MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017
|
|
|
- Arron Potter
- 6 years ago
- Views:
Transcription


1 MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9,
2 Faculty Disclosure Faculty: Peter Leong-Sit MSc, MD, FRCPC, FHRS Associate Professor, Western University Cardiologist, London Heart Rhythm Program Relationships with commercial interests: Grants/Research Support: Bayer Consultant: St. Jude Medical, Medtronic, Johnson & Johnson Speaker s Bureau: Medtronic, Johnson & Johnson, St. Jude Medical, Bayer, Boehringer Ingelheim, Pfizer, Boston Scientific Potential for conflict(s) of interest: Bayer, St. Jude Medical, Medtronic, Johnson & Johnson, Boehringer Ingelheim, Pfizer, Boston Scientific develop and benefit from the sale of products that might be discussed in this program. 2
3 Mitigating Potential Bias All the recommendations involving clinical medicine are based on evidence that is accepted within the profession. All scientific research referred to, reported, or used is in the support or justification of patient care. Recommendations conform to the generally accepted standards. The presentation will mitigate potential bias by ensuring that data and recommendations are presented in a fair and balanced way. Potential bias will be mitigated by presenting a full range of products that can be used in this therapeutic area. 3
4 Learning Objectives 1. To review management strategies for atrial fibrillation 2. To identify good candidates for rhythm control or ablation for atrial fibrillation 3. To provide an overview of atrial fibrillation ablation principles 4. To provide an overview of invasive options for stroke prevention 4
5 Case #1: 66F with prior MI, otherwise healthy Cath: preserved LVEF, non-surgical coronary disease No further CP since MI 3 years ago Frequent daily palpitations Meds: ASA, ramipril 5mg, bisoprolol 5mg, atorvastatin 40mg 5
6 Is this Atrial Fibrillation? a) Yes b) No 6
7 Holter: Is this Atrial Fibrillation? a) Yes b) No 7
8 Is this Atrial Fibrillation? a) Yes b) No 8
9 Is this Atrial Fibrillation? a) Yes b) No 9
10 24-Hour Holter Monitor Predominant rhythm sinus Salvos of AF lasting 15 seconds to 45 minutes correlating with mild palpitations No conduction disease, AV block Mean rate = 80bpm [50-130bpm] Rates in AF = bpm 10
11 Outpatient AF Management AF Management Precipitating cause Stroke Symptoms ASA Warfarin Dabigatran Rivaroxaban Apixaban (LAA Occlusion) Rate Control vs Rhythm Control Medical vs Ablation 11
12 Back to our Case... 66F with paroxysmal AF Prior MI, preserved LVEF, no CHF Otherwise healthy Would you recommend: a) Nothing b) ASA c) Warfarin d) NOAC 12
13 CHADS 2 Score Combination of AFI and SPAF schemes 1 Congestive Heart Failure 1 Hypertension 1 Age > 75 years 1 Diabetes Mellitus 2 Stroke or TIA Score* Stroke rate ( ) ( ) ( ) ( ) ( ) ( ) ( ) *Score 0: Patients can be administered aspirin *Score 1: Patients can be on aspirin or systemic anticoagulation *Score 2: Patients should be on systemic anticoagulation Gage BF, et al. JAMA. 2001;285:
 Score 2/9 = 1.6% (0.3 4.7%) Lip GY et al. Chest. 2010 Feb;137(2):263-72.")
14 CHA 2 DS 2 VASc Score Score 0/9 = 0 thromboembolic events Score 1/9 = 0.6% ( %) Score 2/9 = 1.6% ( %) Lip GY et al. Chest Feb;137(2):
15 Back to our Case... 66F with newly diagnosed AF No hypertension, diabetes, no prior CHF or stroke but prior MI Hence, CHADS 2 score = 0 But CHA 2 DS 2 -VASc score = 3! 15

16 2016 AF Guidelines CHADS-65 Macle L. et al. Can J Cardiol 2016;32:
17 Back to our Case... 66F with newly diagnosed AF No hypertension, diabetes, no prior CHF or stroke but prior MI Hence, CHADS 2 score = 0 But CHA 2 DS 2 -VASc score = 3! Current Canadian guidelines: Over age 65, therefore anticoagulate 17
18 Summary of Approach Any patient above age 65 with AF should have systemic anticoagulation Below age 65 with CHADS2 risk factors should have systemic anticoagulation Below age 65 with vascular disease, ASA is recommended Below age 65 with no vascular disease, nothing is recommended 18
19 Which to Choose? Is warfarin ok for my patient? Mechanical valve. definitely warfarin Excellent INRs (TTR > 70%) may limit benefits of switching Renal Function / Liver Metabolism Poor renal function (GFR < 30-50) Apixaban, rivaroxaban > dabigatran GFR < definitely warfarin Compliance of Once daily vs Twice daily No monitoring of compliance 19
20 2014/2016 Canadian AF Guidelines Emphasis is on choosing the new agents over warfarin rather than choosing between the new agents Warfarin based on RCT data < 6600 pts New agents tested in > 70,000 pts Verma et al. Can J Cardiol 2014;30: Macle et al. Can J Cardiol 2016;32:
21 Limited Use Coverage Clinical Criteria 1) Failed warfarin trial > 2 months > 35% INRs outside therapeutic range 2) Warfarin contraindicated or inability to monitor INRs 21
22 Limited Use Codes Dabigatran = 431 Rivaroxaban = 435 Apixaban = 448 Edoxaban =?coming soon 22
23 WHAT ABOUT BLEEDING RISK?
24 Patient Preferences Lahaye S et al. Thromb Haemost Dec 12;111(4) 24
25 Mortality rate (%) Mortality after major bleed: 5 Phase III trials Warfarin Dabigatran Time (days) The Kaplan Meier analysis indicated a reduced risk for death with dabigatran* vs warfarin during 30 days from the bleeding (P=0.052) Majeed A. et al. Management and Outcomes of Major Bleeding on Dabigatran or Warfarin, American Society of Hematology Conference, Atlanta, GA, Dec





26 Remember: There is Harm in Inaction Single antiplatelet agent Dual antiplatelet therapy 25% 3% 15% No antithrombotics Warfarin subtherapeutic 39% 18% Warfarin therapeutic 82% of AF patients with a 2 nd stroke were not anticoagulated Gladstone DJ, et al. Stroke 2009;40:
27 Case #2: 82F with persistent AF Problem List: Hypertension, Diabetes, Dylipidemia Post-partum DVT with a PE L. breast Ca with mastectomy 2010 CHADS = 3, CHADS-VASc score = 4 On warfarin, suffered large GI bleed 27
28 What is the next step? a) Continue warfarin b) Stop warfarin, start ASA c) Stop warfarin, start NOAC d) Stop warfarin, refer for LA appendage closure 28
29 Case #2 Endoscopy: reactive gastropathy and vascular ectasias Switched to Rivaroxaban 20mg daily, recurrent GI bleed Switched to Apixaban 2.5mg bid, recurrent GI bleed 29



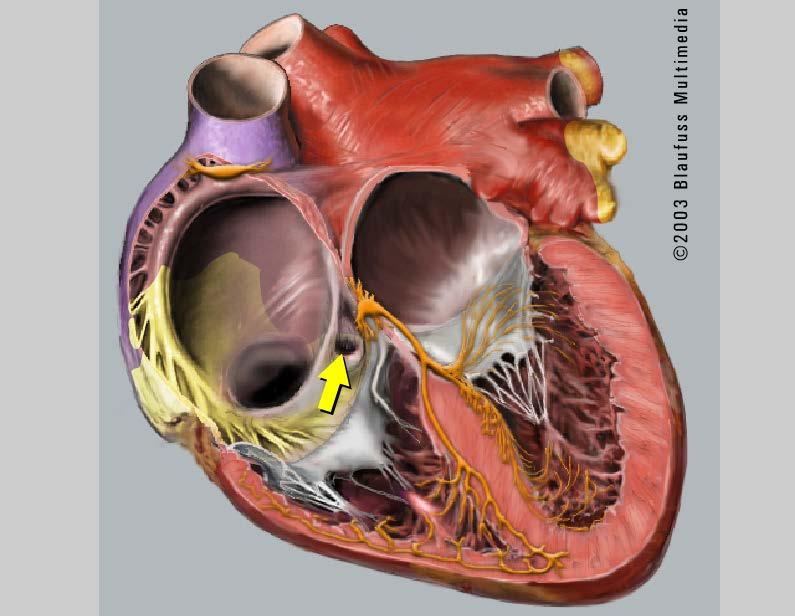
30 Mechanism of Stroke in AF Slow-moving blood that pools can form clot in the LAA, which can embolize and result in Stroke 30

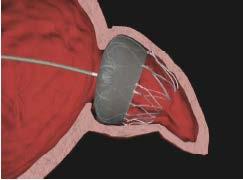

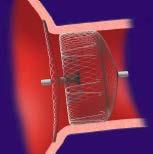
31 Approved Percutaneous Options Amplatzer Cardiac Plug (SJM) Watchman device (BSx) 31


32 The Watchman Left Atrial Appendage Closure Device Maisel W. N Engl J Med 2009 During Endothelialization: Warfarin for 45 days ASA / Plavix for 6 months (TEE) ASA alone

33 Meta-Analysis Shows Comparable Primary Efficacy Results to Warfarin HR p-value Efficacy All stroke or SE Ischemic stroke or SE Hemorrhagic stroke Ischemic stroke or SE >7 days CV/unexplained death All-cause death Major bleed, all Major bleeding, non procedure-related Favors WATCHMAN Favors warfarin Hazard Ratio (95% CI) Source: Holmes DR, et al. Holmes, DR et al. JACC 2015; In Press. Combined data set of all PROTECT AF and PREVAIL WATCHMAN patients versus chronic warfarin patients 33
34 Who should be considered for LAA Closure? 1. Major bleeding while taking anticoagulation therapy 2. Inability to maintain stable INR and not a NOAC candidate 3. CVA/TIA despite therapeutic warfarin or NOAC 34
35 AF Stroke Prevention Key Points Remember CHADS65 risk score NOACs preferred over warfarin NOACs contraindicated in mechanical valves and severe renal failure LAA closure not a replacement for OAC, but can be considered in refractory cases 35
36 Outpatient AF Management AF Management Precipitating cause Stroke Symptoms ASA Warfarin Dabigatran Rivaroxaban Apixaban (LAA Occlusion) Rate Control vs Rhythm Control Medical vs Ablation 36
37 HOW DO I DECIDE BETWEEN RATE VS RHYTHM CONTROL?

38 Case #3: 57M with Lone Paroxsymal AF Severe palpitations 1-3x/month, up to 45 minutes Problem List: mild asthma, solitary kidney with Cr 150 AF with HR = 110bpm 38
39 How should the AF be treated? a) Metoprolol 25mg BID b) Diltiazem 120mg daily c) Digoxin 0.125mg daily d) Amiodarone 200mg daily 39
40 AFib Medical Options 101 Review AVN blocking agents SLOW the AF Beta-receptor antagonist Ca-channel blockers Digoxin Anti-arrhythmic agents STOP the AF Class I: Propafenone, Flecainide Class III: Sotalol, Dronedarone, Amiodarone 40
41 AFFIRM (Rate vs Rhythm) Primary endpoint: All cause mortality N=4,060 No difference between two groups Trend to better survival for rate control after yrs Secondary endpoints functional status QOL ischemic strokes No difference AFFIRM Investigators NEJM 2002;347:
42 Back to Case Young patient with lone PAF Key issue is symptom control Symptoms during AF are poorly rate-controlled (110bpm) Always start with an AVN blocking agent 42
43 Follow-up Visit Patient now on diltiazem 360 mg bid Sinus rates now 50 bpm Repeat Holter: AF episodes still recurrent, but associated with heart rate of bpm 43
44 What is the next step? a) The AF is well rate-controlled... Continue current management b) The AF is still recurrent... Add digoxin c) The AF is still recurrent... Change to an antiarrhythmic medication d) I don t know 44
45 Outpatient AF Management AF Management Precipitating cause Stroke Symptoms ASA Warfarin Dabigatran Rivaroxaban Apixaban (LAA Occlusion) Rate Control vs Rhythm Control Medical vs Ablation 45
46 I TRIED AVN AGENTS AND THE PATIENT STILL FEELS AWFUL. NOW WHAT?
47 Why Rhythm Control? No Symptoms Symptoms Primary evidence-based efficacy is improvement in symptoms Rhythm control should NOT be performed to: Reduce stroke risk Discontinue systemic anticoagulants Make the ECG or Holter look better 47
48 Back to Case... Patient is referred to cardiology / EP specialist They are started on an antiarrhythmic medication What do I need to know? 48
49 Anti-arrhythmic Drug Options Four predominant anti-arrhythmics for rhythm control of AF 1. Propafenone 2. Flecainide (Class I AADs) 3. Sotalol 4. Amiodarone (Class III AADs) 49
50 Anti-arrhythmic Basics Flecainide/Propafenone Requires adjunct AVN blocking agent Contraindicated in heart disease Can widen the QRS or cause VT Typical doses: Flecainide 50mg bid - 150mg bid Propafenone 75mg bid/tid - 300mg tid 50
51 Anti-arrhythmic Basics Sotalol Already has AVN blocking properties Can be used as single agent Dosing 80mg bid - 160mg bid Risk of Torsades de Pointes Contraindicated in Long QT or renal failure Cautious with elderly, females Repeat ECG in 1 wk for QT prolongation 51
52 Anti-arrhythmic Basics Amiodarone Already has AVN blocking properties Can be used as single agent Loading dose: 10g load (400mg bid/tid) Maintenance dose: 200mg daily Requires monitoring for side effects TSH, liver tests every 6 months CXR every year, baseline PFT Ophthalmology, CT chest if symptoms 52
53 Pill-In-The-Pocket Approach Flecainide mg x 1 PRN Propafenone mg x 1 PRN 53
54 AAD Strategy Depends on episode frequency & duration Rare Infrequent Weekly Days Hours Minutes Pill-In-Pocket Maintenance 54
55 Back to Case... Sotalol was started and up-titrated Symptoms continued Patient was switched to Amiodarone and is feeling better Is he going to be considered for cardiac ablation? 55
56 AF Invasive Options Invasive Rate Control AV node ablation (99% success) (with pacemaker implantation) Invasive Rhythm Control Atrial flutter ablation (95% success) Atrial fibrillation ablation (50-80% success) 56

57 AV Node Ablation and Pacemaker Causes complete AV block Atria continue to fibrillate Pacemaker controls HR Must remain on anticoagulation Ultimate rate-control strategy 99% success 1% risk


58 What about invasive rhythm control? Contrast Aflutter and Afib Easier to rhythm control Harder to rate control Simple ablation 95% success Low risk 1-2% Difficult to rhythm control Easier to rate control Complex ablation 50-80% success Higher risk 3-4% 58

59 Atrial Flutter Counterclockwise right atrial reentry
60 Atrial Flutter Ablation Ablation of the cavo-tricuspid isthmus (CTI) Predictable circuit Small lesion set First-line therapy

61 AFib Electrophysiology Chaotic disorganized rhythm
62 Pulmonary Vein Ectopy

63 Fencing off all 4 Veins Success rates for paroxysmal AF is 70-80% Still requires anticoagulation
64 First-line Rhythm Control? Which patients should I refer early? ** Atrial flutter Kerr C, Roy D. Can J Cardiol
65 Stroke Take-Home Points Use CHADS65 risk stratification NOAC preferred over warfarin For those who have a true anticoagulation contraindication, consider LAA closure 65
66 Symptom Take-Home Points For symptomatic atrial fibrillation, start with rate control for most Refer if still symptomatic for initiation of anti-arrhythmic medications or catheter ablation Rhythm control has little role for minimally symptomatic patients Rhythm control does not reduce stroke risk 66
67 Questions? 67
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Half Moon Bay Treatment of Atrial Fibrillation. Dr. Roger A. Winkle MD. Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital
 Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Stroke Prevention in AF: How will it change in the next 5 years? Jeff Healey MD, MSc, FHRS Population Health Research Institute McMaster University
 Stroke Prevention in AF: How will it change in the next 5 years? Jeff Healey MD, MSc, FHRS Population Health Research Institute McMaster University Disclosures Research Grants and speaking fees St. Jude
Stroke Prevention in AF: How will it change in the next 5 years? Jeff Healey MD, MSc, FHRS Population Health Research Institute McMaster University Disclosures Research Grants and speaking fees St. Jude
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Left Atrial Appendage Occlusion
 Left Atrial Appendage Occlusion A new strategy to prevent stroke in atrial fibrillation Ashok Talreja MD and Arijit Chanda MD VHVI symposium 24th February 2018 Outline of presentation 1. Risk of stroke
Left Atrial Appendage Occlusion A new strategy to prevent stroke in atrial fibrillation Ashok Talreja MD and Arijit Chanda MD VHVI symposium 24th February 2018 Outline of presentation 1. Risk of stroke
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Invasive and Medical Treatments for Atrial Fibrillation. Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic
 Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
What s New in the AF Guidelines
 Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Atrial fibrillation and advanced age
 Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Controversies in Atrial Fibrillation and HF
 Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Practical Rate and Rhythm Management of Atrial Fibrillation
 Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Dr Chris Ellis. Consultant Cardiologist Auckland City Hospital Auckland
 Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Left Atrial Appendage Occlusion in the Era of Novel Anticoagulants
 Left Atrial Appendage Occlusion in the Era of Novel Anticoagulants Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac Research Heart Institute, Cedars-Sinai Medical Center,
Left Atrial Appendage Occlusion in the Era of Novel Anticoagulants Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac Research Heart Institute, Cedars-Sinai Medical Center,
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
Treatment strategy decision tree
 strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
Understanding Atrial Fibrillation Management. Roy Lin, MD
 Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion. Greg Francisco, MD, FACC
 Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion Greg Francisco, MD, FACC DISCLOSURES None to declare Estimated 33.5million have AF worldwide (6-7million in
Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion Greg Francisco, MD, FACC DISCLOSURES None to declare Estimated 33.5million have AF worldwide (6-7million in
Atrial fibrillation: current approaches to management
 DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Update in the Management of Atrial Fibrillation
 Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial fibrillation workshop: rate- versus rhythm-control
 Atrial fibrillation workshop: rate- versus rhythm-control Rocky Mountain Internal Medicine Conference Nov, 2011 Dr F. Russell Quinn Cardiac Electrophysiologist, Foothills Medical Centre, Calgary Disclosures
Atrial fibrillation workshop: rate- versus rhythm-control Rocky Mountain Internal Medicine Conference Nov, 2011 Dr F. Russell Quinn Cardiac Electrophysiologist, Foothills Medical Centre, Calgary Disclosures
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Fred Kusumoto Professor of Medicine
 Fred Kusumoto Professor of Medicine Faculty photo will be placed here Kusumoto.Fred@mayo.edu 2015 MFMER 3543652-1 Atrial Fibrillation Presentation Subtitle Here Mayo School of Continuous Professional Development
Fred Kusumoto Professor of Medicine Faculty photo will be placed here Kusumoto.Fred@mayo.edu 2015 MFMER 3543652-1 Atrial Fibrillation Presentation Subtitle Here Mayo School of Continuous Professional Development
קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן
 קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן INTRODUCTION The prevalence of atrial fibrillation (AF) is approximately 1.5 2% of the general population The arrhythmia is associated: with
קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן INTRODUCTION The prevalence of atrial fibrillation (AF) is approximately 1.5 2% of the general population The arrhythmia is associated: with
Left Atrial Appendage Closure Devices. Atrial Fibrillation 10/11/2017
 Left Atrial Appendage Closure Devices Emile Daoud, MD Chief, Cardiac Electrophysiology Wexner Medical Center, The Ohio State University Atrial Fibrillation 1 Adjusted Annual Stroke Risk Using CHA 2 DS
Left Atrial Appendage Closure Devices Emile Daoud, MD Chief, Cardiac Electrophysiology Wexner Medical Center, The Ohio State University Atrial Fibrillation 1 Adjusted Annual Stroke Risk Using CHA 2 DS
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT
 AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
Combined catheter ablation and left atrial appendage closure as a. treatment of atrial fibrillation
 Combined catheter ablation and left atrial appendage closure as a hybrid procedure for the treatment of atrial fibrillation Giulio Molon, MD FACC, FESC, Fellow ANMCO Card Dept, S.Cuore hospital Negrar
Combined catheter ablation and left atrial appendage closure as a hybrid procedure for the treatment of atrial fibrillation Giulio Molon, MD FACC, FESC, Fellow ANMCO Card Dept, S.Cuore hospital Negrar
A Patient Unsuitable for VKA Treatment
 Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Evaluate Risk of Stroke & Bleeding in AF Patients
 XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
Current Guideline for AF Treatment. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
심방세동과최신항응고요법 RACE II AFFIRM 항응고치료는왜중요한가? Rhythm control. Rate control. Anticoagulation 남기병 서울아산병원내과. Clinical Impact of Atrial Fibrillation
 소강당 심방세동과최신항응고요법 남기병 서울아산병원내과 Clinical Impact of Atrial Fibrillation QoL Hospitalization Stroke CHF Mortality 항응고치료는왜중요한가? Rhythm control Rate control Anticoagulation JACC Vol. 38, No. 4, 2001 AFFIRM RACE
소강당 심방세동과최신항응고요법 남기병 서울아산병원내과 Clinical Impact of Atrial Fibrillation QoL Hospitalization Stroke CHF Mortality 항응고치료는왜중요한가? Rhythm control Rate control Anticoagulation JACC Vol. 38, No. 4, 2001 AFFIRM RACE
Samer Nasr, M.D. Mount Lebanon Hospital.
 Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Watchman Implantation Case Presentation and Discussion
 Watchman Implantation Case Presentation and Discussion Walid Saliba, MD, FHRS Director Atrial Fibrillation Center Co-Director AF Stroke Prevention Center Cleveland Clinic Indication FDA NonValvular AF
Watchman Implantation Case Presentation and Discussion Walid Saliba, MD, FHRS Director Atrial Fibrillation Center Co-Director AF Stroke Prevention Center Cleveland Clinic Indication FDA NonValvular AF
Atrial Fibrillation Cases. Dr Paul Broadhurst Consultant Cardiologist
 Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Innovations in AF Management
 Innovations in AF Management Barry Boilson MD PhD FRCPI boilson.barry@mayo.edu Disclosures Relevant None financial relationship(s) with industry None Off Label Usage None Overview Mechanisms of AF AF as
Innovations in AF Management Barry Boilson MD PhD FRCPI boilson.barry@mayo.edu Disclosures Relevant None financial relationship(s) with industry None Off Label Usage None Overview Mechanisms of AF AF as
Rate or Rhythm Control? Epidemiology. Relevant Advances in Atrial Fibrillation 6/20/2011. Stroke Prophylaxis
 Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Saudi Heart Association February 22, 2011
 Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution
 Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
AF review. Petr Polasek
 AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Manuel Castella MD PhD Hospital Clínic, University of
 Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Defining Sub-Clinical Atrial Fibrillation and its management
 Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Update in Left Atrial Appendage Closure Devices. Faisal Al-Samadi MBBS, FRCPC, FACP, FACC, FSCAI, FHRS
 Update in Left Atrial Appendage Closure Devices Faisal Al-Samadi MBBS, FRCPC, FACP, FACC, FSCAI, FHRS Atrial Fibrillation - Overview Higher stroke risk for older patients and those with prior stroke or
Update in Left Atrial Appendage Closure Devices Faisal Al-Samadi MBBS, FRCPC, FACP, FACC, FSCAI, FHRS Atrial Fibrillation - Overview Higher stroke risk for older patients and those with prior stroke or
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Arrhythmias (I) Supraventricular Tachycardias. Disclosures
 Supraventricular Tachycardias. Disclosures") Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto
 Fibrillazione atriale: rischio tromboembolico, Venezia - 27/28 Novembre 2015 Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto Antonio Raviele, MD, FESC,
Fibrillazione atriale: rischio tromboembolico, Venezia - 27/28 Novembre 2015 Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto Antonio Raviele, MD, FESC,
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Atrial Fibrillation: Rate vs. Rhythm. Michael Curley, MD Cardiac Electrophysiology
 Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Relevant Advances in Atrial Fibrillation
 Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisco Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Antiarrhythmic Drug
Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisco Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Antiarrhythmic Drug
Left atrial appendage occlusion
 Kardiologie Left atrial appendage occlusion Mischa Kühne Kardiolunch, 10.9.2015 Overall stroke rate 5% per year CHA 2 DS 2 VASC score Most AF patients need protection from stroke ESC guidelines AF, 2010/2012
Kardiologie Left atrial appendage occlusion Mischa Kühne Kardiolunch, 10.9.2015 Overall stroke rate 5% per year CHA 2 DS 2 VASC score Most AF patients need protection from stroke ESC guidelines AF, 2010/2012
Page 1. Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion. Atrial fibrillation: Scope of the problem
 Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion Benjamin A. D Souza, MD, FACC, FHRS Assistant Professor of Clinical Medicine Penn Presbyterian Medical Center Cardiac
Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion Benjamin A. D Souza, MD, FACC, FHRS Assistant Professor of Clinical Medicine Penn Presbyterian Medical Center Cardiac
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
AF Today: W. For the majority of patients with atrial. are the Options? Chris Case
 AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
Left Atrial Appendage Closure: The Rationale
 Left Atrial Appendage Closure: The Rationale JOHN D. HUMMEL, MD DIRECTOR OF CLINCAL ELECTROPHYSIOLOGY RESEARCH PROFESSOR OF CLINICAL INTERNAL MEDICINE OHIO STATE UNIVERSITY WEXNER MEDICAL CENTER 1 Disclosures
Left Atrial Appendage Closure: The Rationale JOHN D. HUMMEL, MD DIRECTOR OF CLINCAL ELECTROPHYSIOLOGY RESEARCH PROFESSOR OF CLINICAL INTERNAL MEDICINE OHIO STATE UNIVERSITY WEXNER MEDICAL CENTER 1 Disclosures
Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012
 Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012 Professor Dan Atar Head, Dept. of Cardiology Councillor of the ESC,
Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012 Professor Dan Atar Head, Dept. of Cardiology Councillor of the ESC,
Catheter Ablation for Treatment of Atrial Fibrillation 2010 and Beyond
 Catheter Ablation for Treatment of Atrial Fibrillation 2010 and Beyond John M. Miller, MD Professor of Medicine Indiana University School of Medicine Director, Clinical Cardiac Electrophysiology Krannert
Catheter Ablation for Treatment of Atrial Fibrillation 2010 and Beyond John M. Miller, MD Professor of Medicine Indiana University School of Medicine Director, Clinical Cardiac Electrophysiology Krannert
NEW APPROACHES AND NEW ANTICOAGULANTS FOR ATRIAL FIBRILLATION
 NEW APPROACHES AND NEW ANTICOAGULANTS FOR ATRIAL FIBRILLATION MAY 1, 2015 Melissa R. Robinson, MD FACC FHRS CCDS Assistant Professor of Medicine Director of the Complex Arrhythmia Service POINTS TO MAKE
NEW APPROACHES AND NEW ANTICOAGULANTS FOR ATRIAL FIBRILLATION MAY 1, 2015 Melissa R. Robinson, MD FACC FHRS CCDS Assistant Professor of Medicine Director of the Complex Arrhythmia Service POINTS TO MAKE
Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de
 When not to exclude the LAA Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de Barcelona mcaste@clinic.ub.es @mcastellamd Normal hearts Patient in sinus rhythm Patient in AF (with
When not to exclude the LAA Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de Barcelona mcaste@clinic.ub.es @mcastellamd Normal hearts Patient in sinus rhythm Patient in AF (with
Atrial Fibrillation and Common Supraventricular Tachycardias. Sunil Kapur MD
 Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Out with the old, in with The 2010 Atrial Fibrillation Guidelines
 Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011 Outline
Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011 Outline
» A new drug s trial
 » A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
» A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
8/16/2016. Disclosures. Is Uninterrupted OAC Standard of Care for AF Ablation? CHRS 2016, San Francisco. Risk of Stroke Peri-Ablation
 Disclosures Is Uninterrupted OAC Standard of Care for AF Ablation? CHRS 2016, San Francisco Atul Verma, MD FRCPC FHRS Director, Heart Rhythm Program Southlake Regional Health Centre Newmarket, Ontario,
Disclosures Is Uninterrupted OAC Standard of Care for AF Ablation? CHRS 2016, San Francisco Atul Verma, MD FRCPC FHRS Director, Heart Rhythm Program Southlake Regional Health Centre Newmarket, Ontario,
Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France
 Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France LAA Occlusion Is there a real future? Background Protect AF Trial Other Studies CAP, ASAP, Prevail Left Atrial Appendage
Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France LAA Occlusion Is there a real future? Background Protect AF Trial Other Studies CAP, ASAP, Prevail Left Atrial Appendage
AF and arrhythmia management. Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire
 AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
What s new in my specialty?
 What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
ESC. Update of the ESC Guidelines on Medical Therapy. John Camm. ICM Internationales Congress Center München
 ESC 2012 ICM Internationales Congress Center München Update on Consensus Statements on Management of Atrial Fibrillation European Heart Rhythm Association Update of the ESC Guidelines on Medical Therapy
ESC 2012 ICM Internationales Congress Center München Update on Consensus Statements on Management of Atrial Fibrillation European Heart Rhythm Association Update of the ESC Guidelines on Medical Therapy
Management of Atrial Fibrillation in the Hospitalized Patient
 Management of Atrial Fibrillation in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research:
Management of Atrial Fibrillation in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research:
Left Atrial Appendage Closure
 Left Atrial Appendage Closure Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org Risk Factors for Stroke From The Perspective
Left Atrial Appendage Closure Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org Risk Factors for Stroke From The Perspective
Controversies in Risk Stratification
 Controversies in Risk Stratification Things are not as simple as they seem Banff 2017 2015 MFMER 3494750-5 Relative importance Triggers vs Substrate in Pathophysiology of AF AF burden Paroxysmal? Persistent?
Controversies in Risk Stratification Things are not as simple as they seem Banff 2017 2015 MFMER 3494750-5 Relative importance Triggers vs Substrate in Pathophysiology of AF AF burden Paroxysmal? Persistent?
Tricky Cases in Primary Care Anticoagulation in AF
 Tricky Cases in Primary Care Anticoagulation in AF Dr John Wong GPwSI Cardiology & GP Principal Leatherhead Hospital Ashlea Medical Practice 54 year old F Case 1 PMH CREST Syndrome calcinosis finger tips
Tricky Cases in Primary Care Anticoagulation in AF Dr John Wong GPwSI Cardiology & GP Principal Leatherhead Hospital Ashlea Medical Practice 54 year old F Case 1 PMH CREST Syndrome calcinosis finger tips
Atrial Fibrillation Etiologies and Treatment. Shawn Liu Learner Centered Learning Goal
 Atrial Fibrillation Etiologies and Treatment Shawn Liu Learner Centered Learning Goal Pathophysiology Defined by the absence of coordinated atrial systole Results from multiple reentrant electrical waves
Atrial Fibrillation Etiologies and Treatment Shawn Liu Learner Centered Learning Goal Pathophysiology Defined by the absence of coordinated atrial systole Results from multiple reentrant electrical waves
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Fibs and Flutters: The Heart of the Matter
 Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Management of atrial fibrillation a holistic view - Prof. Dr. Martin Borggrefe Mannheim
 a holistic view - Prof. Dr. Martin Borggrefe Mannheim Patients with atrial fibrillation (millions) 16 14 12 10 8 6 4 2 0 Management of atrial fibrillation Expected prevalence of apparent AF 5,1 5,1 5,9
a holistic view - Prof. Dr. Martin Borggrefe Mannheim Patients with atrial fibrillation (millions) 16 14 12 10 8 6 4 2 0 Management of atrial fibrillation Expected prevalence of apparent AF 5,1 5,1 5,9
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen
 What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Devices to Protect Against Stroke in Atrial Fibrillation
 Devices to Protect Against Stroke in Atrial Fibrillation Jonathan C. Hsu, MD, MAS Associate Clinical Professor Division of Cardiology, Section of Cardiac Electrophysiology June 2, 2018 Disclosures Honoraria
Devices to Protect Against Stroke in Atrial Fibrillation Jonathan C. Hsu, MD, MAS Associate Clinical Professor Division of Cardiology, Section of Cardiac Electrophysiology June 2, 2018 Disclosures Honoraria
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation?
 How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Modern management of atrial fibrillation, from blood pressure control to anticoagulation
 Modern management of atrial fibrillation, from blood pressure control to anticoagulation Adel Khalifa S. Hamad, BMS, MD, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist
Modern management of atrial fibrillation, from blood pressure control to anticoagulation Adel Khalifa S. Hamad, BMS, MD, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist
Managing Atrial Fibrillation in the Heart Failure Patient
 Managing Atrial Fibrillation in the Heart Failure Patient Jonathan S. Steinberg, MD Professor of Medicine (adj) University of Rochester School of Medicine & Dentistry Director, Arrhythmia Institute Valley
Managing Atrial Fibrillation in the Heart Failure Patient Jonathan S. Steinberg, MD Professor of Medicine (adj) University of Rochester School of Medicine & Dentistry Director, Arrhythmia Institute Valley
ESC Stockholm Arrhythmias & pacing
 ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
Contemporary Strategies for Catheter Ablation of Atrial Fibrillation
 Contemporary Strategies for Catheter Ablation of Atrial Fibrillation Suneet Mittal, MD Director, Electrophysiology Medical Director, Snyder Center for Atrial Fibrillation The Arrhythmia Institute at The
Contemporary Strategies for Catheter Ablation of Atrial Fibrillation Suneet Mittal, MD Director, Electrophysiology Medical Director, Snyder Center for Atrial Fibrillation The Arrhythmia Institute at The
Survey patients for Sx, signs of AF. Establish AF Dx. Evaluate & Tx underlying heart disease/other causes. Assess adequacy of rate or rhythm control
 Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Atrial Fibrillation in the Emergency Department
 Atrial Fibrillation in the Emergency Department Disclosures Edward Jauch, MD MS Research support National Institutes of Health funding (multiple trials) Novo Nordisk (drug in kind) STOP-IT Study Genentech
Atrial Fibrillation in the Emergency Department Disclosures Edward Jauch, MD MS Research support National Institutes of Health funding (multiple trials) Novo Nordisk (drug in kind) STOP-IT Study Genentech
Atrial Fibrillation. Ivan Anderson, MD RIHVH Cardiology
 Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Conflicts of Interests
 Advances in the Management of Atrial Fibrillation State of the Art in 2013 Overview of AF Stroke risk and anticoagulation Rate control Antiarrhythmic Drug Therapy Catheter ablation Conclusion Hugh Calkins
Advances in the Management of Atrial Fibrillation State of the Art in 2013 Overview of AF Stroke risk and anticoagulation Rate control Antiarrhythmic Drug Therapy Catheter ablation Conclusion Hugh Calkins
Newer Anti-Anginal Agents and Anticoagulants
 Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
Left Atrial Appendage Closure in SCRIPPS CLINIC
 Left Atrial Appendage Closure in Atrial Fibrillation to Prevent Stroke Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
Left Atrial Appendage Closure in Atrial Fibrillation to Prevent Stroke Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org