Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention
|
|
|
- Adrian Cole
- 6 years ago
- Views:
Transcription
1 Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania April 25, 2014 Disclosures None 1
2 Objectives Identify individualized anticoagulant therapy using risk stratification for patients with atrial fibrillation Evaluate the latest clinical data on current and novel anticoagulants Assess the guideline recommendations for anticoagulant and antiplatelet therapy Examine management strategies to improve adherence to anticoagulation therapies Atrial fibrillation Most common arrhythmia in clinical practice Affects >3 million Americans and estimated to reach 16 million by 2050 Responsible for 1 in 5 strokes in US 90% of thromboembolism in AF originates in the left atrial appendage 2


3 CHADS 2 scores establish risk of stroke CHADS 2, developed and validated by Gage et al, is a system for establishing the risk of stroke in patients with non rheumatic atrial fibrillation 1 Patients are awarded points based on comorbidities Condition Points C Congestive heart failure 1 H Hypertension 1 A Age 75 years 1 D Diabetes mellitus 1 S 2 Previous stroke or TIA 2 European Society of Cardiology Guidelines 2 CHADS 2 Score Treatment 0 Aspirin 1 Aspirin or warfarin* 2 Warfarin Risk of Stroke 20% 18% 15% 13% 10% 8% 5% 3% 0% Annual Risk of Stroke 18.2% 12.5% 8.5% 5.9% 4.0% 2.8% 1.9% CHADS 2 Score * Use of aspirin or warfarin is based on additional patient characteristics such as age, number of risk factors, etc. 1 Gage BF et al, JAMA 2001;285: Camm AJ et al, Eur Heart J 2010;31: CHA 2 DS 2 VASc is a newer scoring system CHA 2 DS 2 VASc, developed by Lip et al, is a refinement of the older CHADS 2 Score which includes additional stroke risk factors and puts greater emphasis on age as a risk factor 1 Condition/Risk Factor Points C Congestive heart failure 1 H Hypertension 1 A Age 75 years 2 D Diabetes mellitus 1 S 2 Previous stroke or TIA 2 V Vascular disease 1 A Age years 1 Sc Sex (female gender) 1 European Society of Cardiology Guidelines 2 Risk of Stroke 18% 15% 12% 9% 6% 3% 0% CHA 2 DS 2 -VASc Score Treatment 0 No treatment 1 Aspirin or warfarin or dabigatran 2 Warfarin or dabigatran Annual Risk of Stroke 15.2% 9.8% 9.6% 6.7% 6.7% 3.2% 4.0% 2.2% 1.3% 0.0% CHA 2 DS 2 VASc Score 1 Lip GY et al, Chest. 2010;137(2): Camm AJ et al, Eur Heart J. 2010;31:
4 How do they Compare? Generally, they result in similar treatment recommendations Where they are the same: Both CHADS systems assign 1 point each for presence of congestive heart failure (any), hypertension and diabetes Both CHADS systems assign 2 points for prior TIA or stroke Where they differ: CHA 2 DS 2 VASc puts greater emphasis on age, assigning 1 point for age between years, and 2 points for age >75 years. CHADS 2 only assigns one point for age >75 years CHA 2 DS 2 VASc adds 1 point each for presence of any vascular disease and female gender, which are not included in the CHADS 2 score The Coagulation Cascade Antiplatelet agents: Aspirin, clopidogrel, NSAIDS, dipyridamole Rivaroxaban, Apixaban Dabigatran 4
5 Warfarin effective but limitations exist When taken appropriately, warfarin is effective Monitoring required to ensure therapeutic range (INR) Many foods and medicines interact with warfarin Despite efficacy, warfarin exposes patients to risks (e.g. intracranial hemorrhage and hemorrhagic stroke) Warfarin use represents a challenge to surgeries High rates of discontinuation and non adherence to therapy Warfarin tops the list for emergency hospitalizations for adverse drug events in older Americans 1 1 Budnitz DS, et al. NEJM 2011, 365: Novel Oral Anticoagulants 5
6 Dabigatran RE LY: Randomized Evaluation of Long Term Anticoagulation Therapy Comparison: Stroke or systemic embolism (efficacy) and Major bleeding (safety) Dabigatran 110 mg bid vs Dabigatran 150 mg bid vs Warfarin (INR 2 3) Patients: N = 18,113 with nonvalvular AF + age 75 yrs, previous stroke/tia, LVEF <40%, or Class II-IV CHF; or Age yrs with DM, HTN, or CAD Design: Blinded dabigatran/open-label warfarin Parallel-group, RCT, 1:1:1 randomized Designed as non-inferiority trial Connolly SJ et al. N Engl J Med. 2009;36:
7 RE-LY Trial Reduce the risk of stroke and systemic embolism in patients with non-valvular atrial fibrillation Dabigatran 110 mg PO BID or 150 mg PO BID (blinded) to open-label warfarin 1, 3, or 5 mg (goal INR 2-3) in patients with non-valvular Afib and one or more of the following risk factors: Previous stroke, TIA, or systemic embolism LVEF<40% Symptomatic heart failure, NYHA class >2 Age >75 years Age >65 years with DM, CAD, or HTN 18,113 patients randomized and followed for a median of 2 years Time in Therapeutic Range (TTR) for warfarin: 64% (mean) Dabigatran 150 mg bid compared to warfarin had an approximate 35% decreased risk (RR 0.66, 95% CI , p<0.001) in the primary efficacy event of stroke or systemic embolism Dabigatran 150 mg bid had a trend towards increased risk of bleeding compared to warfarin in major bleeding (not statistically significant) and showed a greater risk for life-threatening bleeding (RR 0.81, 95% CI , p = 0.04) and for GI bleeding (RR 1.50, 95% CI , p<0.001) Design of RE LY: A Non inferiority Trial Randomized Evaluation of Long-Term Anticoagulation Therapy Atrial fibrillation 1 Stroke risk factors Absence of contraindications Blinded event adjudication R Primary outcome: Stroke or systemic embolism Open Blinded Warfarin (Adjusted INR ) n = 6022 Dabigatran 110 mg bid n = 6015 Dabigatran 150 mg bid n = 6076 Follow up: 1-yr minimum, 2-yr median, 3-yr maximum Connolly SJ et al. N Engl J Med. 2009;361:
8 RE LY: Stroke or Systemic Embolism Cumulative hazard rate % P < Warfarin Months Dabigatran 110 Dabigatran 150 Connolly SJ et al. N Engl J Med. 2009;361: RE LY: Bleeding and Net Clinical Benefit Net clinical benefit = Composite of stroke, systemic embolism, MI, pulmonary embolism, death, or major bleeding D 110 mg D 150 mg Warfarin D 110 mg vs warfarin D 150 mg vs warfarin Annual rate Annual rate Annual rate RR (95% CI) P RR (95% CI) P Major bleeding 2.71% 3.11% 3.36% 0.80 ( ) ( ) 0.31 Minor bleeding 13.16% 14.84% 16.37% 0.79 ( ) < ( ) Intracranial bleeding 0.23% 0.30% 0.74% 0.31 ( ) < ( ) <0.001 Net clinical benefit 7.09% 6.91% 7.64% 0.92 ( ) ( ) 0.04 D = dabigatran Connolly SJ et al. N Engl J Med. 2009;361:
9 Dabigatran (Pradaxa) Class: Direct thrombin inhibitor Dose: 150 mg PO bid 75 mg PO bid for CrCl < 30 ml/min (dose not studied) FDA indications: Prevention of stroke or systemic embolism in patients with non-valvular atrial fibrillation Pharmacokinetics: Absorption: absolute oral bioavailability 3-7%; rapid absorption Metabolism: Rapidly and completely converted to dabigatran by esterase-catalyzed hydrolysis; not a CYP450 substrate, inducer, or inhibitor. P-glycoprotein substrate: Avoid use with P-gp inducers (i.e. rifampin); may use with concominant p-gp inhibitors (i.e. ketoconazole, verapamil, amiodarone, clarithromycin) but bioavailability of dabigatran is decreased. Elimination: t 1/2 = hours; 80% renally eliminated Dabigatran (Pradaxa) Monitoring: - aptt: a value 2.5 x normal may indicate overanticoagulation For efficacy, median peak for 150 mg bid dose was ~2x control and was ~1.5x control measured 12 hours after the last dose. Median trough in trial of patients receiving 150 mg bid dose was 52 (40 to 76) seconds. -Ecarin Clotting Time (ECT): median trough in trial of patients receiving the 150 mg bid dose was 64 (44 to 103) seconds Reversal: Maintain adequate diuresis; 60% is dialyzable Fresh frozen plasma PRBC (packed red blood cells) Prothrombin complex concentrates Recombinant Factor VIIa Contraindications: Active bleeding or hypersensitivity to dabigatran 9
10 Dabigatran (Pradaxa) Considerations for surgery: CrCl>50mL/min: D/C drug 1-2 days before procedure CrCl<50mL/min: D/C drug 3-5 days before procedure If major surgery, spinal puncture, or epidural catheter or port is scheduled, consider discontinuing dabigatran for longer times Assess bleeding risk with ECT or aptt Storage Requirements: Both blister packs and bottles must be stored at 77 F. Capsules need to be kept in their original containers until they are used to protect from moisture and avoid potency loss. The product should be used within 4 months of opening the bottle. Conversion from and to Warfarin Converting from warfarin to dabigatran: Discontinue warfarin and start dabigatran when INR <2 Converting to warfarin from dabigatran, recommended start times based on renal function. If CrCl: >50 ml/min, start warfarin 3 days before stopping dabigatran ml/min, start warfarin 2 days before stopping dabigatran ml/min, start warfarin 1 day before stopping dabigatran <15 ml/min, no recommendation made Source: lderpath=/prescribing%20information/pis/pradaxa/pradaxa.pdf 10
11 Rivaroxoban ROCKET AF: Protocol Schema Atrial fibrillation Rivaroxaban 20 mg daily 15 mg for CrCl Randomize Double-blind; Double dummy (N ~ 14,000) Warfarin INR target ( inclusive) 2 of: CHF Hypertension Age 75 Diabetes AND/OR Stroke, TIA, or systemic embolus Monthly monitoring and adherence to standard of care guidelines Primary endpoint: Stroke or non-cns systemic embolism Statistics: Non-inferiority, >95% power, 2.3% warfarin event rate ROCKET AF Investigators. Am Heart J. 2010;159:

12 Rivaroxaban vs Warfarin Efficacy outcomes Stroke/Systemic embolism Hemorrhagic stroke Myocardial infarction Safety outcomes ICH Major bleeding Rivaroxaban better Warfarin better Patel MR et al. N Engl J Med. 2011;365:883-91; Fox KAA et al. Eur Heart J. 2011;32:
13 ROCKET AF Prevention of stroke or systemic embolism in atrial fibrillation ROCKET AF Rivaroxaban 20 mg PO once daily vs. adjusted dose warfarin (target INR of 2-3) Patients with CrCl ml/min use rivaroxaban 15 mg PO once daily Primary efficacy endpoint: composite of ischemic or hemorrhagic stroke and systemic embolism Rivaroxaban demonstrated non-inferiority in primary endpoint HR (hazard ratio) 0.79 (95% CI ) in the per-protocol population and in the intent-to-treat population (p<0.001). Rivaroxaban did NOT demonstrate superiority in the intent-to-treat population» HR 0.88 (95% CI ) statistically NOT significant (p=0.12) Primary safety endpoint: composite of major and clinically relevant nonmajor bleeding events Major and nonmajor bleeding events remained similar between 2 groups HR 1.03 (95% CI ) statistically NOT significant Increased incidence of GI bleeding (3.2%) vs. warfarin (2.2%, p<0.001). ROCKET AF Limitations: Exclusion criteria:» Patients with mechanical valves» Patients taking aspirin >100 mg/day, and aspirin in combination w/ thienopyridine» Concomitant medications (i.e. CYP3A4 inhibitors, inducers, chronic use of NSAIDs) Possible violation of constancy assumption for non-inferiority margin» Study population had higher risk patients CHADS2 score 3.47» Lower mean time-in-therapeutic range (TTR) of 55% compared to other studies (62 to 73%) 13
14 Prescribing information Dabigatran Rivaroxaban Indication To reduce the risk of stroke and systemic embolism in patients with non-valvular AF Dosage CrCl >30 ml/min: 150 mg bid CrCl ml/min: 75 mg bid CrCl >50 ml/min: 20 mg qd CrCl ml/min: 15 mg qd er?docbase=renetnt&folderpath=/prescribi ng%20information/pis/pradaxa/pradaxa.pdf m/sites/default/files/pdf/xa relto_0.pdf#zoom=100 Rivaroxaban (Xarelto) Class: Direct Factor Xa inhibitor Non-FDA Indications: Prevention of stroke or systemic embolism in patients with atrial fibrillation Pharmacokinetics: Absorption: bioavailability of %, take with or without food Metabolism: P-glycoprotein, CYP3A4 substrate Concomitant use of inhibitors will anticoagulant effect Inducers will anticoagulant response If use is unavoidable, can give 20 mg once daily taken with food. Avoid use in patients with moderate or severe hepatic impairment (Child-Pugh B or C). Elimination: half-life of 5-9 h, h (elderly); 66% (renal), 34% (feces) Avoid use in patients with CrCl < 30 ml/min. Caution in patients with CrCl 30 to 50 ml/min monitoring recommended 14
15 Rivaroxaban (Xarelto) Contraindications/Warnings: Black Box Warning: Epidural or spinal hematomas can occur in patients who are anticoagulated and are receiving neuraxial anesthesia or undergoing spinal puncture Hepatic disease Bleeding Concomitant strong CYP3A4, P-glycoprotein inhibitors and inducers Pregnancy Breastfeeding Monitoring: bleeding complications (incidence: 5.8%) Routine monitoring not required Anti-factor Xa assays Most reliable Assays are not standardized and no therapeutic level has been established Prothrombin time (PT)/ INR Dose dependent with PT No standardized assay; INR is standardized for warfarin only Activated partial thromboplastin time (aptt) Not very effective since prolongation only seen at peak drug levels Rivaroxaban (Xarelto) Reversal: No standard antidote Factor VIIa (theoretical due to benefit with fondaparinux(arixtra)) Cost: ~$10,000 for single 90 µg/kg dose in 80 kg patient Prothrombin complex concentrate (PCC) (theoretical) Usefulness in clinical settings not yet established Fresh frozen plasma Short-term reversal, short half-life of 3-5 hours Activated charcoal Considerations for surgery: No exact guidelines established Timing for stopping rivaroxaban will be dependent on half-life 15
")
16 Apixaban (Eliquis) 16
. Intracranial hemorrhage 0.33% per year with apixaban and 0.8% per year with warfarin Rate of any bleeding was 25.")
17 Hemorrhagic stroke 49% lower Ischemic Stroke 8% lower Fatal/Disabling stroke 0.5% per year vs 0.71% Bleeding 327 patients in the apixaban group (2.13% per year as compared with 462 patients in the warfarin group (3.09% per year). Intracranial hemorrhage 0.33% per year with apixaban and 0.8% per year with warfarin Rate of any bleeding was 25.8% per year in the warfarin group and 18.1% in the apixaban group. Absolute reduction of 7.7 percentage points. Fatal bleeding occurred in 34 patients in the apixaban group & 55 patients in the warfarin group 17
18 Class: Factor Xa inhibitor Apixaban(Eliquis) MOA: Direct-acting, reversible factor Xa inhibitor. Inhibits the conversion of prothrombin to thrombin. Dose: 5 mg po BID for patients with non-valvular AF. Decrease to 2.5 mg po BID w/ 2 of the following (age >80, <60 kg, Creat>1.5 Pharmacokinetics: Absorption: rapidly absorbed, reach Cmax within 1-3 hours; 66% bioavailability Metabolism: CYP3A4 substrate to inactive metabolite O- demethyl-apixaban. Drug interactions: Potent 3A4 inhibitors Elimination: t 1/2 12 hours; 25% renally and 55% fecally eliminated. Apixaban(Eliquis) ADRs: Bleeding (6%), nausea (7%), vomiting (5%), constipation (5%) in ADVANCE trials. Elevation of LFTs (the incidence rate was no different from the comparator groups) ALT >3X ULN (~1.1% in ADVANCE-I and ARISTOTLE trials) Monitoring: No routine monitoring is required Anti factor Xa assay Linear relationship between apixaban plasma concentration and factor Xa inhibition No standardized assay Prothrombin time/inr Reversal agent: No standard antidote investigational agent PRT064445: designed to reverse the actions factor Xa inhibitors. preclinical study results demonstrated reversal effects of anticoagulation by enoxaparin, fondaparinux, both factor Xa inhibitors in an animal model. Prothrombin complex concentrates (theoretical) Recombinant factor VII (theoretical) Activated charcoal (preclinical study- reduced apixaban exposure) 18
19 The Bottom Line on Alternatives to Warfarin Dabigatran, rivaroxaban and apixaban have demonstrated safety and efficacy in clinical trials However, real world and long term efficacy and safety and drug interactions have yet to be investigated While new oral anticoagulants may avoid the burden of regular INR monitoring, bleeding risks and high rates of non adherence are still a problem A need exists for an effective means of stroke reduction that does not expose patients to bleeding events or require long term patient adherence Edoxaban 19
20 Inclusion criteria: ENGAGE AF TIMI 21 years of age AF documented within 12 months of randomization CHADS 2 risk assessment 2 Anticoagulation therapy planned for duration of trial Exclusion criteria AF due to reversible disorder Estimated CrCl < 30mL/min High risk of bleeding Use of dual antiplatelet therapy Moderate to severe mitral stenosis Acute coronary syndrome Coronary revascularization stroke within 30 days before randomization Non-compliance to study procedure Design of ENGAGE AF TIMI 48 Patients with moderate to high risk AF Randomize Double-blind; Double dummy (N =21,105) Edoxaban High dose: 60 mg OR Low dose: 30 mg (CrCl 30 50) Warfarin INR 2 3 Study visits on days 8, 15, 29, 60, 3 months and every 3 months thereafter for duration of study 20
21 ENGAGE AF TIMI 48 Primary efficacy end point: stroke or systemic embolism Intent-to-treat analysis found favoring trend high dose Edoxaban vs. warfarin (HR, 0.87; 97.5% CI, 0.73 to 1.04; P=0.08). Intent-to-treat analysis found unfavorable trend with low dose Edoxaban vs. warfarin (HR, 1.13; 97.5% CI, 0.96 to 1.34; P=0.10). Principal safety end point: major bleeding Annualized bleeding events higher with warfarin, 3.43% as compared to high dose Edoxaban at 2.75% (HR, 0.80; 95% CI, 0.71 to 0.91; P<0.001) and low dose Edoxaban at 1.61% (HR, 0.47; 95% CI, 0.41 to 0.55; P<0.001) Major GI bleeding was higher with high dose Edoxaban (1.51%) vs. warfarin (1.23%), and lowest with low dose Edoxaban (0.82%). ENGAGE AF TIMI 48: Primary Efficacy 21
22 Principal Safety Endpoint Conclusions of ENGAGE AF TIMI 48 Low dose and high dose Edoxaban were noninferior to warfarin for prevention of stroke or systemic embolism and were associated with significantly lower rates of bleeding and death from cardiovascular causes. High dose Edoxaban resulted in more GI bleeding versus warfarin and low dose Edoxaban. 22
23 Summary of the 4 NOACs PK/PD of 4 Novel Oral Agents Target Dabigatran Apixaban Rivaroxaban IIa (thrombin) Edoxaban (DU-176b) Xa Xa Xa Hrs to Cmax CYP Metabolism None 15% 32% NR Half-Life 12-14h 8-15h 9-13h 8-10h Renal Elimination 80% 25% 66% 35% CYP = cytochrome P450; NR = not reported Ruff CR and Giugliano RP. Hot Topics in Cardiology 2010; 4: 7-14 Ericksson BI et al. Clin Pharmacokinet 2009; 48: 1-22 Ruff CR et al. Am Heart J 2010; 160:
24 Phase III AF trials RE-LY ROCKET AF ARISTOTLE ENGAGE AF-TIMI 48 Drug Dabigatran Rivaroxaban Apixaban Edoxaban Dose (mg) Freq 150, 110 BID 20 (15*) QD 5 (2.5*) BID 60*, 30* QD N 18,113 14,266 18,206 >21,000 Design PROBE 2 x blind 2 x blind 2 x blind AF criteria AF x 1 <6 mths AF x 2 ( 1 in <30d) AF or AFI x 2 <12 mths AF x 1 <12 mths % VKA naive 50% 38% 43% 40% goal *Dose adjusted in patients with drug clearance. **Max of 10% with CHADS-2 score = 2 and no stroke/tia/see PROBE = prospective, randomized, open-label, blinded end point evaluation VKA = Vitamin K antagonist RE-LY Dabigatran 110 mg Dabigatran 150 mg Warfarin CHADS 2 Mean 0-1 (%) 2 (%) 3+ (%) ROCKET AF Rivaroxaban Warfarin CHADS 2 Mean 2 (%) 3 (%) 4 (%) 5 (%) 6 (%) % ARISTOTLE Apixaban Warfarin CHADS 2 Mean 0-1 (%) 2 (%) 3+ (%) ENGAGE AF-TIMI 48 Edoxaban 60 mg Edoxaban 30 mg Warfarin CHADS 2 Mean 3 (%) 4-6 (%)
 RE-LY ROCKET AF ARISTOTLE ENGAGE AF 64% 58% 62% 68%")
25 Comparison of Trial Metrics Time in Therapeut ic Range (TTR) RE-LY ROCKET AF ARISTOTLE ENGAGE AF 64% 58% 62% 68% 25
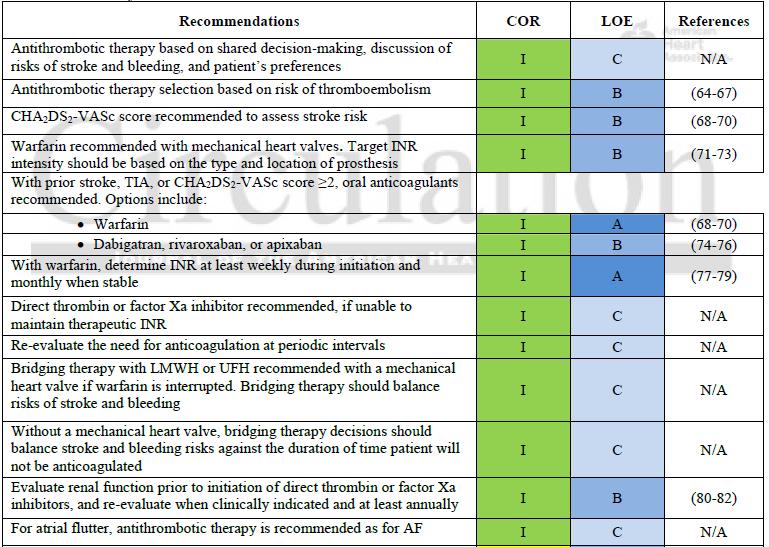

26 Summary of recommendations Summary of Recommendations 26


27 Dosing Recommendations Conclusions PROTECT THE BRAIN! PROTECT THE BRAIN! PROTECT THE BRAIN! Many AF patients, who should be anticoagulated, are not being treated Variety of anticoagulants that can be used to protect against thromboembolic risk in AF Provides the clinician a greater opportunity to select AN anticoagulant 27
Scoring Systems in AF 8/10/2016. Strategies in the Prevention of Atrial Fibrillation-Related Strokes. Overview
 Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients. Giancarlo Agnelli
 NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Beyond Coumadin
 Anticoagulation Beyond Coumadin Saturday, September 21, 2013 Crystal Mountain Resort and Spa Pratik Bhattacharya MD, MPH Stroke Neurologist, Michigan Stroke Network; Assistant Professor of Neurology; Wayne
Anticoagulation Beyond Coumadin Saturday, September 21, 2013 Crystal Mountain Resort and Spa Pratik Bhattacharya MD, MPH Stroke Neurologist, Michigan Stroke Network; Assistant Professor of Neurology; Wayne
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
Stepheny Sumrall, FNP, AGACNP Cardiovascular Clinic of Hattiesburg
 Novel Oral Anticoagulants Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for the Treatment of Atrial Fibrillation and Prevention of Stroke Stepheny Sumrall,
Novel Oral Anticoagulants Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for the Treatment of Atrial Fibrillation and Prevention of Stroke Stepheny Sumrall,
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Old and New Anticoagulants For Stroke Prevention Benefits and Risks
 Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now. Bradley A. Hardin, MD Richard F.
 The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
Novel Anticoagulants PHYSICIANS UPDATE 2014
 Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Engage AF-TIMI 48. Edoxaban in AF: What can we expect? Cardiology Update John Camm. St. George s University of London United Kingdom
 Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
Arrhythmias and Clinical EP Contemporary Management of Anticoagulant Therapies
 Arrhythmias and Clinical EP Contemporary Management of Anticoagulant Therapies Samuel Asirvatham, MD & Ivan Mendoza, MD Saturday, June 24, 2017 11:15 a.m. to 12 p.m. Disclosures Relevant financial relationship(s)
Arrhythmias and Clinical EP Contemporary Management of Anticoagulant Therapies Samuel Asirvatham, MD & Ivan Mendoza, MD Saturday, June 24, 2017 11:15 a.m. to 12 p.m. Disclosures Relevant financial relationship(s)
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation Topics for Today. Clinical Controversies Management of Atrial Fibrillation. Atrial Fibrillation in the ER Topics for Today
 Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
David Stewart, PharmD, BCPS Assistant Professor of Pharmacy Practice East Tennessee State University Bill Gatton College of Pharmacy
 David Stewart, PharmD, BCPS Assistant Professor of Pharmacy Practice East Tennessee State University Bill Gatton College of Pharmacy stewardw@etsu.edu At the conclusion of this program, the audience should
David Stewart, PharmD, BCPS Assistant Professor of Pharmacy Practice East Tennessee State University Bill Gatton College of Pharmacy stewardw@etsu.edu At the conclusion of this program, the audience should
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
Lessons from recent antithrombotic studies and trials in atrial fibrillation
 Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Professional Practice Minutes December 7, 2016
 Professional Practice Minutes December 7, 2016 **New Opportunity for Patient Education** We can now request the educational videos we want our patients to watch after our visit. Video topics include colon
Professional Practice Minutes December 7, 2016 **New Opportunity for Patient Education** We can now request the educational videos we want our patients to watch after our visit. Video topics include colon
Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016
 1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
Newer Anti-Anginal Agents and Anticoagulants
 Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
Thrombosis and Thromboembolsim October Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy
 Thrombosis and Thromboembolsim October 2012 Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy Christian T. Ruff, MD, MPH TIMI Study Group Brigham and Women
Thrombosis and Thromboembolsim October 2012 Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy Christian T. Ruff, MD, MPH TIMI Study Group Brigham and Women
Antithrombotic Efficacy and Safety of Dabigatran Etexilate
 130419 Luncheon Symposium_2013 춘계심장학회 Antithrombotic Efficacy and Safety of Dabigatran Etexilate Hui-Nam Pak, MD, PhD. Division of Cardiology Yonsei University Health System Atrial Fibrillation Risk of
130419 Luncheon Symposium_2013 춘계심장학회 Antithrombotic Efficacy and Safety of Dabigatran Etexilate Hui-Nam Pak, MD, PhD. Division of Cardiology Yonsei University Health System Atrial Fibrillation Risk of
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS
: COMPARISON AND FREQUENTLY ASKED QUESTIONS") NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Anticoagulation Task Force
 Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS
 NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants
 Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants Van Hellerslia, PharmD, BCPS, CACP Clinical Assistant Professor Temple University School of Pharmacy Over 4 million
Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants Van Hellerslia, PharmD, BCPS, CACP Clinical Assistant Professor Temple University School of Pharmacy Over 4 million
Edoxaban in Atrial Fibrillation
 Edoxaban in Atrial Fibrillation Glenn Gormley, MD, PhD Senior Executive Officer and Global Head of R&D, Daiichi Sankyo Co., Ltd Nov. 4, 2014 Tuesday Background Based on the results of ENGAGE AF-TIMI 48,
Edoxaban in Atrial Fibrillation Glenn Gormley, MD, PhD Senior Executive Officer and Global Head of R&D, Daiichi Sankyo Co., Ltd Nov. 4, 2014 Tuesday Background Based on the results of ENGAGE AF-TIMI 48,
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
TSHP 2014 Annual Seminar 1
 Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
NOACs in AF. Dr Colin Edwards Auckland Heart Group and Waitemata DHB. Dr Fiona Stewart Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
Aims. AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies
 in non-valvular AF (NVAF) Practical Issues Patient Case Studies") Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies AF and Stroke AF prevalence approx doubles with each
Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies AF and Stroke AF prevalence approx doubles with each
Disclosure. Objectives. New Anticoagulants 6/5/2014 GHASSAN HADDAD M.D FHM. South Miami hospital Director of the Anticoagulation clinic.
