Thoracoabdominal aortic aneurysm
|
|
|
- Andrea Greene
- 5 years ago
- Views:
Transcription
1 Thoracoabdominal aortic aneurysm
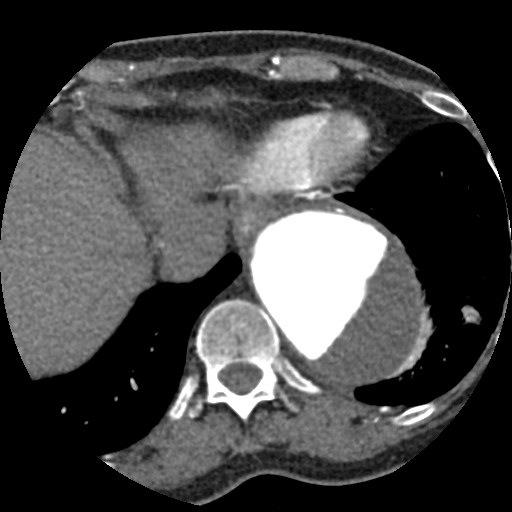
2 Patient (1) - 69 PMH: MVP, aortic root replacement with biological valve (Perimount) and subtotal aortic arch replacement Analysis for oppressive chest complaints reveals large thoracoabdominal aortic aneurysm
3
4
5 Underlying disease? Marfan Ehlers-Danlos Turner s syndrome Polycystic kidney disease Loeys-Dietz syndrome Syphilis / arteritis Traumatic injury
6 Risk factors for rupture? In total 80% will rupture (10-20% 5-year survival) Higher age and COPD increase rupture risk For aneurysm > 6 cm annual rupture risk 7% For aneurysm > 7 cm 43% will rupture Incidence CAD < 30% in contrast to AAA (> 70%)
7 Indications for repair Rupture All symptomatic aneurysms regardless of size should be repaired (pain/pressure) However in 95% no heralding symptoms Acute dissection with malperfusion/ other life-threatening complication Symptomatic aneurysm (pain or compression other organs) Enlargement 1 cm/year Absolute size > 6.5 cm or > 6.0 cm with connective tissue disorder
8 Repair strategies Cardiovascular risk factors Open Endovascular Hybrid Spirometry - most open repairs require single lung ventilation Pre-existing renal function (AKI most important risk factor for early postoperative mortality) CTA with 3-D reconstruction Preoperative workup

9 Modified Crawford classification Extent I Extent II Extent III Extent IV Extent V
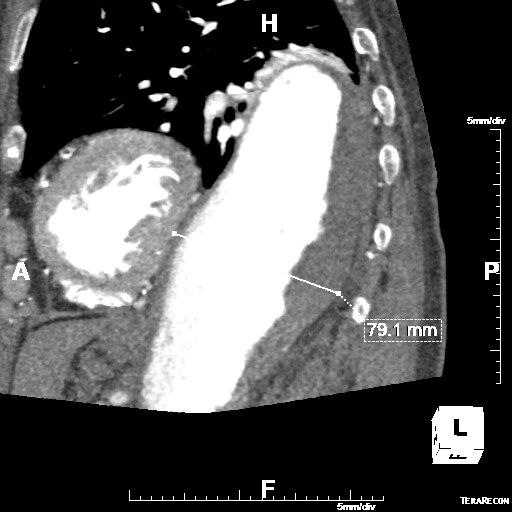
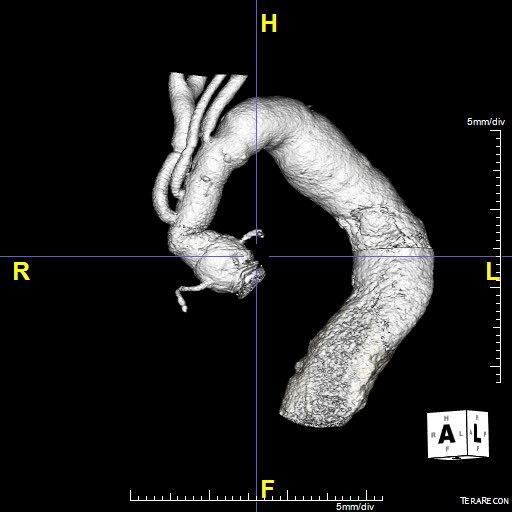
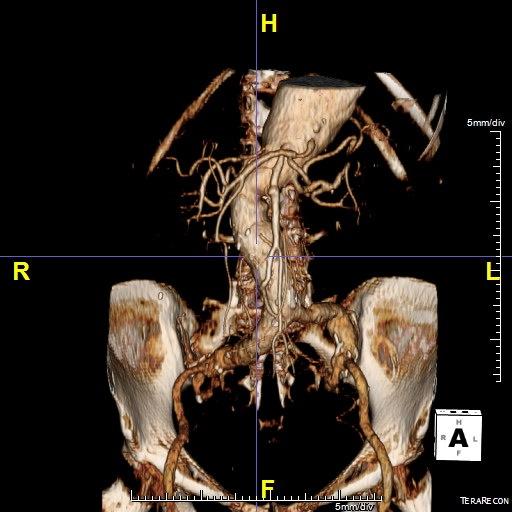
10 Patient (2) Rapidly progressive TAAA 7.9 cm No underlying other disease (degenerative) Extent II Open repair
11 Patient (3) Preoperative ICU admission (28/11) Arterial line (right radial artery) Pulmonary artery catheter (PAP 29/13, CI 3.8) ELD (10 cm H2O)
12 Is CSF drainage useful? CSF drainage No CSF drainage 24 23,7 18 % ,3 7,3 4 4,3 SC damage 30-D mortality In-hospital mortality RCT s N = 3 Cinà CS. J Vasc Surg 2004;40:36-44
13 Risk factors for paraplegia Overall mortality 10% Previous EVAR/TEVAR Preoperative hypotension Intraoperative hypotension Open distal anastomoses Postoperative complications in 200 patients Paraplegia 17 (8.5%) Cerebral infarction 5 (2.5%) Perioperative MI 1 (0.5%) Pneumonia 5 (2.5%) Atelectasis 19 (9.5%) AKI 5 (2.5%) Acute hepatic failure 3 (1.5%) Bowel ischemia 7 (3.5%) Gastrointestinal bleeding 1 (0.5%) Chylothorax 4 (2%) Vocal cord paralysis (left) 16 (8%) Phrenic nerve paralysis 1 (0.5%) Reoperation surgical bleeding 3 (1.5%) Wongkornrat W. Asian Cardiovasc Thorac Ann 2014
14 Intraoperative monitoring Insertion of double lumen endotracheal tube Central access with PA catheter for HD monitoring Arterial monitoring of upper and lower extremities with aortic clamping and left heart bypass Lumbar CSF drain in Extent I and II repair (IT pressure < 10 mmhg) - continue for 3-5 days Monitoring of SSEP/MEP with Extent II repair and hypothermic circulatory arrest
15 Circulatory support LHB with decompression of the proximal circulation in conjunction with distal perfusion through left atrial drainage via the left inferior pulmonary vein and arterial inflow distal to the aortic clamp site usually the iliac system Alternative is partial CP bypass by femoral vein canulation (advanced to RA) and same arterial inflow (includes membrane oxygenation) Circulatory arrest if proximal clamp is impossible with same canulation with total body retrograde perfusion
16 Additional measures to prevent ischemic injury Permissive or active systemic hypothermia (32 0 C) Cold selective renal perfusion (4 0 C) Reattachment of segmental arteries Sequential aortic clamping Selective visceral perfusion

17 Extent I Extent II Extent III Extent IV Extent V
18 Operative procedure 29/ (24 mm Hemabridge from left SA until aortic bifurcation with left-left bypass, CSF drainage, sequential aortic clamping, selective renal perfusion and IC artery reimplantation) left thoracophrenolaparotomy (retroperitoneal approach) - 4 tempi Period 1 - clamp distal LSA and T6 - E to E anastomosis native aorta and prosthesis Period 2 - clamp proximal prosthesis and T12 - reimplantation IC 10 (L/R) Period 3 - clamp distal reimplanted IC10 and infrarenal - reimplantation renal arteries and AMS/TC (single island) Period 4 - clamp infrarenal and above bifurcation - E to E anastomosis native aorta
19 Left-left bypass LUPV and LFA Stage 1 Stage 2 Stage 3 Stage 4
20 Postoperative course ICU return 29/11:16.00 Stable hemodynamics (CI 3 l/min/m2, PAP 35/20, MAP > mmhg) Paroxysmal AF (rate control - spontaneous SR) Sedation immediate stop - no SC damage Extubation 30/11: 08.00
21 Postoperative course Stable renal function (creatinine 47 - adequate diuresis) Restart oral intake 30/11 Removal ELD 02/12 Discharge home 12/12
22 Outcome Open TAAA repair (N) 30-D survival (%) AKI (%) Spinal cord ischemia (%) Crawford Coselli Safi Frederick JR. Ann Cardiothorac Surg 2012;1:
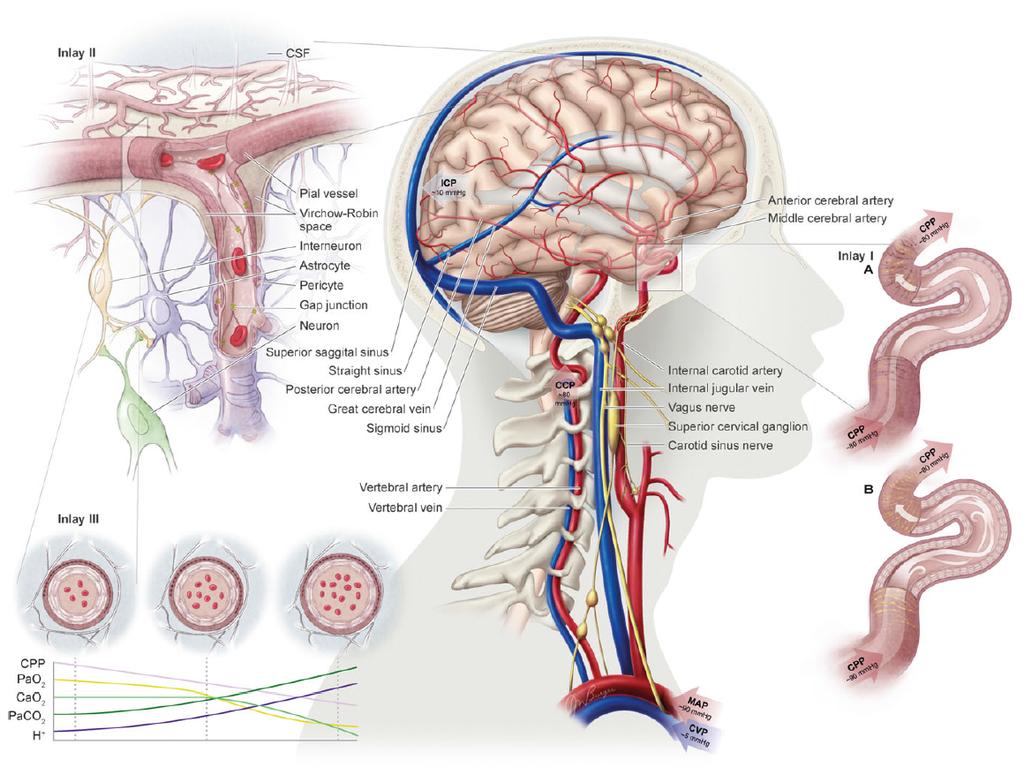
23 CBF manipulation
24 Tight regulation important Nutrient & oxygen supply Limited capacity for substrate storage High metabolic rate
25 Principal regulators Cerebral metabolism PaCO2 Mean arterial pressure (MAP) Autonomic nervous system
26

27 Metabolic regulation PaCO2 PaO2 (< 50 mmhg) 1-3% /mm CO2 3-6% /mm CO2 Appears to be regulated by CaO2 Highly influenced by PaCO2 >> with PaCO2 and << with PaCO2 CBF different for ICA and VA during PaCO2 and PaO2

28 ph or PaCO2? ph Pial arteries ph N PaCO2 N ph or PaCO2 N ph N PaCO2 N ph ph ph N PaCO2 N ph PaCO2
29 Hypoxia Direct vascular mechanisms ph Adenosine? NO? PaO2 Neuron Astrocyte Neurovascular unit
30 Autoregulation - old and new Old New Slope 0.21 Slope 0.81 Buffering capacity against hypertension is certainly better
31 Autoregulation Regulation (change in resistance) probably takes places in all cerebral vessels but larger arteries of the brain play a prominent role. This may also be true for the carotid and vertebral arteries Important interaction with PaCO2
32 Autonomic regulation Cerebrovasculature is extensively innervated by adrenergic and cholinergic fibers arranged in three layers of nerve plexi Sympathetic nervous system (by vasoconstriction) has an important effect on cerebral autoregulation Role of parasympathetic nervous system unclear
33 If regulation is intact (metabolic, autoregulation and autonomic nervous system, it will be very difficult to manipulate cerebral blood flow
34 60 P < 0.05 P < 0.05 MCA MFV (cm/sec) P < 0.05 P < 0.05 P < 0.05 MAP (mmhg) ,5 P < 0.05 CVR (mmhg/(cm/s)) 2 1,5 1 Baseline Low NE High NE High NE + PE High NE + PE (late) PE Kimmerly DS. Clin Physiol Funct Imaging 2003;23:
 86 ± 9 104 ± 9 89 ± 9 106 ±")
 57 ± 18 56 ± 13 52 ± 11 56 ± 13 59 ± 5 62 ± 7 Moppett IK.")
35 Healthy volunteers Ephedrine Dobutamine Dopexamine Dobutamine MAP 25% Before After Before After Before After Ephedrine MAP 25% MAP (mmhg) 86 ± ± 9 89 ± ± 8 89 ± ± 9 Dopexamine CI 25% CI (l/min) NA NA NA NA 2.2 ± ± 0.3 MCAFV (cm/s) 57 ± ± ± ± ± 5 62 ± 7 Moppett IK. BJA 2004;92:39-44
36 3.6 ± 2.9% / mmhg PaCO2 Bisschops LLA. Crit Care Med 2010;38:
37 Cerebral blood flow MFV ACM (cm/sec) SjbO2 (%) T = 0 T = 3 T = 6 T = 9 T = 12 T = 18 T = 24 T = 48 Time after admission to ICU (hrs) 0 T = 0 T = 3 T = 6 T = 9 T = 12 T = 18 T = 24 T = 48 Time after admission to ICU CBF during hypothermia < normothermia without evidence of inadequate oxygen supply = normothermia = hypothermia Buunk G. Intensive Care Med 1996;22: Bisschops LLA. Crit Care Med 2010;38:
38 Sepsis Before *** After 90 MFV ACM (cm/s) MFV ACM (cm/s) Dobutamine PGI2 60 Dob 0 Dob 2 Dob 4 Dob 6 Dob 8 Dob 10 Dob 0 N = 10 Septic encephalopathy MFV ACM correlated with CI but not MAP Berré J. J Crit Care 1994;9:1-6 N = 14 - Septic encephalopathy MFV ACM correlated beter with CI than MAP CEO2 decreased from 46 ± 3% to 36 ± 4% Berré J. Crit Care Med 1997;25:
![Sepsis 120 21 patients with severe sepsis 90 MFV ACM (cm/s) 60 30 NE 7 [2-70] μg/min NE 20 [8-110] μg/min 14 patients had impaired CA defined as a](/docs-images/81/83321948/images/39-1.jpg "CAI outside 0-2 ( MAP%/ CVR%) Patients with a PaCO2 > 40 mmhg all had impaired CA 0 MAP 65 ± 6 MAP 95 ± 13 Taccone FS.")
39 Sepsis patients with severe sepsis 90 MFV ACM (cm/s) NE 7 [2-70] μg/min NE 20 [8-110] μg/min 14 patients had impaired CA defined as a CAI outside 0-2 ( MAP%/ CVR%) Patients with a PaCO2 > 40 mmhg all had impaired CA 0 MAP 65 ± 6 MAP 95 ± 13 Taccone FS. Neurocrit Care 2010;12:35-42
40 Conclusions Under normal circumstances CBF manipulation with inotropic agents / vasopressors is ineffective CBF regulation under normal circumstances is extremely complex and incompletely understood Under pathological circumstances metabolic regulation of CBF appears to be effective in most circumstances but CA apparently not
41 Questions Group 1: How can we measure cerebral autoregulation in daily practice? Group 2. What is the evidence that increasing MAP with NE increases CBF in patients with SAH and delayed ischemia?
42 Questions Group 3: Is cerebral autoregulation intact in comatose patients after a cardiac arrest? Group 4: Design a RCT investigating whether increasing CBF in comatose patients after cardiac arrest would be beneficial
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm
 Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Aortic Arch/ Thoracoabdominal Aortic Replacement
 Aortic Arch/ Thoracoabdominal Aortic Replacement Joseph S. Coselli, M.D. Vice Chair, Department of Surgery Professor, Chief, and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery Baylor
Aortic Arch/ Thoracoabdominal Aortic Replacement Joseph S. Coselli, M.D. Vice Chair, Department of Surgery Professor, Chief, and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery Baylor
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
Thoracoabdominal aortic aneurysms by definition traverse
 Thoracoabdominal Aortic Aneurysm Repair: Open Technique Joseph Huh, MD, Scott A. LeMaire, MD, Scott A. Weldon, MA, CMI, and Joseph S. Coselli, MD Thoracoabdominal aortic aneurysms by definition traverse
Thoracoabdominal Aortic Aneurysm Repair: Open Technique Joseph Huh, MD, Scott A. LeMaire, MD, Scott A. Weldon, MA, CMI, and Joseph S. Coselli, MD Thoracoabdominal aortic aneurysms by definition traverse
SPINAL CORD ISCHEMIA AFTER THORACIC ANEURYSM REPAIR: RISK STRATIFICATION & PREVENTION DISCLOSURES. INDIVIDUAL None
 DISCLOSURES AFTER THORACIC ANEURYSM REPAIR: INDIVIDUAL None RISK STRATIFICATION & PREVENTION INSTITUTIONAL Cook, Inc W. L. Gore, Inc Conrad, J Vasc Surg, 2008 1 Intraoperative Adjuncts Oversew intercostals
DISCLOSURES AFTER THORACIC ANEURYSM REPAIR: INDIVIDUAL None RISK STRATIFICATION & PREVENTION INSTITUTIONAL Cook, Inc W. L. Gore, Inc Conrad, J Vasc Surg, 2008 1 Intraoperative Adjuncts Oversew intercostals
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
How to manage the left subclavian and left vertebral artery during TEVAR
 How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Descending aorta replacement through median sternotomy
 Descending aorta replacement through median sternotomy Mitrev Z, Anguseva T, Belostotckij V, Hristov N. Special hospital for surgery Filip Vtori Skopje - Makedonija June, 2010 Cardiosurgery - Skopje 1
Descending aorta replacement through median sternotomy Mitrev Z, Anguseva T, Belostotckij V, Hristov N. Special hospital for surgery Filip Vtori Skopje - Makedonija June, 2010 Cardiosurgery - Skopje 1
Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider
 Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider Matthias Thielmann, MD, PhD, FAHA Thoracic and Cardiovascular Surgery, West-German Heart and Vascular Center
Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider Matthias Thielmann, MD, PhD, FAHA Thoracic and Cardiovascular Surgery, West-German Heart and Vascular Center
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation
 Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Influence of Perioperative Hemodynamics on Spinal Cord Ischemia in Thoracoabdominal Aortic Repair
 Influence of Perioperative Hemodynamics on Spinal Cord Ischemia in Thoracoabdominal Aortic Repair Yujiro Kawanishi, MD, Kenji Okada, MD, Masamichi Matsumori, MD, Hiroshi Tanaka, MD, Teruo Yamashita, MD,
Influence of Perioperative Hemodynamics on Spinal Cord Ischemia in Thoracoabdominal Aortic Repair Yujiro Kawanishi, MD, Kenji Okada, MD, Masamichi Matsumori, MD, Hiroshi Tanaka, MD, Teruo Yamashita, MD,
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Optimal repair of acute aortic dissection
 Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Selective Visceral Perfusion during Thoracoabdominal Aortic Aneurysm Repair
 Original Article Selective Visceral Perfusion during Thoracoabdominal Aortic Aneurysm Repair Yukio Kuniyoshi, MD, PhD, Kageharu Koja, MD, PhD, Kazufumi Miyagi, MD, Tooru Uezu, MD, Satoshi Yamashiro, MD,
Original Article Selective Visceral Perfusion during Thoracoabdominal Aortic Aneurysm Repair Yukio Kuniyoshi, MD, PhD, Kageharu Koja, MD, PhD, Kazufumi Miyagi, MD, Tooru Uezu, MD, Satoshi Yamashiro, MD,
I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical Department National Taiwan University Hospital
 Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques
 Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques Tariq Almerey MD, January Moore BA, Houssam Farres MD, Richard Agnew MD, W. Andrew Oldenburg MD, Albert Hakaim MD Department of Vascular
Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques Tariq Almerey MD, January Moore BA, Houssam Farres MD, Richard Agnew MD, W. Andrew Oldenburg MD, Albert Hakaim MD Department of Vascular
THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR
 Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
The SPIDER-Graft for Thoracoabdominal Aortic Repair a feasability study in pigs
 The SPIDER-Graft for Thoracoabdominal Aortic Repair a feasability study in pigs Wipper S, Kölbel T, Manzoni D, Duprée A, Sandhu H, Nelis V, Debus ES University Heart Center Hamburg University Heart Center
The SPIDER-Graft for Thoracoabdominal Aortic Repair a feasability study in pigs Wipper S, Kölbel T, Manzoni D, Duprée A, Sandhu H, Nelis V, Debus ES University Heart Center Hamburg University Heart Center
Chairman and O. Wayne Isom Professor Department of Cardiothoracic Surgery Weill Cornell Medicine
 Leonard N. Girardi, M.D. Chairman and O. Wayne Isom Professor Department of Cardiothoracic Surgery Weill Cornell Medicine New York, New York Houston Aortic Symposium Houston, Texas February 23, 2017 weill.cornell.edu
Leonard N. Girardi, M.D. Chairman and O. Wayne Isom Professor Department of Cardiothoracic Surgery Weill Cornell Medicine New York, New York Houston Aortic Symposium Houston, Texas February 23, 2017 weill.cornell.edu
Protecting the brain and spinal cord in aortic arch surgery
 Keynote Lecture Series Protecting the brain and spinal cord in aortic arch surgery Lars G. Svensson Heart & Vascular Institute, Cleveland Clinic, Cleveland, OH, USA Correspondence to: Lars G. Svensson,
Keynote Lecture Series Protecting the brain and spinal cord in aortic arch surgery Lars G. Svensson Heart & Vascular Institute, Cleveland Clinic, Cleveland, OH, USA Correspondence to: Lars G. Svensson,
Open fenestration for complicated acute aortic B dissection
 Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Current treatment of Aortic Aneurysms and Dissections. Adam Keefer, MD, FACS Sean Hislop, MD, FACS
 Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
ORIGINAL ARTICLE. Systemic Temperature and Paralysis After Thoracoabdominal and Descending Aortic Operations
 ORIGINAL ARTICLE Systemic Temperature and Paralysis After Thoracoabdominal and Descending Aortic Operations Lars G. Svensson, MD, PhD; Lev Khitin, MD; Edward M. Nadolny, CCP; Wendy A. Kimmel, CCP Hypothesis:
ORIGINAL ARTICLE Systemic Temperature and Paralysis After Thoracoabdominal and Descending Aortic Operations Lars G. Svensson, MD, PhD; Lev Khitin, MD; Edward M. Nadolny, CCP; Wendy A. Kimmel, CCP Hypothesis:
Accepted Manuscript. Perioperative renal function and thoracoabdominal aneurysm repair: Where do we go from here? Leonard N. Girardi, M.D.
 Accepted Manuscript Perioperative renal function and thoracoabdominal aneurysm repair: Where do we go from here? Leonard N. Girardi, M.D. PII: S0022-5223(18)31804-X DOI: 10.1016/j.jtcvs.2018.06.057 Reference:
Accepted Manuscript Perioperative renal function and thoracoabdominal aneurysm repair: Where do we go from here? Leonard N. Girardi, M.D. PII: S0022-5223(18)31804-X DOI: 10.1016/j.jtcvs.2018.06.057 Reference:
Table I. Associated diseases
 Thoracic and thoracoabdominal aortic aneurysm repair using cardiopulmonary bypass, profound hypothermia, and circulatory arrest via left side of the chest incision Hazim J. Safi, MD, Charles C. Miller
Thoracic and thoracoabdominal aortic aneurysm repair using cardiopulmonary bypass, profound hypothermia, and circulatory arrest via left side of the chest incision Hazim J. Safi, MD, Charles C. Miller
Combination of Myogenic and Neurogenic Motor Evoked Potential Monitoring During Thoracoabdominal Aortic Surgery
 Hiroshima J. Med. Sci. Vol. 67, No. 4, 117~121, December, 2018 HIMJ 67 18 117 Combination of Myogenic and Neurogenic Motor Evoked Potential Monitoring During Thoracoabdominal Aortic Surgery Shinya TAKAHASHI
Hiroshima J. Med. Sci. Vol. 67, No. 4, 117~121, December, 2018 HIMJ 67 18 117 Combination of Myogenic and Neurogenic Motor Evoked Potential Monitoring During Thoracoabdominal Aortic Surgery Shinya TAKAHASHI
Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery
 Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery Are Young Patients More Likely to Develop Adverse Aortic Remodeling of the Remnant Aorta Over Time? Suk Jung Choo¹, Jihoon Kim¹,
Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery Are Young Patients More Likely to Develop Adverse Aortic Remodeling of the Remnant Aorta Over Time? Suk Jung Choo¹, Jihoon Kim¹,
Total arch replacement with separated graft technique and selective antegrade cerebral perfusion
 Masters of Cardiothoracic Surgery Total arch replacement with separated graft technique and selective antegrade cerebral perfusion Teruhisa Kazui 1,2 1 Hamamatsu University School of Medicine, Hamamatsu,
Masters of Cardiothoracic Surgery Total arch replacement with separated graft technique and selective antegrade cerebral perfusion Teruhisa Kazui 1,2 1 Hamamatsu University School of Medicine, Hamamatsu,
Reinhard Kopp, Karin Pfister, Beatrix Cucuruz, Konstantinos Gallis, Piotr M Kasprzak
 Immediate, delayed and late spinal cord ischemia after extended endovascular thoracoabdominal aortic repair Reinhard Kopp, Karin Pfister, Beatrix Cucuruz, Konstantinos Gallis, Piotr M Kasprzak Disclosure
Immediate, delayed and late spinal cord ischemia after extended endovascular thoracoabdominal aortic repair Reinhard Kopp, Karin Pfister, Beatrix Cucuruz, Konstantinos Gallis, Piotr M Kasprzak Disclosure
Thoracoabdominal aortic replacement for Crawford extent II aneurysm after thoracic endovascular aortic repair
 Original Article Thoracoabdominal aortic replacement for Crawford extent II aneurysm after thoracic endovascular aortic repair Haiou Hu, Tie Zheng, Junming Zhu, Yongmin Liu, Ruidong Qi, Lizhong Sun Department
Original Article Thoracoabdominal aortic replacement for Crawford extent II aneurysm after thoracic endovascular aortic repair Haiou Hu, Tie Zheng, Junming Zhu, Yongmin Liu, Ruidong Qi, Lizhong Sun Department
Cardiopulmonary Bypass for Thoracic Aortic Aneurysm: A Report on 488 Cases
 The Journal of The American Society of Extra-Corporeal Technology Cardiopulmonary Bypass for Thoracic Aortic Aneurysm: A Report on 488 Cases Yulong Guan, MD; Jing Yang, MD; Caihong Wan, MD; Meiling He;
The Journal of The American Society of Extra-Corporeal Technology Cardiopulmonary Bypass for Thoracic Aortic Aneurysm: A Report on 488 Cases Yulong Guan, MD; Jing Yang, MD; Caihong Wan, MD; Meiling He;
Abdominal Aortic Aneurysm - Part 1. Learning Objectives. Disclosure. University of Toronto Division of Vascular Surgery
 University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
Lumbar CSF Drains for Thoracic Aortic Surgery
 Lumbar CSF Drains for Thoracic Aortic Surgery John C. Klick, MD CASE CAG Why do them? Open descending thoracic aortic aneurysm repair (still the gold standard) has an incidence of postoperative paraplegia
Lumbar CSF Drains for Thoracic Aortic Surgery John C. Klick, MD CASE CAG Why do them? Open descending thoracic aortic aneurysm repair (still the gold standard) has an incidence of postoperative paraplegia
Type II arch hybrid debranching procedure
 Safeguards and Pitfalls Type II arch hybrid debranching procedure Prashanth Vallabhajosyula, Wilson Y. Szeto, Nimesh Desai, Caroline Komlo, Joseph E. Bavaria Division of Cardiovascular Surgery, University
Safeguards and Pitfalls Type II arch hybrid debranching procedure Prashanth Vallabhajosyula, Wilson Y. Szeto, Nimesh Desai, Caroline Komlo, Joseph E. Bavaria Division of Cardiovascular Surgery, University
debris + 3 debris debris debris Tel: ,3
 13 467 471 2004 debris + 3 13.2 15.47.0 6.5 7.7 0 3 25.012.5 7.0 0 13 467 471 2004 Tel: 075-251-5752 602-8566 463-1 2004 3 7 2004 5 18 30 1 2,3 4 2000 7 debris debris debris 7 13 4 Table 1 Patients profiles
13 467 471 2004 debris + 3 13.2 15.47.0 6.5 7.7 0 3 25.012.5 7.0 0 13 467 471 2004 Tel: 075-251-5752 602-8566 463-1 2004 3 7 2004 5 18 30 1 2,3 4 2000 7 debris debris debris 7 13 4 Table 1 Patients profiles
Surgical treatment of thoracic-abdominal aortic aneurysms
 Cardiovascular Disorders and Medicine Review Article ISSN: 2398-8878 Surgical treatment of thoracic-abdominal aortic aneurysms Marina Alves Jacintho de Mello*, Camila Alcalde Mazza and Edmo Atique Gabriel
Cardiovascular Disorders and Medicine Review Article ISSN: 2398-8878 Surgical treatment of thoracic-abdominal aortic aneurysms Marina Alves Jacintho de Mello*, Camila Alcalde Mazza and Edmo Atique Gabriel
INNOVATION IN CARDIOVASCULAR MEDICINE. AORTA CLINIC. Dr. Jaime Camacho M. Director, Aorta Clinic
 AORTA CLINIC Aorta Clinic Calle 163 A # 13 B- 60 Fundadores Building, 3rd floor Bogota D.C. Colombia Direct Telephone: 6672791 PBX: 667-2727 ext. 3149 e-mail: clinicadeaorta@cardioinfantil.org AORTA CLINIC.
AORTA CLINIC Aorta Clinic Calle 163 A # 13 B- 60 Fundadores Building, 3rd floor Bogota D.C. Colombia Direct Telephone: 6672791 PBX: 667-2727 ext. 3149 e-mail: clinicadeaorta@cardioinfantil.org AORTA CLINIC.
Gelweave TM. Thoracic and Thoracoabdominal Graft Geometries. Ante-Flo TM 4 Branch Plexus. Siena Valsalva TM Trifurcate Arch Graft. Coselli.
 Gelweave TM Thoracic and Thoracoabdominal Graft Geometries Ante-Flo TM 4 Branch Plexus Siena Valsalva TM Trifurcate Arch Graft Coselli Lupiae Product availability subject to local regulatory approval.
Gelweave TM Thoracic and Thoracoabdominal Graft Geometries Ante-Flo TM 4 Branch Plexus Siena Valsalva TM Trifurcate Arch Graft Coselli Lupiae Product availability subject to local regulatory approval.
Modification in aortic arch replacement surgery
 Gao et al. Journal of Cardiothoracic Surgery (2018) 13:21 DOI 10.1186/s13019-017-0689-y LETTER TO THE EDITOR Modification in aortic arch replacement surgery Feng Gao 1,2*, Yongjie Ye 2, Yongheng Zhang
Gao et al. Journal of Cardiothoracic Surgery (2018) 13:21 DOI 10.1186/s13019-017-0689-y LETTER TO THE EDITOR Modification in aortic arch replacement surgery Feng Gao 1,2*, Yongjie Ye 2, Yongheng Zhang
EACTS Adult Cardiac Database
 EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
Open surgical repair of thoracoabdominal aneurysms - the Massachusetts General Hospital experience
 Research Highlight Open surgical repair of thoracoabdominal aneurysms - the Massachusetts General Hospital experience Virendra I. Patel, Robert T. Lancaster, Mark F. Conrad, Richard P. Cambria Division
Research Highlight Open surgical repair of thoracoabdominal aneurysms - the Massachusetts General Hospital experience Virendra I. Patel, Robert T. Lancaster, Mark F. Conrad, Richard P. Cambria Division
Stanford Division of Vascular Surgery
 Stanford Division of Vascular Surgery Interesting Cases 10/11/10 Vascular Surgery HPI: 62yoM with h/o CAD, HTN, ETOH abuse. S/P EVAR in 5/08 for 6cm AAA and right CIA aneurysm. Cook 30x96mm Main Body 24
Stanford Division of Vascular Surgery Interesting Cases 10/11/10 Vascular Surgery HPI: 62yoM with h/o CAD, HTN, ETOH abuse. S/P EVAR in 5/08 for 6cm AAA and right CIA aneurysm. Cook 30x96mm Main Body 24
Endovascular Treatment of Malperfusion Syndrome
 Endovascular Treatment of Malperfusion Syndrome in Type B Aortic Dissection Department of Cardiology, Pusan National luniveristy i Hospital, Han Cheol Lee Endovascular Treatment Indication of Type B Aortic
Endovascular Treatment of Malperfusion Syndrome in Type B Aortic Dissection Department of Cardiology, Pusan National luniveristy i Hospital, Han Cheol Lee Endovascular Treatment Indication of Type B Aortic
Management of Acute Aortic Syndromes. M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria
 Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
3 : 37. Kirit Patel, USA CLASSIFICATION DIAGNOSIS
 3 : 37 Management of Aortic Aneurysms Clinical features and diagnosis of thoracic aortic aneurysm An aneurysm is currently defined as a localized dilatation of the aorta, 50 percent over the normal diameter,
3 : 37 Management of Aortic Aneurysms Clinical features and diagnosis of thoracic aortic aneurysm An aneurysm is currently defined as a localized dilatation of the aorta, 50 percent over the normal diameter,
Experience of endovascular procedures on abdominal and thoracic aorta in CA region
 Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Early- and medium-term results after aortic arch replacement with frozen elephant trunk techniques a single center study
 Featured Article Early- and medium-term results after aortic arch replacement with frozen elephant trunk techniques a single center study Sergey Leontyev*, Martin Misfeld*, Piroze Daviewala, Michael A.
Featured Article Early- and medium-term results after aortic arch replacement with frozen elephant trunk techniques a single center study Sergey Leontyev*, Martin Misfeld*, Piroze Daviewala, Michael A.
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy. Johannes Lammer Medical University Vienna, Austria
 Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Management of Endoleaks
 Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Lumbar Drain Management Thoracic Aortic Aneurysm Surgery
 Lumbar Drain Management Thoracic Aortic Aneurysm Surgery Presented By Tonya L. Page MSN, APRN, ACNP-BC What is a Lumbar drain? A small, flexible, soft plastic tube placed in the lower back (lumbar area)
Lumbar Drain Management Thoracic Aortic Aneurysm Surgery Presented By Tonya L. Page MSN, APRN, ACNP-BC What is a Lumbar drain? A small, flexible, soft plastic tube placed in the lower back (lumbar area)
Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology
 Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology Eduard Charchyan MD, PhD, Yurii Belov MD, PhD, Denis Breshenkov, Alexey
Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology Eduard Charchyan MD, PhD, Yurii Belov MD, PhD, Denis Breshenkov, Alexey
Thoracoabdominal Aorta: Advances and Novel Therapies
 Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
TAAA / Spinal Cord Protection
 TAAA / Spinal Cord Protection Hazim J. Safi, MD Professor and Chair Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science Center at Houston Memorial
TAAA / Spinal Cord Protection Hazim J. Safi, MD Professor and Chair Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science Center at Houston Memorial
Mortality and Paraplegia After Thoracoabdominal Aortic Aneurysm Repair: A Risk Factor Analysis
 ORIGINAL ARTICLES: CARDIOVASCULAR Mortality and Paraplegia After Thoracoabdominal Aortic Aneurysm Repair: A Risk Factor Analysis Joseph S. Coselli, MD, Scott A. LeMaire, MD, Charles C. Miller III, PhD,
ORIGINAL ARTICLES: CARDIOVASCULAR Mortality and Paraplegia After Thoracoabdominal Aortic Aneurysm Repair: A Risk Factor Analysis Joseph S. Coselli, MD, Scott A. LeMaire, MD, Charles C. Miller III, PhD,
AORTIC DISSECTION. DISSECTING ANEURYSMS OF THE AORTA or CLASSIFICATION
 DISSECTING ANEURYSMS OF THE AORTA or AORTIC DISSECTION CLASSIFICATION DeBakey classified aortic dissections into types I, II, and III :- Type I dissection the tear site originates in the ascending aorta,
DISSECTING ANEURYSMS OF THE AORTA or AORTIC DISSECTION CLASSIFICATION DeBakey classified aortic dissections into types I, II, and III :- Type I dissection the tear site originates in the ascending aorta,
University of Florida Department of Surgery. CardioThoracic Surgery VA Learning Objectives
 University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
Cannulation of the femoral artery with retrograde
 PROXIMAL AORTIC PERFUSION FOR COMPLEX ARCH AND DESCENDING AORTIC DISEASE Stephen Westaby, MS, FRCS Takahiro Katsumata, MD Objective: Cannulation of the femoral artery is used routinely for hypothermic
PROXIMAL AORTIC PERFUSION FOR COMPLEX ARCH AND DESCENDING AORTIC DISEASE Stephen Westaby, MS, FRCS Takahiro Katsumata, MD Objective: Cannulation of the femoral artery is used routinely for hypothermic
H. J. Safit, M. P. Campbell, C. C. Miller III, D. C. Iliopoulos, A. Khoynezhad, G. V. Letsou and P. J. Asimacopoulos
 Eur J Vasc Endovasc Surg 14, 118-124 (1997) Cerebral Spinal Fluid Drainage and Distal Aortic Perfusion Decrease the Incidence of Neurological Deficit: The Results of 343 Descending and Thoracoabdominal
Eur J Vasc Endovasc Surg 14, 118-124 (1997) Cerebral Spinal Fluid Drainage and Distal Aortic Perfusion Decrease the Incidence of Neurological Deficit: The Results of 343 Descending and Thoracoabdominal
Evolving Strategy and Results of Spinal Cord Protection in Type I and II Thoracoabdominal Aortic Aneurysm Repair
 Original Article Evolving Strategy and Results of Spinal Cord Protection in Type I and II Thoracoabdominal Aortic Aneurysm Repair Norihiko Shiiya, MD, Takashi Kunihara, MD, Kenji Matsuzaki, MD, and Keishu
Original Article Evolving Strategy and Results of Spinal Cord Protection in Type I and II Thoracoabdominal Aortic Aneurysm Repair Norihiko Shiiya, MD, Takashi Kunihara, MD, Kenji Matsuzaki, MD, and Keishu
Javier Marquez Graciani, MD Attending Dr F. Joglar
 Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Preoperative assessment of a patient for carotid endarterectomy
 Vascular Carotid endarterectomy Preoperative assessment of a patient for carotid endarterectomy Abdominal aortic aneuysm Thoracic aortic aneurysms Vascular 3.D.2.1 James Mitchell (December 24, 2003) Carotid
Vascular Carotid endarterectomy Preoperative assessment of a patient for carotid endarterectomy Abdominal aortic aneuysm Thoracic aortic aneurysms Vascular 3.D.2.1 James Mitchell (December 24, 2003) Carotid
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
How to Determine Tolerance for Branch Vessel Coverage
 How to Determine Tolerance for Branch Vessel Coverage Venita Chandra, MD Clinical Assistant Professor of Surgery Division of Stanford Medical School, Stanford, CA PNEC May 25 th, 2017 DISCLOSURES Venita
How to Determine Tolerance for Branch Vessel Coverage Venita Chandra, MD Clinical Assistant Professor of Surgery Division of Stanford Medical School, Stanford, CA PNEC May 25 th, 2017 DISCLOSURES Venita
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist. M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria
 Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Evidence Surgical aortic arch replacement with a Dacron
Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Evidence Surgical aortic arch replacement with a Dacron
Goals and Objectives. Assessment Methods/Tools
 CA-3 CARDIOVASCULAR ANESTHESIA ROTATION Minneapolis Veterans Administration Medical Center (VAMC) Rotation Site Director: Dr. Karen Ringsred Rotation Duration: 4 weeks Introduction: The patients at the
CA-3 CARDIOVASCULAR ANESTHESIA ROTATION Minneapolis Veterans Administration Medical Center (VAMC) Rotation Site Director: Dr. Karen Ringsred Rotation Duration: 4 weeks Introduction: The patients at the
Interesting Cases - A Case Report: Renal Cell Carcinoma With Tumor Mass In IVC And Heart. O Wenker, L Chaloupka, R Joswiak, D Thakar, C Wood, G Walsh
 ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 3 Number 2 Interesting Cases - A Case Report: Renal Cell Carcinoma With Tumor Mass In IVC And Heart O Wenker, L Chaloupka, R
ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 3 Number 2 Interesting Cases - A Case Report: Renal Cell Carcinoma With Tumor Mass In IVC And Heart O Wenker, L Chaloupka, R
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Preoperative and operative predictors of delayed neurologic deficit following repair of thoracoabdominal aortic aneurysm
 Preoperative and operative predictors of delayed neurologic deficit following repair of thoracoabdominal aortic aneurysm Anthony L. Estrera, MD a Charles C. Miller III, PhD a Tam T. T. Huynh, MD a Ali
Preoperative and operative predictors of delayed neurologic deficit following repair of thoracoabdominal aortic aneurysm Anthony L. Estrera, MD a Charles C. Miller III, PhD a Tam T. T. Huynh, MD a Ali
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation, radiofrequency, anesthetic considerations for, 479 489 Acute aortic syndrome, thoracic endovascular repair of, 457 462 aortic
Index Note: Page numbers of article titles are in boldface type. A Ablation, radiofrequency, anesthetic considerations for, 479 489 Acute aortic syndrome, thoracic endovascular repair of, 457 462 aortic
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
No Disclosure. Aortic Dissection in Japan. This. The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair
 No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns
 CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
Publicado : Interactive CardioVascular Thoracic Surgery 2011;12:650.
 Pulmonary embolism due to biological glue after repair of type A aortic dissection Jose Rubio Alvarez,MD, PhD, 1 Juan Sierra Quiroga, MD, PhD, 1 Anxo Martinez de Alegria MD 2, Jose-Manuel Martinez Comendador,
Pulmonary embolism due to biological glue after repair of type A aortic dissection Jose Rubio Alvarez,MD, PhD, 1 Juan Sierra Quiroga, MD, PhD, 1 Anxo Martinez de Alegria MD 2, Jose-Manuel Martinez Comendador,
Ascending Thoracic Aorta: Postsurgical CT Evaluation
 Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martinez Jimenez, MD GOALS Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martínez MD smartinez-jimenez@saint-lukes.org Saint
Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martinez Jimenez, MD GOALS Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martínez MD smartinez-jimenez@saint-lukes.org Saint
State of Art Hybrid Approach
 State of Art Hybrid Approach for Complex Aorta Diseases Won Ho Kim, MD Division of Cardiology, Eulji University Hospital Eulji University School of Medicine, Daejeon, Korea Introduction.Hybrid procedure
State of Art Hybrid Approach for Complex Aorta Diseases Won Ho Kim, MD Division of Cardiology, Eulji University Hospital Eulji University School of Medicine, Daejeon, Korea Introduction.Hybrid procedure
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection
 Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Advances in the Treatment of Acute Type A Dissection: An Integrated Approach
 Advances in the Treatment of Acute Type A Dissection: An Integrated Approach Joseph E. Bavaria, MD, Derek R. Brinster, MD, Robert C. Gorman, MD, Y. Joseph Woo, MD, Thomas Gleason, MD, and Alberto Pochettino,
Advances in the Treatment of Acute Type A Dissection: An Integrated Approach Joseph E. Bavaria, MD, Derek R. Brinster, MD, Robert C. Gorman, MD, Y. Joseph Woo, MD, Thomas Gleason, MD, and Alberto Pochettino,
THORACIC AORTIC DISSECTION
 The Essence of Aortic Dissection THORACIC AORTIC DISSECTION Aortic dissection can be classified as acute if it s onset has been less than 14 days or chronic if its onset has been more than 14 days. Mortality
The Essence of Aortic Dissection THORACIC AORTIC DISSECTION Aortic dissection can be classified as acute if it s onset has been less than 14 days or chronic if its onset has been more than 14 days. Mortality
2012 What is New in Aortic Surgery: Monitoring and Preventing Spinal Cord Injuries - Teamwork
 2012 What is New in Aortic Surgery: Monitoring and Preventing Spinal Cord Injuries - Teamwork George Silvay, MD, PhD Professor of Anesthesiology The Mount Sinai Medical Center New York, NY I would like
2012 What is New in Aortic Surgery: Monitoring and Preventing Spinal Cord Injuries - Teamwork George Silvay, MD, PhD Professor of Anesthesiology The Mount Sinai Medical Center New York, NY I would like
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Accepted Manuscript. Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi
 Accepted Manuscript Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi PII: S0022-5223(18)32552-2 DOI: 10.1016/j.jtcvs.2018.09.048 Reference: YMTC 13502
Accepted Manuscript Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi PII: S0022-5223(18)32552-2 DOI: 10.1016/j.jtcvs.2018.09.048 Reference: YMTC 13502
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies. Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018
 Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Major Vascular Anaesthesia where is the challenge. Dr B Brandner Consultant in Anaesthesia and Pain Management UCLH, London
 Major Vascular Anaesthesia where is the challenge Dr B Brandner Consultant in Anaesthesia and Pain Management UCLH, London Preoperative challenge Patient selection Patient optimisation Effective multidisciplinary
Major Vascular Anaesthesia where is the challenge Dr B Brandner Consultant in Anaesthesia and Pain Management UCLH, London Preoperative challenge Patient selection Patient optimisation Effective multidisciplinary
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
PACT module High risk surgical patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module High risk surgical patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Intravascular volume effect of Ringer s lactate Double-tracer BV measurement Blood 1097
PACT module High risk surgical patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Intravascular volume effect of Ringer s lactate Double-tracer BV measurement Blood 1097
Total Endovascular Repair Type A Dissection. Eric Herget Interventional Radiology
 Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
(Peripheral) Temperature and microcirculation
 Temperature and microcirculation") (Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
(Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
SELECTIVE ANTEGRADE TECHNIQUE OF CHOICE
 SELECTIVE ANTEGRADE CEREBRAL PERFUSION IS THE TECHNIQUE OF CHOICE MARKO TURINA University of Zurich Zurich, Switzerland What is so special about the operation on the aortic arch? Disease process is usually
SELECTIVE ANTEGRADE CEREBRAL PERFUSION IS THE TECHNIQUE OF CHOICE MARKO TURINA University of Zurich Zurich, Switzerland What is so special about the operation on the aortic arch? Disease process is usually
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial
 An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial wall (intima, media, and adventitia) or the attenuated
An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial wall (intima, media, and adventitia) or the attenuated
Toward Total Endovascular Therapy of the Aorta. Adam W. Beck, MD. Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy
 Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Endovascular Aortic Repair in the Descending Thoraco-Abdominal Aorta A Guide to Perioperative Management
 Page 1 Endovascular Aortic Repair in the Descending Thoraco-Abdominal Aorta A Guide to Perioperative Management Maged Argalious,M.D., MBA Cleveland, Ohio I Introduction In 1991, the first cases of endovascular
Page 1 Endovascular Aortic Repair in the Descending Thoraco-Abdominal Aorta A Guide to Perioperative Management Maged Argalious,M.D., MBA Cleveland, Ohio I Introduction In 1991, the first cases of endovascular
Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication vs Benefit? Mortality? Morbidity?
 Preoperative intraaortic balloon counterpulsation in high-risk CABG Stefan Klotz, M.D. Preoperative IABP in high-risk CABG Questions?? Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication
Preoperative intraaortic balloon counterpulsation in high-risk CABG Stefan Klotz, M.D. Preoperative IABP in high-risk CABG Questions?? Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication