Dr Calum Young Cardiologist Tauranga
|
|
|
- Lambert Morris
- 5 years ago
- Views:
Transcription

1 Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated)
2 GPCME 2016: Anticoagulation in 2016 Calum Young Cardiologist Tauranga
3 Format Why worry? The Burden of AF Five cases Discussion with each case A review of NOACs after Case Two A review of managing bleeding after Case Three Quiz (a very relaxed one!) Or, we can have a brief session on the basics and a longer tea break
4 The Burden of AF Overall prevalence in population is at least 1%, but rises with age (>10% of 80 year olds) Common incidental finding Management: Symptom control (rate versus rhythm control) Risk reduction Stroke Rate-related cardiomyopathy
5 The Burden of AF Overall prevalence in population is at least 1%, but rises with age (>10% of 80 year olds) Common incidental finding Management: Symptom control (rate versus rhythm control) Risk reduction Stroke Rate-related cardiomyopathy
6 The Burden of AF Stroke Risk: Is defined by (CHADS 2 -VASC 2 ): Congestive heart failure Hypertension Age (2 points if 75+ years) Diabetes Stroke/ TIA history (2 points) Vascular disease Sex
7 The Burden of AF Stroke Risk: NOT defined by: Pattern of AF (paroxysmal versus persistent) Left atrial size

8 The Burden of AF
9 What s Wrong With Warfarin?
10 What s Wrong With Warfarin? INR must be kept between strict boundaries (usually ) Risk of bleeds versus risk of stroke Fixed dose regimens a failure! Regular blood tests Rural patients, travellers, needle phobics, poor veins (although options now for finger-prick testing) Medication and dietary interactions Image problem: rat poison
11 What s Wrong With Warfarin? But Warfarin has been round for years Warfarin is cheap (INR testing* not necessarily so) Can be reversed with Vitamin K (orally or IV) *and you and your staff s non-reimbursed time
12 Case Studies One: Two: Three: Four: Five: Quiz Mrs Smith and her past brain bleed Which Drug or No Drug? NOACs and Googleitis I have AF and I need a stent! I have AF and a shiny new valve! Or: NOACs Summary and Managing Bleeds
13
14 Case One 76 year old female Atrial fibrillation which is minimally symptomatic CHADS2-VASC2 score of three (age, gender) 12 years ago, admitted with headache and noted to have a subdural haematoma (conservatively managed)- full recovery How do you manage anticoagulation?
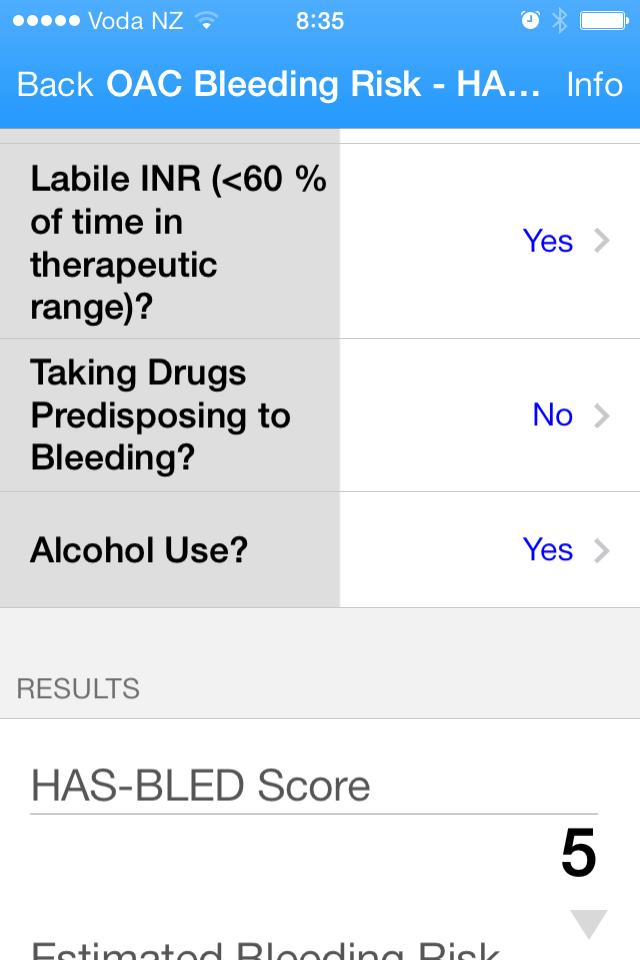
15 The Flipside of Anticoagulation Stroke Risk: Balance anticoagulation risk with bleeding risk (HAS-BLED) Hypertension Abnormal renal and liver function Stroke history Bleeding predisposition Labile INRs Elderly (>65 years) Drugs/ alcohol (include aspirin, NSAIDs)
16 The Flipside of Anticoagulation Stroke Risk: Balance anticoagulation risk with bleeding risk (HAS-BLED) Falls risk is generally considered now to have a minimal impact on decision to commence oral anticoagulation

17 The Flipside of Anticoagulation

18 The Flipside of Anticoagulation

19 The Flipside of Anticoagulation

20 The Flipside of Anticoagulation

21
22 Figure 1. Cumulative risk of recurrent intracranial hemorrhage (ICH) and ischemic event (IE) without resumption of warfarin (A) and from the time point of resuming warfarin (B). Ammar Majeed et al. Stroke. 2010;41: Copyright American Heart Association, Inc. All rights reserved.
23 Figure 2. The total risk for a treatment horizon of 3 years of recurrent intracranial hemorrhage and of ischemic stroke according to the time point of resumption of anticoagulation. Ammar Majeed et al. Stroke. 2010;41: Copyright American Heart Association, Inc. All rights reserved.

24 Case studies
25
26 Case Two Mr RB, NWU year old gentleman Vasculopathy: NSTEMI PCI RCA, with prior PCI RCA 2007 Past peripheral vascular surgery Renovascular disease with atrophic left kidney Creatinine 192, egfr 29 (stable) Paroxysmal AF- on warfarin (currently 3 and 4mg alternate days)
27 Case Two
28 Case Two How will you manage his anti-coagulation needs given this labile INR?
29 Case Two Not suitable for NOAC (renal function) Why the concern? Diet and concomitant medications Compliance issues Should we be more concerned about low or high INRs? High rates of ischaemic events once INR below 2.0 Home or Practice/ Pharmacy testing
30 Case Two What about non-pharmacological methods of stroke reduction?
31 Case Two What about non-pharmacological methods of stroke reduction? Watchman device FDA approved

32
33 Case studies
34 The Era of NOACs

35

36
37 NOACs in NZ Dabigatran (Pradaxa) available since 2011 in New Zealand Some criticism (eg from Haematologists) that introduction was hasty, and little consultation with them (or Cardiologists) Fully funded Licensed for: Non-valvular AF stroke prevention Post-operative DVT/ PE prophylaxis (75mg daily) And now, PE treatment
38 NOACs in NZ Dabigatran: AF: Dose 150mg BD, unless Age >75 or 80 years Impaired renal function, CrCl Post-operative DVT/ PE prophylaxis 220mg (or 150mg) once daily PE treatment 150mg BD
39 NOACs in NZ Re dabigatran and P-glycoprotein inhibitors: Do NOT need to adjust dose in presence of amiodarone use (but can elevate dabigatran levels 14-60%, nor with verapamil (21% dabigatran level increase) Avoid concomitant use with ketoconazole (150% dabigatran level increase) No clinical concerns with quinidine, clarithromycin
40 NOACs in NZ CARM received 345 reports of adverse reactions to dabigatran in the first three months A quarter involved prescriber error Up to a third of patients experience transient, or ongoing, dyspepsia (likely related to the tartaric acid in the dabigatran formulation)
41 NOACs in NZ Rivaroxaban (Xarelto) was funded via an early access programme in New Zealand until late mg once daily (10mg if CrCl 30-49) for non-valvular AF stroke prevention Also licensed for treatment of PE/ DVT
42 NOACs in NZ Apixaban (Eliquis) has limited funding via an early access programme in New Zealand via private Cardiologists only
43
44 The Trials RE-LY, 2009: dabigatran ROCKET-AF, 2011: rivaroxaban ARISTOTLE, 2011: apixaban ENGAGE-AF, 2013: edoxaban
45 RE-LY Trial (2009)
46 Connolly SJ et al. N Engl J Med 2009;361:

47 Connolly SJ et al. N Engl J Med 2009;361:

48 Connolly SJ et al. N Engl J Med 2009;361:
49 Cumulative Hazard Rates for the Primary Outcome of Stroke or Systemic Embolism, According to Treatment Group Connolly SJ et al. N Engl J Med 2009;361:

50 Safety Outcomes, According to Treatment Group Connolly SJ et al. N Engl J Med 2009;361:

51 Treatment Group Connolly SJ et al. N Engl J Med 2009;361:
52 Other NOAC Trials
53 ROCKET-AF, 2011 Patel MR et al. N Engl J Med 2011;365:
54 ARISTOTLE, 2011 Granger CB et al. N Engl J Med 2011;365:
55 ENGAGE-AF, 2013 Giugliano RP et al. N Engl J Med 2013;369:
56 Other Advantages for NOACs Quick spontaneous offset of action No prolonged time off agent required prior to elective surgery, and therefore less likelihood of requiring bridging therapy with heparin/ LMWH Is a definite rebound effect for strokes when stopping oral anticoagulants Prompt onset of action on re-commencement Avoidance of post-operative heparin/ LMWH
57 Switching to NOACs If patient is on warfarin, wait until INR is <2.0 before commencing NOAC Bridging therapy with heparin/ LMWH should not generally be required
58 The Trials Aspirin is now not recommended for stroke prophylaxis in AF Nothing (CHADS 2 VASC 2 0-1), vs Formal OAC Therapy
59 Case Studies
60 Case Three A patient brings in this online article regarding Pradaxa. What are the main issues for discussion? How might you respond to patient concerns?
61
62 Laboratory Monitoring of NOACs aptt TT DTI Specific Factor Xa assays INR levels are NOT reliable for NOAC monitoring
63 Laboratory Monitoring of NOACs Regulatory authorities do not recommend routine plasma measurement of NOAC activity Plasma levels may vary between individuals
64 Case Three New drugs Clinical Trials versus Real World What registries? The Hawthorne Effect Regulatory response to call for plasma monitoring of Dabigatran levels What role of patient selection? Does the presence of a reversal agent influence your response?
65 The Media and NOACs
66

67

68

69
70 Management of Bleeding Supportive care: Fluid resuscitation Red blood cell transfusions Maintenance of renal function Identification of bleeding source Surgical intervention

71

72
73 Issues with Pro-Coagulants TRALI Transfusion-Related Acute Lung Injury A severe reaction particularly to Fresh Frozen Plasma (FFP) Immune associations TACO Transfusion-Associated Circulatory Overload
74 Thirty-day mortality rate after a major bleeding event. Majeed A et al. Circulation. 2013;128: Copyright American Heart Association, Inc. All rights reserved.
75
76 Rivaroxaban Reversal Andexanet alfa 97% reduction in anti-factor Xa activity immediately after infusion FDA review decision pending (by August 2016) Case Studies
77
78 Case Four The patient with AF who needs PCI
79 Case Four The patient with AF who needs PCI Acknowledged that this is an individualised discussion that must be had with patient Strategy should revolve around minimising time on multiple blood-thinning agents Bare-metal stents versus Drug-eluting stents Biodegradable stents Drug-eluting balloons Case Studies
80
81 Case Five 79 year old man Diagnosed with AF 2015 on incidental examination St Judes Mechanical Aortic Valve replacement 2011 for severe aortic stenosis Follow-up echo in 2013 showed satisfactory valve function and normal LV systolic function Warfarin levels have been labile for last 6 months What are the options for oral anti-coagulation?
82 NOACs in NZ In March 2013, CARM reported three NZ cases of blood clots in mechanical valve patients using dabigatran (off label) RE-ALIGN study (published NEJM, September 2013) was terminated early after studying 252 mechanical valve patients randomised to warfarin or dabigatran- due to excess risk with dabigatran

83
84 NOACs in NZ Patients with mechanical heart valves (or severe underlying native valve issues- especially mitral stenosis) should NOT be treated with NOACs Warfarin is the only suitable agent in this group of patients Patients with bioprosthetic valves and AF can be treated with NOACs Case Studies
85 The Quiz
86 Question One: Which patient with atrial fibrillation would be the best potential candidate for dabigatran? a. 78 year old male with a mechanical mitral valve replacement b. 38 year old female with severe mitral stenosis c. 82 year old male with a bioprosthetic mitral valve replacement d. 72 year old female with a creatinine clearance of 18 e. 42 year old male with mechanical aortic valve replacement
87 Question Two: What statement is true? a. Apixaban is available for selected public Cardiology patients via an early access programme b. Rivaroxaban is given once daily c. Edoxaban is widely available overseas but not yet in New Zealand d. Overseas regulatory authorities have recommended avoiding commencing new patients on dabigatran pending new safety data e. Warfarin is safer than the new anticoagulant agents because it can be reversed by Vitamin K
88 Question Three: What statement is true? a. An INR level gives a good indication of plasma dabigatran levels b. Vitamin K can help reverse the effects of dabigatran c. Prior to elective surgery, dabigatran should be withheld for a week prior to the operation date d. When restarting dabigatran after surgery, subcutaneous low-molecular weight heparin should be given as bridging therapy for 3 days e. The half-life of dabigatran is hours
89 Question Four: What factor is least important when selecting appropriate patients (and dose) for NOACs? a. Age b. Patient weight c. Estimated risk of falls d. Renal function e. History of prior bleeding episodes
90 Question Five: What statement is true? a. Apixaban is a direct thrombin inhibitor b. Patients on dabigatran can choose to open the capsules and take the contents in a glass of water if that is easier for them c. Rivaroxaban cannot be packaged in blister packaging d. An antidote for dabigatran is potentially available in NZ e. You can switch a patient from warfarin to dabigatran as soon as the INR is less than 3.0
91 Question Six: My patient with a CHADS2-VASC2 score of 3 had a recent successful cardioversion, and has normal LV systolic function If he remains well and in sinus rhythm, we can stop his oral anticoagulation at 6 week follow-up: YES or NO? (or depends)
92 Quiz Answers
93 Question One: Which patient with atrial fibrillation would be the best potential candidate for dabigatran? a. 78 year old male with a mechanical mitral valve replacement b. 38 year old female with severe mitral stenosis c. 82 year old male with a bioprosthetic mitral valve replacement d. 72 year old female with a creatinine clearance of 18 e. 42 year old male with mechanical aortic valve replacement
94 Question Two: What statement is true? a. Apixaban is available for selected public Cardiology patients via an early access programme b. Rivaroxaban is given once daily c. Edoxaban is widely available overseas but not yet in New Zealand d. Overseas regulatory authorities have recommended avoiding commencing new patients on dabigatran pending new safety data e. Warfarin is safer than the new anticoagulant agents because it can be reversed by Vitamin K
95 Question Three: What statement is true? a. An INR level gives a good indication of plasma dabigatran levels b. Vitamin K can help reverse the effects of dabigatran c. Prior to elective surgery, dabigatran should be withheld for a week prior to the operation date d. When restarting dabigatran after surgery, subcutaneous low-molecular weight heparin should be given as bridging therapy for 3 days e. The half-life of dabigatran is hours
96 Question Four: What factor is least important when selecting appropriate patients (and dose) for NOACs? a. Age b. Patient weight c. Estimated risk of falls d. Renal function e. History of prior bleeding episodes
97 Question Five: What statement is true? a. Apixaban is a direct thrombin inhibitor b. Patients on dabigatran can choose to open the capsules and take the contents in a glass of water if that is easier for them c. Rivaroxaban cannot be packaged in blister packaging d. An antidote for dabigatran is potentially available in NZ e. You can switch a patient from warfarin to dabigatran as soon as the INR is less than 3.0
98 Question Six: My patient with a CHADS2-VASC2 score of 3 had a recent successful cardioversion, and has normal LV systolic function If he remains well and in sinus rhythm, we can stop his oral anticoagulation at 6 week follow-up: YES or NO? (or depends) Case Studies
99 Summary Current studies indicate that NOACs have a net benefit over warfarin Lower strokes Lower bleeding risk The lack of reversal agent for NOACs should be part of the routine patient discussion, but the issue is not necessarily straightforward Supportive therapies etc
100 Summary Currently fully-funded agents are: Warfarin Dabigatran Early-access funding for: Apixaban (generally private patients only) No current funding for: Rivaroxaban



101
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS
: COMPARISON AND FREQUENTLY ASKED QUESTIONS") NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS
 NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Appendix C Factors to consider when choosing between anticoagulant options and FAQs
 Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
Anticoagulation Task Force
 Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now. Bradley A. Hardin, MD Richard F.
 The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
Challenging Anticoagulation Case Studies. Earl J. Hope, M.D. Tower Health Cardiology
 Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator
 Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator at LAUMCRH Review the mechanism of action, indications
Nibal R. Chamoun, Pharm.D., BCPS Clinical Assistant Professor of Pharmacy Practice at the Lebanese American University Clinical Pharmacy Coordinator at LAUMCRH Review the mechanism of action, indications
Preventing Stroke in Patients with Atrial Fibrillation: USING THE EVIDENCE
 Preventing Stroke in Patients with Atrial Fibrillation: USING THE EVIDENCE What Is Atrial Fibrillation? Atrial fibrillation also called AFib or AF is the most common abnormal heart rhythm, affecting an
Preventing Stroke in Patients with Atrial Fibrillation: USING THE EVIDENCE What Is Atrial Fibrillation? Atrial fibrillation also called AFib or AF is the most common abnormal heart rhythm, affecting an
Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016
 1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
TSHP 2014 Annual Seminar 1
 Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA
 Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
Comparison of novel oral anticoagulants (NOACs)
") Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised
 DABIGATRAN RECOMMENDED What it is Indications Date decision last revised") Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
PRESENTATION TITLE. Case Studies
 PRESENTATION TITLE Case Studies 1) SH is a 67 year old male. He has a history of type 2 diabetes, controlled hypertension and peripheral artery disease. He takes naproxen 500mg bd for arthritis and admits
PRESENTATION TITLE Case Studies 1) SH is a 67 year old male. He has a history of type 2 diabetes, controlled hypertension and peripheral artery disease. He takes naproxen 500mg bd for arthritis and admits
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
NOACs in AF. Dr Colin Edwards Auckland Heart Group and Waitemata DHB. Dr Fiona Stewart Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
Aims. AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies
 in non-valvular AF (NVAF) Practical Issues Patient Case Studies") Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies AF and Stroke AF prevalence approx doubles with each
Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies AF and Stroke AF prevalence approx doubles with each
AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China
 AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China Case report 64-year-old Chinese man with history of hypertension,
AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China Case report 64-year-old Chinese man with history of hypertension,
Old and New Anticoagulants For Stroke Prevention Benefits and Risks
 Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
NOACs in AF. Dr Fiona Stewart. Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Fiona Stewart Auckland Heart Group and Auckland DHB NOACS for AF True/False All patients should have a CHA 2 DS 2 VASc risk assessment on diagnosis of AF NOACS are more effective than warfarin
NOACs in AF Dr Fiona Stewart Auckland Heart Group and Auckland DHB NOACS for AF True/False All patients should have a CHA 2 DS 2 VASc risk assessment on diagnosis of AF NOACS are more effective than warfarin
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Novel Anticoagulants: Emerging Evidence
 18/10/2016 Topics: Novel Anticoagulants: Emerging Evidence Dr Matthew Swale Electrophysiologist Genesis Care NOAC Novel Oral Anti Coagulant Now Non-Vit K Oral Anti Coagulant DOAC Direct Oral Anti Coagulant
18/10/2016 Topics: Novel Anticoagulants: Emerging Evidence Dr Matthew Swale Electrophysiologist Genesis Care NOAC Novel Oral Anti Coagulant Now Non-Vit K Oral Anti Coagulant DOAC Direct Oral Anti Coagulant
Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG:
 Atrial Fibrillation in Your Area Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG: a) What was the prevalence of atrial fibrillation (AF)? 6636 (as of 22/10/2015) 2.1%
Atrial Fibrillation in Your Area Question 1: Between 1 July 2014 and 30 June 2015, in the area covered by your CCG: a) What was the prevalence of atrial fibrillation (AF)? 6636 (as of 22/10/2015) 2.1%
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion
 Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion John Rickard MD, MPH Staff Electrophysiologist Cleveland Clinic Agenda NOACs: Update on Real World Data NOAC reversal:
Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion John Rickard MD, MPH Staff Electrophysiologist Cleveland Clinic Agenda NOACs: Update on Real World Data NOAC reversal:
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients. Giancarlo Agnelli
 NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
Dr Mammen Ninan GPwSI in Cardiology
 Dr Mammen Ninan GPwSI in Cardiology AF affects up to 835,000 people in England alone and is expected to rise year after year. AF is a known risk factor for stroke, the 3 rd highest cause of mortality in
Dr Mammen Ninan GPwSI in Cardiology AF affects up to 835,000 people in England alone and is expected to rise year after year. AF is a known risk factor for stroke, the 3 rd highest cause of mortality in
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
Updates in Atrial Fibrillation
 Updates in Atrial Fibrillation Michael Curley, MD Cardiac Electrophysiologist Wheaton Franciscan Medical Group #1 Most common heart rhythm disturbance 1 in 4 Americans over 40 will be diagnosed 3,500,000
Updates in Atrial Fibrillation Michael Curley, MD Cardiac Electrophysiologist Wheaton Franciscan Medical Group #1 Most common heart rhythm disturbance 1 in 4 Americans over 40 will be diagnosed 3,500,000
Anticoagulation Beyond Coumadin
 Anticoagulation Beyond Coumadin Saturday, September 21, 2013 Crystal Mountain Resort and Spa Pratik Bhattacharya MD, MPH Stroke Neurologist, Michigan Stroke Network; Assistant Professor of Neurology; Wayne
Anticoagulation Beyond Coumadin Saturday, September 21, 2013 Crystal Mountain Resort and Spa Pratik Bhattacharya MD, MPH Stroke Neurologist, Michigan Stroke Network; Assistant Professor of Neurology; Wayne
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING
 DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
New Age Anticoagulants: Bleeding Considerations
 Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Show Me the Outcomes!
 Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Stroke Prophylaxis in AFib. Anil K. Gehi, MD Associate Professor of Medicine
 Stroke Prophylaxis in AFib Anil K. Gehi, MD Associate Professor of Medicine Case #1 72 year-old woman with high blood pressure, osteoporosis, pacemaker Noted on routine pacemaker check to have atrial fibrillation
Stroke Prophylaxis in AFib Anil K. Gehi, MD Associate Professor of Medicine Case #1 72 year-old woman with high blood pressure, osteoporosis, pacemaker Noted on routine pacemaker check to have atrial fibrillation
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution
 Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
AF review. Petr Polasek
 AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Atrial Fibrillation. Alan Bell, MD, CCFP. Staff Physician, Humber River Regional Hospital. University of Toronto
 Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging
 and advances in peri-procedural interruption of anticoagulation-- Bridging") Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Analysing Apixaban: Potential Growth Driver for Pfizer and Bristol Myers Squibb. Tro Kalayjian Chief Medical Analyst Chimera Research Group
 Analysing Apixaban: Potential Growth Driver for Pfizer and Bristol Myers Squibb Tro Kalayjian Chief Medical Analyst Chimera Research Group Prevalence of AFib in the US is expected to increase upwards of
Analysing Apixaban: Potential Growth Driver for Pfizer and Bristol Myers Squibb Tro Kalayjian Chief Medical Analyst Chimera Research Group Prevalence of AFib in the US is expected to increase upwards of
Reversal of Novel Oral Anticoagulants. Angelina The, MD March 22, 2016
 Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Drug Class Monograph
 Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
controversies in anticoagulation: optimizing outcome for atrial fibrillation
 controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Patients presenting with acute stroke while on DOACs
 Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention
 Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania
Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania
Management of Atrial Fibrillation in the Hospitalized Patient
 Management of Atrial Fibrillation in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research:
Management of Atrial Fibrillation in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research:
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Content 1. Relevance 2. Principles 3. Manangement
 Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Is Apixaban Effective for the Prevention of Stroke in Patients With Non-Valvular Atrial Fibrillation?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2014 Is Apixaban Effective for the Prevention
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2014 Is Apixaban Effective for the Prevention
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
NEWSLETTER DUE CARE PROGRAM. WINTER 2014 Summer 2015 COMMONLY ASKED QUESTION:
 DUE CARE PROGRAM NEWSLETTER WINTER 2014 Summer 2015 Lisa Sather, RPh DUR Coordinator Mountain-Pacific Quality Health 3404 Cooney Drive Helena, MT 59602 406-457-5818 The DUE CARE PROGRAM, administered by
DUE CARE PROGRAM NEWSLETTER WINTER 2014 Summer 2015 Lisa Sather, RPh DUR Coordinator Mountain-Pacific Quality Health 3404 Cooney Drive Helena, MT 59602 406-457-5818 The DUE CARE PROGRAM, administered by
Atrial Fibrillation. 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018
 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Dr Chris Ellis. Consultant Cardiologist Auckland City Hospital Auckland
 Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Southern Trust Anticoagulant Team
 CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Anticoagulation- Primary Care Guidance for reviewing patients on DOACs Southern Trust Anticoagulant Team Haematology Acute
CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Anticoagulation- Primary Care Guidance for reviewing patients on DOACs Southern Trust Anticoagulant Team Haematology Acute
Scoring Systems in AF 8/10/2016. Strategies in the Prevention of Atrial Fibrillation-Related Strokes. Overview
 Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Atrial fibrillation: current approaches to management
 DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
Engage AF-TIMI 48. Edoxaban in AF: What can we expect? Cardiology Update John Camm. St. George s University of London United Kingdom
 Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
Novel Oral An,coagulants: Prac,cal Aspects. Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015
 Novel Oral An,coagulants: Prac,cal Aspects Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015 The New Oral An,coagulants (NOACs) The Non VKA Oral An,coagulants (NOACs)
Novel Oral An,coagulants: Prac,cal Aspects Caroline Berube, MD Clinical Associate Professor Division of Hematology November 2015 The New Oral An,coagulants (NOACs) The Non VKA Oral An,coagulants (NOACs)
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Anticoagulation in 2014: Using the New Agents Safely
 Anticoagulation in 2014: Using the New Agents Safely Tracy Minichiello, M.D. Professor of Medicine University of California, San Francisco Chief, SF VA Anticoagulation & Thrombosis Service Disclosures
Anticoagulation in 2014: Using the New Agents Safely Tracy Minichiello, M.D. Professor of Medicine University of California, San Francisco Chief, SF VA Anticoagulation & Thrombosis Service Disclosures
Modern Management in Primary Care (AF1)
") Modern Management in Primary Care (AF1) Dr Ravi Assomull Consultant Cardiologist London North West Healthcare NHS Trust Dr Yassir Javaid Primary Care Cardiovascular Lead East Midlands Strategic Clinical
Modern Management in Primary Care (AF1) Dr Ravi Assomull Consultant Cardiologist London North West Healthcare NHS Trust Dr Yassir Javaid Primary Care Cardiovascular Lead East Midlands Strategic Clinical
requesting information regarding atrial fibrillation in NHS Ashford Clinical Commissioning Group
 October 2015 Our Ref: FOI.15.ASH0149 requesting information regarding atrial fibrillation in NHS Ashford Clinical Commissioning Group Original Request Survey attached. Question 1: Between 1 July 2014 and
October 2015 Our Ref: FOI.15.ASH0149 requesting information regarding atrial fibrillation in NHS Ashford Clinical Commissioning Group Original Request Survey attached. Question 1: Between 1 July 2014 and
Patient with high risk for bleeding
 Will Apixaban change practice in atrial fibrillation Luncheon Satellite Sponsored by Pfizer Patient with high risk for bleeding Prof. Amos Katz M.D August 2012: patient background 67-year-old woman History
Will Apixaban change practice in atrial fibrillation Luncheon Satellite Sponsored by Pfizer Patient with high risk for bleeding Prof. Amos Katz M.D August 2012: patient background 67-year-old woman History
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Rate or Rhythm Control? Epidemiology. Relevant Advances in Atrial Fibrillation 6/20/2011. Stroke Prophylaxis
 Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis
 Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Are the days of Warfarin numbered?
 2 nd SAVTE Symposium Are the days of Warfarin numbered? YES Dr. Mohamed A. Abdelaal, MD, FRCPath, FRCPI Consultant Haematologist King Abdulaziz Medical City - Jeddah, Saudi Arabia 1 3 May 2012, Casablanca,
2 nd SAVTE Symposium Are the days of Warfarin numbered? YES Dr. Mohamed A. Abdelaal, MD, FRCPath, FRCPI Consultant Haematologist King Abdulaziz Medical City - Jeddah, Saudi Arabia 1 3 May 2012, Casablanca,
ADVANCES IN ANTICOAGULATION
 ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease
 Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy