CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin
|
|
|
- Stewart Johns
- 6 years ago
- Views:
Transcription
1 Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin Dr. Vikas Tandon Associate Professor, Cardiology McMaster University November 1, 2017
2 CSIM Annual Meeting 2017 Conflict Disclosures I have the following conflicts to declare: Company/Organization Advisory Board or equivalent X X Details Speakers bureau member X X Payment from a commercial organization. (including gifts or other consideration or in kind compensation) X X Grant(s) or an honorarium X X Patent for a product referred to or X X marketed by a commercial organization. Investments in a pharmaceutical organization, medical devices company or communications firm. X Participating or participated in a clinical trial McMaster University Participated in periop research studies including VISION, POISE-2, MANAGE X
3 CSIM Annual Meeting 2017 The following presentation represents the views of the speaker at the time of the presentation. This information is meant for educational purposes, and should not replace other sources of information or your medical judgment. Learning Objectives: Understand the importance of perioperative risk assessment Review the utility of current risk stratification tools Examine the utility of BNP/nt-pro-BNP in the preoperative setting Understand the significance of the postoperative troponin elevation and develop an approach to management

4 Perioperative Care Congress: Science, Evidence and Practice Save the date: Perioperative Care Congress 2018 May 11-13, 2018 Toronto, Ontario CANADA Visit our website or follow us on More information to follow!
5 Case Mrs. B.W. 72 y/o F with significant OA Referred for upcoming total knee arthroplasty Cardiac risk factors DM, HTN, Chol, previous NSTEMI 2003 Otherwise asymptomatic, N vitals, N labs Meds: ASA, Atorvastatin, Coversyl, Bisoprolol OR date July 19, 2016
6 Case Mrs. B.W. What should be done next? 1. Send for cath 2. Take pt straight to the OR, no other consult required 3. Cancel surgery too high risk 4. Consider for a perioperative consult by medicine and/or cardiology teams
7 Is the preoperative consult useful?
8 Scope of problem Worldwide >200,000,000 major noncardiac surgical procedures annually 1:20 suffer myocardial injury/infarction or cardiac arrest/death within 30 days Perioperative cardiac complications account for 1/3 of perioperative deaths
9 Is the preoperative consult useful?
10 Yes! Is the preoperative consult useful? 1. Patients: ethical obligation to patients to give accurate risk assessment for informed decision making 2. Physicians: Gauge CV risk to guide management Further testing if needed Instructions re: medications Postop monitoring Shared care model
11 Good Pre-op Consults Specify: 1. Clear estimation of risk 2. Clear recommendation re: further testing 3. Clear recommendations for medications 4. Clear direction as to degree of post op monitoring i.e. ward bed w tele vs CCU/ICU/Step down bed, trops 5. Clear communication of who will do what
12 Risk Scores RCRI most validated; simplest to use CAD, stroke, CHF, DM, high risk surgery, Creatinine Does not take into account emergency surgeries underestimates cardiac risk by 50% NSQIP likely superior to RCRI Requires an online calculator Underestimates risk as routine troponin screening not done All risk scores will underestimate in >40% pts Limited mobility so pts won t manifest symptoms
13 CCS Recommendation When evaluating cardiac risk, we suggest clinicians use RCRI over other available clinical risk prediction scores Conditional recommendation low-quality evidence
14 Revised Cardiac Risk Index Variables Pts Hx of IHD 1 Hx of CHF 1 Hx of CVD 1 Insulin for diabetes 1 Crt >177 µmol/l 1 High-risk surgery 1 Total RCRI points Risk of MI, cardiac arrest, or death 30 days after surgery 95% CI 0 3.9% 2.8%-5.4% 1 6.0% 4.9%-7.4% % 8.1%-12.6% % 11.1%-20.0% * based on high-quality external validation studies
15 Is Non-Invasive Testing Useful? Current guidelines: Pts with low functional capacity Pts with risk of MI/death 1% When result will change management Stress Nuclear and Stress Echo most common 9% of adults age 40 with int/high risk tested
16 Pharmacological stress echocardiography and radionuclide imaging Several studies, mostly small sample size and small number of events Low quality of evidence most retrospective, few reported risk adjusted associations No study adequately assessed incremental value of stress tests over well-established perioperative cardiac risk factors (e.g., RCRI)

17 CCS Recommendations We recommend against performing preoperative exercise stress test, pharmacological stress echocardiography, or preoperative radionuclide imaging to enhance perioperative cardiac risk estimation
18 Is Cardiac CT Angiography Useful?
19 VISION CCTA Prospective cohort study 12 centers in 8 countries Evaluated whether preop CCTA enhances perioperative risk prediction in 955 at-risk patients Physicians were blinded unless LM detected Systematic Postop Trop monitoring Primary outcome - CV death and nonfatal MI 74 patients (7.7%) within 30 days of surgery
20 Interpretation of VISION CCTA results Although CCTA findings improve risk estimation for patients who will suffer periop CV death or MI CCTA findings are more than 5 X as likely to lead to inappropriate overestimation of risk among patients who will not suffer these outcomes
21 CCS Recommendation We recommend against performing preoperative coronary CT angiography to enhance perioperative cardiac risk estimation Strong recommendation, moderate-quality evidence
22 Biomarkers NT pro-bnp
23 Individual data M-A of 2179 patients 235 suffered death or MI within 30 days after noncardiac surgery Preop NT-proBNP 300 ng/l or BNP 92 ng/l strongest independent preop predictor of death/mi OR, 3.40; 95% CI, Compared to preop clinical model preop natriuretic peptide improved risk estimation among patients who did and did not suffer primary outcome In sample of 1000 patients overall absolute NRI is 155 patients
24 NT-proBNP/BNP Risk of death or MI at 30 days after noncardiac surgery, based on patient s preoperative NT-proBNP or BNP Test result Risk estimate 95% CI NT-proBNP <300 ng/l or BNP <92 mg/l 4.9% 3.9% - 6.1% NT-proBNP value 300 ng/l or BNP 92 mg/l 21.8% 19.0% % compared to RCRI, preop NT-proBNP/BNP results improved risk classification in 155 patients in 1000 patient sample based on risk categories <5%, 5-10%, >10-15%, >15%
25 Biomarkers NT pro-bnp Compared to imaging, NT pro-bnp More accurate Less expensive Convenient and faster due to availability of point of care NT pro-bnp assays due to cost differential b/w NT pro-bnp and consult may have role in determining who needs preop consult
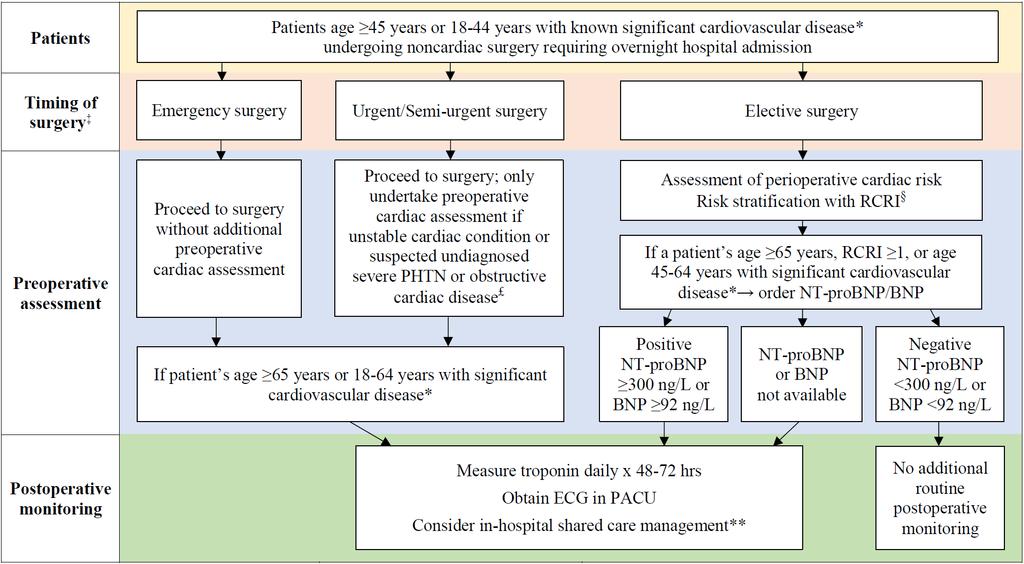
26 CCS Recommendation We recommend measuring NT-proBNP or BNP before noncardiac surgery to enhance perioperative cardiac risk estimation in patients 65 years of age, 45 to 64 years of age with significant cardiovascular disease, or who have RCRI score 1 Strong recommendation, moderate-quality evidence
27 x
28 Case Mrs. B.W. 72 y/o F with significant OA Referred for upcoming total knee arthroplasty Cardiac risk factors DM, HTN, Chol, previous NSTEMI 2003 Otherwise asymptomatic, N vitals, N labs Meds: ASA, Atorvastatin, Coversyl, Bisoprolol OR date July 19, 2016
29 x
30 Troponin monitoring POISE Trial (8351 patients) 65% of patients suffering perioperative MI do not experience ischemic symptoms Presence or absence of signs/symptoms does not change risk 30-day mortality symptomatic MI: aor 4.76 (95% CI, ) asymptomatic MI: aor 4.00 (95% CI, )
31 VISION Study (Botto 2014) Prospective international cohort study 15,065 in-hospital noncardiac surgery patients TnT measured postop days 1,2,3 MINS Criteria TnT 0.03 ng/ml due to myocardial ischemia death at 30 days: MINS - 9.8%, No MINS - 1.1% 84% MINS asymptomatic undetected without troponin monitoring Asymptomatic perioperative TnT elevations adjudicated as myocardial injuries due to ischemia that did not fulfill Universal Definition of MI were also associated with increased risk of 30-day mortality ahr, 3.30; 95% CI,
32 Recommendation We recommend obtaining daily troponin measurements for 48 to 72 hours after noncardiac surgery in patients with baseline risk >5%* for cardiovascular death or nonfatal MI at 30 days after surgery Strong recommendation, moderate-quality evidence * Patients with an elevated NT-proBNP/BNP measurement before surgery or, if there is no NT-proBNP/BNP measurement before surgery, in those who have an RCRI score 1, age 45 to 64 years with significant cardiovascular disease, or age 65 years
33 Approach to MINS Look for and correct physiological abnormalities hypoxia, hypotension, tachycardia (if BP adequate), Hb if <70 If no signs of bleeding initiate ASA 81 mg daily Initiate or intensify Statin therapy
34 Postoperative management of complications ASA and statin in patients suffering myocardial injury after noncardiac surgery Prospective cohort study 415 noncardiac surgery patients who suffered postop MI ASA and statin at discharge reduced 30-day mortality ASA : aor 0.54 (95% CI, ) Statin: aor 0.26 (95% CI, )
35 Recommendations We recommend initiation of long-term ASA and statin in patients who suffer myocardial injury or myocardial infarction after noncardiac surgery Strong recommendation, moderate-quality evidence
36 Case Mrs. B.W. 72 y/o F with significant OA Referred for upcoming total knee arthroplasty Cardiac risk factors DM, HTN, Chol, previous NSTEMI 2003 Otherwise asymptomatic, N vitals, N labs Meds: ASA, Atorvastatin, Coversyl, Bisoprolol Follow up 1, 6, 12, (18, 24) months
37 Conclusions 1. Current clinical risk scores underestimate risk in substantial proportion of patients Revised risk estimations for RCRI in new CCS guidelines Non-invasive testing probably adds little CCTA has net overall effect of putting more patients in wrong risk category 2. NT pro-bnp is more accurate, convenient, faster, and less expensive than non-invasive testing 3. Troponin are strong independent predictor of 30-day mortality after noncardiac surgery 85% of MINS patients asymptomatic (4 TH gen trop) Up to 93% asymptomatic with hs-trops 4. ASA and Statins reduce 30 day mortality in patients with MINS


38 CSIM Annual Meeting 2017 Special thanks to Dr. PJ Devereaux Scientific Leader, Perioperative Research Group, PHRI, McMaster University VISION, POISE 1, POISE 2 MANAGE, HIP ATTACK, VISION 2, POISE 3 Co-Chair, CCS Perioperative Guidelines
39 Comments and Questions
40
41 M-A of dipyridamole stress perfusion prior to vascular surgery

42 M-A of dipyridamole stress perfusion prior to vascular surgery Baseline risk = 7%
43 M-A of dipyridamole stress perfusion prior to vascular surgery Baseline risk = 7%

44 M-A of dipyridamole stress perfusion prior to vascular surgery Baseline risk = 7%
45 M-A of dipyridamole stress perfusion prior to vascular surgery Baseline risk = 7%
46 M-A of dipyridamole stress perfusion prior to vascular surgery Baseline risk = 7%
47 M-A of dipyridamole stress perfusion prior to vascular surgery Baseline risk = 7%
48 Is Non-Invasive Testing Useful? Limitations: Small studies, few events, clinicians not blinded Almost half used a retrospective design No evaluation independent prognostic value Few systematically monitored for MI None reporting net absolute reclassification
49 Net Absolute Reclassification Index how well a new model reclassifies subjects - either appropriately or inappropriately - as compared to an old model i.e. comparison of old model vs. old model + 1 new element RCRI alone vs. RCRI + non invasive test

50 Is Cardiac CT Angiography Useful?
51 VISION CCTA Prospective cohort study 12 centers in 8 countries Evaluated whether preop CCTA enhances perioperative risk prediction in 955 at-risk patients Physicians were blinded unless LM detected Systematic Postop Trop monitoring Primary outcome - CV death and nonfatal MI 74 patients (7.7%) within 30 days of surgery
52 Model with CCTA and RCRI - C=0.66 # of Patients HR 95% CI P RCRI scores CCTA findings Normal Non-obst Obstructive Extensive obst ( ) 1.88 ( ) 4.02 ( ) ( ) 2.05 ( ) 3.76 ( ) <
53 Model with CCTA and RCRI - C=0.66 # of Patients HR 95% CI P RCRI scores CCTA findings Normal Non-obst Obstructive Extensive obst ( ) 1.88 ( ) 4.02 ( ) ( ) 2.05 ( ) 3.76 ( ) <
54 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15% NRI for those who had event: 21.6% 95% CI ) p<0.001 NRI for those who did not have event: -10.7% ( ) p<0.001 Overall NRI: 11% (-0.73, 22.64), p=0.066
55 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15%
56 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15%
57 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15%
58 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15%
59 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15% pts appropriately reclassified 1 pt inappropriately reclassfied Net = 17-1 =16
60 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15% pts appropriately reclassified 1 pt inappropriately reclassfied Net = 17-1 =16
61 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15% pts appropriately reclassified 1 pt inappropriately reclassfied Net = 17-1 =16
62 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15% pts appropriately reclassified 1 pt inappropriately reclassfied Net = 17-1 =16
63 Net reclassification index Models for 30 day probability of CV death and MI Model that included CCTA findings Patients who had an event Patients who did not have an event RCRI only <5% 5-15% >15% <5% 5-15% >15% <5% % >15% pts appropriately reclassified 57 pts appropriately reclassified 1 pt inappropriately reclassfied 151 pts inapprop. reclassified Net = 17-1 = 16 Net = = -94
64 Interpretation of VISION CCTA results Although CCTA findings improve risk estimation for patients who will suffer periop CV death or MI CCTA findings are more than 5 X as likely to lead to inappropriate overestimation of risk among patients who will not suffer these outcomes
65 CCS Recommendation We recommend against performing preoperative coronary CT angiography to enhance perioperative cardiac risk estimation Strong recommendation, moderate-quality evidence
Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD
: What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD") Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting
Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Peri-operative Troponin Measurements - Pathophysiology and Prognosis
 Peri-operative Troponin Measurements - Pathophysiology and Prognosis Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
Peri-operative Troponin Measurements - Pathophysiology and Prognosis Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC. DO's and DON'Ts: Reducing unnecessary perioperative investigations
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DO's and DON'Ts: Reducing unnecessary perioperative investigations Emmanuelle Duceppe, MD FRCPC General Internal Medicine University
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DO's and DON'Ts: Reducing unnecessary perioperative investigations Emmanuelle Duceppe, MD FRCPC General Internal Medicine University
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY
 PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Perioperative Infarcts: Epidemiology, predictors and post-op monitoring
 Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver
 Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Agenda. Disclosures. Surgical Mortality: What is High Risk?
 Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Biomarkers and Arrhythmias/Devices Ulrika Birgersdotter-Green, M.D.
 Biomarkers and Arrhythmias/Devices Ulrika Birgersdotter-Green, M.D. Professor of Medicine Division of Cardiology University of California, San Diego Disclosures Honoraria, Research Grants, Medtronic Honoraria,
Biomarkers and Arrhythmias/Devices Ulrika Birgersdotter-Green, M.D. Professor of Medicine Division of Cardiology University of California, San Diego Disclosures Honoraria, Research Grants, Medtronic Honoraria,
Update on Perioperative Medicine. Update on Perioperative Medicine. Question 1: Clinical Risk Prediction. for the Office-based Practitioner
 Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Cardiac Screening with Electrocardiography, Stress Echocardiography, or Myocardial Perfusion Imaging
 Cardiac Screening with Electrocardiography, Stress Echocardiography, or Myocardial Perfusion Imaging A D V I C E F O R H I G H V A L U E C A R E F R O M T H E A M E R I C A N C O L L E G E O F P H Y S
Cardiac Screening with Electrocardiography, Stress Echocardiography, or Myocardial Perfusion Imaging A D V I C E F O R H I G H V A L U E C A R E F R O M T H E A M E R I C A N C O L L E G E O F P H Y S
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Evaluating the Heart before Non-Cardiac Surgery
 Evaluating the Heart before Non-Cardiac Surgery Dr Rob Stephens Anaesthetist UCLH + UCL the centre for Anaesthesia www.ucl.ac.uk/anaesthesia/people/stephens Google UCL Stephens www.ucl.ac.uk/anaesthesia/people/stephens
Evaluating the Heart before Non-Cardiac Surgery Dr Rob Stephens Anaesthetist UCLH + UCL the centre for Anaesthesia www.ucl.ac.uk/anaesthesia/people/stephens Google UCL Stephens www.ucl.ac.uk/anaesthesia/people/stephens
PERIOPERATIVE CARDIAC RISK ASSESSMENT. Divya Gollapudi, MD
 PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
Current and Future Imaging Trends in Risk Stratification for CAD
 Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Cardiac Risk Assessment in the Preoperative period
 Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD
 HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
Perioperative Myocardial Infarction
 Perioperative Myocardial Infarction Which patient should UNDERGO CORONARY ANGIOGRAPHY? The Cardiologists view Hans Rickli, St.Gallen 1 Experience Standards Risk stratification Team approach.. Tightrope
Perioperative Myocardial Infarction Which patient should UNDERGO CORONARY ANGIOGRAPHY? The Cardiologists view Hans Rickli, St.Gallen 1 Experience Standards Risk stratification Team approach.. Tightrope
Preoperative Cardiac Risk Calculators
 The Fort Lauderdale, Florida Preoperative Cardiac Risk Calculators Steven L. Cohn, MD, FACP, SFHM Professor Emeritus Director - Medical Consultation Service Jackson Memorial Hospital University of Miami
The Fort Lauderdale, Florida Preoperative Cardiac Risk Calculators Steven L. Cohn, MD, FACP, SFHM Professor Emeritus Director - Medical Consultation Service Jackson Memorial Hospital University of Miami
Avoiding Thor s Thunderbolt!
 Avoiding Thor s Thunderbolt! The Urologist s Role in Managing the Peri-operative Risk of Cardio-Ischemic and Embolic Events Philip J. Walther, MD, PhD, MBA, FACS Professor of Urologic Surgery Duke U. School
Avoiding Thor s Thunderbolt! The Urologist s Role in Managing the Peri-operative Risk of Cardio-Ischemic and Embolic Events Philip J. Walther, MD, PhD, MBA, FACS Professor of Urologic Surgery Duke U. School
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality
 Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
SUPPLEMENTARY DOCUMENTS. Supplemental Table 1: Panel members GRADE of recommendation rating and conflicts
 SUPPLEMENTARY DOCUMENTS Supplementary Table of Contents 1. Supplemental Appendix Appendix 1: Members of guidelines panels page 6 2. Supplemental Tables Supplemental Table 1: Panel members GRADE of recommendation
SUPPLEMENTARY DOCUMENTS Supplementary Table of Contents 1. Supplemental Appendix Appendix 1: Members of guidelines panels page 6 2. Supplemental Tables Supplemental Table 1: Panel members GRADE of recommendation
Transfusion triggers in acute coronary syndromes: The MINT trial
 Transfusion triggers in acute coronary syndromes: The MINT trial Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Objectives Review evidence on transfusion triggers
Transfusion triggers in acute coronary syndromes: The MINT trial Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Objectives Review evidence on transfusion triggers
Low Risk Chest Pain. Objectives. Disclosure. Case 1. Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine
 Disclosure Low Risk Chest Pain No Financial Relationships to Disclose No significant investments or savings Unlimited Expenses Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School
Disclosure Low Risk Chest Pain No Financial Relationships to Disclose No significant investments or savings Unlimited Expenses Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School
Overcoming the Risk-Treatment Paradox in Non-STE ACS: It s Time! Christopher Granger, MD
 Overcoming the Risk-Treatment Paradox in Non-STE ACS: It s Time! Christopher Granger, MD Disclosures Research contracts: AstraZeneca, Bayer, Novartis, GSK, Sanofi-Aventis, BMS, Pfizer, The Medicines Company,
Overcoming the Risk-Treatment Paradox in Non-STE ACS: It s Time! Christopher Granger, MD Disclosures Research contracts: AstraZeneca, Bayer, Novartis, GSK, Sanofi-Aventis, BMS, Pfizer, The Medicines Company,
Agenda. Perioperative Cardiac Risk Stratification circa Surgical Mortality: What is High Risk? Presenter Disclosure Information
 9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Preoperative Risk. Geoffrey C Zarrella DO FACC. Assessment
 Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Clinical Controversies in Perioperative Medicine!
 Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD
 Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
Pre-op Risk Assessment. Hal Blanks MD FACC
 Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Biomarkers in cardiovascular disease. Felix J. Rogers, DO, FACOI April 29, 2018
 Biomarkers in cardiovascular disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological
Biomarkers in cardiovascular disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological
Ischemic and bleeding risk stratification in NSTE ACS. Andrzej Budaj Postgraduate Medical School Grochowski Hospital, Warsaw, Poland
 Ischemic and bleeding risk stratification in NSTE ACS Andrzej Budaj Postgraduate Medical School Grochowski Hospital, Warsaw, Poland Disclosure Andrzej Budaj, MD, PhD, reports the following potential conflicts
Ischemic and bleeding risk stratification in NSTE ACS Andrzej Budaj Postgraduate Medical School Grochowski Hospital, Warsaw, Poland Disclosure Andrzej Budaj, MD, PhD, reports the following potential conflicts
Preoperative Evaluation Guidelines and Work up
 Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Stress Testing:Which Study is Indicated for My Patient?
 Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
Update in Perioperative Medicine
 Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
Perioperative Cardiac Management. Emma Sargsyan, MD, FACP
 Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Biomarkers and Arrhythmias/Devices Ulrika Birgersdotter-Green, MD, FHRS
 Biomarkers and Arrhythmias/Devices Ulrika Birgersdotter-Green, MD, FHRS Professor of Medicine Division of Cardiology University of California, San Diego Disclosures Honoraria, Research Grants, Medtronic
Biomarkers and Arrhythmias/Devices Ulrika Birgersdotter-Green, MD, FHRS Professor of Medicine Division of Cardiology University of California, San Diego Disclosures Honoraria, Research Grants, Medtronic
Updates & Controversies in Perioperative Medicine
 Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Updates in Perioperative Medicine Estimating mortality in surgical
Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Updates in Perioperative Medicine Estimating mortality in surgical
Mario Plebani University-Hospital of Padova, Italy
 Mario Plebani University-Hospital of Padova, Italy CK-MB mass assay CHF guidelines use BNP for rule out AST in AMI CK in AMI INH for CK-MB electrophoresis for CK and LD isoenzymes RIA for myoglobin WHO
Mario Plebani University-Hospital of Padova, Italy CK-MB mass assay CHF guidelines use BNP for rule out AST in AMI CK in AMI INH for CK-MB electrophoresis for CK and LD isoenzymes RIA for myoglobin WHO
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Probing prognosis in heart failure Daniel R. Wagner CHL/INCCI/CRP-Santé Luxembourg Disclosures Grants: Cordis, Boston Scientific, Medtronic, Sorin, Hexacath, Abbott,
DECLARATION OF CONFLICT OF INTEREST Probing prognosis in heart failure Daniel R. Wagner CHL/INCCI/CRP-Santé Luxembourg Disclosures Grants: Cordis, Boston Scientific, Medtronic, Sorin, Hexacath, Abbott,
Post Operative Troponin Leak: David Smyth Christchurch New Zealand
 Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Judicious Use of Preoperative Consultants. Relevant disclosures: None. Preoperative Consultation by Specialists: Overall Impact on Outcome?
 Judicious Use of Preoperative Consultants Changing Practice of Anesthesia Meeting 2014 Relevant disclosures: None Rachel Eshima McKay, MD Professor, Anesthesia and Perioperative Director, UCSF Mount Zion
Judicious Use of Preoperative Consultants Changing Practice of Anesthesia Meeting 2014 Relevant disclosures: None Rachel Eshima McKay, MD Professor, Anesthesia and Perioperative Director, UCSF Mount Zion
A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart.
 November 2016 A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart. He consulted Cardiology. No attempt should be made to prognosticate
November 2016 A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart. He consulted Cardiology. No attempt should be made to prognosticate
Simon A. Mahler MD, MS, FACEP Associate Professor Department of Emergency Medicine Wake Forest School of Medicine
 Simon A. Mahler MD, MS, FACEP Associate Professor Department of Emergency Medicine Wake Forest School of Medicine Research funding: American Heart Association Donaghue Foundation/ Association of American
Simon A. Mahler MD, MS, FACEP Associate Professor Department of Emergency Medicine Wake Forest School of Medicine Research funding: American Heart Association Donaghue Foundation/ Association of American
SESSION 5 2:20 3:35 pm
 SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
High-Sensitivity Cardiac Troponin in Suspected ACS
 15 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes STATE-OF-THE-ART High-Sensitivity Cardiac Troponin in Suspected ACS David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care
15 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes STATE-OF-THE-ART High-Sensitivity Cardiac Troponin in Suspected ACS David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW
 PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
Q: Do cardiac risk stratification indexes
 1-MINUTE CONSULT ROHAN MANDALIYA, MD, FACP Clinical Fellow, Division of Gastroenterology and Hepatology, Department of Medicine, Georgetown University Hospital, Washington, DC GENO MERLI, MD, MACP Professor
1-MINUTE CONSULT ROHAN MANDALIYA, MD, FACP Clinical Fellow, Division of Gastroenterology and Hepatology, Department of Medicine, Georgetown University Hospital, Washington, DC GENO MERLI, MD, MACP Professor
Guidelines PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42. Prominent Dutch Cardiovascular Researcher Fired for Scientific Misconduct
 PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
Corporate Medical Policy
 Corporate Medical Policy ST2 Assay for Chronic Heart Failure File Name: Origination: Last CAP Review: Next CAP Review: Last Review: st_assay_for_chronic_heart_failure 2/2015 4/2018 4/2019 4/2018 Description
Corporate Medical Policy ST2 Assay for Chronic Heart Failure File Name: Origination: Last CAP Review: Next CAP Review: Last Review: st_assay_for_chronic_heart_failure 2/2015 4/2018 4/2019 4/2018 Description
Perioperative Medicine 2016 Some Answers, Even More Questions
 Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
Blood transfusions in ICU: double-edged sword. Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal
 Physician-in-Chief, CHUM Professor, University of Montreal") Blood transfusions in ICU: double-edged sword Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Canadian Critical Care Trials Group Collaborating for Impact Leading
Blood transfusions in ICU: double-edged sword Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Canadian Critical Care Trials Group Collaborating for Impact Leading
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Är dagens troponinmetoder tillräckligt känsliga?
 Är dagens troponinmetoder tillräckligt känsliga? Per Venge, MD PhD Professor Department of Medical Sciences Uppsala University and Department of Clinical Chemistry and Pharmacology University Hospital
Är dagens troponinmetoder tillräckligt känsliga? Per Venge, MD PhD Professor Department of Medical Sciences Uppsala University and Department of Clinical Chemistry and Pharmacology University Hospital
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction
 Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction Nadia Bandstein, MD; Rickard Ljung, MD, PhD; Magnus Johansson, MD, PhD; Martin Holzmann,
Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction Nadia Bandstein, MD; Rickard Ljung, MD, PhD; Magnus Johansson, MD, PhD; Martin Holzmann,
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Troponin = 35. Objectives. Low Risk Chest Pain. Does this patient have ACS? Does this patient have ACS? Objectives
 Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
 Biomarkers in Acute Cardiac Disease Samir Arnaout, M.D.FESC Associate Professor of Medicine Internal Medicine i & Cardiology American University of Beirut Time course of the appearance of various markers
Biomarkers in Acute Cardiac Disease Samir Arnaout, M.D.FESC Associate Professor of Medicine Internal Medicine i & Cardiology American University of Beirut Time course of the appearance of various markers
Patient characteristics Intervention Comparison Length of followup
 ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Preoperative Evaluation: Patients with Cardiac Disease
 Advances in Internal Medicine 2012 Preoperative Evaluation: Patients with Cardiac Disease Mary O. Gray, MD Professor of Medicine UC San Francisco Circulation 2007:100:e418-e500 (1) Cardiac Risk Assessment
Advances in Internal Medicine 2012 Preoperative Evaluation: Patients with Cardiac Disease Mary O. Gray, MD Professor of Medicine UC San Francisco Circulation 2007:100:e418-e500 (1) Cardiac Risk Assessment
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy
 Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Which Test When? Avoid the Stress of Stress Testing. Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute
 Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Testing the Asymptomatic CAD Patient: When and Why?
 Testing the Asymptomatic CAD Patient: When and Why? Timothy M. Bateman M.D. Co-Director, Cardiovascular Radiologic Imaging Mid America Heart Institute Professor of Medicine University of Missouri-Kansas
Testing the Asymptomatic CAD Patient: When and Why? Timothy M. Bateman M.D. Co-Director, Cardiovascular Radiologic Imaging Mid America Heart Institute Professor of Medicine University of Missouri-Kansas
Canadian Antiplatelet Therapy Guidelines: 2014 Update James D. Douketis MD, FRCP(C)
") Canadian Antiplatelet Therapy Guidelines: 2014 Update James D. Douketis MD, FRCP(C) Department of Medicine, St. Joseph s Healthcare Hamilton and McMaster University, Hamilton, Canada Disclosures for: James
Canadian Antiplatelet Therapy Guidelines: 2014 Update James D. Douketis MD, FRCP(C) Department of Medicine, St. Joseph s Healthcare Hamilton and McMaster University, Hamilton, Canada Disclosures for: James
High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients with Stable Coronary Heart Disease: KAROLA Study 8 Year FU
 ESC Congress 2011 Paris, France, August 27-31 KAROLA Session: Prevention: Are biomarkers worth their money? Abstract # 84698 High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients
ESC Congress 2011 Paris, France, August 27-31 KAROLA Session: Prevention: Are biomarkers worth their money? Abstract # 84698 High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients
Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test
 Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test Jang-Ho Bae, MD., PhD., FACC. Konyang University Hospital Daejeon, Korea Chest pain in Women ACS Atypical Stable angina F/29
Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test Jang-Ho Bae, MD., PhD., FACC. Konyang University Hospital Daejeon, Korea Chest pain in Women ACS Atypical Stable angina F/29
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Value of troponin measurements in carotid artery revascularization
 Value of troponin measurements in carotid artery revascularization Gert J de Borst Department of Vascular Surgery Postoperative myocardial infarction after NCS: Magnitude of the problem POISE-1: 367 /8,351=
Value of troponin measurements in carotid artery revascularization Gert J de Borst Department of Vascular Surgery Postoperative myocardial infarction after NCS: Magnitude of the problem POISE-1: 367 /8,351=
High Sensitivity Troponin Improves Management. But Not Yet
 High Sensitivity Troponin Improves Management But Not Yet Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory Medicine
High Sensitivity Troponin Improves Management But Not Yet Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory Medicine
Central pressures and prediction of cardiovascular events in erectile dysfunction patients
 Central pressures and prediction of cardiovascular events in erectile dysfunction patients N. Ioakeimidis, K. Rokkas, A. Angelis, Z. Kratiras, M. Abdelrasoul, C. Georgakopoulos, D. Terentes-Printzios,
Central pressures and prediction of cardiovascular events in erectile dysfunction patients N. Ioakeimidis, K. Rokkas, A. Angelis, Z. Kratiras, M. Abdelrasoul, C. Georgakopoulos, D. Terentes-Printzios,
Learning Objectives. Predicting and Preventing Cardiovascular Disease. ACC/AHA Cholesterol Guidelines Key differences vs ATP III
 Presenter Disclosure Information 10:30 11:15am Predicting and Preventing Cardiovascular Disease: Can we put the Cardiologist out of business? The following relationships exist related to this presentation:
Presenter Disclosure Information 10:30 11:15am Predicting and Preventing Cardiovascular Disease: Can we put the Cardiologist out of business? The following relationships exist related to this presentation:
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
4/27/2015. Cardiac Events #1 cause of postoperative complications/ mortality- CHF, complete heart block, MI,
 Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Biomarkers in Heart Disease. Felix J. Rogers, DO, FACOI April 29, 2018
 Biomarkers in Heart Disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological processes,
Biomarkers in Heart Disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological processes,
2/20/2013. Why use imaging in CV prevention? Update on coronary CTA in 2013 Coronary CTA for 1 0 prevention: pros and cons Are we there yet?
 Evolving Role of Coronary CTA in Primary Cardiovascular Disease Prevention: Are We There Yet? Ron Blankstein, M.D., F.A.C.C. Co-Director, Cardiovascular Imaging Training Program Associate Physician, Preventive
Evolving Role of Coronary CTA in Primary Cardiovascular Disease Prevention: Are We There Yet? Ron Blankstein, M.D., F.A.C.C. Co-Director, Cardiovascular Imaging Training Program Associate Physician, Preventive
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Biomarkers in the Assessment of Congestive Heart Failure
 Biomarkers in the Assessment of Congestive Heart Failure Mid-Regional pro-adrenomedullin (MR-proADM) vs BNP & NT-proBNP as Prognosticator in Heart Failure Patients: Results of the BACH Multinational Trial
Biomarkers in the Assessment of Congestive Heart Failure Mid-Regional pro-adrenomedullin (MR-proADM) vs BNP & NT-proBNP as Prognosticator in Heart Failure Patients: Results of the BACH Multinational Trial
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON
 Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON How to Prevent and Manage the Post-Thrombotic Syndrome? Jean-Philippe Galanaud Clinical Thromboembolism & Division of GIM Sunnybrook,
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON How to Prevent and Manage the Post-Thrombotic Syndrome? Jean-Philippe Galanaud Clinical Thromboembolism & Division of GIM Sunnybrook,
2/26/2013. NCDR.13 Case Scenario Presentation Cath PCI Registry. Disclosures. Objectives. Dashboard Implications of Some Major Metrics
 NCDR.13 Case Scenario Presentation Cath PCI Registry Dashboard Implications of Some Major Metrics Disclosures Tony Hermann has nothing to disclose Mark Hutcheson has nothing to disclose Cornelia Anderson
NCDR.13 Case Scenario Presentation Cath PCI Registry Dashboard Implications of Some Major Metrics Disclosures Tony Hermann has nothing to disclose Mark Hutcheson has nothing to disclose Cornelia Anderson
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study
 open access Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study Tej Sheth, 1 Matthew Chan, 2 Craig Butler, 3 Benjamin Chow, 4 Vikas
open access Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study Tej Sheth, 1 Matthew Chan, 2 Craig Butler, 3 Benjamin Chow, 4 Vikas
Financial Disclosures. Coronary Artery Calcification. Objectives. Coronary Artery Calcium 6/6/2018. Heart Disease Statistics At-a-Glace 2017
 Coronary Artery Calcification Dharmendra A. Patel, MD MPH Director, Echocardiography Laboratory Associate Program Director Cardiovascular Disease Fellowship Program Erlanger Heart and Lung Institute UT
Coronary Artery Calcification Dharmendra A. Patel, MD MPH Director, Echocardiography Laboratory Associate Program Director Cardiovascular Disease Fellowship Program Erlanger Heart and Lung Institute UT