Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
|
|
|
- Alvin Farmer
- 5 years ago
- Views:
Transcription
1 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
2 The renal biopsy is a powerful tool in the diagnostic evaluation of allograft dysfunction
3 Evaluation procedure Standard At least two cores whenever possible Light microscopic stainings on serial sections (H&E, PAS, trichrome, methenamine silver) Immunostaining for complement 4d - indicator of antibody-mediated rejection
4 Optional LM: elastin staining - chronic rejection- induced intimal fibrosis IF: IgG, IgA, IgM, C3, C1q - GN tubular HLA-DR expression - acute T-cell-mediated rejection EM - chronic rejection, GN Implantation biopsy for comparison
5 Objective To review the pathology of rejection, CNI toxicity, polyomavirus nephropathy, and posttransplantation glomerulonephritis factors leading to end-stage kidney allograft disease Solez et al. Banff 07 Classification of Renal Allograft Pathology. AJT 8:753, 2008
6 Rejection Inflammatory response initiated by alloantigen recognition Acute T-cell mediated Alloantibody mediated Chronic Alloantibody mediated T-cell mediated
7 Acute T-cell-mediated rejection Inflammatory response against HLA class II antigens expressed on peritubular and glomerular capillary endothelial cells tubular epithelial cells interstitial dendritic cells mesangial cells
8 Acute T-cell-mediated rejection Inflammatory response against HLA class II antigens expressed on peritubular and glomerular capillary endothelial cells tubular epithelial cells interstitial dendritic cells mesangial cells Effector mechanisms CD8 + CTL-mediated cytotoxicity +++ Delayed type hypersensitivity + Antibody-dependent cytotoxicity +
9 Acute T-cell-mediated rejection Peritubular capillaries Interstitium Tubules Tubulointerstitial rejection + Arteries Vascular rejection + Glomeruli Transplant glomerulitis


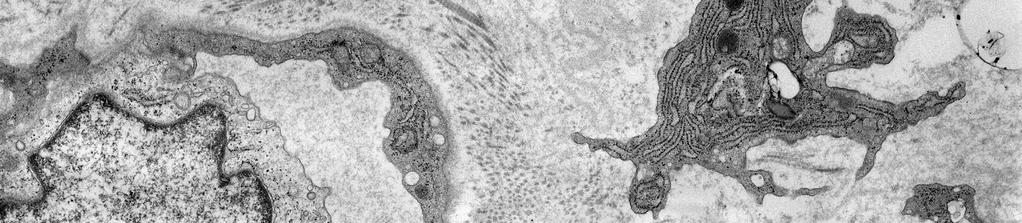
10 Tubulointerstitial rejection Peritubular capillaritis: accumulation of lymphocytes + monocytes
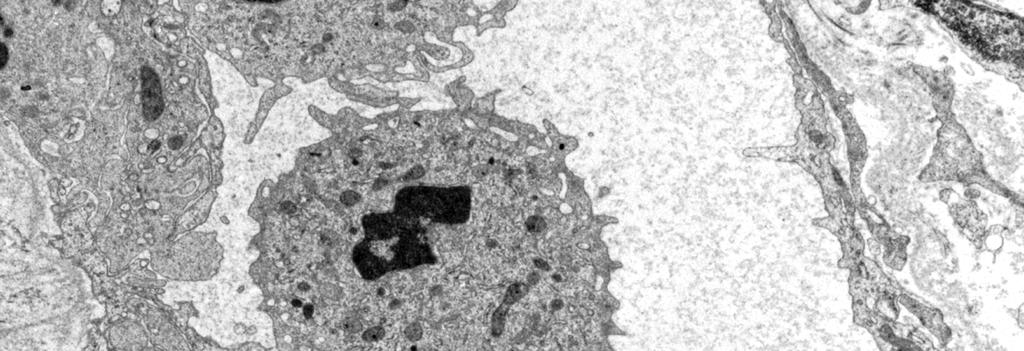
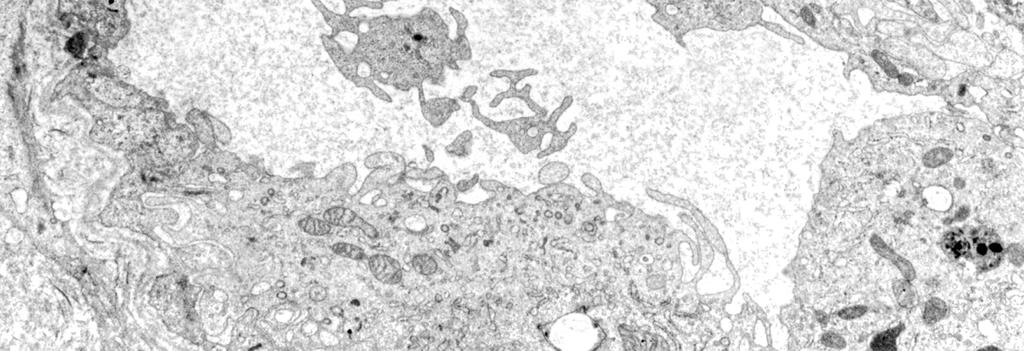
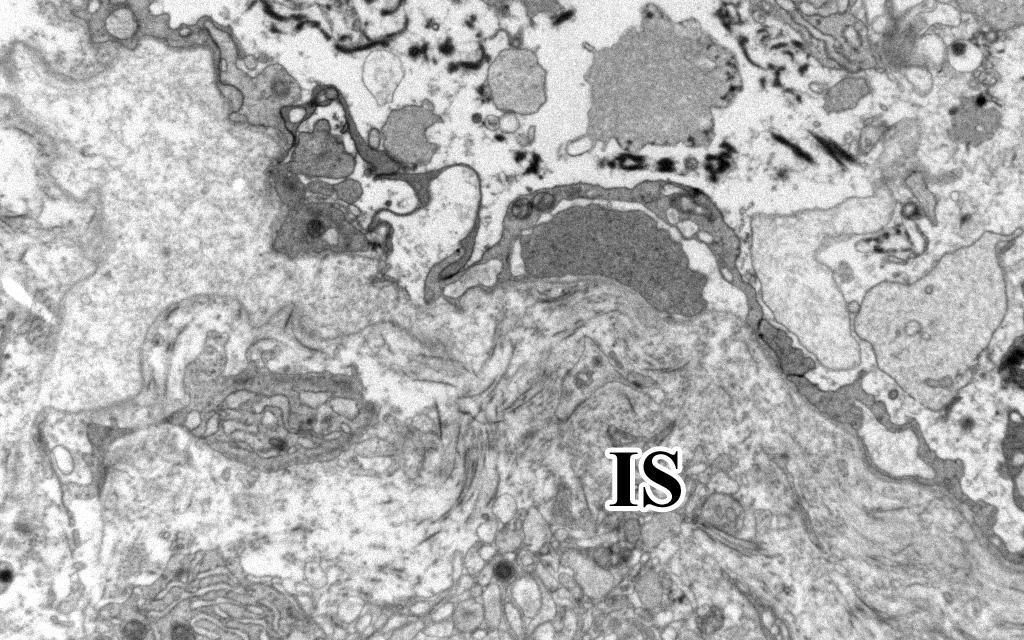
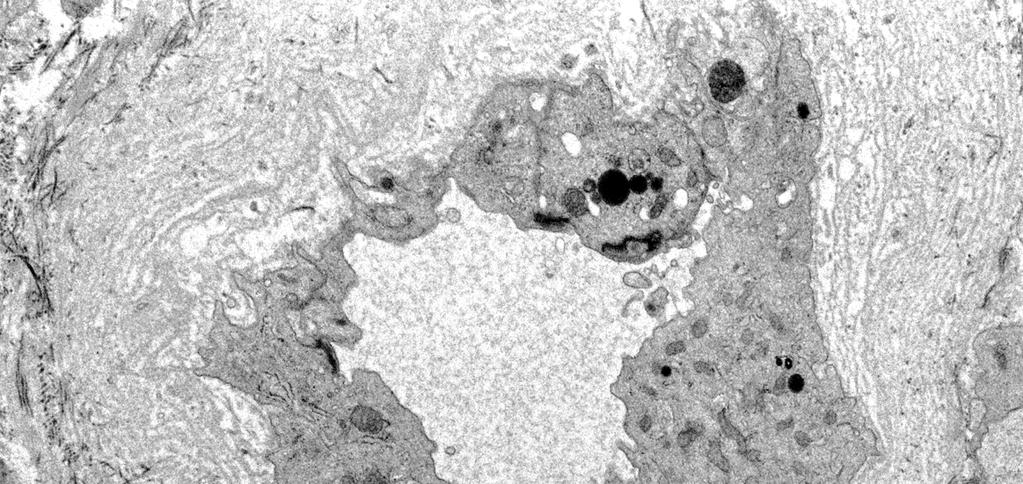
11 Peritubular capillaritis on EM Hypertrophy of endothelial cells, accumulation and emigration of ly-s into the interstitium; CTL-mediated lysis Normal E-selectin ICAM-1 VCAM-1
12 Tubulointerstitial rejection Interstitial infiltrates rich in CTLs, oedema, tubular HLA-DR expression, and tubulitis CD8 +



13 Tubulitis: tubular expression of chemokines induce CTLs to invade the tubules; CTLs injure tubular epithelial cells CTL CTL Apo CTL Apo CTL CTL


14 Subsiding tubulointerstitial rejection: nodular infiltrates around newly formed lymphatic vessels; Tregs, CD4 +, CD8 +, CD68 + ; scanty tubulitis; oedema Ø


15 Differential diagnosis of tubulointerstitial rejection Acute pyelonephritis Infiltrates rich in neutrophils, neutrophilic tubulitis
16 Differential diagnosis of tubulointerstitial rejection Acute pyelonephritis - neutrophilic tubulitis Polyomavirus nephropathy - nuclear inclusion bodies Drug-induced TIN - faint tubular HLA-DR staining Post-transplant lymphoproliferative disease - predominance of B-lymphocytes


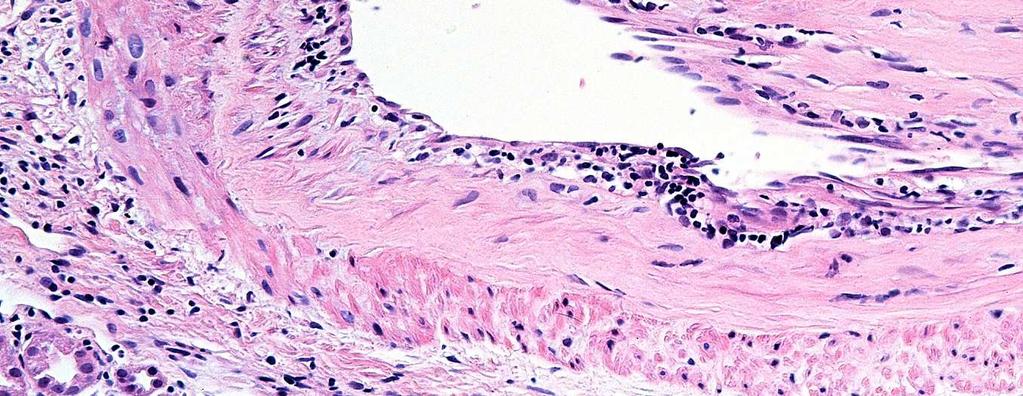
17 Vascular rejection Infiltration of the intima by lymphocytes + monocytes Involves the large arteries more frequently than the interlobular arteries
18 Differential diagnosis Intimal arteritis is pathognomic for acute T-cell-mediated rejection

19 Transplant glomerulitis Infiltration of the capillary loops by lymphocytes + monocytes Isolated transplant glomerulitis: in 10% of cases with acute T-cell-mediated rejection
20 Differential diagnosis Recurrent or de novo proliferative GN (rejection: no glomerular immune deposits)
21 Clinical correlation of acute T-cellmediated rejection Most common cause of a graft dysfunction in the first 3 months after Tx Sudden asymptomatic rise in the serum creatinine level


22 Outcome of acute T-cell-mediated rejection Tubulointerstitial rejection responds well to high-dose iv. steroid therapy Vascular rejection can be reversed with anti-lymphocyte antibody preparations If not: fibrous obliteration of arteries graft loss
23 Acute alloantibody-mediated rejection Donor-specific HLA class I antibodies Complement-mediated cytotoxic injury to the endothelial cells
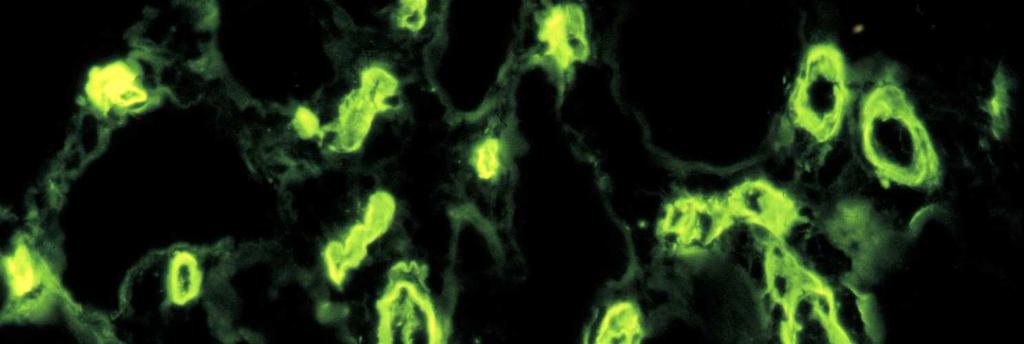
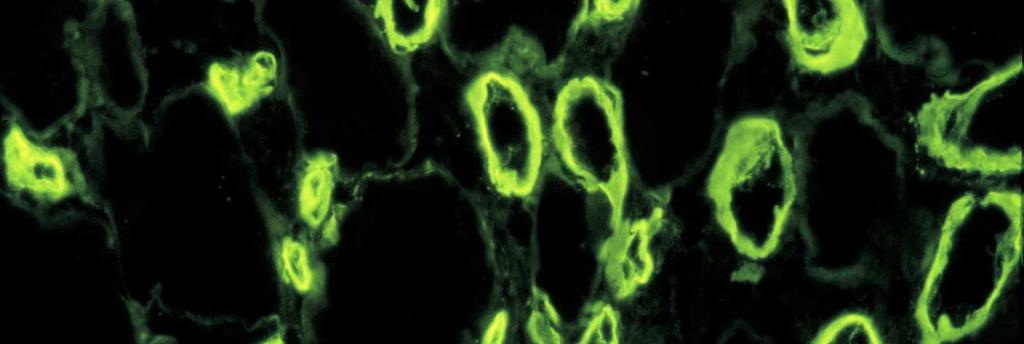
24 Acute alloantibody-mediated rejection Donor-specific HLA class I antibodies Complement 4d degradation product binds to PTC endothelial cells This stable molecule is detected by IF Complement-mediated cytotoxic injury to the endothelial cells


25 Evaluation of C4d Immunofluorescence on frozen sections is more sensitive than immunohistochemistry on paraffin sections



 Transmural arteritis and/or")
26 Diagnostic criteria of acute alloantibodymediated reejction: C4d along PTCs; evidence of tissue injury; demonstration of donor-specific antibodies Evidence of tissue injury 1) ATN-like, minimal inflamm. 2) Capillary-NG margination and/or thromboses 3) Transmural arteritis and/or arterial fibrinoid necrosis Racusen et al. AJT 3:1-7, 2003


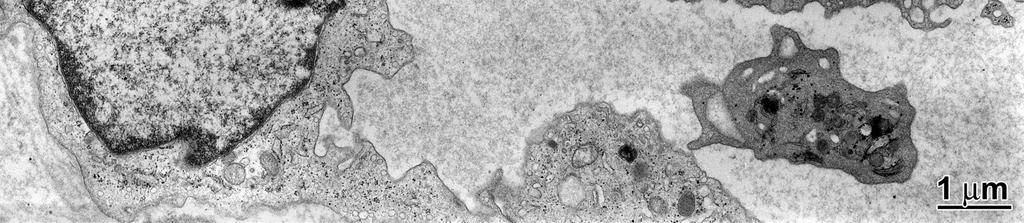
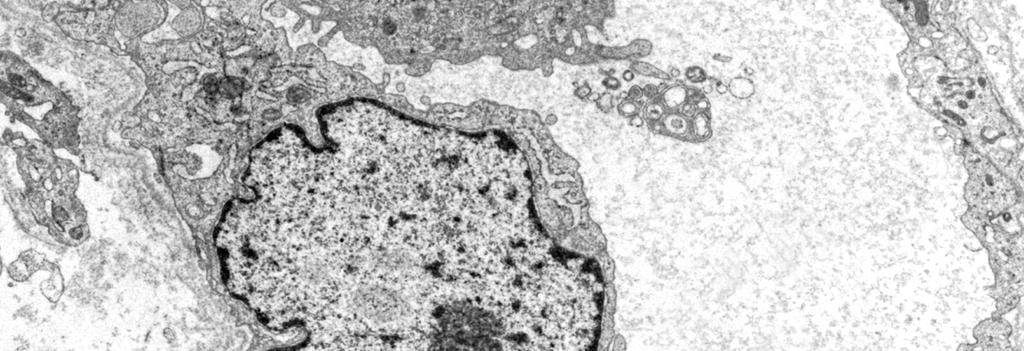
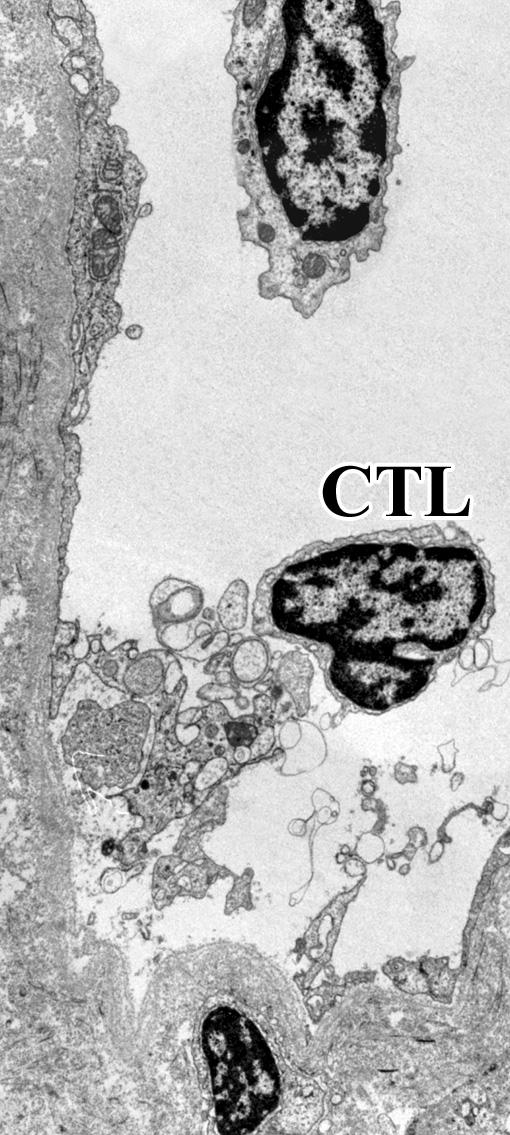
27 Cytotoxic injury to PTC endothelial cells manifests in lysis + apoptosis Liptak et al. AJT 5:2870, 2005
28 Differential diagnosis TMA secondary to CNI toxicity Anti-cardiolipin sy Recurrent HUS Viral infection due to CMV or parvovirus B19
29 Differential diagnosis TMA secondary to CNI toxicity Anti-cardiolipin sy Recurrent HUS Viral infection due to CMV or parvovirus B19 Clue None of these displays C4d positivity along the peritubular capillaries


30 Clinical correlation Infrequent (2-8%) Most common in the first few weeks after Tx; oligoanuria develops within days Therapeutic efforts may reverse the rejection process Poor prognosis
31 Chronic rejection Ongoing, smouldering alloimmune damage to the allograft, mediated predominantly by alloantibodies Vascular lesions are characteristic Transplant arteriopathy Transplant glomerulopathy Transplant capillaropathy
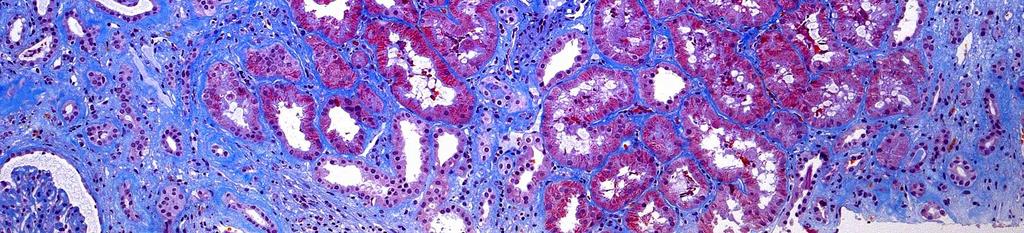
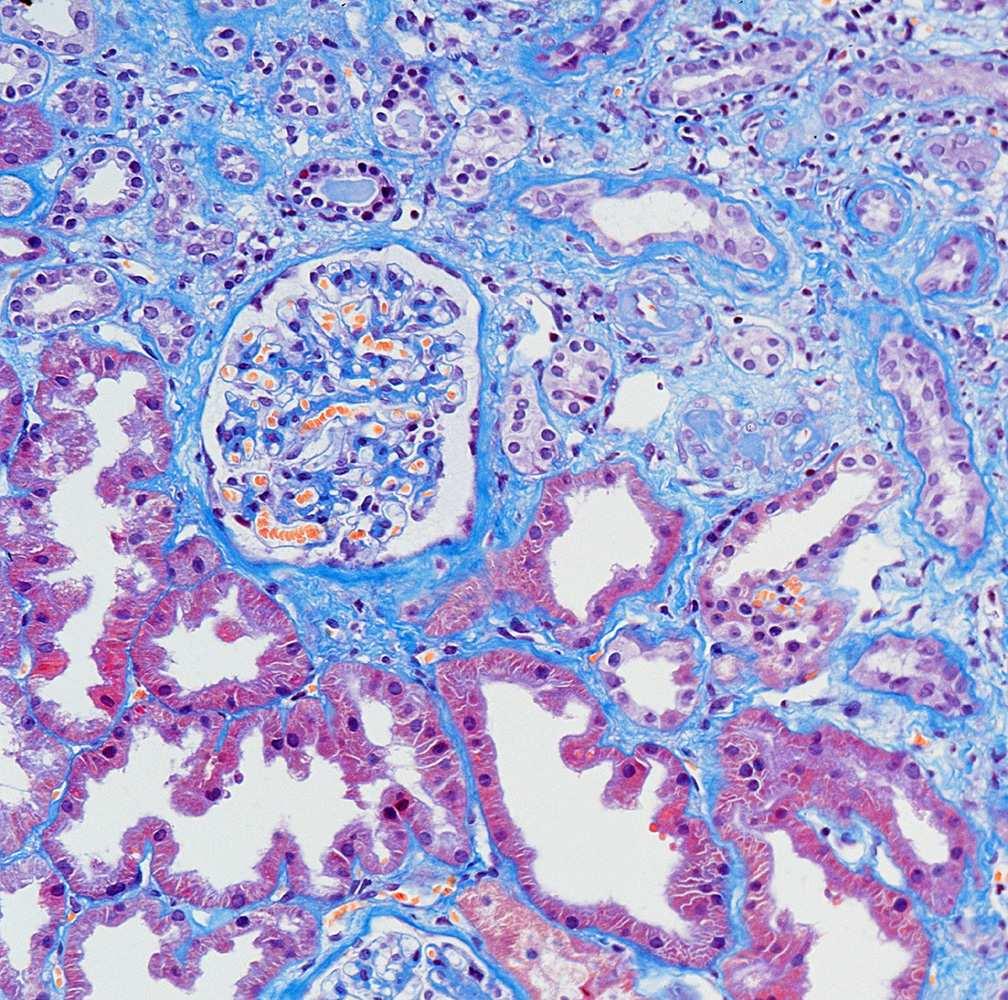
32 Vascular lesions of chronic rejection are associated with interstitial fibrosis and tubular atrophy (IF/TA)


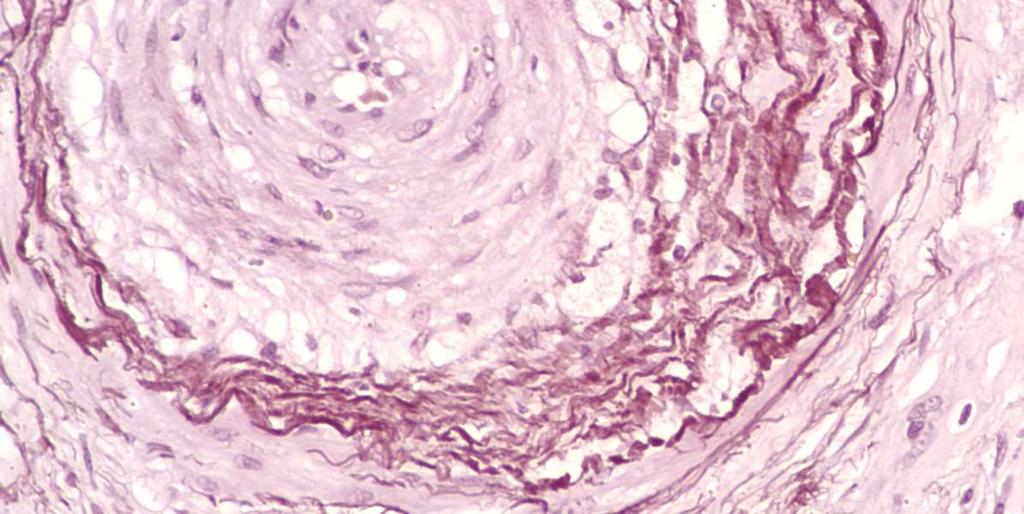
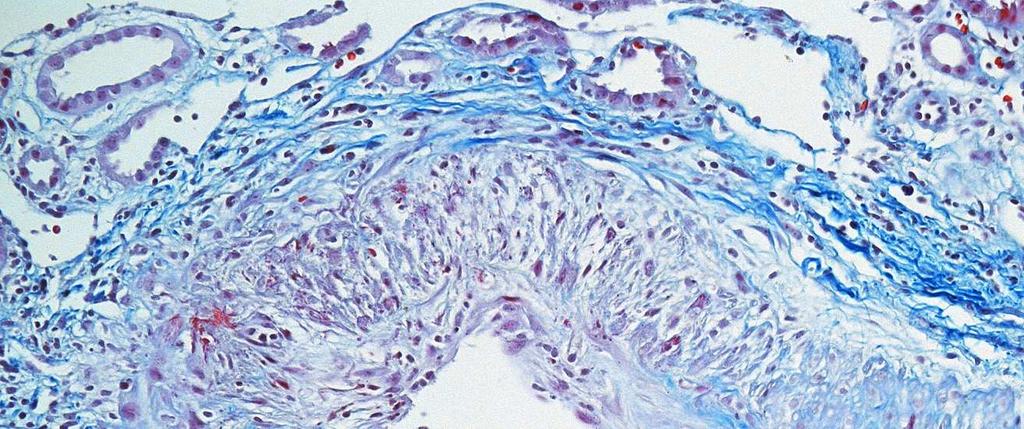
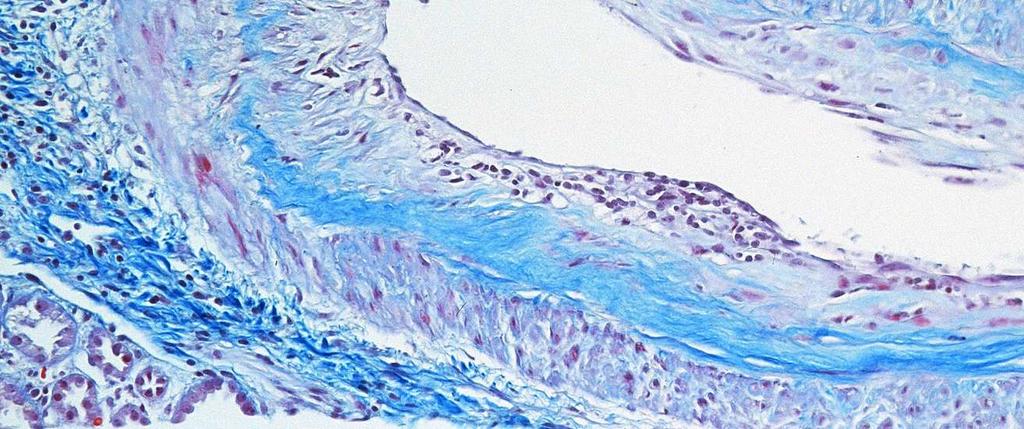
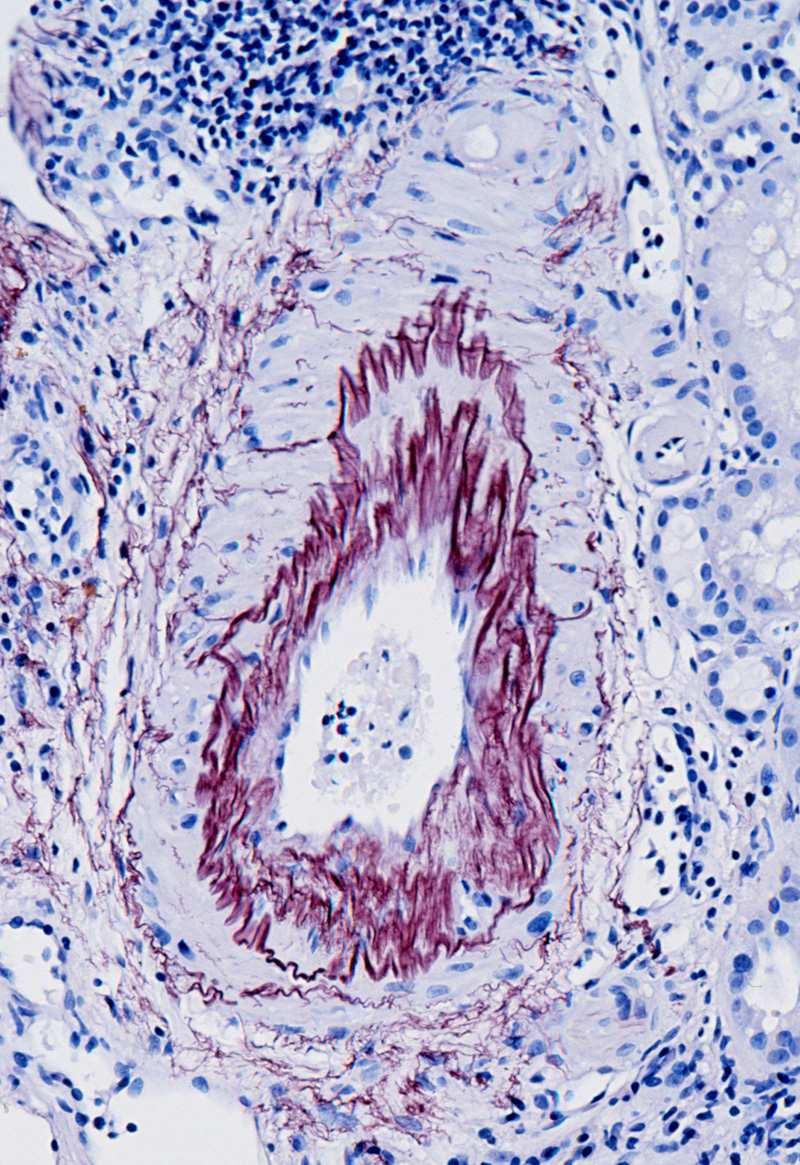
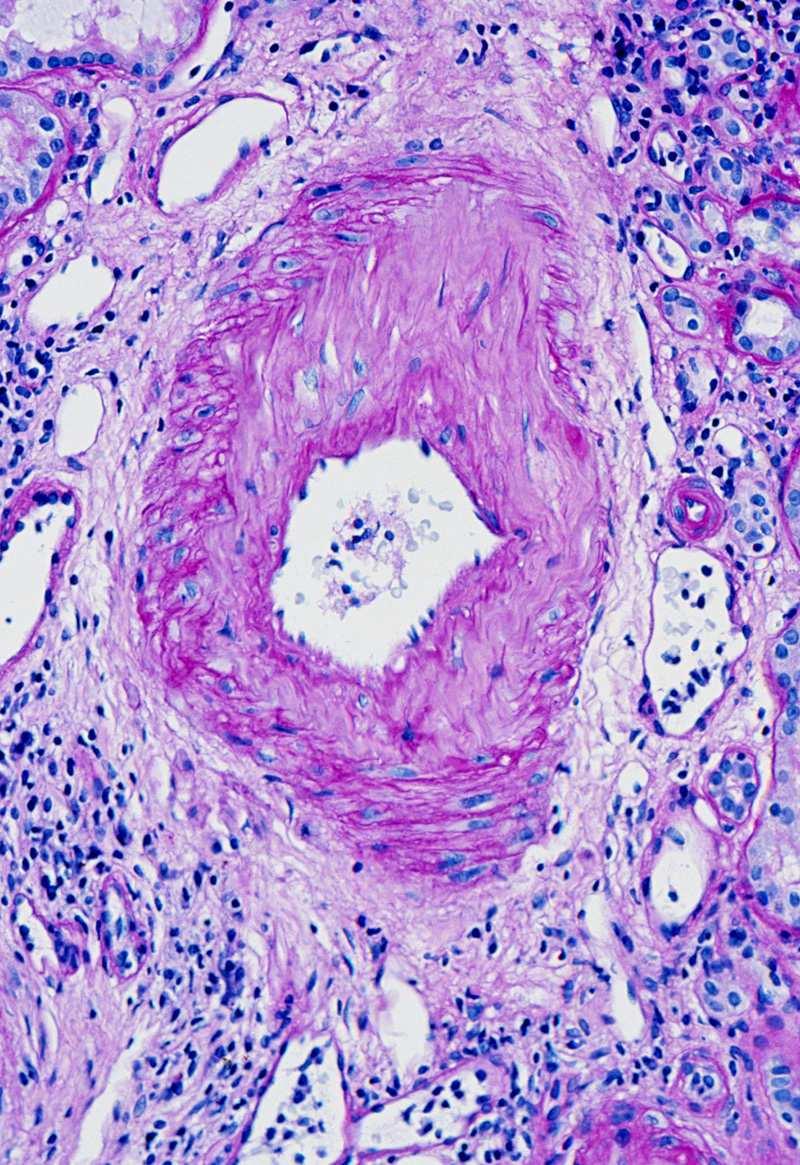
33 Tx arteriopathy: new-onset intimal fibrosis Absence of elastosis


34 Tx arteriopathy is more pronounced in the arcuate and larger arteries than in the small arteries of the superficial cortex
35 Consequence Chronic progressive ischemic injury to the graft parenchyma
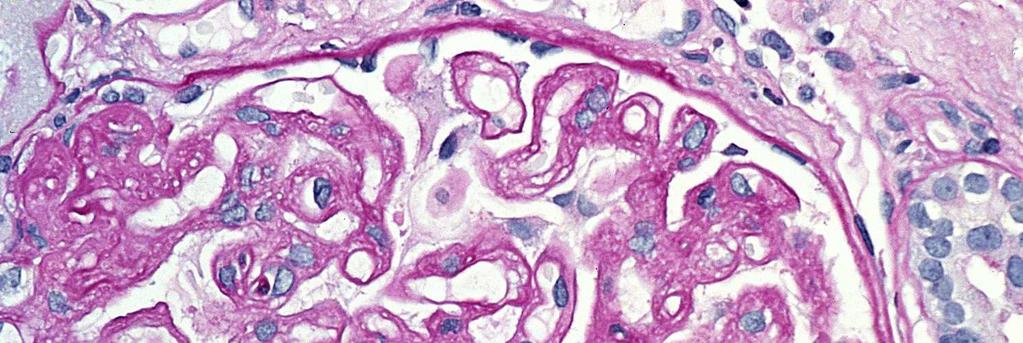
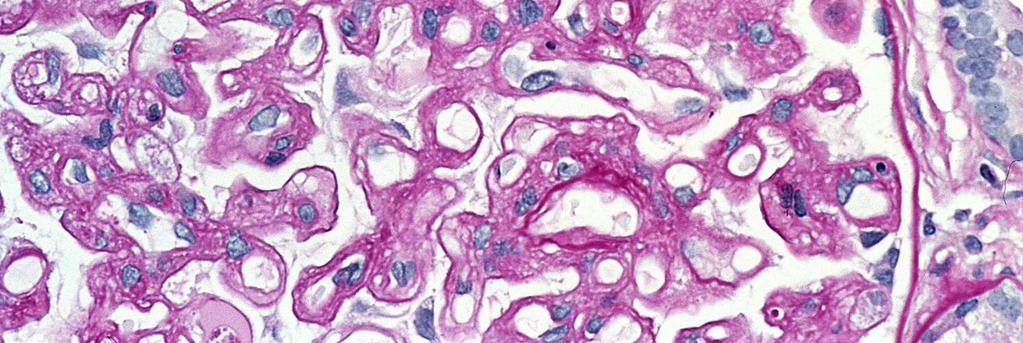
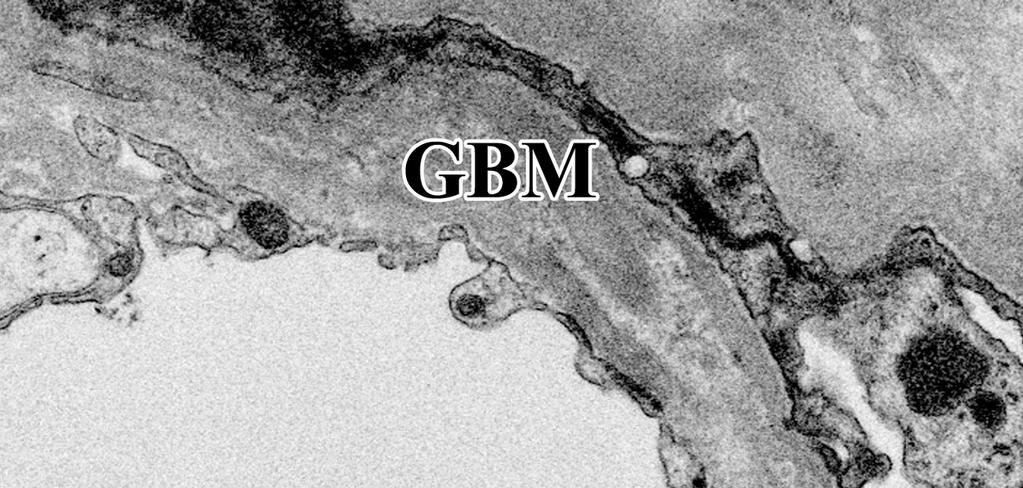
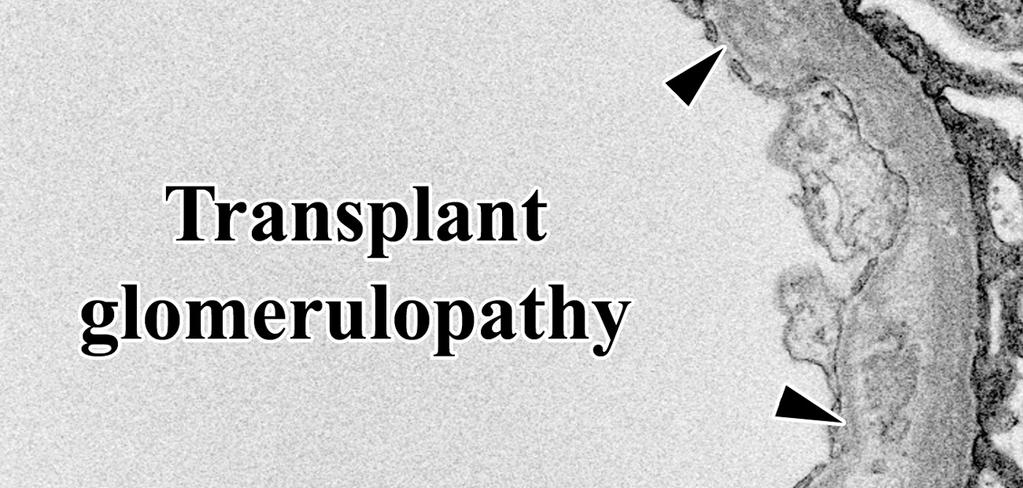
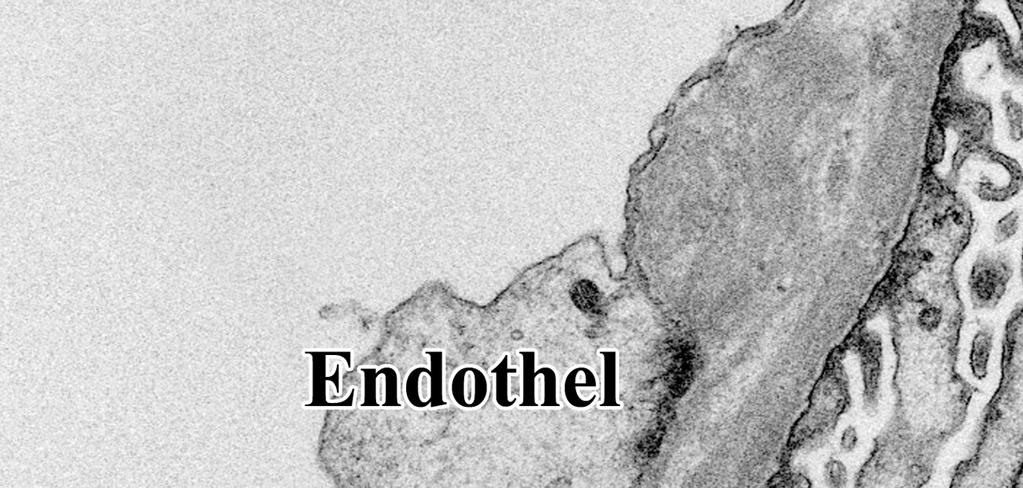
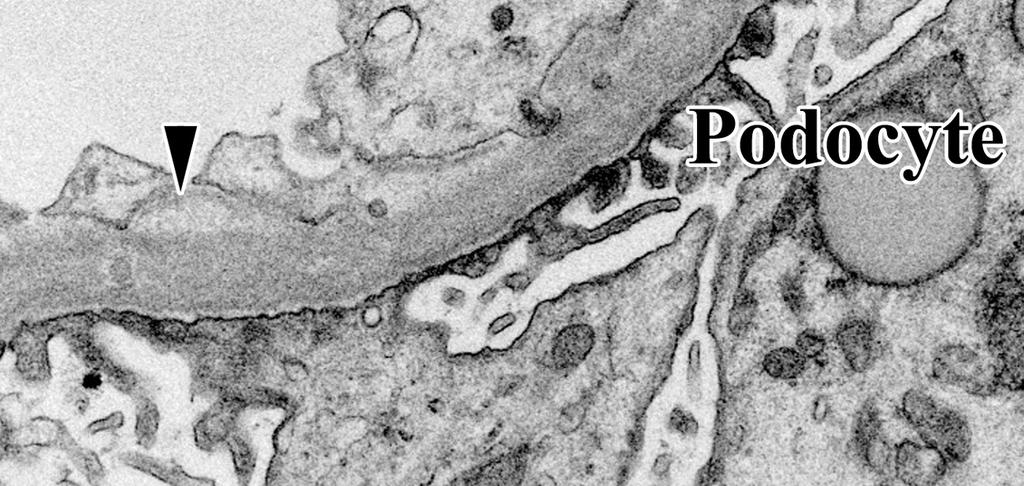
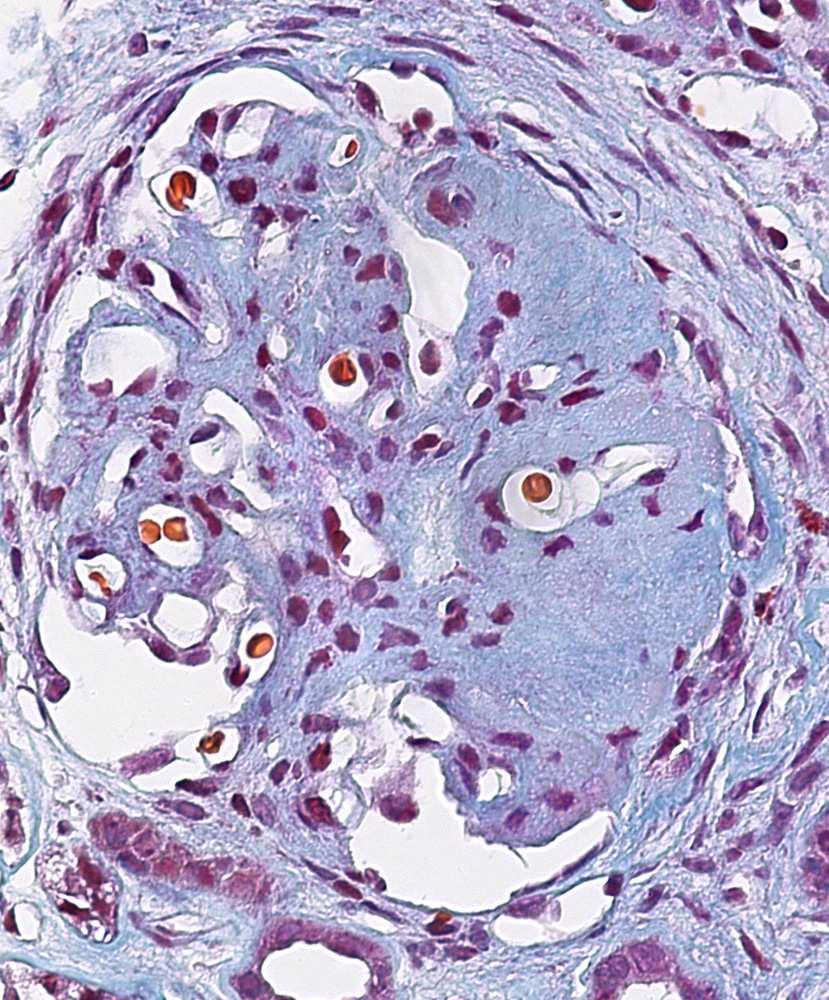
36 Tx glomerulopathy: double-contoured loops; EM: newly formed BM layer(s)
37 Consequences Proteinuria Focal glomerular obsolescence


38 Tx glomerulopathy may resemble to recurrent or de novo MPGN; no immunocomplexes on IF
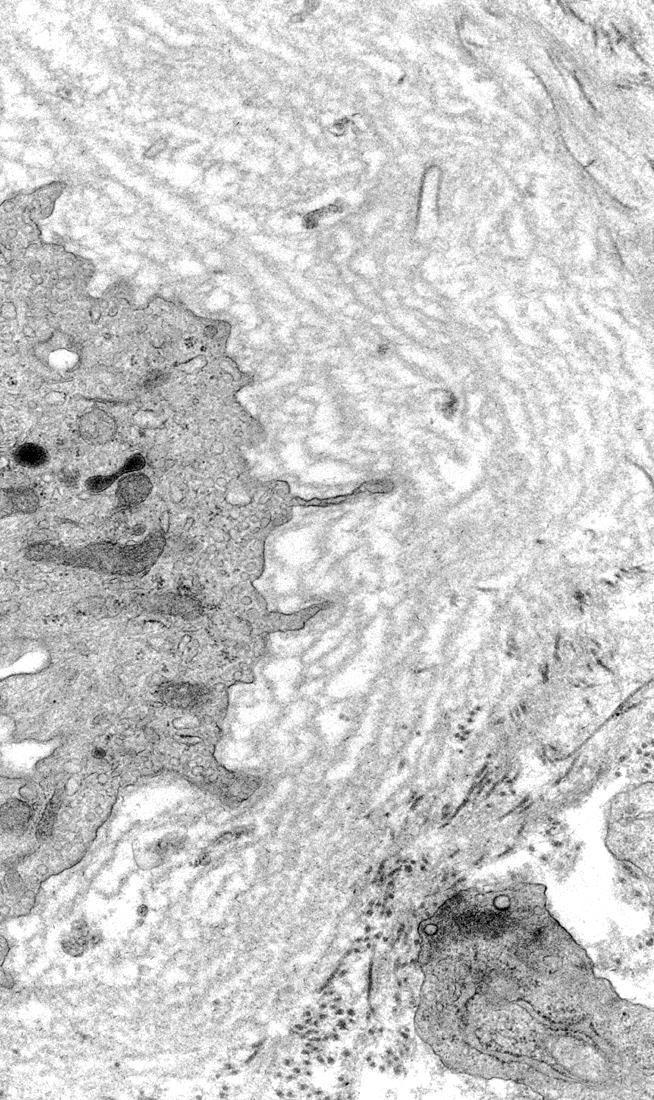
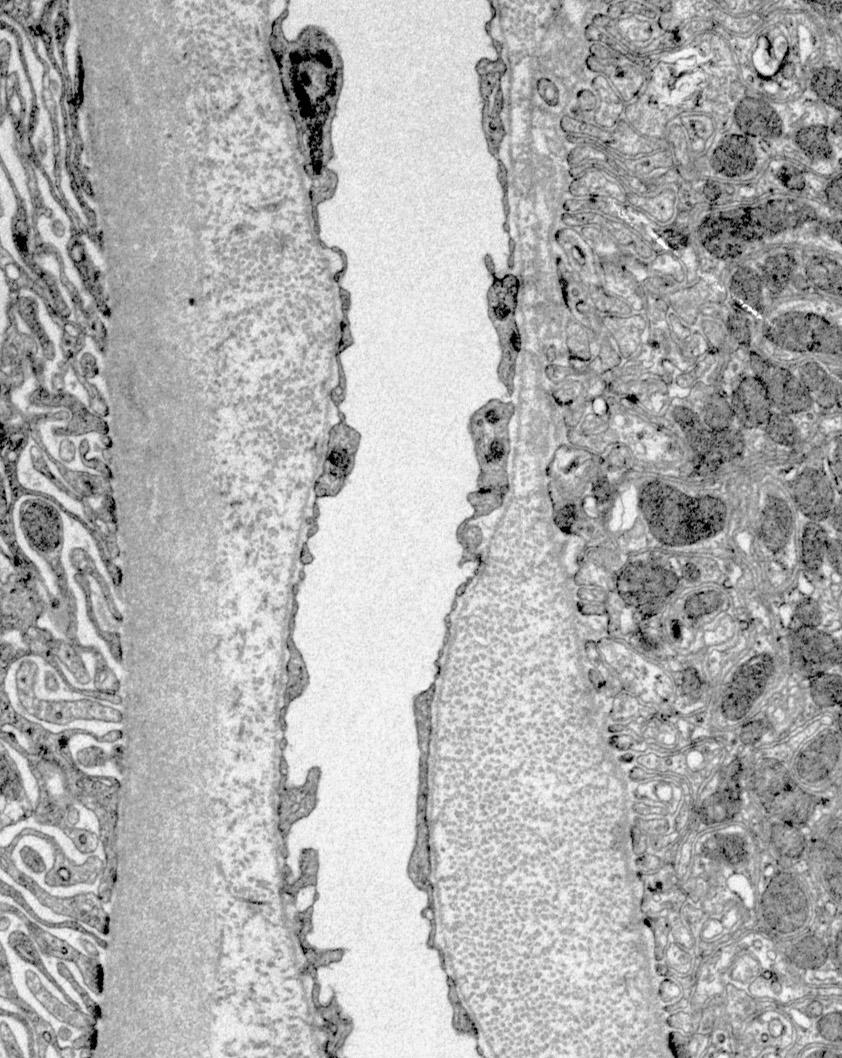
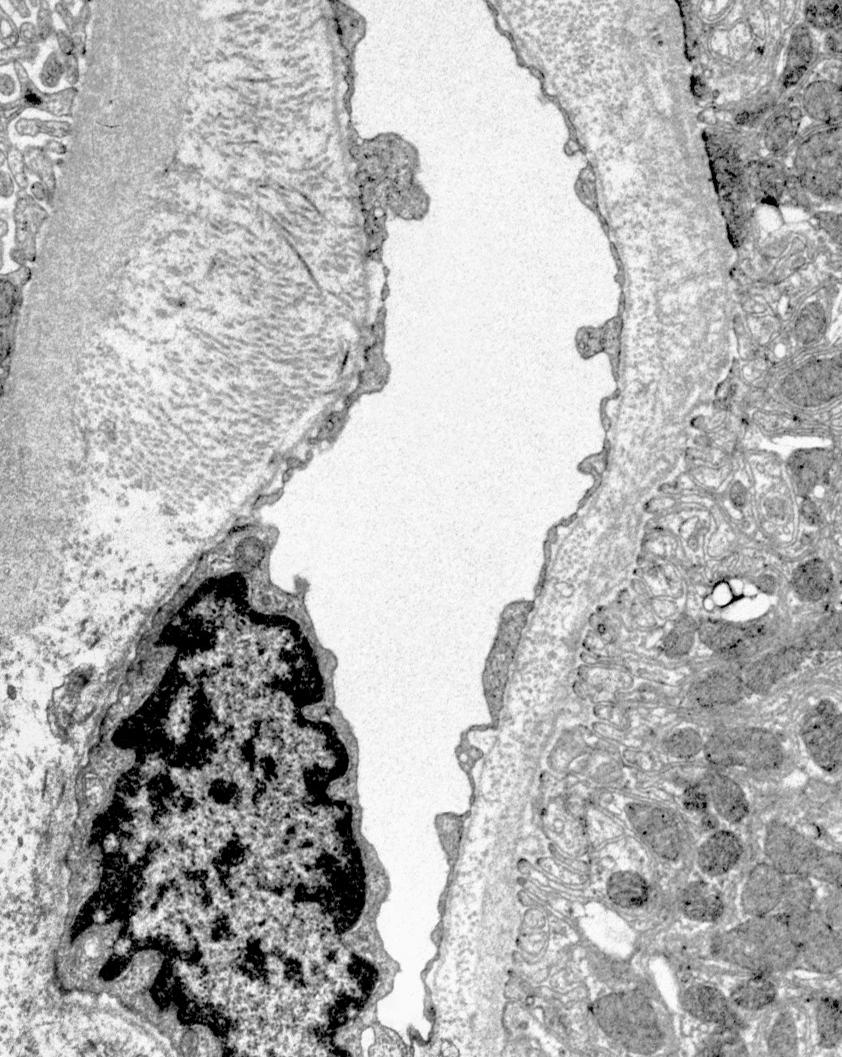
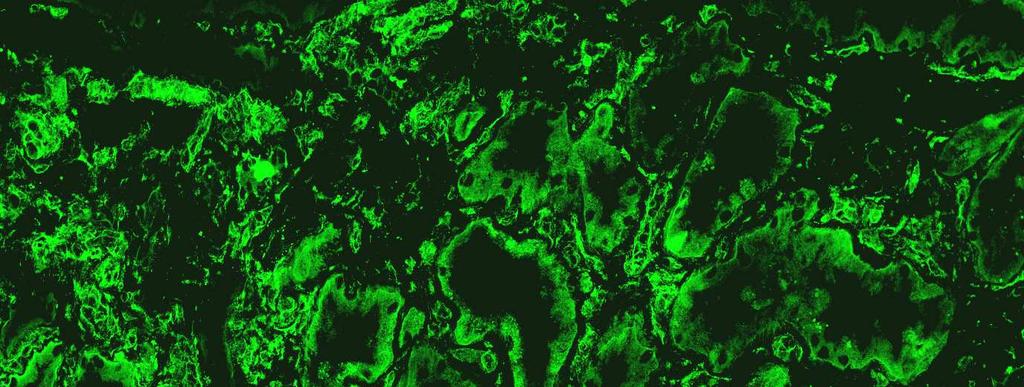
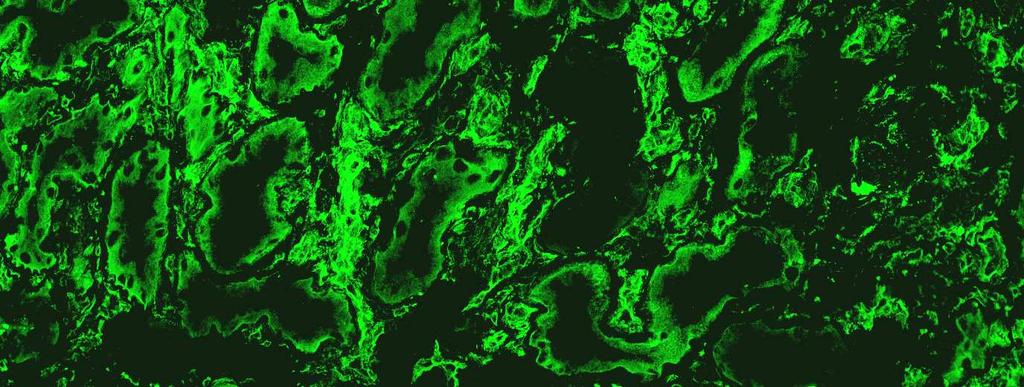
39 Tx capillaropathy: circumferentially laminated BM; pathognomic: 5 or more BM layers; C4d+ along PTCs




40 Tx capillaropathy on light microscopy: thickened and laminated BMs; EM is more sensitive in the verification of TxC Well-functioning graft Chronic rejection
41 Consequence A progressive decrease in the number of PTCs
42 Diagnostic triad of chronic antibodymediated rejection 1) TxA, TxG, TxC either alone or in combination 2) Diffuse C4d deposition in PTCs 3) Presence of donor-specific antibody Solez et al. AJT 7:1-9, 2006

43 Chronic active T-cell-mediated rejection Lymphocytes in arterial intimal fibrosis
44 Clinical correlation of chronic rejection Major cause of graft loss after 1 year Insidious, progressive decline in the GFR, frequently accompanied by proteinuria (often in the nephrotic range) and hypertension
45 Calcineurin inhibitor toxicity Cyclosporin and tacrolimus can cause acute or chronic nephrotoxicity; the lesions are identical Acute toxicity Toxic tubulopathy Vascular toxicity - Acute arteriolopathy - TMA Chronic toxicity Hyaline arteriolopathy Liptak P, Ivanyi B. Nature Clin Pract Nephrol 2: , 2006


46 Toxic tubulopathy Isometric vacuolization of the proximal straight tubules
47 The features of this tubulopathy cannot be distinguished from those of radiocontrast nephrotoxicity or osmotic nephrosis, Differential diagnosis conditions to be considered while making the diagnosis


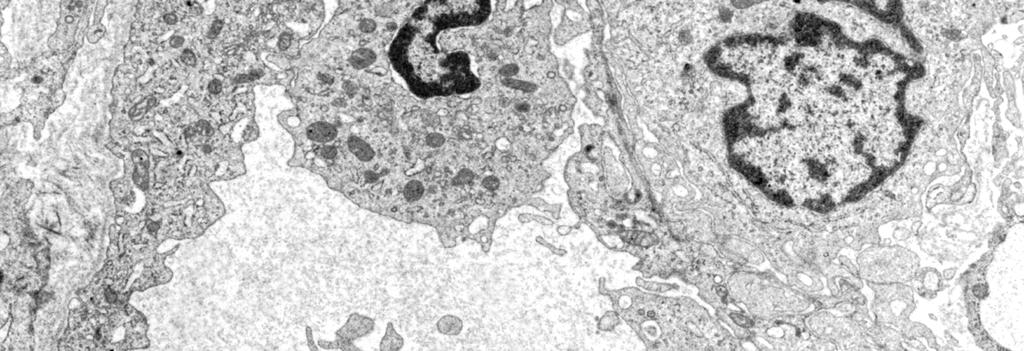
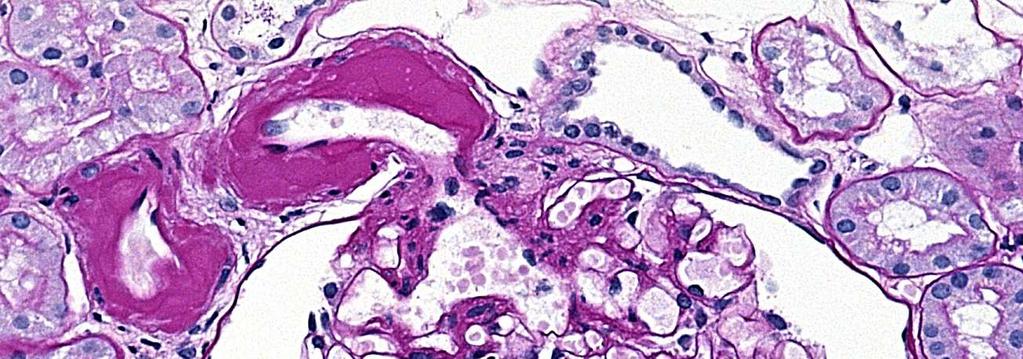
48 Acute arteriolopathy: SMC injury; replacement of damaged myocytes by rounded plasma protein insudates
49 Clinical correlation Acute dysfunction The serum drug level is usually elevated Toxic tubulopathy is reversible Acute arteriolopathy may be irreversible


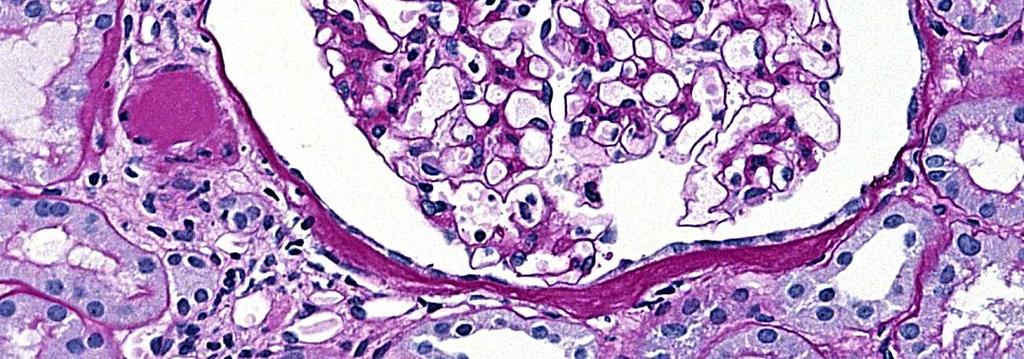
50 TMA: thrombi in glomerular capillary loops
51 Differential diagnosis CNI-induced TMA cannot be differentiated from other forms of TMA by morphology alone Pronounced arterial changes are not typical of CNI-induced TMA Acute humoral rejection (C4d+) Recurrent HUS
52 Clinical correlation Rare Resembles the HUS If the lesions are associated with extensive thrombosis, graft loss develops




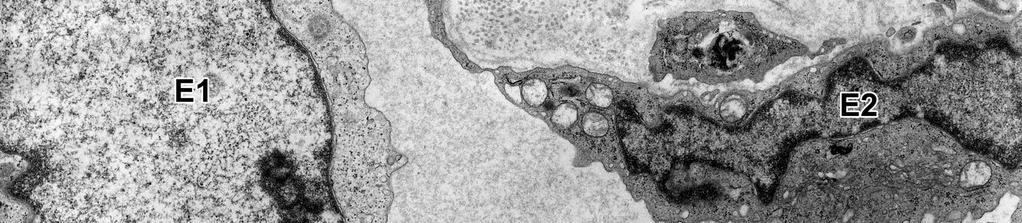
53 Chronic toxicity: hyaline arteriolopathy The damaged SMCs are replaced by beaded hyaline deposits that bulge into the adventitia The insudates are positive for IgM and C3


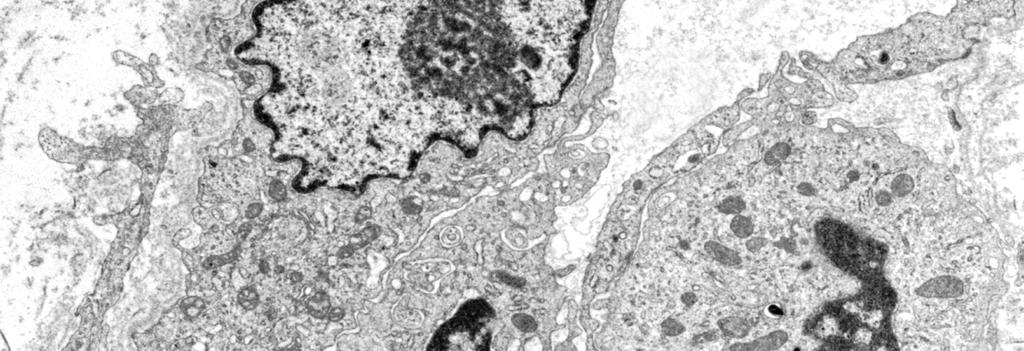
54 Hyaline material (H) is present at sites where media SMCs have dropped out previously. E - swollen endothelial cells, A - apoptotic SMCs.
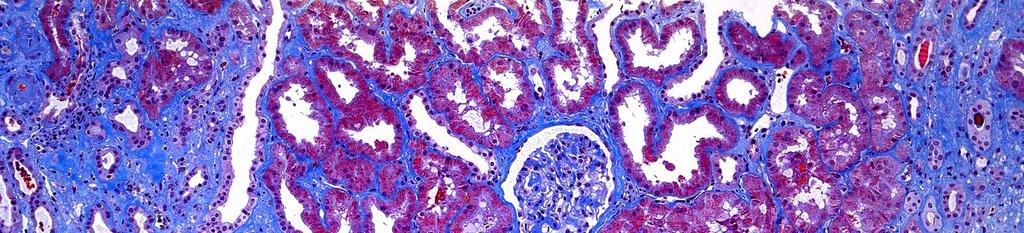
55 Hyaline arteriolopathy is associated with striped IF/TA
56 Differential diagnosis Hyalinosis in ageing, hypertension and diabetes: Mainly subendothelial and rarely extends into the adventitia Necrosis of the SMCs is not observed
57 Clinical correlation Chronic toxicity occurs several months after Tx; the incidence increases with time A slow, insidious rise in the serum creatinine level The kidney damage is irreversible
58 Ageing/hypertension: intimal fibroelastosis; subendothelial arteriolar hyalinosis; patchy segmental/global glomerulosclerosis; IF/TA
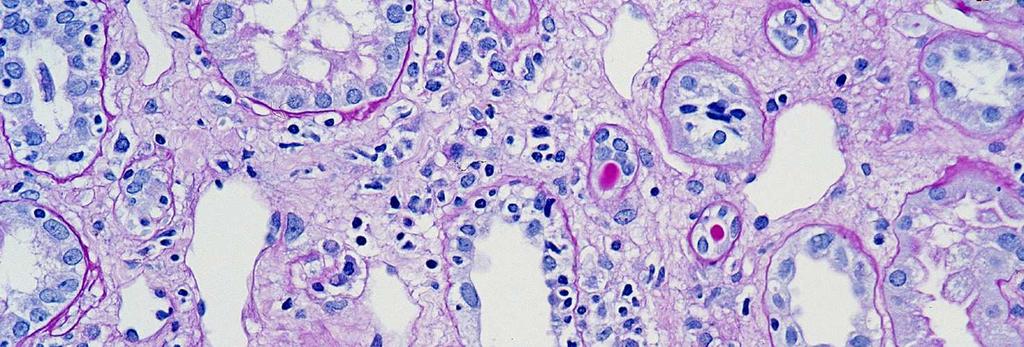
59 Polyomavirus nephropathy The BK polyomavirus exhibits tropism for the renal tubular epithelium, where it establishes latent infection Vigorous immunosuppression can lead to reactivation of the infection and the development of PVN The definitive diagnosis requires an allograft Bx Drachenberg et al. Hum Pathol 36: , 2005


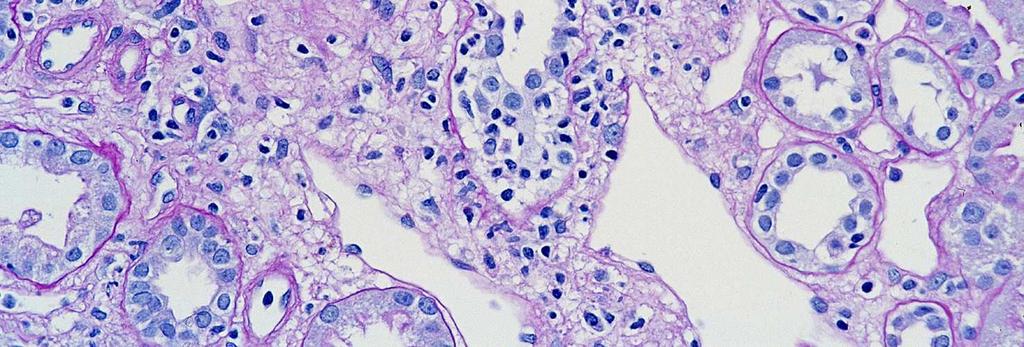
60 Viral replication results in cytopathic changes (nuclear enlargement, inclusion bodies, tubular cell injury)

61 Massive replication leads to cytolysis of tubular epithelial cells and interstitial inflammation


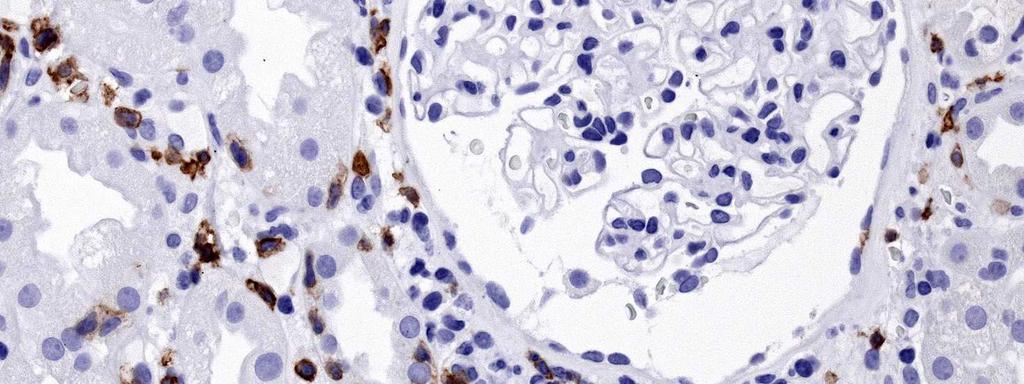
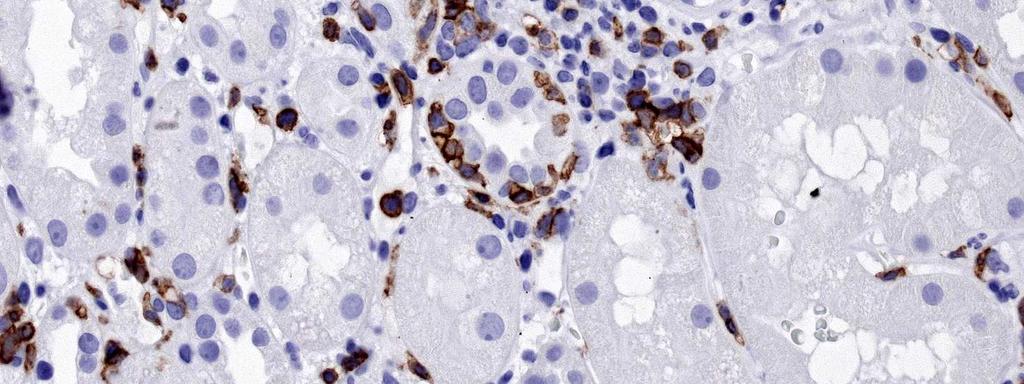
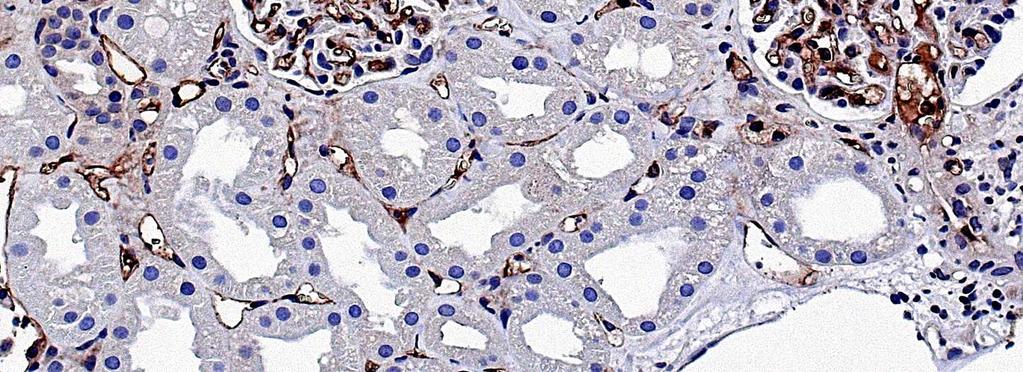
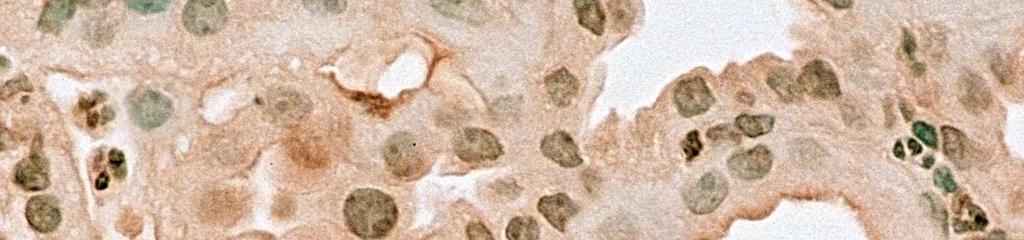
62 Immunostaining with SV40 large T-cell antigen confirms the diagnosis


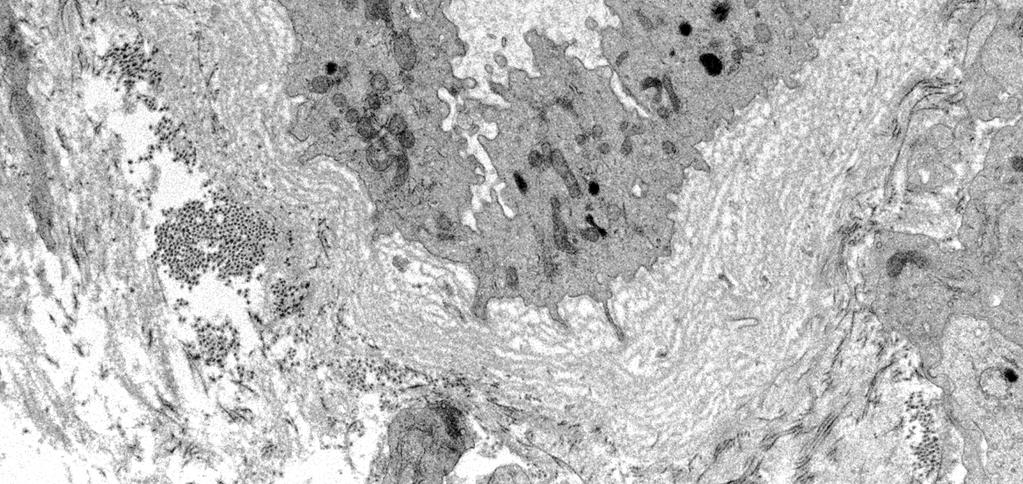
63 EM is also diagnostic: the virions are 40 nm in diameter, arranged in a paracrystalloid structure
64 Differential diagnosis Other viral infections (adenovirus: nm; CMV: nm) Acute rejection (lack of nuclear inclusion bodies, intense tubular HLA-DR expression) Chronic rejection (lack of nuclear inclusion bodies, negative confirmatory tests) Liptak et al. Nature Clin Pract Nephrol 2: , 636, 2006
65 Histologic patterns and clinical stages of PVN Pattern A Viral cytopathic changes with no or only minimal inflammation Early stage No dysfunction Urinary decoy cells Favorable prognosis Hirsch et al. Transplantation 79: , 2005
66 Histologic patterns and clinical stages of PVN Pattern A Viral cytopathic changes with no or only minimal inflammation Pattern B Cytopathic and cytolytic changes with interstitial inflammation Early stage No dysfunction Urinary decoy cells Favorable prognosis Fully developed stage A gradually decreasing renal function Graft loss can exceed 50% Hirsch et al. Transplantation 79: , 2005
67 Histologic patterns and clinical stages of PVN Pattern A Viral cytopathic changes with no or only minimal inflammation Pattern B Cytopathic and cytolytic changes with IS inflammation Pattern C IF/TA Variable cytopathic and inflammatory changes Early stage No dysfunction Urinary decoy cells Favorable prognosis Fully developed stage A gradually decreasing renal function Graft loss can exceed 50% Late/sclerosing stage A severe dysfunction Graft loss is likely Hirsch et al. Transplantation 79: , 2005
68 T-cell-mediated rejection Peritubular capillaritis IS infiltrates rich in CTLs Lymphocytic tubulitis + Intimal arteritis + Glomerulitis Alloantibody-mediated rejection C4d+ along PTCs Evidence of tissue injury: - arterial fibrinoid necrosis - microthrombi - neutrophilic capillaritis - ischemic tubular damage Summary of acute lesions CNI toxicity Isometric vacuolation of tubules Early-stage hyalinization of individual myocytes in afferent arterioles
69 Summary of chronic lesions Rejection Arterial intimal fibrosis Double-contoured glomerular capillary loops PTC BM lamination IF/TA C4d+ along PTCs Ageing/hypertension Intimal fibroelastosis in arteries Nonspecific arteriolar hyalinosis Patchy glomerular sclerosis IF/TA CNI toxicity Hyaline arteriolopathy Patchy glomerular sclerosis Striped IF/TA Polyomavirus NP Cytopathic effects (inclusion bodies and tubular epithelial injury) A varying degree of IS inflammation, IF/TA
70 Post-transplantation transplantation glomerulonephritis Recurrences of GN tend to occur in the first few weeks after Tx De novo GN usually manifests at least a year after Tx
71 Post-transplantation transplantation glomerulonephritis FSGS, MPGN, IgAN and idiopathic diarrhea- negative HUS recur fequently Membranous nephropathy, FSGS, anti-gbm nephritis in Alport patients, and drug-induced TMA are the most common de novo diseases Recurrent or de novo GN often coexists with acute and/or chronic rejection and/or chronic CNI- toxicity, and contribute together to allograft loss Ivanyi B. Nature Clin Pract Nephrol 4: , 457, 2008

.")
72 Recurrent FSGS Proteinuria developed some days after the implantation. 1st Bx, EM: effacement of foot processes. 2. Bx (3 mo later). The FSGS lesion in two glomeruli




73 Coexistence of transplant GP and membranous NP Bx performed because of nephrotic sy that developed 26 mo after Tx.
74 Kidney allograft from a deceased donor ~10 years later: end-stage allograft disease
75 Kidney allograft from a deceased donor Early insults Late insults Additional insults The insults cumulate: end-stage allograft disease Nankivell BJ, Chapman JR. Transplantation 2006;81:
76 Tx Early insults Ischemia reperfusion injury Acute tubular necrosis Acute/subclinical rejection Acute CNI toxicity Late insults Additional insults End-stage allograft disease
77 Tx Early insults Ischemia reperfusion injury Acute tubular necrosis Acute/subclinical rejection Acute CNI toxicity Late insults Chronic rejection Chronic CNI toxicity Polyomavirus NP Hypertension Recurrent/de novo glomerular disease Additional insults End-stage allograft disease
78 Tx Early insults Ischemia reperfusion injury Acute tubular necrosis Acute/subclinical rejection Acute CNI toxicity Additional insults Architectural degradation Cortical ischemia Persistent chronic inflamm. Accelerated ageing Cytokine excess Epithelial-mesenchymal transition and fibrosis Late insults Chronic rejection Chronic CNI toxicity Polyomavirus NP Hypertension Recurrent/de novo glomerular disease End-stage allograft disease

79 Renal allograft removed for end-stage kidney allograft failure The kidney is shrunken, the cortex is no longer separated from the medulla, and the large arteries display severe atherosclerosis
80 Conclusions The application of light microscopic stainings on serial sections the full immunofluorescence panel (C4d,( HLA IgG, IgA, IgM,, C3) tissue sampling for optional EM comparison with a time-zero biopsy C4d, HLA-DR, enables the pathologist to achieve etiologic diagnoses
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Biopsy Features of Kidney Allograft Rejection Banff B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Primer: histopathology of calcineurin-inhibitor toxicity in renal allografts
 Primer: histopathology of calcineurin-inhibitor toxicity in renal allografts Peter Liptak and Bela Ivanyi* SUMMARY Calcineurin inhibitors (ciclosporin and tacrolimus) can cause acute and chronic nephrotoxicity.
Primer: histopathology of calcineurin-inhibitor toxicity in renal allografts Peter Liptak and Bela Ivanyi* SUMMARY Calcineurin inhibitors (ciclosporin and tacrolimus) can cause acute and chronic nephrotoxicity.
Interpretation of Renal Transplant Biopsy. Arthur H. Cohen Wake Forest University School of Medicine Winston-Salem, North Carolina USA
 Interpretation of Renal Transplant Biopsy Arthur H. Cohen Wake Forest University School of Medicine Winston-Salem, North Carolina USA Renal Transplant Biopsies Tissue Processing Ideal world process as
Interpretation of Renal Transplant Biopsy Arthur H. Cohen Wake Forest University School of Medicine Winston-Salem, North Carolina USA Renal Transplant Biopsies Tissue Processing Ideal world process as
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Statement of Disclosure
 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference
 The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Evolution of the approaches toward grading and classifying chronic changes in the renal allograft: Banff classification updates III
 EDITORIAL Advance Access publication 24 February 2014 Evolution of the approaches toward grading and classifying chronic changes in the renal allograft: Banff classification updates III Histopathology
EDITORIAL Advance Access publication 24 February 2014 Evolution of the approaches toward grading and classifying chronic changes in the renal allograft: Banff classification updates III Histopathology
Recognition and Treatment of Chronic Allograft Dysfunction
 Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Kidney Summary. Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA
 Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Renal Pathology- Transplantation. Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic
 Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Histopathological evaluation of renal allograft biopsies in Nepal: interpretation and significance
 Nepal Medical Association Building Exhibition Road, Kathmandu Journal of Pathology of Nepal (2012) Vol. 2, 172-179 Association of Clinical Pathologist of Nepal-2010 Journal of PATHOLOGY of Nepal www.acpnepal.com
Nepal Medical Association Building Exhibition Road, Kathmandu Journal of Pathology of Nepal (2012) Vol. 2, 172-179 Association of Clinical Pathologist of Nepal-2010 Journal of PATHOLOGY of Nepal www.acpnepal.com
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Review of Rituximab and renal transplantation. Dr.E Nemati. Professor of Nephrology
 Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Histopathological findings in transplanted kidneys
 Katsuma et al. Renal Replacement Therapy (2017) 3:6 DOI 10.1186/s41100-016-0089-0 REVIEW Histopathological findings in transplanted kidneys Ai Katsuma, Takafumi Yamakawa, Yasuyuki Nakada, Izumi Yamamoto
Katsuma et al. Renal Replacement Therapy (2017) 3:6 DOI 10.1186/s41100-016-0089-0 REVIEW Histopathological findings in transplanted kidneys Ai Katsuma, Takafumi Yamakawa, Yasuyuki Nakada, Izumi Yamamoto
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Kidneytransplant pathologyrelatedto immunosuppressiveagents
 Kidneytransplant pathologyrelatedto immunosuppressiveagents Helmut Hopfer Pathologie Women, 53 years old. 16 months after kidney transplantation for diabetic nephropathy. Metabolicsyndromeandcoronaryheartdisease.
Kidneytransplant pathologyrelatedto immunosuppressiveagents Helmut Hopfer Pathologie Women, 53 years old. 16 months after kidney transplantation for diabetic nephropathy. Metabolicsyndromeandcoronaryheartdisease.
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Interstitial Inflammation
 Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
Acute renal failure (ARF) in the transplanted kidney represents a
 in the transplanted kidney represents a") Acute Renal Failure in the Transplanted Kidney Kim Solez Lorraine C. Racusen Acute renal failure (ARF) in the transplanted kidney represents a high-stakes area of nephrology and of transplantation practice.
Acute Renal Failure in the Transplanted Kidney Kim Solez Lorraine C. Racusen Acute renal failure (ARF) in the transplanted kidney represents a high-stakes area of nephrology and of transplantation practice.
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification
 Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features.
 Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need
Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Chronic Active TCMR: clinical implications
 Chronic Active TCMR: i, iatr, i-ifta, and the clinical implications Roslyn B. Mannon, M.D. Professor of Medicine, Division of Nephrology Professor of Surgery, Division of Transplantation Director of Research,
Chronic Active TCMR: i, iatr, i-ifta, and the clinical implications Roslyn B. Mannon, M.D. Professor of Medicine, Division of Nephrology Professor of Surgery, Division of Transplantation Director of Research,
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Progressive histological damage in renal allografts is associated with expression of innate and adaptive immunity genes
 http://www.kidney-international.org & 2011 International Society of Nephrology see commentary on page 1254 Progressive histological damage in renal allografts is associated with expression of innate and
http://www.kidney-international.org & 2011 International Society of Nephrology see commentary on page 1254 Progressive histological damage in renal allografts is associated with expression of innate and
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy
 Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy Miklos Z. Molnar, 1 G. V. Ramesh Prasad, 2 Darren A. Yuen, 2,3 Serge Jothy, 4 and Jeffrey S. Zaltzman 2,5 1 Division of
Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy Miklos Z. Molnar, 1 G. V. Ramesh Prasad, 2 Darren A. Yuen, 2,3 Serge Jothy, 4 and Jeffrey S. Zaltzman 2,5 1 Division of
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
renoprotection therapy goals 208, 209
 Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
CKD in Other Organ Transplants
 CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Diagnosis and Management of Acute and Chronic Humoral Rejection. Lars Pape
 Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
The Banff 2015 Kidney Meeting Report: Current Challenges in Rejection Classification and Prospects for Adopting Molecular Pathology
 The Banff 2015 Kidney Meeting Report: Current Challenges in Rejection Classification and Prospects for Adopting Molecular Pathology The Harvard community has made this article openly available. Please
The Banff 2015 Kidney Meeting Report: Current Challenges in Rejection Classification and Prospects for Adopting Molecular Pathology The Harvard community has made this article openly available. Please
The Banff Conferences on renal allograft pathology the latest 2013 report
 615245PSH0010.1177/2010105815615245Proceedings of Singapore HealthcareLoh research-article2015 Review Article PROCEEDINGS OF SINGAPORE HEALTHCARE The Banff Conferences on renal allograft pathology the
615245PSH0010.1177/2010105815615245Proceedings of Singapore HealthcareLoh research-article2015 Review Article PROCEEDINGS OF SINGAPORE HEALTHCARE The Banff Conferences on renal allograft pathology the
ACCME/Disclosure. Case #1. Case History. Dr. Bracamonte has nothing to disclose
 Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
The Histology of Kidney Transplant Failure: A Long-Term Follow-Up Study
 CLINICAL AND TRANSLATIONAL RESEARCH The Histology of Kidney Transplant Failure: A Long-Term Follow-Up Study Maarten Naesens, 1,2,6 Dirk R.J. Kuypers, 1,2 Katrien De Vusser, 1,2 Pieter Evenepoel, 1,2 Kathleen
CLINICAL AND TRANSLATIONAL RESEARCH The Histology of Kidney Transplant Failure: A Long-Term Follow-Up Study Maarten Naesens, 1,2,6 Dirk R.J. Kuypers, 1,2 Katrien De Vusser, 1,2 Pieter Evenepoel, 1,2 Kathleen
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials
 The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
IMMUNOBIOLOGY OF TRANSPLANTATION. Wasim Dar
 IMMUNOBIOLOGY OF TRANSPLANTATION Wasim Dar Immunobiology of Transplantation Overview Transplantation: A complex immunologic process Contributions Innate Immunity Adaptive immunity T Cells B Cells HLA Consequences
IMMUNOBIOLOGY OF TRANSPLANTATION Wasim Dar Immunobiology of Transplantation Overview Transplantation: A complex immunologic process Contributions Innate Immunity Adaptive immunity T Cells B Cells HLA Consequences
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Impact of Subclinical Rejection on Transplantation
 Trends in Transplantation 2007;1:56-60 Impact of Subclinical Rejection on Transplantation David N. Rush for the Winnipeg Transplant Group Transplant Manitoba Adult Kidney Program, University of Manitoba,
Trends in Transplantation 2007;1:56-60 Impact of Subclinical Rejection on Transplantation David N. Rush for the Winnipeg Transplant Group Transplant Manitoba Adult Kidney Program, University of Manitoba,
Histopathology: Vascular pathology
 Histopathology: Vascular pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about these
Histopathology: Vascular pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about these
The Natural History of Chronic Allograft Nephropathy
 The new england journal of medicine original article The Natural History of Chronic Allograft Nephropathy Brian J. Nankivell, M.D., Ph.D., Richard J. Borrows, M.B., B.Chir., Caroline L.-S. Fung, M.B.,
The new england journal of medicine original article The Natural History of Chronic Allograft Nephropathy Brian J. Nankivell, M.D., Ph.D., Richard J. Borrows, M.B., B.Chir., Caroline L.-S. Fung, M.B.,
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant
 James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Deján Dobi, MD. PhD Thesis
 Clinicopathologic Relevance of Vascular Changes Associated with Transplant Glomerulopathy Secondary to Chronic Antibody-mediated Rejection in the Renal Allograft Deján Dobi, MD PhD Thesis Szeged, 2018
Clinicopathologic Relevance of Vascular Changes Associated with Transplant Glomerulopathy Secondary to Chronic Antibody-mediated Rejection in the Renal Allograft Deján Dobi, MD PhD Thesis Szeged, 2018
Light and electron microscopical studies of focal glomerular sclerosis
 J. clin. Path., 1971, 24, 846-850 Light and electron microscopical studies of focal glomerular sclerosis A. H. NAGI, F. ALEXANDER, AND R. LANNIGAN From the Department of Pathology, Queen's University of
J. clin. Path., 1971, 24, 846-850 Light and electron microscopical studies of focal glomerular sclerosis A. H. NAGI, F. ALEXANDER, AND R. LANNIGAN From the Department of Pathology, Queen's University of
The Value of Electron Microscopy in the Diagnosis of Chronic Renal Allograft Rejection
 The Value of Electron Microscopy in the Diagnosis of Chronic Renal Allograft Rejection B. Ivanyi, M.D., E. Kemeny, M.D., E. Szederkenyi, M.D., F. Marofka, M.D., P. Szenohradszky, M.D. Departments of Pathology
The Value of Electron Microscopy in the Diagnosis of Chronic Renal Allograft Rejection B. Ivanyi, M.D., E. Kemeny, M.D., E. Szederkenyi, M.D., F. Marofka, M.D., P. Szenohradszky, M.D. Departments of Pathology
Special thanks to our clinical collaborators Special thanks to our patients. Administration. Andre Baretto
 Antibody-mediated rejection: a prototype for antibody-mediated diseases Phil Halloran Alberta Transplant Applied Genomics Centre Edmonton, Canada Disclosures PFH has shares in TSI a university spinoff
Antibody-mediated rejection: a prototype for antibody-mediated diseases Phil Halloran Alberta Transplant Applied Genomics Centre Edmonton, Canada Disclosures PFH has shares in TSI a university spinoff
NEPHRITIC SYNDROME. By Dr Mai inbiek
 NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
Peritubular capillaries C4d deposits in renal allograft biopsies and anti HLA I/II alloantibodies screening Incidence and clinical importance
 ORIGINAL ARTICLE Port J Nephrol Hypert 2008; 22(1): 37-42 Peritubular capillaries C4d deposits in renal allograft biopsies and anti HLA I/II alloantibodies screening Incidence and clinical importance Helena
ORIGINAL ARTICLE Port J Nephrol Hypert 2008; 22(1): 37-42 Peritubular capillaries C4d deposits in renal allograft biopsies and anti HLA I/II alloantibodies screening Incidence and clinical importance Helena
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Update on Transplant Glomerulopathy
 Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Journal of Nephropathology
 www.nephropathol.com DOI: 10.15171/jnp.2018.24 J Nephropathol. 2018;7(3):101-105 Journal of Nephropathology Relationship of CD147 kidney expression with various pathologic lesions, biochemical and demographic
www.nephropathol.com DOI: 10.15171/jnp.2018.24 J Nephropathol. 2018;7(3):101-105 Journal of Nephropathology Relationship of CD147 kidney expression with various pathologic lesions, biochemical and demographic
Renal manifestations of IgG4-related systemic disease
 Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER
: 30 YEARS LATER") HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting Antibody-Mediated Rejection
 Clinical and Developmental Immunology Volume 2013, Article ID 460316, 6 pages http://dx.doi.org/10.1155/2013/460316 Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting
Clinical and Developmental Immunology Volume 2013, Article ID 460316, 6 pages http://dx.doi.org/10.1155/2013/460316 Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting
Ανάπτυξη Βιοτράπεζας για την Ανίχνευση Πρώιμων Βιοδεικτών σε Ασθενείς με Χρόνια Νεφρική Νόσο
 Ανάπτυξη Βιοτράπεζας για την Ανίχνευση Πρώιμων Βιοδεικτών σε Ασθενείς με Χρόνια Νεφρική Νόσο ΔΗΜΗΤΡΙΟΣ Σ. ΓΟΥΜΕΝΟΣ Νεφρολογικό και Μεταμοσχευτικό Κέντρο Πανεπιστημιακό Νοσοκομείο Πατρών Causes of chronic
Ανάπτυξη Βιοτράπεζας για την Ανίχνευση Πρώιμων Βιοδεικτών σε Ασθενείς με Χρόνια Νεφρική Νόσο ΔΗΜΗΤΡΙΟΣ Σ. ΓΟΥΜΕΝΟΣ Νεφρολογικό και Μεταμοσχευτικό Κέντρο Πανεπιστημιακό Νοσοκομείο Πατρών Causes of chronic
Pharmaceutical pathology
 Pharmaceutical pathology Livia Vida 2018 1. Necrosis, types, examples. Apoptosis. 2. Adaptations I. Degeneration, atrophy. 3. Adaptations II. Hypertrophy, hyperplasia. 4. Pigments. Calcification. 5. Inflammation
Pharmaceutical pathology Livia Vida 2018 1. Necrosis, types, examples. Apoptosis. 2. Adaptations I. Degeneration, atrophy. 3. Adaptations II. Hypertrophy, hyperplasia. 4. Pigments. Calcification. 5. Inflammation
SCORING OF i-ifta: POTENTIAL RULES & ROLE IN CHRONIC TCMR
 SCORING OF i-ifta: POTENTIAL RULES & ROLE IN CHRONIC TCMR Parmjeet Randhawa, MD Professor of Pathology The Thomas E Starzl Transplantation Institute University of Pittsburgh . I HAVE NO CONFLICTS OR FINANCIAL
SCORING OF i-ifta: POTENTIAL RULES & ROLE IN CHRONIC TCMR Parmjeet Randhawa, MD Professor of Pathology The Thomas E Starzl Transplantation Institute University of Pittsburgh . I HAVE NO CONFLICTS OR FINANCIAL
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
No evidence of C4d association with AMR However, C3d and AMR correlated well
 C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
Endothelitis in cardiac allograft biopsy specimens: Possible relationship to antibody-mediated rejection
 http://www.jhltonline.org ORIGINAL CLINICAL SCIENCE Endothelitis in cardiac allograft biopsy specimens: Possible relationship to antibody-mediated rejection Fabio Tavora, MD, a Raghava Munivenkatappa,
http://www.jhltonline.org ORIGINAL CLINICAL SCIENCE Endothelitis in cardiac allograft biopsy specimens: Possible relationship to antibody-mediated rejection Fabio Tavora, MD, a Raghava Munivenkatappa,