Heart Failure October 8, 2011
|
|
|
- Sharleen Hicks
- 5 years ago
- Views:
Transcription
1 HFrEF Michael Muellerleile M.D. Goals of Presentation Touch on pathophysiology of chronic systolic heart failure Review assessment and outpatient pharmacologic management of HFrEF Highlight non-pharmacologic therapy for chronic systolic heart failure and when to refer Cardiac Rehab for HFrEF Stages of Heart Failure STAGE A STAGE B STAGE C STAGE D At Risk : High risk for developing HF Asymptomatic LV dysfunction Symptomatic : Past or current symptoms of HF End-stage HF 1

2 Applying Classification of Recommendations and Level of Evidence Class Class a Class b Class Benefit >>> Risk Procedure/ Treatment SHOULD be performed/ administered Benefit >> Risk Additional studies with focused objectives needed T S REASONABLE to perform procedure/administer treatment Benefit Risk Additional studies with broad objectives needed; Additional registry data would be helpful Procedure/Treatment MAY BE CONSDERED Risk Benefit No additional studies needed Procedure/Treatment should NOT be performed/administered SNCE T S NOT HELPFUL AND MAY BE HARMFUL Level of Evidence: Goals of Presentation Touch on pathophysiology of chronic systolic heart failure Review assessment and outpatient pharmacologic management of HFrEF Highlight non-pharmacologic therapy for chronic systolic heart failure and when to refer Cardiac Rehab for HFrEF 2
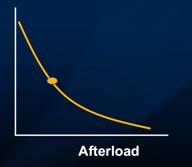
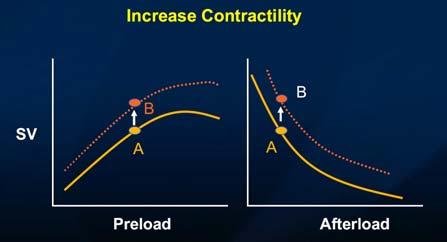
3 SV 3

4 4
5 a b Hospitalized Patient Precipitating Factors for Acute HF t is recommended that the following common potential precipitating factors for acute HF be identified as recognition of these comorbidities, is critical to guide therapy: acute coronary syndromes/coronary ischemia severe hypertension atrial and ventricular arrhythmias infections pulmonary emboli renal failure medical or dietary noncompliance Volume Status nitial Clinical Assessment of Heart Failure dentifying and Evaluating Noncardiac Disorders or Behaviors a b History of alcohol, illicit drugs, chemotherapy drugs. nitial examination should include assessment of the patient s volume status, orthostatic blood pressure changes, measurement of weight 5
 Walking (2 mph) 2.5 Mowing lawn (power mower) 3.0 Walking (3 mph) 3.")
6 nitial Clinical Assessment of Heart Failure nitial Assessment and Examination of Patients With HF a b nitial assessment should be made of the patient s ability to perform activities of daily living. nitial Clinical Assessment of Patients Presenting With Heart Failure Estimated Energy Requirements of Selected Activities (METs) Walking (2 mph) 2.5 Mowing lawn (power mower) 3.0 Walking (3 mph) 3.3 Cycling (leisurely) 3.5 Gardening (no lifting) 4.4 Chopping wood 4.9 Cycling (moderately) 5.7 6
7 nitial Clinical Assessment of Heart Failure nitial Laboratory Evaluation a b nitial laboratory evaluation CBC, urinalysis, serum electrolytes (including calcium and magnesium), BUN, serum creatinine, fasting blood glucose (glycohemoglobin), lipid profile, liver function tests, and TSH. Screening for hemochromatosis, sleep-disturbed breathing, or HV is reasonable in selected patients who present with HF. nitial Clinical Assessment of Heart Failure Diagnostic Tests a b Diagnostic tests for rheumatologic diseases, amyloidosis, or pheochromocytoma are reasonable in patients presenting with HF in whom there is a clinical suspicion of these diseases. nitial Clinical Assessment of Heart Failure a b Measurement of BNP and Noninvasive maging Measurement of natriuretic peptides (BNP) can be useful in the evaluation of patients presenting in the urgent care setting in whom the clinical diagnosis of HF is uncertain. Measurement of natriuretic peptides can be helpful in risk stratification. 7
8 nitial Clinical Assessment of Heart Failure a b Twelve-lead EKG, chest radiograph (posterior-anterior and lateral) should be performed. nitial Clinical Assessment of Heart Failure Two-Dimensional Echocardiography a b Echocardiography with Doppler should be performed to assess (LVEF), left ventricle size, wall thickness, and valve function. Radionuclide ventriculography can be performed to assess LVEF and volumes. nitial Clinical Assessment of With Heart Failure Noninvasive maging and Exercise Testing Detecting Myocardial schemia a b Noninvasive imaging to detect myocardial ischemia is reasonable in patients presenting with HF who have known coronary artery disease and no angina. 8
9 nitial Clinical Assessment of Heart Failure Coronary Revascularization a b Coronary arteriography is reasonable for patients presenting with HF who have chest pain that may or may not be of cardiac origin who have not had evaluation of their coronary anatomy Goals of Presentation Touch on pathophysiology of chronic systolic heart failure Review assessment and outpatient pharmacologic management of HFrEF Highlight non-pharmacologic therapy for chronic systolic heart failure and when to refer Cardiac Rehab for HFrEF Goals of Presentation Touch on pathophysiology of chronic systolic heart failure Review assessment and outpatient pharmacologic management of HFrEF Highlight non-pharmacologic therapy for chronic systolic heart failure and when to refer Cardiac Rehab for HFrEF 9

10 Reduced Left Ventricular Ejection Fraction a b Diuretics and salt restriction are indicated in patients with current or prior symptoms of HF and reduced LVEF who have evidence of fluid retention. Reduced Left Ventricular Ejection Fraction a b Angiotensin-converting enzyme (ACE) inhibitors are recommended for all patients with current or prior symptoms of HF and reduced LVEF. 10


11 Reduced Left Ventricular Ejection Fraction a b bisoprolol, carvedilol, and sustained release metoprolol succinate is recommended for all stable patients with current or prior symptoms of HF and reduced LVEF. Beta Blockers 11
12 Reduced Left Ventricular Ejection Fraction Angiotensin ll Receptor Blockers a b Angiotensin receptor blockers are recommended inpatient with current or prior symptoms of HF and reduced LVEF who are ACE- inhibitor intolerant a b Avoid nonsteroidal anti-inflammatory drugs, most antiarrhythmic drugs, and most calcium channel blocking drugs). Angiotensin Receptor Blockers Reduced Left Ventricular Ejection Fraction a b The Risks of Aldosterone Antagonists Addition of an aldosterone antagonist is recommended in selected patients with moderately severe to severe symptoms of HF and reduced LVEF who can be carefully monitored for preserved renal function and normal potassium concentration. Under circumstances where monitoring for hyperkalemia or renal dysfunction is not anticipated to be feasible, the risks may outweigh the benefits of aldosterone antagonists. 12

13 Spironolactone/Aldactone Reduced Left Ventricular Ejection Fraction Recommendations for Hydralazine and Nitrates a b The combination of hydralazine and nitrates is recommended to improve outcomes for patients self-described as African- Americans, with moderate-severe symptoms on optimal therapy with ACE inhibitors, beta blockers, and diuretics. a b The addition of a combination of hydralazine and a nitrate is reasonable for patients with reduced LVEF who are already taking an ACE inhibitor and beta blocker for symptomatic HF and who have persistent symptoms. Reduced Left Ventricular Ejection Fraction a b A combination of hydralazine and a nitrate might be reasonable in patients with current or prior symptoms of HF and reduced LVEF who cannot be given an ACE inhibitor or ARB because of drug intolerance, hypotension, or renal insufficiency. 13
14 Reduced Left Ventricular Ejection Fraction The Benefits of Digitalis a b Digitalis can be beneficial in patients with current or prior symptoms of HF and reduced LVEF to decrease hospitalizations for HF. Sacubitril/Valsartan Neprilysin inhibitor, sacubitril, (neutral endopeptidase; NEP) via LBQ657, the active metabolite of the prodrug sacubitril ncreased levels of peptides that are degraded by neprilysin, such as natriuretic peptides. Angiotensin angiotensin type-1 (AT1) receptor blocker valsartan. Sacubitril/Valsartan All-cause Mortality PARADGM-HF Number randomized: Ernesto = 4,187 Enalapril = 4,212 All-cause mortality 711 (17.0%) versus 835 (19.8%) Risk ratio 0.80 (0.76, 0.93) p= % reduction 14
15 Sacubitril/Valsartan ADVERSE REACTONS: Angioedema, Hypotension, mpaired Renal Function, Hyperkalemia Sacubitril/Valsartan is contraindicated with concomitant use of an angiotensin-converting enzyme (ACE) inhibitor. f switching from an ACE inhibitor to ENTRESTO allow a washout period of 36 hours between administration of the two drugs. The recommended starting dose of ENTRESTO is 49/51 mg twicedaily. Double the dose of ENTRESTO after 2 to 4 weeks to the target maintenance dose of 97/103 mg twice daily, as tolerated vabradine Corlanor (ivabradine) is a hyperpolarization-activated cyclic nucleotide-gated channel blocker indicated to reduce the risk of hospitalization for worsening heart failure in patients with stable, symptomatic chronic heart failure with left ventricular ejection fraction 35%, who are in sinus rhythm with resting heart rate 70 beats per minute and either are on maximally tolerated dose vabradine Contraindications: Acute decompensated heart failure, Blood pressure less than 90/50 mmhg, Sick sinus syndrome, sinoatrial block or 3rd degree AV block, unless a functioning demand pacemaker is present, Resting heart rate less than 60 bpm prior to treatment, Severe hepatic impairment, Pacemaker dependence (heart rate maintained exclusively by the pacemaker) (4) n combination with strong cytochrome CYP3A4 inhibitors. 15
16 vabradine Dose Adjustment Heart Rate Dose Adjustment: > 60 bpm ncrease dose by 2.5 mg (given twice daily) up to a maximum dose of 7.5 mg twice daily bpm Maintain dose < 50 bpm or signs and symptoms of bradycardia. Decrease dose by 2.5 mg (given twice daily); if current dose is 2.5 mg twice daily, discontinue therapy vabradine Goals of Presentation Touch on pathophysiology of chronic systolic heart failure Review outpatient pharmacologic management of HFrEF Highlight non-pharmacologic therapy for chronic systolic heart failure and when to refer Cardiac Rehab for HFrEF 16
17 Goals of Presentation Touch on pathophysiology of chronic systolic heart failure Review outpatient pharmacologic management of HFrEF Highlight non-pharmacologic therapy for chronic systolic heart failure and when to refer Cardiac Rehab for HFrEF Patients With Reduced Left Ventricular Ejection Fraction Secondary Prevention: CD mplantable Cardioverter-Defibrillator a b A cardioverter-defibrillator (CD) is recommended as secondary prevention to prolong survival in patients with a history of cardiac arrest, ventricular fibrillation, or hemodynamically destabilizing ventricular tachycardia. Reduced Left Ventricular Ejection Fraction a b Primary Prevention: CD CD therapy is recommended for primary prevention of sudden cardiac death to reduce total mortality in patients with nonischemic dilated cardiomyopathy or ischemic heart disease at least 40 days post-myocardial infraction, have an LVEF less than or equal to 35%, with NYHA functional class or symptoms while receiving chronic optimal medical therapy, and who have expectation of survival for more than 1 year. 17

18 Reduced Left Ventricular Ejection Fraction Resynchronization Therapy: BiV a b Patients with LVEF less than or equal to 35%, sinus rhythm, and NYHA functional class or ambulatory class V symptoms despite recommended, optimal medical therapy and who have cardiac dyssynchrony, which is currently defined as a QRS duration greater than or equal to 0.12 seconds, should receive cardiac resynchronization therapy, with or without an CD. Resynchronization Cardiac Rehabilitation for Systolic Heart Failure The Centers for Medicare & Medicaid Services (CMS) has determined that the evidence is sufficient to expand coverage for cardiac rehabilitation services under 42 C.F.R (b)(1)(vii) to beneficiaries with stable, chronic heart failure defined as patients with left ventricular ejection fraction of 35% or less and New York Heart Association (NYHA) class to V symptoms despite being on optimal heart failure therapy for at least six weeks. Stable patients are defined as patients who have not had recent ( 6 weeks) or planned ( 6 months) major cardiovascular hospitalizations or procedures 18

19 Cardiac Rehabilitation for Systolic Heart Failure A major trial of exercise and HF randomly assigned 2331 patients (mean EF, 25%; ischemic etiology, 52%) to either exercise training for 3 months or usual care. n unadjusted analyses, there was no significant difference. HF-ACTON Randomized Controlled Trial Effects of Exercise Training on Health Status in Patients With Chronic Heart Failure Kathryn E. Flynn, PhD David J. Whellan, MD, MHS James A. Blumenthal, PhD Lawrence J. Fine, MD, DrPH Steven J. Keteyian, PhD William E. Kraus, MD Kevin A. Schulman, MD Christopher M. O Connor, MD leana L. Pina, MD Li Lin, MS Stephen J. Ellis, PhD Jonathan G. Howlett, MD Dalane W. Kitzman, MD Nancy Houston Miller, RN, BSN John A. Spertus, MD, MPH Kevin P. Weinfurt, PhD JAMA. 2009;301(14): Cardiac Rehabilitation for Systolic Heart Failure 19
 in the exercise training group. 20")
20 Cardiac Rehabilitation for Systolic Heart Failure Cardiac Rehabilitation for Systolic Heart Failure Cardiac Rehabilitation for Systolic Heart Failure When adjusted for coronary heart disease risk factors, there was an 11% reduction in all-cause mortality, cardiovascular disease mortality, or hospitalizations (P<0.03) in the exercise training group. 20

.")
21 Cardiac Rehabilitation for Systolic Heart Failure The ExTraMATCH study, a meta-analysis, demonstrated improved peak oxygen consumption and decreased all-cause mortality with exercise. Piepoli M.F., Davos C., Francis D.P., et al: Exercise training meta-analysis of trials in patients with chronic heart failure (ExTraMATCH). BMJ 2004; 328: pp. 189 Cardiac Rehabilitation for Systolic Heart Failure Cardiac Rehabilitation for Systolic Heart Failure 21




22 Cardiac Rehabilitation for Heart Failure Cardiac rehabilitation can be useful in clinically stable patients with HF to improve functional capacity, exercise duration, HRQOL, and mortality. Cardiac Rehabilitation for Heart Failure a b Exercise training (or regular physical activity) is recommended as safe and effective for patients with HF who are able to participate to improve functional status Davies EJ, Moxham T, Rees K, et al. Exercise training for systolic heart failure: Cochrane systematic review and meta-analysis. Eur J Heart Fail 2010;12: McKelvie R.S.: Exercise training in patients with heart failure: clinical outcomes, safety, and indications. Heart Fail Rev 2008; 13: pp O Connor C.M., Whellan D.J., Lee K.L., et al: Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTON randomized controlled trial. JAMA 2009; 301: pp Pina.L., Apstein C.S., Balady G.J., et al: Exercise and heart failure: a statement from the American Heart Association Committee on Exercise, Rehabilitation, and Prevention. Circulation 2003; 107: pp


23 23
ACC Heart Failure Guidelines Slide Set
 ACC Heart Failure Guidelines Slide Set Based on the 2009 Focused Update ncorporated nto the ACCF/AHA 2005 guidelines for the Diagnosis and Management of Heart Failure in Adults: A Report of the American
ACC Heart Failure Guidelines Slide Set Based on the 2009 Focused Update ncorporated nto the ACCF/AHA 2005 guidelines for the Diagnosis and Management of Heart Failure in Adults: A Report of the American
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Saudi Heart Failure Guidelines. Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group
 Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart.org/HFGuidelinesToolkit
 2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Corlanor. Corlanor (ivabradine) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.05 Subject: Corlanor Page: 1 of 5 Last Review Date: June 24, 2016 Corlanor Description Corlanor (ivabradine)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.05 Subject: Corlanor Page: 1 of 5 Last Review Date: June 24, 2016 Corlanor Description Corlanor (ivabradine)
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD
 New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD Professor of Medicine, Cell Biology, Radiology and Surgery Director, The Howard Gilman Institute for Heart Valve Disease and the Schiavone
New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD Professor of Medicine, Cell Biology, Radiology and Surgery Director, The Howard Gilman Institute for Heart Valve Disease and the Schiavone
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham
 Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Pharmacology. Update. Learning Objectives. Learning Objectives. for Advanced Practice Nurses
 Pharmacology Update for Advanced Practice Nurses Trish Freeman, RPh, PhD Associate Professor, Pharmacy Practice and Science University of Kentucky College of Pharmacy University of Southern Indiana September
Pharmacology Update for Advanced Practice Nurses Trish Freeman, RPh, PhD Associate Professor, Pharmacy Practice and Science University of Kentucky College of Pharmacy University of Southern Indiana September
I have no disclosures. Disclosures
 I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
CORLANOR (ivabradine) oral tablet
 oral tablet") CORLANOR (ivabradine) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
CORLANOR (ivabradine) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
SCOMPENSO CARDIACO: IL PUNTO DELLA RICERCA
 Journal Club 19 Marzo 2010 SCOMPENSO CARDIACO: IL PUNTO DELLA RICERCA Alessandro Giordano Prevalence of heart failure by sex and age (NHANES:1999-2004) Circulation 2007 Incidence of heart failure by age
Journal Club 19 Marzo 2010 SCOMPENSO CARDIACO: IL PUNTO DELLA RICERCA Alessandro Giordano Prevalence of heart failure by sex and age (NHANES:1999-2004) Circulation 2007 Incidence of heart failure by age
Update in Congestive Hear Failure DRAGOS VESBIANU MD
 Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
New Winners in the World of Heart Failure. Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015
 New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Citation. What is New in the 2013 ACC/AHA HF Guideline. Dimensions in Heart and Vascular Care Penn State Heart and Vascular Institute
 What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION
 MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Balanced information for better care. Heart failure: Managing risk and improving patient outcomes
 Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION
 CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION SACUBITRIL/VALSARTAN (Entresto Novartis Pharmaceuticals) Indication: Heart Failure With Reduced Ejection Fraction Recommendation: The Canadian
CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION SACUBITRIL/VALSARTAN (Entresto Novartis Pharmaceuticals) Indication: Heart Failure With Reduced Ejection Fraction Recommendation: The Canadian
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine
 Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
REVIEW ARTICLE. Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2
 Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2 1 University of Missouri School of Medicine, Columbia, MO 2 Division of Cardiovascular Medicine, Department
Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2 1 University of Missouri School of Medicine, Columbia, MO 2 Division of Cardiovascular Medicine, Department
Learn and LiveSM. ACC/AHA Pocket Guideline. Based on the ACC/AHA 2005 Guideline Update. Diagnosis and Management of Chronic Heart Failure in the Adult
 Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2005 Guideline Update Diagnosis and Management of Chronic Heart Failure in the Adult August 2005 I Assessment Characterization Therapy Special
Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2005 Guideline Update Diagnosis and Management of Chronic Heart Failure in the Adult August 2005 I Assessment Characterization Therapy Special
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Heart. Severe. Failure. Congestive heart failure (CHF) is very. What you can do for your patients
 is very. What you can do for your patients") Focus on CME at the University of Université Manitoba de Sherbrooke By Anne Fradet, MD, FRCP, CSPQ Severe Heart Failure What you can do for your patients The case of Mr. White Mr. White, 72, comes to your
Focus on CME at the University of Université Manitoba de Sherbrooke By Anne Fradet, MD, FRCP, CSPQ Severe Heart Failure What you can do for your patients The case of Mr. White Mr. White, 72, comes to your
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure. Elizabeth Pogge, PharmD, MPH, BCPS, FASCP
 Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Assessment and Diagnosis of Heart Failure
 Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
The Management of Heart Failure after Biventricular Pacing
 The Management of Heart Failure after Biventricular Pacing Juan M. Aranda, Jr., MD University of Florida College of Medicine, Division of Cardiovascular Medicine, Gainesville, Florida Approximately 271,000
The Management of Heart Failure after Biventricular Pacing Juan M. Aranda, Jr., MD University of Florida College of Medicine, Division of Cardiovascular Medicine, Gainesville, Florida Approximately 271,000
PROGRESS AT LAST?: REVIEWING RECENTLY UPDATED ACCF/AHA HEART FAILURE GUIDELINES
 PROGRESS AT LAST?: REVIEWING RECENTLY UPDATED ACCF/AHA HEART FAILURE GUIDELINES Jon Linder, Pharm.D. PGY1 Pharmacy Resident Iowa City VA Health Care System Objectives for Pharmacists Summarize the burden
PROGRESS AT LAST?: REVIEWING RECENTLY UPDATED ACCF/AHA HEART FAILURE GUIDELINES Jon Linder, Pharm.D. PGY1 Pharmacy Resident Iowa City VA Health Care System Objectives for Pharmacists Summarize the burden
Outline. Chronic Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients
 Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients Javed Butler, MD, MPH, MBA Patrick H. Lehan Professor of Medicine Professor of Physiology Chairman,
Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients Javed Butler, MD, MPH, MBA Patrick H. Lehan Professor of Medicine Professor of Physiology Chairman,
Common Drug Review Clinical Review Report
 Common Drug Review Clinical Review Report June 2017 Drug Ivabradine hydrochloride (Lancora) Indication For the treatment of stable chronic heart failure with reduced left ventricular ejection fraction
Common Drug Review Clinical Review Report June 2017 Drug Ivabradine hydrochloride (Lancora) Indication For the treatment of stable chronic heart failure with reduced left ventricular ejection fraction
Heart Failure Management: Continuum of Care
 Healthy Kingsport Conference Heart Failure Management: Continuum of Care Robin Harris PhD, ANP-BC, ACNS-BC Clinical Assistant Professor University of Tennessee College of Nursing Important Info I, Robin
Healthy Kingsport Conference Heart Failure Management: Continuum of Care Robin Harris PhD, ANP-BC, ACNS-BC Clinical Assistant Professor University of Tennessee College of Nursing Important Info I, Robin
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Target dose achievement of evidencebased medications in patients with heart failure with reduced ejection fraction attending a heart failure clinic
 Target dose achievement of evidencebased medications in patients with heart failure with reduced ejection fraction attending a heart failure clinic June Chen 1, Charlotte Galenza 1, Justin Ezekowitz 2,3,
Target dose achievement of evidencebased medications in patients with heart failure with reduced ejection fraction attending a heart failure clinic June Chen 1, Charlotte Galenza 1, Justin Ezekowitz 2,3,
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Initiating New Medications in the Management of Heart Failure
 Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
ESC Guidelines. ESC Guidelines Update For internal training purpose. European Heart Journal, doi: /eurheart/ehn309
 ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
Heart Failure. GP Update Refresher 18 th January 2018
 GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Incidence. 4.8 million in the United States. 400,000 new cases/year. 20 million patients with asymptomatic LV dysfunction
 Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness