Maresce Bizaare AWACC 2013
|
|
|
- Kevin Price
- 5 years ago
- Views:
Transcription

1 Maresce Bizaare AWACC 2013
2 Cytopaenias in HIV Most common complication of HIV Anaemia is most common cytopaenia ITP occurs in 30%, may be first manifestation of HIV
3 Laboratory approach to cytopaenia FBC, diff, smear Retic count haemolysis/peripheral loss or production problem UE/LFT/LDH/CMP Nutritional deficiencies: B12/Folate/Iron studies Hepatitis B/EBV/Parvo BMAT low threshold
4 Some causes of Anaemia Decreased RBC production HIV itself Opportunistic infections Drugs Nutritional deficiencies Malignancy Increased Red cell loss Haemolysis Blood loss Hypersplenism
5 Drugs causing cytopaenias Drug AZT D4T Bactrim INH/Rifampicin Fluconazole Cytopaenia Anaemia, Neutropaenia Neutropaenia, thrombocytopaenia Anaemia, Neutropaenia, Thrombocytopaenia Anaemia, Neutropaenia, Thrombocytopaenia Anaemia, Leucopaenia, Thrombocytopaenia
6 Case 1 Ms PN Consulted for patient with Bicytopaenia 35/40 pregnant From History: On HAART, CD4 235, started in pregnancy, uncertain VL Diagnosed 11 weeks previously with B12 deficiency, had received B12 injections Hb was 6,4 at time, now 11.3 Persistently low plts -->last count 54 Normal WCC No renal impairment
7 Investigations Normal MCV/MCH Coombs negative B12 started to improve (low normal) / Folate normal Iron studies normal Hep B negative Rest of viral screen was negative US abdomen nad Impression: Multifactorial causes B12 deficiency, corrected with injections-> accounts for improving Hb Low platelets (?ITP/ pregnancy related thrombocytopaenia)
8 Management plan Review history: No transfusions, only had 2x B12 injections Assessment: B12 deficiency (Inadequately replaced) and? ITP Plan: Replace B12 appropriately Start prednisone Patient delivered few days later Reviewed in clinic 2/52 later FBC completely normal with plts of 233
9 Learning point Good history Replace B12 appropriately 1000mcg x 5/7 weekly x 4/52 monthly
10 Thrombocytopaenia Thrombotic Thrombocytopaenic Purpura (TTP) ITP Drugs Opportunistic infections Hypersplenism (due to chronic liver disease) Malignancy
11 Isolated Thrombocytopaenia Low threshold to do a BMAT Might pick up Bone marrow infiltrations or opportunistic infections Prednisone 1mg/kg/day Polygam to optimise for surgery Splenectomy Prophylaxis Vaccines: Pneumococcal and Meningococcal prior to splenectomy Pen VK 250mg bd (2 years)
12 Case 2 Ms SB 16 years old Pregnant 24/40 CD4 356, HAART naïve Initial complaint: Lower abdominal pain and haematuria Examination: Apyrexial, pallor, no lymphadenopathy Petechiae + No chronic liver disease, no hepatosplenomegaly No neurological impairment
13 Initial investigations FBC: HB 7.3 Plts 24 WCC 10 UE/LFT normal, LDH elevated -882 (N: ) Iron studies normal B12/Folate normal INR normal ANF neg Coombs neg
14 Initial management Smear not followed up ITP suspected Started on steroids Haematology consulted after 10/7 when no platelet increment noted
15
16 Considerations in patient HIV associated TTP Unlikely: HIV associated ITP Gestational thrombocytopenia
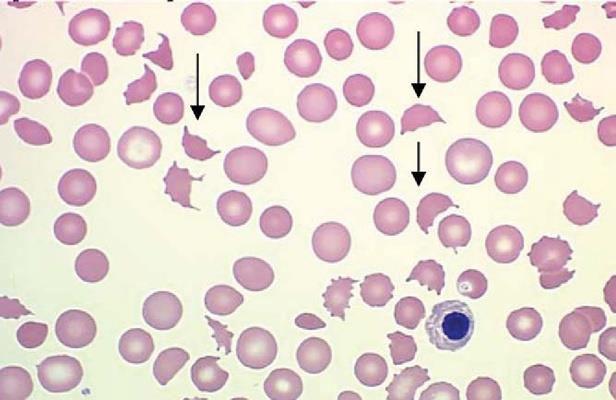
17 TTP Pentad Thrombocytopenia Microangiopathic Haemolytic Anaemia (MAHA) Fluctuating neurological signs Renal impairment Fever
18 Differences No classical Pentad Pathogenesis is different Treatment is different: Responds to plasma infusion, rate of relapse low, HAART essential
19 HIV: A changing landscape Incidence 15-40x that of non-infected individuals >80% of TTP cases in SA found to be HIV+ Missed diagnosis
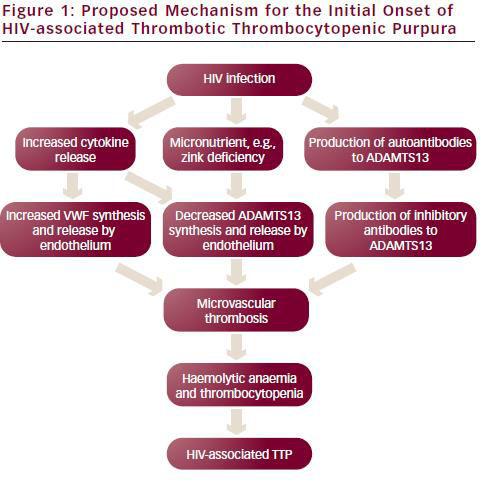
20 HIV associated TTP TTP may be the initial presenting feature of HIV disease Remission is dependent upon improving the immune status of the patient.
21
22
23 Evidence for Plasma infusion Prospective study by Novitsky et al Groote Schuur Hospital Compared HIV associated TTP with HIV negative TTP All HIV+ patients responded to FFP infusions and their platelet count and serum LDH levels normalized significantly faster than the HIV negative group
24 Treatment of HIV-TTP Plasma infusion FDP (Freeze dried plasma) 30ml/kg/day (can add loop diuretic) Adjunctive corticosteroids Prednisone 1mg/kg/day Folate Aspirin once plts > 100 If no response in 72 hours plasma exchange
25 Outcome of patient Platelet count DOA 24 Consult: 13 2/7 of FFP 53 4/7 of FFP 132 8/7 of FFP 229
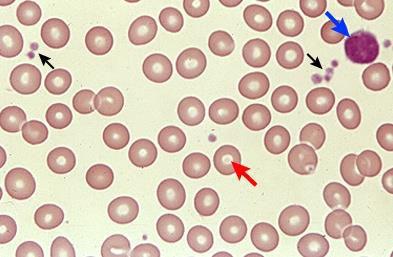
26 Differences between ITP and TTP ITP TTP Clinical Bleeding Clotting Multi-organ involvement Laboratory No fragments Fragments Treatment HAART steroids HAART Steroids FDP Plasma exchange
27 Case 3 Ms ZN 35 years old referred from EDH HAART for 3 years CD4 395, undetectable Viral load Constitutional symptoms TB x3 in past, last 1 sensitive AFB + TB Examination revealed pallor and lymphadenopathy
28 investigations FBC: Hb 9.8 NNA, Wcc 3.53 (ANC 1.28) Plts 282 Smear : no fragments Calcium and LDH were elevated US abdomen showed numerous lymph nodes Lymph node biopsy was done
29 Burkitts lymphoma Very aggressive B cell NHL 1 st lymphoma associated with HIV Incidence increasing in HAART era > 200x fold increase in HIV population HAART not decreased incidence 40% associated with EBV Rapidly dividing, doubling time of hours
30 Burkitt Lymphoma More common when CD4 > 200 Chronic antigenic stimulation of B cells by chronic HIV infection may be the pathogenetic mechanism Responds to chemotherapy HAART has allowed the use of high dose chemotherapy regimens
31 Alar bells ri g.. Clinically: Lymphadenopathy, Heposplenomegaly Jaundice, pyrexia Laboratory: Cytopaenias Elevated WCC (circulating blasts: Burkitts leukaemia) LDH/ Ca elevated K+ elevated Renal impairement
32 Tumor Lysis Syndrome High proliferation rate Suspect if bulky disease Present with: Hyperkalaemia Hyperuricaemia Hyperphosphataemia Renal failure Management: Fluids Urinary alkalinisation Allopurinol
33 Case 4 30 year old Ms GS HAART since June 2013 Nadir CD , (3/12 later), VL uncertain TB 2/52 prior to HAART (CXR changes, constitutional symptoms) Persisting symptoms, sternal mass started to slowly form Anaemia, thrombocytopaenia Extensively investigated for MDR-TB
34 Examination Pallor, no lymphadenopathy Sternal mass Temporal mass Hepatosplenomegaly
35 Co ti uatio.. Investigations: Microcytic Hypochromic anaemia Hb 9.7, plts 112 Normal Ca Elevated LDH >1000 CT : TB spondylitis, features of bronchiectasis, Erosive lesion in relation to manubrium sternum, multiple abdominal lymphadenopathy Hepatomegally with multiple lesions Homogenously enlarged spleen Biopsy of sternal mass: DLBCL
36 Discussion on Diffuse Large B Cell Lymphoma (DLBCL) Most common histological subtype of NHL Incidence in SA is increasing exponentially primarily due to HIV pandemic Most patients symptomatic at presentation Constitutional symptoms, lymphadenopathy, hepatosplenomegaly, bone marrow involvement and cytopaenias more common in advanced stage Comorbidities such as TB increase the frequency and severity of clinical manifestations
37 Discussion Multiple pathologies for cytopaenias In this case: DLBCL and concomitant TB High index of suspicion in patient not improving on TB treatment Biopsy, Biopsy, Biopsy
38 Summary: What to consider in patients with Cytopaenias HIV induced Nutritional deficiency Opportunistic infections (eg TB) If Thrombocytopaenia: ITP / TTP Malignancy
39 Indications for BMAT in HIV+ Unexplained anaemia, abnormal red cell indices, cytopenias Isolated thrombocytopenias Unexplained organomegaly or presence of mass lesions inaccessible for biopsy Microbiological culture for investigation of PUO
40 Case 5 Mr TZ, 34 years old Pulmonary embolus, Right DVT HAART naïve, CD4 89 Examination and rest of baseline laboratory workup was essentially normal
41 Acquired Thrombophilia in HIV population Common Unusual sites common Risk highest with advanced disease (low CD4 and high VL) and co-existing infection and malignancies Contributors to Hypercoaguable state: Increased VWF High incidence of lupus anticoagulant and antiphospholipid antibodies Acquired Protein C and S deficiency
42 Management HAART Prophylaxis in hospitalised immobile patients Thrombophilia testing expensive NB: False + low titres of Antiphospholipid antibodies common
43 Thank you for your time and attention
44 References and acknowledgements OPIE, Jessica. Haematological complications of HIV Infection.SAMJ, [S.l.], v. 102, n. 6, p , mar ASH 2012: Guidelines on the diagnosis and management of TTP and other thrombotic microangiopathies ASH 2012: How to approach thrombocytopenia BJH 2005: Thrombotic thrombocytopenic purpura in patients with retroviral infection is highly responsive to plasma infusion therapy European Oncology and Haematology 2012: HIV-associated Thrombotic Thrombocytopenic Purpura Postgraduate Haematology 2011 Dr JP Singh, Dr N Sewpersad (IALCH department of Haematolgy) Various patients
Cytopaenias in HIV. Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH
 Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
 DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital
 Ray Mun Koo Haematology Advanced Trainee Canberra Hospital") Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
The Bleeding Patient. Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand
 The Bleeding Patient Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand The Bleeding Patient If you prick us, do we not bleed? Disorders of secondary homeostasis: dysfunction
The Bleeding Patient Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand The Bleeding Patient If you prick us, do we not bleed? Disorders of secondary homeostasis: dysfunction
Things to never miss in the office. Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC
 Leonard Minuk MD FRCPC") Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
BBTS Advanced Clinical and laboratory case studies. Therese Callaghan
 BBTS 2017 Advanced Clinical and laboratory case studies Therese Callaghan Disclaimer Nothing to disclose A 52 year old man with history of paranoid schizophrenia presents to A&E with history of abdominal
BBTS 2017 Advanced Clinical and laboratory case studies Therese Callaghan Disclaimer Nothing to disclose A 52 year old man with history of paranoid schizophrenia presents to A&E with history of abdominal
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
A 60 year old woman with altered mental status and thrombotic microangiopathy. Josh Veatch
 A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Thrombocytopenia: a practial approach
 Thrombocytopenia: a practial approach Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Outline Introduction and
Thrombocytopenia: a practial approach Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Outline Introduction and
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Part 1 examination. Haematology: First paper. Tuesday 20 March Candidates must answer all questions. Each question is worth a total of 25 marks.
 Part 1 examination Haematology: First paper Tuesday 20 March 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours Question 1: General Haematology
Part 1 examination Haematology: First paper Tuesday 20 March 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours Question 1: General Haematology
South African HIV Clinicians Society Managing adult treatment through case study discussion
 South African HIV Clinicians Society Managing adult treatment through case study discussion Jade Mogambery Grey s Hospital, Pietermaritzburg Infectious Diseases Unit Referral summary 20-year-old male HIV
South African HIV Clinicians Society Managing adult treatment through case study discussion Jade Mogambery Grey s Hospital, Pietermaritzburg Infectious Diseases Unit Referral summary 20-year-old male HIV
This was a multicenter study conducted at 11 sites in the United States and 11 sites in Europe.
 Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
Acute Immune Thrombocytopenic Purpura (ITP) in Childhood
 in Childhood") Acute Immune Thrombocytopenic Purpura (ITP) in Childhood Guideline developed by Robert Saylors, MD, in collaboration with the ANGELS team. Last reviewed by Robert Saylors, MD September 22, 2016. Key Points
Acute Immune Thrombocytopenic Purpura (ITP) in Childhood Guideline developed by Robert Saylors, MD, in collaboration with the ANGELS team. Last reviewed by Robert Saylors, MD September 22, 2016. Key Points
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust
 Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Anaemia / SCD/ Bleeding disorders in Children
 Anaemia / SCD/ Bleeding disorders in Children Dr Neil Kennedy Handouts by Steve Graham Learning Outcomes Describe mechanisms of anaemia in Malawian children Discuss important causes of anaemia Describe
Anaemia / SCD/ Bleeding disorders in Children Dr Neil Kennedy Handouts by Steve Graham Learning Outcomes Describe mechanisms of anaemia in Malawian children Discuss important causes of anaemia Describe
MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015
 MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015 HIV & MDR :Impact of early ART initiation Adjusted HR: 0.14; p = 0.042 86% reduction in mortality with ART Initiation during MDR-TB treatment 2015
MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015 HIV & MDR :Impact of early ART initiation Adjusted HR: 0.14; p = 0.042 86% reduction in mortality with ART Initiation during MDR-TB treatment 2015
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014
 Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014 The notification letter which contains details of the decision to widen the restriction criteria for rituximab and eltrombopag
Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014 The notification letter which contains details of the decision to widen the restriction criteria for rituximab and eltrombopag
GOOD MORNING! Thursday, July Heidi Murphy, MD Leslie Carter-King, MD
 GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
Renal failure and thrombocytopaenia? Don t forget TTP/HUS. Jonathan Wala Nephrologist
 Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
The importance of thrombocytopenia and its causes
 SYSMEX EDUCATIONAL ENHANCEMENT AND DEVELOPMENT NO 4 2017 SEED HAEMATOLOGY The importance of thrombocytopenia and its causes Key words: Thrombocytopenia, thrombocytopenic, low levels of platelets What is
SYSMEX EDUCATIONAL ENHANCEMENT AND DEVELOPMENT NO 4 2017 SEED HAEMATOLOGY The importance of thrombocytopenia and its causes Key words: Thrombocytopenia, thrombocytopenic, low levels of platelets What is
HEFT Pathology Guideline. GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia
 HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
Haematology for Clinical Finals The take home messages
 Haematology for Clinical Finals The take home messages Paul Greaves: Consultant Haematologist, BHRUT, Romford The whole of haematology in under 20 slides Never Miss Tumour lysis syndrome: Hyperphos, hypocalc,
Haematology for Clinical Finals The take home messages Paul Greaves: Consultant Haematologist, BHRUT, Romford The whole of haematology in under 20 slides Never Miss Tumour lysis syndrome: Hyperphos, hypocalc,
Thrombotic Microangiopathies
 Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Easy Trick to Spot Leukemia for Pediatricians
 Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Effect of under filling tube
 Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
All Wales Lymphoma Panel Lymphoma Course April 2015 Wales Millennium Centre Cardiff
 All Wales Lymphoma Panel Lymphoma Course 23-24 April 2015 Wales Millennium Centre Cardiff Case Histories Online slides at: http://dental.uwcm.ac.uk:82/awlp%20course%202015/view.apml? Professor Sebastian
All Wales Lymphoma Panel Lymphoma Course 23-24 April 2015 Wales Millennium Centre Cardiff Case Histories Online slides at: http://dental.uwcm.ac.uk:82/awlp%20course%202015/view.apml? Professor Sebastian
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS
 UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
WHAT ARE PAEDIATRIC CANCERS
 WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
Idiopathic Thrombocytopenic Purpura
 Idiopathic Thrombocytopenic Purpura Title of Guideline Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of idiopathic thrombocytopenic purpura Dr S Stokley, Consultant
Idiopathic Thrombocytopenic Purpura Title of Guideline Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of idiopathic thrombocytopenic purpura Dr S Stokley, Consultant
UNUSUAL PRESENTATION OF AN USUAL CAUSE OF THROMBOCYTOPENIA SOUTHERN RAILWAY HQ HOSPITAL, PERAMBUR DR. KUMARAN DNB PG
 UNUSUAL PRESENTATION OF AN USUAL CAUSE OF THROMBOCYTOPENIA SOUTHERN RAILWAY HQ HOSPITAL, PERAMBUR DR. KUMARAN DNB PG 5 months old female infant hailing from Thoothukudi brought by her mother referred from
UNUSUAL PRESENTATION OF AN USUAL CAUSE OF THROMBOCYTOPENIA SOUTHERN RAILWAY HQ HOSPITAL, PERAMBUR DR. KUMARAN DNB PG 5 months old female infant hailing from Thoothukudi brought by her mother referred from
DERBY-BURTON CANCER NETWORK CONTROLLED DOC NO:
 OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
Blood Cancers in the Community
 Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
R-FC for Chronic Lymphocytic Leukaemia LKWOS-005/01
 West of Scotland Cancer Network Chemotherapy Protocol R-FC for Chronic Lymphocytic Leukaemia LKWOS-005/01 Indication B cell Chronic Lymphocytic Leukaemia First line therapy in patients under 70 years of
West of Scotland Cancer Network Chemotherapy Protocol R-FC for Chronic Lymphocytic Leukaemia LKWOS-005/01 Indication B cell Chronic Lymphocytic Leukaemia First line therapy in patients under 70 years of
Approccio morfologico alle microangiopatie trombotiche
 Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Interpreting Blood Tests Part 1. Dr Andrew Smith
 Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
An Uncommon Presentation of Large B-cell Lymphoma of the kidney A Case Report and Literature Review
 An Uncommon Presentation of Large B-cell Lymphoma of the kidney A Case Report and Literature Review CHRISTOPHER ADILETTA M.D., AJAZ SHAWL M.D. ST. JOSEPH S HEALTH, SYRACUSE, NY Our Patient Case We present
An Uncommon Presentation of Large B-cell Lymphoma of the kidney A Case Report and Literature Review CHRISTOPHER ADILETTA M.D., AJAZ SHAWL M.D. ST. JOSEPH S HEALTH, SYRACUSE, NY Our Patient Case We present
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
GP Referral Guidelines. for. South Wales Cancer Network. Document Control Sheet. Specialty/Project Haematological Site Specific Group
 GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
QUICK REFERENCE Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP)
") QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Tumour Lysis Syndrome (TLS)
") (TLS) Overview: Tumour lysis syndrome refers to a number of metabolic disturbances (hyperuricaemia, hyperphosphataemia, hyperkalaemia and hypocalcaemia) that occur as the result of rapid cell lysis. This
(TLS) Overview: Tumour lysis syndrome refers to a number of metabolic disturbances (hyperuricaemia, hyperphosphataemia, hyperkalaemia and hypocalcaemia) that occur as the result of rapid cell lysis. This
CD20-positive high-grade non-hodgkin Lymphoma in patients in which R-CHOP is not indicated
 INDICATION CD20-positive high-grade non-hodgkin Lymphoma in patients in which R-CHOP is not indicated TREATMENT INTENT Curative or Disease Modification. PRE-ASSESSMENT 1. Ensure histology is confirmed
INDICATION CD20-positive high-grade non-hodgkin Lymphoma in patients in which R-CHOP is not indicated TREATMENT INTENT Curative or Disease Modification. PRE-ASSESSMENT 1. Ensure histology is confirmed
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL)
") Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
Haematological Cancer Suspected (Adults & Children)
") Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Part 1 examination. Haematology: First paper. Tuesday 25 September 2018
 Part 1 examination Haematology: First paper Tuesday 25 September 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours 1. Haemato-oncology. A 22 year
Part 1 examination Haematology: First paper Tuesday 25 September 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours 1. Haemato-oncology. A 22 year
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
Skin Pathway Group Alemtuzumab in Cutaneous Lymphoma
 Skin Pathway Group Alemtuzumab in Cutaneous Lymphoma Indication: Treatment of patients with Cutaneous Lymphoma (Unlicensed use) Disease control prior to Reduced Intensity Conditioning Stem Cell Transplant
Skin Pathway Group Alemtuzumab in Cutaneous Lymphoma Indication: Treatment of patients with Cutaneous Lymphoma (Unlicensed use) Disease control prior to Reduced Intensity Conditioning Stem Cell Transplant
AWACC HIV Case Study Dr KR Gate Dr H Sunpath McCord s Hospital Medical Department 01/10/2009
 AWACC 2009 HIV Case Study Dr KR Gate Dr H Sunpath McCord s Hospital Medical Department 01/10/2009 Patient Summary 39yo HIV positive man 2/52 history of productive cough, constitutional symptoms and a headache
AWACC 2009 HIV Case Study Dr KR Gate Dr H Sunpath McCord s Hospital Medical Department 01/10/2009 Patient Summary 39yo HIV positive man 2/52 history of productive cough, constitutional symptoms and a headache
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Diagnosis / Lab Findings
 Diagnosis / Lab Findings During at acute episode may see Peripheral smear bite cells, Heinz bodies Reticulocytosis Increased indirect bilirubin G6PD will be normal or high during an acute crisis Repeat
Diagnosis / Lab Findings During at acute episode may see Peripheral smear bite cells, Heinz bodies Reticulocytosis Increased indirect bilirubin G6PD will be normal or high during an acute crisis Repeat
Dialogue between Clinician and Pathologist on CBC report
 Dialogue between Clinician and Pathologist on CBC report Dr. Seema Bhatwadekar Haematologist, Oncohaematologist & Transplant Physician Vadodara. CBC PBS Most important test to make probable diagnosis Crucial
Dialogue between Clinician and Pathologist on CBC report Dr. Seema Bhatwadekar Haematologist, Oncohaematologist & Transplant Physician Vadodara. CBC PBS Most important test to make probable diagnosis Crucial
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Anemia (3).ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh
.ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh") Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
5/5/2010. Goldilocks picture from
 Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Non-immune acquired haemolytic anaemias. Dr.Maysem
 Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
DA-EPOCH-R (Etoposide/Inpatient)
") DA- (Etoposide/Inp) INDICATION High grade lymphoma. Omit rituximab if CD20 negative. PRE-ASSESSMENT 1. Ensure histology is confirmed prior to administration of chemotherapy and document in notes. 2. Record
DA- (Etoposide/Inp) INDICATION High grade lymphoma. Omit rituximab if CD20 negative. PRE-ASSESSMENT 1. Ensure histology is confirmed prior to administration of chemotherapy and document in notes. 2. Record
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Hematologic Emergency. Le Wang, MD, PhD Hematology & Oncology
 Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES ALDO E CELE DACCO
 ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Note: There are other bendamustine protocols, ensure this is the correct one for a given patient.
 INDICATIONS 1 st line treatment for follicular lymphoma with FLIPI score 2 or higher: (NICE TA513- BLUETEQ required) Rituximab refractory follicular lymphoma (progression on R-chemo, R-maintenance or within
INDICATIONS 1 st line treatment for follicular lymphoma with FLIPI score 2 or higher: (NICE TA513- BLUETEQ required) Rituximab refractory follicular lymphoma (progression on R-chemo, R-maintenance or within
FBC interpretation. Dr. Gergely Varga
 FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
CHEMOTHERAPY PROTOCOL FOR ADMINISTRATION OF VENETOCLAX
 CHEMOTHERAPY PROTOCOL FOR ADMINISTRATION OF VENETOCLAX Therapeutic Indications: Venetoclax monotherapy is indicated for the treatment of chronic lymphocytic leukaemia (CLL) in the presence of 17p deletion
CHEMOTHERAPY PROTOCOL FOR ADMINISTRATION OF VENETOCLAX Therapeutic Indications: Venetoclax monotherapy is indicated for the treatment of chronic lymphocytic leukaemia (CLL) in the presence of 17p deletion
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
HIV ASSOCIATED LYMPHOMA. Dr N Rapiti
 HIV ASSOCIATED LYMPHOMA Dr N Rapiti HIV ASSOCIATED LYMPHOMA: OVERVIEW Classification Pathogenesis Prognosis cart Chemotherapy/Radiotherapy/SCT Supportive CASE 40 yr old male, Mr BM, p/w Symptomatic anemia
HIV ASSOCIATED LYMPHOMA Dr N Rapiti HIV ASSOCIATED LYMPHOMA: OVERVIEW Classification Pathogenesis Prognosis cart Chemotherapy/Radiotherapy/SCT Supportive CASE 40 yr old male, Mr BM, p/w Symptomatic anemia
Updates for your practice August 2013 TLALELETSO. HIV & Anemia. Continued on Page 2
 dates for your practice August 2013 TLALELETSO HIV & Anemia In this issue we review anemia and HIV. Medical professionals across all disciplines need to be alert to the hematological complications of HIV
dates for your practice August 2013 TLALELETSO HIV & Anemia In this issue we review anemia and HIV. Medical professionals across all disciplines need to be alert to the hematological complications of HIV
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura
 Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Carfilzomib and Dexamethasone (CarDex)
") Carfilzomib and Dexamethasone (CarDex) Indication Relapsed multiple myeloma for patients who have had only one previous line of therapy (that did not include bortezomib). (NICE TA457) ICD-10 codes Codes
Carfilzomib and Dexamethasone (CarDex) Indication Relapsed multiple myeloma for patients who have had only one previous line of therapy (that did not include bortezomib). (NICE TA457) ICD-10 codes Codes
Contemporary perspectives and initial management of pediatric ITP. William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA
 Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Contemporary perspectives and initial management of pediatric ITP William Beau Mitchell, MD Weill Cornell Medical College New York, NY USA Case Presentation 5 year old female Bruises on trunk, extremities
Chest diseases Hospital Hematology Patient care plans
 Chest diseases Hospital Hematology Patient care plans Hematology Service in CDH in a consultation service for management of hematologic complications of cardiology/ cardiac surgery. Primary hematologic
Chest diseases Hospital Hematology Patient care plans Hematology Service in CDH in a consultation service for management of hematologic complications of cardiology/ cardiac surgery. Primary hematologic
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
X M/ (R) Dose adjusted (DA)-EPOCH-R
 Dose adjusted (DA)-EPOCH-R") X M/ (R) adjusted (DA)-EPOCH-R Indication High-risk CD20+ diffuse large B cell lymphoma especially C-MYC and BCL-2 activated (i.e. double hit lymphoma) and mediastinal sclerosing (thymic) large B cell
X M/ (R) adjusted (DA)-EPOCH-R Indication High-risk CD20+ diffuse large B cell lymphoma especially C-MYC and BCL-2 activated (i.e. double hit lymphoma) and mediastinal sclerosing (thymic) large B cell
GOOD MORNING! July 3, 2014
 GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
BLOOD TRANSFUSION. Dr Lumka Ntabeni
 BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
Management of Cancer Associated Thrombosis (CAT) where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth
 where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth") Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
GP CME. James Liang Consultant Haematologist. Created by: Date:
 GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
Presentation Outline. Disease Background Previous research on platelet recovery rate Goal of our study Methods Results Limitations Conclusions
 Platelet Recovery Rate at Day 5 of Therapeutic Plasma Exchange for Acquired Thrombotic Thrombocytopenic Purpura Can Aid in Identifying Risk of Disease Exacerbation Suzanne Zhou, Yara A. Park, Marian A.
Platelet Recovery Rate at Day 5 of Therapeutic Plasma Exchange for Acquired Thrombotic Thrombocytopenic Purpura Can Aid in Identifying Risk of Disease Exacerbation Suzanne Zhou, Yara A. Park, Marian A.
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
R-GDP: Rituximab, Gemcitabine, Dexamethasone &Cisplatin
 : Rituximab, Gemcitabine, Dexamethasone &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma or high grade T cell non-hodgkin
: Rituximab, Gemcitabine, Dexamethasone &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma or high grade T cell non-hodgkin
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin
 Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Version: 6 Date: 2 nd March 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Version: 6 Date: 2 nd March 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/
R-GemOx. Lymphoma group INDICATION. Relapsed or Refractory Lymphoma, for patients unsuitable for R-GDP regimen. Omit rituximab if CD20- negative
 R-GemOx INDICATION Relapsed or Refractory Lymphoma, for patients unsuitable for R-GDP regimen. Omit rituximab if CD20- negative TREATMENT INTENT Disease modification PRE-ASSESSMENT 1. Ensure histology
R-GemOx INDICATION Relapsed or Refractory Lymphoma, for patients unsuitable for R-GDP regimen. Omit rituximab if CD20- negative TREATMENT INTENT Disease modification PRE-ASSESSMENT 1. Ensure histology
Guidelines for Shared Care Centres and Community Staff
 Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
R-GDP: Rituximab, Gemcitabine, Dexamethasone &Cisplatin
 : Rituximab, &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma. TREATMENT INTENT Palliative or curative depending on context.
: Rituximab, &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma. TREATMENT INTENT Palliative or curative depending on context.