Contents DEFINITION. TYPES EPIDEMIOLOGY PATHOPHYSIOLOGY. CLINICAL PRESENTATION. DIAGNOSIS. TREATMENT. EVALUATION OF THERAPEUTIC OUTCOMES.
|
|
|
- Kristin Glenn
- 5 years ago
- Views:
Transcription

1 Heart Failure
2 Contents DEFINITION. TYPES EPIDEMIOLOGY PATHOPHYSIOLOGY. CLINICAL PRESENTATION. DIAGNOSIS. TREATMENT. EVALUATION OF THERAPEUTIC OUTCOMES.
3 DEFINITION Heart failure (HF) is a progressive clinical syndrome caused by inability of the heart to pump sufficient blood to meet the body s metabolic needs. HF can result from any disorder that reduces ventricular filling (diastolic dysfunction) and/or myocardial contractility (systolic dysfunction).
4 TYPES Types of heart failure: High Output HF Low Output HF Left-sided HF Right-sided HF Biventricular HF
5 TYPES o Diastolic dysfunction o Systolic dysfunction Acute heart failure Chronic heart failure
6 EPIDEMIOLOGY Incidence of HF is greater in men and in the elderly (age > 65 y) The incidence in black women is as high as that of white men
7 PATHOPHYSIOLOGY Causes Systolic dysfunction (decreased contractility): 1. Reduced muscle mass (eg. MI) 2. Dilated cardiomyopathies 3. Ventricular hypertrophy
8 PATHOPHYSIOLOGY Ventricular hypertrophy can be caused by Pressure overload systemic or pulmonary hypertension aortic or pulmonic valve stenosis Volume overload valvular regurgitation high-output states
9 PATHOPHYSIOLOGY Diastolic dysfunction (restriction in ventricular filling): Increased ventricular stiffness Ventricular hypertrophy Infiltrative myocardial diseases endomyocardial Myocardial ischemia and MI Mitral or tricuspid valve stenosis Pericardial disease pericarditis, pericardial tamponade
10 PATHOPHYSIOLOGY The leading causes of HF are: Coronary artery disease Hypertension. As cardiac function decreases after myocardial injury, the heart relies on compensatory mechanisms
11 PATHOPHYSIOLOGY Compensatory mechanisms: 1. Tachycardia and increased contractility through sympathetic nervous system activation 2. The Frank Starling mechanism, whereby increased preload increases stroke volume 3. Vasoconstriction 4. Ventricular hypertrophy and remodeling.
12 PATHOPHYSIOLOGY Although these compensatory mechanisms initially maintain cardiac function, they are responsible for the symptoms of HF and contribute to disease progression. In the neurohormonal model of HF, an initiating event (eg, acute MI) decreased cardiac output; the HF state then becomes a systemic disease whose progression is mediated largely by neurohormones and autocrine/paracrine factors.
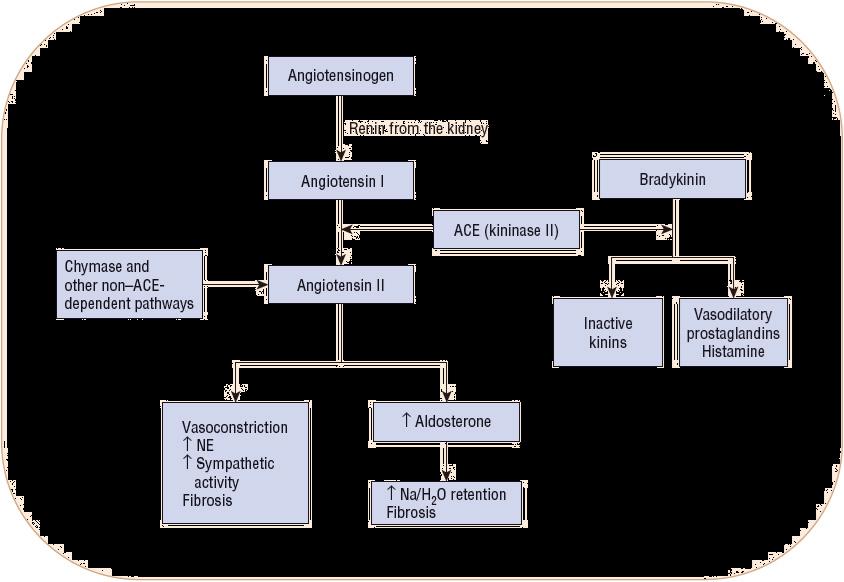
13 PATHOPHYSIOLOGY These substances include: 1. Angiotensin II 2. Norepinephrine 3. Aldosterone 4. Natriuretic peptides 5. Arginine vasopressin 6. Endothelin peptides 7. other circulating biomarkers (eg, C-reactive protein).
 effects; ADH, antidiuretic hormone; CO, cardiac output; HR, heart rate; H2O, water; Na+, sodium; RAAS,")
14 PATHOPHYSIOLOGY Adaptive mechanisms in systolic heart failure. +, beneficial results;, negative (detrimental) effects; ADH, antidiuretic hormone; CO, cardiac output; HR, heart rate; H2O, water; Na+, sodium; RAAS, renin-angiotensin-aldosterone system; SNS, sympathetic nervous system; SV, stroke volume.
15 PATHOPHYSIOLOGY
16 PATHOPHYSIOLOGY Common precipitating factors that may cause a previously compensated HF patient to decompensate include: 1. Myocardial ischemia and MI 2. Atrial fibrillation 3. Pulmonary infections 4. Nonadherence with diet or drug therapy 5. Inappropriate medication use.
17 PATHOPHYSIOLOGY Drugs may precipitate or exacerbate HF because of : Their negative inotropic properties Cardiotoxic properties Sodium- and water-retaining properties.
18 PATHOPHYSIOLOGY Drugs That May Precipitate or Exacerbate Heart Failure Negative inotropic effect Antiarrhythmics (e.g., disopyramide, flecainide, propafenone, and others) β-blockers (e.g., propranolol, metoprolol, atenolol, and others) Calcium channel blockers (e.g., verapamil, diltiazem) Terbinafine Cardiotoxic Doxorubicin Daunomycin Cyclophosphamide Trastuzumab Imatinib Ethanol Amphetamines (e.g., cocaine, methamphetamine)
19 PATHOPHYSIOLOGY Sodium and water retention Nonsteroidal antiinflammatory drugs Cyclooxygenase-2 inhibitors Rosiglitazone and pioglitazone Glucocorticoids Androgens and estrogens Salicylates (high dose) Sodium-containing drugs (e.g., carbenicillin disodium, ticarcillin disodium) Uncertain mechanism Infliximab Etanercept Dronedarone
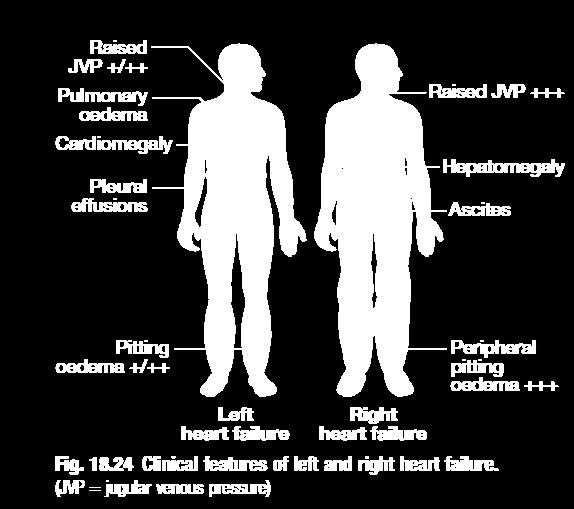
20 General CLINICAL PRESENTATION Patient presentation may range from asymptomatic to cardiogenic shock Symptoms Dyspnea, particularly on exertion Orthopnea Paroxysmal nocturnal dyspnea Exercise intolerance Tachypnea Cough Nocturia
21 CLINICAL PRESENTATION Hemoptysis Abdominal pain Anorexia Fatigue Nausea Bloating Poor appetite, early satiety Ascites Mental status changes Weight gain or loss
22 CLINICAL PRESENTATION Signs Pulmonary rales Pulmonary edema Cool extremities Pleural effusion Tachycardia Narrow pulse pressure Cardiomegaly Peripheral edema Jugular venous distention Hepatojugular reflux Hepatomegaly Venous stasis changes Lateral displacement of apical impulse
23 DIAGNOSIS Consider diagnosis of HF in patients with characteristic signs and symptoms. A complete history and physical examination with appropriate laboratory testing are essential in evaluating patients with suspected HF.
24 DIAGNOSIS Laboratory Tests Electrocardiogram may be normal or it could show numerous abnormalities including acute ST-T wave changes from myocardial ischemia, atrial fibrillation, bradycardia, left ventricular hypertrophy Serum creatinine: it may be increased due to hypoperfusion. Preexisting renal dysfunction can contribute to volume overload Complete blood count useful to determine if heart failure due to reduced oxygen-carrying capacity Chest x-ray: useful for detection of cardiac enlargement, pulmonary edema, and pleural effusions Echocardiogram: used to assess LV size, valve function, pericardial effusion, wall motion abnormalities, and ejection fraction Hyponatremia: serum sodium <130 meq/l (<130 mmol/l) is associated with reduced survival and may indicate worsening volume overload and/or disease progression
25 DIAGNOSIS
26 TREATMENT OF CHRONIC HF Goals of Treatment 1. Improve quality of life 2. Relieve or reduce symptoms 3. Prevent or minimize hospitalizations 4. Slow disease progression 5. Prolong survival.
27 TREATMENT OF CHRONIC HF GENERAL APPROACH The first step is to determine the etiology or precipitating factors. Treatment of underlying disorders (eg, hyperthyroidism) may obviate the need for treating HF. Nonpharmacologic interventions 1. Cardiac rehabilitation 2. Restriction of fluid intake (maximum 2 L/day from all sources) and dietary sodium (<2 3 g of sodium/day).
28 TREATMENT OF CHRONIC HF The American College of Cardiology/American Heart Association (ACC/AHA) staging system provides a more comprehensive framework for evaluating, preventing, and treating HF.
 classification of heart failure.")
29 TREATMENT OF CHRONIC HF Staging and New York Heart Association (NYHA) classification of heart failure.
30 TREATMENT OF CHRONIC HF ACC/AHA stage A: These are patients at high risk for developing heart failure. The emphasis is on identifying and modifying risk factors to prevent development of structural heart disease and subsequent HF. Strategies include smoking cessation and control of hypertension, diabetes mellitus, and dyslipidemia. Although treatment must be individualized, angiotensinconverting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) are recommended for HF prevention in patients with multiple vascular risk factors.
31 TREATMENT OF CHRONIC HF ACC/AHA stage B: In these patients with structural heart disease but no HF signs or symptoms, treatment is targeted at minimizing additional injury and preventing or slowing the remodeling process. In addition to treatment measures outlined for stage A, patients with a previous MI should receive both ACE inhibitors (or ARBs in patients intolerant of ACE inhibitors) and β- blockers regardless of the ejection fraction. Patients with reduced ejection fractions should also receive both agents, regardless of whether they have had an MI.
32 TREATMENT OF CHRONIC HF ACC/AHA stage C: These patients have structural heart disease and previous or current HF symptoms. Most should receive the treatments for stages A and B, as well as initiation and titration of a diuretic (if clinical evidence of fluid retention), ACE inhibitor, and β-blocker (if not already receiving a β-blocker for previous MI, left ventricular [LV] dysfunction, or other indication). If diuresis is initiated, and symptoms improve once the patient is euvolemic, long-term monitoring can begin.
33 TREATMENT OF CHRONIC HF If symptoms do not improve, an aldosterone receptor antagonist, ARB (in ACE inhibitor intolerant patients), digoxin, and/or hydralazine/isosorbide dinitrate (ISDN) may be useful with carefully screened patients. Other general measures include moderate sodium restriction, daily weight measurement, immunization against influenza and pneumococcus, modest physical activity, and avoidance of medications that can exacerbate HF.
34 TREATMENT OF CHRONIC HF ACC/AHA stage D: These are patients with refractory HF (ie, symptoms at rest despite maximal medical therapy). They should be considered for specialized therapies, including mechanical circulatory support continuous IV positive inotropic therapy cardiac transplantation, or hospice care (when no additional treatments are appropriate).
35 Diuretics Compensatory mechanisms in HF stimulate excessive sodium and water retention, often leading to systemic and pulmonary congestion. Consequently, diuretic therapy (in addition to sodium restriction) is recommended for all patients with clinical evidence of fluid retention. However, because they do not alter disease progression or prolong survival, they are not mandatory for patients without fluid retention.
36 Diuretics Thiazide diuretics (eg, hydrochlorothiazide) are relatively weak and are used alone infrequently in HF. However, thiazides or the thiazide-like diuretic metolazone can be used in combination with a loop diuretic to promote very effective diuresis. Thiazides may be preferred over loop diuretics in patients with only mild fluid retention and elevated blood pressure (BP) because of their more persistent antihypertensive effects.
37 Diuretics Loop diuretics (furosemide, bumetanide, and torsemide) are usually necessary to restore and maintain euvolemia in HF. In addition to acting in the thick ascending limb of the loop of Henle, they induce a prostaglandin-mediated increase in renal blood flow that contributes to their natriuretic effect. Unlike thiazides, loop diuretics maintain their effectiveness in the presence of impaired renal function, although higher doses may be necessary.

38 Loop Diuretic Use in Heart Failure Diuretics
39 ACEI Angiotensin Converting Enzyme Inhibitors decrease angiotensin II and aldosterone, attenuating many of their deleterious effects, including reducing ventricular remodeling, myocardial fibrosis, myocyte apoptosis, cardiac hypertrophy, norepinephrine release, vasoconstriction, and sodium and water retention. Clinical trials have produced unequivocal evidence that ACE inhibitors improve symptoms, slow disease progression, and decrease mortality in patients with HF and reduced LVEF (stage C). These patients should receive ACE inhibitors unless contraindications are present. ACE inhibitors should also be used to prevent the development of HF in at-risk patients (ie, stages A and B).

40 ACEI ACE Inhibitors Routinely Used for Treatment of Heart Failure
41 β-blockers β-blockers There is overwhelming clinical trial evidence that certain β- blockers slow disease progression, decrease hospitalizations, and reduce mortality in patients with systolic HF. The ACC/AHA guidelines recommend use of β-blockers in all stable patients with HF and a reduced LVEF in the absence of contraindications or a clear history of β-blocker intolerance. Patients should receive a β-blocker even if symptoms are mild or well controlled with ACE inhibitor and diuretic therapy. It is not essential that ACE inhibitor doses be optimized before a β-blocker is started because the addition of a β-blocker is likely to be of greater benefit than an increase in ACE inhibitor dose.
42 β-blockers β-blockers are also recommended for asymptomatic patients with a reduced LVEF (stage B) to decrease the risk of progression to HF. Initiate β-blockers in stable patients who have no or minimal evidence of fluid overload. Because of their negative inotropic effects, start β-blockers in very low doses with slow upward dose titration to avoid symptomatic worsening or acute decompensation. Titrate to target doses when possible to provide maximal survival benefits.
43 Drug Therapies to Consider for Select Patients Drug Therapies to Consider for Select Patients: Angiotensin-II Receptor Blockers The angiotensin II receptor antagonists block the angiotensin II receptor subtype AT1, preventing the deleterious effects of angiotensin II, regardless of its origin. They do not appear to affect bradykinin and are not associated with the side effect of cough that sometimes results from ACE inhibitor induced accumulation of bradykinin. Also, direct blockade of AT1 receptors allows unopposed stimulation of AT2 receptors, causing vasodilation and inhibition of ventricular remodeling.
44 Angiotensin-II Receptor Blockers Combination therapy with an ARB and ACE inhibitor offers a theoretical advantage over either agent alone through more complete blockade of the deleterious effects of angiotensin II. However, clinical trial results indicate that the addition of an ARB to optimal HF therapy (eg, ACE inhibitors, β-blockers, and diuretics) offers marginal benefits at best with increased risk of adverse effects. The addition of an ARB may be considered with patients who remain symptomatic despite receiving optimal conventional therapy.
45 EVALUATION OF THERAPEUTIC OUTCOMES Monitor BP to ensure that symptomatic hypotension does not develop as a result of drug therapy. Body weight is a sensitive marker of fluid loss or retention, and patients should weigh themselves daily and report changes to their healthcare provider so that adjustments can be made in diuretic doses. Symptoms may worsen initially on β-blocker therapy, and it may take weeks to months before patients notice symptomatic improvement. Routine monitoring of serum electrolytes and renal function is mandatory in patients with HF.
46 Aldosterone Antagonists Aldosterone Antagonists Spironolactone and eplerenone block the mineralocorticoid receptor, the target site for aldosterone. In the kidney, aldosterone antagonists inhibit sodium reabsorption and potassium excretion. However, diuretic effects are minimal, suggesting that their therapeutic benefits result from other actions. Based on clinical trial results demonstrating reduced mortality, low-dose aldosterone antagonists may be appropriate for: (1) patients with mild to moderately severe systolic HF who are receiving standard therapy, & (2) those with LV dysfunction and either acute HF or diabetes early after MI.
47 Aldosterone Antagonists Aldosterone antagonists must be used cautiously and with careful monitoring of renal function and potassium concentration. They should be avoided in patients with renal impairment, recent worsening of renal function, high-normal potassium levels, or a history of severe hyperkalemia. Spironolactone also interacts with androgen and progesterone receptors, which may lead to gynecomastia, impotence, and menstrual irregularities in some patients.
48 Aldosterone Antagonists Initial doses should be low (spironolactone 12.5 mg/day; eplerenone 25 mg/day), especially in the elderly and those with diabetes or creatinine clearance less than 50 ml/min. A spironolactone dose of 25 mg/day was used in one major clinical trial. The eplerenone dose should be titrated to the target dose of 50 mg once daily, preferably within 4 weeks as tolerated by the patient.
49 Digoxin Digoxin Although digoxin has positive inotropic effects, its benefits in HF are related to its neurohormonal effects. Digoxin does not improve survival in patients with HF but does provide symptomatic benefits. In patients with chronic systolic HF and supraventricular tachyarrhythmias such as atrial fibrillation, consider digoxin early in therapy to help control ventricular response rate. For patients in normal sinus rhythm, effects on symptom reduction and quality-of life improvement are evident in patients with mild to severe HF.
50 Digoxin Therefore, digoxin should be used together with standard HF therapies (ACE inhibitors, β-blockers, and diuretics) in patients with symptomatic HF to reduce hospitalizations. Adjust doses to achieve plasma digoxin concentration of 0.5 to 1 ng/ml ( nmol/l). Most patients with normal renal function can achieve this level with a dose of mg/day. Patients with decreased renal function, the elderly, or those receiving interacting drugs (eg, amiodarone) should receive mg every other day.
51 Nitrates and Hydralazine Nitrates and Hydralazine Nitrates (eg, ISDN) and hydralazine have complementary hemodynamic actions. Nitrates are primarily venodilators, producing reductions in preload. Hydralazine is a direct arterial vasodilator that reduces systemic vascular resistance (SVR) and increases stroke volume and cardiac output. The combination of nitrates and hydralazine improves the composite endpoint of mortality, hospitalizations for HF, and quality of life in African Americans who receive standard therapy.
52 TREATMENT OF ADHF TREATMENT OF ACUTE DECOMPENSATED HEART FAILURE Goals of Treatment: 1. Relieve congestive symptoms 2. optimize volume status 3. Treat symptoms of low cardiac output 4. minimize risks of drug therapy so the patient can be discharged in a compensated state on oral drug therapy.
53 TREATMENT OF ADHF GENERAL APPROACH Acute decompensated heart failure (ADHF) involves patients with new or worsening signs or symptoms (often resulting from volume overload and/or hypoperfusion) requiring additional medical care, such as emergency department visits and hospitalizations. Hospitalization is recommended or should be considered depending on patient presentation. Admission to an intensive care unit (ICU) may be required if the patient experiences hemodynamic instability requiring frequent monitoring, invasive hemodynamic monitoring, or rapid titration of IV medications with close monitoring.
54 TREATMENT OF ADHF Address and correct reversible or treatable causes of decompensation. Medications that may aggravate HF should be evaluated carefully and discontinued when possible. The first step in managing ADHF is to ascertain that optimal treatment with oral medications has been achieved. If fluid retention is evident, aggressive diuresis, often with IV diuretics, should be accomplished. Standard treatment should be optimized with an ACE inhibitor and β-blocker.
55 TREATMENT OF ADHF β-blockers should generally be continued during hospitalization unless recent dose initiation or up-titration was responsible for decompensation. In such cases, β-blocker therapy may be temporarily withheld or dose-reduced. Most patients may continue to receive digoxin at a low dose targeting a trough serum concentration of ng/ml ( nmol/l). Appropriate management of ADHF is aided by determination of whether the patient has signs and symptoms of fluid overload ( wet HF) or low cardiac output ( dry HF)
56 Dobutamine Positive Inotropic Agents Dobutamine Dobutamine is a β1- and β2-receptor agonist with some α1- agonist effects. The net vascular effect is usually vasodilation. It has a potent inotropic effect without producing a significant change in heart rate. Initial doses of 2.5 to 5 mcg/kg/min can be increased progressively to 20 mcg/kg/min on the basis of clinical and hemodynamic responses. Dobutamine increases cardiac index because of inotropic stimulation, arterial vasodilation, and a variable increase in heart rate.
57 Milrinone Milrinone Milrinone inhibits phosphodiesterase III and produces positive inotropic and arterial and venous vasodilating effects (an inodilator). It has supplanted use of amrinone, which has a higher rate of thrombocytopenia. During IV administration, milrinone increases stroke volume (and cardiac output) with minimal change in heart rate. It also lowers pulmonary capillary wedge pressure (PCWP) by venodilation and is particularly useful in patients with a low cardiac index and elevated LV filling pressure.
58 Milrinone The most notable adverse events are arrhythmia, hypotension, and, rarely, thrombocytopenia. Measure platelet count before and during therapy. Routine use of milrinone (and perhaps other inotropes) should be discouraged because recent studies suggest a higher in-hospital mortality rate than with some other drugs. However, inotropes may be needed with certain patients, such as those with low cardiac output states with organ hypoperfusion and cardiogenic shock. Milrinone may be considered for patients receiving chronic β- blocker therapy because its positive inotropic effect does not involve stimulation of β-receptors.
59 Dopamine Dopamine Dopamine should generally be avoided in ADHF, but its pharmacologic actions may be preferable to dobutamine or milrinone in patients with marked systemic hypotension or cardiogenic shock in the face of elevated ventricular filling pressures, where dopamine in doses greater than 5 mcg/kg/min may be necessary to raise central aortic pressure. Dopamine produces dose-dependent hemodynamic effects because of its relative affinity for α1-, β1-, β2-, and D1- (vascular dopaminergic) receptors.
60 Dopamine Positive inotropic effects mediated primarily by β1-receptors become more prominent with doses of 2 to 5 mcg/kg/min. At doses between 5 and 10 mcg/kg/min, chronotropic and α1- mediated vasoconstricting effects become more prominent.
61 Vasodilators Vasodilators Arterial vasodilators reduce afterload and cause a reflex increase in cardiac output. Venodilators reduce preload by increasing venous capacitance, improving symptoms of pulmonary congestion in patients with high cardiac filling pressures. Mixed vasodilators act on both arterial resistance and venous capacitance vessels, reducing congestive symptoms while increasing cardiac output.
62 Nitroprusside Nitroprusside Sodium nitroprusside is a mixed arteriovenous vasodilator that acts directly on vascular smooth muscle to increase cardiac index and decrease venous pressure. Despite its lack of direct inotropic activity, nitroprusside exerts hemodynamic effects that are qualitatively similar to those of dobutamine and milrinone. However, nitroprusside generally decreases PCWP, SVR, and BP more than those agents do. Hypotension is an important dose-limiting adverse effect of nitroprusside and other vasodilators. Therefore, nitroprusside is primarily used with patients who have a significantly elevated SVR and often requires invasive hemodynamic monitoring.
63 Nitroprusside Nitroprusside is effective in the short-term management of severe HF in a variety of settings (eg, acute MI, valvular regurgitation, after coronary bypass surgery, decompensated chronic HF). Generally, it will not worsen, and may improve, the balance between myocardial oxygen demand and supply. However, an excessive decrease in systemic arterial pressure can decrease coronary perfusion and worsen ischemia.
64 Nitroglycerin Nitroglycerin IV nitroglycerin decreases preload and PCWP because of functional venodilation and mild arterial vasodilation. It is often the preferred agent for preload reduction in ADHF, especially in patients with pulmonary congestion. In higher doses, nitroglycerin displays potent coronary vasodilating properties and beneficial effects on myocardial oxygen demand and supply, making it the vasodilator of choice for patients with severe HF and ischemic heart disease.
65 Nesiritide Nesiritide is a recombinant product that is identical to endogenous BNP secreted by the ventricular myocardium in response to volume overload. Nesiritide mimics the vasodilatory and natriuretic actions of the endogenous peptide, resulting in venous and arterial vasodilation; increased cardiac output; natriuresis and diuresis; and decreased cardiac filling pressures, sympathetic nervous system activity, and renin angiotensin aldosterone system activity.
66 Nesiritide The role of nesiritide in pharmacotherapy of ADHF remains controversial. Compared with nitroglycerin or nitroprusside, it produces marginal improvement in clinical outcomes and is substantially more expensive. Concerns about potential negative effects on renal function and increased morality are also unsettled.
67 Vasopressin Receptor Antagonists The vasopressin receptor antagonists currently available affect one or two arginine vasopressin (AVP; antidiuretic hormone) receptors, V1A or V2. Stimulation of V1A receptors (located in vascular smooth muscle cells and myocardium) results in vasoconstriction, myocyte hypertrophy, coronary vasoconstriction, and positive inotropic effects. V2 receptors are located in renal tubules, where they regulate water reabsorption.
68 Tolvaptan Tolvaptan selectively binds to and inhibits the V2 receptor. It is an oral agent indicated for hypervolemic and euvolemic hyponatremia in patients with syndrome of inappropriate antidiuretic hormone (SIADH), cirrhosis, and HF. Tolvaptan is typically initiated at 15 mg orally daily and then titrated to 30 or 60 mg daily as needed to resolve hyponatremia. It is a substrate of cytochrome P450-3A4 and is contraindicated with potent inhibitors of this enzyme. The most common side effects are dry mouth, thirst, urinary frequency, constipation, and hyperglycemia.
69 Conivaptan Conivaptan nonselectively inhibits both the V1A and V2 receptors. It is an IV agent indicated for hypervolemic and euvolemic hyponatremia due to a variety of causes; however, it is not indicated for hyponatremia associated with HF.
70 MECHANICAL CIRCULATORY SUPPORT MECHANICAL CIRCULATORY SUPPORT The intraaortic balloon pump (IABP) is typically employed in patients with advanced HF who do not respond adequately to drug therapy, such as those with intractable myocardial ischemia or patients in cardiogenic shock. IV vasodilators and inotropic agents are generally used in conjunction with the IABP to maximize hemodynamic and clinical benefits. Ventricular assist devices are surgically implanted and assist, or in some cases replace, the pumping functions of the right and/or left ventricles.
71 MECHANICAL CIRCULATORY SUPPORT They can be used in the short-term (days to several weeks) for temporary stabilization of patients awaiting an intervention to correct underlying cardiac dysfunction. They can also be used long term (several months to years) as a bridge to heart transplantation. SURGICAL THERAPY Orthotopic cardiac transplantation is the best therapeutic option for patients with chronic irreversible New York Heart Association class IV HF, with a 10-year survival of ~50% in well-selected patients.
72 EVALUATION OF THERAPEUTIC OUTCOMES EVALUATION OF THERAPEUTIC OUTCOMES CHRONIC HEART FAILURE Ask patients about the presence and severity of symptoms and how symptoms affect daily activities. Evaluate efficacy of diuretic treatment by disappearance of the signs and symptoms of excess fluid retention. Physical examination should focus on body weight, extent of jugular venous distention, presence of hepatojugular reflux, and presence and severity of pulmonary congestion (rales, dyspnea on exertion, orthopnea, and paroxysmal nocturnal dyspnea) and peripheral edema. Other outcomes are improvement in exercise tolerance and fatigue, decreased nocturia, and a decrease in heart rate.
73 EVALUATION OF THERAPEUTIC OUTCOMES ACUTE DECOMPENSATED HEART FAILURE Initial stabilization requires adequate arterial oxygen saturation, cardiac index, and blood pressure. Functional end-organ perfusion may be assessed by mental status, renal function sufficient to prevent metabolic complications, hepatic function adequate to maintain synthetic and excretory functions, stable heart rate and rhythm, absence of ongoing myocardial ischemia or MI, skeletal muscle and skin blood flow sufficient to prevent ischemic injury, and normal arterial ph ( ) and serum lactate concentration. These goals are most often achieved with a cardiac index greater than 2.2 L/min/m2, mean arterial BP greater than 60 mm Hg, and PCWP 15 mm Hg or greater.
74 EVALUATION OF THERAPEUTIC OUTCOMES Daily monitoring should include weight, strict fluid intake and output measurements, and HF signs/symptoms to assess the efficacy of drug therapy. Monitoring for electrolyte depletion, symptomatic hypotension, and renal dysfunction should be performed frequently. Vital signs should be assessed frequently throughout the day. Discharge from the ICU requires maintenance of the receding parameters in the absence of ongoing IV infusion therapy, mechanical circulatory support, or positive pressure ventilation.


75 Thank You
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Cardiac Drugs: Chapter 9 Worksheet Cardiac Agents. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate.
 Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Pre-discussion questions
 Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Advanced Care for Decompensated Heart Failure
 Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure. Part I: Etiology and Pathophysiology of Heart Failure
 A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure Dr Badri Paudel GMC Part I: Etiology and Pathophysiology of Heart Failure Heart Failure (HF) Definition A complex clinical
A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure Dr Badri Paudel GMC Part I: Etiology and Pathophysiology of Heart Failure Heart Failure (HF) Definition A complex clinical
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Congestive Heart Failure Patient Profile. Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption
 Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 10/5/2015. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center
 10/5/2015. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Incidence. 4.8 million in the United States. 400,000 new cases/year. 20 million patients with asymptomatic LV dysfunction
 Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION
 MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Pathophysiology: Heart Failure. Objectives
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Clinical Medicine Objectives At the conclusion of this seminar, learner will be able to: 1. Define heart failure as a clinical
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Clinical Medicine Objectives At the conclusion of this seminar, learner will be able to: 1. Define heart failure as a clinical
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 2/20/2017. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center
 2/20/2017. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
CLASIFICATION OF ACUTE HEART FAILURE
 CLASIFICATION OF ACUTE HEART FAILURE CLINICAL STATUS HR SBP mmhg CI L/min/m 2 PCWP mmhg Congestion Killip/Forrester Diuresis Hupoperfusion End-organ hypoperfusion I. Acute decompensated CHF +/ Low normal
CLASIFICATION OF ACUTE HEART FAILURE CLINICAL STATUS HR SBP mmhg CI L/min/m 2 PCWP mmhg Congestion Killip/Forrester Diuresis Hupoperfusion End-organ hypoperfusion I. Acute decompensated CHF +/ Low normal
Topic Page: congestive heart failure
 Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Staging and Treating Patients with Heart Failure Henry Green, III, DVM, DACVIM Purdue University West Lafayette, IN
 Staging and Treating Patients with Heart Failure Henry Green, III, DVM, DACVIM Purdue University West Lafayette, IN There are many different diseases that can cause signs of congestive heart failure(chf)
Staging and Treating Patients with Heart Failure Henry Green, III, DVM, DACVIM Purdue University West Lafayette, IN There are many different diseases that can cause signs of congestive heart failure(chf)
Heart Failure Pharmacotherapy An Update
 Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
CKD Satellite Symposium
 CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
The Art and Science of Diuretic therapy
 The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
Improving Transition of Care in Congestive Heart Failure. Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare
 Improving Transition of Care in Congestive Heart Failure Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare Heart Failure Fastest growing clinical cardiac disease in the United
Improving Transition of Care in Congestive Heart Failure Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare Heart Failure Fastest growing clinical cardiac disease in the United
Diastolic Heart Failure. Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012
 Diastolic Heart Failure Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012 Disclosures Have spoken for Merck, Sharpe and Dohme Sat on a physician advisory
Diastolic Heart Failure Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012 Disclosures Have spoken for Merck, Sharpe and Dohme Sat on a physician advisory
CONGESTIVE CARDIAC FAILURE. Dr.T.Rajathilagam, M.D., S.R.M. Medical College
 CONGESTIVE CARDIAC FAILURE Dr.T.Rajathilagam, M.D., S.R.M. Medical College HEART FUNCTIONS Your heart is an amazing powerhouse that pumps and circulates 5 or 6 gallons of blood each minute through your
CONGESTIVE CARDIAC FAILURE Dr.T.Rajathilagam, M.D., S.R.M. Medical College HEART FUNCTIONS Your heart is an amazing powerhouse that pumps and circulates 5 or 6 gallons of blood each minute through your
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
CHF is a clinical syndrome in which heart failure is accompanied by symptoms and signs of pulmonary and/or peripheral congestion
 Congestive Heart Failure Lokesh Tejwani, MD Heart Failure A patho-physiological state in which abnormality of cardiac function is responsible for failure of the heart to pump blood at a rate commensurate
Congestive Heart Failure Lokesh Tejwani, MD Heart Failure A patho-physiological state in which abnormality of cardiac function is responsible for failure of the heart to pump blood at a rate commensurate
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure
 Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure J. Herbert Patterson, Pharm.D., FCCP One of Four Continuing Education Programs in the Series, Acute Decompensated
Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure J. Herbert Patterson, Pharm.D., FCCP One of Four Continuing Education Programs in the Series, Acute Decompensated
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure
 Journal of Cardiac Failure Vol. 12 No. 1 2006 Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure Overview Acute decompensated heart failure (ADHF) has emerged as a
Journal of Cardiac Failure Vol. 12 No. 1 2006 Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure Overview Acute decompensated heart failure (ADHF) has emerged as a
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Our Readers Have An Attitude Toward Living
 February 2007 America s Wellness Guide Number 43 FREE at Doctor s Offices, Hospitals, Clinics and Kroger Pharmacies in the Midsouth COVER Standard of Care for Heart Failure Management By Arie Szatkowski,
February 2007 America s Wellness Guide Number 43 FREE at Doctor s Offices, Hospitals, Clinics and Kroger Pharmacies in the Midsouth COVER Standard of Care for Heart Failure Management By Arie Szatkowski,
Right-Sided Congestive Heart Failure Basics
 Right-Sided Congestive Heart Failure Basics OVERVIEW Failure of the right side of the heart to pump blood at a sufficient rate to meet the needs of the body or to prevent blood from pooling within the
Right-Sided Congestive Heart Failure Basics OVERVIEW Failure of the right side of the heart to pump blood at a sufficient rate to meet the needs of the body or to prevent blood from pooling within the
Drug Therapy of Heart Failure. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014
 Drug Therapy of Heart Failure Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Drug Therapy of Heart Failure Definition of Heart Failure Causes Classifications
Drug Therapy of Heart Failure Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Drug Therapy of Heart Failure Definition of Heart Failure Causes Classifications
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Means failure of heart to pump enough blood to satisfy the need of the body.
 Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Pathophysiology: Heart Failure. Objectives
 Pathophysiology: Heart Failure Mat Maurer, MD Associate Professor of Clinical Medicine Objectives At the conclusion of this seminar, learners will be able to: 1. Define heart failure as a clinical syndrome
Pathophysiology: Heart Failure Mat Maurer, MD Associate Professor of Clinical Medicine Objectives At the conclusion of this seminar, learners will be able to: 1. Define heart failure as a clinical syndrome
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Innovation therapy in Heart Failure
 Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
The Treatment Targets in Acute Decompensated Heart Failure
 SUCCESS WITH HEART FAILURE The Treatment Targets in Acute Decompensated Heart Failure Gregg C. Fonarow, MD The Ahmanson-UCLA Cardiomyopathy Center, Division of Cardiology, UCLA School of Medicine, Los
SUCCESS WITH HEART FAILURE The Treatment Targets in Acute Decompensated Heart Failure Gregg C. Fonarow, MD The Ahmanson-UCLA Cardiomyopathy Center, Division of Cardiology, UCLA School of Medicine, Los
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Updates in Diagnosis & Management of CHF
 Updates in Diagnosis & Management of CHF N. Goldberg, DO April 30, 2011 CHF CHF is reaching an epidemic level in U.S. and continues to worsen over time Reasons are: HTN Dm with sedentary lifestyle and
Updates in Diagnosis & Management of CHF N. Goldberg, DO April 30, 2011 CHF CHF is reaching an epidemic level in U.S. and continues to worsen over time Reasons are: HTN Dm with sedentary lifestyle and
Objectives. Outline 4/3/2014
 Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Congestive Heart Failure 2015
 Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Angina pectoris due to coronary atherosclerosis : Atenolol is indicated for the long term management of patients with angina pectoris.
 Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for