History. 2D echo before TAVI. 88 female Hypertensive - hyperlipidemic History of LOC syncope Echo: severe AS AV gradient 90 mmhg Good LV LVH
|
|
|
- Georgina Richards
- 5 years ago
- Views:
Transcription


1


2 History 88 female Hypertensive - hyperlipidemic History of LOC syncope Echo: severe AS AV gradient 90 mmhg Good LV LVH 2D echo before TAVI LHC: Normal cors
3

4 Pre severe calcification LVOT calcification

5 DEPLOYMENT
6 DEPLOYMENT
7 DEPLOYMENT

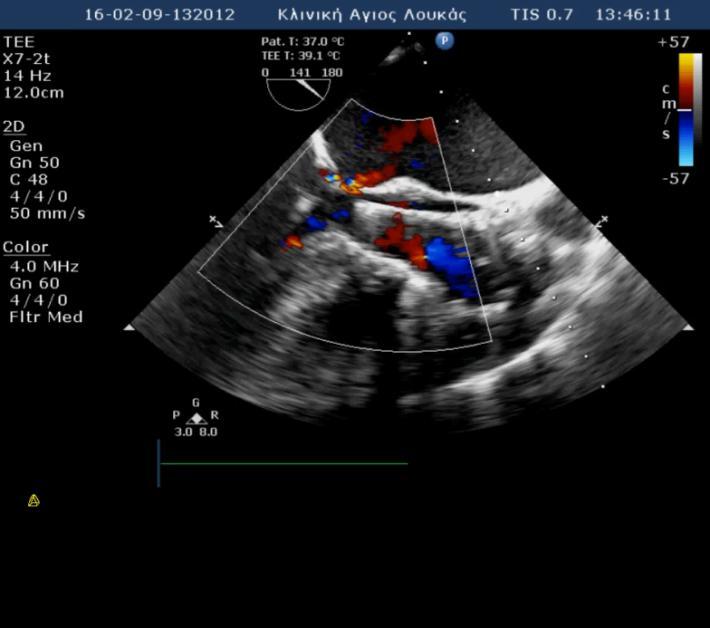

8 Immediately post deployment: incomplete apposition and moderate AR
9 QUESTION 1 FURTHER MANAGEMENT A. leave AR manage conservatively B. post dilatation balloon 20mm C. post dilatation balloon 22mm D. post dilatation balloon 24mm
10 QUESTION 1 FURTHER MANAGEMENT A. leave AR manage conservatively B. post dilatation balloon 20mm C. post dilatation balloon 22mm D. post dilatation balloon 24mm

11 Post dilation semi-compliant balloon 22mm


12 Immediately post dilatation patient became hypotensive; A large pericardial effusion with tamponade was noted;

13 Aortogram showed intraannular rupture with minimal residual AR
14 QUESTION 2 FURTHER MANAGEMENT A. Operation B. Pericardial drainage and operation C. Pericardial drainage and continue antiplatelets antithrombotics D. Pericardial drainage and discontinue antiplatelets antithrombotics
15 QUESTION 2 FURTHER MANAGEMENT A. Operation B. Pericardial drainage and operation C. Pericardial drainage and continue antiplatelets antithrombotics D. Pericardial drainage and discontinue antiplatelets antithrombotics
16 Patient was treated conservatively with pericardial drainage, heparin reversal, interruption of all antithrombotics- antiplatelets and immobilization In consultation with cardiac surgeons and getting advice from TAVI forum, we did not start any antithrombotics-antiplatelets for 6 days Pericardial effusion disappeared and drain removed day number 5
17 Day number 6, patient developed TIA with dysphasia, CT was normal;
18 QUESTION 3 FURTHER MANAGEMENT A. aspirin B. antithrombotics C. Dual antiplatelets D. no antiplatelets - antithrombotics
19 QUESTION 3 FURTHER MANAGEMENT A. aspirin B. antithrombotics C. Dual antiplatelets D. no antiplatelets - antithrombotics

20 Day number 6, patient developed TIA with dysphasia, CT was normal; started on Aspirin and TIA resolved completely. She started mobilization.
21 Day number 12, patient developed signs of pulmonary embolism. CT showed left lower lobe thrombi. CT aortogram did not show paraaortic false aneurysm
22 QUESTION 4 FURTHER MANAGEMENT A. continue with aspirin add sc heparin B. change aspirin to sc heparin C. change aspirin to oral antithrombotics D. continue with aspirin add oral antithrombotics
23 QUESTION 4 FURTHER MANAGEMENT A. continue with aspirin add sc heparin B. change aspirin to sc heparin C. change aspirin to oral antithrombotics D. continue with aspirin add oral antithrombotics


24 Day number 12, patient developed signs of pulmonary embolism. CT showed left lower lobe thrombi. CT aortogram did not show paraaortic false aneurysm. She was started on sc heparin in addition to aspirin and clinical picture improved


25 Patient discharged day number 14 on aspirin and subcutaneous heparin 2 months later remained fully asymptomatic Echo shows no pericardial fluid and minimal AR Subcutaneous heparin is stopped; patient remains on long term aspirin 2D echo 2 months later no pericardial fluid Colour echo 2 months later minimal paravalvular AR
26 3 months later Severe UTI acute renal failure Iv fluids iv antibiotics Renal function fully restored


27 4 months later Chest pain - SOB
28 CRP > 10X INCREASED WCC
29 QUESTION 5 DIAGNOSIS A. Relapse of rupture B. viral pericarditis C. late DRESSLER S
30 QUESTION 5 DIAGNOSIS A. Relapse of rupture B. viral pericarditis C. late DRESSLER S
31 CRP > 10X INCREASE WCC LATE DRESSLER S: STEROIDS + COLCHICINE

32 15 DAYS AFTER STEROIDS pt very well steroids stopped colchicine continued NO PERICARDIAL EFFUSION TRIVIAL AR
33 10 months post TAVI Asymptomatic Colchicine stopped ECHO: no pericardial effusion, TAVI functioning normally
34 1 year FU Pt alive and well TAVI normally functioning ONLY COMPLAIN: lower back pain
35 In conclusion Preventing Annulus Rupture Clinical judgment Good imaging pre TAVR (CT scan, calcifications esp LVOT) Avoid aggressive THV oversizing Avoid oversizing postdilatation balloon (as in our case) Prosthesis Selection (probably self expandable for LVOT calcification) Managing antithromboticsantiplatelets post annulus rupture Judicious use Gradual and staged onset Be aware of complications

36 2 st Case: 31 mm CoreValve- VF Arrest Deployment Aortogram Pre Deployment 1
37 Deployment 2 Deployment 3
38 Deployment 4 Deployment 5


39 Deployment 6 VF arrest- Quick Deployment

40 Final Result


41 Iliac Pre Iliac Post

42 Predictors Post dilation Oversizing 20% Calcifications (LVOT-Sub annular) Annulus Eccentricity? Prevention: Sizing/Slow inflation/self Expandable if adverse features present
43 1 st Case: Aortic rupture peri-tavi Acute or delayed aortic annular rupture is a rare (0-2%) but serious complication with a very poor prognosis, even if emergent surgery is performed Annular rupture may occur after balloon valvuloplasty after valve implantation (more frequently with balloon-expandable valves)
SAPIEN 3 Sizing Considerations:
 SAPIEN 3 Sizing Considerations: Oversizing, Undersizing, or Volume reduction? John Webb MD St Paul s Hospital University of British Columbia Vancouver Disclosure Statement of Financial Interest Within
SAPIEN 3 Sizing Considerations: Oversizing, Undersizing, or Volume reduction? John Webb MD St Paul s Hospital University of British Columbia Vancouver Disclosure Statement of Financial Interest Within
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012
 ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012 TAVR Technologies Current Generation Devices ~ 50,000 patients treated thru 2011 in > 500 interventional centers
ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012 TAVR Technologies Current Generation Devices ~ 50,000 patients treated thru 2011 in > 500 interventional centers
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2/28/2010. Speakers s name: Paul Chiam. I have the following potential conflicts of interest to report: NONE. Antegrade transvenous transseptal route
 Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation
 ESC Congress 2010 28 Aug 2010-01 Sep 2010 Stockholm - Sweden Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation Gian Paolo Ussia, MD Director of Interventional
ESC Congress 2010 28 Aug 2010-01 Sep 2010 Stockholm - Sweden Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation Gian Paolo Ussia, MD Director of Interventional
New York Valves Patient focused evidence-based approach. New York City: 6 December Antonio Colombo
 New York Valves 2018 Patient focused evidence-based approach New York City: 6 December 2018 Antonio Colombo Speaker 7 EMO GVM Centro Cuore Columbus Milan, Italy No conflicts to report Vascular complications
New York Valves 2018 Patient focused evidence-based approach New York City: 6 December 2018 Antonio Colombo Speaker 7 EMO GVM Centro Cuore Columbus Milan, Italy No conflicts to report Vascular complications
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Aortic valve implantation using the femoral and apical access: a single center experience.
 Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Evolut R in bicuspid valve anatomies
 Evolut R in bicuspid valve anatomies U. Gerckens MD University of Rostock, Germany Potential conflicts of interest Speaker's name: Ulrich Gerckens I have the following potential conflicts of interest to
Evolut R in bicuspid valve anatomies U. Gerckens MD University of Rostock, Germany Potential conflicts of interest Speaker's name: Ulrich Gerckens I have the following potential conflicts of interest to
Clinical Indications for Echocardiography
 Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
TAVI IN BICUSPID AOV AND VALVE-IN-VALVE
 TAVI IN BICUSPID AOV AND VALVE-IN-VALVE Petros S. Dardas, MD, FESC St Lukes Hospital Thessaloniki, GREECE 6o ΣΥΝΕΔΡΙΟ ΔΙΑΚΑΘΕΤΗΡΙΑΚΗΣ ΘΕΡΑΠΕΙΑΣ ΚΑΡΔΙΑΚΩΝ ΒΑΛΒΙΔΟΠΑΘΕΙΩΝ ΑΘΗΝΑ 2017 BICUSPID AOV Surgical
TAVI IN BICUSPID AOV AND VALVE-IN-VALVE Petros S. Dardas, MD, FESC St Lukes Hospital Thessaloniki, GREECE 6o ΣΥΝΕΔΡΙΟ ΔΙΑΚΑΘΕΤΗΡΙΑΚΗΣ ΘΕΡΑΠΕΙΑΣ ΚΑΡΔΙΑΚΩΝ ΒΑΛΒΙΔΟΠΑΘΕΙΩΝ ΑΘΗΝΑ 2017 BICUSPID AOV Surgical
Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t
 Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute Cleveland Clinic
Procedural Guidance of TAVR: How to Assure it Goes Right and What to Do If It Doesn t James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute Cleveland Clinic
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
TAVR SPRING 2017 The evolution of TAVR
 TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
Transcatheter Aortic Valve Implantation Management of risks and complications
 Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY)
") Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY) Thomas Walther, Christian W. Hamm, Gerhard Schuler, Alexander Berkowitsch,
Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY) Thomas Walther, Christian W. Hamm, Gerhard Schuler, Alexander Berkowitsch,
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
Emergency TAVI: Does It Exist? Is the Risk Higher?
 Emergency TAVI: Does It Exist? Is the Risk Higher? Gerald Yong MBBS (Hons) FRACP FSCAI Interventional Cardiologist Royal Perth Hospital Western Australia APCASH 12 October 2014 Disclosure Statement of
Emergency TAVI: Does It Exist? Is the Risk Higher? Gerald Yong MBBS (Hons) FRACP FSCAI Interventional Cardiologist Royal Perth Hospital Western Australia APCASH 12 October 2014 Disclosure Statement of
Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC
 TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Corrado Tamburino, MD, PhD
 Paravalvular leak: acceptable or not Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate School of Cardiology Chief Cardiovascular Department, Director Cardiology Division,
Paravalvular leak: acceptable or not Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate School of Cardiology Chief Cardiovascular Department, Director Cardiology Division,
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland
 Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
DISCLOSURE. Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
22/06/2017. Oxford City. Transcatheter aortic valve replacement 2017 guidelines. 1. First time I have heard about it. 2.
 Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
TAVR : Caring for your patients before and after TAVR
 TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR Valve Thrombosis
 TAVR Valve Thrombosis Mohammed Balghith, MD, FACC, FRCPC, FACP, FESC Associate Professor KSAU-HS, Consultant Interventional Cardiologist Ministry of National Guard, King Abdulaziz Cardiac Center, Riyadh
TAVR Valve Thrombosis Mohammed Balghith, MD, FACC, FRCPC, FACP, FESC Associate Professor KSAU-HS, Consultant Interventional Cardiologist Ministry of National Guard, King Abdulaziz Cardiac Center, Riyadh
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
 Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Comments restricted to Sapien and Corevalve 9/12/2016. Disclosures: Core Lab contracts with Edwards Lifesciences, Middlepeak, Medtronic
 Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
The Role of Imaging in Transcatheter Aortic Valve Implantation
 The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison
 Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
*Core lab for numerous trials, for which I receive no direct compensation from sponsors.
 Rebecca T. Hahn, MD, FACC, FASE Director of Interventional Echo Professor of Medicine Columbia University Company Abbott Vascular Gore&Assoc NaviGATE Medtronic Boston Scientific GE Medical Philips Healthcare
Rebecca T. Hahn, MD, FACC, FASE Director of Interventional Echo Professor of Medicine Columbia University Company Abbott Vascular Gore&Assoc NaviGATE Medtronic Boston Scientific GE Medical Philips Healthcare
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Image Assistance in TAVI Why CT? Won-Jang Kim, MD, PhD Clinical Assistant Professor of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea
 Image Assistance in TAVI Why CT? Won-Jang Kim, MD, PhD Clinical Assistant Professor of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea Major Uses of CT in TAVI Ileofemoral Patient Arterial
Image Assistance in TAVI Why CT? Won-Jang Kim, MD, PhD Clinical Assistant Professor of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea Major Uses of CT in TAVI Ileofemoral Patient Arterial
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD
 Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee
 - 5 important lessons learnt from HK experiences Michael KY Lee") Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee Queen Elizabeth Hospital, Hong Kong President, HKSTENT APCASH 2013 SJ Park TAVI Summit 2013
Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee Queen Elizabeth Hospital, Hong Kong President, HKSTENT APCASH 2013 SJ Park TAVI Summit 2013
How to manage TAVI related vascular complications. Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI
 How to manage TAVI related vascular complications Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI Definition VARC-2 consensus statement Complications caused by: Wire Catheter Anything related to vascular access
How to manage TAVI related vascular complications Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI Definition VARC-2 consensus statement Complications caused by: Wire Catheter Anything related to vascular access
TAVI complication. Possible aetiology and how to manage
 TAVI complication. Possible aetiology and how to manage Dr Sanjeevan Pasupati Waikato Hospital, Hamilton, New Zealand Operators: Dr Sanjeevan Pasupati, Mr Nand Kejriwal, Mr Adam Elgamel Valve Positioning
TAVI complication. Possible aetiology and how to manage Dr Sanjeevan Pasupati Waikato Hospital, Hamilton, New Zealand Operators: Dr Sanjeevan Pasupati, Mr Nand Kejriwal, Mr Adam Elgamel Valve Positioning
Percutaneous Management of Severe AS in Octagenarians. Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington
 Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
Dr Winnie Sze-Wun Chan. Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong
 Dr Winnie Sze-Wun Chan Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong Why? Is CT reliable? How to perform the CT study? How to interpret the CT study?
Dr Winnie Sze-Wun Chan Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong Why? Is CT reliable? How to perform the CT study? How to interpret the CT study?
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval?
 Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification. Rheumatic Mitral Stenosis 76yo male
 MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
TAVI: Nouveaux Horizons
 TAVI: Nouveaux Horizons EUAPI580i 432HQ14NP02353 Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Objectifs Les recommandations Le TAVI en chiffre La
TAVI: Nouveaux Horizons EUAPI580i 432HQ14NP02353 Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Objectifs Les recommandations Le TAVI en chiffre La
TAVI Implantation: Rapid Pacing, Pre and Post Dilatation
 TAVI Summit 2012 Seoul, September 9, 2012 TAVI Implantation: Rapid Pacing, Pre and Post Dilatation Eberhard Grube, MD, FACC, FSCAI Medizinische i i Klinik ik und Polikinik II, University i Hospital Bonn,
TAVI Summit 2012 Seoul, September 9, 2012 TAVI Implantation: Rapid Pacing, Pre and Post Dilatation Eberhard Grube, MD, FACC, FSCAI Medizinische i i Klinik ik und Polikinik II, University i Hospital Bonn,
2/10/2012. The Role of Multimodality Imaging in Percutaneous Valve Interventions. This is truly a TEAM work. Overview. Overview
 The Role of Multimodality Imaging in Percutaneous Valve Interventions João L. Cavalcante, MD Advanced Cardiovascular Imaging Cleveland Clinic 02/11/2012 Disclosures: None Movement from surgery to transcatheter
The Role of Multimodality Imaging in Percutaneous Valve Interventions João L. Cavalcante, MD Advanced Cardiovascular Imaging Cleveland Clinic 02/11/2012 Disclosures: None Movement from surgery to transcatheter
PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration in 2018?
 Joint Meeting 1 Aortic and Mitral Club Chairpersons: S.Adamopoulos, M. Vavuranakis, L. Michalis, P. Nihoyannopoulos PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration
Joint Meeting 1 Aortic and Mitral Club Chairpersons: S.Adamopoulos, M. Vavuranakis, L. Michalis, P. Nihoyannopoulos PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
A review of the complications associated with Transcatheter Aortic Valve Implantation.
 A review of the complications associated with Transcatheter Aortic Valve Implantation. Dr Conor McQuillan Transcatheter Aortic Valve Implantation (TAVI) has become the standard of care for treating elderly,
A review of the complications associated with Transcatheter Aortic Valve Implantation. Dr Conor McQuillan Transcatheter Aortic Valve Implantation (TAVI) has become the standard of care for treating elderly,
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Percutaneous VSD closure
 Percutaneous VSD closure Gianfranco Butera San Donato Milanese - Italy Patients selection Pts having hemodynamically significant VSD Left ventricular enlargement (left ventricular overload),defined as
Percutaneous VSD closure Gianfranco Butera San Donato Milanese - Italy Patients selection Pts having hemodynamically significant VSD Left ventricular enlargement (left ventricular overload),defined as
TAVI in Korea, How to Avoid Conduction
 TAVI in Korea, How to Avoid Conduction Disturbance after CoreValve Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul,
TAVI in Korea, How to Avoid Conduction Disturbance after CoreValve Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul,
Pacemaker After Transcatheter Aortic Valve Implantation: Where, When and How?
 Pacemaker After Transcatheter Aortic Valve Implantation: Where, When and How? Michael Glikson, MD, FESC, FACC Davidai Arrhythmia Center, Israel Europace 2011 Conflict of Interest Research grants from device
Pacemaker After Transcatheter Aortic Valve Implantation: Where, When and How? Michael Glikson, MD, FESC, FACC Davidai Arrhythmia Center, Israel Europace 2011 Conflict of Interest Research grants from device
Pacemaker rates Second generation TAVI Devices
 Pacemaker rates Second generation TAVI Devices Florian Krackhardt, M.D. Department of Cardiology Charité Campus Virchow-Klinikum University Hospital Berlin, Germany TAVI The future s looking very positive
Pacemaker rates Second generation TAVI Devices Florian Krackhardt, M.D. Department of Cardiology Charité Campus Virchow-Klinikum University Hospital Berlin, Germany TAVI The future s looking very positive
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR)
") Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Critical role of multi-modality planning in Transcatheter Mitral Valve Replacement
 Critical role of multi-modality planning in Transcatheter Mitral Valve Replacement Dee Dee Wang, MD, FACC, FASE, FSCCT Director Structural Heart Imaging Medical Director 3D Printing Henry Ford Innovations
Critical role of multi-modality planning in Transcatheter Mitral Valve Replacement Dee Dee Wang, MD, FACC, FASE, FSCCT Director Structural Heart Imaging Medical Director 3D Printing Henry Ford Innovations
Cardiac catheterisation in AS
 AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
Lessons From The Computer Model and How We Do Root Replacement
 Lessons From The Computer Model and How We Do Root Replacement Ehud Raanani, MD Cardiac Surgery Leviev Cardiothoracic and Vascular Center Sheba Medical Center Sackler School of Medicine, Tel Aviv University
Lessons From The Computer Model and How We Do Root Replacement Ehud Raanani, MD Cardiac Surgery Leviev Cardiothoracic and Vascular Center Sheba Medical Center Sackler School of Medicine, Tel Aviv University
Simultaneous Acute ST Elevation Myocardial Infarction And Acute Left Subclavian Artery Thrombosis
 Simultaneous Acute ST Elevation Myocardial Infarction And Acute Left Subclavian Artery Thrombosis Chee Yang CHIN, MBChB, MRCP(UK) C.W.L. Chin, P.T.L. Chiam, R.S. Tan National Heart Centre Singapore 26
Simultaneous Acute ST Elevation Myocardial Infarction And Acute Left Subclavian Artery Thrombosis Chee Yang CHIN, MBChB, MRCP(UK) C.W.L. Chin, P.T.L. Chiam, R.S. Tan National Heart Centre Singapore 26
Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry
 Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry E Van Belle, E Teiger, F Juthier, A Vincentelli, B Iung, H Eltchaninoff, J Fajadet,
Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry E Van Belle, E Teiger, F Juthier, A Vincentelli, B Iung, H Eltchaninoff, J Fajadet,
Should We Reconsider using Anticoagulation for Biological Tissue Valves
 Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Prof. Dr. Thomas Walther. TAVI in ascending aorta / aortic root dilatation
 Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Paravalvular Regurgitation is a Risk Factor Following TAVI
 Paravalvular Regurgitation is a Risk Factor Following TAVI Philippe Pibarot, DVM, PhD, FACC, FESC, FASE Canada Research Chair in Valvular Heart Disease INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE
Paravalvular Regurgitation is a Risk Factor Following TAVI Philippe Pibarot, DVM, PhD, FACC, FESC, FASE Canada Research Chair in Valvular Heart Disease INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE
Is Stroke Frequency Declining?
 Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Role of Embolic Protection Devices in TAVR: Are They Needed? Waste of Time and Money?
 Role of Embolic Protection Devices in TAVR: Are They Needed? Waste of Time and Money? Gian Paolo Ussia Campus Bio-medico University, Rome Italy g.ussia@unicampus.it REQUIRED Gian Paolo Ussia I have no
Role of Embolic Protection Devices in TAVR: Are They Needed? Waste of Time and Money? Gian Paolo Ussia Campus Bio-medico University, Rome Italy g.ussia@unicampus.it REQUIRED Gian Paolo Ussia I have no
Complicanze durante TAVI. Brambilla Nedy IRCCS Policlinico San Donato
 Complicanze durante TAVI Brambilla Nedy IRCCS Policlinico San Donato 0 2 4 6 9 11 14 16 22 26 31 33 37 43 52 61 69 78 87 93 106 113 121 151 171 186 201 225 267 283 294 311 349 502 515 709 1007 Number of
Complicanze durante TAVI Brambilla Nedy IRCCS Policlinico San Donato 0 2 4 6 9 11 14 16 22 26 31 33 37 43 52 61 69 78 87 93 106 113 121 151 171 186 201 225 267 283 294 311 349 502 515 709 1007 Number of
VALVULAR HEART DISEASE AORTIC VALVE STENOSIS TAVR PROCEDURE
 CVI SYMPOSIUM 2012 VALVULAR HEART DISEASE AORTIC VALVE STENOSIS TAVR PROCEDURE Luis F. Tami, MD Cardiac Cath Lab Director Memorial Regional Hospital 86 yr old CABG 1995. LIMA to LAD and SVG to OM. Presented
CVI SYMPOSIUM 2012 VALVULAR HEART DISEASE AORTIC VALVE STENOSIS TAVR PROCEDURE Luis F. Tami, MD Cardiac Cath Lab Director Memorial Regional Hospital 86 yr old CABG 1995. LIMA to LAD and SVG to OM. Presented
Appropriate Use of TAVR - now and in the future. A Surgeon s Perspective. Neil Moat Royal Brompton Hospital, London, UK
 Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
First Transfemoral Aortic Valve Implantation In Bulgaria - Crossing The Valve With The Device Is Not Always
 ISPUB.COM The Internet Journal of Cardiology Volume 9 Number 2 First Transfemoral Aortic Valve Implantation In Bulgaria - Crossing The Valve With The Device Is Not T D, J P. Citation T D, J P.. First Transfemoral
ISPUB.COM The Internet Journal of Cardiology Volume 9 Number 2 First Transfemoral Aortic Valve Implantation In Bulgaria - Crossing The Valve With The Device Is Not T D, J P. Citation T D, J P.. First Transfemoral
Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai
 Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai Anesthetic care and considerations Intraoperative events TEE Perioperative complications Most common valvular
Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai Anesthetic care and considerations Intraoperative events TEE Perioperative complications Most common valvular
Preprocedural evaluation for TAVR
 KEBE 30/05/15 Preprocedural evaluation for TAVR Ioannis Iakovou, MD, PhD Interventional Cardiology Onassis Cardiac Surgery Center Athens, Greece Clinical Pathway: Developing Peri- Procedural Protocols
KEBE 30/05/15 Preprocedural evaluation for TAVR Ioannis Iakovou, MD, PhD Interventional Cardiology Onassis Cardiac Surgery Center Athens, Greece Clinical Pathway: Developing Peri- Procedural Protocols
7 th Conference of Transcatheter Heart Valve Therapies
 7 th Conference of Transcatheter Heart Valve Therapies May 18-19, 2018, Athens Hilton Athens, Greece Course Directors Stratis Pattakos MD Konstantinos Spargias MD Panos Vardas MD Co-Directors Nick Bouboulis
7 th Conference of Transcatheter Heart Valve Therapies May 18-19, 2018, Athens Hilton Athens, Greece Course Directors Stratis Pattakos MD Konstantinos Spargias MD Panos Vardas MD Co-Directors Nick Bouboulis
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
DICE Session. The endocarditis team. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 DICE Session. The endocarditis team Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following financial relationships: Consultant
DICE Session. The endocarditis team Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following financial relationships: Consultant
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
David Dexter MD FACS Sentara Vascular Specialists Assistant Professor of Surgery EVMS. Peripheral Complications of TAVR
 David Dexter MD FACS Sentara Vascular Specialists Assistant Professor of Surgery EVMS Peripheral Complications of TAVR TAVR Complications Reported Complications Rates range from 8% to 15% Predictors of
David Dexter MD FACS Sentara Vascular Specialists Assistant Professor of Surgery EVMS Peripheral Complications of TAVR TAVR Complications Reported Complications Rates range from 8% to 15% Predictors of
April 16, 09:00-09:15 중앙대학교 윤신원
 April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D.
 Charles T. Klodell, M.D.") Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Percutaneous Therapy for Calcific Mitral Valve Disease
 31 st Annual State of the Art Echocardiography San Diego, CA February 18, 2018 5:00 5:15 PM 15 min Percutaneous Therapy for Calcific Mitral Valve Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive
31 st Annual State of the Art Echocardiography San Diego, CA February 18, 2018 5:00 5:15 PM 15 min Percutaneous Therapy for Calcific Mitral Valve Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive
Watchman and Structural update..the next frontier. Ari Chanda, MD Cardiology Associates of Fredericksburg
 Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR TTE INTERROGATION BY ALAN MATTHEWS
 TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Aortic stenosis and regurgitation
 1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
 Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Successful Transfemoral Edwards Sapien Aortic. Valve Implantation in a Patient with Previous. Mitral Valve Replacement
 Advanced Studies in Medical Sciences, Vol. 2, 2014, no. 1, 37-45 HIKARI Ltd, www.m-hikari.com http://dx.doi.org/10.12988/asms.2014.31213 Successful Transfemoral Edwards Sapien Aortic Valve Implantation
Advanced Studies in Medical Sciences, Vol. 2, 2014, no. 1, 37-45 HIKARI Ltd, www.m-hikari.com http://dx.doi.org/10.12988/asms.2014.31213 Successful Transfemoral Edwards Sapien Aortic Valve Implantation