 /5/1 New Anticoagulants: Opportunities, Challenges and Practical Considerations GHASSAN HADDAD M.D FHM. Chief of Hospital Medicine i South Miami hospital Director of the Anticoagulation clinic. Financial
/5/1 New Anticoagulants: Opportunities, Challenges and Practical Considerations GHASSAN HADDAD M.D FHM. Chief of Hospital Medicine i South Miami hospital Director of the Anticoagulation clinic. Financial
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging
 and advances in peri-procedural interruption of anticoagulation-- Bridging") Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA
 Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Anticoagulation: Novel Agents
 Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
ADVANCES IN ANTICOAGULATION
 ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
Stroke. 2012;43: ; originally published online August 2, 2012; doi: /STR.0b013e a
 Oral Antithrombotic Agents for the Prevention of Stroke in Nonvalvular Atrial Fibrillation : A Science Advisory for Healthcare Professionals From the American Heart Association/American Stroke Association
Oral Antithrombotic Agents for the Prevention of Stroke in Nonvalvular Atrial Fibrillation : A Science Advisory for Healthcare Professionals From the American Heart Association/American Stroke Association
Dabigatran Evidence in Real Practice
 ADVANCES IN CARDIAC ARRHYTHMIAS and GREAT INNOVATIONS IN CARDIOLOGY XXVII GIORNATE CARDIOLOGICHE TORINESI Torino, Centro Congressi Unione Industriale 23-24 Ottobre 2015 Dabigatran Evidence in Real Practice
ADVANCES IN CARDIAC ARRHYTHMIAS and GREAT INNOVATIONS IN CARDIOLOGY XXVII GIORNATE CARDIOLOGICHE TORINESI Torino, Centro Congressi Unione Industriale 23-24 Ottobre 2015 Dabigatran Evidence in Real Practice
NOACs in AF. Dr Fiona Stewart. Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Fiona Stewart Auckland Heart Group and Auckland DHB NOACS for AF True/False All patients should have a CHA 2 DS 2 VASc risk assessment on diagnosis of AF NOACS are more effective than warfarin
NOACs in AF Dr Fiona Stewart Auckland Heart Group and Auckland DHB NOACS for AF True/False All patients should have a CHA 2 DS 2 VASc risk assessment on diagnosis of AF NOACS are more effective than warfarin
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Volume 7; Number 16 October 2013
 Greater East Midlands Commissioning Support Unit in association with Lincolnshire Clinical Commissioning Groups, Lincolnshire Community Health Services, United Lincolnshire Hospitals Trust and Lincolnshire
Greater East Midlands Commissioning Support Unit in association with Lincolnshire Clinical Commissioning Groups, Lincolnshire Community Health Services, United Lincolnshire Hospitals Trust and Lincolnshire
Survey patients for Sx, signs of AF. Establish AF Dx. Evaluate & Tx underlying heart disease/other causes. Assess adequacy of rate or rhythm control
 Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
controversies in anticoagulation: optimizing outcome for atrial fibrillation
 controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
The Age of the Novel Anticoagulants. Peter Netzler, MD April 21, 2017 Carolina Cardiology Electrophysiology
 The Age of the Novel Anticoagulants Peter Netzler, MD April 21, 2017 Carolina Cardiology Electrophysiology Disclosures Speaker bureau for the Bristol-Myers Squibb and Pfizer alliance for Eliquis Direct
The Age of the Novel Anticoagulants Peter Netzler, MD April 21, 2017 Carolina Cardiology Electrophysiology Disclosures Speaker bureau for the Bristol-Myers Squibb and Pfizer alliance for Eliquis Direct
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Are the days of Warfarin numbered?
 2 nd SAVTE Symposium Are the days of Warfarin numbered? YES Dr. Mohamed A. Abdelaal, MD, FRCPath, FRCPI Consultant Haematologist King Abdulaziz Medical City - Jeddah, Saudi Arabia 1 3 May 2012, Casablanca,
2 nd SAVTE Symposium Are the days of Warfarin numbered? YES Dr. Mohamed A. Abdelaal, MD, FRCPath, FRCPI Consultant Haematologist King Abdulaziz Medical City - Jeddah, Saudi Arabia 1 3 May 2012, Casablanca,
NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation
 1 NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation Atrial fibrillation (AF) affects about 1.2% of the population in the United Kingdom and accounts
1 NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation Atrial fibrillation (AF) affects about 1.2% of the population in the United Kingdom and accounts
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION
 FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION") RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION Craig I. Coleman, PharmD Professor, University of Connecticut School
RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION Craig I. Coleman, PharmD Professor, University of Connecticut School
KCS Congress: Impact through collaboration
 Stroke Prevention in Atrial Fibrillation (SPAF) in Kenya Elijah N. Ogola FACC University of Nairobi Kenya Cardiac Society Annual Scientific Congress Mombasa 28 th June 1 st July 2017 KCS Congress: Impact
Stroke Prevention in Atrial Fibrillation (SPAF) in Kenya Elijah N. Ogola FACC University of Nairobi Kenya Cardiac Society Annual Scientific Congress Mombasa 28 th June 1 st July 2017 KCS Congress: Impact
A Patient Unsuitable for VKA Treatment
 Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Appendix C Factors to consider when choosing between anticoagulant options and FAQs
 Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012
 Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012 Professor Dan Atar Head, Dept. of Cardiology Councillor of the ESC,
Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012 Professor Dan Atar Head, Dept. of Cardiology Councillor of the ESC,
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Σεμινάπιο Ομάδων Δπγαζίαρ ΟΜΑΓΑ ΔΡΓΑΣΙΑΣ ΗΛΔΚΤΡΟΦΥΣΙΟΛΟΓΙΑΣ ΚΑΙ ΒΗΜΑΤΟΓΟΤΗΣΗΣ Κολπική μαπμαπςγή
 Σεμινάπιο Ομάδων Δπγαζίαρ ΟΜΑΓΑ ΔΡΓΑΣΙΑΣ ΗΛΔΚΤΡΟΦΥΣΙΟΛΟΓΙΑΣ ΚΑΙ ΒΗΜΑΤΟΓΟΤΗΣΗΣ Κολπική μαπμαπςγή Δξελίξειρ ζηην ανηιπηκηική αγωγή ζε αζθενείρ με κολπική μαπμαπςγή Ξςδώναρ Σωηήπιορ Μονάδα Δμθπαγμάηων και
Σεμινάπιο Ομάδων Δπγαζίαρ ΟΜΑΓΑ ΔΡΓΑΣΙΑΣ ΗΛΔΚΤΡΟΦΥΣΙΟΛΟΓΙΑΣ ΚΑΙ ΒΗΜΑΤΟΓΟΤΗΣΗΣ Κολπική μαπμαπςγή Δξελίξειρ ζηην ανηιπηκηική αγωγή ζε αζθενείρ με κολπική μαπμαπςγή Ξςδώναρ Σωηήπιορ Μονάδα Δμθπαγμάηων και
Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali
 Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali Gianluca Botto, MD, FAAC, FESC Divisione di Cardiologia Ospedale Sant Anna, Como The Promise of NOAs Antithrombotic
Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali Gianluca Botto, MD, FAAC, FESC Divisione di Cardiologia Ospedale Sant Anna, Como The Promise of NOAs Antithrombotic
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Evaluate Risk of Stroke & Bleeding in AF Patients
 XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
Reviews. Practical Considerations for Using Novel Oral Anticoagulants in Patients With Atrial Fibrillation
 Reviews Practical Considerations for Using Novel Oral Anticoagulants in Patients With Atrial Fibrillation Address for correspondence: A. John Camm, MD Division of Clinical Sciences St. George s University
Reviews Practical Considerations for Using Novel Oral Anticoagulants in Patients With Atrial Fibrillation Address for correspondence: A. John Camm, MD Division of Clinical Sciences St. George s University
Comparison of novel oral anticoagulants (NOACs)
") Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
NOACs Update PD Dr. Jan Steffel Leitender Arzt, Klinik für Kardiologie Co-Leiter Rhythmologie Universitätsspital Zürich
 NOACs Update 2016 PD Dr. Jan Steffel Leitender Arzt, Klinik für Kardiologie Co-Leiter Rhythmologie Universitätsspital Zürich Conflict of Interest Statement o o o o Consulting: Amgen, Astra Zeneca, AtriCure,
NOACs Update 2016 PD Dr. Jan Steffel Leitender Arzt, Klinik für Kardiologie Co-Leiter Rhythmologie Universitätsspital Zürich Conflict of Interest Statement o o o o Consulting: Amgen, Astra Zeneca, AtriCure,
Update with the New Oral Anticoagulants: Today s Issues for the Front Line Pharmacist
 Update with the New Oral Anticoagulants: Today s Issues for the Front Line Pharmacist Peter Thomson, Pharm D. Clinical Resource Pharmacist, Medicine Program Winnipeg Regional Health Authority Clinical
Update with the New Oral Anticoagulants: Today s Issues for the Front Line Pharmacist Peter Thomson, Pharm D. Clinical Resource Pharmacist, Medicine Program Winnipeg Regional Health Authority Clinical
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Dr Calum Young Cardiologist Tauranga
 Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated) GPCME 2016: Anticoagulation
Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated) GPCME 2016: Anticoagulation
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease
 Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy