Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld
|
|
|
- Everett Nash
- 5 years ago
- Views:
Transcription
1 Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld andreas.kistler@stgag.ch
2 Mr. Hyper K. Lemia charged with serial murder Bild entfernt (copyright)


3 Internal and external K + -balance Total bodyk + : 98% intracellular 2% extracellular Plasma: 20 mmol Normal extracellular K: mmol/l Range: mmol/d From: Giebisch et al. In: Medical Physiology 2017
4 Mechanisms leading to hyperkalemia Excess potassium intake Nutrition Potassium supplements Reduced potassium excretion Impaired renal function Impaired aldosterone secretion or action: - Renin-angiotensin-aldosterone system (RAAS) inhibitors - Adrenal insufficiency - Pseudohypoaldosteronism - Hyporeninemic hypoaldosteronism Low distal Na + delivery Potassium redistribution Acidosis Insulin deficiency or resistance Drugs Strenuous exercice Tissue breakdown (tumor lysis, rhabdomyolysis ) Hemolysis
5 Consequences of hyperkalemia Clinical consequences of hyperkalemia are caused by alterations in membrane excitability These consequences may be life-threatening, but symptoms are unspescific and often absent: Neuromuscular: fatigue, weakness, muscle pain or tightness, paresthesias Gastrointestinal: nausea, vomiting Cardiac: palpitations


6 Serum-K + and mortality Predialysis K + and mortailty in HD Time-averaged K + and mortailty in PD K + and mortailty in CKD K + and mortailty in CKD Mean in-hospital K + and mortality after MI Community-based K + and mortality Kovesdy, CJASN 2007 Torlen, CJASN 2012 Nakhoul, Am J Nephrol 2015 Einhorn, Arch Int Med 2009 Goyal, JAMA 2012 Hughes-Austin, CJASN 2017
7 Serum-K + and mortality Hyperkalemia is associated with higher mortality across a spectrum of diseases But: association = causality? Clinical consequences of hyperkalemia depend not only on the K + -level, but: rapidity of onset presence of concomitant electrolyte abnormalities Medications other comorbidities Hence, there is no clear cut off for a critically elevated an also no upper limit for a safe K + -level!


8 Consequences of hyperkalemia Frequency of ECG changes Montague, CJASN 2008



9 Hyperkalemia: a double-edged sword Direct, potentially deleterious cardiac and neuromuscular effects Hyperkalemia prompts the discontinuation of important medications and healthy nutrition


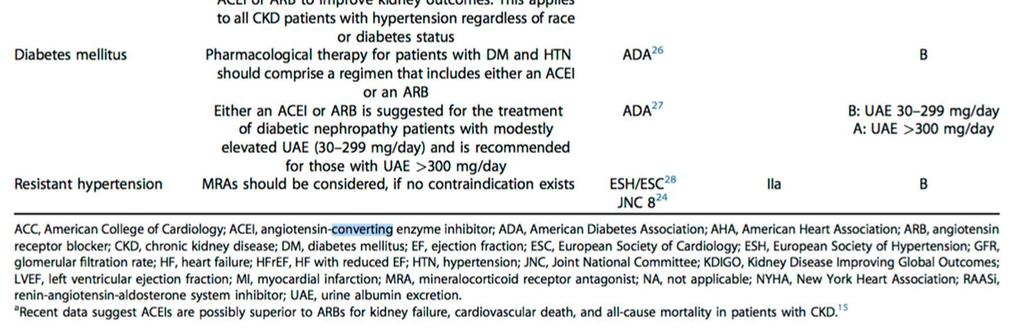
10 Guideline recommendations for RAASi treatment
11 RAASi use in the real world setting Several studies have shown underutilization of RAASi compared to guideline recommendations When RAASi are prescribed, they are often used in submaximal doses
12 Reasons for withholding RAASi therapy ACEi Yes, 66% No, 34% Contraindicated 22.3% Not tolerated 62.5% Reasons Cough 55.9% Hypotension 22.5% Worsening renal function 11.8% Hyperkalaemia 3.9% Other reasons 15.2% ARB Yes, 21.5% No, 78.5% Not indicated 79.1% Contraindicated 6.6 % Not tolerated 6.4% Reasons Hypotension 48.1% Worsening renal function 26.7% Cough 7.2% Hyperkalaemia 5.5% Other reasons 7.9% MRA Yes, 69% No, 31% Not indicated 61.8% Contraindicated 18.9% Not tolerated 14.9% Reasons Renal dysfunction 51.2% Hyperkalaemia 31.4% Gynecomastia 15.3% Other reasons 4.5% Komajda M, et al. Eur J Heart Fail. 2016;18:

13 Reasons for withholding RAASi therapy Hyperkalaemia Acute renal injury Renal artery stenosis Hypotension Very low GFR Unknown/other Discontinuation of RAASi at any time 13.8 Reason for not starting RAASi Yildirim, Ren Fail 2012 Ironically, patientswithriskfactorsforhyperkalemiaarealso thosewhoreceivethegreatestabsolute benefitfromraasi.

14 Hyperkalemia, subsequent RAASi adaptation and mortailty Epstein, Am J Manag Care 2015
15 Hyperkalemia really of concern? RALES: Pitt, NEJM 1999 Spironolactone-Prescription Rate (per 1000 patients) Spironolactone-prescription rate (per 1,000 patients) Online release of RALES Study year Juurlink, NEJM 2004 Rate of administration for hyperkalaemia (per 1000 patients) Rate of admission for hyperkalaemia (per 1,000 patients) Online release of RALES Study year Rate of in-hospital death from hyperkalaemia (per 1,000 patients) Epstein, Kidney Int Suppl 2016 Rate or in-hospital death from HK (per 1000 patients) Online release of RALES Study year
16 Current management of hyperkalemia Potassium redistribution Insulin Glucose Beta-agonists Bicarbonate Facilitate renal potassium excretion Reduce / stop RAASi Loop diuretics Rehydration if volume depleted / less sodium restriction Fludrocortisone Restrict potassium intake Nutritional restrictions Facilitate intestinal potassium excretion Potassium binders Extracorporeal removal Dialysis
17 Potassium-binders available and under evaluation Sodium polystyrene sulfonate (SPS), Resonium Patiromer Calcium Sorbitex, Veltassa Sodium zirconium cyclosilicate, ZS-9 Exchange Ion Na + Ca 2+ Na + Onset of action variable, 2 6 hours 1 7 hours hours 1 Effect duration variable, 6 24 hours hours 3 unclear, 4 12 hours 1 Preparation and administration powder, 15g in 100mL water 2 powder, 8.4/16.8 g in 80mL water, apple juice, cranberry juice 15 powder, 5/10/15 g in 240mL water 1 Dosing 3 4 x daily 2 chronic: 1 x daily with meal 15 subacute: 3 x daily with meal 1 chronic: 1 x daily with meal 1 Setting sub-acute (contraindicated at serum K + < 5.0 mmol/l) 2 chronic (should not replace emergency treatment) 15 subacute or chronic 1 Clinical studies performed 1961: observational study : randomized, single-blind, SPS vs. CPS (3d) : randomized, double-blind, placebo-controlled (7d) 14 RLY : Onset of action (12d) 3 RLY : HD patients (1w) 4 RLY : PEARL (4w) 5 RLY : AMETHYST (52w) 6 RLY : OPAL (12w) 7 RLY : TOURMALINE(4w) 8 ZS-002: Phase II (2/4d) ZS-003: Phase III (3w) 9 ZS-004: HARMONIZE (4w) 10 ZS-005: long-term (52w) 11 Safety profile hypomagnesemia, anemia, edema, nausea, vomiting, constipation, diarrhea, GI tract ulceration or necrosis 2 common: hypomagnesemia, constipation, diarrhea, abdominal pain, flatulence uncommon: nausea, vomiting 15 hypertension, peripheral edema, urinary tract infection, nausea, constipation, anemia, upper respiratory tract infection 11 Availability US: approved since 1958 France: 1980 US: approved since October 2015 EU: approved since July 2017 CH: under review US: under review EU: under review 1. Beccari MV, Meaney CJ. Core Evidence 2017; 12: Fachinformation Resonium, 3. Bushinsky DA, et al. Kidney International 2015;88: Bushinsky DA, et al. Am J Nephrol 2016;44: Pitt B, et al. Eur Heart J 2011;32(7): Bakris G, et al. JAMA 2015;314: Weir MR, et al. N Engl J Med 2015;372(3): Pergola PE, et al. Am J Nephrol 2017;46: Packham DK, et al. N Engl J Med 2015;372(3): Kosiborod M, et al. JAMA 2014;312(21): Fishbane S, et al. ZS-005 data, poster presented at ASN Kidney Week 2017; November 2017; New Orleans, # Scherr L, et al. N Engl J Med 1961;264(39): Nasir K, Ahmad A. J Ayub Med Coll Abbottabad 2014;26(4): Lepage L, et al. Clin J Am Soc Nephrol 2015;10: Patiromer professional information,
18 Conclusions Hyperkalemia is consistently associated with mortality across a wide range of clinical situations Other factors modulate the cardiac toxicity of hyperkalemia and there is no threshold for mortality risk Apart from its direct potentially fatal consequences, hyperkalemia is often responsible for underprescription of RAASi
19 Thank you for your attention
20 Physiological role of K + intracellular Cell volume ph Enzymatic functions extracellular Resting membrane potential Neuromuscular function Cardiac rhythm Vascular tone
21 Mechanisms leading to hyperkalemia Excess potassium intake Nutrition Potassium supplements Potassium redistribution Acidosis Insulin deficiency or resistance Drugs Strenuous exercice Tissue breakdown (tumor lysis, rhabdomyolysis ) Hemolysis Reduced potassium excretion Impaired renal function Impaired aldosterone secretion or action: - Renin-angiotensin-aldosterone system (RAAS) inhibitors - Adrenal insufficiency - Pseudohypoaldosteronism - Hyporeninemic hypoaldosteronism Low distal Na + delivery
Conflict of interest
 Hyperkalemia in Heart and Kidney patients: Rescue is here Wajeh Qunibi, MD, FACP Professor of Medicine University of Texas Health Science Center San Antonio, TX CARDIORENAL CONNECTION April 28, 2017 Conflict
Hyperkalemia in Heart and Kidney patients: Rescue is here Wajeh Qunibi, MD, FACP Professor of Medicine University of Texas Health Science Center San Antonio, TX CARDIORENAL CONNECTION April 28, 2017 Conflict
New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF?
 New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg
New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg
HYPERKALEMIA. Best Practices in Managing. in Chronic Kidney Disease
 + Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
+ Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia
 Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia Nicholas Wettersten, MD Associate Professor Heart Failure, Mechanical Circulatory Support and Transplant March 1 st,
Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia Nicholas Wettersten, MD Associate Professor Heart Failure, Mechanical Circulatory Support and Transplant March 1 st,
PP-US-DSE Relypsa, Inc. All rights reserved. Relypsa and the Relypsa logo are trademarks of Relypsa, Inc.
 1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure
 Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure Barry Greenberg M.D. Distinguished Professor of Medicine Director, Advanced Heart Failure Treatement Program University of California,
Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure Barry Greenberg M.D. Distinguished Professor of Medicine Director, Advanced Heart Failure Treatement Program University of California,
Challenges in RAASi optimization: Hyperkalemia Management Bertram Pitt, M.D.* University of Michigan School of Medicine
 Challenges in RAASi optimization: Hyperkalemia Management Bertram Pitt, M.D.* University of Michigan School of Medicine *Consultant: Bayer, Merck, Relypsa+, Pfizer, Astra Zeneca, Boehringer Ingelheim,
Challenges in RAASi optimization: Hyperkalemia Management Bertram Pitt, M.D.* University of Michigan School of Medicine *Consultant: Bayer, Merck, Relypsa+, Pfizer, Astra Zeneca, Boehringer Ingelheim,
Faculty. Therapeutic Advances in Hyperkalemia. Disclosures. Learning Objectives 9/7/2018. A Pharmacist s Guide to Patient Identification and Treatment
 Faculty Therapeutic Advances in Hyperkalemia Darren W. Grabe, BS, PharmD Associate Professor of Pharmacy Practice Chair, Department of Pharmacy Practice School of Pharmacy and Pharmaceutical Sciences Albany
Faculty Therapeutic Advances in Hyperkalemia Darren W. Grabe, BS, PharmD Associate Professor of Pharmacy Practice Chair, Department of Pharmacy Practice School of Pharmacy and Pharmaceutical Sciences Albany
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
New Approaches for Treating Hyperkalemia: Why, When and How?
 New Approaches for Treating Hyperkalemia: Why, When and How? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor of Medicine Director,
New Approaches for Treating Hyperkalemia: Why, When and How? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor of Medicine Director,
Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia.
 Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia. PP-US-DSE-00032. 2015 Relypsa, Inc. All rights reserved. Relypsa and
Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia. PP-US-DSE-00032. 2015 Relypsa, Inc. All rights reserved. Relypsa and
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 1. To highlight the link between AKI and progression to CKD 2. To discuss the newer agents that have come available for the treatment of hyperkalemia
Jo Abraham MD Division of Nephrology University of Utah 1. To highlight the link between AKI and progression to CKD 2. To discuss the newer agents that have come available for the treatment of hyperkalemia
SUPPLEMENT TO FIRST REPORT
 SUPPLEMENT TO ManagedCare FIRST REPORT PRODUCT BULLETIN This supplement was funded and developed in part, by Relypsa, Inc. MAY 2016 Hyperkalemia, or high potassium, is a potentially lifethreatening condition
SUPPLEMENT TO ManagedCare FIRST REPORT PRODUCT BULLETIN This supplement was funded and developed in part, by Relypsa, Inc. MAY 2016 Hyperkalemia, or high potassium, is a potentially lifethreatening condition
VELTASSA (patiromer) oral suspension
 oral suspension") VELTASSA (patiromer) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
VELTASSA (patiromer) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4:
 Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Lokelma (sodium zirconium cyclosilicate), Veltassa (patiromer)
, Veltassa (patiromer)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.42 Subject: Potassium Binders Page: 1 of 5 Last Review Date: November 30, 2018 Potassium Binders Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.42 Subject: Potassium Binders Page: 1 of 5 Last Review Date: November 30, 2018 Potassium Binders Description
Bruce Spinowitz, M.D. FACP
 Bruce Spinowitz, M.D. FACP Associate Director, Nephrology Vice Chairman, Medicine New York Hospital Queens Clinical Professor of Medicine Weill Medical College of Cornell University McDonough et al. Am
Bruce Spinowitz, M.D. FACP Associate Director, Nephrology Vice Chairman, Medicine New York Hospital Queens Clinical Professor of Medicine Weill Medical College of Cornell University McDonough et al. Am
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
PRODUCT INFORMATION RESONIUM A. Na m
 PRODUCT INFORMATION RESONIUM A NAME OF THE MEDICINE Non-proprietary Name Sodium polystyrene sulfonate Chemical Structure CH - 2 CH SO 3 Na + n CAS Number 28210-41-5 [9003-59-2] CH 2 CH SO - 3 m DESCRIPTION
PRODUCT INFORMATION RESONIUM A NAME OF THE MEDICINE Non-proprietary Name Sodium polystyrene sulfonate Chemical Structure CH - 2 CH SO 3 Na + n CAS Number 28210-41-5 [9003-59-2] CH 2 CH SO - 3 m DESCRIPTION
CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER. The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR
 CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR OUTLINE: A journey through CKD Screening for CKD: The why,
CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR OUTLINE: A journey through CKD Screening for CKD: The why,
Cardiovascular Pharmacotherapy for Heart Failure Management
 Cardiovascular Pharmacotherapy for Heart Failure Management AN UPDATE OF THE LATEST RECOMMENDATIONS AND DATA By: Debby Caraballo, PharmD, PhC, BCPS, AQ-Cardiology Balloon Fiesta Symposium, Albuquerque,
Cardiovascular Pharmacotherapy for Heart Failure Management AN UPDATE OF THE LATEST RECOMMENDATIONS AND DATA By: Debby Caraballo, PharmD, PhC, BCPS, AQ-Cardiology Balloon Fiesta Symposium, Albuquerque,
Medical therapy of AKI complications. Refik Gökmen AKI Academy 18 October 2014
 Medical therapy of AKI complications Refik Gökmen AKI Academy 18 October 2014 Medical therapy of AKI complications Hyperkalaemia Volume status, fluid therapy Acidosis Calcium & phosphate Bleeding risk
Medical therapy of AKI complications Refik Gökmen AKI Academy 18 October 2014 Medical therapy of AKI complications Hyperkalaemia Volume status, fluid therapy Acidosis Calcium & phosphate Bleeding risk
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Développement clinique du Patiromer et futures perspectives
 Développement clinique du Patiromer et futures perspectives Professor Patrick Rossignol Inserm CIC-P 14-33, CHRU de Nancy-University de Lorraine, ALTIR Disclosures consultant: AstraZeneca, Bayer, CTMA,
Développement clinique du Patiromer et futures perspectives Professor Patrick Rossignol Inserm CIC-P 14-33, CHRU de Nancy-University de Lorraine, ALTIR Disclosures consultant: AstraZeneca, Bayer, CTMA,
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
LOKELMA (sodium zirconium cyclosilicate) oral suspension
 oral suspension") LOKELMA (sodium zirconium cyclosilicate) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
LOKELMA (sodium zirconium cyclosilicate) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
SUMMARY OF THE RISK MANAGEMENT PLAN (CH) VELTASSA
 VELTASSA") SUMMARY OF THE RISK MANAGEMENT PLAN (CH) VELTASSA Active Substance: Anatomical Therapeutic Code: MAH or Applicant: Medicinal Product(s) to Which this RMP Refers: Products Concerned (Brand Names): Patiromer
SUMMARY OF THE RISK MANAGEMENT PLAN (CH) VELTASSA Active Substance: Anatomical Therapeutic Code: MAH or Applicant: Medicinal Product(s) to Which this RMP Refers: Products Concerned (Brand Names): Patiromer
keyword: diuretics Drug monitoring Monitoring diuretics in primary care 2 March 2009 best tests
 www.bpac.org.nz keyword: diuretics Drug monitoring Monitoring diuretics in primary care 2 March 2009 best tests Why do we monitor patients taking diuretics and what do we monitor? Monitoring a person on
www.bpac.org.nz keyword: diuretics Drug monitoring Monitoring diuretics in primary care 2 March 2009 best tests Why do we monitor patients taking diuretics and what do we monitor? Monitoring a person on
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Giovambattista Desideri UO Geriatria Università dell Aquila. Iperkaliema e sideropenia nello scompenso cardiaco
 Giovambattista Desideri UO Geriatria Università dell Aquila Iperkaliema e sideropenia nello scompenso cardiaco Kaplan Meier curves for overall survival in (A) men or (B) women with diffrent cancero or
Giovambattista Desideri UO Geriatria Università dell Aquila Iperkaliema e sideropenia nello scompenso cardiaco Kaplan Meier curves for overall survival in (A) men or (B) women with diffrent cancero or
Complications of Acute and Chronic Kidney Disease: A Focus on Hyperkalemia. Mitchell H. Rosner, MD James Tumlin, MD Peter A. McCullough, MD, MPH
 Complications of Acute and Chronic Kidney Disease: A Focus on Hyperkalemia Mitchell H. Rosner, MD James Tumlin, MD Peter A. McCullough, MD, MPH Case #1 A 29 year-old male with ESRD secondary to focal segmental
Complications of Acute and Chronic Kidney Disease: A Focus on Hyperkalemia Mitchell H. Rosner, MD James Tumlin, MD Peter A. McCullough, MD, MPH Case #1 A 29 year-old male with ESRD secondary to focal segmental
COMPOSITION. A film coated tablet contains. Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar (Film coated tablets) Irbesartan
 Irbesartan") Rotazar (Film coated tablets) Irbesartan Rotazar 75 mg, 150 mg, 300 mg COMPOSITION A film coated tablet contains Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar 75 mg, 150 mg, 300 mg PHARMACOLOGICAL
Rotazar (Film coated tablets) Irbesartan Rotazar 75 mg, 150 mg, 300 mg COMPOSITION A film coated tablet contains Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar 75 mg, 150 mg, 300 mg PHARMACOLOGICAL
OPTIMISING RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITOR THERAPY IN HEART FAILURE AND RESISTANT HYPERTENSION: CHALLENGES AND SOLUTIONS
 OPTIMISING RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITOR THERAPY IN HEART FAILURE AND RESISTANT HYPERTENSION: CHALLENGES AND SOLUTIONS This Lorraine University organised, educational event took place
OPTIMISING RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM INHIBITOR THERAPY IN HEART FAILURE AND RESISTANT HYPERTENSION: CHALLENGES AND SOLUTIONS This Lorraine University organised, educational event took place
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
InformRx. Managing Chronic Hyperkalemia. By Pam Scandrett, R.Ph. Risks of High Potassium Levels CLINICAL & REGULATORY NEWS BY PHARMERICA
 Managing Chronic Hyperkalemia By Pam Scandrett, R.Ph. CLINICAL & REGULATORY NEWS BY PHARMERICA JAN/FEB 2019 Potassium (K+) is found inside skeletal muscle, liver, and red blood cells. Normal levels of
Managing Chronic Hyperkalemia By Pam Scandrett, R.Ph. CLINICAL & REGULATORY NEWS BY PHARMERICA JAN/FEB 2019 Potassium (K+) is found inside skeletal muscle, liver, and red blood cells. Normal levels of
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
K+ Ann Crawford, RN, PhD, CNS, CEN
 Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart
DECLARATION OF CONFLICT OF INTEREST TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart
Important aspects of acid-base disorders
 Important aspects of acid-base disorders I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Division of Nephrology, Hypertension and Transplantation University of Florida College
Important aspects of acid-base disorders I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Division of Nephrology, Hypertension and Transplantation University of Florida College
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
SUMMARY OF PRODUCT CHARACTERISTICS 2. QUALITATIVE AND QUANTITATIVE COMPOSITION
 SUMMARY OF PRODUCT CHARACTERISTICS PRODUCT SUMMARY 1. NAME OF THE MEDICINAL PRODUCT Sterile Potassium Chloride Concentrate 15%. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 15% of Potassium Chloride in
SUMMARY OF PRODUCT CHARACTERISTICS PRODUCT SUMMARY 1. NAME OF THE MEDICINAL PRODUCT Sterile Potassium Chloride Concentrate 15%. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 15% of Potassium Chloride in
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
CSI (Clinical Scenario Investigation): Hyperkalemia
: Hyperkalemia") CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment. Jamie Johnston, MD University of Pittsburgh School of Medicine
 Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
The first and only FDA-approved lisinopril oral solution for pediatric patients 6 years of age and older. WARNING: FETAL TOXICITY
 MEDICAS DIFFER FROM 5 drug products that are essentially copies of commercially available LIPRIL ORAL AF IMPORAN SAFEY INA WARNING: FEAL OXIC 5 drug products that are essentially copies of commercially
MEDICAS DIFFER FROM 5 drug products that are essentially copies of commercially available LIPRIL ORAL AF IMPORAN SAFEY INA WARNING: FEAL OXIC 5 drug products that are essentially copies of commercially
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Outpatient Management of Chronic Kidney Disease for the Internist
 Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1
 Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1 Not an actual Parsabiv vial. The displayed vial is for illustrative
Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1 Not an actual Parsabiv vial. The displayed vial is for illustrative
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
FULL DISCLOSURE POLICY AFFECTING CPE ACTIVITIES
 Steering Committee Kristy N. Greene, PharmD, BCPS, BCCCP Clinical Pharmacist Specialist Neuroscience Critical Care Medicine Emory University Hospital Midtown Atlanta, Georgia Kelly Harbourt, PharmD, BCPS,
Steering Committee Kristy N. Greene, PharmD, BCPS, BCCCP Clinical Pharmacist Specialist Neuroscience Critical Care Medicine Emory University Hospital Midtown Atlanta, Georgia Kelly Harbourt, PharmD, BCPS,
0BCore Safety Profile. Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg SE/H/PSUR/0024/003 Date of FAR:
/strength: Film-coated tablet 40, 80, 160, 320 mg SE/H/PSUR/0024/003 Date of FAR:") 0BCore Safety Profile Active substance: Valsartan Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg P-RMS: SE/H/PSUR/0024/003 Date of FAR: 28.02.2013 4.2 Posology and method of administration
0BCore Safety Profile Active substance: Valsartan Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg P-RMS: SE/H/PSUR/0024/003 Date of FAR: 28.02.2013 4.2 Posology and method of administration
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events
 Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
The P&T Committee Lisinopril (Qbrelis )
") Situation Background Assessment The P&T Committee Lisinopril (Qbrelis ) Qbrelis, 1 mg/ml lisinopril oral solution, has recently become an FDA- approved formulation. Current practice at UK Chandler Medical
Situation Background Assessment The P&T Committee Lisinopril (Qbrelis ) Qbrelis, 1 mg/ml lisinopril oral solution, has recently become an FDA- approved formulation. Current practice at UK Chandler Medical
Hyperkalemia Protect, Shift, and Eliminate
 Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Should we be moving away from Kayexalate (Sodium Polystyrene Sulfonate)?
?") Should we be moving away from Kayexalate (Sodium Polystyrene Sulfonate)? Shermaine Ngo, LMPS Pharmacy Resident Preceptor: Joanie Tulloch, Emergency Medicine Rotation May 2017 1 Learning Objectives Describe
Should we be moving away from Kayexalate (Sodium Polystyrene Sulfonate)? Shermaine Ngo, LMPS Pharmacy Resident Preceptor: Joanie Tulloch, Emergency Medicine Rotation May 2017 1 Learning Objectives Describe
RENAL TUBULAR ACIDOSIS An Overview
 RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Invokana (canagliflozin) NEW INDICATION REVIEW
 NEW INDICATION REVIEW") Invokana (canagliflozin) NEW INDICATION REVIEW Introduction Brand name: Invokana Generic name: Canagliflozin Pharmacological class: Sodium-glucose cotransporter 2 (SGLT2) inhibitor Strength and Formulation:
Invokana (canagliflozin) NEW INDICATION REVIEW Introduction Brand name: Invokana Generic name: Canagliflozin Pharmacological class: Sodium-glucose cotransporter 2 (SGLT2) inhibitor Strength and Formulation:
Evaluation of the Treatment Gap Between Clinical Guidelines and the Utilization of Renin-Angiotensin- Aldosterone System Inhibitors
 n REPORT n Evaluation of the Treatment Gap Between Clinical Guidelines and the Utilization of Renin-Angiotensin- Aldosterone System Inhibitors Murray Epstein, MD; Nancy L. Reaven, MA; Susan E. Funk, MBA;
n REPORT n Evaluation of the Treatment Gap Between Clinical Guidelines and the Utilization of Renin-Angiotensin- Aldosterone System Inhibitors Murray Epstein, MD; Nancy L. Reaven, MA; Susan E. Funk, MBA;
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Disclaimer Usage Rights:
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current for the date of this live symposium. All materials contained herein reflect the views of the faculty,
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current for the date of this live symposium. All materials contained herein reflect the views of the faculty,
The Parsabiv Beginner s Book
 The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
PRODUCT INFORMATION UROCIT -K. Wax matrix tablets
 PRODUCT INFORMATION UROCIT -K Wax matrix tablets NAME OF DRUG Potassium Citrate CAS number- 6100-05-6 The empirical formula of potassium citrate is K 3 C 6 H 5 0 7.H 2 O, and its structural formula is:
PRODUCT INFORMATION UROCIT -K Wax matrix tablets NAME OF DRUG Potassium Citrate CAS number- 6100-05-6 The empirical formula of potassium citrate is K 3 C 6 H 5 0 7.H 2 O, and its structural formula is:
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults
 NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults Co-ordinators: Medicines Information Pharmacist Consultation Group: See relevant page in guidance Approver: Medicine Guidelines
NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults Co-ordinators: Medicines Information Pharmacist Consultation Group: See relevant page in guidance Approver: Medicine Guidelines
4/26/2016. Chronic Kidney Disease for PCPs CLAIRE KASSAKIAN, MD NORTHWEST RENAL CLINIC ANNUAL PRACTICAL ADVANCES IN IM SYMPOSIUM
 Chronic Kidney Disease for PCPs CLAIRE KASSAKIAN, MD NORTHWEST RENAL CLINIC ANNUAL PRACTICAL ADVANCES IN IM SYMPOSIUM 1 Disclosures None Overview Epidemiology of CKD in 2016 Hope for HCV Treatment in the
Chronic Kidney Disease for PCPs CLAIRE KASSAKIAN, MD NORTHWEST RENAL CLINIC ANNUAL PRACTICAL ADVANCES IN IM SYMPOSIUM 1 Disclosures None Overview Epidemiology of CKD in 2016 Hope for HCV Treatment in the
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Guideline (2010) Chronic Kidney Disease CKD: Executive Summary of Recommendations (2010) Executive Summary of Recommendations Below are the major recommendations
Chronic Kidney Disease Chronic Kidney Disease (CKD) Guideline (2010) Chronic Kidney Disease CKD: Executive Summary of Recommendations (2010) Executive Summary of Recommendations Below are the major recommendations
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to A case of DYSELECTROLYTEMIA. Dr. Prathyusha Dr. Lalitha janakiraman s unit
 A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
578 Index. Eplerenone, 7, 29, 119, 120, 126, 275, 276,
 Index A AC. See Adenylate cyclase (AC) ACEI. See Angiotensin converting enzyme inhibitors (ACEI) Adenosine, 179, 180, 182 184, 191, 196 198 Adenosine A1 receptor, 179 183, 186, 190 198 Adenylate cyclase
Index A AC. See Adenylate cyclase (AC) ACEI. See Angiotensin converting enzyme inhibitors (ACEI) Adenosine, 179, 180, 182 184, 191, 196 198 Adenosine A1 receptor, 179 183, 186, 190 198 Adenylate cyclase
Overview. Fluid & Electrolyte Disorders. Water distribution. Introduction 5/10/2014
 Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
How to deal with hypotension on dialysis? CME Basics in Nephrology SGN-SSN Interlaken 2016
 How to deal with hypotension on dialysis? CME Basics in Nephrology SGN-SSN Interlaken 2016 PD Dr. med. Andreas Kistler Leitender Arzt Nephrologie und Dialyse Kantonsspital Frauenfeld www.spital-thurgau.ch
How to deal with hypotension on dialysis? CME Basics in Nephrology SGN-SSN Interlaken 2016 PD Dr. med. Andreas Kistler Leitender Arzt Nephrologie und Dialyse Kantonsspital Frauenfeld www.spital-thurgau.ch
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
Paediatric Nephrology Date of submission March 2014
 Hyperkalaemia Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline for the assessment and management of hyperkalaemia
Hyperkalaemia Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline for the assessment and management of hyperkalaemia
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Acid-Base Balance Dr. Gary Mumaugh
 Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
Diagnosis and treatment of hyperkalemia
 REVIEW CME CREDIT LEARNING OBJECTIVE: Readers will assess, find the cause of, and treat hyperkalemia BIFF F. PALMER, MD Professor of Internal Medicine, Department of Internal Medicine, University of Texas
REVIEW CME CREDIT LEARNING OBJECTIVE: Readers will assess, find the cause of, and treat hyperkalemia BIFF F. PALMER, MD Professor of Internal Medicine, Department of Internal Medicine, University of Texas
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
A retrospective study of emergency department potassium disturbances: severity, treatment, and outcomes
 Clin Exp Emerg Med 2017;4(2):73-79 https://doi.org/10.15441/ceem.16.194 A retrospective study of emergency department potassium disturbances: severity, treatment, and outcomes Adam J Singer 1, Henry C
Clin Exp Emerg Med 2017;4(2):73-79 https://doi.org/10.15441/ceem.16.194 A retrospective study of emergency department potassium disturbances: severity, treatment, and outcomes Adam J Singer 1, Henry C
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University
 RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34