The Art and Science of Diuretic therapy
|
|
|
- Wilfred Bishop
- 5 years ago
- Views:
Transcription
1 The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC

2 Heart failure: fluid overload

3 Diuretics in the context of HF therapy
4 Clinical symptoms of fluid retention Oedema (preferably legs: grading ankle/calf/thigh) Pulmonary rales Raised jugular venous pressure Hepatomegaly/hepatojugular reflux Pleural effusion Ascites Additional diagnostic workup to identify fluid retention: X- ray, echocardiography, abdominal ultrasound Camm AJ, et al. The ESC Textbook of Cardiovascular Medicine. 2nd ed. 2009;851-8.
5 Goal of diuretic The goal of diuretic treatment in heart failure is not simply to increase urinary excretion of sodium chloride, but : 1- Achieve negative short-term sodium chloride and water balance (here termed decongestion). 2- In the longer term, to reduce extracellular fluid volume.

6 Diuretics in :Impact on morbidity?

7 Neuroendocrine effects of diuretics in CHF
8 Loop diuretic: good Block NKC absorption in ascending limb of loop of Helene. Block NKC in the vascular smooth muscle cause VD. Inhibit tubule- glomerular feedback, so, this effect lead to increase in glomerular filtration rate. Increase the level of prostaglandin in the proximal tubules increase GFR.
9 Bad Block NKC in the macula densa which stimulate secretion of renin ( bad ). Ceiling, need he drug to be above the naturesis threshold for longer time. Post diuretic sodium retention : there low sodium excretion in between the doses. Braking phenomenon: diuretic response is reduced with subsequent does of diuretic dose, due to activation of RAAS, activation of sympathetic, nephron remolding, depletion of extracellular volume. Nephron remolding: stimulation of distal nephron to augment sodium reabsorption.
10 Pharmacologic effect Ceiling. Post-diuretic sodium retention. Braking phenomenon. Nephron Remodeling. Rebound.
11 Diuretics have complex effects on renal and systemic hemodynamics, which are influenced by the dose and route of administration, concomitant disease and treatment, and longterm use.

12 Diuretic effects on RAAS
13 Initiation of diuretic therapy Diuretics are recommended in patients with HF and clinical signs or symptoms of congestion. Check renal function and serum electrolytes. Start with thiazide, but most patients will receive loop diuretics due to higher efficacy to induce diuresis and natriuresis. Salt restriction is required to ensure diuretic effect. Self adjustment of diuretic dose can be based on daily weight measurements on HF outpatients. Basal regular drug intake should be pursued to avoid severe fluctuations in fluid retention due to over-compensation mechanisms.
14 Diuretic monitoring: Regular drug intake to maintain efficacy (to prevent rebound and increased fluid retention in drug-free intervals). Minimum dose to achieve diuresis and manage congestion should be used to minimize adverse effects Side effects from multi-drug therapy (hyperkalaemia exacerbated by additional ACE-I therapy) Regular (daily) weight measurement to ensure stable fluid balance

15 Potential problems with diuretic therapy

16 Differential diagnosis: hyponatraemia in heart failure
17 Diuretic resistance Defined as the failure of diuretics to achieve decongestion, which is manifest by a low urine sodium concentration, despite the use of maximal recommended doses. Continuous infusion of diuretic therapy is frequently used in such patients.
18 When diuretics do not achieve decongestion despite the use of maximal doses, the patient is typically said to be diuretic resistant. Single doses of furosemide (250 mg) are often considered to be maximal, although recommendations vary.
19 Diuretic-resistant patients are at high risk for illness and death, and this scenario, which is frequently associated with kidney dysfunction, is often termed the cardiorenal syndrome.
20 Causes of Diuretic Resistance. Inadequate dose of diuretic Non adherence.( Not taking drug. High sodium intake ). Pharmacokinetic factors 1- Slow absorption of diuretic because of gut edema 2- Impaired secretion of diuretic into the tubule lumen 1- Chronic kidney disease 2- Aging 3- Drugs ( NSAID, Probenecid)
21 Hypoproteinemia Hypotension Nephrotic syndrome Antinatriuretic drugs (NSAID, Antihypertensive agents) Low renal blood flow Nephron remodeling Neurohormonal activation

22 Diuretics in severe congestion?

23 I.V. diuretics in acute HF:

24 Management of diuretic resistance
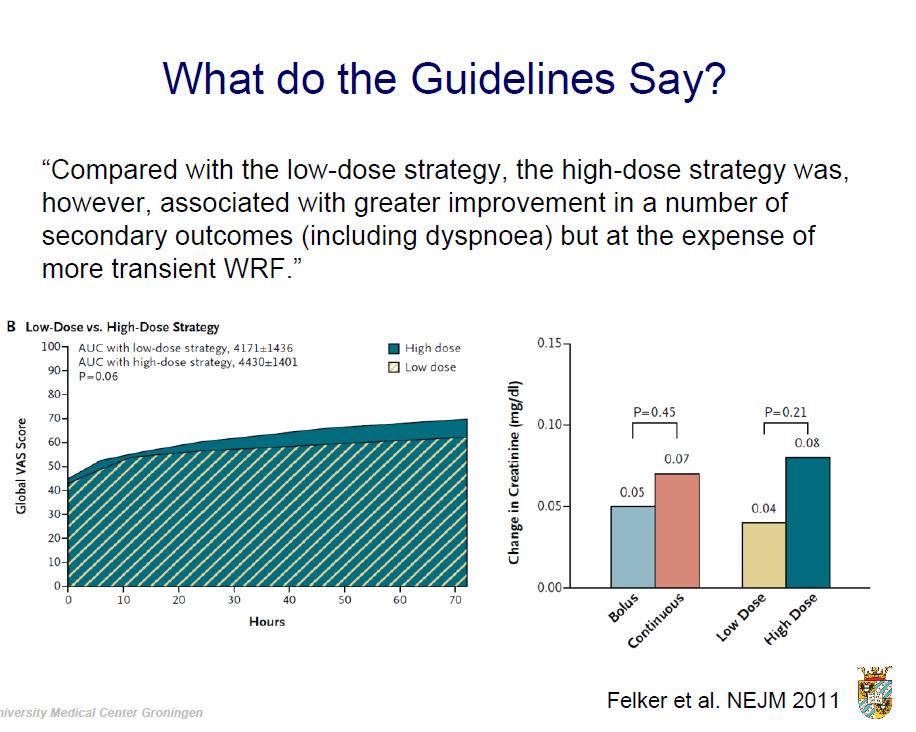
25 DOSE-HF (n=308) 25 High dose associated with greater diuresis but higher creatinine COMPOSITE END POINT* *Global assessment of symptoms (VAS), change in serum creatinine Felker et al NEJM 2011;364; :23:52 AM
26
27
28 CARdiorenal REScue Study in Acute Decompensated Heart Failure (CARESS-HF) Prospective, randomized trial Primary endpoint Change in scr and weight together as a bivariate endpoint assessed at 96 hrs post enrollment Secondary Endpoint PE assessed at days 1-3 and 7 days Treatment failure, weight and fluid loss, clinical decongestion, peak scr, change in electrolytes, LOS, biomarkers, change in diuretic doses all at various time points
29 Diuretic regimen in CARESS HF Diuretic Grid Suggested Dose Current Dose Daily Loop Dose Thiazide A <80 mg 40 mg IV bolus + 5 mg/h None B mg 80 mg IV bolus + 10 mg/h C mg 80 mg IV bolus + 20 mg/h D >240 mg 80 mg IV bolus + 30 mg/h 5 mg metolazone once daily 5 mg metolazone twice daily 5 mg metolazone twice daily
30 Diuretic regimen in CARESS HF Daily assessment of Urine output (UO) UO >5 L/d Reduce current diuretic regimen if desired UO 3 5 L/d Continue current diuretic regimen UO <3 L/d Advance to next After 48 Hrs Consider dopamine or dobutamine at 2 mg/kg/h if SBP <110 mm Hg and EF < 40% or RV systolic dysfunction. Consider nitroglycerin or nesiritide if SBP >120 mm Hg (any EF) and severe symptoms H Consider hemodynamic guided IV therapy, LVAD, dialysis, or ultrafiltration crossover
31 Changes in Serum Creatinine and Wt at 96 H (Bivariate Response)
32 Change in serum creatinine

33 Body weight change
34 Conclusion The use of a stepped pharmacologictherapy algorithm was superior to a strategy of ultrafiltration for the preservation of renal function at 96 hours, with a similar amount of weight loss with the two approaches. Ultrafiltration was associated with a higher rate of adverse events

35 Torasemide on outcome in HF The TORasemide In Congestive heart failure (TORIC) study

36 MRA improve outcome in HF: The RALES trial (NYHA class III IV)

37 MRA improve outcome in HF: The EPHESUS and EMPHASIS trial
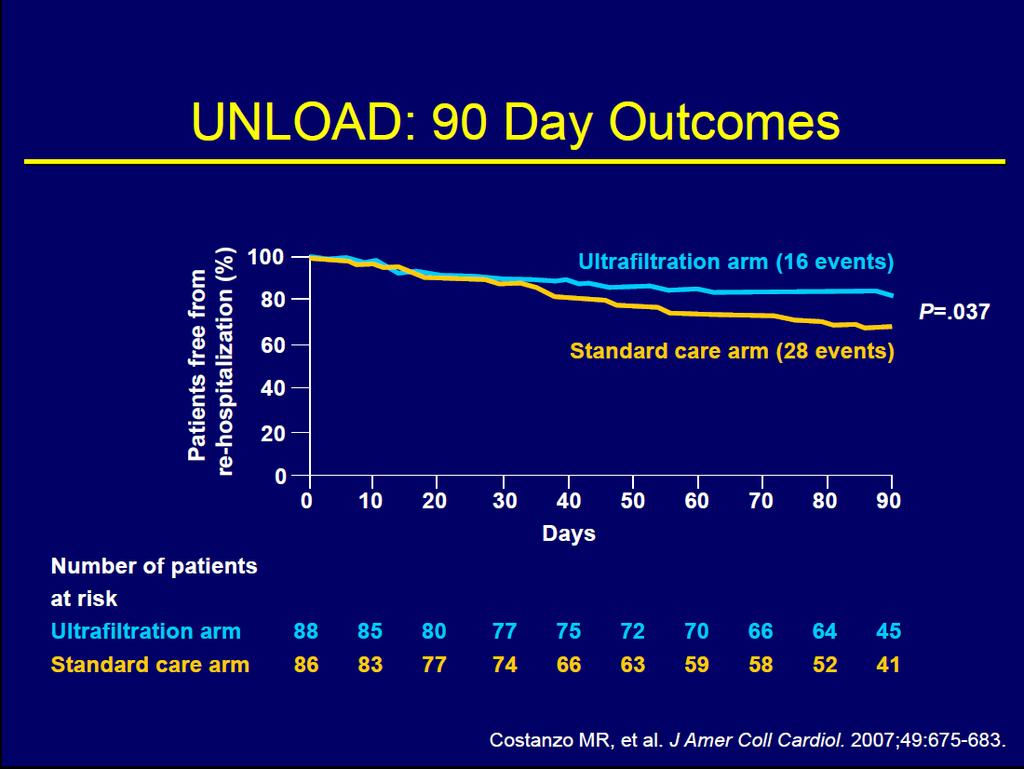
38 The UNLOAD Study The UNLOAD :Study 200 patients (100 each arm) randomized, multi-center study comparing ultrafiltration versus standard care for acutely decompensated patients Superior salt & water removal/weight loss At 48 hours, ultrafiltration demonstrated 38% greater weight loss 28% greater net fluid loss Improved Dyspnea score At 90 days, reduced readmissions 50% reduction in re-hospitalization episodes 63% reduction in total re-hospitalized days 52% reduction in unscheduled clinic/er visits Costanzo MR et al. J Am Coll Cardiol. 2007;49:
39
40 Tolvaptan The oral vasopressin-2 receptor antagonist tolvaptan inhibits the action of antidiuretic hormone and increases excretion of free water(aquaresis).
41 Outcome Study with Tolvaptan (EVEREST), which evaluated patients who were hospitalized for heart failure (with or without hyponatremia), did not show superiority of tolvaptan over placebo with respect to long-term clinical outcomes, although potentially beneficial effects with respect to volume status and symptoms were observed in the study group.
42 Dopamine Low renal blood flow contributes to sodium retention in ADHF by limiting sodium filtration, increasing sodium reabsorption, and reducing renal delivery of diuretics to the proximal tubule. Since dopamine increases renal blood flow and excretion of urinary sodium at low doses, it might therefore augment natriuresis. Similar, considerations apply to natriuretic peptides.
43 ROSE-AHF trial, 360 patients who were hospitalized for ADHF with impaired renal function were randomly assigned to furosemide plus dopamine infusion (at a dose of 2 μg per kilogram of body weight per minute), nesiritide (at a dose of μg per kilogram per minute), or placebo. Neither active drug affected the primary end points of urine volume or change in cystatin C level during the ensuing 72 hours.
44 Conclusion Skillful use of diuretic therapy remains fundamental to the successful management of heart failure. Understanding the physiological effects as well as the pharmacokinetic and pharmacodynamic properties of these drugs is key for safe and effective use.

45

46 I.V. diuretics in acute heart failure

47 Commonly used diuretics and dosages
Pivotal Role of Renal Function in Acute Heart failure
 Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
The Cardiorenal Syndrome in Heart Failure
 The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
Overcoming the Cardiorenal Syndrome
 Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
ROSE-AHF and Beyond. Gerasimos Filippatos, FESC, FHFA President Heart Failure Association
 ROSE-AHF and Beyond Gerasimos Filippatos, FESC, FHFA President Heart Failure Association From: Braunwald s Heart Disease. 9th ed. Philadelphia, Elsevier, 2011 Determinants and forms of worsening renal
ROSE-AHF and Beyond Gerasimos Filippatos, FESC, FHFA President Heart Failure Association From: Braunwald s Heart Disease. 9th ed. Philadelphia, Elsevier, 2011 Determinants and forms of worsening renal
Hyponatremia in Heart Failure: why it is important and what should we do about it?
 Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Management of Acute Heart Failure
 Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Cardio-Renal Syndrome in Acute Heart Failure:
 Cardio-Renal Syndrome in Acute Heart Failure: Target for Therapy Marvin A. Konstam, M.D. Research support and/or consulting relevant to this lecture: Merck, Otsuka, Johnson & Johnson; Amgen; Cardiokine
Cardio-Renal Syndrome in Acute Heart Failure: Target for Therapy Marvin A. Konstam, M.D. Research support and/or consulting relevant to this lecture: Merck, Otsuka, Johnson & Johnson; Amgen; Cardiokine
Cardiorenal Syndrome: What the Clinician Needs to Know. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Cardiorenal Syndrome: What the Clinician Needs to Know William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Renal Hemodynamics in Heart Failure Glomerular
Cardiorenal Syndrome: What the Clinician Needs to Know William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Renal Hemodynamics in Heart Failure Glomerular
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Biomarkers for optimal management of heart failure. Cardiorenal syndrome. Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland
 Biomarkers for optimal management of heart failure Cardiorenal syndrome Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland Presenter Disclosure Information V-P Harjola The following
Biomarkers for optimal management of heart failure Cardiorenal syndrome Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland Presenter Disclosure Information V-P Harjola The following
Heart Failure and Renal Failure. Gerasimos Filippatos, MD, FESC, FHFA President HFA
 Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
THE KIDNEY IN HYPOTENSIVE STATES. Benita S. Padilla, M.D.
 THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
Cardiorenal syndrome. Sofie Gevaert. Ghent University Hospital, Belgium
 Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial
: A Randomized Clinical Trial") Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial Horng H Chen MD on behalf of the NHLBI Heart Failure Clinical Research Network Background AHF + Renal
Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial Horng H Chen MD on behalf of the NHLBI Heart Failure Clinical Research Network Background AHF + Renal
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Cardiorenal Syndrome
 SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
Defining and Managing the Cardiorenal Syndrome in Acute Decompensated Heart Failure. Barry M. Massie Professor of Medicine UCSF
 Defining and Managing the Cardiorenal Syndrome in Acute Decompensated Heart Failure Barry M. Massie Professor of Medicine UCSF DISCLOSURES Consulting fees: Merck-Novacardia Novartis Bristol Myers Squibb
Defining and Managing the Cardiorenal Syndrome in Acute Decompensated Heart Failure Barry M. Massie Professor of Medicine UCSF DISCLOSURES Consulting fees: Merck-Novacardia Novartis Bristol Myers Squibb
Case Report Triple Diuretics and Aquaretic Strategy for Acute Decompensated Heart Failure due to Volume Overload
 Case Reports in Cardiology Volume 2013, Article ID 750794, 4 pages http://dx.doi.org/10.1155/2013/750794 Case Report Triple Diuretics and Aquaretic Strategy for Acute Decompensated Heart Failure due to
Case Reports in Cardiology Volume 2013, Article ID 750794, 4 pages http://dx.doi.org/10.1155/2013/750794 Case Report Triple Diuretics and Aquaretic Strategy for Acute Decompensated Heart Failure due to
Objectives 6/14/2016. Cardiorenal Syndrome: Critical Link Between Heart and Kidney
 Cardiorenal Syndrome: Critical Link Between Heart and Kidney Chris M. Bell, ACNP Cardiology Associates of North Mississippi Objectives Review the 5 Subtypes of the Cardiorenal Syndrome (CRS) Discuss the
Cardiorenal Syndrome: Critical Link Between Heart and Kidney Chris M. Bell, ACNP Cardiology Associates of North Mississippi Objectives Review the 5 Subtypes of the Cardiorenal Syndrome (CRS) Discuss the
Cardiorenal Syndrome
 Cardiorenal Syndrome Peenida Skulratanasak, M.D. Division of Nephrology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University Definition of Cardiorenal syndrome (CRS) Structural
Cardiorenal Syndrome Peenida Skulratanasak, M.D. Division of Nephrology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University Definition of Cardiorenal syndrome (CRS) Structural
Heart Failure and Renal Disease Cardiorenal Syndrome
 Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Recognizing and Treating Patients with the Cardio-Renal Syndrome
 Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure
 Journal of Cardiac Failure Vol. 12 No. 1 2006 Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure Overview Acute decompensated heart failure (ADHF) has emerged as a
Journal of Cardiac Failure Vol. 12 No. 1 2006 Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure Overview Acute decompensated heart failure (ADHF) has emerged as a
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
State of the Art: acute heart failure Is it just congestion?
 ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Biomarkers, the Kidney and the Heart: Acute Kidney Injury
 Biomarkers, the Kidney and the Heart: Acute Kidney Injury 12th Annual Conference on Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices San Diego May 13, 2016 Ravindra
Biomarkers, the Kidney and the Heart: Acute Kidney Injury 12th Annual Conference on Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices San Diego May 13, 2016 Ravindra
Practical Points in Cardiorenal Syndrome
 Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Heart failure: what should be changed? Prof. Gerasimos Filippatos Attikon University Hospital
 Heart failure: what should be changed? Prof. Gerasimos Filippatos Attikon University Hospital Disclosures Chair or Committee Member of trials or registries sponsored by Novartis, Bayer, Cardiorentis, Servier
Heart failure: what should be changed? Prof. Gerasimos Filippatos Attikon University Hospital Disclosures Chair or Committee Member of trials or registries sponsored by Novartis, Bayer, Cardiorentis, Servier
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
State-of-the-Art: Treatment of Renal Dysfunction in Heart Failure. W. H. Wilson Tang, MD Cleveland Clinic, U.S.A.
 State-of-the-Art: Treatment of Renal Dysfunction in Heart Failure W. H. Wilson Tang, MD Cleveland Clinic, U.S.A. Heart Failure Exacerbates Renal Insufficiency ADHERE Registry: Prevalence of CKD by egfr
State-of-the-Art: Treatment of Renal Dysfunction in Heart Failure W. H. Wilson Tang, MD Cleveland Clinic, U.S.A. Heart Failure Exacerbates Renal Insufficiency ADHERE Registry: Prevalence of CKD by egfr
Nesiritide: Harmful or Harmless?
 Nesiritide: Harmful or Harmless? Michael P. Dorsch, Pharm.D., and Jo Ellen Rodgers, Pharm.D. Nesiritide is the recombinant form of human B-type (brain) natriuretic peptide (BNP), and its amino acid sequence
Nesiritide: Harmful or Harmless? Michael P. Dorsch, Pharm.D., and Jo Ellen Rodgers, Pharm.D. Nesiritide is the recombinant form of human B-type (brain) natriuretic peptide (BNP), and its amino acid sequence
Journal Watch. January. REVIEW: Diuretic Resistance in heart failure HEART FAILURE AND TRANSPLANTATION
 Journal Watch January 2018 Lavanya Bellumkonda, MD, PhD Yale University School of Medicine New Haven, Connecticut, USA lavanya.bellumkonda@yale.edu Josephine Chou, MD Yale University School of Medicine
Journal Watch January 2018 Lavanya Bellumkonda, MD, PhD Yale University School of Medicine New Haven, Connecticut, USA lavanya.bellumkonda@yale.edu Josephine Chou, MD Yale University School of Medicine
Volume Control in. Wafaa El Aroussy,MD Prof of Cardiology Kasr El Aini Faculty of Medicine September 29 th, 2011
 Volume Control in Heart Failure Wafaa El Aroussy,MD Prof of Cardiology Kasr El Aini Faculty of Medicine September 29 th, 2011 What is Heart Failure Heart failure is a multisystem disorder which is characterised
Volume Control in Heart Failure Wafaa El Aroussy,MD Prof of Cardiology Kasr El Aini Faculty of Medicine September 29 th, 2011 What is Heart Failure Heart failure is a multisystem disorder which is characterised
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
A. Study Purpose and Rationale Background
 A. Study Purpose and Rationale Background Congestive heart failure (CHF) affects roughly 6 million people in the United States with incidence rates rising steadily. Of even more concern, however, is the
A. Study Purpose and Rationale Background Congestive heart failure (CHF) affects roughly 6 million people in the United States with incidence rates rising steadily. Of even more concern, however, is the
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
A patient with acute heart failure and renal impairment ACCA Masterclass 2017
 A patient with acute heart failure and renal impairment Dr Sofie Gevaert Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009:
A patient with acute heart failure and renal impairment Dr Sofie Gevaert Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009:
G. Allen Bryant III, M.D.,F.A.S.N Director Medical Subspecialties LMH Co-Director Renal Services LMH LMPC Chairman of Board
 G. Allen Bryant III, M.D.,F.A.S.N Director Medical Subspecialties LMH Co-Director Renal Services LMH LMPC Chairman of Board Presentation Outline/Goals Convince you that having combined LV dysfunction and
G. Allen Bryant III, M.D.,F.A.S.N Director Medical Subspecialties LMH Co-Director Renal Services LMH LMPC Chairman of Board Presentation Outline/Goals Convince you that having combined LV dysfunction and
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
3/30/2010 ACUTE DECOMPENSATED HEART FAILURE. Robert E. Hobbs, MD CLEVELAND CLINIC. Year Patients in US (millions)
") ACUTE DECOMPENSATED HEART FAILURE Robert E. Hobbs, MD CLEVELAND CLINIC EPIDEMIOLOGY OF HEART FAILURE Patients in US (millions) 10.0 10 8 550,000 new cases annually 6 4 5 million Americans have HF; likely
ACUTE DECOMPENSATED HEART FAILURE Robert E. Hobbs, MD CLEVELAND CLINIC EPIDEMIOLOGY OF HEART FAILURE Patients in US (millions) 10.0 10 8 550,000 new cases annually 6 4 5 million Americans have HF; likely
Advanced Care for Decompensated Heart Failure
 Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
University of Groningen. Diuretic response and renal function in heart failure ter Maaten, Jozine Magdalena
 University of Groningen Diuretic response and renal function in heart failure ter Maaten, Jozine Magdalena IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Diuretic response and renal function in heart failure ter Maaten, Jozine Magdalena IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
Cardio-renal syndrome.
 Review Article Cardio-renal syndrome. http://www.alliedacademies.org/archives-of-general-internal-medicine/ ISSN: 2591-7951 Dhiraj Kumar*, Abhijeet Yelale, Girish Sabnis, Hetan Shah, Charan Lanjewar, Prafulla
Review Article Cardio-renal syndrome. http://www.alliedacademies.org/archives-of-general-internal-medicine/ ISSN: 2591-7951 Dhiraj Kumar*, Abhijeet Yelale, Girish Sabnis, Hetan Shah, Charan Lanjewar, Prafulla
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Blood Pressure Regulation 2. Faisal I. Mohammed, MD,PhD
 Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2. Faisal I. Mohammed, MD,PhD
 Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
Using Lung Ultrasound to Diagnose and Manage Acute Heart Failure
 Using Lung Ultrasound to Diagnose and Manage Acute Heart Failure Jennifer Martindale, MD Assistant Professor Department of Emergency Medicine SUNY Downstate/Kings County Hospital Brooklyn, NY What is acute
Using Lung Ultrasound to Diagnose and Manage Acute Heart Failure Jennifer Martindale, MD Assistant Professor Department of Emergency Medicine SUNY Downstate/Kings County Hospital Brooklyn, NY What is acute
Osteopathic Physicians and Surgeons of
 Diuretic Resistance Osteopathic Physicians and Surgeons of Oregon Annual Conference September 14-16, 2018 Diuretic Resistance: When What You are Doing Stops Working Mark D. Baldwin D.O. FACOI Chair, Department
Diuretic Resistance Osteopathic Physicians and Surgeons of Oregon Annual Conference September 14-16, 2018 Diuretic Resistance: When What You are Doing Stops Working Mark D. Baldwin D.O. FACOI Chair, Department
DIURETICS. Assoc. Prof. Bilgen Başgut
 DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
Case Presentation. This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Furosemide: Properties, Alternatives, and the Medication Approval Process. Heather Brown EMS 209-Advanced Pharmacology Don Knox
 Furosemide: Properties, Alternatives, and the Medication Approval Process Heather Brown EMS 209-Advanced Pharmacology Don Knox Pre-hospital treatment of critical patients is a key factor in determining
Furosemide: Properties, Alternatives, and the Medication Approval Process Heather Brown EMS 209-Advanced Pharmacology Don Knox Pre-hospital treatment of critical patients is a key factor in determining
Heart-failure or Kidney Failure?
 Heart-failure or Kidney Failure? Dr Ajith James Consultant Nephrologist Barts Health and BHRUT Mr AR 65 yrs Case Type 2 DM, IHD-MI 1998, 2003. PCI x 3. CABG 2008, HT CCF with LVEF 30% 2014. NYHA Class
Heart-failure or Kidney Failure? Dr Ajith James Consultant Nephrologist Barts Health and BHRUT Mr AR 65 yrs Case Type 2 DM, IHD-MI 1998, 2003. PCI x 3. CABG 2008, HT CCF with LVEF 30% 2014. NYHA Class
YOU will treat patients with heart MANAGING HEART FAILURE: 11/4/2014 ALL DIURETICS ARE NOT CREATED EQUAL. failure.
 MANAGING HEART FAILURE: ALL DIURETICS ARE NOT CREATED EQUAL SUZANNE FRAZIER MS, CRNP, NP C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY MEDICAL CENTER Impact of Heart Failure In
MANAGING HEART FAILURE: ALL DIURETICS ARE NOT CREATED EQUAL SUZANNE FRAZIER MS, CRNP, NP C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY MEDICAL CENTER Impact of Heart Failure In
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes?
 Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Monitoring of Renal Function in Heart Failure
 Monitoring of Renal Function in Heart Failure Adriaan A. Voors, cardiologist The Netherlands Disclosures AAV received consultancy fees and/or research grants from: Alere, Bayer, Cardio3Biosciences, Celladon,
Monitoring of Renal Function in Heart Failure Adriaan A. Voors, cardiologist The Netherlands Disclosures AAV received consultancy fees and/or research grants from: Alere, Bayer, Cardio3Biosciences, Celladon,
Tiny Jaarsma Linköping University No conflict of interest
 Detrimental effects of sodium in heart failure - Tiny Jaarsma Linköping University No conflict of interest Sodium restriction in Heart Failure Why? Prevention of heart failure Blood pressure treatment
Detrimental effects of sodium in heart failure - Tiny Jaarsma Linköping University No conflict of interest Sodium restriction in Heart Failure Why? Prevention of heart failure Blood pressure treatment
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1
 Lecture 18: Endocrine control of renal function. p. 1") BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
Clinical efficacy of ultrafiltration in the treatment of acute decompensated heart failure with diuretic resistance.
 Biomedical Research 2017; 28 (14): 6155-6159 ISSN 0970-938X www.biomedres.info Clinical efficacy of ultrafiltration in the of acute decompensated heart failure with diuretic resistance. Jian Zhang, Qi
Biomedical Research 2017; 28 (14): 6155-6159 ISSN 0970-938X www.biomedres.info Clinical efficacy of ultrafiltration in the of acute decompensated heart failure with diuretic resistance. Jian Zhang, Qi
014 Chapter 14 Created: 9:25:14 PM CST
 014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology
 Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Ultrafiltration in Decompensated Heart Failure. Description
 Subject: Ultrafiltration in Decompensated Heart Failure Page: 1 of 9 Last Review Status/Date: September 2014 Ultrafiltration in Decompensated Heart Failure Description Ultrafiltration is a technique being
Subject: Ultrafiltration in Decompensated Heart Failure Page: 1 of 9 Last Review Status/Date: September 2014 Ultrafiltration in Decompensated Heart Failure Description Ultrafiltration is a technique being
Management of Advanced Systolic Heart Failure. Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University
 Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
Beneficial Role of Tolvaptan in the Control of Body Fluids Without Reductions in Residual Renal Function in Patients Undergoing Peritoneal Dialysis
 Advances in Peritoneal Dialysis, Vol. 29, 2013 Takefumi Mori, 1,2,3 Ikuko Oba, 1 Kenji Koizumi, 1 Mayumi Kodama, 1 Miwako Shimanuki, 1 Mizuho Tanno, 1 Makiko Chida, 1 Mai Saito, 1 Hideyasu Kiyomoto, 1
Advances in Peritoneal Dialysis, Vol. 29, 2013 Takefumi Mori, 1,2,3 Ikuko Oba, 1 Kenji Koizumi, 1 Mayumi Kodama, 1 Miwako Shimanuki, 1 Mizuho Tanno, 1 Makiko Chida, 1 Mai Saito, 1 Hideyasu Kiyomoto, 1
CASE STUDIES IN ADVANCED HEART FAILURE
 CASE STUDIES IN ADVANCED HEART FAILURE Navin Rajagopalan, MD Director, Congestive Heart Failure Medical Director, Cardiac Transplantation Gill Heart Institute, Cardiovascular Medicine DISCLOSURES NOTHING
CASE STUDIES IN ADVANCED HEART FAILURE Navin Rajagopalan, MD Director, Congestive Heart Failure Medical Director, Cardiac Transplantation Gill Heart Institute, Cardiovascular Medicine DISCLOSURES NOTHING
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion.
 The Kidney Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion. The kidney has 6 roles in the maintenance of homeostasis. 6 Main Functions 1. Ion Balance
The Kidney Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion. The kidney has 6 roles in the maintenance of homeostasis. 6 Main Functions 1. Ion Balance
Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment
 ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
** TMP mean page 340 in 12 th edition. Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2:
 QUESTION Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2: Urine flow rate = 1 ml/min Urine inulin concentration = 100 mg/ml Plasma inulin concentration = 2 mg/ml
QUESTION Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2: Urine flow rate = 1 ml/min Urine inulin concentration = 100 mg/ml Plasma inulin concentration = 2 mg/ml
Heart Failure with Reduced EF. Dino Recchia, MD, FACC, FHFSA
 Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Pearls in Acute Heart Failure Management
 Pearls in Acute Heart Failure Management Best Practices Juan M. Aranda Jr., M.D. Professor of Medicine Medical Director of Heart Failure/ Transplant Program University of Florida College of Medicine Disclosures:
Pearls in Acute Heart Failure Management Best Practices Juan M. Aranda Jr., M.D. Professor of Medicine Medical Director of Heart Failure/ Transplant Program University of Florida College of Medicine Disclosures:
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Counter-Current System Regulation of Renal Functions
 Counter-Current System Regulation of Renal Functions Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most
Counter-Current System Regulation of Renal Functions Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most
How to define the target population?
 Heart Failure 2011 22-24 May. Gothenburg, Sweden Mortality or morbidity as target in acute heart failure trials How to define the target population? Marco Metra, Brescia The Burden of Acute HF Acute HF
Heart Failure 2011 22-24 May. Gothenburg, Sweden Mortality or morbidity as target in acute heart failure trials How to define the target population? Marco Metra, Brescia The Burden of Acute HF Acute HF
CLASIFICATION OF ACUTE HEART FAILURE
 CLASIFICATION OF ACUTE HEART FAILURE CLINICAL STATUS HR SBP mmhg CI L/min/m 2 PCWP mmhg Congestion Killip/Forrester Diuresis Hupoperfusion End-organ hypoperfusion I. Acute decompensated CHF +/ Low normal
CLASIFICATION OF ACUTE HEART FAILURE CLINICAL STATUS HR SBP mmhg CI L/min/m 2 PCWP mmhg Congestion Killip/Forrester Diuresis Hupoperfusion End-organ hypoperfusion I. Acute decompensated CHF +/ Low normal
Ultrafiltration in Decompensated Heart Failure. Description
 Subject: Ultrafiltration in Decompensated Heart Failure Page: 1 of 7 Last Review Status/Date: September 2016 Ultrafiltration in Decompensated Heart Failure Description Ultrafiltration is a technique being
Subject: Ultrafiltration in Decompensated Heart Failure Page: 1 of 7 Last Review Status/Date: September 2016 Ultrafiltration in Decompensated Heart Failure Description Ultrafiltration is a technique being
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
State of the Art Treatment - Hyponatremia, Heart Rate, et al
 State of the Art Treatment - Hyponatremia, Heart Rate, et al Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from
State of the Art Treatment - Hyponatremia, Heart Rate, et al Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from
Therapeutics of Diuretics
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
(Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Regulation of Body Fluids: Na + and Water Linda Costanzo, Ph.D.
 Regulation of Body Fluids: Na + and Water Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. Why body sodium content determines ECF volume and the relationships
Regulation of Body Fluids: Na + and Water Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. Why body sodium content determines ECF volume and the relationships
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Solving the Revolving Door
 Solving the Revolving Door Managing Heart Failure at Transitions of Care and Beyond Brent N. Reed, PharmD, BCCP Associate Professor University of Maryland School of Pharmacy ATRIUM Cardiology Collaborative
Solving the Revolving Door Managing Heart Failure at Transitions of Care and Beyond Brent N. Reed, PharmD, BCCP Associate Professor University of Maryland School of Pharmacy ATRIUM Cardiology Collaborative
BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1
 Problem Set #8 Solutions p. 1") BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1 1. a. Proximal tubule. b. Proximal tubule. c. Glomerular endothelial fenestrae, filtration slits between podocytes of Bowman's capsule.
BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1 1. a. Proximal tubule. b. Proximal tubule. c. Glomerular endothelial fenestrae, filtration slits between podocytes of Bowman's capsule.
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Renal-Related Questions
 Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Kidney and urine formation
 Kidney and urine formation Renal structure & function Urine formation Urinary y concentration and dilution Regulation of urine formation 1 Kidney and urine formation 1.Renal structure & function 1)General
Kidney and urine formation Renal structure & function Urine formation Urinary y concentration and dilution Regulation of urine formation 1 Kidney and urine formation 1.Renal structure & function 1)General
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and