Challenges in RAASi optimization: Hyperkalemia Management Bertram Pitt, M.D.* University of Michigan School of Medicine
|
|
|
- Alfred Cobb
- 6 years ago
- Views:
Transcription

1 Challenges in RAASi optimization: Hyperkalemia Management Bertram Pitt, M.D.* University of Michigan School of Medicine *Consultant: Bayer, Merck, Relypsa+, Pfizer, Astra Zeneca, Boehringer Ingelheim, Forrest Laboratories, SC Pharmaceuticals+, KPB biosciences+, PharMain+, Tricida+, Aurasence+, DaVinci Therapeutics+, Sarfez, Stealth Peptides +Stock options

2 A case of hyperkalaemia during RAASi use 78-year old female 6 years history of severe heart failure with reduced ejection fraction post AMI Chronic AF rate ~65/min Blood pressure: 124/72 mmhg Renal function and electrolytes: egfr: 45 ml/min/1.73 m 2, Na mmol/l, K mmol/l (was 4.8 mmol/l before Spironolactone) Treatment: Perindopril 4 mg od; furosemide 80 mg od; bisoprolol 5 mg od; warfarin 2 mg od; atorvastatin 20 mg od; spironolactone 50 mg od What would you do? Stop spironolactone? Reduce dose of spironolactone? Something else?
 ARNi to replace ACEi Yes Therapy")
 Still symptomatic and LVEF 35%")

3 Patient s treatment in line with ESC HFrEF guidelines 2016 Patient with symptomatic HFrEF Class I Diuretics to relieve symptoms and signs of congestion If LEVF 35% despite OMT or a history of symptomatic VT/NF, implant ICD Able to tolerate ACEi (ARB) ARNi to replace ACEi Yes Therapy with ACEi and beta-blocker (Up-titrate to maximum tolerated evidence-based doses) Consider digoxin or H-ISDN or LVAD, or heart transplantation Yes Still symptomatic and LVEF 35% Yes Add MR antagonist (Up-titrate to maximum tolerated evidence-based dose) Still symptomatic and LVEF 35% Yes Sinus rhythm, QRS duration 130 msec Evaluate need for CRT These above treatments may be combined if included Resistant symptoms No No Sinus rhythm, HR 70 bpm Ivabradine Yes No further action required Consider reducing diuretic dose Class IIa Ponikowski P, et al. Eur Heart J. 2016;37:
4 Adding a mineralocorticoide (MRA) to an ACE improves patient outcomes RALES and EMPHASIS Heart Failure MRA Improved Survival in HF Patients 1. Pitt B, et el. N Engl J Med. 1999; 341: Zannad F, et al. N Engl J Med. 2011; 364:

5 MRA use increases the risk of HK, especially in patients with CKD and a decline in renal function after RAASi initiation Rate of hyperkalaemia (% of patients) RALES study ,0 15,4 Placebo 8,5 25,6 Spironolactone 6,7 18,2 13,3 Baseline egfr 60 Baseline egfr <60 No WRF WRF 30,2 Baseline Renal Function Intra-study Change in Renal Function egfr, estimated glomerular filtration rate; MRA, mineralocorticoid receptor antagonists; WRF, worsening renal function Vardeny O, et al. J Am Coll Cardiol. 2012;60:


6 Hyperkalaemia at hospital admission: CKD and/or RAASi * * Event rate per 100 patient-months ,77 2,30 CKD No RAASi RAASi No CKD *p < versus no CKD Event rate adjusted for: race, gender, age, CCI, cancer, diabetes, CVD, and RAAS blocker treatment within 30 days. CCI, Charlson Comorbidity Index; CKD, chronic kidney disease; CVD, cardiovascular disease; RAASi, renin-angiotensin-aldosterone system inhibitor. Adapted from: Einhorn LM, et al. Arch Intern Med 2009;169:
7 The risk for HK is increased with age and comorbidities 0,9 Comorbid 65 yr 95% Conf Limits Control 65 yr 95% Conf Limits Predicted Probability of Mortality 0,8 0,7 0,6 0,5 0,4 0,3 0,2 0,1 Comorbid yr 95% Conf Limits Normal Range Control yr 95% Conf Limits Adjusted Mortality * by Serum K + Level in Patients 45 to 64 Years and 65 Years With and Without Comorbid Illness 0 2,5 3,0 3,5 4,0 4,5 5,0 5,5 6,0 6,5 7,0 7,5 8,0 Levels of Serum Potassium (meq/l) * Evaluated through de-identified medical records ( ) of individuals with 2 meq/l serum K + readings (Humedica, Cambridge, MA). Spline analyses were performed to assess mortality at 0.1 meq/l increments of serum K + after adjusting for covariates and interactions. Comorbid patients are those with diabetes, heart failure, CKD stages 3-5, cardiovascular disease, or hypertension. Pitt B, et al. AHA
 Nature Reviews Nephrology 6, 245-246 (May 2010) Robert W.")
8 The risk of HK is limiting RAASi use An extensive study of patients with CKD or heart failure who were treated with RAAS inhibitors revealed an incidence of hyperkalemia of 5 10% (Weir, M & Rolfe, M. Clin. J. Am. Soc. Nephrol. 5, ; 2010) Nature Reviews Nephrology 6, (May 2010) Robert W. Schrier 8

9 European healthcare professionals are withholding RAASi due to HK M Komajda, SD, et al. Eur J Heart Fail. 2016;18:
10 PARADIGM-HF study: Despite novel approaches to RAASi therapy, hyperkalaemia is still an issue with ARNIs PARADIGM-HF selected a population at low risk for hyperkalemia prior to randomization Excluded patients with egfr <30 ml/min/1.73 m 2 Excluded patients with a serum [K + ] of more than 5.2 meq/l at screening (or >5.4 meq/l at randomization) Had a run-in phase on ACEi that excluded 6% of patients due to AEs, then a run-in phase on LCZ-696 that excluded another 6% of patients due to AEs, which selected a population that would be at low risk for hyperkalaemia But hyperkalaemia rates remained high despite a carefully selected population >5.5 meq/l: 16.1% LCZ-696 vs 17.3% ACEi (P=0.15) >6.0 meq/l: 4.3% LCZ-696 vs 5.6% ACEi (P=0.007) 1 meq/l = 1 mmol/l AE, adverse event; ACEi, angiotensin converting enzyme inhibitor; CKD, chronic kidney disease; egfr, estimated glomerular filtration rate; RAASi, renin-angiotensin-aldosterone system inhibitor ARNI, angiotensin receptor-neprilysin inhibitor McMurray JJ, et al. N Engl J Med. 2014;371:
 14 12 10 8 6 4 2 0 Clinical trials 2 2,5 6 Community-based 12 2 3 4 5 RALES EMPHASIS Shah 2005 Bozkurt 2003 n=822 n=1,336 n=551 n=104 1. Desai AS. Curr Heart Failure Rep.")
11 The incidence of hyperkalaemia in real-world studies far exceeds that seen in clinical trials 1 Hyperkalaemia with spironolactone in real-world vs clinical trials in patients with heart failure Patients (%) Clinical trials 2 2,5 6 Community-based RALES EMPHASIS Shah 2005 Bozkurt 2003 n=822 n=1,336 n=551 n= Desai AS. Curr Heart Failure Rep. 2009;6:272 80; 2.Pitt B, et al. N Engl J Med. 1999;341:709 17; 3. Zannad F, et al. N Engl J Med. 2011;364:11 21; 4. Shah KB, et al. J Am Coll Cardiol. 2005;46:845 49; 5. Bozkurt B, et al. J Am Coll Cardiol. 2003;41:
12 Patients who experience HK once are at greater risk of recurrent HK events ~50% of patients with hyperkalaemia* had 2 or more recurrences within 1 year Some patients experienced >20 recurrent episodes within 1 year HK, hyperkalaemia *Hyperkalaemia was defined as serum [K + ] 5.5 meq/l (1 meq/l = 1 mmol/l); 70 individuals (0.21%) had more than 20 episodes in 1 year Einhorn LM, et al. Arch Intern Med. 2009;169:
13 Hyperkalemia Contributes to ED Visits, Hospitalizations, and Health Care Costs 2011 ED Visits Primary Diagnosis of Hyperkalemia 2011 Hospitalizations Primary Diagnosis of Hyperkalemia ED visits Admitted to hospital from ED Hospitalizations Discharged to another hospital, institution, or home health care ED visits (n) ED visits (n) All patients Medicare members 0 All patients Medicare members In 2011, the estimated total annual hospital charges for Medicare admissions with hyperkalemia as primary diagnosis were ~$697 million Average Medicare LOS was 3.2 days; mean charges of $24,085 per stay One-third were discharged to another short-term hospital, institution, or home health care ED: emergency department, LOS: length of stay. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. Accessed October 21,

14 Hyperkalemia Is a Leading Reason for Not Starting RAASi and the Major Reason for Discontinuation of RAASi in CKD Patients 279 CKD patients Baseline mean GFR was 33.3 ml/min/1.73 m 2 and the serum K + was 4.73 meq/l Patients (%) Hyperkalemia Acute renal injury Renal artery stenosis Hypotension Very low GFR Unknown/other 13,8 Yildirim T, et al. Ren Fail. 2012;34(9): ,6 Reason for Not Starting RAASi Discontinuation of RAASi at Any Time (80 patients) (51 patients) 14
15 Poor monitoring of serum [K + ] levels after the initiation of MRA therapy in real-world studies Evaluation of 10,443 Medicare beneficiaries with heart failure and incident MRA therapy 91.6% of patients had serum [K + ] first measured in the 120 days prior to MRA initiation However, only 13.3% had guideline suggested measurement of serum [K + ] in the early (1 10 days) follow-up period (11 90 days after MRA initiation) Overall, 55% of patients did not receive any monitoring of serum [K + ] in the early postinitiation period and 22.3% did not receive any monitoring of serum [K + ] during the extended follow-up period Regular monitoring of serum [K + ] is needed in clinical practice after patients start MRA therapy MRA, mineralocorticoid receptor antagonist Cooper, LG, et al. JAMA. 2015;314:
16 Guidelines recommend dose reduction or discontinuation if HK is a problem during RAASi therapy >6.0 KDIGO Guidelines do not provide recommendations 4 NICE 5 : Stop RAASi if >6.0 Serum K + (meq/l) >5.5 K/DOQI 6 : don t start RAASi if > 5.0 ESC HF, 2 K/DOQI 6 : Reduce dose of/stop ACEi/ARB, MRA if >5.5 NICE 5 : don t start RAASi if >5.0 HFSA 3 : MRA not recommended >5.0 >5.0 ACA/AHA HF 1 : Maintain AA Serum K + Threshold Before Change in RAASi Guidelines Recommendation 1 Yancy CW, et al. J Am Coll Cardiol June 5 [E-pub ahead of print]. 2 McMurray JJ, et al. Eur Heart J. 2012;33(14): Heart Failure Society of America, Lindenfeld J, et al. J Card Fail. 2010;16(6):e1-e KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3(1). 5 National Institute for Health and Care Excellence (NICE) [UK]. Chronic kidney disease (CG73): Early identification and management of chronic kidney disease in adults in primary and secondary care e
17 Current treatment options for hyperkalaemia: No effective long term option Calcium gluconate salt 1 Hypertonic solution Insulin 1 ᵦ-andrenoreceptor antagonists 1 Membrane stabilization K + redistribution K + elimination Removal / reduction of drugs that serum K + Dialysis 1 SPS/CPS 1 RAASi reduction 2 3 Loop diuretics 1 Sodium bicarbonate 1 Low K + diet 2 Onset of action Therapy Immediate minutes >1 hour >6 hours Maintenance Acute Subacute Chronic Note: SPS, sodium polystyrene sulfonate; CPS, calcium polystyrene sulfonate 1 Weisberg L. Crit Care Med. 2008; 36 (12): Palmer BF, et al. N Engl J Med. 2004;351(6): National Kidney Foundation. Guideline 17


18 Many Patients Are Already on Low Carb and Low Salt: Hyperkalemia Now Adds Potassium Restrictions What s Left to Eat? Track fluid intake Avoid alcohol Limit caffeine Low protein in severe CKD 18
19 Hyperkalemia Loop diuretics are effective in lowering serum potassium However, Loop diuretics are associated with hypochloremia (serum chloride <96 meq/l) resulting in: Diuretic Resistance Renal Dysfunction If persistent 14 days after hospitalization for Acute HF reduced survival Hamberg, J.S. et al Circ Heart Fail, 2016 Ter Maaten, J.M. et al Circ Heart Fail, 2016
20 Hyperkalemia Reducing the dose or discontinuing the use of a RAASi is an effective strategy to reduce serum K + and the clinical consequences of hyperkalemia However discontinuing a RAASi in a patient with HFREF and or CKD places the patient at increased risk of CV death Pitt B, 2016

21 Potassium Lowering Drugs Pitt B, et al. Hyp 2015; 66:731
22 SPS (Kayexalate) and CPS are the only current drugs that remove excess potassium from the body Sodium polystyrene sulfonate was approved for the treatment of hyperkalaemia by the FDA in 1958 and in France in 1980 SPS is a cation-exchange resin that is administered orally or rectally 2 In 2009, the FDA added gastrointestinal safety warnings and precautions to the label 1,2 intestinal necrosis (particularly with concomitant sorbitol) which may be fatal, and other serious gastrointestinal adverse reactions Resin is a source of sodium caution is advised in patients who cannot tolerate increases in sodium load (i.e. severe CHF, severe HTN, marked oedema or renal damage) 2 Not an option for long-term use CHF, congestive heart failure; FDA, Food and Drug Administration; HTN, hypertension; SPS, sodium polystyrene sulfonate SPS sodium polystyrene sulfonate CPS, calcium polystyrene sulfonate 1. Sterns RH, et al. J Am Soc Nephrol. 2010;21:733 35; 2. Kayexalate (sodium polystyrene sulfonate) [Package Insert]. Sanofi-Aventis US LLC, Bridgewater, NJ;
23 Sodium Polystyrene Sulfonate (SPS) SPS removes mg of K + in exchange for 2-3 mg of Na + A single daily dose of SPS contains approximately 60 mg of Na + Administration of SPS to patients with renal failure and hyperkalemia is associated with: Worsening edema Weight gain Poor blood pressure control Nasir, K. et al; J. Ayub Med Coll Abbottabad2014; 26:455 Berlyne, GM et al Lancet 1966; Jan 22:791

24 Patients who benefit the most from RAASi therapy are the patients at greatest risk of hyperkalaemia Catch 22: Hyperkalemia vs RAASi benefits? Prescribe RAASi and accept the presence of hyperkalemia? Discontinue/ down-titrate RAASi and lose the benefits on clinical outcomes? CATCH-22 RAASi, renin-angiotensin-aldosterone system inhibitor Palmer BF, et al. N Engl J Med. 2004;351:

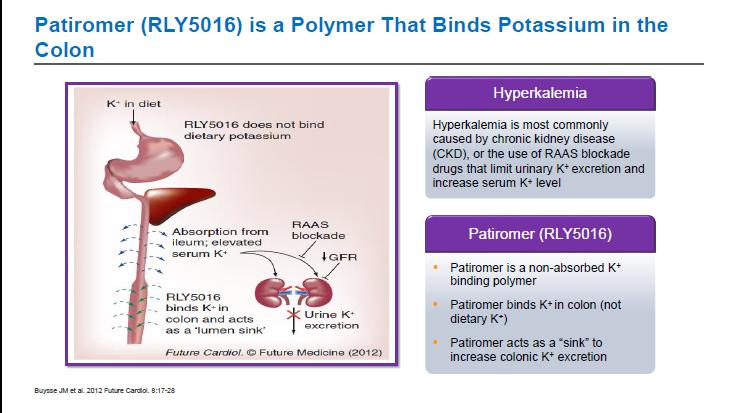
25 ECS Guidelines for heart failure 2016: New option? Two new potassium binders (patiromer and sodium zirconium cyclosilicate) are currently under consideration for regulatory approval. Initial results from patients with HF are available and confirm the efficacy of these therapies in reducing serum potassium and preventing recurrent hyperkalemia in patients with HF and CKD in the context of treatment with RAAS inhibitors. Ponikowski P et al. Rev Esp Cardiol (Engl Ed) Dec;69(12):1167. doi: /j.rec
26
27 K + decreased by 1.01mmol/L, 76% Final K p<0.001 Mean age 64yrs, egfr: 35, K + 5.6mmol/L Weir M et al. NEJM 2015;372: K + rise to 5.5mmol/L: Placebo 60%, Patiromer 15%, p<
28 Primary Endpoint: Mean Change in Serum K+ From Baseline to Week 4 During the Treatment Phase (Part A) Mean (±SE) Serum K + (meq/l) 6,0 5,8 5,6 5,4 5,2 5,0 4,8 4,6 Heart Failure No Heart Failure meq/l 0,0-0,2-0,4-0,6-0,8-1,0-1,2 Treatment Phase Primary Endpoint: Mean Change from Baseline to Week 4 Mean Baseline Serum K + (meql/l) N = HF (95% CI, -1.16, -0.95) p<0.001 No HF (95% CI, -1.06, -0.90) p<0.001 p=0.22 for interaction Secondary endpoint: 76% and 75% of patients with and without HF, respectively, had serum K to < 5.1 meq/l at week 4 4,4 4,2 4,0 0.0 Day Week Week Week Week Baseline Mean (±SE) serum K + change from baseline (meq/l) Heart failure -0.5± ± ± ± ±0.05 No heart failure -0.5± ± ± ± ±0.04 CI: 95% confidence interval; HF: heart failure; K + : potassium; SE: standard error. From Pitt B, et al. Eur J Heart Fail. 2015;17: The Authors, published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology; licensed under a Creative Commons Attribution-NonCommercial-NoDerivs License. 28
29 OPAL-HK Part B: Effect of Continuing Versus Discontinuing Patiromer on Mean Serum Aldosterone Exploratory Endpoint Weir M, et al. Presented at the ASH 2015 Annual Scientific Meeting; New York, NY; May 15-19, Poster LB-1. 29

30 OPAL-HK Part B: Effect of Continuing Versus Discontinuing Patiromer on Mean Serum Systolic and Diastolic BP Weir M, et al. Presented at the ASH 2015 Annual Scientific Meeting; New York, NY; May 15-19, Poster LB-1. 30
 did not have a central lab serum K + value at baseline and")
31 AMETHYST-DN: Least Squares Mean (95% CI) Serum K+ Levels Over 52 Weeks and During Posttreatment Follow-up Compliance throughout the entire study ranged from 86.7% to 95.9% across dose groups and strata All serum K + analyses are based on central lab values; 3 patients (2 with mild HK and 1 with moderate HK) did not have a central lab serum K + value at baseline and therefore are not included in the analysis at this timepoint. * At all timepoints, p<0.001 (2-sided t-test) for lease squares mean changes from baseline and week 52 (or from last dose of patiromer received during the study. BL: baseline, F/Up: followup, HK: hyperkalemia. Bakris G., et al., JAMA 2015; 314:
 and on 1 ACEi or ARB or βb; OR 2. Documented Hx hyperk + < 6 mo* that led to discontinuation of AA, ACEi or ARB or βb Patiromer 12.")


32 PEARL-HF Study Design Subjects with a history of chronic HF, aged 18 or older, clinically indicated to receive spironolactone with a serum K + at screening between meq/l and: 1. CKD (egfr <60 ml/min) and on 1 ACEi or ARB or βb; OR 2. Documented Hx hyperk + < 6 mo* that led to discontinuation of AA, ACEi or ARB or βb Patiromer 12.6g BID (n 50) No Patiromer Dose Titration in PEARL-HF Spiro 25 mg Spiro 50 mg Placebo (n 50) Day 15 Spiro to 50 mg if K + >3.5 to 5.1 Day 28 1 : Endpoints Mean change in serum K + from BL at Day 28 2 : % of patients with serum K + >5.5 meq/l at any time % of patients eligible for dose titration to Spiro 50 mg ACEi: angiontensin converting enzyme inhibitor, ARB: angiotension receptor blocker, βb: beta blocker, AA: aldosterone antagonist, Hx: history Spiro: spironolactone. Note: In the publication, 15g BID (30g total) is reported which refers to dosing calculation that incorporates the weight of the exchange ion and sorbitol complex; Current dosing reflects the active moiety only where 15g BID = 12.6g BID (25.2g total) * Leading to d/c of RAASi or βb. Pitt B, Anker SD, Bushinsky DA, et al. Eur Heart J. 2011;32(7):
 5.1 4.9 4.")
33 PEARL-HF Primary Efficacy Endpoint: Change From Baseline in Serum K+ (LOCF) by Study Visit Serum K + (meq/l) Patiromer (n=55) Placebo (n=49) P value Baseline Change from baseline <0.001 Difference Patiromer vs placebo <0.001 Spironolactone initiated at 25 mg/d on Day 1 Spironolactone increased to 50 mg/day on Day 15 if K 5.1 LS Mean Serum K + (meq/l) LOCF: last observation carried forward. * ** *P < 0.01 **P < ** Study Day ** ** ** Placebo Patiromer RLY5016 N=49 N=55 Pitt B, Anker SD, Bushinsky DA, et al. Eur Heart J. 2011;32(7):
 36 (74%) 0.019 Pitt B, Anker SD, Bushinsky DA, et al. Eur Heart J. 2011;32(7):820-828.")
34 PEARL-HF Secondary Efficacy Endpoint: Proportion of Subjects Able to Increase Spironolactone Dose to 50 mg/day Patiromer (n=55) Placebo (n=49) p value Subjects able to titrate up spironolactone dose 50 (91%) 36 (74%) Pitt B, Anker SD, Bushinsky DA, et al. Eur Heart J. 2011;32(7):
35 35

36 ZS 9 Sarwar, CMS et al. JACC 2016; 68:1575
37
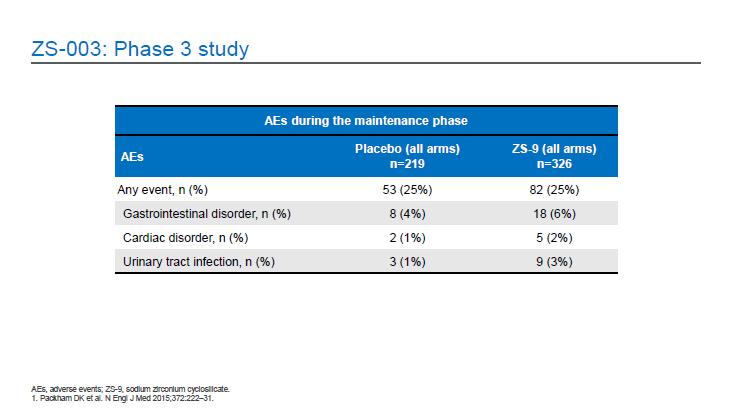
38 ZS9: Tolerability in Heart Failure Patients on RAASi from a Phase 3 Study Incidence of Adverse Events with ZS9 and placebo Acute Maintenance Phase 10g ZS9 Placebo 5g ZS9 10gZS9 15gZS9 N=256 N=85 N=45 N=51 N=56 0 (0) 2 (2:4%) 1 (2.2%) 3(5.9%) 8(14.3%) Peripheral edema Am Soc Nephrol, 2015
39 Potassium Binders: Potential Future Clinical Trials Evaluate their effectiveness in reducing CV events in patients with CKD, DM, HF and or resistant hypertension in whom RAAS-I have been shown to be effective but who have discontinued a RAAS-I due to hyperkalemia Enable the use of RAAS-Is, especially MRAs in patients with an egfr <30->/=15 ml/min/1.73 m2 Prevent the occurrence of hyperkalemia and CV events in patients known to benefit from RAAS-Is but who have not been started due to the fear of inducing hyperkalemia
40 Are Potassium Binders the Solution? Summary/Conclusions Potassium binders are effective in reducing serum potassium and allowing the maintenance or reintroduction of RAASi, especially MRAs in patients with HF and or CKD. The long term effectiveness in reducing CV death vs discontinuing or reducing the dose of a RAASi remaining to be determined. Pitt B, 2017
New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF?
 New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg
New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg
Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure
 Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure Barry Greenberg M.D. Distinguished Professor of Medicine Director, Advanced Heart Failure Treatement Program University of California,
Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure Barry Greenberg M.D. Distinguished Professor of Medicine Director, Advanced Heart Failure Treatement Program University of California,
Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia.
 Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia. PP-US-DSE-00032. 2015 Relypsa, Inc. All rights reserved. Relypsa and
Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia. PP-US-DSE-00032. 2015 Relypsa, Inc. All rights reserved. Relypsa and
Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld
 Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld andreas.kistler@stgag.ch www.nephrologie-thurgau.ch Mr. Hyper K. Lemia charged with serial murder Bild entfernt (copyright)
Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld andreas.kistler@stgag.ch www.nephrologie-thurgau.ch Mr. Hyper K. Lemia charged with serial murder Bild entfernt (copyright)
New Approaches for Treating Hyperkalemia: Why, When and How?
 New Approaches for Treating Hyperkalemia: Why, When and How? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor of Medicine Director,
New Approaches for Treating Hyperkalemia: Why, When and How? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor of Medicine Director,
Conflict of interest
 Hyperkalemia in Heart and Kidney patients: Rescue is here Wajeh Qunibi, MD, FACP Professor of Medicine University of Texas Health Science Center San Antonio, TX CARDIORENAL CONNECTION April 28, 2017 Conflict
Hyperkalemia in Heart and Kidney patients: Rescue is here Wajeh Qunibi, MD, FACP Professor of Medicine University of Texas Health Science Center San Antonio, TX CARDIORENAL CONNECTION April 28, 2017 Conflict
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Giovambattista Desideri UO Geriatria Università dell Aquila. Iperkaliema e sideropenia nello scompenso cardiaco
 Giovambattista Desideri UO Geriatria Università dell Aquila Iperkaliema e sideropenia nello scompenso cardiaco Kaplan Meier curves for overall survival in (A) men or (B) women with diffrent cancero or
Giovambattista Desideri UO Geriatria Università dell Aquila Iperkaliema e sideropenia nello scompenso cardiaco Kaplan Meier curves for overall survival in (A) men or (B) women with diffrent cancero or
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
PP-US-DSE Relypsa, Inc. All rights reserved. Relypsa and the Relypsa logo are trademarks of Relypsa, Inc.
 1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Cardiovascular Pharmacotherapy for Heart Failure Management
 Cardiovascular Pharmacotherapy for Heart Failure Management AN UPDATE OF THE LATEST RECOMMENDATIONS AND DATA By: Debby Caraballo, PharmD, PhC, BCPS, AQ-Cardiology Balloon Fiesta Symposium, Albuquerque,
Cardiovascular Pharmacotherapy for Heart Failure Management AN UPDATE OF THE LATEST RECOMMENDATIONS AND DATA By: Debby Caraballo, PharmD, PhC, BCPS, AQ-Cardiology Balloon Fiesta Symposium, Albuquerque,
HYPERKALEMIA. Best Practices in Managing. in Chronic Kidney Disease
 + Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
+ Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia
 Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia Nicholas Wettersten, MD Associate Professor Heart Failure, Mechanical Circulatory Support and Transplant March 1 st,
Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia Nicholas Wettersten, MD Associate Professor Heart Failure, Mechanical Circulatory Support and Transplant March 1 st,
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Développement clinique du Patiromer et futures perspectives
 Développement clinique du Patiromer et futures perspectives Professor Patrick Rossignol Inserm CIC-P 14-33, CHRU de Nancy-University de Lorraine, ALTIR Disclosures consultant: AstraZeneca, Bayer, CTMA,
Développement clinique du Patiromer et futures perspectives Professor Patrick Rossignol Inserm CIC-P 14-33, CHRU de Nancy-University de Lorraine, ALTIR Disclosures consultant: AstraZeneca, Bayer, CTMA,
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much?
 2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart
DECLARATION OF CONFLICT OF INTEREST TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure. Elizabeth Pogge, PharmD, MPH, BCPS, FASCP
 Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 1. To highlight the link between AKI and progression to CKD 2. To discuss the newer agents that have come available for the treatment of hyperkalemia
Jo Abraham MD Division of Nephrology University of Utah 1. To highlight the link between AKI and progression to CKD 2. To discuss the newer agents that have come available for the treatment of hyperkalemia
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
INIBITORI NEPRILISINA
 INIBITORI NEPRILISINA Marco Canepa, MD, PhD Università degli Studi di Genova Cardiologia, Ospedale Policlinico San Martino IRCCS marco.canepa@unige.it ARNI: ANGIOTENSIN RECEPTOR NEPRILYSIN INHIBITORS
INIBITORI NEPRILISINA Marco Canepa, MD, PhD Università degli Studi di Genova Cardiologia, Ospedale Policlinico San Martino IRCCS marco.canepa@unige.it ARNI: ANGIOTENSIN RECEPTOR NEPRILYSIN INHIBITORS
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE. Marc Ferrini (Lyon Fr)
") What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC
 Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Faiez Zannad. Institut Lorrain du Coeur et des Vaisseaux. CIC - Inserm
 Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Practical considerations for the use of ARNI in CHF: clinical cases. J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece
 Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists
 I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
OPTIMISING RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITOR THERAPY IN HEART FAILURE AND RESISTANT HYPERTENSION: CHALLENGES AND SOLUTIONS
 OPTIMISING RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITOR THERAPY IN HEART FAILURE AND RESISTANT HYPERTENSION: CHALLENGES AND SOLUTIONS This Lorraine University organised, educational event took place
OPTIMISING RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITOR THERAPY IN HEART FAILURE AND RESISTANT HYPERTENSION: CHALLENGES AND SOLUTIONS This Lorraine University organised, educational event took place
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
REVIEW ARTICLE. Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2
 Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2 1 University of Missouri School of Medicine, Columbia, MO 2 Division of Cardiovascular Medicine, Department
Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2 1 University of Missouri School of Medicine, Columbia, MO 2 Division of Cardiovascular Medicine, Department
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Faculty. Therapeutic Advances in Hyperkalemia. Disclosures. Learning Objectives 9/7/2018. A Pharmacist s Guide to Patient Identification and Treatment
 Faculty Therapeutic Advances in Hyperkalemia Darren W. Grabe, BS, PharmD Associate Professor of Pharmacy Practice Chair, Department of Pharmacy Practice School of Pharmacy and Pharmaceutical Sciences Albany
Faculty Therapeutic Advances in Hyperkalemia Darren W. Grabe, BS, PharmD Associate Professor of Pharmacy Practice Chair, Department of Pharmacy Practice School of Pharmacy and Pharmaceutical Sciences Albany
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients
 Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients Javed Butler, MD, MPH, MBA Patrick H. Lehan Professor of Medicine Professor of Physiology Chairman,
Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients Javed Butler, MD, MPH, MBA Patrick H. Lehan Professor of Medicine Professor of Physiology Chairman,
Sacubitril/Valsartan unter der Lupe Subgruppenanalysen, real world data,
 Sacubitril/Valsartan unter der Lupe Subgruppenanalysen, real world data, praktische Erfahrungen michael.boehm@uks.eu M. Böhm Innere Medizin III (Kardiologie / Angiologie / Internistische Intensivmedizin)
Sacubitril/Valsartan unter der Lupe Subgruppenanalysen, real world data, praktische Erfahrungen michael.boehm@uks.eu M. Böhm Innere Medizin III (Kardiologie / Angiologie / Internistische Intensivmedizin)
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd
 SMC No. (793/12) Pfizer Ltd") eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd 08 June 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS Boards
eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd 08 June 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS Boards
Heart Failure. Guillaume Jondeau Hôpital Bichat, Paris, France
 Heart Failure Guillaume Jondeau Hôpital Bichat, Paris, France Epidemiology Importance of PEF Europe I-PREFER study. Abstract: 2835 Prevalence of HF Preserved LV systolic Function older (65 vs 62 y, p
Heart Failure Guillaume Jondeau Hôpital Bichat, Paris, France Epidemiology Importance of PEF Europe I-PREFER study. Abstract: 2835 Prevalence of HF Preserved LV systolic Function older (65 vs 62 y, p
WHAT S NEW IN HEART FAILURE
 WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Contemporary Advanced Heart Failure Therapy
 Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Management of chronic heart failure: update J. Parissis Attikon University Hospital
 Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
SUPPLEMENT TO FIRST REPORT
 SUPPLEMENT TO ManagedCare FIRST REPORT PRODUCT BULLETIN This supplement was funded and developed in part, by Relypsa, Inc. MAY 2016 Hyperkalemia, or high potassium, is a potentially lifethreatening condition
SUPPLEMENT TO ManagedCare FIRST REPORT PRODUCT BULLETIN This supplement was funded and developed in part, by Relypsa, Inc. MAY 2016 Hyperkalemia, or high potassium, is a potentially lifethreatening condition
Beta-blockers in heart failure: evidence put into practice
 Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
VELTASSA (patiromer) oral suspension
 oral suspension") VELTASSA (patiromer) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
VELTASSA (patiromer) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Disclosures for Presenter
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Heart Failure with Reduced EF. Dino Recchia, MD, FACC, FHFSA
 Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure. Disclosures. Objectives: 8/28/2017. This is not a virus. It doesn t go away. none
 Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Bruce Spinowitz, M.D. FACP
 Bruce Spinowitz, M.D. FACP Associate Director, Nephrology Vice Chairman, Medicine New York Hospital Queens Clinical Professor of Medicine Weill Medical College of Cornell University McDonough et al. Am
Bruce Spinowitz, M.D. FACP Associate Director, Nephrology Vice Chairman, Medicine New York Hospital Queens Clinical Professor of Medicine Weill Medical College of Cornell University McDonough et al. Am
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
2/3/2017. Objectives. Effective Heart Failure Management through Evidence Based Practice and Innovation
 Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
9/10/ , American Heart Association 2
 Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion
 Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion Professor Dr. med. Roger Hullin Leiter Programm für Schwere Herzinsuffizienz, VAD & Herztransplantation Suisse Romande Klinik
Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion Professor Dr. med. Roger Hullin Leiter Programm für Schwere Herzinsuffizienz, VAD & Herztransplantation Suisse Romande Klinik
Heart Failure and Renal Disease Cardiorenal Syndrome
 Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Scientific conclusions and detailed explanation of the scientific grounds for the differences from the PRAC recommendation
 Annex I Scientific conclusions, grounds for variation to the terms of the marketing authorisations and detailed explanation of the scientific grounds for the differences from the PRAC recommendation 1
Annex I Scientific conclusions, grounds for variation to the terms of the marketing authorisations and detailed explanation of the scientific grounds for the differences from the PRAC recommendation 1
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Sodium and HF: Myth?
 Sodium and HF: Myth? Ileana L. Piña, MD, MPH, FACC Professor of Medicine and Epidemiology/Population Health Albert Einstein College of Medicine Associate Chief for Academic Affairs Cardiology Montefiore-Einstein
Sodium and HF: Myth? Ileana L. Piña, MD, MPH, FACC Professor of Medicine and Epidemiology/Population Health Albert Einstein College of Medicine Associate Chief for Academic Affairs Cardiology Montefiore-Einstein
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Evaluation of the Treatment Gap Between Clinical Guidelines and the Utilization of Renin-Angiotensin- Aldosterone System Inhibitors
 n REPORT n Evaluation of the Treatment Gap Between Clinical Guidelines and the Utilization of Renin-Angiotensin- Aldosterone System Inhibitors Murray Epstein, MD; Nancy L. Reaven, MA; Susan E. Funk, MBA;
n REPORT n Evaluation of the Treatment Gap Between Clinical Guidelines and the Utilization of Renin-Angiotensin- Aldosterone System Inhibitors Murray Epstein, MD; Nancy L. Reaven, MA; Susan E. Funk, MBA;
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
Mihai Gheorghiade MD
 Mihai Gheorghiade MD Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, Chicago, Illinois On behalf of: Stephen J Greene MD; Javed Butler MD MPH MBA; Gerasimos Filippatos
Mihai Gheorghiade MD Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, Chicago, Illinois On behalf of: Stephen J Greene MD; Javed Butler MD MPH MBA; Gerasimos Filippatos
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events
 Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine
 Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Highlight Session Heart failure and cardiomyopathies Michel KOMAJDA Paris France
 Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
New Winners in the World of Heart Failure. Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015
 New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure