann Herz-Zentrum Bad Krozingen
 New insights in stent thrombosis: Platelet function monitoring Franz-Josef Neumann Herz-Zentrum Bad Krozingen New insights in stent thrombosis: Platelet function monitoring Variability of residual platelet
New insights in stent thrombosis: Platelet function monitoring Franz-Josef Neumann Herz-Zentrum Bad Krozingen New insights in stent thrombosis: Platelet function monitoring Variability of residual platelet
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
The Korean Society of Cardiology COI Disclosure
 The Korean Society of Cardiology COI Disclosure Name of First Author: Yongwhi Park The authors have no financial conflicts of interest to disclose concerning the presentation 2017 Annual Spring Scientific
The Korean Society of Cardiology COI Disclosure Name of First Author: Yongwhi Park The authors have no financial conflicts of interest to disclose concerning the presentation 2017 Annual Spring Scientific
Disclosure Slide. Controversies in Anticoagulation. Presenter Disclosure Information. Challenges in Anticoagulation
 1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
Stable CAD, Elective Stenting and AFib
 Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease
 Interventional Cardiology and Cath Labs The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease Manesh R. Patel MD Chief,
Interventional Cardiology and Cath Labs The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease Manesh R. Patel MD Chief,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
A patient with an acute coronary syndrome one year ago. Options for antiplatelet treatment
 A patient with an acute coronary syndrome one year ago. Options for antiplatelet treatment Ronen Durst, MD Cardiology Department Hadassah, Hebrew University Medical Center. Chairman, Israeli society for
A patient with an acute coronary syndrome one year ago. Options for antiplatelet treatment Ronen Durst, MD Cardiology Department Hadassah, Hebrew University Medical Center. Chairman, Israeli society for
New antiplatelets in NSTEMI. Overview: dual anti-platelet oral therapy
 Cairo, Egypt 2010 New antiplatelets in NSTEMI Steen D. Kristensen, FESC Department of Cardiology Aarhus University Hospital Skejby Denmark Overview: dual anti-platelet oral therapy Aspirin Clopidogrel
Cairo, Egypt 2010 New antiplatelets in NSTEMI Steen D. Kristensen, FESC Department of Cardiology Aarhus University Hospital Skejby Denmark Overview: dual anti-platelet oral therapy Aspirin Clopidogrel
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο)
") Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017
 EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor
 Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor Nicolas W. Shammas, MS, MD, FACC Coronary and Peripheral Interventionalist Cardiovascular Medicine, PC Research Director,
Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor Nicolas W. Shammas, MS, MD, FACC Coronary and Peripheral Interventionalist Cardiovascular Medicine, PC Research Director,
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
La terapia antiaggregante nel paziente con stroke
 La terapia antiaggregante nel paziente con stroke Paolo Gresele Dipartimento di Medicina, Sez. Medicina Interna e Cardiovascolare Università di Perugia XXVII Congresso Nazionale FCSA Milano, 20-22 Ottobre
La terapia antiaggregante nel paziente con stroke Paolo Gresele Dipartimento di Medicina, Sez. Medicina Interna e Cardiovascolare Università di Perugia XXVII Congresso Nazionale FCSA Milano, 20-22 Ottobre
Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI
 Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI Ομάδες Εργασίας Φεβρουάριος 2016 Ξανθοπούλου Ιωάννα Καρδιολόγος Επιμ Β ΠΓΝΠατρών Nothing to disclose Platelet function testing (PFT) is helpful in identifying
Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI Ομάδες Εργασίας Φεβρουάριος 2016 Ξανθοπούλου Ιωάννα Καρδιολόγος Επιμ Β ΠΓΝΠατρών Nothing to disclose Platelet function testing (PFT) is helpful in identifying
ISCHEMIC HEART DISEASE
 ESC CONGRESS HIGHLIGHTS ISCHEMIC HEART DISEASE Francesco Cosentino (Stockholm, S) Declaration of Interest Advisory Board/Speaker: AstraZeneca, Roche, Boehringer-Ingelheim, Bristol-Myers Squibb, Merck,
ESC CONGRESS HIGHLIGHTS ISCHEMIC HEART DISEASE Francesco Cosentino (Stockholm, S) Declaration of Interest Advisory Board/Speaker: AstraZeneca, Roche, Boehringer-Ingelheim, Bristol-Myers Squibb, Merck,
Why and How Should We Switch Clopidogrel to Prasugrel?
 Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Optimal medical therapy in patients with stable CAD
 Optimal medical therapy in patients with stable CAD Robert Storey Professor of Cardiology, University of Sheffield and Academic Director and Honorary Consultant Cardiologist, Cardiology and Cardiothoracic
Optimal medical therapy in patients with stable CAD Robert Storey Professor of Cardiology, University of Sheffield and Academic Director and Honorary Consultant Cardiologist, Cardiology and Cardiothoracic
Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis Alaide Chieffo
 Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis 11.45-12.07 Alaide Chieffo San Raffaele Scientific Institute, Milan, Italy Historical Perspective 25 20 15 10 5 0 Serruys 1991
Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis 11.45-12.07 Alaide Chieffo San Raffaele Scientific Institute, Milan, Italy Historical Perspective 25 20 15 10 5 0 Serruys 1991
Byeong-Keuk Kim, M.D. Ph D. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, M.D. Ph D Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea CASE, M/64 C.C; Recently aggravated chest discomfort for 3 days
Byeong-Keuk Kim, M.D. Ph D Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea CASE, M/64 C.C; Recently aggravated chest discomfort for 3 days
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
ANTIPLATELET REGIMENS:
 ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia
 GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin
 Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin Marc S. Sabatine, MD, MPH on behalf of the PEGASUS-TIMI 54 Executive
Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin Marc S. Sabatine, MD, MPH on behalf of the PEGASUS-TIMI 54 Executive
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial Outcomes in patients with and planned PCI Ph.Gabriel Steg*, Stefan James, Robert A
compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial Outcomes in patients with and planned PCI Ph.Gabriel Steg*, Stefan James, Robert A