HYPERTENSION. Dr. Ahmed A. Elberry, MBBCH, MSc, MD Assistant Professor of Clinical Pharmacy Faculty of pharmacy, KAU. Hypertension
|
|
|
- Darrell Williams
- 5 years ago
- Views:
Transcription

1 HYPERTENSION Dr. Ahmed A. Elberry, MBBCH, MSc, MD Assistant Professor of Clinical Pharmacy Faculty of pharmacy, KAU 1 Hypertension It is a sustained of arterial bl. pr. 140/90 Causes: ry: Essential or Idiopathic : 90-95% of cases 2ry: about 5% of cases Disease: Renal or renovascular disease Coarctation of the aorta Endocrine disease: eg: Phaeochomocytoma Cushing syndrome Acromegaly Drugs (Iatrogenic) 2 1

2 Drug-Induced HT: 1- Hormones: 3- CNS: Steroids Anxiolytic: Buspirone Estrogens & OC Anesthetic: Ketamine Desflurane Erythropoietin 2- Autonomic: Phenylpropanolamines Clonidine withdrawal Ergotamine Sibutramine Antiparkinsonian: Bromocryptine Antiepileptic: Carbamazepine Antiemetic: Metoclopramide Antidepressants: Venlafaxine 4- Antiinflammatory: NSAIDs Methylphenidate 5- Immunosuppressive: cyclosporine/tacrolimus Risk factors for 1ry HT Controllable Risk Factors Uncontrollable Risk Factors 1- Salt intake 2- Alcohol 3- Stress 4- Weight (Obesity) 1- Heredity 2- Age 5- exercise 3- Race :More in - Men: Women: after menopause African Americans 2


3 JNC 7 Classification of BP: The 7th report of the Joint National Committee on Detection, Evaluation & Treatment of High Bl Pr (JNC 7) classifies adult BP as shown Classification rmal Prehypertension Stage 1 hypertension Stage 2 hypertension Systolic BP Diastolic BP. (mmhg) < (mmhg) < NB.: If systolic & diastolic lie in different stages, the highest is considered Diastolic bl.pr. is generally more reliable, while, systolic is more important in elderly 5 Manifestations Usually NO SYMPTOMS! The Silent Killer May have: Headache Blurry vision Chest Pain Frequent urination at night 6 3

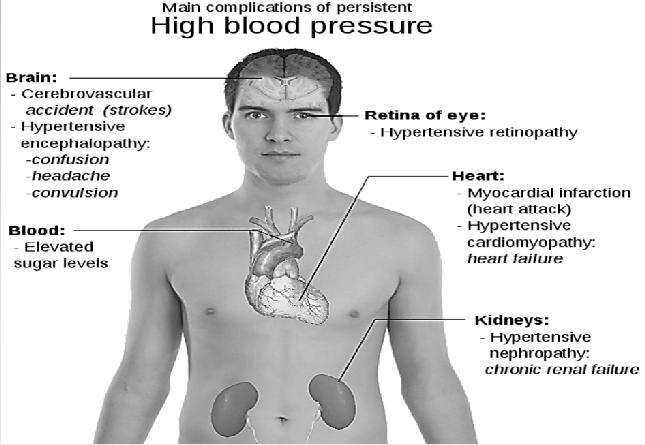
4 Complications of HT 7 Treatment of HT npharmacological Pharmacological 8 4

5 n pharmacological therapy Include: Approximate SBP Reduction 1- Adopt DASH eating plan 8-14 mmhg 2- Dietary sodium 2-8 mmhg 3- Alcohol consumption 2-4 mmhg 4- Weight 5-20 mmhg/ 10 kg weight loss 5- Physical activity 4-9 mmhg Indication: patients with prehypertension. Patients diagnosed with stage 1 or 2 hypertension should be placed on lifestyle modifications & drug therapy concurrently. 9 DASH Eating Plan 1. saturated fat, cholesterol & total fat 2. red meat 3. sweets & sugar containing beverages 4. fruits, vegetables & fiber 5. low fat diary products & plant protein 6. magnesium, potassium & calcium DASH Can reduce BP in 2 weeks (SBP, 8-14 mmhg) 5
6 Pharmacological treatment 1st line 1ry options: (ABCD) Diuretics, ACE inhibitors (or ARBs)*, CCBs & β-blockers** Alternatives: Sympatholytics: central α2-agonists, α1-blockers, peripheral adrenergic neurone antagonists (guanithidine, reserpine, α-methyldopa) direct renin inhibitors (Aliskiren) Direct arterial vasodilators: (hydralazine, minoxidil, diazoxide) *ACE inhibitors (or ARBs) are contraindicated in pregnancy **BBs are not indicated as first line therapy for elderly (age 60 and above) 11 The A B C D classes (1st line) D A Diuretics ACEI, ARB Ca channelblockers DIURETICS βblockers ACEI and ARB D A Fourth Choice, Useful First Good and third Best Choice Choice Second Best Choice B C Can be combined combined with D, AC Can be be combined with A, D Can Can be combined with with D, B,A, CB, B C β-blockers Ca-Blockers 12 6

7 GOAL OF THERAPY -PLUSHypertension With Framingham risk factor 10% 1-Framingham risk factor 10% 2- DM 3- Renal Disease 4- CAD < 140/90 mmhg < 130/80 mmhg -PLUSHF < 120/80 mmhg Stage 1: monotherapy Stage 2: combination therapy

8 Algorithm for Treatment of HT Lifestyle Modifications t at Goal Blood Initial Drug Choices Without Compelling Indications Stage 1 HTN Thiazide diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. With Compelling Indications Stage 2 HTN 2-drug combination for most (usually thiazide diuretic and ACEI, or ARB, or BB, or CCB) Drug(s) for the compelling indications t at Goal Blood Pressure Optimize dosages or add additional drugs Compelling Indications Compelling Indication Initial Therapy Options Sequential therapy Diabetes ACEI (or ARB) THIAZ, BB, CCB Chronic kidney disease (CKD) ACEI (or ARB) CAD BB + ACEI (or ARB) Recurrent stroke prevention ACEI (or ARB) + THIAZ HF BB + THIAZ + ACEI (or ARB) - THIAZ for BP control - CCB fro ischemia control - Aldosterone antagonist for severe HF - Hydralazine or nitrates for black patients 8
 : Spironolactone & Eplerenone 1. 2.")
9 Diuretics 1. Thiazides: As hydrochlorthiazide (HCTZ) or chlorthalidone 2. Loop Diuretics: Furosemide (lasix) twice daily Torsemide once daily 3. Potassium-Sparing Diuretics: n-aldosterone antagonists: Triamterene & Amiloride. Aldosterone antagonists (more potent) : Spironolactone & Eplerenone Thiazide Diuretics Indication: of choice for treating HT (it has both diuretic & direct VD effect) all are equally effective. Dosage: Starting dose of HCTZ (Esidrex) or chlorthalidone of 12.5 mg once daily. Maintenance dose of 25 mg once daily effectively lower BP with low incidence of SE. SE: Hpokalemia, Hyponatremia, Hypomagnesemia, Hypochloremic alkolosis Hyper uricemia, Hyper glycemia, Hyper lipidemia, Hyper sensitivity Hypercalcemia Ca


10 2- Loop diuretics Indication: of choice for: severe CKD (GFR<30 ml/min./1.73 m2) Lt ventricular dysfunction, or severe edema (because potent diuresis is often needed in these patients). SE: Hpokalemia, Hyponatremia, Hypomagnesemia, Hypochloremic alkolosis Hyper uricemia, Hyper glycemia, Hyper lipidemia, Hyper sensitivity Hypocalcemia, Deafness, Dehydration Ca++ NB.: Loop diuretics have less effect on serum lipids & glucose 19 Hypokalemia K+ Manifestation: Muscle fatigue or cramps. Serious cardiac arrhythmias may occur, esp. in patients: receiving digitalis, with LV hypertrophy, with IHD. Monitoring: Serum K+ should be measured at baseline & within 4 w of initiating therapy or after increasing diuretic doses. Management: Intermittent use of the least effective dose K+ rich food (bananas, potatoes, avocados) KCl supplement (20 40 meq/day) Add K+ sparing diuretic 20 10


11 3- K+-Sparing Diuretics Indication: Patients who develop hypokalemia while on a thiazide diuretic. SE: Hyperkalemia, especially in: chronic kidney disease DM, concurrent treatment with an ACE.I, ARB, NSAID, or K+ supplement. Gynecomastia with Spironolactone (in up to 10% of patients), but this effect occurs rarely with eplerenone. 21 ACEIs 11
![ACEIs 1. S.H containing: Captopril (capoten): [Active drug, given 2-3 times daily, absorption is affected by food] 2.](/docs-images/95/122739650/images/12-2.jpg "n-s.h containing: Active drug Lisinopril (zestril) & Enalaprilate (given IV in emergency hypertension) Prodrugs")
 is the active metabolite of Enalapril ACE.")
12 ACEIs 1. S.H containing: Captopril (capoten): [Active drug, given 2-3 times daily, absorption is affected by food] 2. n-s.h containing: Active drug Lisinopril (zestril) & Enalaprilate (given IV in emergency hypertension) Prodrugs Enalapril (renitec) - Perindopril - Benazepril Ramipril Trandolapril - Fosinopril NB.: Enalaprilate (enalaprilic acid) is the active metabolite of Enalapril ACE.I is more effective in young white patients than in black or elderly 24 12
13 ACEIs Side effects: 1) Related to S.H: 1. Allergy 2. Taste (Dysgeusia) 3. Protinuria 4. Neutropenia 2) Related to ACE Cough due to bradykinin 1st dose Hypotension (esp. in elderly & heart failure). So tart with low dose with slow dose titration Hyperkalemia ARF esp. in bilateral renal art. stenosis 25 ACEIs Contraindications: Hypotension Pregnancy (They are fetopathic may cause oligohydramnios pulmonary hypoplasia growth retardation fetal death) Bilateral renal artery stenosis Drug interactions: Na+ depleting diuretics initial Hypotension K+ retaining diuretics hyperkalemia NSAID Hypotensive Effect Through Inhibition of Bradykinin & PGs Antacids absorption 26 13
 Long acting: Amlodipine (rvasc)")

14 AT-II Blockers (ARBs) Candesartan - Losartan (Cozar) - Olmesartan Valsartan Eprosartan -Irbesartan Telmisartan Actions & Uses As ACEI Side effects As ACEI but with less cough 27 CCB Classification: Dihydropyridine: Short acting: Nifedipine (Adalat, Epilat) Long acting: Amlodipine (rvasc) nisoldipine felodipine isradipine n-dihydropyridine: Verapamil (isoptin) Diltiazem (cardizem) Side effects: 1. Bl.V.: Headache flush Hypotension ankle oedema 2. Heart: Bradycardia with Diltiazem & marked with verapamil Reflex Tachycardia with nifedipine 3. G.I.T.: Constipation is marked with verapamil
 synthesis PGs Classification: 1. 2.")
 Sotalol Nadolol Timolol B.")
15 β-blockers Mechanism of antihypertensive effect: Block -1 of Heart COP. Block -1 of CNS Sympathetic outflow. Block -1 of Kidney Renin. Block Pre-synaptic Release of r-adr. Resetting the sensitivity of Baro-receptors. Prostacyclin (VD) synthesis PGs Classification: according to Selectivity according to Lipid solubility 29 Classification according to Selectivity ISA A. n- selective: Pindolol Oxprenolol Propranolol (Inderal) Sotalol Nadolol Timolol B. Cardio-selective (B1) Acebutolol Atenolol (Tenormin) Bisoprolol (Concor) Betaxolol Metoprolol (Lopressor) Esmolol L.A tes Extensive hepatic 1st pass metabolism Eye drop in glaucoma. Ultrashort. I.V. Infusion
 - Medraxalol Classification of according to Lipid solubility Lipophilic Hydrophilic 1. G.I.T.")
 Propranolol. Oxprenolol. Metoprolol. Timolol - Mainly Renal. Longer (12-24 Hs) Nadolol.")
16 NB.: Vasodilator B- Blockers: 1. 2-Partial agonist: Celiprolol: (Selective 1 Block ISA LA) 2. Nitrogenic effect ( production of NO): Nebivolol 3. 1-blocking effect: Labetalol Bucindolol Carvedilol (dilatrend) - Medraxalol Classification of according to Lipid solubility Lipophilic Hydrophilic 1. G.I.T. Absorption: 2. Passage across B.B.B.: - Well Absorbed. Pass BBB has CNS. effects. - Poorly absorbed. t pass BBB has little CNS effect 3. Metabolism: 4. Duration of Action: 5. Examples: - Extensive hepatic. Short (4-6 Hours) Propranolol. Oxprenolol. Metoprolol. Timolol - Mainly Renal. Longer (12-24 Hs) Nadolol. Atenolol. Sotalol. Bisoprolol 32 16

 ] Hyperkalemia Atherosclerosis ( HDL & Triglycerides) Sudden withdrawal")
 Hypoglycemia in insulin or oral hypoglycemic treatment.")
17 SE & contraindications Side effects Contraindications - Sedation - depression - sleep disturbances (only in lipophilic B.B. crossing BBB) I. CNS: II. CVS: 1.Heart: 1.Heart failure - Heart block - Bradycardia B.V. 2.Cold extremities, Raynaud's phenomenon, numbness, tingling 3.B.P. 3.Hypotension III. Respiration IV. Metabolism - Precipitate acute attack of B.A. in asthmatics V. Others Hypoglycemia (severe in patient receiving insulin or oral hypoglycemic [coma can occur without warning (silent death) ] Hyperkalemia Atherosclerosis ( HDL & Triglycerides) Sudden withdrawal withdrawal syndrome sympathetic over activity and precipitation of anginal attack even myocardial infarction Severe depression (use hydrophilic B.B.) H.F. - Hear block - severe bradycardia With Verapamil: H.F. & H. Block Variant angina. Raynaud's phenomenon & P.V.D & alone in pheochromocytoma Hypotension - Bronchial asthma (use selective B1) Hypoglycemia in insulin or oral hypoglycemic treatment. Never stop suddenly. 33 α1-receptor Blockers Prazosin (Minipress), terazosin, and doxazosin (Cardura) Side Effects: Initial Syncopal Attack (1st dose phenomenon). An αattack of severe postural hypotension. Start by small dose while patient is recumbent (At Bed Time), then increase the dose gradually Sexual dysfunction after long use in males & failure of ejaculation Salt & H2O retention as it C.O. R.B.F. So, Diuretic is added

 & Dry nasal mucosa 1.")
18 Central α2-agonists Include: Clonidine, guanabenz, guanfacine, & methyldopa Mechanism: Selective α2 & Imidazoline I1 Agonist (15 : 1) Hypotension by: 1. Sympathetic outflow from C.N.S. 2. Presynaptic Release of N.A. 3. Kidney: Release of Renin Side effects of centrally acting drugs Sudden Withdrawal Rebound severe hypertension Treat by Re-using Clonidine or by -Blocker + -Blocker. 2. Sedation 3. Dry mouth (xerostomia) & Dry nasal mucosa Moxonidine (physiotens) & Rilmenidine (Hyperium): They are selective I1 agonist used in ttt of hypertension Less liable to cause sedation 36 18
 Mechanism: (Depletion) * Side effects: 1) Parasymp. Predominance: 1.")
19 Peripheral adrenergic neurone depressants Include Guanethidine Reserpine Methyldopa (act centrally also) 37 Guanethidine Reserpine *Kinetic - Incompletely absorbed - t pass B.B.B - Slowly excreted in urine *Kinetic: - Well absorbed - Passes B.B.B - Slowly excreted in urine Mechanism ( Release) Mechanism: (Depletion) * Side effects: 1) Parasymp. Predominance: 1. Nasal congestion 2. Bradycardia 3. Postural hypotension 4. Diarrhea * Side effects: 1) Parasymp. Predominance: 1.Nasal congestion {Stuffiness} 2.Bradycardia 3.Hypotension 4.Diarrhea 2) Others: 2) Others: 1. Na & H2O retention 1. Parotid pain 2.Weight gain 2. Failure of ejaculation 3.Peptic ulcer 4.Endocrinal disturbance 5.Breast cancer. 6.Impotence 3) C.N.S: 1. Psychic depression 2. Nightmares 3. Parkinsonism -Methyldopa *Kinetic - Well absorbed - Passes B.B.B - Transformed to -methyl NA Mechanism ( synthesis & Central) * Side effects: 1) Parasymp. Predominance: 1.Nasal congestion 2.Bradycardia 3.Hypotension 4.Diarrhea 2) Other: 1.Na & H20 retention weight gain 2.Liver toxicity 3.Bone marrow Depression 3) C.N.S: 1. Psychic depression 2. Night mares 3. Parkinsonism 4. Sedation 38 19

20 Direct renin inhibitors (Aliskirin (Tecturna )) Inhibit directly the renin Similar to ACEIs & ARBs & contraindicated in pregnancy Used once orally as an alternative antihypertensive agent Direct Arterial Vasodilators Include: Hydralazine - Minoxidil - Diazoxide Actions & effects : Direct Arterio-dilator Bl.Pr useful in Hypertension Bl.Pr symp & after load Co useful in H.F Disadvantages & general SE: 1. Bl.Pr sympathetic leading to: Tachycardia & Angina [Add - blockers] Rennin edema [Add diuretic] (So, they are not used alone, but used in combination with - blockers & diuretics) 2. V.D Headache congestion flush 40 20




.")

21 (1)Hydralazine (2) Minoxidil (3) Diazoxide Side effects 1. Hypersensitivity in the form of:. Hypertrichosis - Rash - Rheumatoid arthritis - Systemic lupus erythematosus like syndrome 2. GIT upset 3. Peripheral neuritis 1. Hyperglycemia 2. Hyperuricemia (as it is related to Thiazide diuretic) Uses Orally& I.V 1. Hypertension & emergency 2. H.F Orally 1. Hypertension 2. H.F 3. Locally in alopecia I.V Emergency Hypertension 41 SPECIAL POPULATIONS Pregnancy: African Americans: Methyldopa is the drug of choice Alternatives: ΒB & CCBs. ACEI & ARBs are contraindicated (teratogens). Thiazides & CCBs are particularly effective. Response is significantly when either class is combined with a BB, ACEI, or ARB. Older People: Diuretics & ACEI can be used safely, but in smallerthan-usual initial doses, and titrations should occur over a longer period to minimize the risk of hypotension. Centrally acting agents & BB should be avoided or used with caution because they are associated with dizziness & postural hypotension. 21
22 HYPERTENSIVE CRISIS This image cannot currently be display ed. 180/110 & may be classified into: Hypertensive urgency: without target organ damage (TOD) (eg. Encephalopathy, unstable angina, renal failure & papilledema) ttt: adjusting maintenance therapy by adding a new antihypertensive and/or increasing the dose of a present drug. Hypertensive emergency: with TOD ttt: require immediate BP reduction to limit new or progressing target-organ damage. 43 Goal in treatment of hypertensive crisis The goal: not to lower BP to normal; as rapid drops in BP may cause end- organ ischemia or infarction. The initial target is MAP 25% within minutes to hours. If BP is then stable, it can be reduced to 160/ mm Hg within the next 2-6 hours. Additional gradual decrease toward the goal BP after hours


23 Treatment of hypertensive crises Hypertensive urgency: Acute administration of short-acting oral drugs (captopril or labetalol) followed by careful observation for several hours to ensure gradual BP reduction. Captopril mg may be given at 1- to 2-hour intervals. The onset of action is min. Labetalol mg, followed by additional doses every 2-3 h. Hypertensive emergency: Nitroprusside is the drug of choice in most cases. Given as a IV infusion (0.25 to 10 mcg/kg/min.) Onset of action is immediate & disappears within 1-2 min of discontinuation. When infusion is continued 72 h., serum thiocyanate levels should be measured, & infusion should be stopped if the level 12 mg/dl. Other Parentral drugs used in emergency HT Nitroprusside Nitroglycerin Nicardipine Diazoxide Esmolol Enalaprilate Fenoldopam Hydralazine Labetalol 46 23
24 Causes of Resistant HT 1. Improper BP measurement 2. Identifiable causes of HTN 3. Excess sodium intake 4. Excess alcohol intake 5. Inadequate diuretic or medication therapy 6. Drug actions and interactions: NSAIDs, sympathomimetics, oral contraceptives, OTC drugs & herbal supplements 24
25 25
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
8/20/2018. Objectives. What is hypertension? cont. What is hypertension? Epidemiology cont. Epidemiology
 Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
New classification of HT Systolic Diastolic Normal <120 <80 Prehypertension Stage1HT Stage 2 HT >160 or >100
 Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Introduction. Factors affecting blood pressure: 1-COP = HR X SV mainly affect SBP. 2-TPR = diameter of arterioles X viscosity of blood affect DBP
 Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Antihypertensive Agents
 Antihypertensive Agents Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Süzer Farmakoloji 3. Baskı 2005
Antihypertensive Agents Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Süzer Farmakoloji 3. Baskı 2005
Antihypertensive Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014
 Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Antihypertensive Drugs What is Hypertension: A common, incurable, persistent, but usually
Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Antihypertensive Drugs What is Hypertension: A common, incurable, persistent, but usually
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Prof dr Aleksandar Raskovic DIRECT VASODILATORS
 Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
ANTIHYPERTENSIVES. Assoc. Prof. Bilgen Başgut
 ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Antihypertensive Drugs. Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017
 Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017 Antihypertensive Drugs What is Hypertension? A common, incurable, persistent, but usually
Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017 Antihypertensive Drugs What is Hypertension? A common, incurable, persistent, but usually
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC
 DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
LESSON ASSIGNMENT. After completing this lesson you will be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Antihypertensive Drugs. Nafrialdi
 Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension is also an important risk factor in the development of chronic kidney disease and heart failure.
 Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Hypertension (HTN) Lecture Note
 Lecture Note") Hypertension (HTN) Lecture Note October, 2009 Chuang-Ye Hong, MD, PhD, FACP Wan-Fang Hospital Taipei Medical University Outline Definition Epidemiology Measurement of BP Secondary cause Target organ damage
Hypertension (HTN) Lecture Note October, 2009 Chuang-Ye Hong, MD, PhD, FACP Wan-Fang Hospital Taipei Medical University Outline Definition Epidemiology Measurement of BP Secondary cause Target organ damage
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI
 DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
ANTIHYPERTENSIVE DRUGS
 ANTIHYPERTENSIVE DRUGS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: September 28, 2010 Materials on: Exam #3 Required reading: Katzung, Chapter 11 1 1 in 3 adults HYPERTENSION 64% of
ANTIHYPERTENSIVE DRUGS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: September 28, 2010 Materials on: Exam #3 Required reading: Katzung, Chapter 11 1 1 in 3 adults HYPERTENSION 64% of
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS ALISKIREN 150MG TABLET RASILAZ RENIN INHIBITOR
 S/N ME OF MEDICATIONS BRANDED/GENERIC DRUG CLASS * UNIT PRICE RANGE (SGD$) 1 ACEBUTOLOL HCL 100MG CAPSULE SECTRAL BETA BLOCKERS 0.50 2 ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS 0.33 3 ALISKIREN
S/N ME OF MEDICATIONS BRANDED/GENERIC DRUG CLASS * UNIT PRICE RANGE (SGD$) 1 ACEBUTOLOL HCL 100MG CAPSULE SECTRAL BETA BLOCKERS 0.50 2 ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS 0.33 3 ALISKIREN
8/19/2016. No Conflicts. I struggled with everything cardiac in nursing school.
 Cindy Weston, DNP, RN, CCRN, CNS CC, FNP BC Assistant Professor, Texas A&M Health Science Center College of Nursing Describe and define epidemiology and pathophysiology of hypertension Differentiate JNC8
Cindy Weston, DNP, RN, CCRN, CNS CC, FNP BC Assistant Professor, Texas A&M Health Science Center College of Nursing Describe and define epidemiology and pathophysiology of hypertension Differentiate JNC8
Cardiovascular Risk Reduction in Diabetic Mellitus. Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist
 Physician / Cardiologist") Cardiovascular Risk Reduction in Diabetic Mellitus Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist Cardiovascular Risk Reduction in Diabetic Mellitus Disclosures
Cardiovascular Risk Reduction in Diabetic Mellitus Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist Cardiovascular Risk Reduction in Diabetic Mellitus Disclosures
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Prof. Ramzy H. El Mawardy. Cairo Egypt 2009
 Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety
 New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Andrew Straw, PharmD, BC-ADM
New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Andrew Straw, PharmD, BC-ADM
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Network Hypertension Algorithm
 Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
ANTIHYPERTENSIVE AGENTS AND VASODILATORS. Lecture 5
 ANTIHYPERTENSIVE AGENTS AND VASODILATORS Lecture 5 Hypertension Blood pressure BP = CO x PVR n Interaction between autonomic nervous system, cardiovascular system and renal system Normal: 110/70 Prehypertension
ANTIHYPERTENSIVE AGENTS AND VASODILATORS Lecture 5 Hypertension Blood pressure BP = CO x PVR n Interaction between autonomic nervous system, cardiovascular system and renal system Normal: 110/70 Prehypertension
Top 200 Section 4. Cardiovascular Drugs
 Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Blood pressure (BP) control. Hypertension
 control. Hypertension") Blood pressure (BP) control Normal heart function Blood pressure (BP) control blood pressure (BP) cardiac output (CO) = total peripheral resistance (TPR) heart rate (HR) filling pressure arteriolar volume
Blood pressure (BP) control Normal heart function Blood pressure (BP) control blood pressure (BP) cardiac output (CO) = total peripheral resistance (TPR) heart rate (HR) filling pressure arteriolar volume
INDIAN HYPERTENSION GUIDELINES-II
 HYPERTENSION IN SPECIAL SITUATIONS Hypertension with diabetes mellitus Co-existence of hypertension and diabetes is being increasingly recognised. 30-35% of hypertensives are detected to have diabetes.
HYPERTENSION IN SPECIAL SITUATIONS Hypertension with diabetes mellitus Co-existence of hypertension and diabetes is being increasingly recognised. 30-35% of hypertensives are detected to have diabetes.
ASEBP and ARTA TARP Drugs and Reference Price by Categories
 ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Physician/Clinic Collaborative Practice Agreement
 Physician/Clinic Collaborative Practice Agreement Effective October 1, 2010, Connecticut Senate Bill 428 (PA 10-117) extends to all settings and medical conditions the opportunity for licensed pharmacists
Physician/Clinic Collaborative Practice Agreement Effective October 1, 2010, Connecticut Senate Bill 428 (PA 10-117) extends to all settings and medical conditions the opportunity for licensed pharmacists
Chapter 10 Worksheet Blood Pressure and Antithrombotic Agents
 Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Antihypertensive Agents
 1. Blood Pressure Regulation Antihypertensive Agents - 2007 Edward JN Ishac. Ph.D. Associate Professor, Dept. Pharmacology & Toxicology Office: Smith 742; Tel: 828 2127 eishac@hsc.vcu.edu Frank's formula,
1. Blood Pressure Regulation Antihypertensive Agents - 2007 Edward JN Ishac. Ph.D. Associate Professor, Dept. Pharmacology & Toxicology Office: Smith 742; Tel: 828 2127 eishac@hsc.vcu.edu Frank's formula,
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Cardiac Medications At A Glance
 Cardiac Medications At A Glance 1) Anticoagulants (Also known as Blood Thinners.) Dalteparin (Fragmin), Danaparoid (Orgaran) Enoxaparin (Lovenox) Heparin (various) Tinzaparin (Innohep) Warfarin (Coumadin)
Cardiac Medications At A Glance 1) Anticoagulants (Also known as Blood Thinners.) Dalteparin (Fragmin), Danaparoid (Orgaran) Enoxaparin (Lovenox) Heparin (various) Tinzaparin (Innohep) Warfarin (Coumadin)
Angina pectoris due to coronary atherosclerosis : Atenolol is indicated for the long term management of patients with angina pectoris.
 Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Pharmacology of the Sympathetic Nervous System II
 Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Hypertension. Kaveh Eslami Pharm.D, board certified clinical pharmacy resident Clinical pharmacy department Tehran university of medical science
 Hypertension Kaveh Eslami Pharm.D, board certified clinical pharmacy resident Clinical pharmacy department Tehran university of medical science 2 EPIDEMIOLOGY Approximately 31% of the population (72 million
Hypertension Kaveh Eslami Pharm.D, board certified clinical pharmacy resident Clinical pharmacy department Tehran university of medical science 2 EPIDEMIOLOGY Approximately 31% of the population (72 million
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN
 Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN Objectives Identify Normal Systolic and Diastolic Blood pressures Recognize common Antihypertensive
Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN Objectives Identify Normal Systolic and Diastolic Blood pressures Recognize common Antihypertensive
HYPERTENSION. Background for understanding the Hypertension literature. Case presentation. Approach to Treatment. Jeffrey J. Kaufhold, MD Nephrology
 HYPERTENSION Background for understanding the Hypertension literature. Case presentation Approach to Treatment Jeffrey J. Kaufhold, MD Nephrology 2009 HYPERTENSION SUMMARY Background for understanding
HYPERTENSION Background for understanding the Hypertension literature. Case presentation Approach to Treatment Jeffrey J. Kaufhold, MD Nephrology 2009 HYPERTENSION SUMMARY Background for understanding
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University