Aims. AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies
|
|
|
- Donna Heath
- 5 years ago
- Views:
Transcription
1 Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies

2 AF and Stroke AF prevalence approx doubles with each decade (9% at years) 1 Stroke prevalence increases nearly 5 fold when AF is present 2 In patients with AF, blood clots tend to form in the atria, particularly within the left atrial appendage These clots may travel to the brain, causing an ischaemic stroke Around 20% of ischaemic strokes are caused by blood clots originating in the heart (cardioembolic); of these, AF is the most common cause 3 1. NICE CG36 Atrial fibrillation Wolf PA et al. Stroke 1991;22: ; 3. Paciaroni M et al. Stroke 2007;38:
3 2-year age-adjusted incidence of stroke/1,000 Patients with AF have approx fivefold increased ischaemic stroke risk Framingham Heart Study (N=5,070) Risk ratio=4.8 p< Individuals Individuals *Patients were seldom treated with antithrombotic therapy when this study was performed in line with clinical practice at the time without AF with AF* 1. Adapted from Wolf PA et al. Stroke 1991;22:

4 Risk factors for stroke and thrombo-embolism in non-valvular AF AF= atrial fibrillation; EF = ejection fraction (as documented by echocardiography, radionuclide ventriculography, cardiac catheterization, cardiac magnetic resonance imaging, etc.); LV = left ventricular; TIA = transient ischaemic attack.

5 CHADS 2 score and stroke rate *The adjusted stroke rate was derived from the multivariable analysis assuming no aspirin usage; these stroke rates are based on data from a cohort of hospitalised AF patients, published in 2001, with low numbers in those with a CHADS 2 score of 5 and 6 to allow an accurate judgement of the risk in these patients. Given that stroke rates are declining overall, actual stroke rates in contemporary non-hospitalised cohorts may also vary from these estimates. Adapted from Gage BF et al. AF = atrial fibrillation; CHADS 2 = cardiac failure, hypertension, age, diabetes, stroke (doubled).

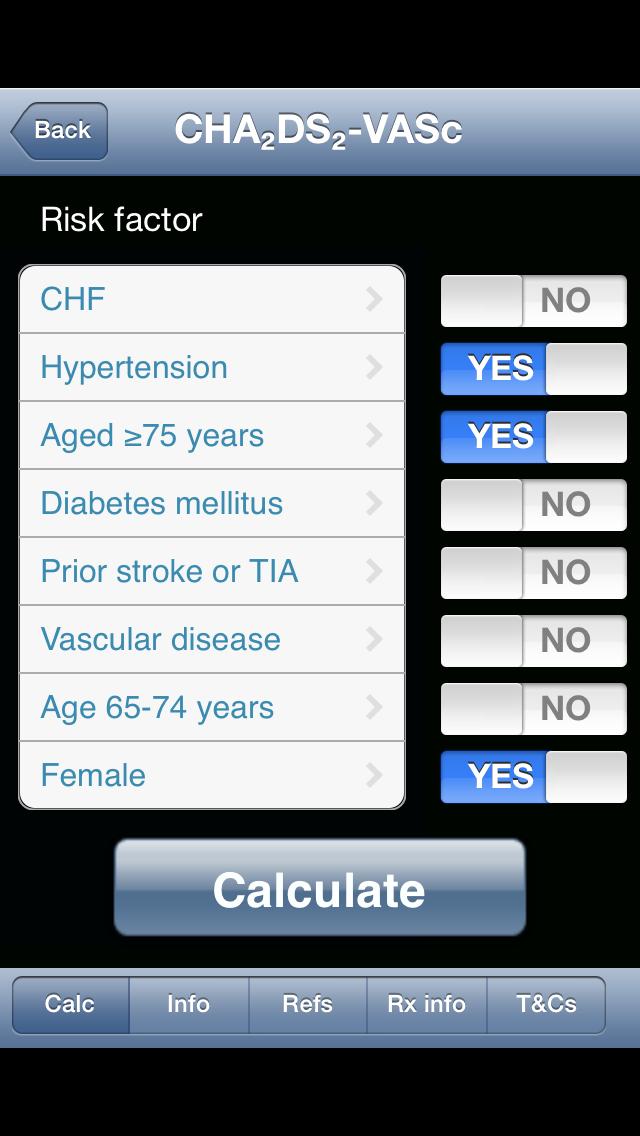
6 Risk factor-based point-based scoring system - CHA 2 DS 2 -VASc *Prior myocardial infarction, peripheral artery disease, aortic plaque. Actual rates of stroke in contemporary cohorts may vary from these estimates.

7 Adjusted stroke rate according to CHA 2 DS 2 -VASc score
8 CHADS 2 score Why use CHA 2 DS 2 -VASc? CHA 2 DS 2 VaSc score % of n Stroke risk per 100pt yrs 0-1 n=47, % 0.84 ( ) % 1.79 ( ) % 3.67 (3.34-4) % 5.75 ( ) 4 3.1% 8.18 ( ) Olesen et al, Thrombosis and haemostasis June 2012
9 CHADS 2 score Why use CHA 2 DS 2 -VASc? CHA 2 DS 2 VaSc score % of n Stroke risk per 100pt yrs 0-1 n=47, % 0.84 ( ) % 1.79 ( ) % 3.67 (3.34-4) % 5.75 ( ) 4 3.1% 8.18 ( ) 0 n= Olesen et al, Thrombosis and haemostasis June 2012

10 The HAS-BLED bleeding risk score *Hypertension is defined as systolic blood pressure > 160 mmhg. INR = international normalized ratio.

11
12 Choice of anticoagulant in AF: ESC Guidelines 2012 Atrial fibrillation Valvular AF Yes Best option Alternative Adapted from: Camm et al. Eu Heart J August 2012 NOAC VKA
13 Choice of anticoagulant in AF: ESC Guidelines 2012 Atrial fibrillation Yes Valvular AF <65 years and lone AF (including female) No Assess risk of stroke (CHA 2 DS 2 -VASc score) Yes No (i.e. non-valvular AF) Best option Alternative 0 No antithrombotic therapy Adapted from: Camm et al. Eu Heart J August 2012 NOAC VKA
14 Choice of anticoagulant in AF: ESC Guidelines 2012 Atrial fibrillation Yes Valvular AF <65 years and lone AF (including female) No Assess risk of stroke (CHA 2 DS 2 -VASc score) Yes No (i.e. non-valvular AF) Best option Alternative 0 1 >2 No antithrombotic therapy Adapted from: Camm et al. Eu Heart J August 2012 Oral anticoagulant therapy Assess bleeding risk (HAS-BLED score) Consider patient values and preferences NOAC* VKA *NOACs are broadly preferable to VKA in the vast majority of patients with NVAF For full recommendations please refer to the ESC Guidelines for the management of atrial fibrillation (2012 update).
15 The Aspirin Story Weak evidence for aspirin efficacy OAC 39% risk reduction compared antiplatelet Risk of major bleeding or ICH similar to OAC Warfarin risk/year Aspirin risk/year HR (95% CI) Major extracranial haemorrhage ( ) All major haemorrhage ( ) BAFTA study 2007 in patients >75yrs Aspirin and clopidogrel is more effective than single therapy and less effective than OAC but with higher bleeding risk
16 Oral anti-coagulation is shown to be effective for stroke prevention in AF Study, year Reduction of risk of thromboembolism in AF 1 Relative risk reduction (95% CI) Absolute risk reduction AFASAK I, 1989; 1990 SPAF I, 1991 BAATAF, 1991 CAFA, 1991 SPINAF, 1992 EAFT, 1993 All trials (n=6) 2.6% 4.7% 2.4% 1.2% 3.3% 8.4% primary prevention 2.7, secondary prevention % 50% 0 50% 100% Favours VKA Favours placebo Hart RG et al. Ann Intern Med 2007;146:
17 Age, years Oral anti-coagulation: benefit risk improves with increasing age Net clinical benefit: events prevented per 100 person-years < Worse with warfarin Better with warfarin Singer DE et al. Ann Intern Med 2009;151:
18 Odds ratio for event Oral Anticoagulant Therapy - Warfarin Warfarin reduces stroke risk by 64% and all cause mortality by 26% (metanalysis) But Ischaemic stroke Intracranial bleeding 5 Target INR International normalized ratio






19 Drug and food interactions with warfarin
20 % of patients without stroke Poor INR control increases the risk of stroke in real-world practice Stroke survival in 37,907 AF patients UK General Practice Research Database (27,458 warfarin users and 10,449 not treated with an antithrombotic) No warfarin %TTR > < 30 I I I I I I Months Adapted from Gallagher et al. Thromb Haemost 2011;106:

21 Anticoagulant Drugs Rivaroxaban and Apixaban Dabigatran
22 Contraindications to Warfarin Poor medication compliance Liver disease or severe hepatic impairment Bleeding diathesis Alcohol abuse High falls risk High bleeding risk All Oral Anticoagulants See SPC for each medicine for specific information

23 Dabigatran Rivaroxaban Apixaban Edoxaban Direct Thrombin Inhibitor Xa inhibitor
24 Dabigatran Rivaroxaban Apixaban Edoxaban Direct Thrombin Inhibitor Xa inhibitor No monitoring or food interactions Take with food
25 Dabigatran Rivaroxaban Apixaban Edoxaban Direct Thrombin Inhibitor 80% renal excretion Xa inhibitor No monitoring or food interactions Take with food 35% renal excretion 27% renal excretion 50% renal excretion
26 Dabigatran Rivaroxaban Apixaban Edoxaban Direct Thrombin Inhibitor Xa inhibitor No monitoring or food interactions Take with food 80% renal excretion 35% renal excretion 27% renal excretion 50% renal excretion Dyspepsia 5-10% Poss increase MI No GI problems
27 Dabigatran Rivaroxaban Apixaban Edoxaban Direct Thrombin Inhibitor Xa inhibitor No monitoring or food interactions Take with food 80% renal excretion 35% renal excretion 27% renal excretion 50% renal excretion Dyspepsia 5-10% No GI problems 150mg bd 20mg od 5mg bd 15-60mg od 110mg bd if >80, frail, verapamil 15mg od if GFR ml/min 2.5mg bd if GFR mg bd if 2+ of: >80 yrs, <60 kg, cr >133μmol/l
28 Dabigatran Rivaroxaban Apixaban Edoxaban Direct Thrombin Inhibitor Xa inhibitor No monitoring or food interactions Take with food 80% renal excretion 35% renal excretion 27% renal excretion 50% renal excretion Dyspepsia 5-10% No GI problems 150mg bd 20mg od 5mg bd 15-60mg od 110mg bd if >80, frail, verapamil 15mg od if GFR ml/min 2.5mg bd if GFR mg bd if 2+ of: >80 yrs, <60 kg, cr >133μmol/l No antidote or easy monitoring test
29 Dosage according to renal function 1,2,3 Creatinine clearance 50 + ml/min 20mg Once daily 5 mg bd 150mg BD or 110mg BD Creatinine clearance 50 + ml/min Creatinine clearance ml/min 15mg Once daily 5mg bd 150mg BD with caution. Consider using 110mg BD if high bleeding risk. Dose adjust based on age, weight and medications Creatinine clearance ml/min Creatinine clearance ml/min Creatinine clearance <15 ml/min 15mg Once daily with caution Not recommended 2.5 mg bd* Not recommended Contraindicated Creatinine clearance <30 ml/min Rivaroxaban Apixaban Dabigatran 1. Xarelto SmPC 2. Pradaxa SmPC 3. Eliquis SmPC * * Patients with 2 of the following: age 80 years, body weight 60 kg, or a serum creatinine level 1.5 mg/dl (133 μmol/l).



30 Verapamil: Use Rivaroxaban Diltiazem: Use Dabigatran, Apixaban or Rivaroxaban (with caution) Amiodarone: Use Rivaroxaban with caution Dronedarone: Stick to warfarin xfordjournals.org/ Please refer to the relevant SPCs for further information.
31 RE-LY: Study Design Non-Valvular Atrial fibrillation 1 Risk Factor Absence of contra-indications 951 centers in 44 countries NVAF with: 1.Previous stroke or TIA 2.a left ventricular ejection fraction < 40% 3.NYHA class II or higher heart-failure symptoms within 6 months 4.> 75 years or an age of 65 to 74 years plus diabetes mellitus, hypertension, or coronary artery disease. Blinded Event Adjudication Open Blinded Warfarin adjusted (INR ) N=6000 Dabigatran Etexilate 110 mg BID N=6000 Dabigatran Etexilate 150 mg BID N=6000 Primary Endpoint: Stroke or non-cns Systemic Embolism Connolly SJ, et al. N Engl J Med. 2009;361:
32 Rocket AF Design Non-Valvular Atrial Fibrillation Risk Factors CHF Hypertension At least 2 or Age 75 3 required* Diabetes OR Stroke, TIA or Systemic embolus Rivaroxaban 20 mg daily 15 mg for Cr Cl ml/min Randomize Double Blind / Double Dummy (n ~ 14,000) Warfarin INR target ( inclusive) Monthly Monitoring Adherence to standard of care guidelines Primary Endpoint: Stroke or non-cns Systemic Embolism * Enrollment of patients without prior Stroke, TIA or systemic embolism and only 2 factors capped at 10% Rocket AF Investigators, AHA 2010
33 Aristotle Design Non-Valvular Atrial Fibrillation 1 Risk Factors CHF Hypertension Age 75 Diabetes Stroke, TIA or Systemic embolus Apixaban 5 mg twice daily 2.5 mg bd if 2 or age>80, weight<60kg or Cr>133umol/l Randomize Double Blind / Double Dummy (n ~18201) Warfarin INR target ( inclusive) Monthly Monitoring Adherence to standard of care guidelines Primary Endpoint: Stroke or non-cns Systemic Embolism Granger et al, Aristotle NEJM Sept 2011
34 Drug/trial (vs warfarin) Stroke/ thromboembolism Haemorrhagic stroke Ischaemic stroke Major bleeding Dabigatran 150/RELY 34% RRR 0.58% ARR P<0.001 Dabigatran 110/RELY Non inferior Rivaroxaban /ROCKET-AF Non inferior Apixaban/ 21% RRR ARISTOTLE 0.33% ARR P = 0.01 Results are from a comparison of individual NOACs with warfarin. These data are not based on direct comparisons between NOACs and should therefore be interpreted with caution.
35 Drug/trial (vs warfarin) Stroke/ thromboembolism Haemorrhagic stroke Ischaemic stroke Major bleeding Dabigatran 150/RELY 34% RRR 0.58% ARR P< % RRR 0.28% ARR P<0.001 Dabigatran 110/RELY Non inferior 69% RRR 0.26% ARR P<0.001 Rivaroxaban /ROCKET-AF Non inferior 41% RRR 0.18% ARR P = Apixaban/ ARISTOTLE 21% RRR 0.33% ARR P = % RRR 0.23% ARR P <0.001 Results are from a comparison of individual NOACs with warfarin. These data are not based on direct comparisons between NOACs and should therefore be interpreted with caution.
36 Drug/trial (vs warfarin) Stroke/ thromboembolism Haemorrhagic stroke Ischaemic stroke Major bleeding Dabigatran 150/RELY 34% RRR 0.58% ARR P< % RRR 0.28% ARR P< % RRR 0.28% ARR P=0.03 Dabigatran 110/RELY Non inferior 69% RRR 0.26% ARR P< % RRI 0.14% ARI P=0.35 Rivaroxaban /ROCKET-AF Non inferior 41% RRR 0.18% ARR 6% RRR 0.08% ARR P = P = 0.58 Apixaban/ ARISTOTLE 21% RRR 0.33% ARR P = % RRR 0.23% ARR P < % RRR 0.06% ARR P=0.42 Results are from a comparison of individual NOACs with warfarin. These data are not based on direct comparisons between NOACs and should therefore be interpreted with caution.
37 Drug/trial (vs warfarin) Stroke/ thromboembolism Haemorrhagic stroke Ischaemic stroke Major bleeding Dabigatran 150/RELY 34% RRR 0.58% ARR P< % RRR 0.28% ARR P< % RRR 0.28% ARR P=0.03 Similar Dabigatran 110/RELY Non inferior 69% RRR 0.26% ARR P< % RRI 0.14% ARI P= % RRR 0.65% ARR P=0.003 Rivaroxaban /ROCKET-AF Non inferior 41% RRR 0.18% ARR 6% RRR 0.08% ARR Similar P = P = 0.58 Apixaban/ ARISTOTLE 21% RRR 0.33% ARR P = % RRR 0.23% ARR P < % RRR 0.06% ARR P= % RRR 0.96% ARR P<0.001 Results are from a comparison of individual NOACs with warfarin. These data are not based on direct comparisons between NOACs and should therefore be interpreted with caution.
38 Averroes: Apixaban v Aspirin 5599 patients unsuitable/unwilling warfarin 55% RRR in stroke/embolism. (2.1% ARR) No difference major bleeding 1000 NVAF patients Rx Apixaban versus ASA would prevent: 21 patients Strokes/systemic emboli 1 33 CV Hospitalisations 2 1 Connolly SJ et al. N Engl J Med 2011;364: Hohnloser et al. Europ H J 2013 Sep;34(35):2752-9
39 Summary? Warfarin and NOACs are all effective drugs for stroke and systemic embolus prevention in patients with NVAF NOACs all reduce risk of haemorrhagic stroke cf warfarin Predictable anticoagulation for NOACs No antidotes for NOACs Effect of NOACs can t be easily monitored NOACs excretion depends on renal function NOACs more expensive but other savings to NHS and meets cost effectiveness
40 Cost Implications NOACs approx /year Warfarin costs 11-12/year Warfarin clinic costs very variable Difficult to control patients cost more Reduced strokes/complications with NOACs vs warfarin, saves money
41 Which one to choose? Dabigatran Rivaroxaban Apixaban Pros 150mg better stroke reduction than warfarin 150mg best ischaemic stroke reduction 110mg bd less major bleeding than warfarin Cons Higher GI side effects Twice daily Most susceptible to renal impairment These data are not based on direct comparisons between NOACs and should therefore be interpreted with caution.
42 Which one to choose? Dabigatran Rivaroxaban Apixaban Pros Cons 150mg better stroke reduction than warfarin 150mg best ischaemic stroke reduction 110mg bd less major bleeding than warfarin Higher GI side effects Twice daily Most susceptible to renal impairment Once daily Use down to CrCl 15 Can go in dosette Well tolerated Fewer drug interactions Not clearly superior to warfarin Higher GI bleeding Take with food These data are not based on direct comparisons between NOACs and should therefore be interpreted with caution.
43 Which one to choose? Dabigatran Rivaroxaban Apixaban Pros 150mg better stroke reduction than warfarin Once daily More effective than aspirin with no bleeds 150mg best ischaemic stroke reduction 110mg bd less major bleeding than warfarin Use down to CrCl 15 Can go in dosette Well tolerated Fewer drug interactions Better stroke reduction than warfarin (& major bleeding) Small Mortality benefit Can go in dosette Well tolerated Best data in renal failure Cons Higher GI side effects Not clearly superior to warfarin Twice daily Twice daily Higher GI bleeding Most susceptible to renal impairment Take with food These data are not based on direct comparisons between NOACs and should therefore be interpreted with caution.
44 NICE is Naughty NICE AF 2014 Anticoagulation may be with apixaban, dabigatran etexilate, rivaroxaban or a vitamin K antagonist. Discuss the options for anticoagulation with the person and base the choice on their clinical features and preferences. [new 2014] NICE CKD 2014 Consider apixaban in preference to warfarin in people with a confirmed egfr of ml/min/1.73 m2 and nonvalvular atrial fibrillation who have 1 or more of the following risk factors: prior stroke or transient ischaemic attack age 75 years or older hypertension diabetes mellitus symptomatic heart failure. [new 2014]
45 Practical considerations Who to switch Switching patients Warfarin to NOAC NOAC to warfarin Between NOACs Long term follow up Bleeding Operations
46 Practical considerations (see SPCs) Switching patients Stop warfarin and start NOAC when INR<2-3 Start warfarin 2-3 days before stopping NOAC & stop when INR>2
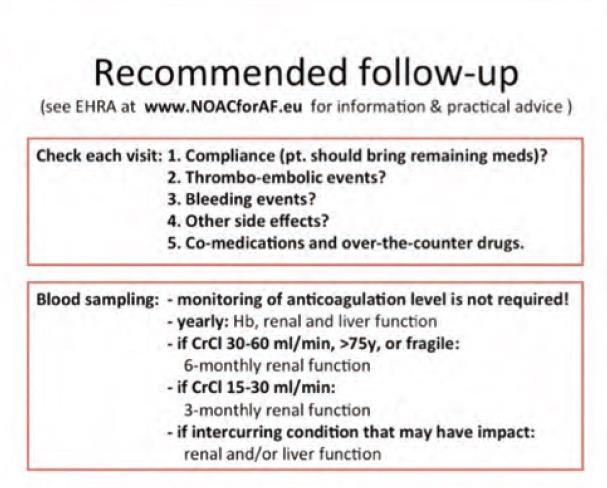
47 Follow Up
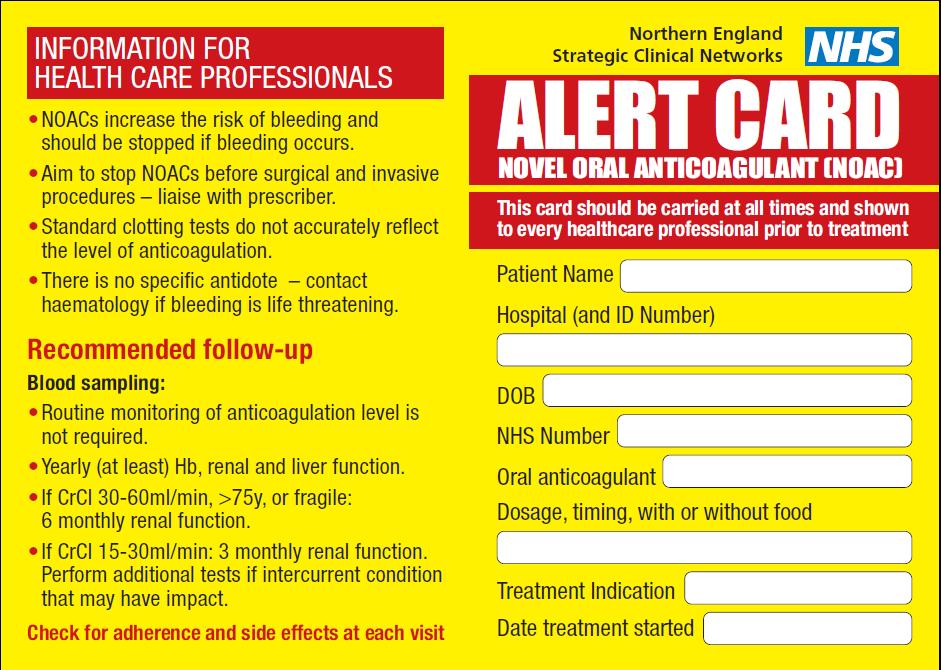
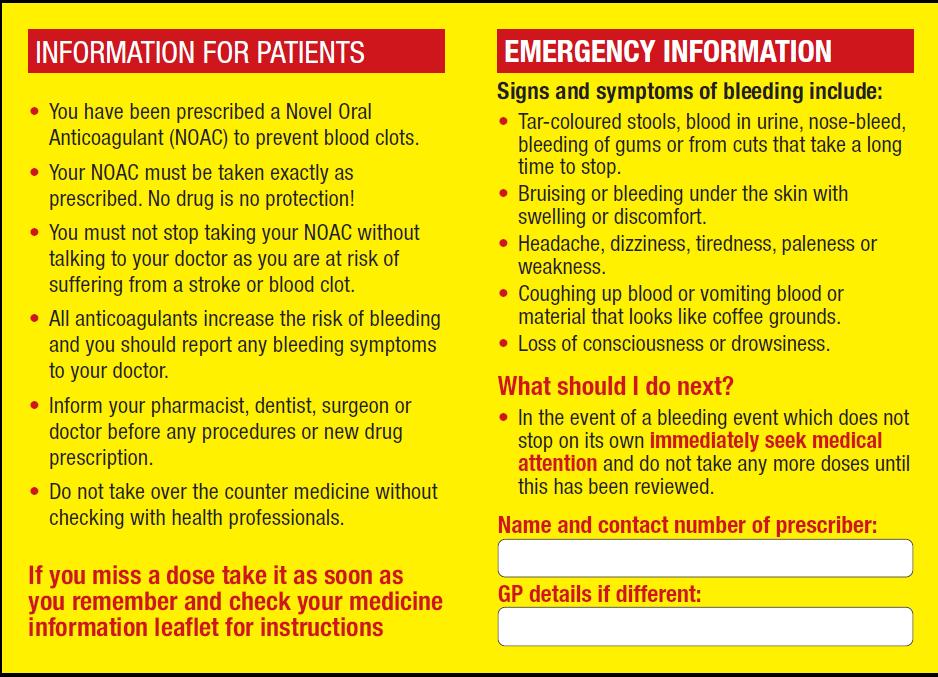
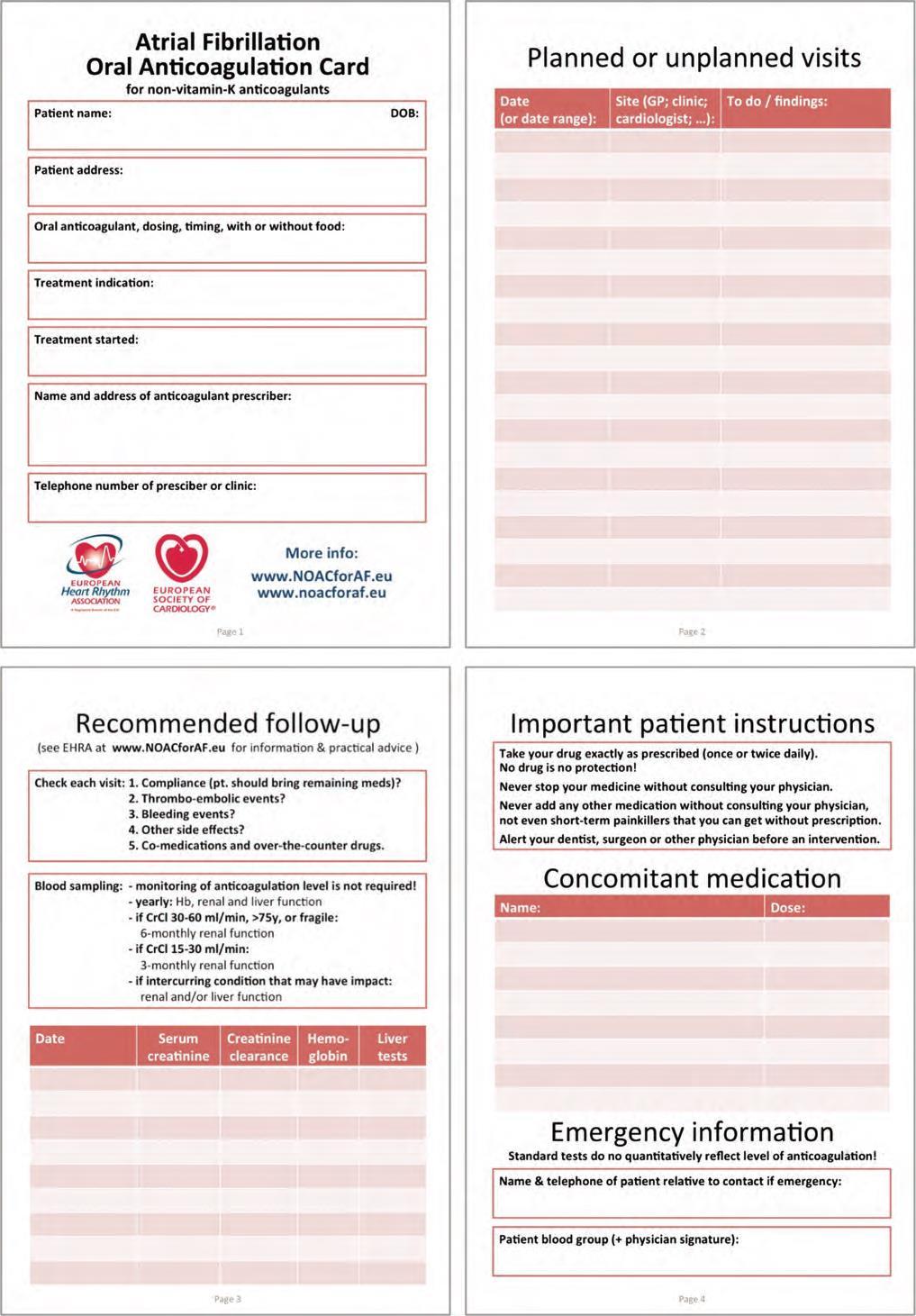
48 Standardised NOAC card
49 Bleeding Patients on NOAC presenting with bleeding Check haemodynamic status, basic coagulation tests to assess anticoagulation effect (e.g. aptt for dabigatran, PT or anti Xa activity for rivaroxaban), renal function, etc. Minor Delay next dose or discontinue treatment Moderate-severe Symptomatic/supportive treatment Mechanical compression Fluid replacement Blood transfusion Oral charcoal if recently ingested a Very severe Consider rfviia or PCC Charcoal filtration a / haemodialysis *a * haemodialysis unlikely to be an effective means of managing apixaban overdose - a With dabigatran Adapted from Camm et al. Eur Heart J 2012;e-published August 2012, doi: /eurheartj/ehs

50 Invasive procedures and surgery Stop NOAC at least 24 hours before intervention (depends on type surgery and GFR) If this is not possible, assess relative risk of bleeding compared to urgency of intervention Restart as soon as possible after the intervention if situation allows and haemostasis established Please refer to individual product SPC for further information
51 Case 1 58 male Bus driver in Hexham Asymptomatic NVAF at work medical egfr 60 CHA 2 DS 2 -VASc = 2, (diabetes and hypertension) 2.2% risk stroke/yr Warfarin commenced by GP Struggles due to work to get to clinic
52 Case 2 45 man with first episode of NVAF after chest infection (>48hrs) Symptomatic Normal heart on echo egfr normal Works away Planning cardioversion
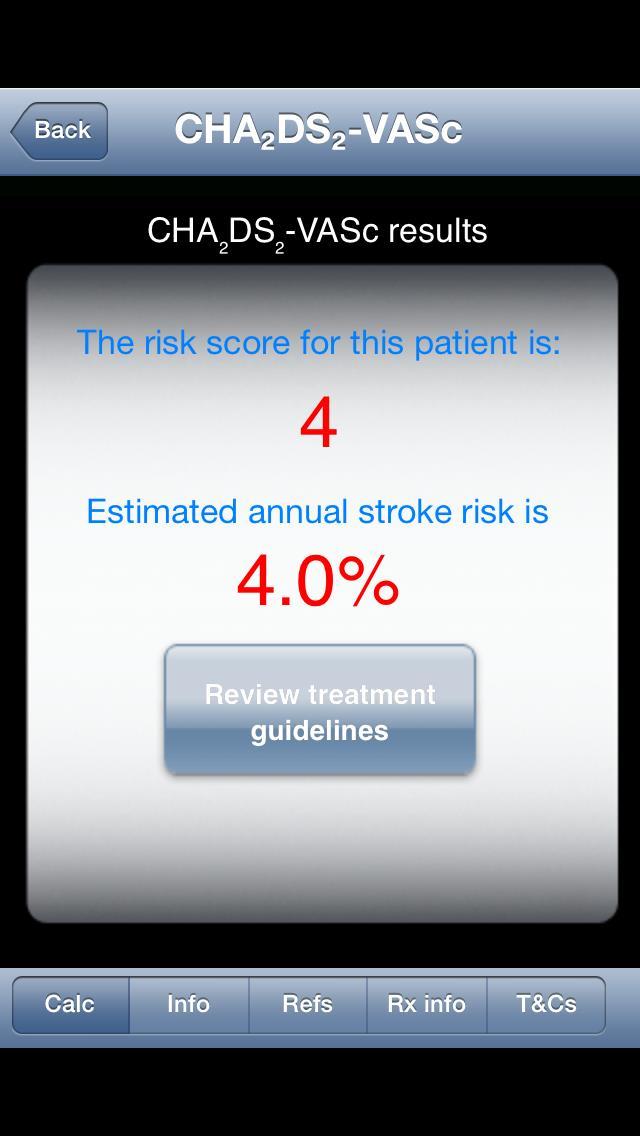
53 Case 3 76 female Persistent NVAF CHA 2 DS 2 -VASc = 4 (age, gender, BP) Estimated stroke risk 4% per year Mild cognitive impairment Supportive family but can t manage warfarin Dosette box for meds
54 Case 4 85 female Frail (58kg) but cognitively aware Previous IDA investigated appropriately Cr 135 egfr 27 Persistent NVAF CHA 2 DS 2 -VASc = 7 (age, gender, BP, stroke & vasc disease) Estimated stroke risk 9.6% per year
55 Case 5 67 man Impaired LV function, IHD, BP, diabetes Paroxysmal NVAF CHA 2 DS 2 -VASc = 5 Estimated stroke risk 6.7% per year Subtherapeutic INR despite 13mg warfarin
56 Case 6 78 female Persistent NVAF CHA 2 DS 2 -VASc = 3 Estimated stroke risk 3.2% per year Hair loss with warfarin
57 Case 7 35 man Paroxysmal NVAF, pill in pocket Otherwise fit What if female
 Amiodarone: Use Rivaroxaban with caution Dronedarone: Stick")
58 Case 8 69 woman Persistent NVAF Asthma, Hypertension CHA 2 DS 2 -VASc = 3 Rx digoxin and diltiazem for rate control Hates taking warfarin as likes to cruise.. What if on Verapamil Verapamil: Use Rivaroxaban Diltiazem: Use Dabigatran or Rivaroxaban (with caution) Amiodarone: Use Rivaroxaban with caution Dronedarone: Stick to warfarin
59 Case 9 75 male Longstanding AF on warfarin Presents with ischaemic stroke Good recovery
60 Case man Persistent AF CKD secondary to BP and DM, egfr 25 CHA 2 DS 2 -VASc = 4 Estimated stroke risk 4% per year What if egfr 15
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
PRESENTATION TITLE. Case Studies
 PRESENTATION TITLE Case Studies 1) SH is a 67 year old male. He has a history of type 2 diabetes, controlled hypertension and peripheral artery disease. He takes naproxen 500mg bd for arthritis and admits
PRESENTATION TITLE Case Studies 1) SH is a 67 year old male. He has a history of type 2 diabetes, controlled hypertension and peripheral artery disease. He takes naproxen 500mg bd for arthritis and admits
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
NOACs in AF. Dr Colin Edwards Auckland Heart Group and Waitemata DHB. Dr Fiona Stewart Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016
 1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
Modern Management in Primary Care (AF1)
") Modern Management in Primary Care (AF1) Dr Ravi Assomull Consultant Cardiologist London North West Healthcare NHS Trust Dr Yassir Javaid Primary Care Cardiovascular Lead East Midlands Strategic Clinical
Modern Management in Primary Care (AF1) Dr Ravi Assomull Consultant Cardiologist London North West Healthcare NHS Trust Dr Yassir Javaid Primary Care Cardiovascular Lead East Midlands Strategic Clinical
Dr Chris Ellis. Consultant Cardiologist Auckland City Hospital Auckland
 Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Antithrombotic Efficacy and Safety of Dabigatran Etexilate
 130419 Luncheon Symposium_2013 춘계심장학회 Antithrombotic Efficacy and Safety of Dabigatran Etexilate Hui-Nam Pak, MD, PhD. Division of Cardiology Yonsei University Health System Atrial Fibrillation Risk of
130419 Luncheon Symposium_2013 춘계심장학회 Antithrombotic Efficacy and Safety of Dabigatran Etexilate Hui-Nam Pak, MD, PhD. Division of Cardiology Yonsei University Health System Atrial Fibrillation Risk of
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised
 DABIGATRAN RECOMMENDED What it is Indications Date decision last revised") Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients. Giancarlo Agnelli
 NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
Scoring Systems in AF 8/10/2016. Strategies in the Prevention of Atrial Fibrillation-Related Strokes. Overview
 Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
Appendix C Factors to consider when choosing between anticoagulant options and FAQs
 Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
Appendix C Factors to consider when choosing between anticoagulant options and FAQs Choice of anticoagulant for non-valvular* atrial fibrillation: Clinical decision aid Patients should already be screened
Stepheny Sumrall, FNP, AGACNP Cardiovascular Clinic of Hattiesburg
 Novel Oral Anticoagulants Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for the Treatment of Atrial Fibrillation and Prevention of Stroke Stepheny Sumrall,
Novel Oral Anticoagulants Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for the Treatment of Atrial Fibrillation and Prevention of Stroke Stepheny Sumrall,
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Volume 7; Number 16 October 2013
 Greater East Midlands Commissioning Support Unit in association with Lincolnshire Clinical Commissioning Groups, Lincolnshire Community Health Services, United Lincolnshire Hospitals Trust and Lincolnshire
Greater East Midlands Commissioning Support Unit in association with Lincolnshire Clinical Commissioning Groups, Lincolnshire Community Health Services, United Lincolnshire Hospitals Trust and Lincolnshire
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Dr. Khalid Khan Consultant Cardiologist
 Dr. Khalid Khan Consultant Cardiologist BCUHB (Wrexham) WCS Spring Meeting 2012 When the pulse is irregular and tremulous and the beats occur at intervals, then the impulse of life fades; when the pulse
Dr. Khalid Khan Consultant Cardiologist BCUHB (Wrexham) WCS Spring Meeting 2012 When the pulse is irregular and tremulous and the beats occur at intervals, then the impulse of life fades; when the pulse
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation
 1 NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation Atrial fibrillation (AF) affects about 1.2% of the population in the United Kingdom and accounts
1 NHS Lanarkshire Guidance on Anticoagulant treatment for patients with non-valvular atrial fibrillation Atrial fibrillation (AF) affects about 1.2% of the population in the United Kingdom and accounts
A Patient Unsuitable for VKA Treatment
 Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Results from RE-LY and RELY-ABLE
 Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Atrial Fibrillation Topics for Today. Clinical Controversies Management of Atrial Fibrillation. Atrial Fibrillation in the ER Topics for Today
 Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Anticoagulation Beyond Coumadin
 Anticoagulation Beyond Coumadin Saturday, September 21, 2013 Crystal Mountain Resort and Spa Pratik Bhattacharya MD, MPH Stroke Neurologist, Michigan Stroke Network; Assistant Professor of Neurology; Wayne
Anticoagulation Beyond Coumadin Saturday, September 21, 2013 Crystal Mountain Resort and Spa Pratik Bhattacharya MD, MPH Stroke Neurologist, Michigan Stroke Network; Assistant Professor of Neurology; Wayne
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Thrombosis and Thromboembolsim October Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy
 Thrombosis and Thromboembolsim October 2012 Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy Christian T. Ruff, MD, MPH TIMI Study Group Brigham and Women
Thrombosis and Thromboembolsim October 2012 Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy Christian T. Ruff, MD, MPH TIMI Study Group Brigham and Women
KCS Congress: Impact through collaboration
 Stroke Prevention in Atrial Fibrillation (SPAF) in Kenya Elijah N. Ogola FACC University of Nairobi Kenya Cardiac Society Annual Scientific Congress Mombasa 28 th June 1 st July 2017 KCS Congress: Impact
Stroke Prevention in Atrial Fibrillation (SPAF) in Kenya Elijah N. Ogola FACC University of Nairobi Kenya Cardiac Society Annual Scientific Congress Mombasa 28 th June 1 st July 2017 KCS Congress: Impact
controversies in anticoagulation: optimizing outcome for atrial fibrillation
 controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012
 Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012 Professor Dan Atar Head, Dept. of Cardiology Councillor of the ESC,
Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012 Professor Dan Atar Head, Dept. of Cardiology Councillor of the ESC,
DOAC the story so far... Dr GM Benson Director NI Haemophilia and Thrombosis Centre BHSCT
 DOAC the story so far... Dr GM Benson Director NI Haemophilia and Thrombosis Centre BHSCT A rose by any other name.. Recommendation on the nomenclature for oral anticoagulants: communication from the SSC
DOAC the story so far... Dr GM Benson Director NI Haemophilia and Thrombosis Centre BHSCT A rose by any other name.. Recommendation on the nomenclature for oral anticoagulants: communication from the SSC
IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS?
 IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS? J.Y. LE HEUZEY Georges Pompidou Hospital, René Descartes University, Paris H E G P Munich, August 27, 2012 Disclosure Consultant / Conferences / Advisory
IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS? J.Y. LE HEUZEY Georges Pompidou Hospital, René Descartes University, Paris H E G P Munich, August 27, 2012 Disclosure Consultant / Conferences / Advisory
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Dabigatran Evidence in Real Practice
 ADVANCES IN CARDIAC ARRHYTHMIAS and GREAT INNOVATIONS IN CARDIOLOGY XXVII GIORNATE CARDIOLOGICHE TORINESI Torino, Centro Congressi Unione Industriale 23-24 Ottobre 2015 Dabigatran Evidence in Real Practice
ADVANCES IN CARDIAC ARRHYTHMIAS and GREAT INNOVATIONS IN CARDIOLOGY XXVII GIORNATE CARDIOLOGICHE TORINESI Torino, Centro Congressi Unione Industriale 23-24 Ottobre 2015 Dabigatran Evidence in Real Practice
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Survey patients for Sx, signs of AF. Establish AF Dx. Evaluate & Tx underlying heart disease/other causes. Assess adequacy of rate or rhythm control
 Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali
 Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali Gianluca Botto, MD, FAAC, FESC Divisione di Cardiologia Ospedale Sant Anna, Como The Promise of NOAs Antithrombotic
Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali Gianluca Botto, MD, FAAC, FESC Divisione di Cardiologia Ospedale Sant Anna, Como The Promise of NOAs Antithrombotic
Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion
 Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion John Rickard MD, MPH Staff Electrophysiologist Cleveland Clinic Agenda NOACs: Update on Real World Data NOAC reversal:
Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion John Rickard MD, MPH Staff Electrophysiologist Cleveland Clinic Agenda NOACs: Update on Real World Data NOAC reversal:
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Novel Anticoagulants PHYSICIANS UPDATE 2014
 Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention
 Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania
Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING
 DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
Lessons from recent antithrombotic studies and trials in atrial fibrillation
 Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now. Bradley A. Hardin, MD Richard F.
 The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated?
 Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated? Renato D. Lopes, MD MHS PhD Professor of Medicine Division of Cardiology Duke Clinical
Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated? Renato D. Lopes, MD MHS PhD Professor of Medicine Division of Cardiology Duke Clinical
Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care
 Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care 11 th and 25 th September 2014 3 KEY OBJECTIVES OF TALK 1.
Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care 11 th and 25 th September 2014 3 KEY OBJECTIVES OF TALK 1.
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Dr Mammen Ninan GPwSI in Cardiology
 Dr Mammen Ninan GPwSI in Cardiology AF affects up to 835,000 people in England alone and is expected to rise year after year. AF is a known risk factor for stroke, the 3 rd highest cause of mortality in
Dr Mammen Ninan GPwSI in Cardiology AF affects up to 835,000 people in England alone and is expected to rise year after year. AF is a known risk factor for stroke, the 3 rd highest cause of mortality in
Atrial fibrillation: current approaches to management
 DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
Novel Anticoagulants: Emerging Evidence
 18/10/2016 Topics: Novel Anticoagulants: Emerging Evidence Dr Matthew Swale Electrophysiologist Genesis Care NOAC Novel Oral Anti Coagulant Now Non-Vit K Oral Anti Coagulant DOAC Direct Oral Anti Coagulant
18/10/2016 Topics: Novel Anticoagulants: Emerging Evidence Dr Matthew Swale Electrophysiologist Genesis Care NOAC Novel Oral Anti Coagulant Now Non-Vit K Oral Anti Coagulant DOAC Direct Oral Anti Coagulant
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
The Challenge and Opportunities for Stroke Prevention in AF
 20th International Symposium on Thromboembolism October 2013 in London, United Kingdom Plenary Session I: Thromboembolic Stroke The Challenge and Opportunities for Stroke Prevention in AF John Camm St.
20th International Symposium on Thromboembolism October 2013 in London, United Kingdom Plenary Session I: Thromboembolic Stroke The Challenge and Opportunities for Stroke Prevention in AF John Camm St.
Model guidance for prescribers
 Model guidance for prescribers Dabigatran Etexilate and Rivaroxaban for the Prevention of Stroke and Systemic Embolism in Adults with Non-valvular Atrial Fibrillation This document includes the following
Model guidance for prescribers Dabigatran Etexilate and Rivaroxaban for the Prevention of Stroke and Systemic Embolism in Adults with Non-valvular Atrial Fibrillation This document includes the following
Anti coagulation Treatment Effects of Age Impact of NOAC. June 2014 Dov Gavish MD FESC Tel Aviv University ISRAEL
 Anti coagulation Treatment Effects of Age Impact of NOAC June 2014 Dov Gavish MD FESC Tel Aviv University ISRAEL PE VTE: deep vein thrombosis and pulmonary embolism are common in elderly Thrombosis is
Anti coagulation Treatment Effects of Age Impact of NOAC June 2014 Dov Gavish MD FESC Tel Aviv University ISRAEL PE VTE: deep vein thrombosis and pulmonary embolism are common in elderly Thrombosis is
Newer Anti-Anginal Agents and Anticoagulants
 Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
Dr Calum Young Cardiologist Tauranga
 Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated) GPCME 2016: Anticoagulation
Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated) GPCME 2016: Anticoagulation
New oral factor Xa inhibitors. Lessons from AVERROES and ARISTOTLE trials
 New oral factor Xa inhibitors. Lessons from AVERROES and ARISTOTLE trials Dimitri Richter, MD, FESC, FAHA Head of Cardiac Dept., Athens Euroclinic General Secretary of Hellenic Lipidology Society Member
New oral factor Xa inhibitors. Lessons from AVERROES and ARISTOTLE trials Dimitri Richter, MD, FESC, FAHA Head of Cardiac Dept., Athens Euroclinic General Secretary of Hellenic Lipidology Society Member
New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy
 New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy Hans-Christoph Diener Department of Neurology and Stroke Center University Hospital Essen Germany Conflict of Interest
New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy Hans-Christoph Diener Department of Neurology and Stroke Center University Hospital Essen Germany Conflict of Interest
NOACs in AF. Dr Fiona Stewart. Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Fiona Stewart Auckland Heart Group and Auckland DHB NOACS for AF True/False All patients should have a CHA 2 DS 2 VASc risk assessment on diagnosis of AF NOACS are more effective than warfarin
NOACs in AF Dr Fiona Stewart Auckland Heart Group and Auckland DHB NOACS for AF True/False All patients should have a CHA 2 DS 2 VASc risk assessment on diagnosis of AF NOACS are more effective than warfarin
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
NOAC 2015: What Have We Learned?
 NOAC 2015: What Have We Learned? Milan Gupta, MD Canadian Cardiovascular Research Network University of Toronto, McMaster University www.ccrnmd.com Disclosures Honoraria / Research Grants Abbott, Aegerion
NOAC 2015: What Have We Learned? Milan Gupta, MD Canadian Cardiovascular Research Network University of Toronto, McMaster University www.ccrnmd.com Disclosures Honoraria / Research Grants Abbott, Aegerion
What s New in the AF Guidelines
 Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION
 FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION") RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION Craig I. Coleman, PharmD Professor, University of Connecticut School
RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION Craig I. Coleman, PharmD Professor, University of Connecticut School
Evaluate Risk of Stroke & Bleeding in AF Patients
 XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution
 Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
AF review. Petr Polasek
 AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
2 Summary of NICE TA 249: Atrial fibrillation - Dabigatran Etexilate
 Service Notification in response to DHSSPS endorsed NICE Technology Appraisals NICE TA 249: Atrial fibrillation - Dabigatran Etexilate 1 Name of Commissioning Team Long Term Conditions Commissioning Team
Service Notification in response to DHSSPS endorsed NICE Technology Appraisals NICE TA 249: Atrial fibrillation - Dabigatran Etexilate 1 Name of Commissioning Team Long Term Conditions Commissioning Team
The Age of the Novel Anticoagulants. Peter Netzler, MD April 21, 2017 Carolina Cardiology Electrophysiology
 The Age of the Novel Anticoagulants Peter Netzler, MD April 21, 2017 Carolina Cardiology Electrophysiology Disclosures Speaker bureau for the Bristol-Myers Squibb and Pfizer alliance for Eliquis Direct
The Age of the Novel Anticoagulants Peter Netzler, MD April 21, 2017 Carolina Cardiology Electrophysiology Disclosures Speaker bureau for the Bristol-Myers Squibb and Pfizer alliance for Eliquis Direct
TSHP 2014 Annual Seminar 1
 Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
Defining Sub-Clinical Atrial Fibrillation and its management
 Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
Implementation of NICE TA 249 and NICE TA 256
 Implementation of NICE TA 249 and NICE TA 256 Dabigatran and rivaroxaban for the prevention of stroke and systemic embolism in atrial fibrillation Version 1.0 Background NICE has recently issued guidance
Implementation of NICE TA 249 and NICE TA 256 Dabigatran and rivaroxaban for the prevention of stroke and systemic embolism in atrial fibrillation Version 1.0 Background NICE has recently issued guidance
Stroke Prevention & Atrial Fibrillation. Susanne Christie Arrhythmia Nurse Specialist 24 th September 2015
 Stroke Prevention & Atrial Fibrillation Susanne Christie Arrhythmia Nurse Specialist 24 th September 2015 Learning Outcomes What is Atrial Fibrillation? Why is Atrial Fibrillation important? What causes
Stroke Prevention & Atrial Fibrillation Susanne Christie Arrhythmia Nurse Specialist 24 th September 2015 Learning Outcomes What is Atrial Fibrillation? Why is Atrial Fibrillation important? What causes
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
Show Me the Outcomes!
 Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS
: COMPARISON AND FREQUENTLY ASKED QUESTIONS") NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Half Moon Bay Treatment of Atrial Fibrillation. Dr. Roger A. Winkle MD. Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital
 Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest