Pulmonary hypertension
|
|
|
- Gerard Hunt
- 5 years ago
- Views:
Transcription
1 Pulmonary hypertension Rafael Hirsch, MD Adult Congenital Heart Unit Dept. of Cardiology, Beilinson Hospital-Rabin Medical Center and Sackler School of Medicine, Tel Aviv University
2 Pulmonary hypertension? A bad term that should be abandoned Systemic arterial hypertension = increased small vessel resistance Increased cardiac output or systemic venous pressure do not cause systemic arterial hypertension Pulmonary arterial hypertension can be the result of several pathophysiological processes: Increased flow, increased venous pressure, increased arteriolar (rarely venular) resistance and any combination of the above.
3 Pulmonary hypertension - definition Catheterization obtained mean pulmonary artery pressure >25 mmhg, normal or reduced cardiac output and pulmonary vascular resistance > 3 Woods (non indexed) Exercise induced mean PA pressure >30 mmhg very problematic definition Suggestion: mmhg borderline
4 Diagnosis and monitoring Systemic arterial hypertension easy Often incidental finding on routine measurement Easy to follow up and adjust treatment Primary = common secondary = rare Pulmonary hypertension difficult, no direct access to arterial tree Pressure alone is not enough to assess response to treatment Primary = rare secondary = common
5 Updated Clinical Classification of Pulmonary Hypertension (Dana Point, 2008) 1. Pulmonary arterial hypertension (PAH) 1.1. Idiopathic PAH 1.2. Heritable BMPR ALK1, endoglin (with or without hereditary hemorrhagic telangiectasia) Unknown 1.3. Drug- and toxin-induced 1.4. Associated with Connective tissue diseases HIV infection Portal hypertension Congenital heart diseases Schistosomiasis Chronic hemolytic anemia 1.5 Persistent pulmonary hypertension of the newborn 1'. Pulmonary veno-occlusive disease (PVOD) and/or pulmonary capillary hemangiomatosis (PCH) 2. Pulmonary hypertension owing to left heart disease 2.1. Systolic dysfunction 2.2. Diastolic dysfunction 2.3. Valvular disease 3. Pulmonary hypertension owing to lung diseases and/or hypoxia 3.1. Chronic obstructive pulmonary disease 3.2. Interstitial lung disease 3.3. Other pulmonary diseases with mixed restrictive and obstructive pattern 3.4. Sleep-disordered breathing 3.5. Alveolar hypoventilation disorders 3.6. Chronic exposure to high altitude 3.7. Developmental abnormalities 4. Chronic thromboembolic pulmonary hypertension (CTEPH) 5. Pulmonary hypertension with unclear multifactorial mechanisms 5.1. Hematologic disorders: myeloproliferative disorders, splenectomy 5.2. Systemic disorders: sarcoidosis, pulmonary Langerhans cell histiocytosis: lymphangioleiomyomatosis, neurofibromatosis, vasculitis 5.3. Metabolic disorders: glycogen storage disease, Gaucher disease, thyroid disorders 5.4. Others: tumoral obstruction, fibrosing mediastinitis, chronic renal failure on dialysis

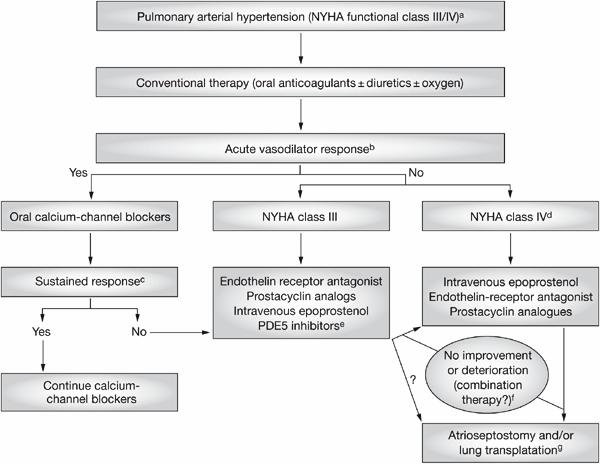
6 יתר ל חץ דם ראתי דרגה IV
7 Idiopathic pulmonary hypertension Not primary Incidence 2-5/1,000,000 Females>males Median age at diagnosis 37 years Familial in 6-10% BMPR2 (TGF-beta) Autosomal dominant variable penetrance Two hit hypothesis Genetic anticipation children more sick than parents Rare veno-occlusive disease and pulmonary capillary hemangiomatosis
8 Prognosis natural history Median survival 2.8 years from diagnosis 1 year 68%, 3 years 48%, 5 years - 34% The heart is the most affected organ. Prognosis worse when RA pressure, cardiac index, pericardial effusion BNP, NT-pro-BNP levels FC by 6 minutes walking distance < 380 meters
9 Diseases and conditions with PH Scleroderma very severe, poor prognosis, histology not inflammatory Inflammatory diseases SLE, mixed Liver disease 4-15% candidates liver transplantation. CI-PA pressure >35 mmhg HIV 1/200 Drugs amphetamine derivatives e.g fenfluramine other anorexigens
10 CHD patients with PHT Elevated venous pressure MS, supra mitral membrane and cor triatriatum: rare and treatable surgically will not be further discussed Malformations with initial left to right shunt and almost inevitable shunt reversal with Eisenmenger syndrome: VSD, PDA, complex CHD with unrestricted pulmonary flow, large surgical central shunts Malformations with left to right shunt and occasional development of Eisenmenger syndrome: ASD Progressive pulmonary hypertension in repaired shunt lesions.
11 Bedside diagnosis of pulmonary hypertension History murmur and/or heart failure in childhood, previous operation of lt. rt. shunt lesion, previous palliation with central shunt Symptoms - cyanosis on exertion, syncope, declining exercise capacity, angina pectoris, palpitations
12 Bedside diagnosis (cntd.) Physical examination pulse oximetry arms and legs!!, clubbing, sustained RV heave, loud (single) P2 (dd CTGA), absence of stenotic murmur, absence of continuous murmur, diastolic Graham Steell murmur ECG - Right forces Chest x-ray: plethora vs. pruning and peripheral oligemia, heart shadow suggestive of CHD, situs anomaly etc.
13 Echocardiography TTE+TEE Establish the existence of pulmonary hypertension and assess severity Etiology r/o left heart disease incl. myocardial dysf. systolic/diastolic mitral stenosis incl. supra-valve membrane and cor triatriatum, pulm. vein stenoses etc., shunt lesions ASD VSD PDA AVSD and complex CHD
14 Echocardiography (cntd) Evaluate impact of PHT on heart structure and function RV size and function, RVH, tricuspid regurgitation, diastolic interaction with LV, systemic venous hypertension distention of veins, bulging of interatrial septum, rt. lt. shunting PFO or septostomy, thrombosis in situ in pulmonary tree Follow up serial studies, assess effect of treatment, record complications and deterioration
15 Echocardiography - pitfalls In early PPH normal (no TR trace) look for PI, acceleration, septum etc. False positive in pulmonary stenosis, in VSD when cursor cuts TR and VSD jets. Pulmonary systolic pressure may be increased in some hyperdynamic conditions with mean pressure still in normal range. (35-55 mmhg TR gradient) Missing shunt lesions sinus venosus defects, anomalous veins, AP-window, PDA (shunt jet is of low velocity). Patients may not be blue yet TTE is not enough to r/o CHD. All patients should have TEE before making a diagnosis of PPH
16 Catheterization Should be performed with meticulous attention to details. On room air extensive set of saturations to r/o anomalous veins and unexpected shunt lesions In collateral circulation go distal enough Try to cross the ias and have an LV cath to write simultaneous pressure with wedge on both lungs Repeat measurement on oxygen by mask for 20 minutes and again after potent vasodilator (NO, iloprost inhalation). Calculations should include disolved oxygen. Indexed resistances should be the standard
17 Assessing operability of shunt lesions A calculated indexed PVR of up to 7 Woods x msq with oxygen or potent pulmonary vasodilator is usually operable with good chance of resolution Indexed PVR >12 Woods x msq is usually considered inoperable Indexed PVR 8-12 Woods x msq is less predictable. Some advocate a prolonged trial with medication and repeat study
18 PHT in repaired CHD Assuming the PVR at the time of repair was still in the operable or borderline range, the continuing rise in resistance is an autonomous and unpredictable process, quite similar to that in PPH. Still, the rate of progression is usually far slower, probably because of a more heterogeneous genetic susceptibility The pathophysiology is similar to PPH, having two separate circulations, with the systemic circulation being totally dependent on the pulmonary circulation.

19 שלושת המסלולים לפעולת תכשירים נגד יתר לחץ דם ראתי
20 Drugs improve functional class, hemodynamics and survival (?) Endothelin receptor antagonists non selective (bosentan) selective sitaxentan and ambrisentan (no interaction coumadin, less liver toxicity) PDE inhibitors sildenafil and tadalafil Prostacycline analgues epoprostenol (iv only), trepostinil (sc, iv, in testing inhaled and oral), iloprost (inhaled, iv) Rehab programs - physical activity seems promising alternative
21 Deteriorating patient and unsettled issues Combination therapy (wait for deterioration or initiate early?) Atrial septostomy for syncope Lung, double lung, heart lung transplantation (40% 5 year survival) Pulmonary thrombendarterectomy (excellent option in good hands 3% mortality) Should we treat FC II patients? (Early study). FDA approval of ambrisentan for class II and III
22
23 Paul Wood The Croonian Lecture
24 Eisenmenger syndrome This is the form of PHT that is unique to CHD Tissue perfusion is adequate, as systemic circulation is not dependent on pulmonary flow The poor oxygen content of the blue blood is compensated for by secondary erythrocytosis Except for ASD, pulmonary pressure cannot exceed systemic pressure
25 Eisenmenger syndrome the eighth wonder of the world Unique pathophysiology, allowing people with the same malignant vascular disease in the lungs that kills PPH patients in 3-5 years, to live up to years and sometimes more, with often a reasonable quality of life Surprising improved survival over the last decades for an untreatable disease partly due to improved understanding and fewer management mistakes Survival is better for simple lesions than complex CHD
26 Care of Eisenmenger patients do s Close follow up and monitoring of physical findings (edema, saturation) blood tests, functional class, echo myocardial function and valves (not pulmonary pressure ) Holter monitoring for palpitations and syncope (not routine) Therapeutic phlebotomies only for hyperviscosity symptoms. Proper fluid replacement (preferably colloid) Use filters on venous lines Hospitalize for hemopthysis and sedate
27 Care of Eisenmenger patients don ts Avoid anti aggregants and anti coagulants unless absolute indication Avoid unnecessary medical procedures by all means. Prepare thoroughly for unavoidable ones Avoid pregnancy which is still considered a major maternal risk Avoid dehydration, hot places (disco) Avoid long haul flights (split)
28 Pharmacological intervention in Eisenmenger syndrome Simple drugs are helpful: digoxin, careful use of diuretics, amiodarone, oxygen (for symptoms) PHT specific medication: early studies included PPH patients and repaired CHD, not Eisenmengers. Concern that vasodilators can worsen cyanosis (probably not a problem) Long survival with reasonable quality of life; very different from PPH. Treat for thirty years? Stopping medication can cause rebound. Therefore timing of intervention is crucial.
29 PH specific drugs in Eisenmenger Breathe 5 - Comparison bosenthan vs placebo in eisenmenger improved walking distance and hemodynamics Naples open label 22 patients improved everything incl. cath parameters India tadalafil improved everything incl. cath parameters Leuven treatment delays need for transplantation but not death
30 70 years old Eisenmenger patient Large VSD Engineer, worked until timely retirement On amlodipine for hypertension, digoxin, diuretics O2 saturation 78% Hb 19g% more difficult to walk recently Has two six minutes tests walks more than 500 m each time - reassurance Than has a chest CT ordered by a pulmonologist
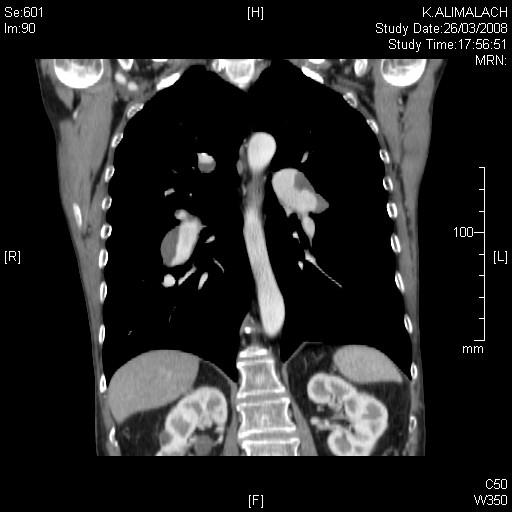
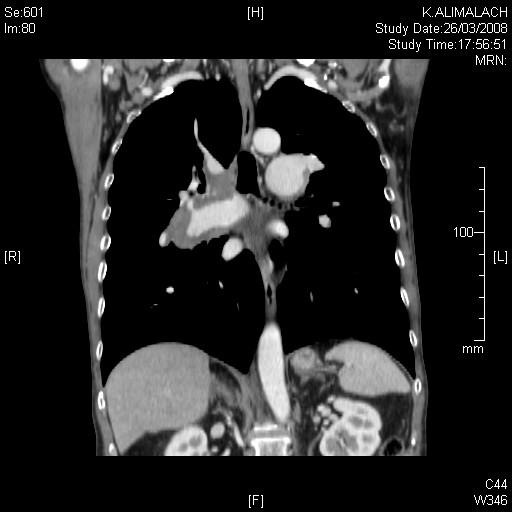
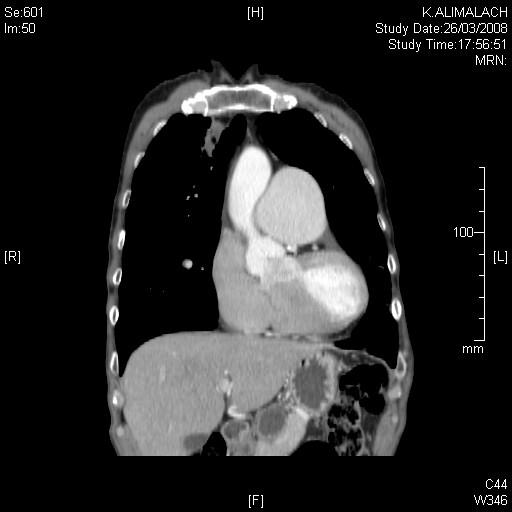

31
32 Suggestion Congenital heart specialists are the best equipped professionals for the initial evaluation of patients with pulmonary hypertension
33 Venice classification Pulmonary arterial hypertension (PAH) 1.1. Idiopathic (IPAH) 1.2. Familial (FPAH) 1.3. Associated with (APAH): Collagen vascular disease Congenital systemic-to-pulmonary shunts** Portal hypertension HIV infection Drugs and toxins Other (thyroid disorders, glycogen storage disease, Gaucher disease, hereditary hemorrhagic telangiectasia, hemoglobinopathies, myeloproliferative disorders, splenectomy) 1.4. Associated with significant venous or capillary involvement Pulmonary veno-occlusive disease (PVOD) Pulmonary capillary hemangiomatosis (PCH) 1.5. Persistent pulmonary hypertension of the newborn 2. Pulmonary hypertension with left heart disease 2.1. Left-sided atrial or ventricular heart disease 2.2. Left-sided valvular heart disease 3. Pulmonary hypertension associated with lung diseases and/or hypoxemia 3.1. Chronic obstructive pulmonary disease 3.2. Interstitial lung disease 3.3. Sleep-disordered breathing 3.4. Alveolar hypoventilation disorders 3.5. Chronic exposure to high altitude 3.6. Developmental abnormalities 4. Pulmonary hypertension due to chronic thrombotic and/or embolic disease 4.1. Thromboembolic obstruction of proximal pulmonary arteries 4.2. Thromboembolic obstruction of distal pulmonary arteries 4.3. Non-thrombotic pulmonary embolism (tumor, parasites, foreign material) 5. Miscellaneous Sarcoidosis, histiocytosis X, lymphangiomatosis, compression of pulmonary vessels (adenopathy, tumor, fibrosing mediastinitis)
Pulmonary hypertension
 Pulmonary hypertension Rafael Hirsch, MD Adult Congenital Heart Unit Dept. of Cardiology, Beilinson Hospital-Rabin Medical Center and Sackler School of Medicine, Tel Aviv University Pulmonary hypertension?
Pulmonary hypertension Rafael Hirsch, MD Adult Congenital Heart Unit Dept. of Cardiology, Beilinson Hospital-Rabin Medical Center and Sackler School of Medicine, Tel Aviv University Pulmonary hypertension?
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 has classified pulmonary hypertension into five different groups: (2)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.17 Subject: Remodulin Page: 1 of 5 Last Review Date: June 24, 2016 Remodulin Description Remodulin
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.17 Subject: Remodulin Page: 1 of 5 Last Review Date: June 24, 2016 Remodulin Description Remodulin
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 has classified pulmonary hypertension into five different groups: (2)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.16 Subject: Letairis Page: 1 of 6 Last Review Date: June 24, 2016 Letairis Description Letairis (ambrisentan)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.16 Subject: Letairis Page: 1 of 6 Last Review Date: June 24, 2016 Letairis Description Letairis (ambrisentan)
PVDOMICS. Study Introduction. Kristin Highland, MD Gerald Beck, PhD. NHLBI Pulmonary Vascular Disease Phenomics Program
 PVDOMICS Study Introduction Kristin Highland, MD Gerald Beck, PhD NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of
PVDOMICS Study Introduction Kristin Highland, MD Gerald Beck, PhD NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of
ADCIRCA (tadalafil) The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)") RATIONALE FOR INCLUSION IN PA PROGRAM Background Pulmonary arterial hypertension is a rare disorder of the pulmonary arteries in which the pulmonary arterial pressure rises above normal levels in the absence
RATIONALE FOR INCLUSION IN PA PROGRAM Background Pulmonary arterial hypertension is a rare disorder of the pulmonary arteries in which the pulmonary arterial pressure rises above normal levels in the absence
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 has classified pulmonary hypertension into five different groups: (2)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.21 Subject: Orenitram Page: 1 of 6 Last Review Date: June 24, 2016 Orenitram Description Orenitram
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.21 Subject: Orenitram Page: 1 of 6 Last Review Date: June 24, 2016 Orenitram Description Orenitram
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 has classified pulmonary hypertension into five different groups: (2)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.13 Section: Prescription Drugs Effective Date: July 1 2016 Subject: Tyvaso Page: 1 of 4 Last Review
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.13 Section: Prescription Drugs Effective Date: July 1 2016 Subject: Tyvaso Page: 1 of 4 Last Review
REVATIO (sildenafil)
") RATIONALE FOR INCLUSION IN PA PROGRAM Background Pulmonary arterial hypertension is a rare disorder of the pulmonary arteries in which the pulmonary arterial pressure rises above normal levels in the absence
RATIONALE FOR INCLUSION IN PA PROGRAM Background Pulmonary arterial hypertension is a rare disorder of the pulmonary arteries in which the pulmonary arterial pressure rises above normal levels in the absence
APPROACH TO THE ICCU PATIENT WITH PULMONARY HYPERTENSION
 APPROACH TO THE ICCU PATIENT WITH PULMONARY HYPERTENSION Rafael Hirsch, Adult Congenital Heart Unit Dept. of Cardiology Rabin Medical Center Beilinson Campus & Tel Aviv University Sackler School of Medicine,
APPROACH TO THE ICCU PATIENT WITH PULMONARY HYPERTENSION Rafael Hirsch, Adult Congenital Heart Unit Dept. of Cardiology Rabin Medical Center Beilinson Campus & Tel Aviv University Sackler School of Medicine,
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (3)
 has classified pulmonary hypertension into five different groups: (3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.15 Subject: Flolan Veletri Page: 1 of 5 Last Review Date: September 15, 2017 Flolan Veletri Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.15 Subject: Flolan Veletri Page: 1 of 5 Last Review Date: September 15, 2017 Flolan Veletri Description
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 has classified pulmonary hypertension into five different groups: (2)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.10 Subject: Uptravi Page: 1 of 6 Last Review Date: September 15, 2017 Uptravi Description Uptravi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.10 Subject: Uptravi Page: 1 of 6 Last Review Date: September 15, 2017 Uptravi Description Uptravi
22nd Annual Heart Failure 2018 an Update on Therapy. Pulmonary Arterial Hypertension: Contemporary Approach to Treatment
 22nd Annual Heart Failure 2018 an Update on Therapy Pulmonary Arterial Hypertension: Contemporary Approach to Treatment Ronald J. Oudiz, MD, FACP, FACC, FCCP Professor of Medicine The David Geffen School
22nd Annual Heart Failure 2018 an Update on Therapy Pulmonary Arterial Hypertension: Contemporary Approach to Treatment Ronald J. Oudiz, MD, FACP, FACC, FCCP Professor of Medicine The David Geffen School
PDE5 INHIBITOR POWDERS Sildenafil powder, Tadalafil powder
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Sildenafil and Tadalafil are marketed as Revatio and Adcirca for pulmonary arterial hypertension. This is a rare disorder of the pulmonary arteries in which
RATIONALE FOR INCLUSION IN PA PROGRAM Background Sildenafil and Tadalafil are marketed as Revatio and Adcirca for pulmonary arterial hypertension. This is a rare disorder of the pulmonary arteries in which
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 has classified pulmonary hypertension into five different groups: (2)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.23 Subject: Sildenafil Citrate Powder Page: 1 of 6 Last Review Date: September 15, 2017 Sildenafil
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.23 Subject: Sildenafil Citrate Powder Page: 1 of 6 Last Review Date: September 15, 2017 Sildenafil
PVDOMICS. Study Introduction. Kristin Highland, MD Gerald Beck, PhD. NHLBI Pulmonary Vascular Disease Phenomics Program
 PVDOMICS Study Introduction Kristin Highland, MD Gerald Beck, PhD NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of
PVDOMICS Study Introduction Kristin Highland, MD Gerald Beck, PhD NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of
The World Health Organization (WHO) has classified pulmonary hypertension into five different groups: (2)
 has classified pulmonary hypertension into five different groups: (2)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Tracleer Page: 1 of 6 Last Review Date: September 15, 2017 Tracleer Description Tracleer (bosentan)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Tracleer Page: 1 of 6 Last Review Date: September 15, 2017 Tracleer Description Tracleer (bosentan)
Neonatal and Pediatric Pulmonary Vascular Disease
 Neonatal and Pediatric Pulmonary Vascular Disease Emma Olson, MS, ARNP Pediatric Cardiology Nurse Practitioner Canadian Respiratory Conference April 14, 2018 Financial Interest Disclosure (over the past
Neonatal and Pediatric Pulmonary Vascular Disease Emma Olson, MS, ARNP Pediatric Cardiology Nurse Practitioner Canadian Respiratory Conference April 14, 2018 Financial Interest Disclosure (over the past
Pulmonary arterial hypertension. Pulmonary arterial hypertension: newer therapies. Definition of PH 12/18/16. WHO Group classification of PH
 Pulmonary arterial hypertension Pulmonary arterial hypertension: newer therapies Ramona L. Doyle, MD Clinical Professor of Medicine, UCSF Attending Physician UCSF PH Clinic Definition and classification
Pulmonary arterial hypertension Pulmonary arterial hypertension: newer therapies Ramona L. Doyle, MD Clinical Professor of Medicine, UCSF Attending Physician UCSF PH Clinic Definition and classification
Recruitment and Consenting
 1 Recruitment and Consenting MOP Chapter 4 NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of Health with support from
1 Recruitment and Consenting MOP Chapter 4 NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of Health with support from
Pulmonary Hypertension in 2012
 Pulmonary Hypertension in 2012 Evan Brittain, MD December 7, 2012 Kingston, Jamaica VanderbiltHeart.com Disclosures None VanderbiltHeart.com Outline Definition and Classification of PH Hemodynamics of
Pulmonary Hypertension in 2012 Evan Brittain, MD December 7, 2012 Kingston, Jamaica VanderbiltHeart.com Disclosures None VanderbiltHeart.com Outline Definition and Classification of PH Hemodynamics of
Paediatric PAH in the current era
 Paediatric PAH in the current era Dunbar Ivy, MD The Children s Hospital Heart Institute University of Colorado School of Medicine Paediatric PAH in the current era & A Gap Analysis Dunbar Ivy, MD The
Paediatric PAH in the current era Dunbar Ivy, MD The Children s Hospital Heart Institute University of Colorado School of Medicine Paediatric PAH in the current era & A Gap Analysis Dunbar Ivy, MD The
Update in Pulmonary Arterial Hypertension
 Update in Pulmonary Arterial Hypertension Michael J Sanley, MD April 12, 2018 Disclosures I have nothing to disclose 2 1 Case Presentation 67 yo male with atrial fibrillation, CLL on IVIG, presents with
Update in Pulmonary Arterial Hypertension Michael J Sanley, MD April 12, 2018 Disclosures I have nothing to disclose 2 1 Case Presentation 67 yo male with atrial fibrillation, CLL on IVIG, presents with
Pulmonary Hypertension. Murali Chakinala, M.D. Washington University School of Medicine
 Pulmonary Hypertension Murali Chakinala, M.D. Washington University School of Medicine Pulmonary Circulation Alveolar Capillary relationship Pulmonary Circulation High flow, low resistance PVR ~1/15 of
Pulmonary Hypertension Murali Chakinala, M.D. Washington University School of Medicine Pulmonary Circulation Alveolar Capillary relationship Pulmonary Circulation High flow, low resistance PVR ~1/15 of
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT
 DRAFT") European Medicines Agency London, 18 December 2008 Doc. Ref. EMEA/CHMP/EWP/356954/2008 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT CHMP GUIDELINE ON THE CLINICAL INVESTIGATIONS OF MEDICINAL
European Medicines Agency London, 18 December 2008 Doc. Ref. EMEA/CHMP/EWP/356954/2008 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT CHMP GUIDELINE ON THE CLINICAL INVESTIGATIONS OF MEDICINAL
Effective Strategies and Clinical Updates in Pulmonary Arterial Hypertension
 Effective Strategies and Clinical Updates in Pulmonary Arterial Hypertension Hap Farber Director, Pulmonary Hypertension Center Boston University School of Medicine Disclosures 1) Honoria: Actelion, Gilead,
Effective Strategies and Clinical Updates in Pulmonary Arterial Hypertension Hap Farber Director, Pulmonary Hypertension Center Boston University School of Medicine Disclosures 1) Honoria: Actelion, Gilead,
Ειδικές θεραπείες σε µη-αρτηριακή πνευµονική υπέρταση, πότε; - Στέλλα Μπρίλη Α Πανεπιστηµιακή Καρδιολογική Κλινική Ιπποκράτειο Νοσοκοµείο Αθηνών
 Ειδικές θεραπείες σε µη-αρτηριακή πνευµονική υπέρταση, πότε; - Στέλλα Μπρίλη Α Πανεπιστηµιακή Καρδιολογική Κλινική Ιπποκράτειο Νοσοκοµείο Αθηνών . Updated Clinical Classification of Pulmonary Hypertension
Ειδικές θεραπείες σε µη-αρτηριακή πνευµονική υπέρταση, πότε; - Στέλλα Μπρίλη Α Πανεπιστηµιακή Καρδιολογική Κλινική Ιπποκράτειο Νοσοκοµείο Αθηνών . Updated Clinical Classification of Pulmonary Hypertension
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal. Drugs for the treatment of pulmonary arterial hypertension
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Draft remit / appraisal objective: Draft scope To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Draft remit / appraisal objective: Draft scope To appraise the clinical and cost effectiveness
Valutazione del neonato con sospetta ipertensione polmonare
 Valutazione del neonato con sospetta ipertensione polmonare Cardiologia Pediatrica Seconda Università degli Studi di Napoli A.O. R.N. dei Colli-Monaldi Napoli Hypoxiemic infant Full or near-term neonate
Valutazione del neonato con sospetta ipertensione polmonare Cardiologia Pediatrica Seconda Università degli Studi di Napoli A.O. R.N. dei Colli-Monaldi Napoli Hypoxiemic infant Full or near-term neonate
Multimodality imaging for PAH: Is CT better than MRI?
