Rischio emorragico e trombotico nella TE e PV
|
|
|
- Ophelia Newman
- 5 years ago
- Views:
Transcription

1 Convegno Interregionale SIE Delegazione Triveneto Approfondimento sulle sindromi mielodisplastiche e mieloproliferative Sessione: Sindromi Mieloproliferative Croniche Rischio emorragico e trombotico nella TE e PV Marco Ruggeri Hematology Department, San Bortolo Hospital Vicenza, Italy
2 Major complications in Polycythemia Vera (PV) and Essential Thrombocythemia (ET) (PVSG and WHO 2001) Chronic disorders with a long survival (> 15 years) Low rate of transformation into acute leukemia or overt myelofibrosis (~10-15% at 15 years) Increased rate of venous and arterial thrombosis Increased rate of hemorrhage Major contributors to morbidity and mortality Elliott M and Tefferi A Br J Haematol; 2005
3 Essential Thrombocythemia (ET) MPN (WHO 2008) with a long survival: survival rate at 10 y: 89% survival rate at 15 y: 80% Low rate of transformation into acute leukemia or overt myelofibrosis: Leukemic transformation rate at 10 y: 0.7%; at 15 y: 2.1% Rate of progression to myelofibrosis at 10 y: 0.8%; at 15 y : 9.3% Barbui T et al. JCO ; 2011
4 Rough percentage of major thrombosis and hemorrhage from different series Thrombosis Hemorrhage* Ratio H/T^ PV ET Presentation: range average Follow up: average range Presentation: range average Follow up: average range *Including minor hemorrhages in some series ^ratio H/T calculated only using the series reporting both H and T events
5 Randomised trials in polycythaemia vera with rates of important end-points for each of the treatment arms Mc Mullin M et al, Br J Haematol; 2005
6 RCT in ET Study Cortelazzo NEJM 1995 Harrison NEJM 2005 Therapy None HU HU + ANA + (ASA 69%) (ASA 70%) ASA(100%) ASA (100%) 300 mg mg mg Rate of thrombosis (2 years) 24% 4% 4% 8%
7 Aim of cytoreductive treatment To reduce the rate of cardiovascular events Some concerns about an increase rate of leukemic transformation with cytoreductive agents
8 Risk of AML/MDS without treatment PV F.U.(y) A.L/pts (%) Berk et al, 1981 phlebotomy 8.6 2/134 (1.5) (PVSG-01) Finazzi et al, 2005 phleb or INF 8.4 5/669 (0.7) (ECLAP) times higher than in the general population ET F.U.(y) A.L./pts Murphy et al, 1997 no therapy 7.3 1/7 (PVSG-12) Sterkers et al, 1998 no therapy 8 0/31 (retrospective) Finazzi et al, 2000 no therapy 6 0/20 (HU vs no therapy) Rare event (= in the general population?) in untreated patients (often without karyotype analysis at diagnosis: CML )
9 Risk of AML/MDS in PV with treatment Study Therapy N patients FU (y.median) AML % Annual inc. RCT Berk 81 Chloramb P Haanen 82 P Busulph Najean 97 P (max) P32+HU (max) Najean 97 HU (max) Pipobrom. 142 similar Obs.Prospect. Donovan 84 HU Tarstarky 97 HU Passamonti00 Pipobrom Kiladjian 03 Pipobrom ECLAP 05 Ph-HU-P Obs.Retrospect. GISP 95 Ph-HU-BU Brodman 00 Ph-HU-BU Gangat 07 No drugs/ ANA/INF HU Other Others mo 67mo 72mo 161mo
10 Risk of AML/MDS in ET with treatment Study Therapy N patients FU (median) AML % RCT Finazzi 00 HU 77 6y HU+BUS 15 6y 5 33 Harrison 05 HU m Ana* m *30% previous HU Prosp. Obs. Murphy 97 HU y BUS y HU + BUS y Retros. Obs. Sterkers 98 P y 2 7 P32 + CHT 11 8y 1 9 BUS 35 8y 1 3 BUS + CHT 6 8y 1 17 HU 201 8y HU + CHT 50 8y 7 14 Pipobro 12 8y 0 0 Pipo + CHT 31 8y 5 16

11 Blood 2011

12 Blood 2011

13 JCO 2011
14 Treatment according to individual risk factors Reduction of the rate of cardiovascular events is at the cost of an increased risk of AL/MDS evolution (myelofibrotic evolution?) Rationale for risk stratification according to thrombotic risk, to select for CHT only high-risk patients
15 Established thrombotic risk factors for PV and ET 1. Age 2. Previous thrombosis
16 PV Thrombotic risk factors in PV and ET Age PVSG-01, Sem.Hematol 1986; 431 PV, RCT Advanced age is associated with a statistical significant increased risk of thrombosis GISP Ann Internal Med 1995; 1213 PV, retrospective Age < events/100 pts/y Age > events/100 pts/y ECLAP, J Clin Oncol 2005: 1638 PV, prospective, F.U.: 3 y Vascular complications in patients age > 65 y: 5% patient-year; HR 2 (CI ; p < 0.006) vs age < 65 y ET Cortelazzo et al, J Clin Oncol 1990, retrospective, 100 pts Incidence rate: 1.7 p/y age < 40 y; 6.3 p/y age y; 15.1 p/y age > 60 y (OR age > 60: 10,1; CI ) Besses et al, Leukemia 1999, retrospective, 148 pts Cumulative rate (6 y F.U.): 35.6% > 60 y vs 21.4% < 60 y Wolanskyj et al, Mayo Clin Proc 2006, retrospective, 322 pts, F.U.: 13.6 y RR age > 60 y: 1.51 (CI , p= 0.03), multivariable analysis Carobbio et al, Blood 2007, retrospective, 439 pts, F.U.: 6.2 y HR age * > 60 y: 2.3 (CI , p= 0.04) * and or history of thrombosis
17 Thrombotic risk factors for PV and ET Previous thrombosis PV GISP Ann Internal Med 1995: 1213 PV, retrospective. 24.6% thrombosis in patients with prior thrombosis vs 17.3% with no prior thrombosis; p= ECLAP, J Clin Oncol 2005: 1638 PV, prospective, F.U.: 3 y Incidence of vascular complications in patients with a previous thrombotic events: 4.93% patientsyear, HR: 1.95, CI , p = ET Cortelazzo et al, J Clin Oncol 1990, retrospective, 100 pts Incidence rate: 31.4 p/y with previous thrombosis vs 3.4 p/y with no previous thrombosis, OR 13 (4-41.5) Besses et al, Leukemia 1999, retrospective, 148 pts HR for previous vascular complications: 3 (1.5-6; p=0.001) Wolanskyj et al, Mayo Clin Proc 2006, retrospective, 322 pts, F.U y RR for previous vascular complications: 1.73 ( ; p=0.03) Carobbio et al, Blood 2007, retrospective, 439 pts, F.U. 6.2 y HR age * > 60 y: 2.3 (CI , p= 0.04) * and or history of thrombosis
18 ? Age and previous thrombosis are patientrelated risk factors; not disease-specific Age and previous thrombosis are not modified risk-factors Age is a continuous variable : a different effect changing stratification? Concept of dynamic risk profile
19 Other (target ) thrombotic risk factors in PV and ET? 1. Platelet count 2. Hematocrit (PV) 3. Fibrosis 4. Leukocytosis 5. JAK2 V617F
20 Thrombotic risk factors in PV and ET Platelet count PV PVSG 01 (PVSG-01, Semin Hematol, 1986) platelet count (either baseline or near the event) did not predict thrombosis ECLAP, Blood 2007, prospective, 1638 pts Rate of thrombosis Plt > 400 x 10 9 /L: 8.3% HR: 0.96, CI , p=0.81 Plt < 400 x 10 9 /L: 9.3% ET Cortelazzo et al, J Clin Oncol 1990, retrospective, 100 pts No association between platelet count and rate of thrombosis Besses et al, Leukemia 1999, retrospective, 148 pts No association between platelet count and rate of thrombosis Carobbio et al, Blood 2007, retrospective, 439 pts, F.U. 6.2 y HR for plt count > 700 x 10 9 /L : 0.7 (CI ) p=0.1 No significant correlation between platelet count and thrombosis

21

22 Blood, 2010
")
23 Univariate and multivariate analysis for risk factors predicting thrombotic events in follow-up (events, n 27) Blood, 2010


24
25 Thrombotic risk factors in PV Hematocrit Pearson et al, Lancet 1978 Direct association between Htc > 0.45 and rate of thrombosis Implication for treatment: 0.45: target value for venosection

26 Thrombotic risk factors in PV Hematocrit: ECLAP cohort HR in Htc 45% vs > 45-50% for: Death: 0.85, CI Major thrombosis: 0.94, CI Total thrombosis: 0.97, CI CYTO-PV: ongoing RCT evaluating % thrombosis in Htc > 45% vs < 45%
27 Thrombotic risk factors in PV White blood cell Petti et al, Leukemia, 1998; retrospective, 390 pts, F.U.: 9 months WBC > 20K vs < 12K = 5.2 HR (CI p=0.002) for death Gangat el al, Br J Haematol 2007; retrospective, 459 pts, F.U.: 64 months WBC > 15K vs < 15K : p < for VTE
28 Thrombotic risk factors in PV White blood cell ECLAP, Blood 2007; prospective, pts, F.U 3 y Analysis: WBC > 15k vs < 10k baseline; HR adjusted for CHT and ASA Major thrombosis (169) HR 1.71 ( ) p=0.017 AT (121) HR 1.67 ( ) p ns VTE (51) HR 1.81 ( ) p ns AMI (41) HR 2.84 ( ) p=0.013 Stroke/TIA (54) HR 0.93 ( ) p ns PAT (21) HR 1.72 ( ) p ns


29 Thrombotic risk factors in ET :White blood cell
30 Thrombotic risk factors in ET White blood cell PT1 study, N Engl J Med 2005 Intervention HU (404) ANA (405) OR p Primary EP ( ) 0.03 AT ( ) 0.04 VTE ( ) Hemorrhage ( ) Death ns Myelofibrosis ( ) 0.01

31 Thrombotic risk factors in ET White blood cell PT1 study N Engl J Med 2005 Similar control of platelet count but no effect of ANA on WBC level WBC > ANA vs HU, p< 0.001
32 Thrombotic risk factors in ET White blood cell But what about the absolute risk in study-cohort (Carobbio et al, Blood 2007)? 67 events in 439 pts in 6 y: 15% (2.5% per y) High WBC Low WBC Total Thrombosis No thrombosis Total Absolute risk in high WBC = 43/221: 19%; in low WBC= 24/218: 11% Thrombosis rate per 100 p/y : 3.2 (high) vs 1.8 (low) Prospective, validation study possible only enrolling a very high number of patients!
33 JAK2 V617F mutation and thrombosis Early 2005: five groups reported the presence of an acquired point mutation, G1849T in Jak2 gene in patients with Ph-negative MPD (detected in 95% of PV and 50%-60% of ET patients) G1849T results in V to F substitution in JAK2 molecule (JAK2 V617F ) within its auto-inhibitory pseudo kinase domain Cytokine independent activation Unregolated cell proliferation
34 Studies addressing the association between JAK2 V617F and thrombosis in ET Study Pt JAK2 V617F Association? Confounding factors Cheung yes NR Heller yes Age, Hb Finazzi yes Hb, WBC Ohyashiki yes Hb, WBC Carobbio no Hb, WBC Kittur yes Age, Hb, WBC Alvarez no Hb Vannucchi yes Age, Htc Hsiao yes Hb, WBC
35 Association between JAK2 V617F and thrombosis in ET: systematic review OR thrombosis OR AT OR VTE Ziakas, Haematologica patients CI CI Dahabreh et al Thromb Res patients Lussana et al, Thromb Res patients CI CI CI
36 Thrombotic risk and JAK2V617F allele burden in PV Vannucchi et al, Leukemia 2007: prospective evaluation, 173 pts, F.U.: 24 months (median) Analysis: > 75% vs < 25% mutant allele Splenomegaly : RR 4.7, p < Pruritus : RR 3.1, p < CV events : RR 7.1, p = Correlation not confirmed in another study (Tefferi et al, Leukemia 2007)


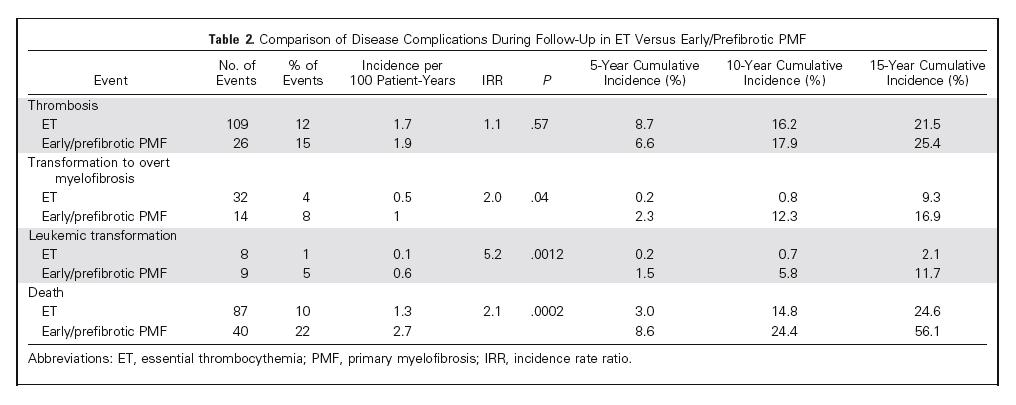
37 Fibrosis and thrombosis in ET JCO 2011

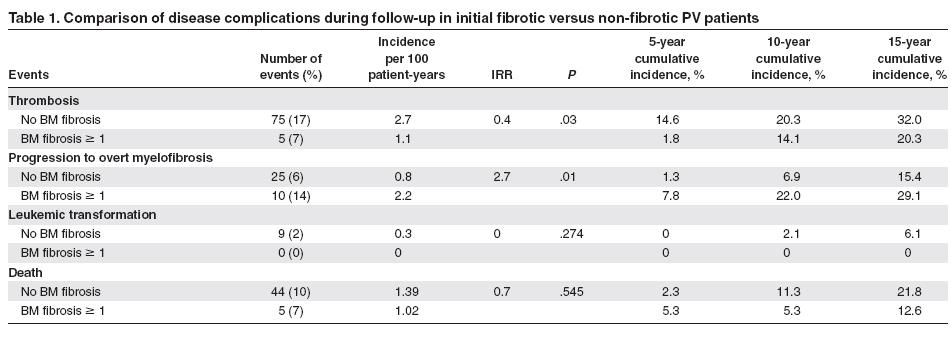
38 Fibrosis and thrombosis in PV
, specific therapy for PV and ET, antithrombotic and anti-hemorrhagic")
39 Enrollment: 105 PV and 150 ET consecutive patients diagnosed from January 1985 to June 2005 with at least one surgical procedure from diagnosis to June 2005 (311 procedures). Data collection: patients characteristics and clinical events before and after surgery (3 months of follow-up), specific therapy for PV and ET, antithrombotic and anti-hemorrhagic prophylaxis
40 Thrombotic and hemorrhagic risk after surgery in PV and ET End-points Major thrombotic events defined as in ECLAP Study (NEJM 2004) Major hemorrhages included intracranial, ocular, joint, or retroperitoneal bleeding; episodes requiring surgery or angiographic intervention and any bleeding causing a hemoglobin loss of 2 gr/dl at least and/or requiring 2 or more blood units transfusions
41 Thrombotic and hemorrhagic risk after surgery in PV and ET Type of intervention Variable PV ET P Emergency procedures 11/128 (8.1%) 15/183 (8%) 0.91 Abdominal surgery laparoscopy/laparotomy 6/33 (18.1%) 15/58 (25.8%) Major surgery 65/128 (50%) 91/183 (49%) 0.87 General anaesthesia 74/128 (58%) 120/183 (65%) 0.529
42 Thrombotic and hemorrhagic risk after surgery in PV and ET Antithrombotic prophylaxis Data available in 292/311, 93.8%, surgeries 126/292 (43.2%) LMWH 38/292 (13%) UH 5/292 (1.7%) warfarin 123/292 (42.1%) no prophylaxis; in 45/123 (36.6%) ASA was administered peri-intervention 189/255 (74%) ongoing cytoreductive treatment; in 9 case a short cycle was administered
43 Thrombotic and hemorrhagic risk after surgery in PV and ET Post-surgery outcomes (3 months follow-up) 259/311 (83.2%) no events 24 thrombosis (7.3%, 12 AT, 12 VTE) 23 major hemorrhages (7.3%) 7 minor hemorrhages 5 deaths (surgery-related, within 3 months) VTE more frequent in PV than in ET (7.7% vs 1.0%, P=0.002)
44 Thrombotic and hemorrhagic risk after surgery in PV and ET Strong risk gradient for AT with the presence of one or more CV risk factors (OR for 4 or more risk factors: 40.9: p= 0.003) Platelet count and hematocrit at surgery (median 477 x 109/L and 42.6%) not associated with AT nor with VTE No correlation between bleeding episodes and type of cmpd, use of antithrombotic prophylaxis and type of surgery
 than in the general population; a relationship was found between JAK2 V617F and fetal loss (p>0.05) JAK2 V617F patients had an odds ratio of 2.02 (95% CI: 1.1-3.")
45 Pregnancy, JAK2 V617F and thrombosis 103 pregnancies occurred in 62 women with ET; half of the studied women carried the JAK2 V617VF mutation Fetal loss in women with ET was higher (OR 3.4, CI 3-3.9, p < 0.001) than in the general population; a relationship was found between JAK2 V617F and fetal loss (p>0.05) JAK2 V617F patients had an odds ratio of 2.02 (95% CI: ) of developing complications in comparison with JAK2WT
46 Prognostic classification in terms of thrombotic risk in PV and ET Established risk factors Potential novel risk factors* Age > 60 years Leukocytosis Previous thrombosis JAK2 V617F Surgery Pregnancy * validation in large, prospective clinical trials required
47 Thrombosis risk oriented management in PV and ET Risk Category PV ET Low High Phlebotomy + ASA Myelosuppression +/- Phlebotomy + ASA No therapy or ASA Myelosuppresion + ASA



48
49 ?? Current risk stratification is designed to estimate the likelihood of thrombotic complications Different stratification and management strategies in case of other therapeutic target (survival, leukemic/myelodisplatic evolutions, myelofibrotic transformation?

50 JCO 2011


51
52 Risk factors for hemorrhage Platelet count > million/µl Previous bleeding (ECLAP entire cohort, Marchioli et al 2005) AVWS (reviewed by Michiels, 2004) Surgery (Ruggeri et al, Blood 2008) Anagrelide (?): (UK PT-1 Study, Harrison et al 2005) Antithrombotic prophylaxis
53 Prevention and treatment of thrombotic complications in ET: efficacy and safety of aspirin PJJ van Genderen et al, Br J Haematol 1997 Incidence of thrombotic and bleeding complications in 68 ET patients Treatment FU Thrombosis Bleeding (p/y) (x 100/p/y) (x 100/p/y) Careful observation Aspirin Cytoreduction Aspirin + cytoreduction


54 Blood, 2010
55

56

57

58
59 Primary prevention with low dose aspirin Low dose aspirin is effective in reducing the risk of arterial thrombosis The net benefit of aspirin as a form of primary prophylaxis becomes manifest when the individual risk of thrombosis is > 3 events per 100 pts/year
60 Implications of primary prevention trial results for PV and ET Even assuming a basal risk and an absolute increase of bleeding due to treatment similar to that of general population, any advantage of aspirin in PV and ET is expected only when the basal treatment risk is 3-4/100/yr The basal thrombotic risk in pts ET is not available since all series include pts treated with aspirin (for PV data from ECLAP study, placebo arm)

61

62

63



64
65 Clinical vignette -January 2010: male patient; age 70 years; ET diagnosis (PLT 733 x 10 9 /L; BM biopsy; JAK2 WT) *diabetes mellitus * dual antiplatelet (ASA + clopidogrel) from september 2009 for carotid bare- metal stent (asymptomatic stenosis) -January 2011: PLT 700 x 10 9 /L: ASA + clopidogrel -August 2011: PLT 642 x 10 9 /L: ASA + clopidogrel -November 2011: PLT 757 x 10 9 /L: ASA + clopidogrel

66 February 2012: death for cerebellar hemorrhage PLT 619 x 10 9 /L
67 Pts Sex Age (y) Diagnosis Therapy Setting Since: PFG M 80 ET Dual DES Nov 11 EE M 73 PV Dual DES Mar 12 MI M 80 PV Dual DES Sep 10 FP M 50 ET Dual DES Nov 06 DMR M 78 ET Dual Peripheral Stent Dic 11 SF M 56 PV TAO FA Dic 10 ASA Ictus RM M 87 ET TAO IMA Sep 11 ASA (2) GE M 80 ET Dual DES Feb 12 CB F 75 PV TAO ASA DAG F 79 PV TAO ASA ICTUS TIA EP TIA Oct 09 Jun 06
68 Dual or Mono Antiplatelet Therapy for Patients With Acute Ischemic Stroke or Transient Ischemic Attack: Systematic Review and Meta-Analysis of Randomized Controlled Trials Stroke RCT, 3766 patients mono antiplatelet dual therapy RR Stroke recurrence 5% ( ) Composite vascular event 6% 4.4% 0.75( ) Combination vascular event + death 9.1% 1.7% 0.71( ) Major bleeding 0.4% 0.9% 2.09( )

69 Twenty-seven major bleeds were recorded, with an incidence of 0.9% patient-years The incidence of major bleeding in per cent patient-years was: -0.8 antiplatelet agents -0.9 vitamin K antagonists -2.8 antiplatelet agents plus vitamin K antagonists Haematologica 2008
70 ??? Is dual antiaplatelet therapy or antiplatelet + warfarin) safe in ET and PV patients?
Managing ET in Tiziano Barbui MD
 Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes A critical reappraisal of anagrelide in the management of ET
 European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes 2012 Clinical i l Aspects of Polycythemia and Essential Thrombocythemia A critical reappraisal of anagrelide in the management
European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes 2012 Clinical i l Aspects of Polycythemia and Essential Thrombocythemia A critical reappraisal of anagrelide in the management
Prognostic models in PV and ET
 Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]
![Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]](/thumbs/87/95709298.jpg "Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]") Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
Leukemic transformation of MPN: Therapy related or unrelated?
 Leukemic transformation of MPN: Therapy related or unrelated? Jean Jacques KILADJIAN, MD, PhD Clinical Investigations Center Saint Louis Hospital Paris Diderot University Leukemic transformation: a long
Leukemic transformation of MPN: Therapy related or unrelated? Jean Jacques KILADJIAN, MD, PhD Clinical Investigations Center Saint Louis Hospital Paris Diderot University Leukemic transformation: a long
Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012
 Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012 Outline Case presentation Overview of PV Disease course Mechanisms of thrombosis Case Presentation
Why do patients with polycythemia vera clot? Kinsey McCormick Hematology Fellows conference August 10, 2012 Outline Case presentation Overview of PV Disease course Mechanisms of thrombosis Case Presentation
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update
 Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
Hydroxyurea: the comparator in studies with new anti-jak2 inhibitors
 Hematology Meeting Reports 2009;3(3):108 114 SESSION VIII xg. Finazzi T. Barbui 1 x Divisione di Ematologia e 1 Fondazione per la Ricerca Ospedali Riuniti di Bergamo, Italy Hydroxyurea: the comparator
Hematology Meeting Reports 2009;3(3):108 114 SESSION VIII xg. Finazzi T. Barbui 1 x Divisione di Ematologia e 1 Fondazione per la Ricerca Ospedali Riuniti di Bergamo, Italy Hydroxyurea: the comparator
Emerging diagnostic and risk stratification criteria
 PV STATE OF MIND Polycythemia vera: Emerging diagnostic and risk stratification criteria Rami S. Komrokji, MD Moffitt Cancer Center, Tampa, Florida Disclosure These slides were developed by Incyte Corporation
PV STATE OF MIND Polycythemia vera: Emerging diagnostic and risk stratification criteria Rami S. Komrokji, MD Moffitt Cancer Center, Tampa, Florida Disclosure These slides were developed by Incyte Corporation
Is the recommended hematocrit target in polycythemia vera evidence based? Tiziano BARBUI, MD Ospedali Riuniti, Bergamo, Italy
 Is the recommended hematocrit target in polycythemia vera evidence based? Tiziano BARBUI, MD Ospedali Riuniti, Bergamo, Italy We have generated a transgenic mouse line that reaches a hematocrit concentration
Is the recommended hematocrit target in polycythemia vera evidence based? Tiziano BARBUI, MD Ospedali Riuniti, Bergamo, Italy We have generated a transgenic mouse line that reaches a hematocrit concentration
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms
 Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
CLINICAL CASE PRESENTATION
 European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera
 Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera Alessandro M. Vannucchi, MD Laboratorio Congiunto MMPC Department of Experimental and Clinical Medicine University
Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera Alessandro M. Vannucchi, MD Laboratorio Congiunto MMPC Department of Experimental and Clinical Medicine University
Molecular aberrations in MPN. and use in the clinic. Timothy Devos MD PhD
 Molecular aberrations in MPN and use in the clinic Timothy Devos MD PhD MB&C2017 24-3-2017 Introduction 1951: William Dameshek MPD MPN = clonal, hematopoietic stem cell disorders, proliferation in BM of
Molecular aberrations in MPN and use in the clinic Timothy Devos MD PhD MB&C2017 24-3-2017 Introduction 1951: William Dameshek MPD MPN = clonal, hematopoietic stem cell disorders, proliferation in BM of
MALATTIE MIELOPROLIFERATIVE CRONICHE
 MALATTIE MIELOPROLIFERATIVE CRONICHE Dott. Roberto Latagliata Policlinico Umberto I Università Sapienza, Roma Highlights from EHA 2017: some points to address today WHO 2016 MPN classification: hot topics
MALATTIE MIELOPROLIFERATIVE CRONICHE Dott. Roberto Latagliata Policlinico Umberto I Università Sapienza, Roma Highlights from EHA 2017: some points to address today WHO 2016 MPN classification: hot topics
Biologia molecolare delle malattie mieloproliferative croniche Ph1-negative tipiche
 41 CONGRESSO NAZIONALE SIE Bologna 14-17 Ottobre 2007 Biologia molecolare delle malattie mieloproliferative croniche Ph1-negative tipiche Alessandro M. Vannucchi Dip.. di Ematologia, Università degli Studi
41 CONGRESSO NAZIONALE SIE Bologna 14-17 Ottobre 2007 Biologia molecolare delle malattie mieloproliferative croniche Ph1-negative tipiche Alessandro M. Vannucchi Dip.. di Ematologia, Università degli Studi
The treatment of polycythaemia vera: an update in the JAK2 era
 Intern Emerg Med (2007) 2:13 18 DOI 10.1007/s11739-007-0003-4 IM REVIEW G. Finazzi T. Barbui The treatment of polycythaemia vera: an update in the JAK2 era Received: 31 August 2006 / Accepted in original
Intern Emerg Med (2007) 2:13 18 DOI 10.1007/s11739-007-0003-4 IM REVIEW G. Finazzi T. Barbui The treatment of polycythaemia vera: an update in the JAK2 era Received: 31 August 2006 / Accepted in original
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Current Prognostication in Primary Myelofibrosis
 Current Prognostication in Primary Myelofibrosis Francisco Cervantes Hematology Department, Hospital Clínic, Barcelona, Spain Florence, April 2011 Survival in PMF No. patients: 1,054 Median Srv (95% CI):
Current Prognostication in Primary Myelofibrosis Francisco Cervantes Hematology Department, Hospital Clínic, Barcelona, Spain Florence, April 2011 Survival in PMF No. patients: 1,054 Median Srv (95% CI):
Research Article Gender and Vascular Complications in the JAK2 V617F-Positive Myeloproliferative Neoplasms
 Thrombosis Volume 2011, Article ID 874146, 8 pages doi:10.1155/2011/874146 Research Article Gender and Vascular Complications in the JAK2 V617F-Positive Myeloproliferative Neoplasms Brady L. Stein, 1 Alfred
Thrombosis Volume 2011, Article ID 874146, 8 pages doi:10.1155/2011/874146 Research Article Gender and Vascular Complications in the JAK2 V617F-Positive Myeloproliferative Neoplasms Brady L. Stein, 1 Alfred
Practice Patterns in the Diagnosis and Treatment of Polycythemia Vera in the Post JAK2 V617F Discovery Era
 1238 Original Research Practice Patterns in the Diagnosis and Treatment of Polycythemia Vera in the Post JAK2 V617F Discovery Era Elizabeth M. Kander, MD a ; Alison R. Moliterno, MD b ; Alfred Rademaker,
1238 Original Research Practice Patterns in the Diagnosis and Treatment of Polycythemia Vera in the Post JAK2 V617F Discovery Era Elizabeth M. Kander, MD a ; Alison R. Moliterno, MD b ; Alfred Rademaker,
Polycytemia Vera, Essential Thrombocythemia and Myelofibrosis: prognosis and treatment
 Polycytemia Vera, Essential Thrombocythemia and Myelofibrosis: prognosis and treatment BHS Training course 2013-2015 Timothy Devos POLYCYTEMIA VERA PV: clinical manifestations thrombosis (art > ven) facial
Polycytemia Vera, Essential Thrombocythemia and Myelofibrosis: prognosis and treatment BHS Training course 2013-2015 Timothy Devos POLYCYTEMIA VERA PV: clinical manifestations thrombosis (art > ven) facial
Essential thrombocythemia treatment algorithm 2018
 Tefferi et al. (2018) 8:2 DOI 10.1038/s41408-017-0041-8 CURRENT TREATMENT ALGORITHM Essential thrombocythemia treatment algorithm 2018 Ayalew Tefferi 1, Alessandro M. Vannucchi 2 and Tiziano Barbui 3 Open
Tefferi et al. (2018) 8:2 DOI 10.1038/s41408-017-0041-8 CURRENT TREATMENT ALGORITHM Essential thrombocythemia treatment algorithm 2018 Ayalew Tefferi 1, Alessandro M. Vannucchi 2 and Tiziano Barbui 3 Open
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
EUROPEAN RCT IN MPDs
 EUROPEAN RCT IN MPDs A. Multicenter, Multinational -EORTC -ECLAP -ANHIDRET B. Multicenter, National -French PV RCTs -Italian ET RCT - PT- RCTs C. European Leukemia NET studies D. Future: JAK-2 inhibitor
EUROPEAN RCT IN MPDs A. Multicenter, Multinational -EORTC -ECLAP -ANHIDRET B. Multicenter, National -French PV RCTs -Italian ET RCT - PT- RCTs C. European Leukemia NET studies D. Future: JAK-2 inhibitor
RESPONSE (NCT )
") Changes in Quality of Life and Disease-Related Symptoms in Patients With Polycythemia Vera Receiving Ruxolitinib or Best Available Therapy: RESPONSE Trial Results Abstract #709 Mesa R, Verstovsek S, Kiladjian
Changes in Quality of Life and Disease-Related Symptoms in Patients With Polycythemia Vera Receiving Ruxolitinib or Best Available Therapy: RESPONSE Trial Results Abstract #709 Mesa R, Verstovsek S, Kiladjian
Polycythemia Vera and Essential Thombocythemia A Single Institution Experience
 INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 29 No 4, 2008 7 Original Article-I Polycythemia Vera and Essential Thombocythemia A Single Institution Experience CECIL ROSS, NAVYA, VANAMALA AND KARUNA
INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 29 No 4, 2008 7 Original Article-I Polycythemia Vera and Essential Thombocythemia A Single Institution Experience CECIL ROSS, NAVYA, VANAMALA AND KARUNA
Do All Patients With Polycythemia Vera or Essential Thrombocythemia Need Cytoreduction?
 1539 Do All Patients With Polycythemia Vera or Essential Thrombocythemia Need Cytoreduction? Kamya Sankar, MD, a and Brady L. Stein, MD, MHS a,b,c Abstract Polycythemia vera (PV) and essential thrombocythemia
1539 Do All Patients With Polycythemia Vera or Essential Thrombocythemia Need Cytoreduction? Kamya Sankar, MD, a and Brady L. Stein, MD, MHS a,b,c Abstract Polycythemia vera (PV) and essential thrombocythemia
JAK2 Inhibitors for Myeloproliferative Diseases
 JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs
 MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Disclosure of
MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Disclosure of
Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis. Francesco Passamonti Università degli Studi dell Insubria, Varese
 Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis Francesco Passamonti Università degli Studi dell Insubria, Varese DIPSS during f-up IPSS at diagnosis Diagnose MF and genotype
Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis Francesco Passamonti Università degli Studi dell Insubria, Varese DIPSS during f-up IPSS at diagnosis Diagnose MF and genotype
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms
 Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
The prognostic relevance of serum lactate dehydrogenase and mild bone marrow reticulin fibrosis in essential thrombocythemia
 Received: 3 February 2017 Revised: 13 February 2017 Accepted: 14 February 2017 DOI: 10.1002/ajh.24689 RESEARCH ARTICLE The prognostic relevance of serum lactate dehydrogenase and mild bone marrow reticulin
Received: 3 February 2017 Revised: 13 February 2017 Accepted: 14 February 2017 DOI: 10.1002/ajh.24689 RESEARCH ARTICLE The prognostic relevance of serum lactate dehydrogenase and mild bone marrow reticulin
Polycythemia vera (PV), a myeloproliferative disorder
, a myeloproliferative disorder") Myeloproliferative Disorders research paper Polycythemia vera in young patients: a study on the long-term risk of thrombosis, myelofibrosis and leukemia FRANCESCO PASSAMONTI, LUCIA MALABARBA, ESTER ORLANDI,
Myeloproliferative Disorders research paper Polycythemia vera in young patients: a study on the long-term risk of thrombosis, myelofibrosis and leukemia FRANCESCO PASSAMONTI, LUCIA MALABARBA, ESTER ORLANDI,
Focus on aggressive polycythemia vera
 Focus on aggressive polycythemia vera Jerry L. Spivak, MD Professor of Medicine and Oncology Director, the Johns Hopkins Center for the Chronic Myeloproliferative Disorders Johns Hopkins University School
Focus on aggressive polycythemia vera Jerry L. Spivak, MD Professor of Medicine and Oncology Director, the Johns Hopkins Center for the Chronic Myeloproliferative Disorders Johns Hopkins University School
How to monitor MPN patients
 How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
SPOTLIGHT SPOTLIGHT REVIEW. Evidence and expertise in the management of polycythemia vera and essential thrombocythemia
 (2008) 22, 1494 1502 & 2008 Macmillan Publishers Limited All rights reserved 0887-6924/08 $30.00 www.nature.com/leu REVIEW Evidence and expertise in the management of polycythemia vera and essential thrombocythemia
(2008) 22, 1494 1502 & 2008 Macmillan Publishers Limited All rights reserved 0887-6924/08 $30.00 www.nature.com/leu REVIEW Evidence and expertise in the management of polycythemia vera and essential thrombocythemia
How I treat high risk myeloproliferative neoplasms. Francesco Passamonti Università dell Insubria Varese - Italy
 How I treat high risk myeloproliferative neoplasms Francesco Passamonti Università dell Insubria Varese - Italy How I treat high risk MF MF Treatment ELN 2018 Guidelines Anemia (Hb < 10 g/dl) Splenomegaly
How I treat high risk myeloproliferative neoplasms Francesco Passamonti Università dell Insubria Varese - Italy How I treat high risk MF MF Treatment ELN 2018 Guidelines Anemia (Hb < 10 g/dl) Splenomegaly
CLINICAL POLICY DEPARTMENT: Medical Management DOCUMENT NAME: JakafiTM REFERENCE NUMBER: NH.PHAR.98
 PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination
 Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
ESSENTIAL thrombocythemia is a myeloproliferative
 1132 THE NEW ENGLAND JOURNAL OF MEDICINE April 27, 1995 HYDROXYUREA FOR PATIENTS WITH ESSENTIAL THROMBOCYTHEMIA AND A HIGH RISK OF THROMBOSIS SERGIO CORTELAZZO, M.D., GUIDO FINAZZI, M.D., MARCO RUGGERI,
1132 THE NEW ENGLAND JOURNAL OF MEDICINE April 27, 1995 HYDROXYUREA FOR PATIENTS WITH ESSENTIAL THROMBOCYTHEMIA AND A HIGH RISK OF THROMBOSIS SERGIO CORTELAZZO, M.D., GUIDO FINAZZI, M.D., MARCO RUGGERI,
Polycythemia vera: Emerging diagnostic and risk stratification criteria
 This article, sponsed by Incyte Cpation, is based on a paid interview with Rami S. Komrokji, MD, of Moffitt Cancer Center, Tampa, Flida, conducted on May 4, 2015. Polycythemia vera: Emerging diagnostic
This article, sponsed by Incyte Cpation, is based on a paid interview with Rami S. Komrokji, MD, of Moffitt Cancer Center, Tampa, Flida, conducted on May 4, 2015. Polycythemia vera: Emerging diagnostic
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Ruben A. Mesa, MD & John Camoranio, MD Mayo Clinic
 Arizona, USA Prognosis & MPN Management in 2013 Ruben A. Mesa, MD & John Camoranio, MD Mayo Clinic Arizona, USA Understanding MPN Therapy Options Prognosis and Goals (Mesa & Camoriano) Evolving Rx ET (Vannucchi)
Arizona, USA Prognosis & MPN Management in 2013 Ruben A. Mesa, MD & John Camoranio, MD Mayo Clinic Arizona, USA Understanding MPN Therapy Options Prognosis and Goals (Mesa & Camoriano) Evolving Rx ET (Vannucchi)
Blood Reviews 26 (2012) Contents lists available at SciVerse ScienceDirect. Blood Reviews. journal homepage:
 Contents lists available at SciVerse ScienceDirect. Blood Reviews. journal homepage:") Blood Reviews 26 (2012) 205 211 Contents lists available at SciVerse ScienceDirect Blood Reviews journal homepage: www.elsevier.com/locate/blre REVIEW Front-line therapy in polycythemia vera and essential
Blood Reviews 26 (2012) 205 211 Contents lists available at SciVerse ScienceDirect Blood Reviews journal homepage: www.elsevier.com/locate/blre REVIEW Front-line therapy in polycythemia vera and essential
DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS. Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands
 DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands RECENT DEVELOPMENTS Better anti-platelet agents: Prasugrel and Ticagrelor to replace
DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands RECENT DEVELOPMENTS Better anti-platelet agents: Prasugrel and Ticagrelor to replace
Dental Management Considerations for Patients on Antithrombotic Therapy
 Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
International Journal of Scientific & Engineering Research, Volume 8, Issue 12, December-2017 ISSN
 ISSN 2229-5518 286 Overview of management strategies toward Thrombocythemia Mayada Amin Aljudaibi, Reem Ali Mohammed Alamoodi, Abrar Ali Mohammed Alamoodi, Samar Mohammed Hasan Al_Hashemi, Bashayer Sadagah
ISSN 2229-5518 286 Overview of management strategies toward Thrombocythemia Mayada Amin Aljudaibi, Reem Ali Mohammed Alamoodi, Abrar Ali Mohammed Alamoodi, Samar Mohammed Hasan Al_Hashemi, Bashayer Sadagah
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Polycythemia vera is a clonal disorder of the. Treatment of polycythemia vera. decision making and problem solving TIZIANO BARBUI, GUIDO FINAZZI
 Haematologica 1998; 83:143-149 decision making and problem solving Treatment of polycythemia vera TIZIANO BARBUI, GUIDO FINAZZI Department of Hematology, Ospedali Riuniti, Bergamo, Italy Abstract Background
Haematologica 1998; 83:143-149 decision making and problem solving Treatment of polycythemia vera TIZIANO BARBUI, GUIDO FINAZZI Department of Hematology, Ospedali Riuniti, Bergamo, Italy Abstract Background
Polycythemia vera treatment algorithm 2018
 Tefferi et al. (2018) 8:3 DOI 10.1038/s41408-017-0042-7 CURRENT TREATMENT ALGORITHM Polycythemia vera treatment algorithm 2018 Ayalew Tefferi 1, Alessandro M. Vannucchi 2 and Tiziano Barbui 3 Open Access
Tefferi et al. (2018) 8:3 DOI 10.1038/s41408-017-0042-7 CURRENT TREATMENT ALGORITHM Polycythemia vera treatment algorithm 2018 Ayalew Tefferi 1, Alessandro M. Vannucchi 2 and Tiziano Barbui 3 Open Access
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease
 The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
International Journal of Gerontology
 International Journal of Gerontology 7 (2013) 40e44 Contents lists available at SciVerse ScienceDirect International Journal of Gerontology journal homepage: www.ijge-online.com Original Article JAK2 V617F
International Journal of Gerontology 7 (2013) 40e44 Contents lists available at SciVerse ScienceDirect International Journal of Gerontology journal homepage: www.ijge-online.com Original Article JAK2 V617F
DISCLOSURE. What I am Talking About. Rational Use of Antiplatelet Agents. Aspirin. Tom DeLoughery, MD MACP FAWM
 Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Approach to patients with essential thrombocythaemia and very high platelet counts: what is the evidence for treatment?
 review Approach to patients with essential thrombocythaemia and very high platelet counts: what is the evidence for treatment? Lorenzo Falchi, 1 Prithviraj Bose, 2 Kate J. Newberry 2 and Srdan Verstovsek
review Approach to patients with essential thrombocythaemia and very high platelet counts: what is the evidence for treatment? Lorenzo Falchi, 1 Prithviraj Bose, 2 Kate J. Newberry 2 and Srdan Verstovsek
Disclosure. Financial disclosure: National Advisory Board & Research Grant from Boehringer-Ingelheim
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
New Therapies for MPNs
 Pomalidomide and IMIDS in Myelofibrosis New Therapies for MPNs Fourth International Workshop on CML and MPN Natchez Louisiana Ruben A. Mesa, MD Professor of Medicine Mayo Clinic College of Medicine Director
Pomalidomide and IMIDS in Myelofibrosis New Therapies for MPNs Fourth International Workshop on CML and MPN Natchez Louisiana Ruben A. Mesa, MD Professor of Medicine Mayo Clinic College of Medicine Director
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
After acute coronary syndromes patients continue to have recurrent ischemic events despite revascularization and dual antiplatelet therapy
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Survival and Disease Progression in Essential Thrombocythemia Are Significantly Influenced by Accurate Morphologic Diagnosis: An International Study
 Published Ahead of Print on July 11, 2011 as 10.1200/JCO.2010.34.5298 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.34.5298 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Published Ahead of Print on July 11, 2011 as 10.1200/JCO.2010.34.5298 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.34.5298 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Splanchnic vein thrombosis in myeloproliferative neoplasms: treatment algorithm 2018
 Finazzi et al. (2018) 8:64 DOI 10.1038/s41408-018-0100-9 CURRENT TREATMENT ALGORITHM Splanchnic vein thrombosis in myeloproliferative neoplasms: treatment algorithm 2018 Guido Finazzi 1, Valerio De Stefano
Finazzi et al. (2018) 8:64 DOI 10.1038/s41408-018-0100-9 CURRENT TREATMENT ALGORITHM Splanchnic vein thrombosis in myeloproliferative neoplasms: treatment algorithm 2018 Guido Finazzi 1, Valerio De Stefano
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
MPNs: JAK2 inhibitors & beyond. Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt
 NCI, Cairo University, Egypt") MPNs: JAK2 inhibitors & beyond Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt Myeloproliferative Neoplasms (MPNs) AGENDA: 1. Molecular biology 2. New WHO diagnostic criteria. 3. Risk stratification
MPNs: JAK2 inhibitors & beyond Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt Myeloproliferative Neoplasms (MPNs) AGENDA: 1. Molecular biology 2. New WHO diagnostic criteria. 3. Risk stratification
Frequent reduction or absence of detection of the JAK2-mutated clone in JAK2V617F-positive patients within the first years of hydroxyurea therapy
 Frequent reduction or absence of detection of the JAK2-mutated clone in JAK2V617F-positive patients within the first years of hydroxyurea therapy François Girodon, 1,2 Céline Schaeffer, 1 Cédric Cleyrat,
Frequent reduction or absence of detection of the JAK2-mutated clone in JAK2V617F-positive patients within the first years of hydroxyurea therapy François Girodon, 1,2 Céline Schaeffer, 1 Cédric Cleyrat,
Bone marrow histopathology in Ph - CMPDs. - the new WHO classification - Juergen Thiele Cologne, Germany
 Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
La terapia antiaggregante nel paziente con stroke
 La terapia antiaggregante nel paziente con stroke Paolo Gresele Dipartimento di Medicina, Sez. Medicina Interna e Cardiovascolare Università di Perugia XXVII Congresso Nazionale FCSA Milano, 20-22 Ottobre
La terapia antiaggregante nel paziente con stroke Paolo Gresele Dipartimento di Medicina, Sez. Medicina Interna e Cardiovascolare Università di Perugia XXVII Congresso Nazionale FCSA Milano, 20-22 Ottobre
Post-ASH 2015 CML - MPN
 Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Latest updates in Myeloproliferative Neoplasms. Elizabeth Hexner, MD, MSTR
 Latest updates in Myeloproliferative Neoplasms Elizabeth Hexner, MD, MSTR Disclosures Nothing to disclose Agenda/Goals Treatment goals in PV Indications for cytoreduction in patients polycythemia vera
Latest updates in Myeloproliferative Neoplasms Elizabeth Hexner, MD, MSTR Disclosures Nothing to disclose Agenda/Goals Treatment goals in PV Indications for cytoreduction in patients polycythemia vera
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
Stifel Nicolaus 2013 Healthcare Conference. John Scarlett, M.D. Chief Executive Officer September 11, 2013
 Stifel Nicolaus 2013 Healthcare Conference John Scarlett, M.D. Chief Executive Officer September 11, 2013 1 forward-looking statements Except for the historical information contained herein, this presentation
Stifel Nicolaus 2013 Healthcare Conference John Scarlett, M.D. Chief Executive Officer September 11, 2013 1 forward-looking statements Except for the historical information contained herein, this presentation
Clinical Perspective The Hematologist s View
 SPLANCHNIC VEIN THROMBOSIS. TYPICAL OR ATYPICAL MPN? Giovanni Barosi Unit of Clinical Epidemiology/Center ofr the Study of Myelofibrosis. IRCCS Policlinico S. Matteo Foundation, Pavia Lisbon, 4-5 May 2012
SPLANCHNIC VEIN THROMBOSIS. TYPICAL OR ATYPICAL MPN? Giovanni Barosi Unit of Clinical Epidemiology/Center ofr the Study of Myelofibrosis. IRCCS Policlinico S. Matteo Foundation, Pavia Lisbon, 4-5 May 2012
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Published Ahead of Print on October 13, 2009 as /JCO J Clin Oncol by American Society of Clinical Oncology INTRODUCTION
 Published Ahead of Print on October 13, 9 as 1.1/JCO.9.23. The latest version is at http://jco.ascopubs.org/cgi/doi/1.1/jco.9.23. JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Pegylated Interferon
Published Ahead of Print on October 13, 9 as 1.1/JCO.9.23. The latest version is at http://jco.ascopubs.org/cgi/doi/1.1/jco.9.23. JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Pegylated Interferon
How I Treat Myelofibrosis. Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom
 How I Treat Myelofibrosis Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom Primary Myelofibrosis Archiv Fur Pathol. 1879;78:475-96. 2 cases of leukemia with peculiar blood and marrow findings
How I Treat Myelofibrosis Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom Primary Myelofibrosis Archiv Fur Pathol. 1879;78:475-96. 2 cases of leukemia with peculiar blood and marrow findings
Mielofibrosi: inquadramento dei fattori prognostici
 Mielofibrosi: inquadramento dei fattori prognostici Francesco Passamon, Division of Hematology University Hospital, Fondazione Macchi Varese, Italy Reduced survival in PMF and causes of death Median OS
Mielofibrosi: inquadramento dei fattori prognostici Francesco Passamon, Division of Hematology University Hospital, Fondazione Macchi Varese, Italy Reduced survival in PMF and causes of death Median OS
Predictive factors of thrombosis for patients with essential thrombocythaemia: A single center study*
 Original papers Predictive factors of thrombosis for patients with essential thrombocythaemia: A single center study* Iwona Prajs A F, Kazimierz Kuliczkowski F Department and Clinic of Hematology, Blood
Original papers Predictive factors of thrombosis for patients with essential thrombocythaemia: A single center study* Iwona Prajs A F, Kazimierz Kuliczkowski F Department and Clinic of Hematology, Blood
London Cancer. Myelofibrosis guidelines. August Review August Version v1.0. Page 1 of 12
 London Cancer Myelofibrosis guidelines August 2013 Review August 2013 Version v1.0 Page 1 of 12 CONTENTS 1. DIAGNOSIS... 3 1a. BCSH (2012)... 3 1b. WHO (2009) diagnostic criteria for PMF:... 4 2. MOLECULAR
London Cancer Myelofibrosis guidelines August 2013 Review August 2013 Version v1.0 Page 1 of 12 CONTENTS 1. DIAGNOSIS... 3 1a. BCSH (2012)... 3 1b. WHO (2009) diagnostic criteria for PMF:... 4 2. MOLECULAR
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
What is next: Emerging JAK2 inhibitor combination studies. Alessandro M. Vannucchi. Section of Hematology, University of Florence, Italy
 ymposium JAK2 Inhibition in Myelofibrosis: What Can We Expect in the Clinic? 4 5 May 2012 Lisbon, Portugal What is next: Emerging JAK2 inhibitor combination studies Alessandro M. Vannucchi ection of Hematology,
ymposium JAK2 Inhibition in Myelofibrosis: What Can We Expect in the Clinic? 4 5 May 2012 Lisbon, Portugal What is next: Emerging JAK2 inhibitor combination studies Alessandro M. Vannucchi ection of Hematology,
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016
 for Polycythemia Vera March 3, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ruxolitinib (Jakavi) for Polycythemia Vera March 3, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
New WHO Classification of Myeloproliferative Neoplasms
 New WHO Classification of Myeloproliferative Neoplasms Hans Michael Kvasnicka Senckenberg Institute of Pathology, University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Principles and rationale
New WHO Classification of Myeloproliferative Neoplasms Hans Michael Kvasnicka Senckenberg Institute of Pathology, University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Principles and rationale
Polycythemia Vera: From New, Modified Diagnostic Criteria to New Therapeutic Approaches
 Polycythemia Vera: From New, Modified Diagnostic Criteria to New Therapeutic Approaches Margherita Maffioli, MD, Barbara Mora, MD, and Francesco Passamonti, MD Drs Maffioli and Mora are hematologists in
Polycythemia Vera: From New, Modified Diagnostic Criteria to New Therapeutic Approaches Margherita Maffioli, MD, Barbara Mora, MD, and Francesco Passamonti, MD Drs Maffioli and Mora are hematologists in
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Influence of platelet and white blood cell counts on major thrombosis analysis from a patient registry in essential thrombocythemia
 European Journal of Haematology 97 (511 516) ORIGINAL ARTICLE Influence of platelet and white blood cell counts on major thrombosis analysis from a patient registry in essential thrombocythemia Veronika
European Journal of Haematology 97 (511 516) ORIGINAL ARTICLE Influence of platelet and white blood cell counts on major thrombosis analysis from a patient registry in essential thrombocythemia Veronika
CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management
 AJH CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management Author: Ayalew Tefferi If you wish to receive credit for this activity,
AJH CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management Author: Ayalew Tefferi If you wish to receive credit for this activity,
Chi sono i candidati agli inibitori di JAK2
 Chi sono i candidati agli inibitori di JAK2 Francesco Passamon, Hematology, University Hospital Varese, Italy Ruxoli8nib (US approved in MF; EAP study and compassionate use in Italy) SAR302503 (phase 3
Chi sono i candidati agli inibitori di JAK2 Francesco Passamon, Hematology, University Hospital Varese, Italy Ruxoli8nib (US approved in MF; EAP study and compassionate use in Italy) SAR302503 (phase 3
Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist
 Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist Wisconsin Institute of Discovery Karen Rossi/Bristol-Myers Squibb Morey A. Blinder, MD Washington University, St. Louis, MO March
Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist Wisconsin Institute of Discovery Karen Rossi/Bristol-Myers Squibb Morey A. Blinder, MD Washington University, St. Louis, MO March
JAK inhibitors in Phmyeloproliferative
 Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
Novel drugs in MPNs: Histone-Deacetylase Inhibitors
 Novel drugs in MPNs: HistoneDeacetylase Inhibitors 1st Annual Florence MPN Meeting April 16, 2011 Guido Finazzi Chronic Myeloproliferative Neoplasm Unit Division of Hematology Ospedali Riuniti di Bergamo,
Novel drugs in MPNs: HistoneDeacetylase Inhibitors 1st Annual Florence MPN Meeting April 16, 2011 Guido Finazzi Chronic Myeloproliferative Neoplasm Unit Division of Hematology Ospedali Riuniti di Bergamo,
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Subclinical AF: Implications of device based episodes
 Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Transplants for MPD and MDS
 Transplants for MPD and MDS The question is really who to transplant, with what and when. Focus on myelofibrosis Jeff Szer Royal Melbourne Hospital Myelodysplasia Little needs to be said Despite new therapies
Transplants for MPD and MDS The question is really who to transplant, with what and when. Focus on myelofibrosis Jeff Szer Royal Melbourne Hospital Myelodysplasia Little needs to be said Despite new therapies