Reperfusion Strategies for the STEMI Patient - PCI versus Thrombolysis
|
|
|
- Eric Sutton
- 6 years ago
- Views:
Transcription
1 Reperfusion Strategies for the STEMI Patient - PCI versus Thrombolysis Scott Mikesell, DO, FACC, FSCAI, FSVM STEMI Program Director Cardiac Catheterization Laboratory Director St. Luke s Hospital, Duluth, Minnesota

2 Disclosures Disclosures: I have no financial relationships or other conflict of interests to disclose, and I will not discuss off label use and/or investigational use in my presentation
3 Terminology STEMI = ST Elevation Myocardial Infarction PCI = Percutaneous coronary intervention PTCA = Percutaneous transluminal coronary angioplasty ACS = Acute coronary syndrome Thrombolysis = Fibrinolysis
4 Outline 1. STEMI Case 2. Epidemiology 3. Fibrinolysis 4. PCI
5 CASE

6 MZ 44 yo male with minimal past medical history presents with chest pain.
7 MZ After the diagnosis he was given 81mg aspirin x 4 600mg clopidogrel 5000 units of unfractionated heparin Morphine sulfate
8 MZ He was emergently transferred to the cardiac catheterization laboratory.

9 MZ
10 MZ
11 MZ PCI was performed with one drug eluting stent placed.
12 MZ
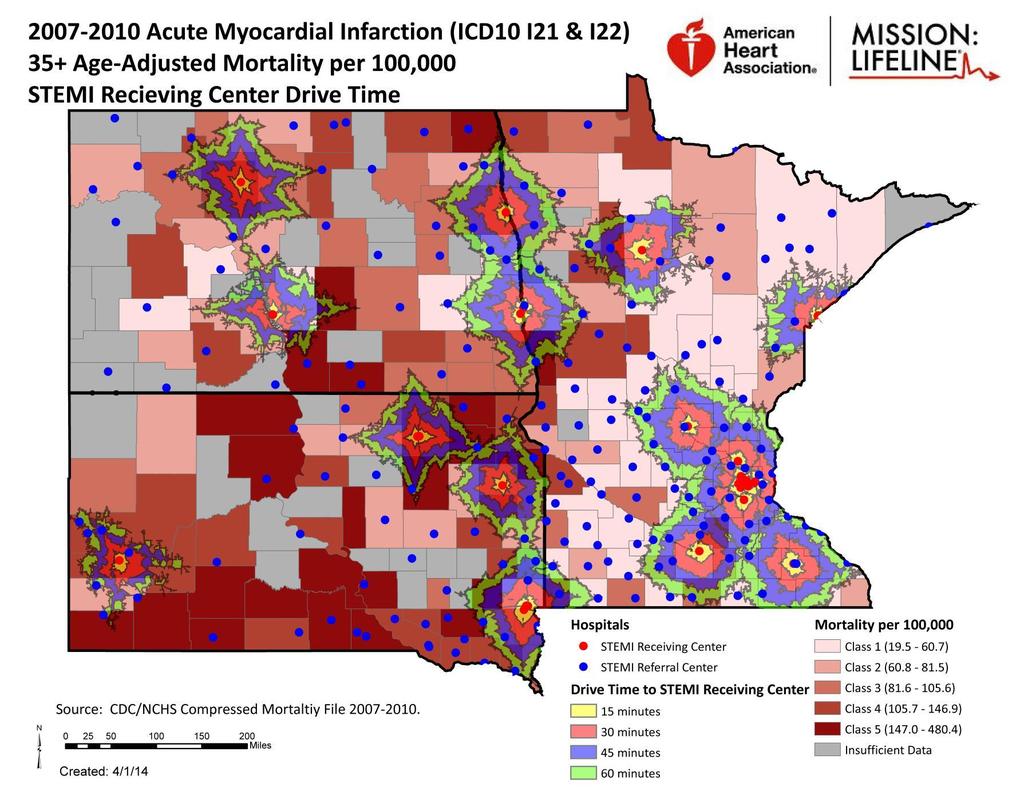
13 EPIDEMIOLOGY
14 Epidemiology 680,300 patients were discharged from US hospitals with the diagnosis of ACS. STEMI comprises 25-40% of myocardial infarctions in the US. 30% of STEMI patients are women in the US. 23% of STEMI patients have diabetes mellitus in the US.
15 STEMI PROTOCOL
16 TIME
17

18 Clinical Course
 Duration > 15 minutes < 12 hours ST Elevation as defined by diagnostic criteria on pg.")
19 The Protocol Minnesota STEMI GUIDELINE! Minnesota Mission: Lifeline Statewide STEMI Interfacility Transfer Guideline! IDENTIFY / CONFIRM STEMI Signs & Symptoms suspect for AMI (Acute Myocardial Infarction) Duration > 15 minutes < 12 hours ST Elevation as defined by diagnostic criteria on pg. 2 Pre-Hospital STEMI confirmed by 12 L ECG trained ALS EMS recognize ST segment elevation of 1 mm in 2 contiguous leads, Confirmed Interpretation of STEMI transmitted, or ECG Monitor interpretative statement infers: Acute Myocardial Infarction with pt. signs & symptoms suspect of AMI Estimated FMC to PCI 120 minutes Or FMC > 120 minutes, and one of the following: Fibrinolytic Ineligible Resuscitated out-of-hospital cardiac arrest patients whose initial ECG shows STEMI Evidence of either Cardiogenic Shock or Acute Severe CHF Top Patient Care Priorities: Establish DNR / Resuscitation Status Obtain vital signs and assess pain level on scale of 1-10 Cardiac Monitor & attach hands-free defibrillator pads Establish Saline Lock - large bore needle (left arm preferred) Oxygen PRN at 2 L/min and titrate to SpO2 > 90% Assess Allergies (Note if reaction to IV Contrast?) Notes:! **Do NOT give Lytic/TNK! All: Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Ticagrelor 180 mg PO (If Ticagrelor not available, then give Clopidogrel 600 mg PO) ACTIVATE TRANSPORT Establish availability and ETA of Air or Ground ALS EMS for Interfacility Transfer to PCI Hospital Estimate FMC (first medical contact) to Potential PCI: (Allow approx. 20 min after arrival to PCI capable hospital Estimated FMC to PCI minutes Establish if Fibrinolytic appropriate (See page 2 for contraindications) Goal: Door to Needle < 30 minutes 1. For all ages transferring not utilizing Pharmaco-invasive strategy proceed to Full Dose Fibrinolytic Strategy 2. For patients transferring to Abbott NW/MHI utilizing Pharmaco-invasive strategy, administer HALF-Dose TNK IV and transfer for PCI (Dosing table pg. 2) 3. For patients transferring to CentraCare St Cloud Consult Cardiologist prior to implementing >120 minute protocol All: Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Clopidogrel 600 mg PO TNK HALF Dose IV ACTIVATE CODE STEMI / STEMI ALERT AT PCI HOSPITAL (See Page 2 for phone #, or follow your regional STEMI protocol) TRANSPORT PATIENT AS SOON AS POSSIBLE! Fax or Transmit ECG and other pertinent records (EMS reports, allergies, past medical history, etc.) Patient Care When Time Allows: ACTIVATE YOUR INTERNAL STEMI ALERT Alert appropriate provider(s) and team members ESTABLISH KEY TIMES: Symptom Onset: First Medical Contact: ETA to PCI Hospital:! Estimated FMC to PCI >120 minutes Establish if Fibrinolytic appropriate (See page 2 for contraindications) Goal: Door to Needle < 30 minutes **For all ages transferred with an estimated FMC to PCI > 180 minutes All: Aspirin 81 mg x 4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units Heparin IV Drip 12 Units/kg/hr, max 1,000 Units/hr For AGE 75 years old: Clopidogrel 300 mg PO TNK FULL-Dose IV* For AGE > 75 years old Clopidogrel 75 mg PO TNK HALF Dose IV Establish 2 nd large bore IV with Normal ( Left arm preferred) Obtain Appropriate Labs: Troponin, CBC, Potassium, Creatinine, PT/ INR, aptt Nitroglycerin 0.4 mg SL every 5 min or Nitropaste PRN for chest pain (hold for SBP < 90) Evaluate if erectile dysfunction or pulmonary hypertension medications taken in the past 48 hours including: Sildenafil (Viagra, Revatio), Vardenafil (Levitra, Staxyn), Avanafil (Stendra), or Tadalafil (Cialis, Adcirca), and if so, hold nitrates for 48 hours! Minnesota STEMI GUIDELINE! Mission: Lifeline Statewide STEMI Interfacility Transfer Guideline!! RELATIVE CONTRAINDICATIONS FOR FIBRINOLYSIS Chest Pain / Symptom Onset > 6 hours Current use of oral anticoagulants (Warfarin, Dabigatran, Rivaroxaban, Apixaban, etc.) Uncontrolled hypertension on presentation (SBP > 180 or DBP > 90 mmhg) History of ischemic stroke more than 3 months, dementia, or known intracranial pathology not covered in contraindications Traumatic or prolonged CPR (over 10 minutes) Major surgery within last 3 weeks Recent internal bleeding (within last 2-4 weeks) Minnesota STEMI (ST Elevation Myocardial Infarction) Diagnostic Criteria: ST elevation at the J point in at least 2 contiguous leads of 2 mm (0.2 mv) in men or 1.5 mm (0.15 mv) in women in leads V2 V3 and/or of 1 mm (0.1mV) in other contiguous chest leads or the limb leads Signs & symptoms of discomfort suspect for AMI (Acute Myocardial Infarction) or STEMI with a duration > 15 minutes < 12 hours Although new, or presumably new, LBBB at presentation occurs infrequently and may interfere with ST-elevation analysis, care should be exercised in not considering this an acute myocardial infarction (MI) in isolation...if in doubt, immediate consultation with PCI receiving center is recommended ECG demonstrates evidence of ST depression suspect of a Posterior MI consult with PCI receiving center If initial ECG is not diagnostic but suspicion is high for STEMI, obtain serial 12 Lead ECG s at 5-10 minute intervals ABSOLUTE CONTRAINDICATIONS FOR FIBRINOLYSIS Chest Pain / Symptom Onset > 12 hours Suspected aortic dissection Any prior intracranial hemorrhage Structural cerebral vascular lesion or malignant intracranial neoplasm Any active bleeding (excluding menses) Ischemic stroke within 3 months Significant closed-head or facial trauma within 3 months Pregnancy Notes:!! AHA Mission: Lifeline STEMI Recommendations: FMC (First Medical Contact)-to-First ECG time < 10 minutes unless pre-hospital ECG obtained All eligible STEMI patients receiving a Reperfusion Therapy (Primary PCI or fibrinolysis) Fibrinolytic eligible STEMI patients with Door-to-Needle time < 30 minutes Primary PCI eligible patients transferred to a PCI receiving center with referring center Door in- Door out (Length of Stay) < 45 min Referring Center ED or Pre-Hospital First Medical Contact-to-PCI time < 120 minutes (including transport time) All STEMI patients without a contraindication receiving Aspirin prior to referring center ED discharge! Page 2 of 2 Final Approved Destination! CITY! Primary!PCI!Receiving! Hospital! STEMI! Activation! Phone!#:! Fax!#!for! Records:! Bemidji MN Sanford Health Coon Rapids MN Mercy Hospital Duluth MN St. Luke's Health Duluth MN Essentia St. Mary's Edina MN Fairview Southdale Fargo ND Essentia Health Fargo ND Sanford Health or Eau Claire WI Mayo Clinic Health Eau Claire WI Sacred Heart Hospital Grand Forks ND Altru Health System or La Crosse WI Gundersen Mankato MN Mayo Clinic Health Hospital EMS Minneapolis MN Abbott NW / MHI Minneapolis MN Hennepin County or or Minneapolis MN U of MN. - Fairview Robinsdale MN North Memorial Rochester MN Mayo St. Mary's St. Cloud MN CentraCare Health St. Louis Park MN Methodist St. Paul MN Regions St. Paul MN St. Joseph's Health East St. Paul MN United Hospital Sioux Falls SD Avera Heart Hospital Sioux Falls SD Avera McKennan Sioux Falls SD Sanford Health or Watertown SD Prairie Lakes Health (Other) (Other)!!
20 Initial Evaluation Minnesota STEMI GUIDELINE! IDENTIFY / CONFIRM! Minnesota Mission: STEMI Lifeline Statewide STEMI Interfacility Transfer ACTIVATE Guideline TRANSPORT Signs & Symptoms suspect for AMI (Acute Myocardial Establish availability and! Infarction) IDENTIFY Duration / CONFIRM > 15 STEMI minutes < 12 hours ACTIVATE ETA of Air TRANSPORT or Ground ALS ST Elevation Signs as & defined Symptoms by diagnostic suspect for criteria AMI (Acute on pg. Myocardial Establish EMS for availability Interfacility and 2 Infarction) Duration > 15 minutes < 12 hours ETA Transfer of Air or to Ground PCI Hospital ALS Pre-Hospital STEMI confirmed by 12 L ECG trained ALS EMS for Interfacility ST Elevation as defined by diagnostic criteria on pg. 2 EMS recognize ST segment elevation of 1 mm in 2 Transfer Estimate to PCI FMC Hospital Pre-Hospital STEMI confirmed by 12 L ECG trained ALS (first contiguous EMS leads, recognize Confirmed ST segment Interpretation elevation of of 1 mm STEMI in 2 Estimate medical FMC contact) (first to transmitted, contiguous or ECG leads, Monitor Confirmed interpretative Interpretation statement of infers: STEMI medical Potential contact) PCI: to Acute Myocardial transmitted, or Infarction ECG Monitor with interpretative pt. signs statement & symptoms infers: Potential (Allow approx. PCI: 20 min after suspect of Acute AMI Myocardial Infarction with pt. signs & symptoms (Allow approx. 20 min after suspect of AMI arrival to PCI capable hospital arrival to PCI capable hospital ACTIVATE YOUR! INTERNAL STEMI ALERT ACTIVATE Alert YOUR appropriate provider(s) INTERNAL and STEMI team members ALERT Alert appropriate provider(s) and team members ESTABLISH KEY TIMES: ESTABLISH Symptom KEY TIMES: Onset: Symptom First Onset: Medical Contact: First Medical ETA to Contact: PCI Hospital: ETA to PCI Hospital: Estimated Estimated FMC to PCI FMC to 120 PCI minutes 120 minutes Estimated FMC to to PCI minutes! Estimated Estimated FMC to FMC PCI >120 to PCI minutes >120 minutes Or FMC > Or 120 FMC minutes, > 120 minutes, and one and of one the of the Establish if if Fibrinolytic appropriate (See (See following: following: page page 2 for 2 for contraindications) Establish Establish if Fibrinolytic if Fibrinolytic appropriate appropriate (See page 2 for contraindications) Goal: Door to Needle < 30 minutes (See page 2 for contraindications) Fibrinolytic Ineligible Goal: Door to Needle 30 minutes Goal: Door to Needle < 30 minutes Fibrinolytic Resuscitated Ineligible out-of-hospital cardiac Goal: Door to Needle < 30 minutes 1. For all ages transferring not utilizing Resuscitated arrest out-of-hospital patients whose cardiac initial ECG 1. For Pharmaco-invasive all ages transferring strategy not proceed utilizing to **For all ages transferred with an arrest patients shows whose STEMI initial ECG Pharmaco-invasive Full Dose Fibrinolytic strategy Strategy proceed to estimated **For FMC all ages to PCI transferred > 180 minutes with an shows STEMI Evidence of either Cardiogenic Shock Full Dose Fibrinolytic Strategy estimated FMC to PCI > 180 minutes or Acute Severe CHF 2. For patients transferring to Abbott All: Evidence of either Cardiogenic Shock NW/MHI utilizing Pharmaco-invasive or Acute Severe CHF 2. For patients transferring to Abbott Aspirin 81 mg x 4 chewed All: **Do NOT give Lytic/TNK! strategy, administer HALF-Dose TNK IV NW/MHI utilizing Pharmaco-invasive (*Dose to achieve 324 mg) and transfer for PCI (Dosing table pg. 2) Heparin Aspirin IV Bolus mg Units/kg, x 4 chewed **Do NOT give Lytic/TNK! strategy, administer HALF-Dose TNK IV 3. For patients transferring to CentraCare max 4,000 (*Dose Units to achieve 324 mg) All: and transfer for PCI (Dosing table pg. 2) St Cloud Consult Cardiologist prior to Heparin Heparin IV Drip IV 12 Bolus Units/kg/hr, 60 Units/kg, Aspirin 81 mg x4 chewed 3. For implementing patients transferring >120 minute to protocol max 1,000 CentraCare max 4,000 Units/hr Units (*Dose to achieve 324 mg) All: St Cloud Consult Cardiologist prior to Heparin IV Drip 12 Units/kg/hr, Heparin IV Bolus 60 Units/kg, Aspirin 81 mg x4 chewed All: For AGE 75 years old: max 4,000 Units (No IV Heparin Drip) implementing >120 minute protocol max 1,000 Units/hr Aspirin 81 mg x4 chewed Clopidogrel 300 mg PO (*Dose to achieve Ticagrelor mg) PO (*Dose to achieve 324 mg) TNK FULL-Dose IV* Heparin IV (If Bolus Ticagrelor 60 Units/kg, not available, then give All: Heparin IV Bolus 60 Units/kg, For AGE 75 years old: max 4,000 Clopidogrel Units (No 600 IV mg Heparin PO) Drip) Aspirin max 4, mg Units x4 chewed (No IV Heparin Drip) For AGE Clopidogrel > 75 years old 300 mg PO Ticagrelor 180 mg PO Clopidogrel 600 mg PO Clopidogrel (*Dose to achieve 324 mg) TNK FULL-Dose 75 mg PO IV* (If Ticagrelor not available, then give TNK HALF Dose IV TNK HALF Dose IV Heparin IV Bolus 60 Units/kg, Clopidogrel 600 mg PO) max 4,000 Units (No IV Heparin Drip) For AGE > 75 years old Clopidogrel 600 mg PO Clopidogrel 75 mg PO ACTIVATE CODE STEMI / STEMI ALERT AT PCI HOSPITAL TNK HALF Dose IV TNK HALF Dose IV (See Page 2 for phone #, or follow your regional STEMI protocol)
21 Initial Evaluation!! STEMI (ST Elevation Myocardial Infarction) Diagnostic Criteria: ST elevation at the J point in at least 2 contiguous leads of 2 mm (0.2 mv) in men or 1.5 mm (0.15 mv) in women in leads V2 V3 and/or of 1 mm (0.1mV) in other contiguous chest leads or the limb leads Signs & symptoms of discomfort suspect for AMI (Acute Myocardial Infarction) or STEMI with a duration > 15 minutes < 12 hours Although new, or presumably new, LBBB at presentation occurs infrequently and may interfere with ST-elevation analysis, care should be exercised in not considering this an acute myocardial infarction (MI) in isolation...if in doubt, immediate consultation with PCI receiving center is recommended ECG demonstrates evidence of ST depression suspect of a Posterior MI consult with PCI receiving center If initial ECG is not diagnostic but suspicion is high for STEMI, obtain serial 12 Lead ECG s at 5-10 minute intervals Chest Pain / Symptom Onset > 12 hours Suspected aortic dissection Any prior intracranial hemorrhage Structural cerebral vascular lesion or malignant intracranial neoplasm Any active bleeding (excluding menses) Ischemic stroke within 3 months Significant closed-head or facial trauma within 3 months Pregnancy Destination! CITY Primary!PCI!Receiving! Hospital Activation! Records:! Chest Pain / Symptom Onset > 6 hours Current use of oral anticoagulants (Warfarin, Dabigatran, Rivaroxaban, Apixaban, etc.) Uncontrolled hypertension on presentation (SBP > 180 or DBP > 90 mmhg) Mankato MN Mayo Clinic Health
22 Fibrinolytic Ineligible Resuscitated out-of-hospital cardiac arrest patients whose initial ECG shows STEMI Evidence of either Cardiogenic Shock or Acute Severe CHF Think Backwards **Do NOT give Lytic/TNK! All: Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Ticagrelor 180 mg PO (If Ticagrelor not available, then give Clopidogrel 600 mg PO) 1. For all ages transferring not utilizing Pharmaco-invasive strategy proceed to Full Dose Fibrinolytic Strategy 2. For patients transferring to Abbott NW/MHI utilizing Pharmaco-invasive strategy, administer HALF-Dose TNK IV and transfer for PCI (Dosing table pg. 2) All: Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Clopidogrel 600 mg PO TNK HALF Dose IV! Goal: Door to Needle < 30 minutes **For all ages transferred with an estimated FMC to PCI > 180 minutes All: Aspirin 81 mg x 4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units Heparin IV Drip 12 Units/kg/hr, max 1,000 Units/hr For AGE 75 years old: Clopidogrel 300 mg PO TNK FULL-Dose IV* For AGE > 75 years old Clopidogrel 75 mg PO TNK HALF Dose IV ACTIVATE CODE STEMI / STEMI ALERT AT PCI HOSPITAL (See Page 2 for phone #, or follow your regional STEMI protocol) TRANSPORT PATIENT AS SOON AS POSSIBLE! Fax or Transmit ECG and other pertinent records (EMS reports, allergies, past medical history, etc.) Establish DNR / Resuscitation Status Obtain vital signs and assess pain level on scale of 1-10 Cardiac Monitor & attach hands-free defibrillator pads Establish Saline Lock - large bore needle (left arm preferred) Oxygen PRN at 2 L/min and titrate to SpO2 > 90% Assess Allergies (Note if reaction to IV Contrast?) Establish 2 nd large bore IV with Normal ( Left arm preferred) Obtain Appropriate Labs: Troponin, CBC, Potassium, Creatinine, PT/ INR, aptt Nitroglycerin 0.4 mg SL every 5 min or Nitropaste PRN for chest pain (hold for SBP < 90) Evaluate if erectile dysfunction or pulmonary hypertension medications taken in the past 48 hours including: Sildenafil (Viagra, Revatio), Vardenafil (Levitra, Staxyn), Avanafil (Stendra),
23 THROMBOLYSIS
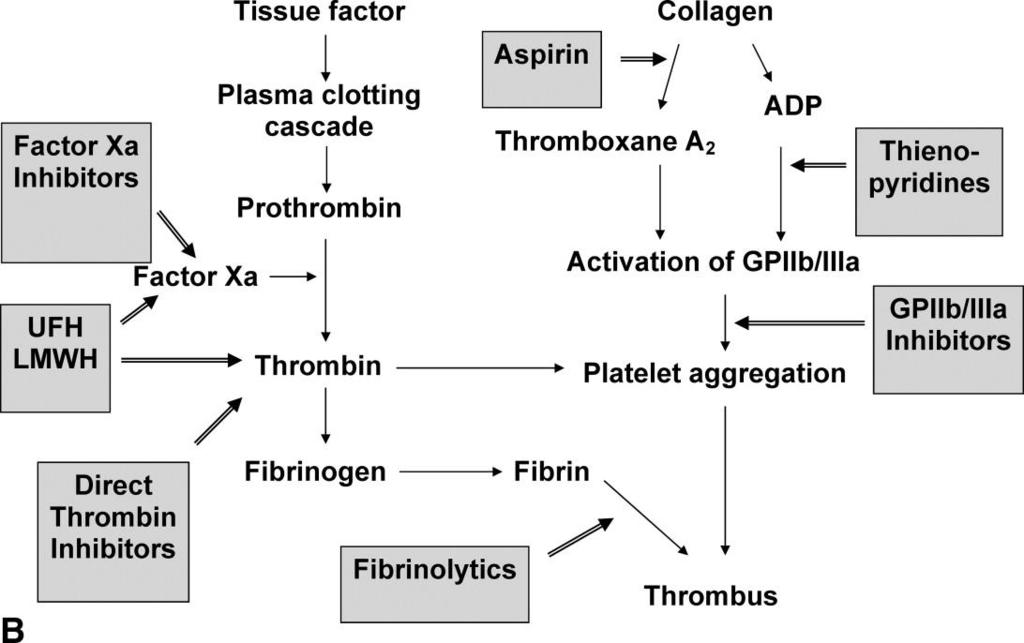
24 Coagulation Cascade
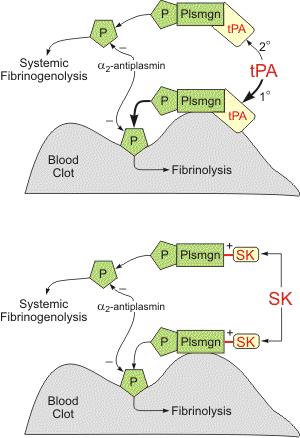
25 Fibrinolysis
26 Fibrinolysis
27 Fibrinolysis Pitfalls Arterial thrombi are rich in platelets and relatively resistant to fibrinolysis. Initial reperfusion fails in ~20% of patients. Doubled mortality rates. 5-8% of patients experience reocclusion during the index hospitalization.
28 Addition of Clopidogrel to Fibrinolysis
29 Addition of Clopidogrel to Fibrinolysis

30 Addition of Clopidogrel to Fibrinolysis
31 farction) Duration > 15 minutes < 12 hours T Elevation as defined by diagnostic criteria on pg. 2 Establish availability and ETA of Air or Ground ALS EMS for Interfacility Transfer Times >120 Minutes Symptom Onset: medical contact) to Potential PCI: (Allow approx. 20 min after FMC > 120 minutes, and one of the following: ibrinolytic Ineligible esuscitated out-of-hospital cardiac rrest patients whose initial ECG hows STEMI vidence of either Cardiogenic Shock r Acute Severe CHF **Do NOT give Lytic/TNK! spirin 81 mg x4 chewed Dose to achieve 324 mg) eparin IV Bolus 60 Units/kg, ax 4,000 Units (No IV Heparin Drip) icagrelor 180 mg PO f Ticagrelor not available, then give lopidogrel 600 mg PO) Estimated FMC to PCI minutes Establish if Fibrinolytic appropriate (See page 2 for contraindications) Goal: Door to Needle < 30 minutes 1. For all ages transferring not utilizing Pharmaco-invasive strategy proceed to Full Dose Fibrinolytic Strategy 2. For patients transferring to Abbott NW/MHI utilizing Pharmaco-invasive strategy, administer HALF-Dose TNK IV and transfer for PCI (Dosing table pg. 2) All: Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Clopidogrel 600 mg PO TNK HALF Dose IV!! Estimated FMC to PCI >120 minutes Establish if Fibrinolytic appropriate (See page 2 for contraindications) Goal: Door to Needle < 30 minutes **For all ages transferred with an estimated FMC to PCI > 180 minutes All: Aspirin 81 mg x 4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units Heparin IV Drip 12 Units/kg/hr, max 1,000 Units/hr For AGE 75 years old: Clopidogrel 300 mg PO TNK FULL-Dose IV* For AGE > 75 years old Clopidogrel 75 mg PO TNK HALF Dose IV Fax or Transmit ECG and other pertinent records
32 !! Patient Based Considerations ST elevation the J point in least 2 contiguous leads of 2 mm (0.2 mv) in men or 1.5 mm (0.15 mv) in wome and/or of 1 mm (0.1mV) in other contiguous chest leads or the limb leads Signs & symptoms of discomfort suspect for AMI (Acute Myocardial Infarction) or STEMI with a duration > 15 minute Although new, or presumably new, LBBB at presentation occurs infrequently and may interfere with ST-elevation an be exercised in not considering this an acute myocardial infarction (MI) in isolation...if in doubt, immediate consultat receiving center is recommended ECG demonstrates evidence of ST depression suspect of a Posterior MI consult with PCI receiving center ABSOLUTE CONTRAINDICATIONS FOR FIBRINOLYSIS Chest Pain / Symptom Onset > 12 hours Suspected aortic dissection Any prior intracranial hemorrhage Structural cerebral vascular lesion or malignant intracranial neoplasm Any active bleeding (excluding menses) Ischemic stroke within 3 months Significant closed-head or facial trauma within 3 months Pregnancy Destination! CITY Primary!PCI!Receiving! Hospital Activatio! RELATIVE CONTRAINDICATIONS FOR FIBRINOLYSIS Chest Pain / Symptom Onset > 6 hours Current use of oral anticoagulants (Warfarin, Dabigatran, Rivaroxaban, Apixaban, etc.) Uncontrolled hypertension on presentation (SBP > 180 or DBP > 90 mmhg) History of ischemic stroke more than 3 months, dementia, or known intracranial pathology not covered in contraindications Traumatic or prolonged CPR (over 10 minutes) Major surgery within last 3 weeks Recent internal bleeding (within last 2-4 weeks) Mankato MN Mayo Clinic Health EMS Minneapolis MN Abbott NW / MHI Minneapolis MN Hennepin County Minneapolis MN U of MN. - Fairview Robinsdale MN North Memorial Rochester MN Mayo St. Mary's St. Cloud MN CentraCare Health St. Louis Park MN Methodist St. Paul MN Regions St. Paul MN St. Joseph's Health East St. Paul MN United Hospital Sioux Falls SD Avera Heart Hospital Sioux Falls SD Avera McKennan
33
34
35
36
37
38 PCI
39 ! PCI Arm (<120 minutes transfer time) Infarction) Duration > 15 minutes < 12 hours ST Elevation as defined by diagnostic criteria on pg. 2 Establish availability and ETA of Air or Ground ALS EMS for Interfacility medical contact) to Potential PCI: (Allow approx. 20 min after Estimated FMC to PCI 120 minutes Estimated F Or FMC > 120 minutes, and one of the following: Fibrinolytic Ineligible Resuscitated out-of-hospital cardiac arrest patients whose initial ECG shows STEMI Evidence of either Cardiogenic Shock or Acute Severe CHF **Do NOT give Lytic/TNK! All: Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Ticagrelor 180 mg PO (If Ticagrelor not available, then give Clopidogrel 600 mg PO) Establish if Fibrinolytic appropriate (See page 2 for contraindications) Goal: Door to Needle < 30 minutes 1. For all ages transferring not utilizing Pharmaco-invasive strategy proceed to Full Dose Fibrinolytic Strategy 2. For patients transferring to Abbott NW/MHI utilizing Pharmaco-invasive strategy, administer HALF-Dose TNK IV and transfer for PCI (Dosing table pg. 2) ents transferring to CentraCare St Cloud Consult Cardiologist prior to implementing >120 minute protocol All: Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Clopidogrel 600 mg PO TNK HALF Dose IV Establis (See pa Goal: D **For all age estimated F All: Aspirin (*Dose Heparin max 4,0 Heparin max 1,0 For AGE Clopido TNK F For AGE > Clopido TNK H Fax or Transmit ECG and other pertinent records
40
41
42 ANCILLARY CONSIDERATIONS
43 Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Ticagrelor 180 mg PO (If Ticagrelor not available, then give Clopidogrel 600 mg PO) All: Aspirin 81 mg x4 chewed (*Dose to achieve 324 mg) Heparin IV Bolus 60 Units/kg, max 4,000 Units (No IV Heparin Drip) Clopidogrel 600 mg PO TNK HALF Dose IV Other Priorities! Heparin IV Drip 12 Units/kg/hr, max 1,000 Units/hr For AGE 75 years old: Clopidogrel 300 mg PO TNK FULL-Dose IV* For AGE > 75 years old Clopidogrel 75 mg PO TNK HALF Dose IV Fax or Transmit ECG and other pertinent records Top Patient Care Priorities: Establish DNR / Resuscitation Status Obtain vital signs and assess pain level on scale of 1-10 Cardiac Monitor & attach hands-free defibrillator pads Establish Saline Lock - large bore needle (left arm preferred) Oxygen PRN at 2 L/min and titrate to SpO2 > 90% Assess Allergies (Note if reaction to IV Contrast?) Notes:! Patient Care When Time Allows: Establish 2 nd large bore IV with Normal ( Left arm preferred) Obtain Appropriate Labs: Troponin, CBC, Potassium, Creatinine, PT/ INR, aptt Nitroglycerin 0.4 mg SL every 5 min or Nitropaste PRN for chest pain (hold for SBP < 90) Evaluate if erectile dysfunction or pulmonary hypertension medications taken in the past 48 hours including: Sildenafil (Viagra, Revatio), Vardenafil (Levitra, Staxyn), Avanafil (Stendra), or Tadalafil (Cialis, Adcirca), and if so, hold nitrates for 48 hours
44 or Minneapolis MN U of MN. - Fairview Robinsdale MN North Memorial Rochester MN Mayo St. Mary's St. Cloud MN CentraCare Health STEMI Recommendations St. Louis Park MN Methodist St. Paul MN Regions St. Paul MN St. Joseph's Health East St. Paul MN United Hospital Sioux Falls SD Avera Heart Hospital Sioux Falls SD Avera McKennan Sioux Falls SD Sanford Health or Watertown SD Prairie Lakes Health (Other) (Other)!! AHA Mission: Lifeline STEMI Recommendations: FMC (First Medical Contact)-to-First ECG time < 10 minutes unless pre-hospital ECG obtained All eligible STEMI patients receiving a Reperfusion Therapy (Primary PCI or fibrinolysis) Fibrinolytic eligible STEMI patients with Door-to-Needle time < 30 minutes Primary PCI eligible patients transferred to a PCI receiving center with referring center Door in- Door out (Length of Stay) < 45 min Referring Center ED or Pre-Hospital First Medical Contact-to-PCI time < 120 minutes (including transport time) All STEMI patients without a contraindication receiving Aspirin prior to referring center ED discharge
45 THANK YOU
ST Elevation Myocardial Infarction (STEMI) Reperfusion Order Set
 Reperfusion Order Set") Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
ST Elevated Myocardial Infarction- Latest AHA recommendations
 ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
* * FORM REV. 02/2019 Page 1 of 4. TNKASE (tenecteplase) / ACUTE STEMI ORDERS SCHEDULED MEDICATIONS:
 / ACUTE STEMI ORDERS SCHEDULED MEDICATIONS:") 1. Is this a CMS inpatient only procedure? Yes, admit as inpatient, proceed to # 3 No, proceed to # 2 2. Do you expect that the patient s condition will require a hospital stay that will cross two midnights
1. Is this a CMS inpatient only procedure? Yes, admit as inpatient, proceed to # 3 No, proceed to # 2 2. Do you expect that the patient s condition will require a hospital stay that will cross two midnights
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Blod clot: Hospital acquired potentially preventable venous thromboembolism
 Quality Measures Blod clot: Warfarin therapy discharge instructions Blod clot: Hospital acquired potentially preventable venous thromboembolism Thrombolytic Therapy Blod clot: Warfarin therapy discharge
Quality Measures Blod clot: Warfarin therapy discharge instructions Blod clot: Hospital acquired potentially preventable venous thromboembolism Thrombolytic Therapy Blod clot: Warfarin therapy discharge
Objectives. Treatment of ACS. Early Invasive Strategy. UA/NSTEMI General Concepts. UA/NSTEMI Initial Therapy/Antithrombotic
 Objectives Treatment of ACS Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Define early invasive strategy and what patients typically receive this approach Compare/contrast the medications
Objectives Treatment of ACS Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Define early invasive strategy and what patients typically receive this approach Compare/contrast the medications
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki. 2013, American Heart Association
 NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
STEMI, Non-STEMI, Chest Pain?
 Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
STEMI in the State of Jefferson ASSET - 5 Years Later. Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center
 STEMI in the State of Jefferson ASSET - 5 Years Later Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center Sept 22, 2008 Percent # Procedures Performed Coronary
STEMI in the State of Jefferson ASSET - 5 Years Later Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center Sept 22, 2008 Percent # Procedures Performed Coronary
Acute Coronary Syndrome including STEMI
 Portage County EMS Patient Care Guidelines Acute Coronary Syndrome including STEMI Note: The goal is to deliver a STEMI patient to a cardiac center within 60 minutes of first ALS patient contact. Cardiac
Portage County EMS Patient Care Guidelines Acute Coronary Syndrome including STEMI Note: The goal is to deliver a STEMI patient to a cardiac center within 60 minutes of first ALS patient contact. Cardiac
GWTG-CAD: Mission: Lifeline Focus July 2017 PMT FORM SELECTION. Pre-Hospital/Arrival
 GWTG-CAD: Mission: Lifeline Focus July 2017 PMT FORM SELECTION Page 1 Legend: BOLD = Required ^ = MLL Data Element Admin (Tab) ^Patient ID: Physician/Provider NPI: DOB: / / ^Arrival Date/Time: Race: Hispanic
GWTG-CAD: Mission: Lifeline Focus July 2017 PMT FORM SELECTION Page 1 Legend: BOLD = Required ^ = MLL Data Element Admin (Tab) ^Patient ID: Physician/Provider NPI: DOB: / / ^Arrival Date/Time: Race: Hispanic
When the learner has completed this module, she/he will be able to:
 Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Treatment of Acute Coronary Syndromes
 Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Optimal System Specification by Point of Care Operations Manual
 Optimal System Specification by Point of Care Operations Manual The Steering Committee of the Reperfusion of Acute Myocardial Infarction in Carolina Emergency Departments (RACE) Project Version 2.1 April
Optimal System Specification by Point of Care Operations Manual The Steering Committee of the Reperfusion of Acute Myocardial Infarction in Carolina Emergency Departments (RACE) Project Version 2.1 April
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Acute Coronary Syndrome (ACS) Initial Evaluation and Management
 Initial Evaluation and Management") Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences
 Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences Dr. Henry H. Ting, Mayo Clinic College of Medicine Dr. James G. Jollis,, Duke University Medical Center Mayo Clinic STEMI System for Transferred
Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences Dr. Henry H. Ting, Mayo Clinic College of Medicine Dr. James G. Jollis,, Duke University Medical Center Mayo Clinic STEMI System for Transferred
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
EMT. Chapter 14 Review
 EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 Available at ALL facilities Non Categorized SUB ED Chest Pain: STEMI Protocol(SUB)* SUB ED Chest Pain: STEMI Protocol Lab Orders(SUB)* ED Rainbow Tubes(SUB)* ***Reminder: Order ED Rainbow Tubes (SUB) as
Available at ALL facilities Non Categorized SUB ED Chest Pain: STEMI Protocol(SUB)* SUB ED Chest Pain: STEMI Protocol Lab Orders(SUB)* ED Rainbow Tubes(SUB)* ***Reminder: Order ED Rainbow Tubes (SUB) as
Acute myocardial infarction (AMI) and unstable angina
 and unstable angina") Part 8: Stabilization of the Patient With Acute Coronary Syndromes Acute myocardial infarction (AMI) and unstable angina (UA) are part of a spectrum of clinical disease collectively identified as acute
Part 8: Stabilization of the Patient With Acute Coronary Syndromes Acute myocardial infarction (AMI) and unstable angina (UA) are part of a spectrum of clinical disease collectively identified as acute
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Pre Hospital and Initial Management of Acute Coronary Syndrome
 Pre Hospital and Initial Management of Acute Coronary Syndrome Dr. Muhammad Fadil, SpJP 3rd SymCARD 2013 Classification of ACS ESC Guidelines for the management of Acute Coronary Syndrome in patients without
Pre Hospital and Initial Management of Acute Coronary Syndrome Dr. Muhammad Fadil, SpJP 3rd SymCARD 2013 Classification of ACS ESC Guidelines for the management of Acute Coronary Syndrome in patients without
Goals: Widen Your Understanding of the Wide QRS!
 Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Sanford Chest Pain Network: Improving Rural STEMI Outcomes
 Sanford Chest Pain Network: Improving Rural STEMI Outcomes Naveen Rajpurohit, MD Cardiovascular Fellow Sanford Cardiovascular Institute Sanford Heart Hospital The University of South Dakota Sioux Falls,
Sanford Chest Pain Network: Improving Rural STEMI Outcomes Naveen Rajpurohit, MD Cardiovascular Fellow Sanford Cardiovascular Institute Sanford Heart Hospital The University of South Dakota Sioux Falls,
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
9/24/2013. Thrombolytics in 2013: Never Say Never. September 19 th, 2013 Scott M Lilly, MD PhD. Clinical Case
 September 19 th, 2013 Scott M Lilly, MD PhD Thrombolytics in 2013: Never Say Never Clinical Case 2 1 Evolution of STEMI Therapy The importance of absolute rest in bed for several days is clear James B
September 19 th, 2013 Scott M Lilly, MD PhD Thrombolytics in 2013: Never Say Never Clinical Case 2 1 Evolution of STEMI Therapy The importance of absolute rest in bed for several days is clear James B
Emergency Department Chest Pain, Suspected Cardiac Adult Order Set
 Form Title Form Number Chest Pain, Suspected Cardiac Adult Order Set 20746 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0
Form Title Form Number Chest Pain, Suspected Cardiac Adult Order Set 20746 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Know the Quality of our Care at Every Step. Kansas City ACS Summit BI-State Cardiovascular Education Consortium
 Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Presenters: Disclaimer. Definitions. Deanna Jones, RN, CCRN. Annmarie Keck, RN, CEN
 Presenters: Deanna Jones, RN, CCRN Cardiac Level 1 Coordinator, Providence Sacred Heart Medical Center and Children s Hospital, Spokane, WA Annmarie Keck, RN, CEN Clinical Outreach Educator Northwest MedStar,
Presenters: Deanna Jones, RN, CCRN Cardiac Level 1 Coordinator, Providence Sacred Heart Medical Center and Children s Hospital, Spokane, WA Annmarie Keck, RN, CEN Clinical Outreach Educator Northwest MedStar,
Name Authentication Date (Position or Committee) Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee
 Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee") Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Improving the Outcomes of
 Improving the Outcomes of STEMI Shelley Valaire, ACP; and Robert Welsh, MD, FRCPC Presented at the University of Alberta s 6th Annual Cardiology Update for General Practitioners and Internists, Edmonton,
Improving the Outcomes of STEMI Shelley Valaire, ACP; and Robert Welsh, MD, FRCPC Presented at the University of Alberta s 6th Annual Cardiology Update for General Practitioners and Internists, Edmonton,
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Thrombolysis in Acute Myocardial Infarction
 CHAPTER 70 Thrombolysis in Acute Myocardial Infarction J. S. Hiremath Introduction Reperfusion of the occluded coronary artery at the earliest is the most important aim of management of STEMI. Once a flow
CHAPTER 70 Thrombolysis in Acute Myocardial Infarction J. S. Hiremath Introduction Reperfusion of the occluded coronary artery at the earliest is the most important aim of management of STEMI. Once a flow
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
EMS Recognition Webinar August 24, 2017
 EMS Recognition Webinar August 24, 2017 Today s objectives: Provide you with some rationale regarding the importance of reducing FMC to device time Provide you with an overview of the 2017 Mission: Lifeline
EMS Recognition Webinar August 24, 2017 Today s objectives: Provide you with some rationale regarding the importance of reducing FMC to device time Provide you with an overview of the 2017 Mission: Lifeline
4. Which survey program does your facility use to get your program designated by the state?
 STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11
 Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11") May 2011 1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11 Yes b) If confirmed please provide details on the number of
May 2011 1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11 Yes b) If confirmed please provide details on the number of
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
 A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
EMS & Systems of Care The State of Jefferson experience with STEMI, Stroke & more
 EMS & Systems of Care The State of Jefferson experience with STEMI, Stroke & more Paul S. Rostykus, MD, MPH Jackson County EMS Supervising Physician Ashland Community Hospital ED drrostykus@jcems.net 45
EMS & Systems of Care The State of Jefferson experience with STEMI, Stroke & more Paul S. Rostykus, MD, MPH Jackson County EMS Supervising Physician Ashland Community Hospital ED drrostykus@jcems.net 45
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
Transfer in D2B. Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland. The Problem
 Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Diagnosis and Management of Acute Myocardial Infarction
 Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
How to give thrombolysis in acute myocardial infarction
 Page 1 of 6 How to give thrombolysis in acute myocardial infarction Original article: Michael Tam In the major urban hospitals, there will be little place for thrombolysis in acute STEMI (STelevation myocardial
Page 1 of 6 How to give thrombolysis in acute myocardial infarction Original article: Michael Tam In the major urban hospitals, there will be little place for thrombolysis in acute STEMI (STelevation myocardial
Mission: Lifeline EMS Recognition : FMC to Device < 90 Minutes Worksheet
 Mission: Lifeline EMS Recognition : FMC to Device < 90 Minutes Worksheet Did Pt. Receive PCI FMC to PCI < 90 Minutes Exclusions Documented Delay after hospital arrival (Refer to Page 4 in EMS Recognition
Mission: Lifeline EMS Recognition : FMC to Device < 90 Minutes Worksheet Did Pt. Receive PCI FMC to PCI < 90 Minutes Exclusions Documented Delay after hospital arrival (Refer to Page 4 in EMS Recognition
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION. STREAM 1Y AHA 2013 P Sinnaeve
 STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
Critical Review Form Therapy Objectives: Methods:
 Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
The Burden & Management of Ischaemic Heart Disease in Kenya
 The Burden & Management of Ischaemic Heart Disease in Kenya Dr Harun A Otieno FACC Tuesday, October 6th: Session X PASCAR & CSM Joint Congress 2015, Mauritius Disclosures With regards to this presentation,
The Burden & Management of Ischaemic Heart Disease in Kenya Dr Harun A Otieno FACC Tuesday, October 6th: Session X PASCAR & CSM Joint Congress 2015, Mauritius Disclosures With regards to this presentation,
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
AIMS: CHEST PAIN. Causes of chest pain. Causes of chest pain: Cardiac causes: Acute coronary syndromes pericarditis thoracic aortic dissection
 CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
Rural Minnesota STEMI Systems of Care
 CARDIOVASCULAR HEALTH UNIT Rural Minnesota STEMI Systems of Care Almost 250,000 Americans experience ST-elevation Myocardial Infarction (STEMI), the deadliest form of heart attack, each year. Of approximately
CARDIOVASCULAR HEALTH UNIT Rural Minnesota STEMI Systems of Care Almost 250,000 Americans experience ST-elevation Myocardial Infarction (STEMI), the deadliest form of heart attack, each year. Of approximately
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology
 Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
STEMI ST Elevation Myocardial Infarction
 STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies
 Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Acute Coronary Syndrome (2019) ANEK KANOKSILP Central Chest Institute of Thailand
 ANEK KANOKSILP Central Chest Institute of Thailand") Acute Coronary Syndrome (2019) ANEK KANOKSILP Central Chest Institute of Thailand โรคหลอดเล อดแดงแข ง (Atherosclerosis) ป จจ ยเส 4 ยงท 4ทา ให เก ดโรคหลอดเล อดแดงแข ง (Atherosclerosis) ปร บเปล ( ยนได เบาหวาน
Acute Coronary Syndrome (2019) ANEK KANOKSILP Central Chest Institute of Thailand โรคหลอดเล อดแดงแข ง (Atherosclerosis) ป จจ ยเส 4 ยงท 4ทา ให เก ดโรคหลอดเล อดแดงแข ง (Atherosclerosis) ปร บเปล ( ยนได เบาหวาน
Therapies for ACS The Articles You ve Got to Know!!
 Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Management of STEMI in era of Reperfusion. Eagles Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police
 Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Time Sensitive Disease. Parinya Tianwibool, M.D., FTCEP Department of Emergency medicine,chiangmai university
 Time Sensitive Disease Parinya Tianwibool, M.D., FTCEP Department of Emergency medicine,chiangmai university Stroke Cardiac arrest STEMI Septic shock On the scene Cincinnati Prehospital Stroke Scale
Time Sensitive Disease Parinya Tianwibool, M.D., FTCEP Department of Emergency medicine,chiangmai university Stroke Cardiac arrest STEMI Septic shock On the scene Cincinnati Prehospital Stroke Scale
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD
 Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD Should PCI center activate the cathlab off EMS field interpretation of ECG? Is this happening consistently in New Mexico? What is acceptable rate
Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD Should PCI center activate the cathlab off EMS field interpretation of ECG? Is this happening consistently in New Mexico? What is acceptable rate
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI?
 SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
Thrombolysis, adjunctive pharmacology and interventions
 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation ESC Annual Congress Munich, 2012 Thrombolysis, adjunctive pharmacology and interventions
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation ESC Annual Congress Munich, 2012 Thrombolysis, adjunctive pharmacology and interventions
STEMI Presentation and Case Discussion. Case #1
 STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
Antithrombotic Therapy in ACS Pretreatment in STEMI. Christian W. Hamm Kerckhoff Heart & Thorax Center Bad Nauheim Germany
 Antithrombotic Therapy in ACS Pretreatment in STEMI Christian W. Hamm Kerckhoff Heart & Thorax Center Bad Nauheim Germany Potential conflicts of interest Speaker s name: Christian W. Hamm I have the following
Antithrombotic Therapy in ACS Pretreatment in STEMI Christian W. Hamm Kerckhoff Heart & Thorax Center Bad Nauheim Germany Potential conflicts of interest Speaker s name: Christian W. Hamm I have the following
Dashboard and Outcomes Report with Case Studies
 Dashboard and Outcomes Report with Case Studies Kim Hustler Clinical Quality Consultant, American College of Cardiology The following relationships exist: Kim Hustler: No Disclosures Section F- Procedures
Dashboard and Outcomes Report with Case Studies Kim Hustler Clinical Quality Consultant, American College of Cardiology The following relationships exist: Kim Hustler: No Disclosures Section F- Procedures