 UNIVERSITÀ DEGLI STUDI DI TORINO Facoltà di Medicina e Chirurgia Dipartimento di Scienze Chirurgiche Istituto di Radiologia Azienda Ospedaliera Universitaria Città della Salute e della scienza di Torino
UNIVERSITÀ DEGLI STUDI DI TORINO Facoltà di Medicina e Chirurgia Dipartimento di Scienze Chirurgiche Istituto di Radiologia Azienda Ospedaliera Universitaria Città della Salute e della scienza di Torino
Pulmonary Hypertension: ICD-10 I27.0, I27.2
 Dr Manish Barman, MD. Membership and Affiliations ESC, European association of cardiovascular prevention and rehabilitation. Acute Cardiovascular Care Association. ESC, Working Group on Hypertension &
Dr Manish Barman, MD. Membership and Affiliations ESC, European association of cardiovascular prevention and rehabilitation. Acute Cardiovascular Care Association. ESC, Working Group on Hypertension &
Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, and Pulmonary Thromboendarterectomy Program
 Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, and Pulmonary Thromboendarterectomy Program Advanced Heart Failure & Cardiac Transplant Temple University
Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, and Pulmonary Thromboendarterectomy Program Advanced Heart Failure & Cardiac Transplant Temple University
Pulmonary Hypertension: Another Use for Viagra
 Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
ADVANCED THERAPIES FOR PHARMACOLOGICAL TREATMENT OF PULMONARY HYPERTENSION
 Status Active Medical and Behavioral Health Policy Section: Medicine Policy Number: II-107 Effective Date: 04/21/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members
Status Active Medical and Behavioral Health Policy Section: Medicine Policy Number: II-107 Effective Date: 04/21/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members
PULMONARY HYPERTENSION
 PULMONARY HYPERTENSION REVIEW & UPDATE Olga M. Fortenko, M.D. Pulmonary & Critical Care Medicine Pulmonary Vascular Diseases Sequoia Hospital 650-216-9000 Olga.Fortenko@dignityhealth.org Disclosures None
PULMONARY HYPERTENSION REVIEW & UPDATE Olga M. Fortenko, M.D. Pulmonary & Critical Care Medicine Pulmonary Vascular Diseases Sequoia Hospital 650-216-9000 Olga.Fortenko@dignityhealth.org Disclosures None
4/14/2010. Pulmonary Hypertension: An Update. Tim Williamson, MD, FCCP. University of Kansas Hospital. Normal Physiology
 Pulmonary Hypertension: An Update Tim Williamson, MD, FCCP Director, Pulmonary Vascular Program University of Kansas Hospital Normal Physiology 1 Pulmonary Perfusion 101 High Pressure Low Pressure Pulmonary
Pulmonary Hypertension: An Update Tim Williamson, MD, FCCP Director, Pulmonary Vascular Program University of Kansas Hospital Normal Physiology 1 Pulmonary Perfusion 101 High Pressure Low Pressure Pulmonary
Dr. Md. Rajibul Alam Prof. of Medicine Dinajpur Medical college
 Dr. Md. Rajibul Alam Prof. of Medicine Dinajpur Medical college PULMONARY HYPERTENSION Difficult to diagnose early Because Not detected during routine physical examination and Even in advanced cases symptoms
Dr. Md. Rajibul Alam Prof. of Medicine Dinajpur Medical college PULMONARY HYPERTENSION Difficult to diagnose early Because Not detected during routine physical examination and Even in advanced cases symptoms
2/4/2011. Nathan Kerner, M.D.
 Nathan Kerner, M.D. Definition Elevated pressures - cut off usually >40 mmhg pulmonary artery systolic pressure (PASP) Usually associated with elevated pulmonary vascular resistance (PVR) measured in dynessec/cm
Nathan Kerner, M.D. Definition Elevated pressures - cut off usually >40 mmhg pulmonary artery systolic pressure (PASP) Usually associated with elevated pulmonary vascular resistance (PVR) measured in dynessec/cm
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 SILDENAFIL oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage Guideline
SILDENAFIL oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage Guideline
Instructions: This form is completed and entered for all participants. Database will skip over sections that do not apply.
 Revision of 08/30/2017 Form #102 Page 1 of 6 PVDOMICS STUDY PVD Assessment - Form #102 Instructions: This form is completed and entered for all participants. Database will skip over sections that do not
Revision of 08/30/2017 Form #102 Page 1 of 6 PVDOMICS STUDY PVD Assessment - Form #102 Instructions: This form is completed and entered for all participants. Database will skip over sections that do not
Pulmonary Hypertension Perioperative Management
 Pulmonary Hypertension Perioperative Management Bruce J Leone, MD Professor of Anesthesiology Chief, Neuroanesthesiology Vice Chair for Academic Affairs Mayo Clinic Jacksonville, Florida Introduction Definition
Pulmonary Hypertension Perioperative Management Bruce J Leone, MD Professor of Anesthesiology Chief, Neuroanesthesiology Vice Chair for Academic Affairs Mayo Clinic Jacksonville, Florida Introduction Definition
Teaching Round Claudio Sartori
 Teaching Round 14.03.2017 Claudio Sartori Cas clinique Femme 47 ans, connue pour un BPCO, asthénie, douleurs thoraciques, dyspnée à l effort, œdèmes membres inférieurs, deux syncopes. Tabac, BMI 31 kg/m2
Teaching Round 14.03.2017 Claudio Sartori Cas clinique Femme 47 ans, connue pour un BPCO, asthénie, douleurs thoraciques, dyspnée à l effort, œdèmes membres inférieurs, deux syncopes. Tabac, BMI 31 kg/m2
Corporate Medical Policy
 Corporate Medical Policy Pulmonary Hypertension, Drug Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pulmonary_hypertension_drug_management 06/1998 3/2018 3/2019 3/2018
Corporate Medical Policy Pulmonary Hypertension, Drug Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pulmonary_hypertension_drug_management 06/1998 3/2018 3/2019 3/2018
Sildenafil Citrate Powder. Sildenafil citrate powder. Description. Section: Prescription Drugs Effective Date: January 1, 2016
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.06.15 Subject: Sildenafil Citrate Powder Page: 1 of 6 Last Review Date: December 3, 2015 Sildenafil Citrate
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.06.15 Subject: Sildenafil Citrate Powder Page: 1 of 6 Last Review Date: December 3, 2015 Sildenafil Citrate
Acute Vasodilator Testing in Pulmonary Hypertension: What, When, and How?
 Acute Vasodilator Testing in Pulmonary Hypertension: What, When, and How? Teresa De Marco, MD University of California, San Francisco Disclosures: Grants/Research: United Therapeutics, Lung Biotechnology,
Acute Vasodilator Testing in Pulmonary Hypertension: What, When, and How? Teresa De Marco, MD University of California, San Francisco Disclosures: Grants/Research: United Therapeutics, Lung Biotechnology,
ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY
 ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY Contents Eligibility criteria for Pulmonary Arterial Hypertension therapy...2-6 Initial Application for funding of Pulmonary Arterial Hypertension
ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY Contents Eligibility criteria for Pulmonary Arterial Hypertension therapy...2-6 Initial Application for funding of Pulmonary Arterial Hypertension
Right Ventricular Failure and Pulmonary Hypertension 2011
 Right Ventricular Failure and Pulmonary Hypertension 2011 George G. Sokos, DO FACC Assistant Professor of Medicine, Temple University Director, Advanced Heart Failure and Cardiac Transplant Fellowship
Right Ventricular Failure and Pulmonary Hypertension 2011 George G. Sokos, DO FACC Assistant Professor of Medicine, Temple University Director, Advanced Heart Failure and Cardiac Transplant Fellowship
Current and Emerging Drugs in Pulmonary Vascular Pharmacology Dr AS Paul DM Seminar 08 September 06
 Current and Emerging Drugs in Pulmonary Vascular Pharmacology Dr AS Paul DM Seminar 08 September 06 Pulmonary Hypertension A mean pressure of greater than 25 mm Hg at rest (normal ~14 mm Hg) or greater
Current and Emerging Drugs in Pulmonary Vascular Pharmacology Dr AS Paul DM Seminar 08 September 06 Pulmonary Hypertension A mean pressure of greater than 25 mm Hg at rest (normal ~14 mm Hg) or greater
PULMONARY HYPERTENSION & THALASSAEMIA
 3rd Pan-American Thalassaemia Conference Buenos Aires 2010 Dr Malcolm Walker Cardiologist University College & the Heart Hospital LONDON Clinical Director Hatter Cardiovascular Institute - UCLH PULMONARY
3rd Pan-American Thalassaemia Conference Buenos Aires 2010 Dr Malcolm Walker Cardiologist University College & the Heart Hospital LONDON Clinical Director Hatter Cardiovascular Institute - UCLH PULMONARY
Pulmonary Hypertension: Classification
 Pulmonary Hypertension: Pathophysiology and Classification M. Maggiorini Medical Intensive Care Unit University Hospital Zürich Pulmonary hypertension is a disease of the pulmonary circulation with many
Pulmonary Hypertension: Pathophysiology and Classification M. Maggiorini Medical Intensive Care Unit University Hospital Zürich Pulmonary hypertension is a disease of the pulmonary circulation with many
Pulmonary Vascular Disorders
 Progress in Respiratory Research 41 Pulmonary Vascular Disorders Bearbeitet von M. Humbert, R. Souza, G. Simonneau, F.J.F. Herth 1. Auflage 2012. Buch. X, 290 S. Hardcover ISBN 978 3 8055 9914 6 Gewicht:
Progress in Respiratory Research 41 Pulmonary Vascular Disorders Bearbeitet von M. Humbert, R. Souza, G. Simonneau, F.J.F. Herth 1. Auflage 2012. Buch. X, 290 S. Hardcover ISBN 978 3 8055 9914 6 Gewicht:
PULMONARY HYPERTENSION
 PULMONARY HYPERTENSION MARTIN T. MPE CARDIOLOGIST MEDICLINIC HEART HOSPITAL CASE REPORT A 35 year old female, general worker. Married with 2 children with the youngest aged 12 years. Presenting complaints
PULMONARY HYPERTENSION MARTIN T. MPE CARDIOLOGIST MEDICLINIC HEART HOSPITAL CASE REPORT A 35 year old female, general worker. Married with 2 children with the youngest aged 12 years. Presenting complaints
Cardiac Catheterization is Unnecessary in the Evaluation of Patients with Pulmonary Hypertension: CON
 Cardiac Catheterization is Unnecessary in the Evaluation of Patients with Pulmonary Hypertension: CON Dunbar Ivy, MD The Children s s Hospital Heart Institute 1 Diagnostic Evaluation: Right Heart Cardiac
Cardiac Catheterization is Unnecessary in the Evaluation of Patients with Pulmonary Hypertension: CON Dunbar Ivy, MD The Children s s Hospital Heart Institute 1 Diagnostic Evaluation: Right Heart Cardiac
Pulmonary hypertension. Miloslav Špaček, MD
 Pulmonary hypertension Miloslav Špaček, MD Key points Pulmonary hypertension (PH) is a hemodynamic and pathophysiological abnormality found in many clinical conditions, most commonly heart and lung disease
Pulmonary hypertension Miloslav Špaček, MD Key points Pulmonary hypertension (PH) is a hemodynamic and pathophysiological abnormality found in many clinical conditions, most commonly heart and lung disease
SA XXXX Special Authority for Subsidy
 SA XXXX Special Authority for Subsidy Special authority approved by the Pulmonary Arterial Hypertension (PAH) Panel. Application forms can be obtained from PHARMAC s website: www.pharmac.govt.nz or: PAH
SA XXXX Special Authority for Subsidy Special authority approved by the Pulmonary Arterial Hypertension (PAH) Panel. Application forms can be obtained from PHARMAC s website: www.pharmac.govt.nz or: PAH
Pulmonary Hypertension. Pulmonary Arterial Hypertension Diagnosis, Impact and Outcomes
 Pulmonary Hypertension Pulmonary Arterial Hypertension Diagnosis, Impact and Outcomes Pulmonary Arterial Hypertension Disease of small pulmonary arteries Characteristic changes Medial hypertrophy Intimal
Pulmonary Hypertension Pulmonary Arterial Hypertension Diagnosis, Impact and Outcomes Pulmonary Arterial Hypertension Disease of small pulmonary arteries Characteristic changes Medial hypertrophy Intimal
2nd ECHO ASE-ASEAN: Bangkok 22nd October DR. TAN JU LE Pulmonary Hypertension Services National Heart Centre SINGAPORE
 2nd ECHO ASE-ASEAN: Bangkok 22nd October 2016 DR. TAN JU LE Pulmonary Hypertension Services National Heart Centre SINGAPORE Definition of Pulmonary Hypertension and Cor Pulmonale Epidemiology and Pathophysiology
2nd ECHO ASE-ASEAN: Bangkok 22nd October 2016 DR. TAN JU LE Pulmonary Hypertension Services National Heart Centre SINGAPORE Definition of Pulmonary Hypertension and Cor Pulmonale Epidemiology and Pathophysiology
Update on pulmonary HTN
 Update on pulmonary HTN Feras Bader, MD, MS, FACC Associate Professor of Medicine- Cardiology University of Utah School of Medicine Director, Advanced Heart Failure and Transplant Program Dabbous Cardiac
Update on pulmonary HTN Feras Bader, MD, MS, FACC Associate Professor of Medicine- Cardiology University of Utah School of Medicine Director, Advanced Heart Failure and Transplant Program Dabbous Cardiac
Pulmonary Hypertension: Clinical Features & Recent Advances
 Pulmonary Hypertension: Clinical Features & Recent Advances Lisa J. Rose-Jones, MD Assistant Professor of Medicine, Division of Cardiology Advanced Heart Failure/Cardiac Transplantation & Pulmonary Hypertension
Pulmonary Hypertension: Clinical Features & Recent Advances Lisa J. Rose-Jones, MD Assistant Professor of Medicine, Division of Cardiology Advanced Heart Failure/Cardiac Transplantation & Pulmonary Hypertension
Phosphodiesterase Type 5 Inhibitors: ADCIRCA (tadalafil) oral tablet REVATIO (sildenafil) oral suspension and tablet
 oral tablet REVATIO (sildenafil) oral suspension and tablet") REVATIO (sildenafil) oral suspension and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
REVATIO (sildenafil) oral suspension and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
Review Article Diagnosis and Management of Pulmonary Arterial Hypertension
 Pulmonary Medicine Volume 2011, Article ID 845864, 13 pages doi:10.1155/2011/845864 Review Article Diagnosis and Management of Pulmonary Arterial Hypertension Jeanne Houtchens, Douglas Martin, and James
Pulmonary Medicine Volume 2011, Article ID 845864, 13 pages doi:10.1155/2011/845864 Review Article Diagnosis and Management of Pulmonary Arterial Hypertension Jeanne Houtchens, Douglas Martin, and James
Pulmonary Heart Disease: Evaluation and Management
 Pulmonary Heart Disease: Evaluation and Management Robert C. Bourge, MD Professor of Medicine, Radiology, and Surgery Drummond Chair of Cardiovascular Medicine Vice Chair of Clinical Affairs, Department
Pulmonary Heart Disease: Evaluation and Management Robert C. Bourge, MD Professor of Medicine, Radiology, and Surgery Drummond Chair of Cardiovascular Medicine Vice Chair of Clinical Affairs, Department
Pulmonary Hypertension: Definition and Unmet Needs
 Heart Failure Center Hadassah University Hospital Pulmonary Hypertension: Definition and Unmet Needs Israel Gotsman The Heart Failure Center Hadassah University Hospital I DO NOT have a financial interest/
Heart Failure Center Hadassah University Hospital Pulmonary Hypertension: Definition and Unmet Needs Israel Gotsman The Heart Failure Center Hadassah University Hospital I DO NOT have a financial interest/
2009 ESC ERS Pulmonary Hypertension Guidelines and Connective Tissue Disease Norifumi Nakanishi 1
 Allergology International. 2011;60:419-424 DOI: 10.2332 allergolint.11-rai-0362 REVIEW ARTICLE 2009 ESC ERS Pulmonary Hypertension Guidelines and Connective Tissue Disease Norifumi Nakanishi 1 ABSTRACT
Allergology International. 2011;60:419-424 DOI: 10.2332 allergolint.11-rai-0362 REVIEW ARTICLE 2009 ESC ERS Pulmonary Hypertension Guidelines and Connective Tissue Disease Norifumi Nakanishi 1 ABSTRACT
final 1. Pulmonary Vascular Changes in Heart Disease. Normal Post-Natal Changes in the Pulmonary Circulation. Exercise. Pulmonary Circulation
 Vascular Changes in Heart Disease Normal Circulatory Dynamics Physiology Hypertension Definition Classification Pathology Pathophysiology Clinical Manifestations Diagnosis Treatment Normal Circulatory
Vascular Changes in Heart Disease Normal Circulatory Dynamics Physiology Hypertension Definition Classification Pathology Pathophysiology Clinical Manifestations Diagnosis Treatment Normal Circulatory
PULMONARY HYPERTENSION RESPIRATORY & CRITICAL CARE CONFERENCE APRIL 21, 2016 LAURA G. HOOPER
 PULMONARY HYPERTENSION RESPIRATORY & CRITICAL CARE CONFERENCE APRIL 21, 2016 LAURA G. HOOPER OUTLINE Brief review of WHO Group Classification Scheme Subgroups we ll focus on: WHO Group I Pulmonary Arterial
PULMONARY HYPERTENSION RESPIRATORY & CRITICAL CARE CONFERENCE APRIL 21, 2016 LAURA G. HOOPER OUTLINE Brief review of WHO Group Classification Scheme Subgroups we ll focus on: WHO Group I Pulmonary Arterial
Clinical implication of exercise pulmonary hypertension: when should we measure it?
 Clinical implication of exercise pulmonary hypertension: when should we measure it? Jang-Young, Kim Wonju College of Medicine, Yonsei Univ. Exercise pulmonary hypertension (EPH) Introduction of pulmonary
Clinical implication of exercise pulmonary hypertension: when should we measure it? Jang-Young, Kim Wonju College of Medicine, Yonsei Univ. Exercise pulmonary hypertension (EPH) Introduction of pulmonary
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
Advanced Therapies for Pharmocological Treatment of Pulmonary Arterial Hypertension. Original Policy Date
 MP 5.01.07 Advanced Therapies for Pharmocological Treatment of Pulmonary Arterial Hypertension Medical Policy Section Prescription Drug Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
MP 5.01.07 Advanced Therapies for Pharmocological Treatment of Pulmonary Arterial Hypertension Medical Policy Section Prescription Drug Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
ACTIVITY DESCRIPTION Target Audience Learning Objectives
 ACTIVITY DESCRIPTION Target Audience This continuing medical education activity is planned to meet the needs of primary care physicians who can contribute to early detection of disease and who are responsible
ACTIVITY DESCRIPTION Target Audience This continuing medical education activity is planned to meet the needs of primary care physicians who can contribute to early detection of disease and who are responsible
Pulmonary Hypertension and Left Heart Disease: What s good for the goose is not necessary good for the gander
 Pulmonary Hypertension and Left Heart Disease: What s good for the goose is not necessary good for the gander Jacqueline Fearon-Clarke, MA, ACNP-BC Heart Failure and Pulmonary Hypertension Nurse Practitioner
Pulmonary Hypertension and Left Heart Disease: What s good for the goose is not necessary good for the gander Jacqueline Fearon-Clarke, MA, ACNP-BC Heart Failure and Pulmonary Hypertension Nurse Practitioner
Approach to Pulmonary Hypertension in the Hospital
 Approach to Pulmonary Hypertension in the Hospital Todd M Bull MD Professor of Medicine Director Pulmonary Vascular Disease Center Director Center for Lungs and Breathing Division of Pulmonary Sciences
Approach to Pulmonary Hypertension in the Hospital Todd M Bull MD Professor of Medicine Director Pulmonary Vascular Disease Center Director Center for Lungs and Breathing Division of Pulmonary Sciences
Pulmonary hypertension
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2012 Pulmonary hypertension Glaus, T M Posted at the Zurich Open Repository
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2012 Pulmonary hypertension Glaus, T M Posted at the Zurich Open Repository
Pulmonary Hypertension: Follow-up in adolescence and adults
 Pulmonary Hypertension: Follow-up in adolescence and adults Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of Muenster Germany
Pulmonary Hypertension: Follow-up in adolescence and adults Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of Muenster Germany
Pulmonary Arterial Hypertension - Overview
 Pulmonary Arterial Hypertension - Overview J. Shaun Smith, MD Co-Director, Pulmonary Vascular Disease Program Assistant Professor of Medicine Division of Pulmonary, Critical Care and Sleep Medicine The
Pulmonary Arterial Hypertension - Overview J. Shaun Smith, MD Co-Director, Pulmonary Vascular Disease Program Assistant Professor of Medicine Division of Pulmonary, Critical Care and Sleep Medicine The
Pulmonary Arterial Hypertension - Overview
 Pulmonary Arterial Hypertension - Overview J. Shaun Smith, MD Co-Director, Pulmonary Vascular Disease Program Assistant Professor of Medicine Division of Pulmonary, Critical Care and Sleep Medicine The
Pulmonary Arterial Hypertension - Overview J. Shaun Smith, MD Co-Director, Pulmonary Vascular Disease Program Assistant Professor of Medicine Division of Pulmonary, Critical Care and Sleep Medicine The
Recent Treatment of Pulmonary Artery Hypertension. Cardiology Division Yonsei University College of Medicine
 Recent Treatment of Pulmonary Artery Hypertension Cardiology Division Yonsei University College of Medicine Definition Raised Pulmonary arterial pressure (PAP) WHO criteria : spap>40 mmhg NIH Criteria
Recent Treatment of Pulmonary Artery Hypertension Cardiology Division Yonsei University College of Medicine Definition Raised Pulmonary arterial pressure (PAP) WHO criteria : spap>40 mmhg NIH Criteria
The Epidemiology of At Risk groups for Pediatric PH. The Epidemiology of At Risk groups for Pediatric PH. Disclosures
 The Epidemiology of At Risk groups for Pediatric PH R.M.F. Berger Disclosures The has received fees for advisory board and steering committee activities of Prof. Berger from: - Actelion, - Bayer, - Glaxo-Smith-Kline,
The Epidemiology of At Risk groups for Pediatric PH R.M.F. Berger Disclosures The has received fees for advisory board and steering committee activities of Prof. Berger from: - Actelion, - Bayer, - Glaxo-Smith-Kline,
CONUNDRUMS IN PULMONARY ARTERIAL HYPERTENSION
 CONUNDRUMS IN PULMONARY ARTERIAL HYPERTENSION MOHAMMED RAFIQUE ESSOP MILPARK HOSPITAL and UNIVERSITY OF THE WITWATERSRAND POINTS FOR DISCUSSION What is the pathogenetic mechanism of PAH? Importance of
CONUNDRUMS IN PULMONARY ARTERIAL HYPERTENSION MOHAMMED RAFIQUE ESSOP MILPARK HOSPITAL and UNIVERSITY OF THE WITWATERSRAND POINTS FOR DISCUSSION What is the pathogenetic mechanism of PAH? Importance of
PULMONARY HYPERTENSION For Cardiologists
 PULMONARY HYPERTENSION For Cardiologists Pulmonary Hypertension Classification Pulmonary Hypertension General Definition Resting Systolic PAP Resting Diastolic PAP Resting Mean PAP > 35mmHg > 15mmHg >
PULMONARY HYPERTENSION For Cardiologists Pulmonary Hypertension Classification Pulmonary Hypertension General Definition Resting Systolic PAP Resting Diastolic PAP Resting Mean PAP > 35mmHg > 15mmHg >
The growing interest in pulmonary hypertension (PH) in
 in") Eur Respir J 2010; 36: 986 990 DOI: 10.1183/09031936.00038410 CopyrightßERS 2010 EDITORIAL Pulmonary hypertension and pulmonary arterial hypertension: a clarification is needed N. Galiè, M. Palazzini and
Eur Respir J 2010; 36: 986 990 DOI: 10.1183/09031936.00038410 CopyrightßERS 2010 EDITORIAL Pulmonary hypertension and pulmonary arterial hypertension: a clarification is needed N. Galiè, M. Palazzini and
It has been more than a decade since
 doi: 10.1111/j.1751-7133.2010.00192.x R EVIEW P APER Differentiating Pulmonary Arterial and Pulmonary Venous and the Implications for Therapy It has been more than a decade since the Second World Symposium
doi: 10.1111/j.1751-7133.2010.00192.x R EVIEW P APER Differentiating Pulmonary Arterial and Pulmonary Venous and the Implications for Therapy It has been more than a decade since the Second World Symposium
Pulmonary vascular remodelling: causes, mechanisms and consequences
 Pulmonary vascular remodelling: causes, mechanisms and consequences Ralph Schermuly Department of Pulmonary Pharmacotherapy University of Giessen and Marburg Lung Center email: ralph.schermuly@ugmlc.de
Pulmonary vascular remodelling: causes, mechanisms and consequences Ralph Schermuly Department of Pulmonary Pharmacotherapy University of Giessen and Marburg Lung Center email: ralph.schermuly@ugmlc.de
Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced
 Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced Heart Failure & Cardiac Transplant Temple University
Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced Heart Failure & Cardiac Transplant Temple University
Pediatric Pulmonary Hypertension: Inside Out
 Pediatric Pulmonary Hypertension: Inside Out Asma Razavi, MD Assistant Professor Pediatric Critical Care Medicine Loma Linda University Children s Hopsital Disclosures I have no conflicts of interest to
Pediatric Pulmonary Hypertension: Inside Out Asma Razavi, MD Assistant Professor Pediatric Critical Care Medicine Loma Linda University Children s Hopsital Disclosures I have no conflicts of interest to
Disclosures. Objectives 6/16/2016. A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension
 A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension Susan P. D Anna MSN, APN-BC, CHFN June 24, 2016 Disclosures Objectives Differentiate structure and function of RV and LV
A Look at the Other Side: Focus on the Right Ventricle and Pulmonary Hypertension Susan P. D Anna MSN, APN-BC, CHFN June 24, 2016 Disclosures Objectives Differentiate structure and function of RV and LV
SCIENTIFIC DISCUSSION
 European Medicines Agency Evaluation of Medicines for Human Use Product name: TRACLEER Procedure No. EMEA/H/C/401/II/27 SCIENTIFIC DISCUSSION 7 Westferry Circus, Canary Wharf, London, E14 4HB, UK Tel.
European Medicines Agency Evaluation of Medicines for Human Use Product name: TRACLEER Procedure No. EMEA/H/C/401/II/27 SCIENTIFIC DISCUSSION 7 Westferry Circus, Canary Wharf, London, E14 4HB, UK Tel.
A Best Practices Approach to Treating Pulmonary Hypertension for the ED and Acute Care Provider. Disclosures
 A Best Practices Approach to Treating Pulmonary Hypertension for the ED and Acute Care Provider Sean M. Studer, MD, MSc Chief, Pulmonary & Critical Care Director, Pulmonary Hypertension & Lung Transplantation
A Best Practices Approach to Treating Pulmonary Hypertension for the ED and Acute Care Provider Sean M. Studer, MD, MSc Chief, Pulmonary & Critical Care Director, Pulmonary Hypertension & Lung Transplantation
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH
 Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
2015 State-of-the-Art Management of Pulmonary Hypertension Based on an Understanding of the Various Etiologies
 2015 State-of-the-Art Management of Pulmonary Hypertension Based on an Understanding of the Various Etiologies Vallerie V. McLaughlin, MD, FACC, FAHA Kim A Eagle MD Endowed Professor of Cardiovascular
2015 State-of-the-Art Management of Pulmonary Hypertension Based on an Understanding of the Various Etiologies Vallerie V. McLaughlin, MD, FACC, FAHA Kim A Eagle MD Endowed Professor of Cardiovascular
THERAPEUTICS IN PULMONARY ARTERIAL HYPERTENSION Evidences & Guidelines
 THERAPEUTICS IN PULMONARY ARTERIAL HYPERTENSION Evidences & Guidelines Vu Nang Phuc, MD Dinh Duc Huy, MD Pham Nguyen Vinh, MD, PhD, FACC Tam Duc Cardiology Hospital Faculty Disclosure No conflict of interest
THERAPEUTICS IN PULMONARY ARTERIAL HYPERTENSION Evidences & Guidelines Vu Nang Phuc, MD Dinh Duc Huy, MD Pham Nguyen Vinh, MD, PhD, FACC Tam Duc Cardiology Hospital Faculty Disclosure No conflict of interest
Advances in Pharmacotherapy of PAH
 24 th Annual Advances in Heart Disease Advances in Pharmacotherapy of PAH Gabriel Gregoratos, MD 12/14/2007 UCSF Cardiology 1 Faculty Disclosure Statement for Gabriel Gregoratos, MD Nothing to disclose
24 th Annual Advances in Heart Disease Advances in Pharmacotherapy of PAH Gabriel Gregoratos, MD 12/14/2007 UCSF Cardiology 1 Faculty Disclosure Statement for Gabriel Gregoratos, MD Nothing to disclose
Identifying Appropriate Treatment & Management Strategies in Pulmonary Arterial Hypertension
 Identifying Appropriate Treatment & Management Strategies in Pulmonary Arterial Hypertension Harold I. Palevsky, M.D. Perelman School of Medicine of the University of Pennsylvania Penn Presbyterian Medical
Identifying Appropriate Treatment & Management Strategies in Pulmonary Arterial Hypertension Harold I. Palevsky, M.D. Perelman School of Medicine of the University of Pennsylvania Penn Presbyterian Medical
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Disclosure. RV is not the innocent bystander 10/1/16. Assessment and Management of Pulmonary Heart Disease in the Female Patient
 Assessment and Management of Pulmonary Heart Disease in the Female Patient Oct 1, 2016 Deborah Women s Heart Center Susan E Wiegers, MD, FASE, FACC Professor of Medicine Senior Associate Dean of Faculty
Assessment and Management of Pulmonary Heart Disease in the Female Patient Oct 1, 2016 Deborah Women s Heart Center Susan E Wiegers, MD, FASE, FACC Professor of Medicine Senior Associate Dean of Faculty
Advanced Therapies for Pharmacological Treatment of Pulmonary Arterial Hypertension
 MEDICAL POLICY 5.01.522 Advanced Therapies for Pharmacological Treatment of Pulmonary Arterial Hypertension BCBSA Ref. Policy: 5.01.09* Effective Date: Dec. 1, 2017 Last Revised: Nov. 21, 2017 Replaces:
MEDICAL POLICY 5.01.522 Advanced Therapies for Pharmacological Treatment of Pulmonary Arterial Hypertension BCBSA Ref. Policy: 5.01.09* Effective Date: Dec. 1, 2017 Last Revised: Nov. 21, 2017 Replaces: