h Miracle on Ice Conference Minneapolis Heart Institute at Abbott Northwestern Hospital
|
|
|
- Charity Wells
- 6 years ago
- Views:
Transcription
1 Intensive Care Management from the Experts Dr. David Seder Maine Medical Center Dr William Parham ANW Intensivist Program Dr Lisa Kirkland ANW Intensivist Program Dr. Michael Mooney Program Director and Moderator Objectives Review the anticipated impact of therapeutic hypothermia on cardiac output measurements Describe the intravenous fluid infusion process for lowering body temperature Discuss use of short-acting sedation and paralytics for therapeutic hypothermia Summarize the induction, maintenance and rewarming phases of therapeutic hypothermia h





2 Neurological Resuscitation after Cardiac Arrest Managing the patient during Induction, Maintenance, and Rewarming David Seder MD Maine Medical Center Director of Neurocritical Care Disclosures No financial conflicts ALL applications described are offlabel! Grant support from MMC NSI and MRC

 17.")
 Mortality among patients surviving to be hospitalized Ontario")
3 Crit Care Med 2009;37 (Suppl):S211-S222. Epidemiology of OHCA Cardiac arrest is common 295,000 OHCA per year in US 23% VF 31% Bystander CPR Median survival all rhythms 7.9%, VF 21% Best EMS systems: ie: Seattle (resuscitated) 17.5% survival to hospital discharge 34% VT/VF subgroup IHCA adults: 19% (despite 95% witnessed or monitored) Mortality among patients surviving to be hospitalized Ontario 72% ( ) Taipei 75% (2003-4) Goteborg 68% (2003-5) Rochester 65% ( ) Circulation 2010;Jan 26:e12-13
4 Is the cup half empty? Nationally, the survival rate of OHCA is < 8% Half of patients who survive to be hospitalized die in the hospital Half of those who are discharged from the hospital have neurological disability Why bother? or half full? 40% of MMC OHCA survivors have GNO 55-60% with VT/VF & without shock have GNO A statewide program in Az of bystander CPR, CCR, and hypothermia led to a tripling of OHCA survival! These patients have a chance

:926-34")
5 Northern Hypothermia Network Acta Anaesthesiol Scand Aug;53(7): Acta Anaesthesiol Scand Aug;53(7):926-34

:926-34 Factors associated with survival Acta")
6 NHN CA outcomes 37 centers, 7 countries 986 patients received TH after CA % CPC 1-2 among asystole/pea Acta Anaesthesiol Scand Aug;53(7): Factors associated with survival Acta Anaesthesiol Scand Aug;53(7):926-34
7 From what do survivors die? Cause of Death in OHCA Cause of death in IHCA 23% 9% 68% HIE Cardiac MOSF 51% 23% 26% HIE Cardiac 3d 3rd MOSF Laver. Intensive Care Med 2004;30:2126 Mechanisms of brain injury in circulatory arrest Primary Injury: Energy failure due to ATP depletion Secondary injury: Loss of transcellular electrolyte gradients Ca h, Na +, Cl - enter, K + exits cell Water follows Na + into cells causing cytotoxic edema Lipid peroxidases damage membranes Neurotransmitter release causes excitotoxicity Activation of apoptotic pathways Microvascular thrombosis Reperfusion injury

8 Other secondary injury Uncontrolled seizure activity Hypotension, hypoperfusion Postresuscitation syndrome ICP crisis Autoregulatory failure Fever Re-arrest Hypoxia Derangements of glucose metabolism Neurology 2008;72:744 The hours after ROSC Mediators of cerebral blood flow after CA: Changes in blood viscosity Sludging of erythrocytes Development of platelet aggregates Heavy concentrations in post-ischemic tissue beds Imbalance of the coagulation system Endothelial flaps Compression by swollen glial cells Increased cerebral vascular tone and resistance Resuscitation 2003;58:337






9 Cardiac arrest associated brain injury CAABI No flow affects the most metabolically active areas of brain Cortex Basal ganglia Cerebellum Low flow affects the watershed areas between vascular territories 75 yo man OHCA Unwitnessed arrest VF on EMS arrival 35 minutes CPR and resuscitation Therapeutic hypothermia 108h after ROSC, GCS 4 CMO at family request





10 Shrunken eosinophilic neuron (anoxic neuron) is the hallmark of HIE Pseudolaminar necrosis Rationale for temperature modulation after brain injury Death Spiral Hypothermia drives fatally injured cells away from lysis and toward apoptosis Hypothermia drives marginally injured cells away from apoptosis and toward recovery Intracellular calcium mediates injury and most apoptotic pathways Crit Conn 2008;7(4):16
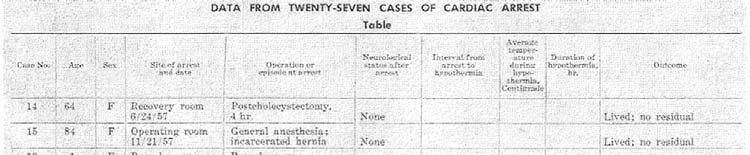
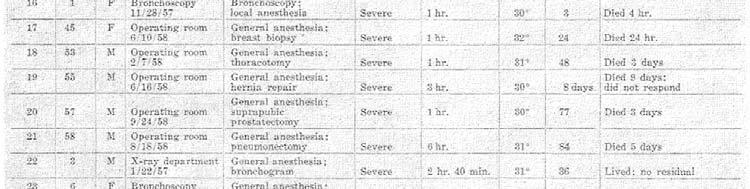

11 Anesthesia and Analgesia 1959;38 (6): 423 Anesthesia and Analgesia 1959;38 (6): 423
12 Clinical evidence for TH after CA Largest RCT of TH in OHCA survivors 275 patients randomized to TH or routine care Europe Absolute 16% increase in chance of a good neurological outcome Absolute 14% decrease in 6 month mortality N Engl J Med 2002;346: Clinical evidence for TH after CA N Engl J Med 2002;346:549-56


 Nonrandomized data Polderman.")
13 Clinical evidence for TH after CA New Engl J Med 2002; 346: Australian Randomized clinical trial conducted Randomized on alternating days to TH or routine care TH: good outcome 49%, routine care good outcome: 26% (p=0.046) Nonrandomized data Polderman. Lancet 2008, 371:

14 Lausanne 55 VT/VF OHCA treated with TH Compared to historical controls Similar DT, severity of illness CPC 1-2: 56% vs. 26% pre-th Effect of the implementation of a therapeutic hypothermia protocol on neurological outcome after out-of-hospital VF/VT arrest -Crit Care Med 2006;34:1865 Japan 400 patients with variable implementation ti of TH Developed model to isolate the interaction between use of TH and outcomes at different time points. No benefit of TH in DT < 15 minutes. Crit Care Aug 16;14(4):R155

15 What are the risks of TH? More infections Lung Trends toward more bleeding* Electrolyte shifts Clinically insignificant bradycardia Changes in drug metabolism HCASG. NEJM 2002;346: Skeptic s arguments 3300 patients screened in HACA to enroll 275 over 6 years Does not reflect real world experience Most commonly managed patients not included Many non TH patients t were allowed to develop fever Unfair comparitor? Single multicenter RCT should not set standard of care
16 TTM Trial European trial of TH (33C) vs TN (36.5C) in CA survivors Niklas Neilsen PI (INTCAR founder) Multinational trial Do we need to prove the efficacy of TH, again? What are the consequences of a poorly designed or inconclusive trial result? 2005 AHA ACLS Guidelines Unconscious adult patients with ROSC after out-of- hospital cardiac arrest should be cooled to 32 C to 34 C (89.6 F to 93.2 F) for 12 to 24 hours when the initial rhythm was VF (Class IIa). Similar therapy may be beneficial for patients with non- VF arrest out of hospital or for in-hospital arrest (Class IIb).




17 Only 10% patients with OHCA will meet RCT criteria for TH The decision to initiate TH is usually based on clinical judgement of risk and benefit, not on proof! Risks Infections Bleeding Need for sedation N Engl J Med 2002;346: Benefits Strongly neuroprotective Decreased mortality Better neurological outcome TH after Cardiac Arrest Clinical criteria for therapeutic hypothermia No more than 8 hours have elapsed since the return of spontaneous circulation. Encephalopathy is present, typically defined as the patient being unable to follow verbal commands. There is no life-threatening infection or bleeding. Aggressive care is warranted and desired by the patient or the patient s surrogate decision-maker Terminal underlying disease Impending cardiopulmonary collapse



18 The Devil s in the details How to cool Baltimore, 1955 Portland, Maine, 2006
19 Basics of Therapeutic Hypothermia There are 3 phases of treatment: Induction Rapidly bring the temperature to 32-34C Sedate with propofol or midazolam during TH Paralyze to suppress heat production Maintenance maintain the goal temperature at 33C Standard hours (optimal duration is unknown) Suppress shivering De-cooling (rewarming) Most dangerous period: hypotension, cerebral edema, seizures Goal is to reach normal body temperature over 12-24h Stop all sedation when normal body temperature is achieved Induction: how to cool Monitor core temperature Bladder, esophagus, or central venous/pulmonary arterial Cold fluid 30cc/kg LR or 0.9%NS over 30 minutes 2-2.5C temperature reduction No adverse cardiovascular results Rare to cause pulmonary edema Ice packs and cooling mats Effective, but difficult to control rate of temperature change Overcooling is dangerous
20 Induction: how to cool Commercial cooling devices Servo mechanism varies temperature re of circulating water or air (prevents overcooling) External (surface cooling) systems Hydrogel heat exchange pads Cold water circulating through plastic suit Cold water immersion awaiting safety data Invasive (catheter based) systems Heat exchange catheter in SVC or IVC Plastic or metalic heat-exchange catheter Cold IVF Polderman patients, 2-3L over C to 34.6 C, MAP increased by 15mmHg, no pulmonary edema Bernard patients 30cc/kg LR at 4 C over 30 min: 35.5 C to 33.8 C Improvements in MAP, renal function, no pulmonary edema Polderman. Crit Care Med 2005;33:2744 Bernard. Resuscitation 2003;56:9


21 Cold IVF 2-3L of Ringers or Saline at 4C decreases body temperature No effect on LVEF by echo Improved hemodynamic indices Kim. Circulation 2005;112:715
22 Induction How I do it Examine and place BIS monitor Give 30-40cc/kg IVF at 4ºC over 30 minutes LR or NS Pressure bag, not IV pump Sedate and paralyze the patient Apply a commercial cooling device Monitor and replace potassium and magnesium Antibiotics, usually Ventilate to a normal ph, and PaO2>110 Maintain i a MAP > 80 CVC, Arterial catheter, CO/CI/SVV device Comparison of cooling methods Traditional cooling inexpensive & available Effective Very high incidence overcooling Noninvasive cooling devices Safe no insertion, lots of clinical experience Effective, unless patients very heavy Expensive Invasive cooling devices Most effective at tight temperature control Better for heavy patients Insertional dangers: thrombosis, infection, placement-related injury Expensive Crit Care 2007;11:R91 INDUCTION MAINTENANCE

23 Outcomes with Surface vs Endovascular Cooling


24 Utility of the Medivance Arctic Sun for TH after Cardiac Arrest Effective at Induction 80% within 4h 90% within 6h 100% within 9h 2 pts got adjuvant cooling: ice or fluids Effective at maintenance 96.7% of the maintenance phase was spent in the target temperature range Jarrah. Neurocrit Care 2009;11:S23 90 patients with OHCA VF arrest and TH randomized mg/dl mg/dl Hypoglycemia defined as <54mg/dl Moderate hypoglycemia 18% vs 2% No mortality diff (33% 35%) mg/dl difference (33% vs
25 Measurement of Blood Glucose MMC prospectively enrolled 12 CA survivors and measured concurrent AG, VG, FBG Mean glucose values higher during TH >20% discrepancy FBG vs AG in 5% when T>36C, and 17% when T<34% FBG values uniformly higher than AG values Maintenance: How I do it Surface cooling for most patients with bladder or esophageal temperature Intravascular cooling if they need a CVC, have skin problems, or if I have extra time ceeg CO/CI and preload monitoring MAP > 80 Bispectral index when paralyzed to make sure they re out


26 Five patients who were not out 5/204 awoke during TH after CA All witnessed arrests 0-1 minute low flow minutes No flow BIS1 = BIS after first dose of NMB BIS1: 43,52,54,52,63 All were receiving propofol and/or fentanyl De-cooling Vasodilation causes hypotension May require several liters IVF, increased vasopressors More shivering Inflammation increases at higher temperature post-resuscitation syndrome Increased ICP Watch for hyperkalemia Primarily in renal failure SEIZURES


27 Patients do not like to rewarm, even if you call it decooling. Shivering Drives up systemic metabolic rate Increased CO2 production Increased O2 consumption Major cardiac stressor Drives up cerebral oxygen consumption Favors ischemia Uncomfortable Stroke Dec;39(12):

; A467 Shiverplots EMG BSAS EMG Power (db) 60 50 40 30 20 10 0 * * *")
28 BIS monitor can be used to quantify shivering p=0.001 CC EMG db from BIS monitor correlated with the validated BSAS EMG power correlates with rate of cooling May. Crit Care Med 2009;37 (12 Supp); A467 Shiverplots EMG BSAS EMG Power (db) * * * 22:55 0:13 1:31 2:49 4:07 5:25 6:43 8:01 9:19 10:37 11:55 13:13 14:31 16:30 17:48 19:06 20:24 21:42 23:00 Time * BSAS
29 Shiverplots Each additional shivering episode associated with 35% increase in odds of GNO Management of shivering Neuromuscular blockade Vecuronium bolus 0.1mg/kg prn BSAS>2 Cisatricurium in renal failure Propofol Alpha blockade Dexmedetomidine infusion or clonidine Scheduled acetaminophen, buproprion p Meperidine or fentanyl Focal counterwarming Magnesium infusion (serum level 3-4mg/dl)
30 Sedation and analgesia during therapeutic hypothermia Comfort Antiepileptic effects HCASG Midaz 0.125mg/kg/hr Fentanyl 2mcg/kg/hr Pancuronium 0.1 mg/kg q2h 70kg man/32h 280mg midazolam 4480mcg fentanyl 224 mg pancuronium That s a lot of drugs! New Engl J Med 2002;346:549 Crit Care Med 2006;34:1865 Drug metabolism during hypothermia: what do we know? Propofol concentrations 30% higher at 34ºC than 37ºC (healthy volunteers) Fentanyl concentrations 5%/ ºC (healthy swine) Pharmacotherapy 2009;28:102 Anesth Analg 1995;80:1007 Anesthesiology 1999;91:A444


31 Sedation Deep, antiepileptic sedation, or Light sedation with ceeg, or BIS-guided sedation Seizures prior to therapeutic hypothermia 19-34% incidence overall Myoclonic status epilepticus traditionally associated with 100% mortality NCSE present, less common due to absence of NMB Patients rarely received propofol or BDZ -Ann Neurol 1994; 35: Neurology 1988; 38: Intensive Care Med 2006; 32:
 seized 6/9 NCSE 7/9 generalized")
 had SE What do the seizures mean?")


32 19 children ceeg x72h during TH after CA 9 (47%) seized 6/9 NCSE 7/9 generalized 8/9 during late TH or rewarming periods 6 (32%) had SE What do the seizures mean? Are they markers for terrible and irreversible brain injury? Are they causing active, ongoing injury? Should we treat? If so, how? MSE NCSE Neurology 2008;72:744

33 ICU care following CA Many techniques for performing TH Electrolytes Glucose management Management of shivering Perfusing BP Seizure detection Antibiotics for aspiration or ALI Analgosedation Medication dosing Hospital size and CA outcome >109, patients in the NIS Mortality was lower at urban, teaching, and large hospitals Intensive Care Med 2009;35(3):505-11

:30-4 Thank You! Horstmann et al. Brain atrophy in the aftermath of cardiac arrest.")
34 CA volume vs outcomes 4674 patients from 39 hospitals Overall mortality was 56.8% Not all patients comatose After adjusting for age and severity of illness, institutional mortality ranged from 46% to 68% Annual case volume strongly associated with outcome Resuscitation Jan;80(1):30-4 Thank You! Horstmann et al. Brain atrophy in the aftermath of cardiac arrest. NEUROLOGY 2010;74:
35 1. Central Venous Pressures Managing MAP > 60 and CVP >8 CO /Index frequency Value during hypothermia? Cardiac outputs on done upon arrival to ICU; what should a protocol suggest to follow Cooling Cardiac output vs normal temp Cardiac Output? 2. Sedation vs Paralytics Shorter acting Sedation and use of Paralytics What about Versed, Precedex, Propofol? Train of 4 monitoring, D/C paralytic when temp back at 36. C vs 37.0 C Consider bolus dosing vs continuous drip
36 3. EEG Monitoring Continuous EEG monitoring (Neuro Prognostication) Practicality/Benefits Seizures 4. LINES IV Fluids and Line Placement Order of events to utilize IV fluids to cool faster Where is the best place to place lines ICU, Cath Lab or ED?
37 5. Non Phamaceutical Interventions for shivering Shivering, how do we control it? What are some Non pharmaceutical interventions we can apply? Do heated vent circuits it have impact? 6. Management of fever post cooling How should we treat the rebound fever after cooling is stopped?
38 7. Magnesium Levels Magnesium levels, importance Goal of magnesium level during TH
Curricullum Vitae. Dr. Isman Firdaus, SpJP (K), FIHA
, FIHA") Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
The Evidence Base. Stephan A. Mayer, MD. Columbia University New York, NY
 Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Hypothermia After Cardiac Arrest: Where Are We Now?
 Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Case Presentation. Cooling. Case Presentation. New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation
 New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
Hypothermia: The Science and Recommendations (In-hospital and Out)
") Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Patient Case. Post cardiac arrest pathophysiology 10/19/2017. Disclosure. Objectives. Patient Case-TM
 Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
RACE CARS: Hospital Response. David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012
 L MODULE 9 RACE CARS: Hospital Response David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012 2 Objectives: Post-cardiac arrest syndrome Therapeutic hypothermia
L MODULE 9 RACE CARS: Hospital Response David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012 2 Objectives: Post-cardiac arrest syndrome Therapeutic hypothermia
Objectives. Trends in Resuscitation POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE?
 POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
Induced Hypothermia for Cardiac Arrest. Heather Hand RN,CCRN,CNRN,ATCN,LNC
 Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest. Objectives: U.S. stats
 Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
Enhancing 5 th Chain TTM after Cardiac Arrest
 Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Mild. Moderate. Severe. 32 to to and below
 Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
Post-Resuscitation Care. Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena
 Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association
 POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association - 2016 Nicole Kupchik MN, RN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest
POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association - 2016 Nicole Kupchik MN, RN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest
New Therapeutic Hypothermia Techniques
 New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Therapeutic Hypothermia
 Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Therapeutic Hypothermia. Jonas Cooper, MD MPH
 Therapeutic Hypothermia Jonas Cooper, MD MPH Hypothermia in Cardiology Early cardiac surgery included cooling to 15 C and stopping all blood flow for one hour while surgery proceeded Belsey RH et al. Profound
Therapeutic Hypothermia Jonas Cooper, MD MPH Hypothermia in Cardiology Early cardiac surgery included cooling to 15 C and stopping all blood flow for one hour while surgery proceeded Belsey RH et al. Profound
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest
 Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Therapeutic Hypothermia: 2011 Research Update. Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine
 Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Regionalization of Post-Cardiac Arrest Care
 Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Disclosures. Pediatrician Financial: none Volunteer :
 Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Hypothermic Resuscitation 1 st Intercontinental Emergency Medicine Congress, Belek-Antalya 2014
 Hypothermic Resuscitation 1 st Intercontinental Emergency Medicine Congress, Belek-Antalya 2014 Jasmin Arrich Department of Emergency Medicine Medical University of Vienna jasmin.arrich@meduniwien.ac.at
Hypothermic Resuscitation 1 st Intercontinental Emergency Medicine Congress, Belek-Antalya 2014 Jasmin Arrich Department of Emergency Medicine Medical University of Vienna jasmin.arrich@meduniwien.ac.at
Hypothermia Post Cardiac Arrest: An Update
 Hypothermia Post Cardiac Arrest: An Update Justin Lundbye, M.D., FACC Hospital of Central Connecticut Justin.Lundbye@HHCHealth.org Outline Background Whom to Cool How to Cool Post Cardiac Arrest Care Other
Hypothermia Post Cardiac Arrest: An Update Justin Lundbye, M.D., FACC Hospital of Central Connecticut Justin.Lundbye@HHCHealth.org Outline Background Whom to Cool How to Cool Post Cardiac Arrest Care Other
Samphant Ponvilawan Bumrungrad International
 Samphant Ponvilawan Bumrungrad International Definitions Artificial circulation using VA ECMO as an alternative to ventilation and external cardiac massage Indications Out-of-Hospital Cardiac Arrest (OHCA)
Samphant Ponvilawan Bumrungrad International Definitions Artificial circulation using VA ECMO as an alternative to ventilation and external cardiac massage Indications Out-of-Hospital Cardiac Arrest (OHCA)
IN HOSPITAL CARDIAC ARREST AND SEPSIS
 IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
Management of Post Cardiac Arrest Syndrome
 Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
Therapeutic Hypothermia for Post Cardiac Arrest Plan Initial Orders
 Arrest Plan Initial Orders Weight Allergies Therapeutic Hypothermia Guidelines ***Required to continue with ordering Plan.*** Strict Intake and Output q1h, throughout cooling and re warming. Set Up for
Arrest Plan Initial Orders Weight Allergies Therapeutic Hypothermia Guidelines ***Required to continue with ordering Plan.*** Strict Intake and Output q1h, throughout cooling and re warming. Set Up for
Hypothermia Induction Methods
 Hypothermia Induction Methods Advantages and Disadvantages Xia Luo, M.D. Vice President, Clinical Education ZOLL Corporation Targeted Temperature Management (TTM) Temperature is one of the four vital signs
Hypothermia Induction Methods Advantages and Disadvantages Xia Luo, M.D. Vice President, Clinical Education ZOLL Corporation Targeted Temperature Management (TTM) Temperature is one of the four vital signs
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care
 Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Case: 65 year old post-cardiac arrest patient with myoclonus
 Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Therapeutic hypothermia following cardiac arrest
 TITLE: Therapeutic hypothermia following cardiac arrest AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
TITLE: Therapeutic hypothermia following cardiac arrest AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST
 THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST Heather Harrington RN, BScN, CNCC(c) Clinical Nurse Educator Sunnybrook Health Sciences Centre Objectives Define Therapeutic Hypothermia (TH) Describe current
THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST Heather Harrington RN, BScN, CNCC(c) Clinical Nurse Educator Sunnybrook Health Sciences Centre Objectives Define Therapeutic Hypothermia (TH) Describe current
Neuroprognostication after cardiac arrest
 Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
CARES Targeted Temperature Management (TTM) Module
 Module") CARES Targeted Temperature Management (TTM) Module OHCA Data Dictionary June 2014 1 CASE NUMBER This is the number assigned to the patient by the hospital. The case number is the number the hospital assigns
CARES Targeted Temperature Management (TTM) Module OHCA Data Dictionary June 2014 1 CASE NUMBER This is the number assigned to the patient by the hospital. The case number is the number the hospital assigns
SYSTEM-WIDE POLICY & PROCEDURE MANUAL. Policy Title: Hypothermia Post Cardiac Arrest Policy Number: PC-124. President & CEO Page 1 of 9
 Approved By: President & CEO Date Page 1 of 9 POLICY: PURPOSE: To define and describe the implementation of induced hypothermia post cardiac arrest and the nursing assessment and interventions required
Approved By: President & CEO Date Page 1 of 9 POLICY: PURPOSE: To define and describe the implementation of induced hypothermia post cardiac arrest and the nursing assessment and interventions required
Update in Therapeutic Hypothermia Post Cardiac Arrest
 Learning Objectives Update in Therapeutic Hypothermia Post Cardiac Arrest Allison Forni, PharmD, BCPS Clinical Pharmacy Specialist UMass Memorial Medical Center, Worcester MA Learning Objective 1: Describe
Learning Objectives Update in Therapeutic Hypothermia Post Cardiac Arrest Allison Forni, PharmD, BCPS Clinical Pharmacy Specialist UMass Memorial Medical Center, Worcester MA Learning Objective 1: Describe
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest
 ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Epinephrine Cardiovascular Emergencies Symposium 2018
 Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Cardio Pulmonary Cerebral Resuscitation
 Cardio Pulmonary Cerebral Resuscitation Brain Under Pressure October 3, 2017 Canadian Critical Care Forum Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto
Cardio Pulmonary Cerebral Resuscitation Brain Under Pressure October 3, 2017 Canadian Critical Care Forum Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto
Therapeutic Hypothermia after Resuscitated Cardiac Arrest
 Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Targeted Temperature Management: Normothermia for Neuroprotection
 Targeted Temperature Management: Normothermia for Neuroprotection I. Rationale Elevated body temperature is associated with increased cerebral metabolic rate and associated metabolic demand, which can
Targeted Temperature Management: Normothermia for Neuroprotection I. Rationale Elevated body temperature is associated with increased cerebral metabolic rate and associated metabolic demand, which can
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
Frank Guyette, MD, MS, MPH Jon Rittenberger, MD, MSc Cliff Callaway, MD, PhD University of Pittsburgh Department of Emergency Medicine
 Frank Guyette, MD, MS, MPH Jon Rittenberger, MD, MSc Cliff Callaway, MD, PhD University of Pittsburgh Department of Emergency Medicine Disclosures Philips Healthcare: Faculty Learning Objectives Upon completion
Frank Guyette, MD, MS, MPH Jon Rittenberger, MD, MSc Cliff Callaway, MD, PhD University of Pittsburgh Department of Emergency Medicine Disclosures Philips Healthcare: Faculty Learning Objectives Upon completion
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Targeted Temperature Management in Post Cardiac Arrest Patients
 Targeted Temperature Management in Post Cardiac Arrest Patients Treesa Joseph, PharmD PGY-1 Pharmacy Resident Atlantic Health System Continuing Education Presentation June 15 th, 2017 Objectives Explain
Targeted Temperature Management in Post Cardiac Arrest Patients Treesa Joseph, PharmD PGY-1 Pharmacy Resident Atlantic Health System Continuing Education Presentation June 15 th, 2017 Objectives Explain
Post-resuscitation care for adults. Jerry Nolan Royal United Hospital Bath
 Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
CRS Center for Resuscitation Science
 Therapeutic hypothermia after cardiac arrest and in critical care Speaker disclosures Research Funding: NIH NHLBI Philips Healthcare Doris Duke Foundation American Heart Association CRS Center for Resuscitation
Therapeutic hypothermia after cardiac arrest and in critical care Speaker disclosures Research Funding: NIH NHLBI Philips Healthcare Doris Duke Foundation American Heart Association CRS Center for Resuscitation
Ipotermia terapeutica nel bambino: manca l evidenza?
 Ipotermia terapeutica nel bambino: manca l evidenza? Andrea Moscatelli UOSD Terapia Intensiva Neonatale e Pediatrica Dipartimento Integrato di Alta Intensita` di Cura e Chirurgia Istituto Giannina Gaslini
Ipotermia terapeutica nel bambino: manca l evidenza? Andrea Moscatelli UOSD Terapia Intensiva Neonatale e Pediatrica Dipartimento Integrato di Alta Intensita` di Cura e Chirurgia Istituto Giannina Gaslini
Cardiac Arrest January 2017 CPR /3/ Day to Survival Propensity Matched
 Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE
 Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE Inclusion Criteria all must be present Cardiac arrest with return of spontaneous circulation (ROSC) ROSC within 60 mins of witnessed arrest;
Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE Inclusion Criteria all must be present Cardiac arrest with return of spontaneous circulation (ROSC) ROSC within 60 mins of witnessed arrest;
Therapeutic Hypothermia After Cardiac Arrest: Best Practices 2014
 Therapeutic Hypothermia After Cardiac Arrest: Best Practices 2014 Deborah Klein, RN, MSN, ACNS-BC, CCRN, CHFN, FAHA Clinical Nurse Specialist Coronary ICU, Heart Failure ICU, and Cardiac Short Stay/PACU/CARU
Therapeutic Hypothermia After Cardiac Arrest: Best Practices 2014 Deborah Klein, RN, MSN, ACNS-BC, CCRN, CHFN, FAHA Clinical Nurse Specialist Coronary ICU, Heart Failure ICU, and Cardiac Short Stay/PACU/CARU
Resuscitation Science : Advancing Care for the Sickest Patients
 Resuscitation Science : Advancing Care for the Sickest Patients William Hallinan University of Rochester What is resuscitation science? Simply the science of resuscitation : Pre arrest Arrest care Medical
Resuscitation Science : Advancing Care for the Sickest Patients William Hallinan University of Rochester What is resuscitation science? Simply the science of resuscitation : Pre arrest Arrest care Medical
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital
 Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
in Cardiac Arrest Management Sean Kivlehan, MD, MPH May 2014
 in Cardiac Arrest Management Sean Kivlehan, MD, MPH May 2014 1. Capnography 2. Compressions 3. CPR Devices 4. Hypothermia 5. Access 6. Medications Outline Capnography & Termination Significantly Associated
in Cardiac Arrest Management Sean Kivlehan, MD, MPH May 2014 1. Capnography 2. Compressions 3. CPR Devices 4. Hypothermia 5. Access 6. Medications Outline Capnography & Termination Significantly Associated
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto
 New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto COI Declaration Industry and ROC ALS Taskforce ILCOR Author
New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto COI Declaration Industry and ROC ALS Taskforce ILCOR Author
Disclosures. Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 ECG. Case. Case. Case Summary 4/22/2016
 Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 Nothing to disclose. Disclosures Ivan J Chavez MD Case ECG History 60 y/o male No prior history of CAD In
Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 Nothing to disclose. Disclosures Ivan J Chavez MD Case ECG History 60 y/o male No prior history of CAD In
Current status of temperature management in the neuro-icu
 Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
Cardiac Critical Care Lance Cohen, MD MBBCh FCCP
 Cardiac Critical Care 2011 Lance Cohen, MD MBBCh FCCP Open Heart Surgery Program Lance Cohen, MD MBBCh FCCP Medical Director - HSU Open Heart Surgery Program Team Cardiac Surgeons Richard Perryman, MD
Cardiac Critical Care 2011 Lance Cohen, MD MBBCh FCCP Open Heart Surgery Program Lance Cohen, MD MBBCh FCCP Medical Director - HSU Open Heart Surgery Program Team Cardiac Surgeons Richard Perryman, MD
Therapeutic Hypothermia and Pharmacologic Considerations. Genelle Butz, PharmD Director of Pharmacy CarolinaEast Medical Center August 6, 2013
 Therapeutic Hypothermia and Pharmacologic Considerations Genelle Butz, PharmD Director of Pharmacy CarolinaEast Medical Center August 6, 2013 Disclosures Disclosure tatement: I have no financial or personal
Therapeutic Hypothermia and Pharmacologic Considerations Genelle Butz, PharmD Director of Pharmacy CarolinaEast Medical Center August 6, 2013 Disclosures Disclosure tatement: I have no financial or personal
Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti
 Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti U.O.C Anestesia e Terapia Intensiva Policlinico San Martino - GENOVA Natural Course of Neurological Recovery Following Cardiac Arrest Cardiac
Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti U.O.C Anestesia e Terapia Intensiva Policlinico San Martino - GENOVA Natural Course of Neurological Recovery Following Cardiac Arrest Cardiac
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Targeted temperature management after post-anoxic brain insult: where do we stand?
 Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017
 Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
Post Cardiac Arrest Care. From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
 Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
(31189) Hypothermia Initiation Phase One
 Hypothermia Initiation Phase One") Hypothermia Initiation Phase One Diagnosis Allergies For hypothermia tracking purposes only. Please do not uncheck.- Required Cardiac Emergency Tracking For hypothermia tracking purposes only. Consults
Hypothermia Initiation Phase One Diagnosis Allergies For hypothermia tracking purposes only. Please do not uncheck.- Required Cardiac Emergency Tracking For hypothermia tracking purposes only. Consults
Lesson learnt from big trials. Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ.
 Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Therapeutic Hypothermia ANZCA 2013
 Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
12/1/2017. Disclosure. When I was invited to give a talk in Tokyo 2011 at the 4 th International. Hypothermia Symposium
 Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
3/6/2017. Endovascular Selective Cerebral Hypothermia First-in-Human Experience
 Endovascular Selective Cerebral Hypothermia First-in-Human Experience Ronald Jay Solar, Ph.D. San Diego, CA 32 nd Annual Snowmass Symposium March 5-10, 2017 Introduction Major limitations in acute ischemic
Endovascular Selective Cerebral Hypothermia First-in-Human Experience Ronald Jay Solar, Ph.D. San Diego, CA 32 nd Annual Snowmass Symposium March 5-10, 2017 Introduction Major limitations in acute ischemic
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Science Behind Resuscitation. Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013
 Science Behind Resuscitation Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013 Conflict of Interest No Financial or Industrial Conflicts Slides: Drs. Nelson, Cole and Larabee
Science Behind Resuscitation Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013 Conflict of Interest No Financial or Industrial Conflicts Slides: Drs. Nelson, Cole and Larabee
Neurotrauma: The Place for Cooling
 Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
201 0 Miracle on Ice Conference Minneapolis Heart Institute at Abbott Northwestern Hospital
 Miracle on Ice 2010 :Therapeutic Hypothermia for Cardiac Arrest Patients Sept 9 10, 2010 Allina Commons Midtown Exchange Minneapolis, Minnesota Course Directors: Barbara Tate Unger RN, BS,FAACVPR,FAHA
Miracle on Ice 2010 :Therapeutic Hypothermia for Cardiac Arrest Patients Sept 9 10, 2010 Allina Commons Midtown Exchange Minneapolis, Minnesota Course Directors: Barbara Tate Unger RN, BS,FAACVPR,FAHA
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Purpose/goal: To provide nurses with information on how they can best care for patients receiving therapeutic hypothermia.
 CNE: Temp management ANT, June 2014 Therapeutic hypothermia after cardiac arrest By Julie M. Waters RN MS CCRN Continuing Nursing Education Learning objectives 1. Describe therapeutic hypothermia (TH).
CNE: Temp management ANT, June 2014 Therapeutic hypothermia after cardiac arrest By Julie M. Waters RN MS CCRN Continuing Nursing Education Learning objectives 1. Describe therapeutic hypothermia (TH).
Module 3 Troubleshooting/Case Studies
 Module 3 Troubleshooting/Case Studies If an alarm or alert occurs, the ARCTIC SUN Temperature Management System will produce both an audible and visual cue A screen will appear that displays: alarm or
Module 3 Troubleshooting/Case Studies If an alarm or alert occurs, the ARCTIC SUN Temperature Management System will produce both an audible and visual cue A screen will appear that displays: alarm or
Identifying Best Practice for Out-of-Hospital Cardiac Arrest (OHCA) in the Hospital Setting
 in the Hospital Setting") Identifying Best Practice for Out-of-Hospital Cardiac Arrest (OHCA) in the Hospital Setting Mary Ann Peberdy, MD, FACC, FAHA C. Kenneth Wright Professor of Cardiology & Professor of Emergency Medicine
Identifying Best Practice for Out-of-Hospital Cardiac Arrest (OHCA) in the Hospital Setting Mary Ann Peberdy, MD, FACC, FAHA C. Kenneth Wright Professor of Cardiology & Professor of Emergency Medicine
State of the art lecture: 21st Century Post resuscitation management
 State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
Outcomes with ECMO for In Hospital Cardiac Arrest
 Outcomes with ECMO for In Hospital Cardiac Arrest Subhasis Chatterjee, MD, FACS, FACC, FCCP. ECMO Program Director CHI Baylor St. Lukes Medical Center/ Texas Heart Institute Asst. Professor of Surgery,
Outcomes with ECMO for In Hospital Cardiac Arrest Subhasis Chatterjee, MD, FACS, FACC, FCCP. ECMO Program Director CHI Baylor St. Lukes Medical Center/ Texas Heart Institute Asst. Professor of Surgery,
PATIENT CARE MANUAL. Guideline For Managing Shivering In Neurocritical Care Patients Undergoing Therapeutic Temperature Modulation
 PATIENT CARE MANUAL MANUAL CODE: SUBJECT: Guideline For Managing Shivering In Neurocritical Care Patients Undergoing Therapeutic Temperature Modulation DATE ISSUED: DATE REVISED: SUPERSEDES: CROSS REFERENCES:
PATIENT CARE MANUAL MANUAL CODE: SUBJECT: Guideline For Managing Shivering In Neurocritical Care Patients Undergoing Therapeutic Temperature Modulation DATE ISSUED: DATE REVISED: SUPERSEDES: CROSS REFERENCES:
Please consult package insert for more detailed safety information and instructions for use. BMD/AS50/0516/0115
 Indications for Use: The ARCTIC SUN Temperature Management System is a thermal regulating system, indicated for monitoring and controlling patient temperature in adult and pediatric patients of all ages.
Indications for Use: The ARCTIC SUN Temperature Management System is a thermal regulating system, indicated for monitoring and controlling patient temperature in adult and pediatric patients of all ages.
JUST SAY NO TO DRUGS?
 JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
Post Resuscitation Care
 Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment