Update in Congestive Hear Failure DRAGOS VESBIANU MD
|
|
|
- Harriet Underwood
- 5 years ago
- Views:
Transcription
1 Update in Congestive Hear Failure DRAGOS VESBIANU MD
2 Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks. He also has a hard time climbing steps. Denies cough and has occasional wheezing. He usually sleeps on 2 pillows because of back problems. Has gained 10 lbs in the last month, but it s not unusual for his weight to fluctuate.
3 Case PMH: HTN, DM 2, HLD, COPD Meds: Lipitor, HCTZ, Metformin, Lantus, Advair, Albuterol BID Physical exam: Comfortable, not SOB at rest Bilateral wheezing and rales lower lungs S1, S2, RRR +1 b/l LE pitting edema
4 Symptoms in HF Common Symptoms: -dyspnea -edema -fatigue -wheezing Subtle symptoms: -abdominal pain, nausea, anorexia -confusion -lethargy
5 Initial Workup of Stage C HF After detailed history; Initial laboratory evaluation: CBC, urinalysis, CMP (including calcium and magnesium), fasting lipid profile, TSH, iron panel, Serial monitoring, when indicated, should include serum electrolytes and renal function, BNP, +/-CE A 12-lead ECG should be performed initially on all patients presenting with HF. Chest X-ray in all patients with new onset HF. Echocardiogram in all patients with new dx of HF (MUGA in some) Repeat echo usually for a significant change in clinical status or for consideration of changes after therapy or to evaluate for device therapy. Noninvasive stress imaging or cardiac cath is reasonable in HF and suspected CAD
6 Role of BNP in chronic HF BNP and NT-proBNP are sensitive (92-93%) and can help rule out heart failure BNP has prognostic value and can be used for risk stratification BNP guided therapy may play a role especially in hospitalized patients.
7 Case You start the patient on Lasix 40 mg BID. He calls in 5 days to let you know he is doing much better. You check an Echocardiogram that shows, LVH, bilateral atrial enlargement, EF of 30% What do you do next?
8 Definition of Heart Failure Classification I. Heart Failure with Reduced Ejection Fraction (HFrEF) Ejection Fraction Description 40% Also referred to as systolic HF. Randomized clinical trials have mainly enrolled patients with HFrEF and it is only in these patients that efficacious therapies have been demonstrated to date. II. Heart Failure with Preserved Ejection Fraction (HFpEF) 50% Also referred to as diastolic HF. Several different criteria have been used to further define HFpEF. The diagnosis of HFpEF is challenging because it is largely one of excluding other potential noncardiac causes of symptoms suggestive of HF. To date, efficacious therapies have not been identified. a. HFpEF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their characteristics, treatment patterns, and outcomes appear similar to those of patient with HFpEF. b. HFpEF, Improved >40% It has been recognized that a subset of patients with HFpEF previously had HFrEF. These patients with improvement or recovery in EF may be clinically distinct from those with persistently preserved or reduced EF. Further research is needed to better characterize these patients.
9 Classification of Heart Failure A B C D ACCF/AHA Stages of HF At high risk for HF but without structural heart disease or symptoms of HF. Structural heart disease but without signs or symptoms of HF. Structural heart disease with prior or current symptoms of HF. Refractory HF requiring specialized interventions. None I I II III IV NYHA Functional Classification No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF. Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF. Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.
10 Pharmacological Treatment for Stage C HFrEF Tequila shot vs Penicillin shot I IIa IIb III Diuretics are recommended in patients with HFrEF who have evidence of fluid retention, unless contraindicated, to improve symptoms. I IIa IIb III ACE inhibitors are recommended in patients with HFrEF and current or prior symptoms, unless contraindicated, to reduce morbidity and mortality. I IIa IIb III ARBs are recommended in patients with HFrEF with current or prior symptoms who are ACE inhibitor-intolerant, unless contraindicated, to reduce morbidity and mortality.
11 Pharmacological Treatment for Stage C HFrEF (cont.) Tequila shot vs Penicillin shot I IIa IIb III Harm Routine combined use of an ACE inhibitor, ARB, and aldosterone antagonist is potentially harmful for patients with HFrEF. I IIa IIb III Use of 1 of the 3 beta blockers proven to reduce mortality (i.e., bisoprolol, carvedilol, and sustainedrelease metoprolol succinate) is recommended for all patients with current or prior symptoms of HFrEF, unless contraindicated, to reduce morbidity and mortality.
12 Neprilysin as a Therapeutic Target Neprilysin breaks down endogenous vasoactive peptides, including the natriuretic peptides Inhibition of neprilysin potentiates the action of those peptides Because angiotensin II is also a substrate for neprilysin, neprilysin inhibitors must be co-administered with a RAAS blocker The combination of a neprilysin inhibitor and an ACEI is associated with unacceptably high rates of angioedema Natriuretic peptides Adrenomedullin Bradykinin Substance P (angiotensin II) Neprilysin Inactive fragments Sacubitril/Valsartan (LCZ696): Angiotensin Receptor Neprilysin Inhibitor (ARNI) Corti R et al. Circulation. 2001;104:
13
14 PARADIGM-HF: CV Death or HF Hospitalization (Primary Endpoint) 1. McMurray JJ et al. N Engl J Med. 2014;371:
15 SHIFT Trial Primary Composite Endpoint: CV Death or Hospitalization for Worsening HF Swedberg K et al. Lancet. 2010;376:
16 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure COR LOE Recommendation I B-R ACEI or ARB or ARNI in conjunction with β blockers + MRA (where appropriate) is recommended for patients with chronic HFrEF to reduce morbidity and mortality I B-R In patients with chronic, symptomatic HFrEF NYHA class II or III who tolerate an ACEI or ARB, replacement by an ARNI is recommended to further reduce morbidity and mortality III B-R ARNI should NOT be administered concomitantly with ACEI or within 36 hours of last ACEI dose III C-EO ARNI should NOT be administered to patients with a history of angioedema COR LOE Recommendations IIa B-R Ivabradine can be beneficial to reduce HF hospitalization for patients with symptomatic (NYHA class II-III), stable, chronic HFrEF (LVEF 35%) who are receiving GDMT, including a β blocker at maximally tolerated dose, and who are in sinus rhythm with a heart rate 70 bpm at rest 1. Yancy CW et al. J Am Coll Cardiol. 2016;68:
17 Pharmacological Treatment for Stage C HFrEF (cont.) I IIa IIb III Aldosterone receptor antagonists [or mineralocorticoid receptor antagonists (MRA)] are recommended in patients with NYHA class II-IV and who have LVEF of 35% or less, unless contraindicated, to reduce morbidity and mortality. Patients with NYHA class II should have a history of prior cardiovascular hospitalization or elevated plasma natriuretic peptide levels to be considered for aldosterone receptor antagonists. Creatinine should be 2.5 mg/dl or less in men or 2.0 mg/dl or less in women (or estimated glomerular filtration rate >30 ml/min/1.73m2) and potassium should be less than 5.0 meq/l. Careful monitoring of potassium, renal function, and diuretic dosing should be performed at initiation and closely followed thereafter to minimize risk of hyperkalemia and renal insufficiency.
18 Pharmacological Treatment for Stage C HFrEF (cont.) I IIa IIb III Aldosterone receptor antagonists are recommended to reduce morbidity and mortality following an acute MI in patients who have LVEF of 40% or less who develop symptoms of HF or who have a history of diabetes mellitus, unless contraindicated. I IIa IIb III Harm Inappropriate use of aldosterone receptor antagonists is potentially harmful because of life-threatening hyperkalemia or renal insufficiency when serum creatinine greater than 2.5 mg/dl in men or greater than 2.0 mg/dl in women (or estimated glomerular filtration rate <30 ml/min/1.73m2), and/or potassium above 5.0 meq/l.
19 Pharmacological Treatment for Stage C HFrEF (cont.) I IIa IIb III The combination of hydralazine and isosorbide dinitrate is recommended to reduce morbidity and mortality for patients self-described as African Americans with NYHA class III IV HFrEF receiving optimal therapy with ACE inhibitors and beta blockers, unless contraindicated. I IIa IIb III A combination of hydralazine and isosorbide dinitrate can be useful to reduce morbidity or mortality in patients with current or prior symptomatic HFrEF who cannot be given an ACE inhibitor or ARB because of drug intolerance, hypotension, or renal insufficiency, unless contraindicated.
20 Medical Therapy for Stage C HFrEF: Magnitude of Benefit Demonstrated in RCTs GDMT RR Reduction in Mortality NNT for Mortality Reduction (Standardized to 36 mo) RR Reduction in HF Hospitalizations ACE inhibitor or ARB 17% 26 31% Beta blocker 34% 9 41% Aldosterone antagonist 30% 6 35% Hydralazine/nitrate 43% 7 33%
21 Case Your guy had a few no shows in the clinic and you get a call from your hospitalist colleagues that he got admitted for CHF exacerbation. He presented to the hospital with shortness of breath and 30 lbs weight gain. BP is 160/96, HR is 93, sat 90% on RA. Positive JVDs, crackles bilaterally. BNP is Now on Coreg 6.25 mg, Lisinopril 10 mg and Spironolactone 25 mg How should approach his CHF exacerbation.
22 Triggers for acute decompensation Non compliance with medications Non compliance with diet Poorly controlled HTN Ischemia/ACS Afib Infections (demand ischemia) PE Worsening renal function
23 Management of acute decompensation Volume control Afterload and preload reduction Positive pressure ventilation Initiation of neuro-hormonal drugs Morphine use

24 Implantable Cardiac Defibrillators (ICD) Sustained ventricular tachycardia is associated with sudden cardiac death in HF. About one-third of mortality in HF is due to sudden cardiac death. ICDs for primary prevention have been shown to improve survival in selected patients with HF
25 Indications for ICD Therapy ICD therapy is recommended for primary prevention of SCD in selected patients with HFrEF at least 40 days post- MI with LVEF 35%, and NYHA class II or III symptoms on chronic GDMT, who are expected to live 1 year ICD therapy is recommended for primary prevention of SCD in selected patients with HFrEF at least 40 days post- MI with LVEF 30%, and NYHA class I symptoms while receiving GDMT, who are expected to live 1 year ** ICDs do not improve symptoms; most patients should be on GDMT; should have an expected lifeexpectancy of at least 1 year 2013 ACCF/AHA Guideline for the Management of Heart Failure
26 Sinus node Cardiac Resynchronization Pacing: Consequences of a Prolonged QRS Delayed Ventricular Activation Delayed lateral wall contraction Disorganized ventricular contraction Decreased pumping efficiency AV node Conduction block Reduction in diastolic filling times Prolongation of the duration of mitral regurgitation
27 Mechanism: Ventricular Resynchronization Sinus node AV node Conduction block Stimulation therapy Intraventricular Activation Organized ventricular activation sequence Coordinated septal and freewall contraction Improved pumping efficiency
28 Device Therapy for Stage C HFrEF I IIa IIb III I IIa IIb III ICD therapy is recommended for primary prevention of SCD to reduce total mortality in selected patients with nonischemic DCM or ischemic heart disease at least 40 days post-mi with LVEF of 35% or less, and NYHA class II or III symptoms on chronic GDMT, who have reasonable expectation of meaningful survival for more than 1 year. NYHA Class III/IV I IIa IIb III CRT is indicated for patients who have LVEF of 35% or less, sinus rhythm, left bundle-branch block (LBBB) with a QRS duration of 150 ms or greater, and NYHA class II, III, or ambulatory IV symptoms on GDMT. NYHA Class II
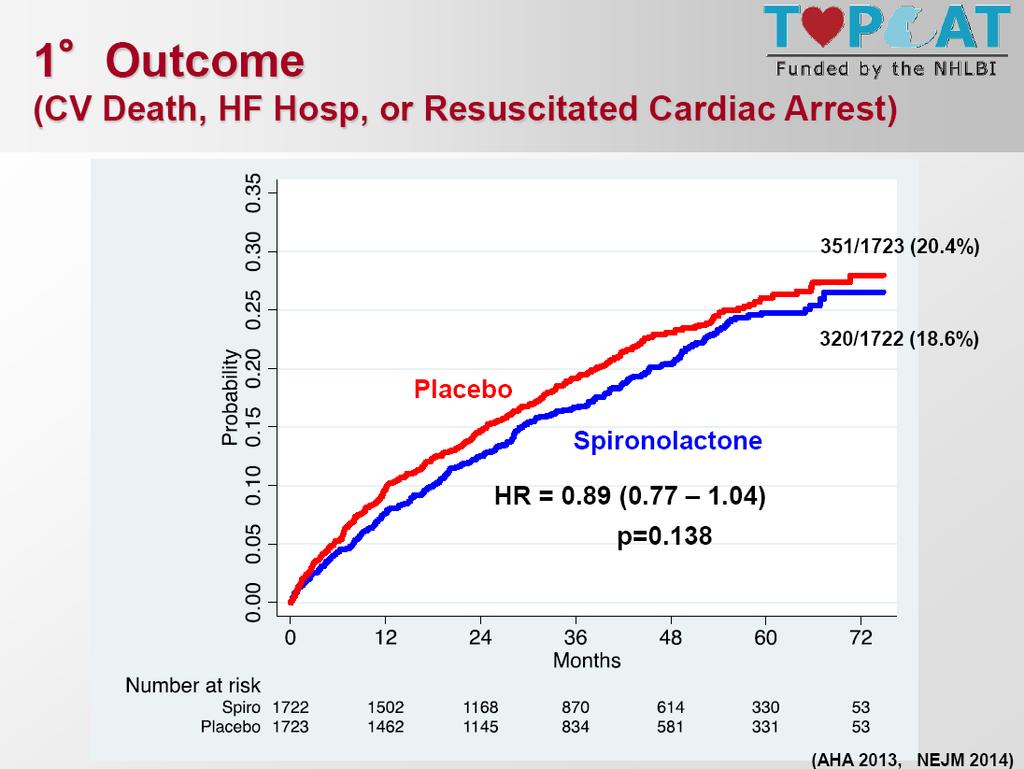
29 HFpEF THERAPY Goals Control symptoms Improve HRQOL Prevent hospitalization Prevent mortality Strategies Identification of comorbidities Treatment Diuresis to relieve symptoms of congestion Follow guideline driven indications for comorbidities, e.g., HTN, AF, CAD, DM Revascularization or valvular surgery as appropriate HFpEF HFrEF Trials THERAPY have not shown Goals Control symptoms Patient education Prevent hospitalization Prevent specifically mortality in HFpEF significant mortality or morbidity benefit with use of ACEI/ARB No trials showing definite benefit of Beta blockers, Drugs for routine use Diuretics for fluid retention ACEI sildenafil or ARB Beta blockers Aldosterone antagonists TOPCAT trial: Randomizeddouble blind trial of spironolactone (15-45 mg) vs. placebo in HFpEF patients (LVEF >45%) with Prior HF hospitalization or BNP > 100 pg/ml Drugs for use in selected patients Hydralazine/isosorbide dinitrate ACEI and ARB Digoxin In selected patients CRT ICD Revascularization or valvular surgery as appropriate Goals Con Imp Red rea Est of-li Optio Adv mea Hea Chr Tem MC Exp dru Pal hos ICD
30
31
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Citation. What is New in the 2013 ACC/AHA HF Guideline. Dimensions in Heart and Vascular Care Penn State Heart and Vascular Institute
 What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
What s new in the 2017 heart failure guidelines. Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA
 What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges
 Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Outline. Chronic Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Heart Failure. Disclosures. Objectives: 8/28/2017. This is not a virus. It doesn t go away. none
 Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
Guideline Management of Chronic Heart Failure
 Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers") Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 4 2 3.5 4. 1. 1991 21 237 US prevalence*: 5. million US annual incidence: 7, Annual mortality: 22,754 5-1% depending on severity Cost:
Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 4 2 3.5 4. 1. 1991 21 237 US prevalence*: 5. million US annual incidence: 7, Annual mortality: 22,754 5-1% depending on severity Cost:
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
9/10/ , American Heart Association 2
 Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Contemporary Advanced Heart Failure Therapy
 Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Practical considerations for the use of ARNI in CHF: clinical cases. J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece
 Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE
 OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE GUIDELINE FOR THE MANAGEMENT OF HEART FAILURE Background: Heart failure (HF) is a complex clinical syndrome that results from
OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE GUIDELINE FOR THE MANAGEMENT OF HEART FAILURE Background: Heart failure (HF) is a complex clinical syndrome that results from
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
2/15/2017. Disclosures. Heart Failure = Big Problem. Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017
 Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Improving Long-Term Outcomes in Chronic Heart Failure
 Improving Long-Term Outcomes in Chronic Heart Failure Sponsored by Integrity Continuing Education, Inc.. Supported by an Educational grant from Novartis. 1 Faculty Affiliation and Disclosures Paul J. Hauptman,
Improving Long-Term Outcomes in Chronic Heart Failure Sponsored by Integrity Continuing Education, Inc.. Supported by an Educational grant from Novartis. 1 Faculty Affiliation and Disclosures Paul J. Hauptman,
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure. Elizabeth Pogge, PharmD, MPH, BCPS, FASCP
 Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses
 Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center
Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center
Heart.org/HFGuidelinesToolkit
 2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed
 Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed Alan S. Maisel MD FACC Professor of Medicine, University of California, San Diego, Director, CCU and Heart Failure Program San Diego
Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed Alan S. Maisel MD FACC Professor of Medicine, University of California, San Diego, Director, CCU and Heart Failure Program San Diego
Disclosure: Investigator in industry sponsored trials by Novartis
 Disclosure: Investigator in industry sponsored trials by Novartis Update in the Management of Chronic Heart Failure Family Medicine Grand Rounds November 14, 2017 Arunima Misra, MD Baylor College of Medicine
Disclosure: Investigator in industry sponsored trials by Novartis Update in the Management of Chronic Heart Failure Family Medicine Grand Rounds November 14, 2017 Arunima Misra, MD Baylor College of Medicine
Saudi Heart Failure Guidelines. Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group
 Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Cardiovascular Pharmacotherapy for Heart Failure Management
 Cardiovascular Pharmacotherapy for Heart Failure Management AN UPDATE OF THE LATEST RECOMMENDATIONS AND DATA By: Debby Caraballo, PharmD, PhC, BCPS, AQ-Cardiology Balloon Fiesta Symposium, Albuquerque,
Cardiovascular Pharmacotherapy for Heart Failure Management AN UPDATE OF THE LATEST RECOMMENDATIONS AND DATA By: Debby Caraballo, PharmD, PhC, BCPS, AQ-Cardiology Balloon Fiesta Symposium, Albuquerque,
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine
 Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Highlight Session Heart failure and cardiomyopathies Michel KOMAJDA Paris France
 Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs?
 How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs? Gregg C. Fonarow, MD FACC, FAHA, FHFSA Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA
How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs? Gregg C. Fonarow, MD FACC, FAHA, FHFSA Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA
Heart Failure Pharmacotherapy An Update
 Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than cancer
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than cancer") Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 8 6 4 2 3.5 4.8 1. 1991 21 237 US prevalence*: 5.8 million US annual incidence: 67, Annual mortality: 282,754 5-1% depending on severity
Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 8 6 4 2 3.5 4.8 1. 1991 21 237 US prevalence*: 5.8 million US annual incidence: 67, Annual mortality: 282,754 5-1% depending on severity
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much?
 2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
Pre-discussion questions
 Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Vitals HR 90 BP 125/58 Tmax 98.7F O2 Sat 97% on NC 2L/min BMP SCr 1.78 K 3.9 Gluc 194 A1c 7.5 Cardiac LVEF 55% NTproBNP 9,200 Troponin 0.
 ALDOSTERONE ANTAGONIST IN HEART FAILURE WITH PRESERVED EJECTION FRACTION ABBREVIATIONS BMP: basic metabolic panel HPI: history of present illness CAD: coronary artery disease HR: heart rate PINHUI (JUDY)
ALDOSTERONE ANTAGONIST IN HEART FAILURE WITH PRESERVED EJECTION FRACTION ABBREVIATIONS BMP: basic metabolic panel HPI: history of present illness CAD: coronary artery disease HR: heart rate PINHUI (JUDY)
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection