H. Arjomand, MD, FACC, FSCAI, FSVM Director, Cardiac Cath Lab & Endovascular Medicine Cardiovascular Care of New Hampshire & York Hospital Seacoast
|
|
|
- Matilda Harvey
- 6 years ago
- Views:
Transcription

1


2 H. Arjomand, MD, FACC, FSCAI, FSVM Director, Cardiac Cath Lab & Endovascular Medicine Cardiovascular Care of New Hampshire & York Hospital Seacoast of NH & Southern ME

3 Disclosure Dr. Arjomand does not anticipate discussing unlabeled uses of any commercial product Dr. Arjomand does not anticipate discussing any investigational products Dr. Arjomand has no financial relationships to disclose


4 Philadelphia The Thinker (Rodin Museum)
5 Seacoast of Maine & New Hampshire

6 Seacoast of New Hampshire & Maine Portsmouth, NH, April 01, 2013
7 Outline Antiplatelet therapy in patients undergoing coronary intervention Antithrombotic therapy in patients with venous thromboemblism (VTE) Advanced management of patients with resistant hypertension Endovascular therapy in patients with atrial fibrillation Therapeutic options in patients with valvular heart disease (aortic stenosis)
8 Clinical Case 78 y/o man with history of: Smoking, HTN, Dyslipidemia, TIA, asthma Presents with: Chest pain at rest EKG: Inferior ST-segment depression Lab: elevated troponin: 3.8 Management:: Underwent cardiac cath and PCI/Stenting Was treated with combination antiplatelet therapy



 Aspirin +")
9 Combination Anti-platelet Therapy Current guidelines: One year after PCI/Stenting Drug-eluting stents: minimum one year Bare-metal stent: minimum one month Options: Aspirin + Clopidogrel (Plavix) Aspirin + Prasgurel (Effient) Aspirin + Ticagrelor (Brilinta)

10 CURE Trial: Primary End Point: MI/Stroke/CV Death Cumulative Hazard Rate * In combination with standard therapy Placebo + ASA* Clopidogrel + ASA* Months of Follow-Up The CURE Trial Investigators. N Engl J Med. 2001;345: % 9.3% 20% RRR P < N = 12,562
11 TRITON Trial : Primary Endpoint: CV Death, MI, Stroke 15 Primary Endpoint (%) 10 5 HR 0.77 P= HR 0.80 P= ASA + Clopidogrel ASA + Prasugrel 12.1 (781) 9.9 (643) HR 0.81 ( ) P= NNT= 46 0 ITT= 13,608 LTFU = 14 (0.1%) Days
 10 5 ASA + Ticagrelor 11.58 11.20 ASA + Clopidogrel 2 1 HR 0.84 (95% CI 0.77 0.92), p=0.0003 HR 1.04 (95% CI 0.95 1.13), p=0.434 0 0 No.")
12 PLATO Trial: 13 Primary efficacy endpoint 15 Primary safety endpoint K-M estimated rate (%) ASA + Clopidogrel ASA + Ticagrelor K-M estimated rate (%) 10 5 ASA + Ticagrelor ASA + Clopidogrel 2 1 HR 0.84 (95% CI ), p= HR 1.04 (95% CI ), p= No. at risk Ticagrelor Clopidogrel Months from randomization 9,333 8,628 8,460 9,291 8,521 8,362 8,219 6,743 5,161 4,147 8,124 6,743 5,096 4, Months from randomization 9,235 7,246 6,826 6,545 5,129 3,783 3,433 9,186 7,305 6,930 6,670 5,209 3,841 3,479 K-M = Kaplan-Meier; HR = hazard ratio; CI = confidence interval * Wallentin, L et al., New Eng J Med. 2009;361:
13 Antiplatelet Therapy: Available options: Clopidogrel, Prasugrel, Ticagrelor Factoids to know when choosing antiplatelet therapy: Prasugrel & Ticagrelor: More effective than Clopidogrel More expensive than clopidogrel No direct comparison between Prasugrel & Ticagrelor Contraindicated: Prasugrel: patients with prior TIA/Stroke,?age,?body weight Ticagrelor: patients with asthma and advanced AV block


14 Clinical Case (follow-up): Ischemic chest pain resolved Stopped smoking (reportedly!) Discharged on: Combination anti-platelet therapy ASA + Clopidogrel Anti-Ischemic therapy: Statin Beta Blocker ACE inhibitor
15
16 Clinical Case 56 y/o woman with history of: Smoking and HTN Presents with: SOB and Right lower extremity swelling after a longdistance car travel LE Venous Doppler & MRV (Magnetic Resonance Venous): Right iliofemoral vein thrombosis (DVT) Chest CT: positive for pulmonary embolism (PE) Management: Anticogulation therapy Inpatient vs Outpatient? Regimen? Iv heparin or Enoxaparin + Warfarin or?

17 EINSTEIN PE Trial Study design Randomized, open-label, event-driven, non-inferiority study Up to 48 hours heparins/fondaparinux treatment permitted before study entry 88 primary efficacy outcomes needed Non-inferiority margin: 2.0 Predefined treatment period of 3, 6, or 12 months Day 1 Day 21 Objectively confirmed PE ± DVT N=4833 R Rivaroxaban Rivaroxaban 15 mg bid 20 mg od Enoxaparin bid for at least 5 days, 30-day poststudy treatment period plus VKA INR 2.5 (range ) Primary efficacy outcome: first recurrent VTE Principal safety outcome: first major or non-major clinically relevant bleeding
 Recurrent DVT + PE 0 2 (<0.1) Non-fatal PE 22 (0.9) 19 (0.8) Fatal PE/unexplained death where PE cannot be ruled out 10 (0.4) 6 (0.2) HR 0.75 1.12 1.68* 0 1.00 2.00 Rivaroxaban superior p=0.")
18 EINSTEIN PE Trial: Primary efficacy outcome analysis Rivaroxaban (N=2419) Enoxaparin/VKA (N=2413) n (%) n (%) First symptomatic recurrent VTE 50 (2.1) 44 (1.8) Recurrent DVT 18 (0.7) 17 (0.7) Recurrent DVT + PE 0 2 (<0.1) Non-fatal PE 22 (0.9) 19 (0.8) Fatal PE/unexplained death where PE cannot be ruled out 10 (0.4) 6 (0.2) HR * Rivaroxaban superior p=0.57 for superiority (two-sided) Rivaroxaban non-inferior P= for non-inferiority (one-sided) Rivaroxaban inferior *Potential relative risk increase <68.4%; absolute risk difference 0.24% ( 0.5 to 1.02)
 5 n/n (%) n/n (%) p-value 4 3 249/2412 274/2405 0.90 (0.76 1.07) 2 (10.3) (11.4) p=0.")
19 EINSTEIN PE Trial: Principal safety outcome: major or non-major clinically relevant bleeding Cumulative event rate (%) 15 Enoxaparin/VKA 14 N= Rivaroxaban 8 N= Rivaroxaban Enoxaparin/VKA HR (95% CI) 5 n/n (%) n/n (%) p-value / / ( ) 2 (10.3) (11.4) p= Time to event (days) Number of patients at risk Rivaroxaban Enoxaparin/VKA Safety population
 Enoxaparin/VKA n/n (%) HR (95% CI) p-value Cumulative event rate (%) 2.5 2.0 1.5 1.0 0.5 26/2412 (1.")
 Number of patients at risk Rivaroxaban 2412 2281 2248")
20 EINSTEIN PE Trial: Major bleeding 3.0 Rivaroxaban n/n (%) Enoxaparin/VKA n/n (%) HR (95% CI) p-value Cumulative event rate (%) /2412 (1.1) 52/2405 (2.2) 0.49 ( ) p= Enoxaparin/VKA N=2405 Rivaroxaban N=2412 Safety population Time to event (days) Number of patients at risk Rivaroxaban Enoxaparin/VKA
; p non-inferiority =0.0026 for non-inferiority margin of 2.0 Similar findings for principal safety outcome: HR=0.90 (0.76 1.07); p=0.23 Superiority for major bleeding: HR=0.49 (0.31 0.")
21 EINSTEIN PE Trial: Conclusions In patients with acute symptomatic PE with or without DVT, Rivaroxaban (Xarelto) showed: Non-inferiority to LMWH/VKA for efficacy: HR=1.12 ( ); p non-inferiority = for non-inferiority margin of 2.0 Similar findings for principal safety outcome: HR=0.90 ( ); p=0.23 Superiority for major bleeding: HR=0.49 ( ) p=0.0032

22 Anticoagulation Therapy & PE Available options: Bridge therapy, Warfarin, Xarelto Factoids to consider when choosing anticoagulation therapy: Cost Co-existing diseases:? Mechanical prosthetic valve Concomitant therapy Anti-platelet therapy Adherence with INR testing
23 Clinical Case (follow-up): Due to extensive Right lower extremity thrombosis and leg swelling, patient received inpatient treatment: Treatment with iv heparin and Warfarin Underwent endovascular ultrasoundaccelerated thrombolysis of Right iliofemoral DVT Was discharged home on Warfarin (insurance reasons)
24
25 Clinical Case 71 y/o man with history of: HTN, dyslipidemia, prior stroke Presents with: Suboptimal BP control while on 4 antihypertensive medications Work-up: no evidence of secondary HTN (no renal artery disease, normal serology, ) Management: Available options:? Renal denervation?

:249-258. doi:10.")
26 Renal Denervation for Hypertension J Am Coll Cardiol Intv. 2012;5(3): doi: /j.jcin
:249-258. doi:10.1016/j.jcin.2011.")
27 Renal Denervation for Hypertension Fluoroscopic Images of Catheter Positions in the Renal Artery Radiofrequency catheter positioned in the right renal artery. Contrast injection into the right renal artery. J Am Coll Cardiol Intv. 2012;5(3): doi: /j.jcin
28 Simplicity HTN-2 Trial: Patient disposition Esler M D et al. Circulation 2012;126:

29 Simplicity HTN-2 Trial: Change in office-based blood pressure Esler M D et al. Circulation 2012;126:



30 Simplicity HTN-3 Trial: Patient selection Design: Multi-center, prospective, randomized trial study of Goal: Assess safety and effectiveness of renal denervation in subjects with uncontrolled hypertension Primary outcome: Change in Office Systolic Blood Pressure [ Time Frame: Baseline to 6 months post-randomization Estimated Enrollment: 530 Study Start Date: September 2011 Estimated Primary Completion Date: June 2013 (Final data collection date for primary outcome measure)
31 Eligible Patients for Renal Denervation: Office-based blood pressure >160 mm/hg (>150 mm/hg in patients with type diabetes) Three or more antihypertensive drugs have been used in adequate dosage and combination, including use of a diuretic. Have attempted to modify blood pressure with lifestyle changes. Secondary hypertension has been excluded. Pseudoresistance has been excluded with the use of ambulatory blood-pressure monitoring. Patients have preserved renal function (glomerular filtration rate >45 ml/min/1.732). Absence of polar or accessory arteries, no renal artery stenosis, and no prior renal revascularization.
32
33 Clinical Case 82 y/o man with history of: HTN, gastric ulcer, GI bleeding Presents with: Transient right-sided weakness (Left hemispheric TIA) EKG: atrial fibrillation Echo: normal LV function TEE: clot in left atrial appendage Carotid: mild plaque Management: Anticoagulation? Additional therapy given risk of bleeding with longterm anticoagulation
34 Non-Valvular Atrial Fibrillation Background Lifetime risk of atrial fibrillation in men & women above 40 years old is 1 in 4 Up to 20% of ischemic strokes occur in patients with atrial fibrillation Need for long-term anticoagulation Contraindications to anticoagulation exist in 30-40% of patients Bleeding risk with lifelong anticoagulation

35 Non-Valvular Atrial Fibrillation Stroke Pathology Causes of stroke in atrial fibrillation: Insufficient contraction of left atrial appendage (LAA) leads to stagnant blood flow 90% of thrombus found in LAA embolization of LAA clot leads to stroke TEE-based risk factors Enlarged LAA Reduced inflow and outflow velocities Spontaneous Echo contrast

36 WATCHMAN LAA Closure Technology Fact: 90% of thrombus found in LAA Question: Why NOT Occlude it?
37 PROTECT AF Clinical Trial Design Prospective, randomized study of WATCHMAN LAA Device vs longterm warfarin therapy 2:1 allocation ratio device to control 800 patients enrolled from Feb 2005 to Jun 2008 Device group (463) Control group (244) Roll-in group (93) 59 enrolling centers (U.S. & Europe) Follow-up requirements TEE follow-up at 45 days, 6 months and 1 year Clinical follow-up biannually up to 5 years Regular INR monitoring while taking warfarin Enrollment continues in Continued Access Protocol (CAP Study)
38 Intent-to-Treat PROTECT AF Trial: Primary Efficacy Results Device Control Posterior probabilities Events Total Rate Events Total Rate RR Non- Superiority Cohort (no.) pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) inferiority pt-yr (2.6, 6.7) (3.0, 9.1) (0.39, 1.67) pt-yr (2.1, 5.2) (2.8, 7.6) (0.37, 1.41) Event-free probability patient-year analysis WATCHMAN Control Days Randomization allocation (2 device:1 control) ITT cohort: patients analyzed based on their randomly assigned group (regardless of treatment received)
39 Intent-to-Treat PROTECT AF Trial: Primary Safety Results Device Control Events Total Rate Events Total Rate RR Cohort (no.) pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) 600 pt-yr (8.5, 15.3) (1.9, 7.2) (1.48, 6.43) 900 pt-yr (6.4, 11.3) (2.2, 6.7) (1.18, 4.13) Event-free probability patient-year analysis Device Control Days Randomization allocation (2 device:1 control) ITT cohort: patients analyzed based on their randomly assigned group (regardless of treatment received)
40 Summary Long-term anticoagulation treatment of patients with AF has been found effective, but presents difficulties and risk PROTECT AF trial evaluated the WATCHMAN device compared to warfarin and found: Hemorrhagic stroke risk is significantly lower with the device. When hemorrhage occurred, risk of death was markedly increased All cause stroke and all cause mortality risk are equivalent to that with warfarin There are early safety events, specifically pericardial effusion; these events have decreased over time.
41
42 Clinical Case 69 y/o woman with history of: Smoking, COPD (on home oxygen) Presents with: Syncope Work-up: no arrhythmia/conduction disease, no anemia, no neurologic abnormality Echo: normal LV function, severe aortic stenosis (AS) Management: Treatment of aortic valve disease (AS)
43 Aortic Stenosis Symptoms: SAD Syncope Angina Dyspnea (CHF) Management: Treatment of aortic valve disease (AS) SAVR Surgical Aortic Valve Replacement TAVR Transcatheter Aortic Valve Replacement
 The large vascular access sheath is inserted.")
44 Percutaneous Access and Closure (A) The femoral artery is punctured and a guidewire placed within the artery. Percutaneous sutures are placed using a pre-closure device. (B) The large vascular access sheath is inserted. (C) Following sheath removal the sutures are tightened.
45


 Co-Primary Endpoint: Composite of All-Cause Mortality and Repeat")
46 PARTNER Study Design (Placement of AoRTic TraNscathetER Valve) Symptomatic Severe Aortic Stenosis ASSESSMENT: High-Risk AVR Candidate 3,105 Total Patients Screened N = 699 High Risk Total = 1,057 patients 2 Parallel Trials: Individually Powered Inoperable N = 358 Yes ASSESSMENT: Transfemoral Access No ASSESSMENT: Transfemoral Access Transfemoral (TF) Transapical (TA) Yes No 1:1 Randomization 1:1 Randomization 1:1 Randomization Not In Study N = 244 N = 248 N = 104 N = 103 N = 179 N = 179 TF TAVR VS AVR TA TAVR VS AVR TF TAVR VS Standard Therapy Primary Endpoint: All-Cause Mortality at 1 yr (Non-inferiority) Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority) Co-Primary Endpoint: Composite of All-Cause Mortality and Repeat Hospitalization (Superiority)

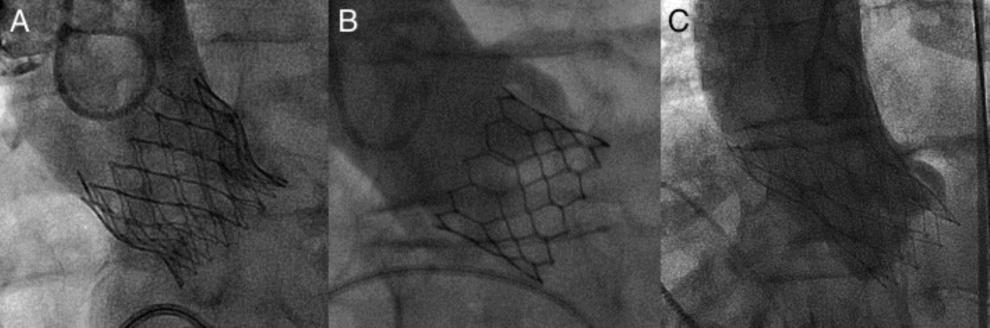
47 Current Status of Transcatheter Aortic Valve Replacement Current Widely Available Transcatheter Valves (A) The Edwards SAPIEN THV balloon-expandable valve (Edwards Lifesciences, Irvine, California) incorporates a stainless steel frame, bovine pericardial leaflets,x and a fabric sealing cuff. (B) The SAPIEN XT THV (Edwards Lifesciences) utilizes a cobalt chromium alloy frame and is compatible with lower profile delivery catheters. ( C) The Medtronic CoreValve (Medtronic, Minneapolis, Minnesota) incorporates a self-expandable frame, porcine pericardial leaflets, and a pericardial seal. J Am Coll Cardiol. 2012;60(6): doi: /j.jacc
48 Transcatheter Aortic Valve Replacement (TAVR): PARTNER 1B Trial The PARTNER 1B Trial Compared Transarterial TAVR to Medical Management in Extremely High-Risk (Inoperable) Patients. Time to event analyses of death (A), death due to cardiac causes (B), rehospitalization (C), and the combined endpoint of death or stroke (D). PARTNER = Placement of AoRTic TraNscathetER Valve. J Am Coll Cardiol. 2012;60(6): doi: /j.jacc
49 Transcatheter Aortic Valve Replacement PARTNER 1A Trial The PARTNER 1A 2-Year Outcomes After Transcatheter or Surgical Aortic Valve Replacement Kaplan-Meier time-to-event curves are shown for death by intention to treat (A) and as-treated (B), stroke (C), and the composite of death or stroke (D). Mortality and stroke rates were similar. Reprinted from Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med 2011;364: , with the permission of the Massachusetts Medical Society. PARTNER = Placement of AoRTic TraNscathetER Valve. J Am Coll Cardiol. 2012;60(6): doi: /j.jacc
![PARTNER 1A Trial All-Cause Mortality (ITT) HR [95% CI] = 0.93 [0.74, 1.15] p (log rank) = 0.483 34.](/docs-images/79/79002588/images/50-3.jpg "6% 44.8% 44.2% 26.8% 33.7% 24.3% No.")
50 PARTNER 1A Trial All-Cause Mortality (ITT) HR [95% CI] = 0.93 [0.74, 1.15] p (log rank) = % 44.8% 44.2% 26.8% 33.7% 24.3% No. at Risk TAVR AVR
51 Conclusions: At 3 years, in patients with symptomatic severe AS who were high-risk candidates for surgical AVR There was no difference in all-cause mortality between TAVR and surgery Baseline predictors of mortality were different for TAVR (e.g. BMI, PVD) and surgery (e.g. STS score, mod/severe MR) Symptom improvement was similar in both groups and maintained thru three years At 3 years, strokes were similar in TAVR and surgery patients, despite increased peri-procedural neurologic events in TAVR patients There was no late (after 30 days) stroke hazard in TAVR compared with surgery
52
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France
 Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France LAA Occlusion Is there a real future? Background Protect AF Trial Other Studies CAP, ASAP, Prevail Left Atrial Appendage
Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France LAA Occlusion Is there a real future? Background Protect AF Trial Other Studies CAP, ASAP, Prevail Left Atrial Appendage
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Is Stroke Frequency Declining?
 Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Oral rivaroxaban versus standard therapy for the acute and continued treatment of symptomatic deep vein thrombosis. The EINSTEIN DVT study.
 Oral rivaroxaban versus standard therapy for the acute and continued treatment of symptomatic deep vein thrombosis. The EINSTEIN DVT study Comments Harald Darius, Berlin Disclosures for Harald Darius Research
Oral rivaroxaban versus standard therapy for the acute and continued treatment of symptomatic deep vein thrombosis. The EINSTEIN DVT study Comments Harald Darius, Berlin Disclosures for Harald Darius Research
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Watchman and Structural update..the next frontier. Ari Chanda, MD Cardiology Associates of Fredericksburg
 Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
PERCUTANEOUS STRUCTURAL UPDATES TAVR WATCHMAN(LEFT ATRIAL APPENDAGE OCCLUDERS) MITRACLIP PARAVALVULAR LEAK REPAIRS ASD/PFO CLOSURES VALVULOPLASTIES
 MITRACLIP PARAVALVULAR LEAK REPAIRS ASD/PFO CLOSURES VALVULOPLASTIES") PERCUTANEOUS STRUCTURAL UPDATES TAVR WATCHMAN(LEFT ATRIAL APPENDAGE OCCLUDERS) MITRACLIP PARAVALVULAR LEAK REPAIRS ASD/PFO CLOSURES VALVULOPLASTIES Dr.Vinny K.Ram No disclosures TAVR 1 Lesson number 1:
PERCUTANEOUS STRUCTURAL UPDATES TAVR WATCHMAN(LEFT ATRIAL APPENDAGE OCCLUDERS) MITRACLIP PARAVALVULAR LEAK REPAIRS ASD/PFO CLOSURES VALVULOPLASTIES Dr.Vinny K.Ram No disclosures TAVR 1 Lesson number 1:
Antithrombotic. DAPT or OAC?
 Antithrombotic treatment after TAVI: DAPT or OAC? Striking the right balance. Pascal Vranckx MD, PhD. Hartcentrum Hasselt, Belgium. Disclosure of Interest Pascal Vranckx has the following potential conflicts
Antithrombotic treatment after TAVI: DAPT or OAC? Striking the right balance. Pascal Vranckx MD, PhD. Hartcentrum Hasselt, Belgium. Disclosure of Interest Pascal Vranckx has the following potential conflicts
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS
 Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Update on Percutaneous Therapies for Structural Heart Disease. William Thomas MD Director of Structural Heart Program Tucson Medical Center
 Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
Left Atrial Appendage Occlusion
 Left Atrial Appendage Occlusion A new strategy to prevent stroke in atrial fibrillation Ashok Talreja MD and Arijit Chanda MD VHVI symposium 24th February 2018 Outline of presentation 1. Risk of stroke
Left Atrial Appendage Occlusion A new strategy to prevent stroke in atrial fibrillation Ashok Talreja MD and Arijit Chanda MD VHVI symposium 24th February 2018 Outline of presentation 1. Risk of stroke
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute
 Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
2/28/2010. Speakers s name: Paul Chiam. I have the following potential conflicts of interest to report: NONE. Antegrade transvenous transseptal route
 Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center
Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center") The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVI After PARTNER-2 : The Hamilton Approach
 TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Dental Management Considerations for Patients on Antithrombotic Therapy
 Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
NON SURGICAL TREATMENT OF CARDIAC DISEASE PETER J SABIA, MD FACC ASSOCIATES IN CARDIOLOGY SILVER SPRING, MARYLAND
 NON SURGICAL TREATMENT OF CARDIAC DISEASE PETER J SABIA, MD FACC ASSOCIATES IN CARDIOLOGY SILVER SPRING, MARYLAND TOPICS ATRIAL SEPTAL DEFECT VSD IHSS PERCUTANEOUS AORTIC VALVE PERCUTANEOUS MITRAL VALVE
NON SURGICAL TREATMENT OF CARDIAC DISEASE PETER J SABIA, MD FACC ASSOCIATES IN CARDIOLOGY SILVER SPRING, MARYLAND TOPICS ATRIAL SEPTAL DEFECT VSD IHSS PERCUTANEOUS AORTIC VALVE PERCUTANEOUS MITRAL VALVE
Left Atrial Appendage Closure: Moving Beyond Blood Thinners to Prevent Stroke in Atrial Fibrillation October 29, 2016
 Left Atrial Appendage Closure: Moving Beyond Blood Thinners to Prevent Stroke in Atrial Fibrillation October 29, 2016 Jesse Jorgensen, MD, FACC Director, Cardiac Cath Lab, Greenville Health System Disclosures
Left Atrial Appendage Closure: Moving Beyond Blood Thinners to Prevent Stroke in Atrial Fibrillation October 29, 2016 Jesse Jorgensen, MD, FACC Director, Cardiac Cath Lab, Greenville Health System Disclosures
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients
 Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study
 Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study Meagan Sullivan, PharmD PGY2 Cardiology Pharmacy Resident University of Chicago Medicine
Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study Meagan Sullivan, PharmD PGY2 Cardiology Pharmacy Resident University of Chicago Medicine
Aortic Stenosis: Open vs TAVR vs Nothing
 Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Bioprosthetic Mitral Valve Dysfunction: Innovation and Evolution of a New Therapeutic Technique
 Bioprosthetic Mitral Valve Dysfunction: Innovation and Evolution of a New Therapeutic Technique Charanjit S. Rihal MD MBA Professor and Chair Division of Cardiovascular Diseases Mayo Clinic DISCLOSURES
Bioprosthetic Mitral Valve Dysfunction: Innovation and Evolution of a New Therapeutic Technique Charanjit S. Rihal MD MBA Professor and Chair Division of Cardiovascular Diseases Mayo Clinic DISCLOSURES
Embolic Protection Devices for Transcatheter Aortic Valve Replacement
 Embolic Protection Devices for Transcatheter Aortic Valve Replacement James M. McCabe, MD Medical Director, Cardiac Cath Lab University of Washington Seattle, WA Disclosures Proctoring and honoraria for
Embolic Protection Devices for Transcatheter Aortic Valve Replacement James M. McCabe, MD Medical Director, Cardiac Cath Lab University of Washington Seattle, WA Disclosures Proctoring and honoraria for
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D.
 Charles T. Klodell, M.D.") Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Integrating Innovative Technologies into the Care of Cardiac Patients
 Integrating Innovative Technologies into the Care of Cardiac Patients Marc J. Semigran MD Medical Director, Heart Failure & Cardiac Transplantation MGH Associate Professor Harvard Medical School Presenter
Integrating Innovative Technologies into the Care of Cardiac Patients Marc J. Semigran MD Medical Director, Heart Failure & Cardiac Transplantation MGH Associate Professor Harvard Medical School Presenter
Update interventional Cardiology Hans Rickli St.Gallen
 Update interventional Cardiology 2012 Hans Rickli St.Gallen 26.11.2012 Review of Literature ESC-Highlights TCT/AHA-Highlights Update interventional cardiology 2012 Structural Heart Disease Transcatheter
Update interventional Cardiology 2012 Hans Rickli St.Gallen 26.11.2012 Review of Literature ESC-Highlights TCT/AHA-Highlights Update interventional cardiology 2012 Structural Heart Disease Transcatheter
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
TCT mdbuyline.com Clinical Trial Results Summary
 TCT 2012 Clinical Trial Results Summary FAME2 Trial: FFR (fractional flow reserve) guided PCI in all target lesions Patients with significant ischemia, randomized 1:1 Control arm: not hemodynamically significant
TCT 2012 Clinical Trial Results Summary FAME2 Trial: FFR (fractional flow reserve) guided PCI in all target lesions Patients with significant ischemia, randomized 1:1 Control arm: not hemodynamically significant
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Watchman a Stroke Prevention Technology for Patients with Atrial Fibrillation
 Watchman a Stroke Prevention Technology for Patients with Atrial Fibrillation Scripps hospital,la Jolla, CA Atrial fibrillation is a major source of cardiogenic embolic related stroke 500,000 strokes per
Watchman a Stroke Prevention Technology for Patients with Atrial Fibrillation Scripps hospital,la Jolla, CA Atrial fibrillation is a major source of cardiogenic embolic related stroke 500,000 strokes per
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원
 Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015
 in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015") Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Prostate Biopsy Alerts
 Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON
 THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
Atrial Fibrillation Topics for Today. Clinical Controversies Management of Atrial Fibrillation. Atrial Fibrillation in the ER Topics for Today
 Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Transcatheter Aortic Valve Replacement TAVR
 Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
Update on Oral Anticoagulation for Mechanical Heart Valves
 Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD
 Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes
 SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
Patients selection criteria for LAA occlusion. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Patients selection criteria for LAA occlusion Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Atrial Fibrillation The most common cardiac arrhythmia. Confers
Patients selection criteria for LAA occlusion Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Atrial Fibrillation The most common cardiac arrhythmia. Confers
Percutaneous Left Atrial appendage occlusion and anticoagulation therapy Nicolas Lellouche, MD, PhD
 Percutaneous Left Atrial appendage occlusion and anticoagulation therapy Nicolas Lellouche, MD, PhD Fédération de Cardiologie Hôpital Henri Mondor Créteil Atrial Fibrillation is a major cause of Stroke
Percutaneous Left Atrial appendage occlusion and anticoagulation therapy Nicolas Lellouche, MD, PhD Fédération de Cardiologie Hôpital Henri Mondor Créteil Atrial Fibrillation is a major cause of Stroke
How to Prevent Thromboembolic Complications in TAVI
 How to Prevent Thromboembolic Complications in TAVI PETER WENAWESER, MD Swiss Cardiovascular Centre, University Hospital, Bern, Switzerland Potential Conflicts of Interest Proctoring and lecture fees from
How to Prevent Thromboembolic Complications in TAVI PETER WENAWESER, MD Swiss Cardiovascular Centre, University Hospital, Bern, Switzerland Potential Conflicts of Interest Proctoring and lecture fees from
Challenges in Anticoagulation Bridging and Emerging Therapies. Disclosures and Relationships. Objectives. Dr. Cumbler has no conflicts of interest
 Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Disclosure Slide. Controversies in Anticoagulation. Presenter Disclosure Information. Challenges in Anticoagulation
 1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Should We Reconsider using Anticoagulation for Biological Tissue Valves
 Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Xarelto (rivaroxaban)
") Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Emerging Cardiac Technologies. Thomas D. Conley, MD FACC FSCAI BHHI Primary Care Symposium February 27, 2015
 Emerging Cardiac Technologies Thomas D. Conley, MD FACC FSCAI BHHI Primary Care Symposium February 27, 2015 None Financial Disclosures Examples of Emerging Technologies Therapeutic Bioabsorbable Stents
Emerging Cardiac Technologies Thomas D. Conley, MD FACC FSCAI BHHI Primary Care Symposium February 27, 2015 None Financial Disclosures Examples of Emerging Technologies Therapeutic Bioabsorbable Stents
Is Oral Rivaroxaban Safe and Effective in the Treatment of Patients with Symptomatic DVT?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Disclosures. Updates in Interventional Cardiology and Guidelines 6/12/2017. No Conflicts of Interest
 Updates in Interventional Cardiology and Guidelines Krishan Soni, MD, MBA, FACC Assistant Professor of Medicine Division of Cardiology Disclosures No Conflicts of Interest Final syllabus available by email:
Updates in Interventional Cardiology and Guidelines Krishan Soni, MD, MBA, FACC Assistant Professor of Medicine Division of Cardiology Disclosures No Conflicts of Interest Final syllabus available by email:
Is there enough evidence for DAPT after endovascular intervention for PAOD?
 Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS
 Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients:
 Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van
Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
How Long Patietns Will Be on Dual Antiplatelet Therapy?
 How Long Patietns Will Be on Dual Antiplatelet Therapy? Ron Waksman,, MD, FACC Professor of Medicine (Cardiology) Georgetown University Associate Director, Division of Cardiology, Washington Hospital Center
How Long Patietns Will Be on Dual Antiplatelet Therapy? Ron Waksman,, MD, FACC Professor of Medicine (Cardiology) Georgetown University Associate Director, Division of Cardiology, Washington Hospital Center
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre
 TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
DISCLOSURE. What I am Talking About. Rational Use of Antiplatelet Agents. Aspirin. Tom DeLoughery, MD MACP FAWM
 Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN