Out with the old, in with The 2010 Atrial Fibrillation Guidelines
|
|
|
- Nicholas Lawson
- 5 years ago
- Views:
Transcription
1 Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011
2 Outline Introduction Level of Evidence Rate Control Strategy Rhythm Control Strategy Catheter Ablation ED Management Thromboembolism prophylaxis Post-Operative AF (POAF)
3 Level of Evidence
4 2010 CCS AF Guidelines Grades of Recommendation Assessment Development and Evaluation Acknowledges values and preferences Explicit comprehensive criteria for downgrading and upgrading quality ratings Transparent process of moving from evidence to recommendations Explicit acknowledgement of values and preferences Clear pragmatic interpretation of strong versus weak recommendations Useful for systematic reviews and health technology assessments, as well as guidelines Guyatt GH, et. al. BMJ. 2008; 336:
5 GRADE: Quality of evidence HIGH Future research unlikely to change confidence in estimate of effect MODERATE Further research likely to have an important impact on confidence in estimate of effect and may change the estimate LOW Further research very likely to have a significant impact on the estimate of effect and is likely to change the estimate VERY LOW The estimate of effect is very uncertain
6 GRADE: Strength of Recommendation Quality of evidence quality of evidence = probability that a strong recommendation is indicated Difference b/w desirable and undesirable effects Values & preferences Cost difference between desirable and undesirable effects = probability that a strong recommendation is indicated variation or uncertainty in values and preferences = probability that a conditional recommendation is indicated cost = likelihood that a strong recommendation is indicated
7 Goals of Therapy
8 2010 CCS Guidelines Goals of ventricular rate control should be to improve symptoms and quality of life which are attributable to excessive ventricular rates. (Strong recommendation, low quality) Goals of rhythm control therapy should be to improve patient symptoms and clinical outcomes, and that these do not necessarily imply the elimination of all AF. (Strong recommendation, moderate quality)

9 SAF Score QoL of the AF patient should be assessed in routine care using the CCS SAF scale (Conditional Recommendation, Low-Quality Evidence). 9
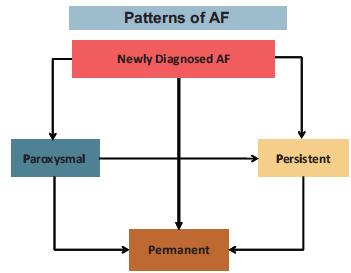
10 AF Classification
11 Rate or Rhythm
12 Rate VS Rhythm Rate AND/OR Rhythm
13 2010 CCS Guidelines In stable patients with recent-onset AF/AFL, a strategy of rate or rhythm control could be selected (Strong Recommendation, High-Quality Evidence). May require both simultaneously Recommended frequent re-evaluation
14 Rate or Rhythm Favour rate control Favours rhythm control Persistent AF Paroxysmal AF Newly detected AF Recurrent AF 1 st episode of AF Less symptomatic Symptomatic > 65 y.o. < 65 y.o. HTN No HTN No CHF CHF Rhythm failure No rhythm failure Patient preference Patient preference
15 Rate Control
16 Rate Target 2004 CCS < 80bpm at rest <110 bpm during 6-min walk <100 bpm on average 2006 ACC/AHA 2010 ECS 80 bpm at rest <110 bpm at rest <80 bpm at rest and <110 bpm with exercise if symptomatic or tachycardiomyopathy, on lenient control
17 RACE II Design Population Treatment Follow-up Randomized, open label, non-inferiority N=614; < 80y/o, permanent AF, mean resting HR >80 bpm Strict: resting HR < 80bpm, < 110bpm w/ exercise Lenient: HR < 110bpm 2-3 years HR achieved Strict: 75 bpm; Lenient: 86 bpm 1 o outcome (composite) Lenient control was non-inferior to strict control in terms of major clinical events New Engl J Med 2010;362:
18 2010 CCS Guidelines Treatment for rate control of persistent or permanent AF or AFL should aim for a resting HR of < 100 bpm (Strong Recommendation, High-Quality Evidence).


19

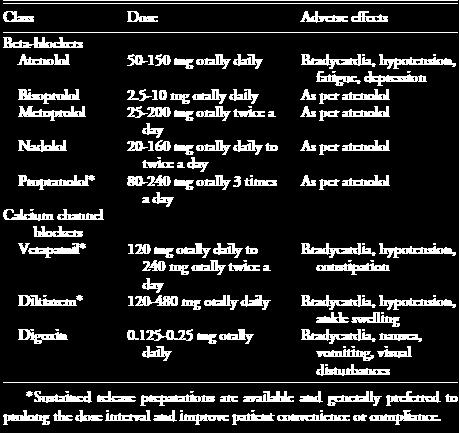

20 Rate Control Drugs 20
21 2010 CCS Guidelines Dronedarone may be added for additional rate control in patients with uncontrolled ventricular rates despite therapy with BBs, CCBs, digoxin (Conditional Recommendation, Moderate- Quality Evidence). Amiodarone for rate control should be reserved for exceptional cases in which other means are not feasible or are insufficient (Conditional Recommendation,Low-Quality Evidence).
22 ERATO Design Population Treatment Follow-up N=174, RCT, DB, parallel groups Permanent AF Dronedarone 400mg PO BID vs Placebo *in addition to standard therapy 6 months 1 o Endpoint Ventricular rate Results At day 14 of 11.7 bpm (P <.0001). Effect sustained throughout 6-months. At max exercise of 24.5 bpm (P <.0001); no in exercise tolerance. The effects additive to BB, CCB, digoxin. Tolerated well, no organ toxicities or proarrhythmia. Am Heart J 2008;156:527e1-e9. 22
23 2010 Guidelines Consider AV junction ablation and implantation of a permanent pacemaker in symptomatic patients with uncontrolled ventricular rates during AF despite maximally tolerated combination pharmacologic therapy (Strong Recommendation, Moderate-Quality Evidence).
24 Rhythm Control
25 Rhythm Control Rate vs rhythm control, no difference on mortality (AFFIRM, RACE, PIAF trials, AF- CHF) Rhythm control does not incidence of thromboembolism
26 2010 CCS Guidelines May use rhythm-control strategy for patients with AF/ AFL who remain symptomatic with rate-control therapy or in whom rate-control therapy is unlikely to control symptoms (Strong Recommendation, Moderate-Quality Evidence). The goal of rhythm-control therapy is improvement in patient symptoms and clinical outcomes, and not necessarily the elimination of all AF (Strong Recommendation, Moderate-Quality Evidence).

27

28 2010 ECS: Rhythm Control
29 ATHENA Design Population Treatment RCT, PLB, DB, parallel arm N=4628; AF and >1 of: 70yrs+, HTN, DM, previous stroke or left atrial diameter > 50mm, EF < 40%. Excludied patients with severe HF. Baseline 71yrs; CAD=30%; HF=21%; EF<35% = 3.9%. Dronedarone 400 mg BID vs placebo; f/u for 21 months 1 o Endpoint First CV hospitalization or death Results Dronedarone = 24% in CV hospitalizations or death (p<0.001); Overall mortality NSS (p = 0.18); CV mortality with dronedarone (p = 0.03). ADR: GI SEs and creatinine Conclusion Dronedarone incidence of death or hospitalizations and is safe and effective in the chronic management of AF in high-risk patients. New Engl J Med 2009;360:668-78
30 ANDROMEDA Stopped Design RCT, PLB, DB Population N=627; 18 y.o. recently hospitalized with HF and SOB NYHA III- IV. Baseline 71yrs; MI=54%; ischemic heart dx=66%; AF=36-39%; 40% NYHA Class II; 57% NYHA Class III Treatment Endpoints Results Note Dronedarone 400mg PO BID vs Placebo x 2 months f/u Death (any cause) or hospitalization for worsening HF death in dronedarone group HR=2.13 ( ) P=0.03 Sponsor s hypothesis mortality is a consequence of early discontinuation of ACEI or ARB due to dronedarone s ability to inhibit creatinine secretion. New Engl J Med 2008;358:
31 Rhythm Control Drugs Drug Dose Efficacy at 1y Flecanide mg BID Propafenone mg TID Amiodarone mg OD (after 10 g loading) Dronedarone 400 mg BID Toxicity 30-50% Ventricular tachycardia Bradycardia Rapid ventricular response to 30-50% AF/AFL (1:1 conduction) Propafenone = abnormal taste 60-70% Photosensitivity Bradycardia GI upset Thyroid dysfunction Hepatic toxicity Neuropathy, tremor Pulmonary toxicity Torsades de pointes (rare) 40% GI upset Bradycardia Comments Contraindicated in patients with CAD or LV dysfunction Should be combined with an AV nodal blocking agent Low risk of proarrhythmia in a wide range of populations Limited by systemic side effects Most side effects are dose and duration related Very effective for rate control Only antiarrhythmic shown to reduce hospitalizations and cardiovascular mortality (ATHENA May mortality in patients with recently decompensated HF, EF <35% (ANDROMEDA) Effective rate-control agent New drug limited experience outside trials Sotalol mg BID 30-50% Torsades de pointes Bradycaria Beta-blocker SE Should be avoided in patients at high risk of torsades VT - especially women aged 65 y taking diuretics or those with renal insufficiency. QT interval should be monitored 1 wk after starting. Use cautiously when EF <40%. Heart rhythm specialists may use with lower EFs if patient has ICD 31
32 Pill in Pocket Recommended in recurrent, infrequent, longlasting episodes of AF (Strong Recommendation, Moderate Quality Evidence) Flecainide ( mg) or propafenone ( mg) +/- short-acting beta-blocker (metoprolol mg) or CCB Efficacy: 50-80% acute termination of AF
33 ED Management
34 ED Management Lack of clear evidence AFFIRM and AF-CHF excluded <48 hrs onset of symptoms Equal evidence for either strategy for AF < 48hrs 34
35 2010 CCS Guidelines For patients with acute hemodynamic instability secondary to rapid recent-onset AF/AFL, immediate electrical conversion to sinus rhythm (Strong Recommendation, Low-Quality Evidence). In hemodynamically stable patients with AF/AFL of known duration < 48 hours in whom a strategy of rhythm control has been selected: Rate-slowing agents alone are acceptable while awaiting spontaneous conversion (Strong Recommendation, Moderate-Quality Evidence). Synchronized electrical cardioversion or pharmacologic cardioversion may be used when a decision is made to cardiovert patients in the ED. (Strong Recommendation, Moderate-Quality Evidence). Antiarrhythmic drugs may be used to pretreat patients before electrical cardioversion in ED in order to decrease early recurrence of AF and to enhance cardioversion efficacy (Conditional Recommendation, Low- Quality Evidence). 35

36 36
37 Pharmacologic Cardioversion 37
38 38
39 Thromboembolism in ED Hemodynamically stable patients with AF/AFL of known duration < 48 hours for whom a strategy of rhythm control has been selected may generally undergo cardioversion without prior or subsequent anticoagulation. However, if the patient is at particularly high risk of stroke (eg, mechanical valve, rheumatic heart disease, recent stroke, or transient ischemic attack), cardioversion should be delayed and the patient should receive OAC for 3 weeks before and at least 4 weeks postcardioversion. Following attempted CV: If AF or AFL persists, recurs, or if symptoms suggest that the presenting AF/AFL has been recurrent, antithrombotic therapy should be commenced and continued indefinitely. If NSR is achieved, the need for ongoing antithrombotic therapy should be determined based on the risk of stroke according to CHADS2 score and early consultant follow-up should be arranged (Strong Recommendation, Low-Quality Evidence). 39
40 40
41 ED Rate Control 41

42 42
43 Thromboembolism in ED Hemodynamically stable patients with AF/AFL of > 48 hours or uncertain duration for whom a strategy of rhythm control has been selected should have rate control optimized and receive therapeutic OAC therapy (warfarin [INR 2-3] or dabigatran) for 3 weeks before and at least 4 weeks post-cardioversion. Following attempted CV: If AF/AFL persists or recurs or if symptoms suggest that the presenting AF/AFL has been recurrent, the patient should have antithrombotic therapy continued indefinitely. If sinus rhythm is achieved and sustained for 4 weeks, the need for ongoing antithrombotic therapy should be determined based on the risk of stroke, and in selected cases, expert consultation may be required (Strong Recommendation, Moderate-Quality Evidence). 43
44 Disposition After conversion to sinus rhythm has been achieved, whether antiarrhythmic drug therapy is indicated should be based on the estimated probability of recurrence and the symptoms during AF. Long-term therapy will need to be determined by an appropriate outpatient consultation (Conditional Recommendation, Low-Quality Evidence). 44
45 Catheter Ablation 45
46 Catheter Ablation of AF Alternative for maintaining sinus rhythm when drugs have been ineffective or intolerable, who remain in symptomatic AF. More effective at maintaining SR than drugs AND improves QOL. How does it work? Use for rhythm control, particularly effective in paroxysmal AF. 90% of triggering foci in AF originate in or around the pulmonary veins (PV) of the left atrium (LA), which can be responsible for both triggering and maintaining AF. The areas around the PVs are ablated, thus isolating them from the LA, and eliminating the triggering foci and preventing AF.
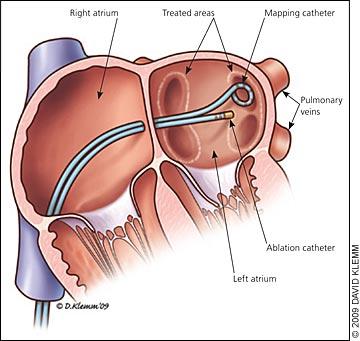

47 Catheter Ablation h"p:// h"p://
48 2010 CCS Guidelines Catheter ablation to maintain sinus rhythm in select patients with symptomatic AF and mild-moderate structural heart disease who are refractory or intolerant to 1 anti-arrhythmic medication. (Conditional Recommendation, Moderate Quality Evidence). Catheter ablation of AF in patients who remain symptomatic following adequate trials of anti-arrhythmic drug therapy and in whom a rhythm control strategy remains desired. (Strong Recommendation, Moderate Quality Evidence) Catheter ablation to maintain sinus rhythm as first-line therapy for relief of symptoms in highly selected patients with symptomatic, paroxysmal AF. (Conditional Recommendation, Low Quality Evidence)
49 Anticoagulation in Catheter Ablation Anticoagulation: warfarin 1-2 months prior and 3-6 months following. Possible TEE to rule out thrombus prior to procedure. Anticoagulation during procedure is maintained by preprocedure warfarin (at lower end of INR target) or LMWH bridging before and after. Patients should continue indefinite anticoagulation as determined by their preablation CHADS 2 score.
50 Risks & Efficacy Risks Vascular access complication: Hematoma Pseudoaneurysm AV fistula Cardiac perforation Thromboembolism Damage to esophagus Efficacy More effective than antiarrhythmic drug therapy and associated with a decrease in cardiovascular hospitalizations 60-75% success rate after 1 procedure; 75-90% after 2 Significant improvement in QOL 50
51 Surgical Therapy 51
52 Surgical therapy Open heart surgery approach to break patterns of conductivity Role for therapy in conjunction with other heart surgeries, such as valve replacement, when presurgical AF exists. Evidence shows much higher rates of sinus rhythm in patients who received concomitant AF surgery during other heart procedures than those who did not Anticoagulation must be continued long-term as determined by pre-operative CHADS 2 score as there is no data to suggest a decrease in stroke risk following this procedure.
53 2010 CCS AF Guidelines Surgical AF ablation procedure be undertaken in association with mitral valve surgery in patients with AF when there is a strong desire to maintain sinus rhythm, the likelihood of success of the procedure is deemed to be high, and the additional risk is low. (Strong Recommendation, Moderate Quality Evidence) In patients with AF who are undergoing aortic valve surgery or coronary artery bypass surgery, we suggest that a surgical AF ablation procedure be undertaken when there is a strong desire to maintain sinus rhythm, the success of the procedure is deemed to be high, and the additional risk low. (Conditional Recommendation, Low-Quality Evidence) Oral anticoagulant therapy be continued following surgical AF ablation in patients with a CHADS2 score >/= 2. (Strong Recommendation, Moderate- Quality Evidence)
54 Thromboembolism and Bleeding Risk 54
55 Risk of Stroke CHADS 2 score Validated form of assessing stroke risk in patients with AF If score is 0 then very low risk, ASA is sufficient If >/= 1 then OAC is recommended CHA 2 DS 2 -VASc score Included in European guidelines, validated in the Euro Heart Survey of AF patients Contains more variables than CHADS 2 Intended for use in patients with a slow CHADS 2 (0 or 1) to determine need for stroke prevention CCS recommendation is to continue the use of CHADS 2 55
56 Risk of Stroke 56

57 Scoring Systems 57
58 Therapeutic Alternatives ASA vs. no treatment Warfarin vs. no treatment ASA vs. Warfarin Stroke Risk RRR for all stroke of 19% (95% CI, 1% to 35%) ARR of 0.8% per year in primary prevention trials and 2.5% per year in secondary prevention trials RRR for all stroke of 64% (95% CI, 49% to 74%; ischemic or hemorrhagic RRR for all stroke of 39% (95% CI, 19%-53%) in favour of vitamin K antagonists Bleeding Risk No significant differences in major extracranial hemorrhage or mortality 0.3% excess of major extracranial hemorrhage (p = NS). ARR of mortality of about 1.6% per year No significant differences in major extracranial hemorrhage or mortality as per meta-analysis
59 Therapeutic Alternatives ASA and clopidogrel vs. warfarin ASA and clopidogrel vs. ASA alone Stroke Risk Outcome: composite of stroke, non-cns embolus, MI, and vascular death RR = 1.44 (95% CI, ; P =.0003) Risk of major vascular events was reduced with the combo: RR 0.89; 95% CI, ; (P =.01) Bleeding Risk The RR for major bleeding was 1.10 (95% CI, ) with the combination Major bleeding increased with combo: 2.0% vs 1.3% per year; RR 1.57; 95% CI, ; ( P <.01)
60 Dabigatran: RE-LY Design Population Treatment Endpoints Results For 1 o outcome Results For risk of bleeding:2 o Open labelled RCT with 2 yr f/u, non-inferiority trial N=18311, mean CHADS 2 =2.1, 20% also on ASA, mean age=71 Exclusion: CrCl < 30 or any condition that increased bleeding Dabigatran 110 mg BID vs. Dabigatran 150 mg BID vs. warfarin (INR 2-3) 1 o : all stroke (ischemic or hemorrhagic) OR non-central nervous system embolus Dabigatran 150 mg vs. warfarin: RR 0.66 (95% CI ) P <.001 for superiority Dabigatran 110 mg vs. warfarin: RR 0.91 (95% CI ) P <.001 for noninferiority Dabigatran 150 mg vs. warfarin: RR 0.93, P =.31 Dabigatran 110 mg vs. warfarin: RR 0.8, P =
61 Risk of Bleeding Risk stratification tools: HEMORR 2 HAGES Uses many variables, some difficult to attain (such as genetic factors) to determine annual risk of hospitalization for hemorrhage. HAS-BLED Developed as part of ESC guidelines See next slide for criteria Performs at least as well as HEMORR 2 HAGES
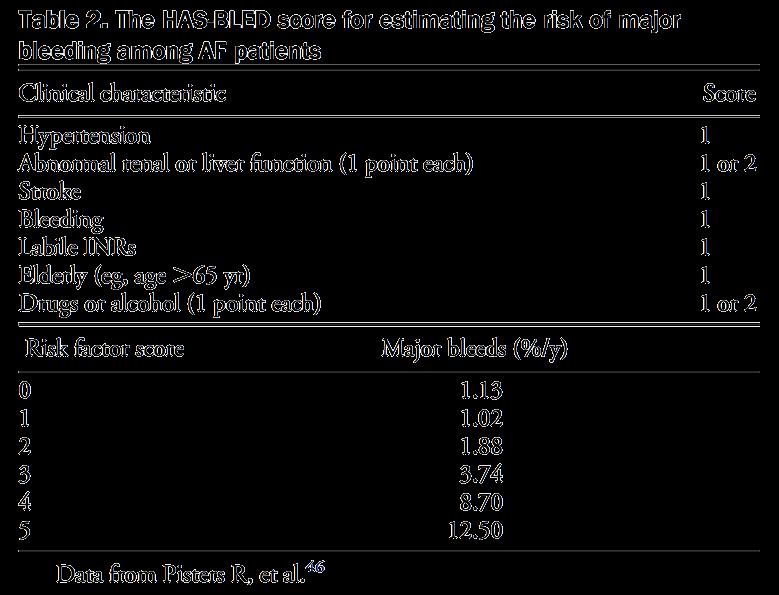

62 HAS-BLED
63 2010 CCS AF Guidelines All patients with AF/AFL (paroxysmal, persistent, or permanent) should be stratified using a predictive index for stroke (eg, CHADS2) and for the risk of bleeding (eg, HAS-BLED) and most patients should receive antithrombotic therapy (Strong Recommendation, High-Quality Evidence) Patients at very low risk of stroke (CHADS 2 = 0) should receive aspirin ( mg/d) (Strong Recommendation, High-Quality Evidence). Patients at low risk of stroke (CHADS 2 = 1) should receive OAC therapy (either warfarin [INR 2 to 3] or Dabigatran) (Strong Recommendation, High-Quality Evidence). Based on individual riskbenefit considerations, aspirin is a reasonable alternative for some (Conditional Recommendation, Moderate-Quality Evidence). 63
64 2010 CCS AF Guidelines Patients at moderate risk of stroke (CHADS 2 >/=2 should receive OAC therapy (either warfarin [INR 2-3] or Dabigatran) (Strong Recommendation, High-Quality Evidence). When OAC therapy is indicated, most patients should receive dabigatran in preference to warfarin. In general, the dose of dabigatran 150 mg by mouth twice a day is preferable to a dose of 110 mg by mouth twice a day (exceptions discussed in text) (Conditional Recommendation, High-Quality Evidence). 64

65

66

67
68 Other Agents: Apixaban Oral direct acting factor Xa inhibitor AVERROES: compared with ASA in AF when warfarin was not an option; terminated for early efficacy at 5mg po BID without an increase in the risk of major bleeds or intracranial hemorrhage ARISTOTLE: ongoing study comparing apixaban to warfarin for the prevention of stroke and systemic embolism in patients with AF and risk factors for stroke. 68
69 Other Agents: Rivaroxaban Oral direct acting factor Xa inhibitor ROCKET-AF: Rivaroxaban 20mg daily (or 15 mg if mild renal impairment) vs. warfarin (INR 2-3) Showed rivaroxaban to be non-inferior to warfarin with regards to all stroke and systemic embolism. Comparable rates of bleeding between the two arms.
 or Dabigatran 150 BID * CEC = Chua, Elliot, Chernushkin 70")
70 CEC* Hierarchy for Bleeding ASA or Clopidogrel ASA and Clopidogrel Dabigatran 110 BID Warfarin (INR 2-3) or Dabigatran 150 BID * CEC = Chua, Elliot, Chernushkin 70











71 CEC Hierarchy of Efficacy AVERROES Apixaban? Dabigatran 150 BID Dabigatran 110 BID or Warfarin (INR 2-3) or?rivaroxaban ASA and Clopidogrel RE-LY RE-LY ROCKET-AF ACTIVE ASA SPAF 71
72 AF Post-Cardiac Surgery


73 Burgess DC, et. al. Eur Heart J; 2006
74 POAF - Prevention Patients on beta-blocker before cardiac surgery continue through operative procedure (Strong Recommendation, High Quality Evidence). Patients not on beta-blocker before surgery, initiate immediately after the procedure (Conditional Recommendation, Low Quality Evidence).
75 POAF - Prevention Patients with contraindication to beta-blocker before or after cardiac surgery, consider prophylaxis with amiodarone (Strong Recommendation, High Quality Evidence). Patients whith contraindication to beta-blocker and amiodarone consider IV Mg (Conditional Recommendation, Moderate Quality Evidence) or biatrial pacing (Conditional Recommendation, Low Quality Evidence).
76 POAF - Prevention Patients at high risk of POAF consider prophylactic therapy with sotalol or combination including 2 of: beta-blocker, amiodarone, IV magnesium, biatrial pacing (Conditional Recommendation, Low to Moderate Quality Evidence).
77 POAF - Treatment POAF with a rapid ventricular response to be treated with a beta-blocker, a NDHP CCB, or amiodarone to establish rate control. Betablocker is preferred (Strong Recommendation, High Quality Evidence). POAF may be appropriately treated with either a rate-control or rhythm-control strategy (Conditional Recommendation, Low Quality Evidence).
78 POAF - Treatment Consideration to be given to anticoagulation therapy if POAF persists for >72 hrs. (Conditional Recommendation, Low Quality Evidence). Reconsideration of the ongoing need for POAF therapies should be undertaken in 6-12 weeks (Strong Recommendation, Moderate Quality Evidence).

79 The END... 79
What s New in the AF Guidelines
 Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Understanding Atrial Fibrillation Management. Roy Lin, MD
 Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Current Guideline for AF Treatment. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Practical Rate and Rhythm Management of Atrial Fibrillation
 Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
심방세동과최신항응고요법 RACE II AFFIRM 항응고치료는왜중요한가? Rhythm control. Rate control. Anticoagulation 남기병 서울아산병원내과. Clinical Impact of Atrial Fibrillation
 소강당 심방세동과최신항응고요법 남기병 서울아산병원내과 Clinical Impact of Atrial Fibrillation QoL Hospitalization Stroke CHF Mortality 항응고치료는왜중요한가? Rhythm control Rate control Anticoagulation JACC Vol. 38, No. 4, 2001 AFFIRM RACE
소강당 심방세동과최신항응고요법 남기병 서울아산병원내과 Clinical Impact of Atrial Fibrillation QoL Hospitalization Stroke CHF Mortality 항응고치료는왜중요한가? Rhythm control Rate control Anticoagulation JACC Vol. 38, No. 4, 2001 AFFIRM RACE
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Half Moon Bay Treatment of Atrial Fibrillation. Dr. Roger A. Winkle MD. Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital
 Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med
 Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med None There s no reason to panic. While it is true that one of the crew members is ill, slightly. Absence of discrete P waves Chaotic
Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med None There s no reason to panic. While it is true that one of the crew members is ill, slightly. Absence of discrete P waves Chaotic
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Fibs and Flutters: The Heart of the Matter
 Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Treatment strategy decision tree
 strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
Atrial Fibrillation: It s More than a Rhythm
 Atrial Fibrillation: It s More than a Rhythm Relax and Learn at the Farm 2013 DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular Nursing Education Associates 1 The Quality of a Person s Life is Directly Proportional
Atrial Fibrillation: It s More than a Rhythm Relax and Learn at the Farm 2013 DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular Nursing Education Associates 1 The Quality of a Person s Life is Directly Proportional
Invasive and Medical Treatments for Atrial Fibrillation. Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic
 Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
» A new drug s trial
 » A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
» A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
Dronedarone: Need to Perform a CV Outcome Safety Study
 Dronedarone: Need to Perform a CV Outcome Safety Study Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, Boehringer-Ingelheim, Daiichi-Sankyo, Bristol Myers Squibb, Otsuka, Janssen
Dronedarone: Need to Perform a CV Outcome Safety Study Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, Boehringer-Ingelheim, Daiichi-Sankyo, Bristol Myers Squibb, Otsuka, Janssen
Rate or Rhythm Control? Epidemiology. Relevant Advances in Atrial Fibrillation 6/20/2011. Stroke Prophylaxis
 Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
ESC Stockholm Arrhythmias & pacing
 ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
Are Drugs Better? Dr Mauro Lencioni. Drugs or ablation as first line treatment for AF? Consultant Cardiologist & Electrophysiologist
 Are Drugs Better? Drugs or ablation as first line treatment for AF? Dr Mauro Lencioni Consultant Cardiologist & Electrophysiologist The Philosophical Issue What do we mean by Better? Outcome measures Measurement
Are Drugs Better? Drugs or ablation as first line treatment for AF? Dr Mauro Lencioni Consultant Cardiologist & Electrophysiologist The Philosophical Issue What do we mean by Better? Outcome measures Measurement
Atrial Fibrillation Management in the ED. J Fisher May 2014"
 Atrial Fibrillation Management in the ED J Fisher May 2014" A 48 yr old man presents with palpitations. He had a big night last night with old mates. ECG How will you manage him? Why important? Common
Atrial Fibrillation Management in the ED J Fisher May 2014" A 48 yr old man presents with palpitations. He had a big night last night with old mates. ECG How will you manage him? Why important? Common
Treatment of Atrial Fibrillation in Heart Failure
 Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Atrial fibrillation workshop: rate- versus rhythm-control
 Atrial fibrillation workshop: rate- versus rhythm-control Rocky Mountain Internal Medicine Conference Nov, 2011 Dr F. Russell Quinn Cardiac Electrophysiologist, Foothills Medical Centre, Calgary Disclosures
Atrial fibrillation workshop: rate- versus rhythm-control Rocky Mountain Internal Medicine Conference Nov, 2011 Dr F. Russell Quinn Cardiac Electrophysiologist, Foothills Medical Centre, Calgary Disclosures
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Medical management of AF: drugs for rate and rhythm control
 Medical management of AF: drugs for rate and rhythm control Adel Khalifa Sultan Hamad, BMS, MD, FGHRS, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist Head of Electrophysiology
Medical management of AF: drugs for rate and rhythm control Adel Khalifa Sultan Hamad, BMS, MD, FGHRS, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist Head of Electrophysiology
5/5/2010. World incidence 720, 000 new cases / year. World prevalence 5.55 million AF prevalence increasing with aging of population
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Samer Nasr, M.D. Mount Lebanon Hospital.
 Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Controversies in Atrial Fibrillation and HF
 Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
AF and arrhythmia management. Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire
 AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
Relevant Advances in Atrial Fibrillation
 Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisco Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Antiarrhythmic Drug
Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisco Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Antiarrhythmic Drug
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology World incidence 720, 000 new cases / year World prevalence 5.5 million
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology World incidence 720, 000 new cases / year World prevalence 5.5 million
Atrial fibrillation and advanced age
 Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Online Supplement. Management of Atrial Fibrillation: Complete Guidelines Listing
 1 Online Supplement Management of Atrial Fibrillation: Complete Guidelines Listing Laurent Macle, MD (Co-Chair), Jason Andrade, MD, Clare Atzema, MD, Alan D. Bell, MD, John A. Cairns, MD, Stuart Connolly,
1 Online Supplement Management of Atrial Fibrillation: Complete Guidelines Listing Laurent Macle, MD (Co-Chair), Jason Andrade, MD, Clare Atzema, MD, Alan D. Bell, MD, John A. Cairns, MD, Stuart Connolly,
Dr Chris Ellis. Consultant Cardiologist Auckland City Hospital Auckland
 Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017
 MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017 1 Faculty Disclosure Faculty: Peter Leong-Sit MSc, MD, FRCPC, FHRS Associate Professor, Western University Cardiologist, London Heart
MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017 1 Faculty Disclosure Faculty: Peter Leong-Sit MSc, MD, FRCPC, FHRS Associate Professor, Western University Cardiologist, London Heart
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital
 Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Hypertension and Atrial Fibrillation in 2017
 Boma Inn, Eldoret, 24th 25thFebruary 2017 Hypertension and Atrial Fibrillation in 2017 Dr Mzee Ngunga Consultant Cardiologist Aga Khan University Hospital, Nairobi Objectives 1. Understand the relationship
Boma Inn, Eldoret, 24th 25thFebruary 2017 Hypertension and Atrial Fibrillation in 2017 Dr Mzee Ngunga Consultant Cardiologist Aga Khan University Hospital, Nairobi Objectives 1. Understand the relationship
Fred Kusumoto Professor of Medicine
 Fred Kusumoto Professor of Medicine Faculty photo will be placed here Kusumoto.Fred@mayo.edu 2015 MFMER 3543652-1 Atrial Fibrillation Presentation Subtitle Here Mayo School of Continuous Professional Development
Fred Kusumoto Professor of Medicine Faculty photo will be placed here Kusumoto.Fred@mayo.edu 2015 MFMER 3543652-1 Atrial Fibrillation Presentation Subtitle Here Mayo School of Continuous Professional Development
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Update in the Management of Atrial Fibrillation
 Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Canadian Cardiovascular Society Atrial Fibrillation Guidelines
 Canadian Cardiovascular Society 2010 Atrial Fibrillation Guidelines Table of Contents Table of Contents... 2 Author Listing... 3 Chapter 2: Atrial Fibrillation: Etiology and Initial Investigations... 6
Canadian Cardiovascular Society 2010 Atrial Fibrillation Guidelines Table of Contents Table of Contents... 2 Author Listing... 3 Chapter 2: Atrial Fibrillation: Etiology and Initial Investigations... 6
UC SF. Division of General Internal Medicine UNIVERSITY OF CALIFORNIA SAN FRANCISCO, DIVISION OF HOSPITAL MEDICINE
 Updates in the Management of Atrial Fibrillation Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic UC SF Division of
Updates in the Management of Atrial Fibrillation Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic UC SF Division of
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן
 קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן INTRODUCTION The prevalence of atrial fibrillation (AF) is approximately 1.5 2% of the general population The arrhythmia is associated: with
קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן INTRODUCTION The prevalence of atrial fibrillation (AF) is approximately 1.5 2% of the general population The arrhythmia is associated: with
Atrial Fibrillation. Ivan Anderson, MD RIHVH Cardiology
 Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Objectives for Technicians. Objectives for Pharmacists. Pathophysiology. Conflict of Interest. Atrial Fibrillation
 Warfar IN or Warfar-OUT? And Other Updates in the Management of Atrial Fibrillation Kimberly Ackerbauer, PharmD, BCPS Clinical Pharmacy Specialist Rush University Medical Center Conflict of Interest I
Warfar IN or Warfar-OUT? And Other Updates in the Management of Atrial Fibrillation Kimberly Ackerbauer, PharmD, BCPS Clinical Pharmacy Specialist Rush University Medical Center Conflict of Interest I
Cardiovascular Pharmacotherapy Update
 Cardiovascular Pharmacotherapy Update Debby Caraballo, PharmD, PhC, BCPS April 30 th 2011 Objectives Review recent updates in cardiovascular pharmacotherapy Discuss the updates to Afib, UA/NSTEMI, STEMI/PCI
Cardiovascular Pharmacotherapy Update Debby Caraballo, PharmD, PhC, BCPS April 30 th 2011 Objectives Review recent updates in cardiovascular pharmacotherapy Discuss the updates to Afib, UA/NSTEMI, STEMI/PCI
A Patient Unsuitable for VKA Treatment
 Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care
 Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care 11 th and 25 th September 2014 3 KEY OBJECTIVES OF TALK 1.
Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care 11 th and 25 th September 2014 3 KEY OBJECTIVES OF TALK 1.
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Dronedarone for the treatment of non-permanent atrial fibrillation
 Dronedarone for the treatment of non-permanent atrial Issued: August 2010 last modified: December 2012 guidance.nice.org.uk/ta197 NICE has accredited the process used by the Centre for Health Technology
Dronedarone for the treatment of non-permanent atrial Issued: August 2010 last modified: December 2012 guidance.nice.org.uk/ta197 NICE has accredited the process used by the Centre for Health Technology
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Atrial Fibrillation: Beyond the AFFIRM trial
 Atrial Fibrillation: Beyond the AFFIRM trial Daniel J. Cantillon MD FACC FHRS Cardiac Electrophysiology and Pacing Assistant Professor, Lerner College of Medicine Cleveland Clinic, Heart & Vascular Institute
Atrial Fibrillation: Beyond the AFFIRM trial Daniel J. Cantillon MD FACC FHRS Cardiac Electrophysiology and Pacing Assistant Professor, Lerner College of Medicine Cleveland Clinic, Heart & Vascular Institute
Conflicts of Interests
 Advances in the Management of Atrial Fibrillation State of the Art in 2013 Overview of AF Stroke risk and anticoagulation Rate control Antiarrhythmic Drug Therapy Catheter ablation Conclusion Hugh Calkins
Advances in the Management of Atrial Fibrillation State of the Art in 2013 Overview of AF Stroke risk and anticoagulation Rate control Antiarrhythmic Drug Therapy Catheter ablation Conclusion Hugh Calkins
Atrial Fibrillation: Rate vs. Rhythm. Michael Curley, MD Cardiac Electrophysiology
 Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Management of Acute Atrial Fibrillation
 Management of Acute Atrial Fibrillation Tanner Moser, PharmD PGY- Internal Medicine Pharmacy Resident May, 08 Objectives: Pharmacists Explain the epidemiology, pathophysiology, and risks associated with
Management of Acute Atrial Fibrillation Tanner Moser, PharmD PGY- Internal Medicine Pharmacy Resident May, 08 Objectives: Pharmacists Explain the epidemiology, pathophysiology, and risks associated with
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Modern management of atrial fibrillation, from blood pressure control to anticoagulation
 Modern management of atrial fibrillation, from blood pressure control to anticoagulation Adel Khalifa S. Hamad, BMS, MD, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist
Modern management of atrial fibrillation, from blood pressure control to anticoagulation Adel Khalifa S. Hamad, BMS, MD, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist
Atrial Fibrillation and Heart failure
 Atrial Fibrillation and Heart failure and a bit about anticoagulation Tim Sutton, Consultant Cardiologist Middlemore Hospital, Manukau City and Auckland Heart Group Why Does AF Cause Heart Failure Impaired
Atrial Fibrillation and Heart failure and a bit about anticoagulation Tim Sutton, Consultant Cardiologist Middlemore Hospital, Manukau City and Auckland Heart Group Why Does AF Cause Heart Failure Impaired
Management of Atrial Fibrillation in the Hospitalized Patient
 Management of Atrial Fibrillation in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research:
Management of Atrial Fibrillation in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research:
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT
 AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
Management of atrial fibrillation a holistic view - Prof. Dr. Martin Borggrefe Mannheim
 a holistic view - Prof. Dr. Martin Borggrefe Mannheim Patients with atrial fibrillation (millions) 16 14 12 10 8 6 4 2 0 Management of atrial fibrillation Expected prevalence of apparent AF 5,1 5,1 5,9
a holistic view - Prof. Dr. Martin Borggrefe Mannheim Patients with atrial fibrillation (millions) 16 14 12 10 8 6 4 2 0 Management of atrial fibrillation Expected prevalence of apparent AF 5,1 5,1 5,9
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Atrial Fibrillation. Epidemiology. Goals 11/12/2012. Faithful marker for age and underlying cardiopulmonary disease
 Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
ESC. Update of the ESC Guidelines on Medical Therapy. John Camm. ICM Internationales Congress Center München
 ESC 2012 ICM Internationales Congress Center München Update on Consensus Statements on Management of Atrial Fibrillation European Heart Rhythm Association Update of the ESC Guidelines on Medical Therapy
ESC 2012 ICM Internationales Congress Center München Update on Consensus Statements on Management of Atrial Fibrillation European Heart Rhythm Association Update of the ESC Guidelines on Medical Therapy
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
Atrial Fibrillation in the Emergency Department
 Atrial Fibrillation in the Emergency Department Disclosures Edward Jauch, MD MS Research support National Institutes of Health funding (multiple trials) Novo Nordisk (drug in kind) STOP-IT Study Genentech
Atrial Fibrillation in the Emergency Department Disclosures Edward Jauch, MD MS Research support National Institutes of Health funding (multiple trials) Novo Nordisk (drug in kind) STOP-IT Study Genentech
Innovations in AF Management
 Innovations in AF Management Barry Boilson MD PhD FRCPI boilson.barry@mayo.edu Disclosures Relevant None financial relationship(s) with industry None Off Label Usage None Overview Mechanisms of AF AF as
Innovations in AF Management Barry Boilson MD PhD FRCPI boilson.barry@mayo.edu Disclosures Relevant None financial relationship(s) with industry None Off Label Usage None Overview Mechanisms of AF AF as
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Atrial Fibrillation Ablation: in Whom and How
 Update on Consensus Statement on Management of Atrial Fibrillation: EHRA 2012 Atrial Fibrillation Ablation: in Whom and How Update of HRS/EHRA AF/ECAS Ablation Document 2012 Anne M Gillis MD FHRS Professor
Update on Consensus Statement on Management of Atrial Fibrillation: EHRA 2012 Atrial Fibrillation Ablation: in Whom and How Update of HRS/EHRA AF/ECAS Ablation Document 2012 Anne M Gillis MD FHRS Professor
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution
 Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
AF review. Petr Polasek
 AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Saudi Heart Association February 22, 2011
 Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation
 Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Polypharmacy - arrhythmic risks in patients with heart failure
 Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Aims. AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies
 in non-valvular AF (NVAF) Practical Issues Patient Case Studies") Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies AF and Stroke AF prevalence approx doubles with each
Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies AF and Stroke AF prevalence approx doubles with each
Show Me the Outcomes!
 Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
Atrial Fibrillation 2009
 Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Atrial Fibrillation Cases. Dr Paul Broadhurst Consultant Cardiologist
 Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Defining Sub-Clinical Atrial Fibrillation and its management
 Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
ABLATION OF CHRONIC AF
 ABLATION OF CHRONIC AF A PISAPIA ST JOSEPH HOSPITAL MARSEILLE MEET 2008 Atrial Fibrillation The most common significant heart rhythm disturbance Incidence increases with age and the development of structural
ABLATION OF CHRONIC AF A PISAPIA ST JOSEPH HOSPITAL MARSEILLE MEET 2008 Atrial Fibrillation The most common significant heart rhythm disturbance Incidence increases with age and the development of structural
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
12 월 1 일 EP conference
 12 월 1 일 EP conference Classification ( ACC/AHA/ESC ) Paroxysmal : start and stop by themselves, lasting less than 24hrs sometimes lasting up to 7days Persistent : lasting more than 7 days or that requre
12 월 1 일 EP conference Classification ( ACC/AHA/ESC ) Paroxysmal : start and stop by themselves, lasting less than 24hrs sometimes lasting up to 7days Persistent : lasting more than 7 days or that requre
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation
 The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
AF in Andrew Staniforth. Mayo Course March 2014
 AF in 2014 Andrew Staniforth Mayo Course March 2014 European Heart Journal 2010; 31: 2369 2429 www escardio.org/guidelines Q1 (Indications for anticoagulation) For stroke prevention in AF, which of the
AF in 2014 Andrew Staniforth Mayo Course March 2014 European Heart Journal 2010; 31: 2369 2429 www escardio.org/guidelines Q1 (Indications for anticoagulation) For stroke prevention in AF, which of the
Stroke Prevention & Atrial Fibrillation. Susanne Christie Arrhythmia Nurse Specialist 24 th September 2015
 Stroke Prevention & Atrial Fibrillation Susanne Christie Arrhythmia Nurse Specialist 24 th September 2015 Learning Outcomes What is Atrial Fibrillation? Why is Atrial Fibrillation important? What causes
Stroke Prevention & Atrial Fibrillation Susanne Christie Arrhythmia Nurse Specialist 24 th September 2015 Learning Outcomes What is Atrial Fibrillation? Why is Atrial Fibrillation important? What causes