Percutaneous Approaches to Aortic Disease in 2018
|
|
|
- Phillip Nicholson
- 6 years ago
- Views:
Transcription

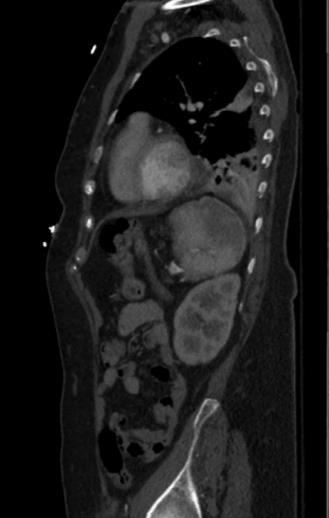
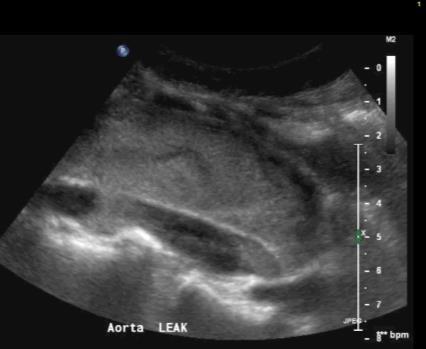
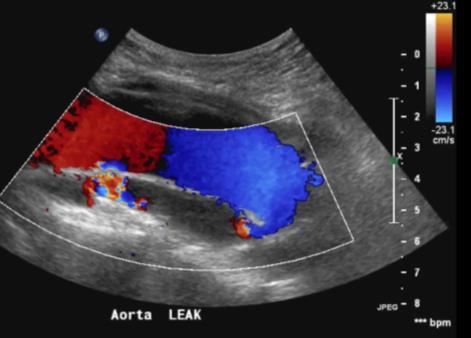
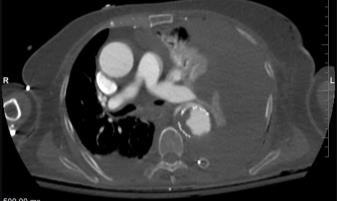
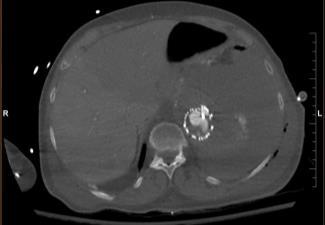
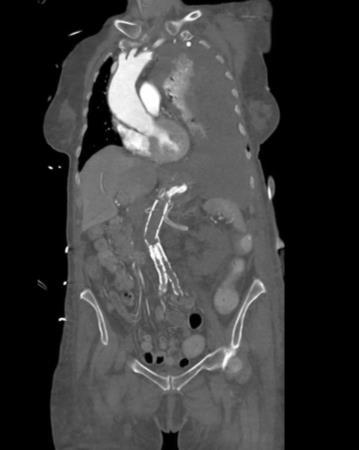
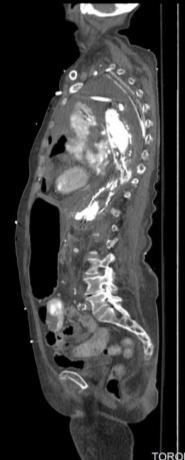
1 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper abdominal pain for 1-2 weeks GP sent her for abdominal ultrasound Possible thoracic aortic aneurysm Sent to ER where she was found to be hypertensive CT 5.8 cm thoracoabdominal aneurysm, intramural hematoma, pleural effusions R 1

2 What is the rate of rupture over a lifespan? A. 20% B. 40% C. 60% D. 80% E. 100% Thoracoabdominal Aortic Aneurysm Incidence of thoracic aortic aneurysms is 10 per 100,000 person years Natural history of aneurysms is dissection or rupture Up to 80% will eventually rupture 10-20% 5-year survival for those untreated Females develop TAA later in life then men but have a higher risk of rupture Advanced age is a risk for rupture COPD increases the risk of rupture by 3.6 times Diameter is related to rupture risk Annual risk is 7% when >6 cm R 2



3 Classification Safi s modification to Crawford Type 1 Type 2 Type 3 Type 4 Type 5 6 th intercostal space Diaphragm Lt SC to renal arteries Lt SC to aortic bifurcation Below 6 th space to abdominal Below diaphragm to aortic bifurcation Below 6 th space to visceral segments Case Type 1 Distal to subclavian until SMA and celiac, no involvement at renal arteries Despite controlling blood pressure repeat CT 2-days later demonstrated 5 mm increase in the intramural hematoma Patient remained symptomatic 3
4 What would you do? A. Medical management B. Intervention (surgery/percutaneous) What would you do? A. Medical management B. Intervention (surgery/percutaneous) 4
5 Case Due to multiple comorbidities, planned for TEVAR Indications For Repair Rupture Acute dissection resulting in malperfusion or other life altering complications Symptomatic states regardless of size/extent Pain consistent with rupture and unexplained by other causes Compression of adjacent organs 95% occur without symptoms Documented enlargement > 1 cm/year or substantial growth approaching absolute size criteria Absolute size >6.5 cm or >6.0 cm in patients with connective tissue disorders Absolute size criteria must be adjusted in patients of extreme of size Cutoffs determined based on risk of rupture>mortality of the proposed procedure 5





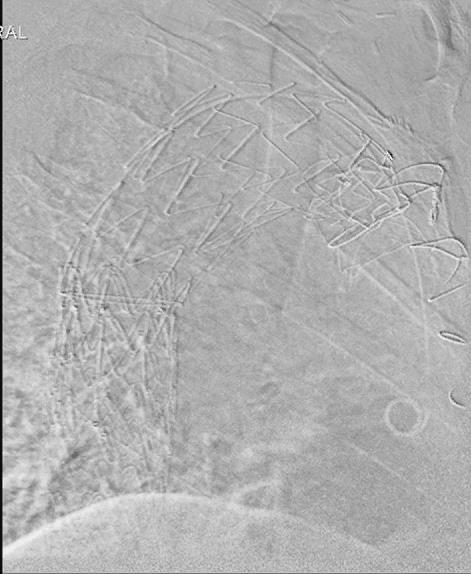
6 Thoracic Endovascular Repair (TEVAR) Minimally invasive approach Placing a stent-graft in the thoracoabdominal aorta for the treatment of a variety of thoracic aortic pathologies Devices approved in US differ in terms of metallic support, radial support, flexibility GORE TAG Cook TX2 Medtronic Valiant Bolton Relay TEVAR vs Surgery No RCT directly comparing open and endovascular repair of the thoracic aorta Survival Spinal Cord Injury Better outcomes due to: lack of sternotomy and thoracotomy No need to cross-clamp the aorta less blood loss lower incidence of end-organ ischemia fewer episodes of respiratory dependency quicker recovery Circulation. 2008;118:
7 Indications for EVAR Thoracic aortic aneurysms (original approval in 2005) Traumatic aortic injury Systemic anticoagulation can be held for those with concomitant head injury Used in younger patients but long-term data is not available and surveillance increases the cumulative radiation dose Complicated type B aortic dissection Penetrating aortic ulcer/intramural hematoma Aortoesophageal fistula Treatment of EVAR complications Patient Selection Initially for those who were not suitable for open surgery Individualized approach Age Patient risk factors for perioperative morbidity and mortality Not ideal for infected aneurysms or connective tissue disease Not for those who do not meet the anatomic criteria to place any of the available endografts Inability to comply with surveillance (relative) 7



8 Procedural Considerations 1. Aortic anatomy 2. Extent of aortic disease 3. Available landing zones location of attachment and length of coverage relates to the risk and complexity of the procedure as well as component selection and stresses on the devices Ann Cardiothorac Surg 2016;5(3): Planning -Imaging Computed tomography angiography Information on external and endoluminal diameter of the aorta at the proximal and distal seal zones length of aortic coverage degree of angulation and tortuosity of the aorta important side branches thrombus burden calcification Magnetic resonance angiography can be used but does not demonstrate vessel wall calcification well 8

:738-43 Debranching When a graft covers important aortic side branches, open vascular surgery to bypass these vessels may be needed prior to thoracic stent-grafting placement Surgery can be")
9 Planning Generally, a 2-cm length of normal diameter aorta is required to achieve a seal (proximal and distal) Device deployment close to or within the arch must closely appose the "inner curve" of the arch Increase risk of graft collapse, migration, and failure of aneurysm exclusion If the proximal end of the graft is oriented towards the apex of such a curve --"bird-beaking" Suitable illiac artery morphology is required for delivery Specific parameters for individual devices are given in the instructions for use (IFU) for each device bird-beaking Journal of Endovascular Therapy 17(6): Debranching When a graft covers important aortic side branches, open vascular surgery to bypass these vessels may be needed prior to thoracic stent-grafting placement Surgery can be avoided by using combined fenestrated or branched abdominal aortic endografts in situ fenetration with a needle or laser during emergencies 9



10 Post Op Surveillance CT angiography within 1 month 6 months Then yearly Case Post operatively, she developed lower limb weakness Spinal drain was inserted and she commenced hyperbaric treatment 10
11 Complications Iliofemoral Access Ischemic Spinal Cerebrovascular Extremity Visceral Post-Implantation Syndrome Fistulas Device Aortoesophageal Aortopulmonary Leaks Migration Infolding/Collapse Separation Perioperative Morbidity and Mortality Perioperative mortality Iliofemoral Access Complication Ischemic Complications Elective 1.9-3% Emergent ~20% 12% Spinal Chord 3-11% Cerebral vascular 4-8% Extremity 8-26% Risk is comparable to open surgery Risk related to amount of thoracic coverage, perioperative hypotension and long procedure duration May be reduced with prophylactic spinal drain placement Risk is comparable to open surgery Risk factors include: proximal deployment of the graft; presence of mobile atheroma in the arch; and prior stroke Risk comes from covering subclavian artery Avoid by bypassing However, perioperative mortality and other complications may be increased Risk of death associated with degree of renal dysfunction Visceral ~14% occurs with coverage of the celiac axis 11



12 Post Implantation Syndrome Occurs early postoperative period Characterized by leukocytosis, fever, and elevation of inflammatory mediators such as C-reactive protein, IL-6, and TNF-alpha Due to endothelial activation by the endoprosthesis For thoracic aortic stent-grafts, development of either unilateral or bilateral reactive pleural effusions is not uncommon Incidence of 37-73% Treatment?? supportive Late Complications - Fistulas Aortobronchial 33% mortality Aortopulmonary 45% mortality Treat with EVAR+surgery J Am Coll Cardiol Intv 2009;2:
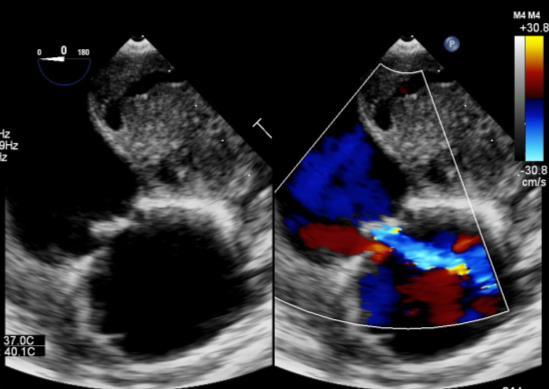
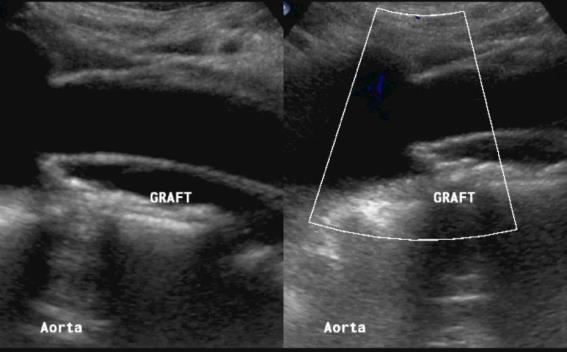

13 Complications -Endoleak % Post open aortic graft for AAA Ultrasound Contrast Improves Diagnosis Courtesy: H Leong-Poi 13
 and pooled specificity is 0.782 (CI 0.741 0.820).")

 Type V (endotension) Expansion of an aortic aneurysm in the absence")
14 8 articles (n = 454 pts) Pooled sensitivity of CEUS at detecting endoleak is (CI ) and pooled specificity is (CI ). Types of Endoleaks after EVAR Type I Perigraft flow due to inadequate graft seal Type II Branch arteries backbleed because of collateral flow Type III Persistent flow between the segments of a modular graft Type IV flow through endograft material (graft porosity) Type V (endotension) Expansion of an aortic aneurysm in the absence of demonstrable endoleak 14
 no intervention If persistent (>6 months) intervene Endovascular repair No intervention.")

15 Management of Endoleaks after EVAR Type I perigraft flow due to inadequate seal II branch artery backbleed III flow between segments IV graft porosity V - endotension Endovascular repair Management Unclear. Observation. If transient (<6 months) no intervention If persistent (>6 months) intervene Endovascular repair No intervention. Resolves spontaneously with normalization of coagulation profile Exclude undiagnosed leak/thrombus. If no cause discovered, open surgical conversion is required if aneurysm sac grows Device Complications Device Infolding/Collapse Occurs primarily in young trauma patients Related to severe proximal aortic angulation or to oversizing the device at the time of placement Patients present with symptoms of acute aortic occlusion Journal ofvascular Surgery, Volume 55, Issue 3, March 2012, Pages




16 Device Complications - Migration Baseline 6-months >10 mm caudally % over 6-12 month period Causes excessive over-sizing tortuous seal zone anatomy J Vasc Surg 2008;48:54-63 Device Complications Device Separation Occurs in cases of multiple overlapping stents 16

17 Most Device Complications Are Managed with a Second Intervention Rate is between % depending on duration of follow-up J Vasc Surg March ; 59(3): Survival depends on original etiology J Thorac Cardiovasc Surg 2015;149:


18 Case PEA arrest during hyperbaric treatment CXR Case 18

19 Summary For patients with or without involvement of the abdominal aorta, endovascular stent-grafting is a reasonable alternative to open surgery There is a significant rate of secondary intervention required following stent-grafting for endoleak, graft migration, and progression of the underlying disease that indicated the endograft However, due to decreased perioperative morbidity, this approach makes it preferable to open repair for many indications Routine follow-up imaging is mandatory Thank you for listening 19
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
My personal experience with INCRAFT in standard and challenging cases
 My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
Redo treatment and open conversion after TEVAR
 Redo treatment and open conversion after TEVAR Roberto Chiesa Vascular Surgery, Vita-Salute University Scientific Institute San Raffaele Milan, Italy Number of procedures Off-Label indications for TEVAR
Redo treatment and open conversion after TEVAR Roberto Chiesa Vascular Surgery, Vita-Salute University Scientific Institute San Raffaele Milan, Italy Number of procedures Off-Label indications for TEVAR
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Endoanchor-assisted TEVAR
 Endoanchor-assisted TEVAR May 29, 2015 NCVH2015 Grayson H. Wheatley III, MD Director of Aortic and Endovascular Surgery Associate Professor of Surgery Temple University School of Medicine Disclosures Consultant
Endoanchor-assisted TEVAR May 29, 2015 NCVH2015 Grayson H. Wheatley III, MD Director of Aortic and Endovascular Surgery Associate Professor of Surgery Temple University School of Medicine Disclosures Consultant
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry
 University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Thoracoabdominal Aorta: Advances and Novel Therapies
 Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
3 : 37. Kirit Patel, USA CLASSIFICATION DIAGNOSIS
 3 : 37 Management of Aortic Aneurysms Clinical features and diagnosis of thoracic aortic aneurysm An aneurysm is currently defined as a localized dilatation of the aorta, 50 percent over the normal diameter,
3 : 37 Management of Aortic Aneurysms Clinical features and diagnosis of thoracic aortic aneurysm An aneurysm is currently defined as a localized dilatation of the aorta, 50 percent over the normal diameter,
COMPLICATIONS OF TEVAR
 COMPLICATIONS OF TEVAR P. Bergeron, A.Petrosyan, F.Markatis, T.Abdulamit, J.-C. Trastour IMAD CONGRESS 2010 Liège Belgium BACKGROUND Stentgrafting is a recognized treatment for TAA & TAD and has been proposed
COMPLICATIONS OF TEVAR P. Bergeron, A.Petrosyan, F.Markatis, T.Abdulamit, J.-C. Trastour IMAD CONGRESS 2010 Liège Belgium BACKGROUND Stentgrafting is a recognized treatment for TAA & TAD and has been proposed
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations
 The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System
 Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System K. Oikonomou Department of Vascular Surgery Regensburg University Disclosures W.L. Gore & Associates Sponsored Presentation
Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System K. Oikonomou Department of Vascular Surgery Regensburg University Disclosures W.L. Gore & Associates Sponsored Presentation
How to achieve a successful proximal sealing in TEVAR? Pr L Canaud
 How to achieve a successful proximal sealing in TEVAR? Pr L Canaud CHU de Montpellier France Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic. Proximal neck
How to achieve a successful proximal sealing in TEVAR? Pr L Canaud CHU de Montpellier France Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic. Proximal neck
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment
 Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical Department National Taiwan University Hospital
 Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Experience of endovascular procedures on abdominal and thoracic aorta in CA region
 Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Management of Endoleaks
 Management of Endoleaks Murray Shames, MD Professor and Chief, Director Tampa General Hospital Aortic Program Vice Chair of Research, Dept. of Surgery Conflict of Interests: Speaker: Gore, Medtronic, Cook
Management of Endoleaks Murray Shames, MD Professor and Chief, Director Tampa General Hospital Aortic Program Vice Chair of Research, Dept. of Surgery Conflict of Interests: Speaker: Gore, Medtronic, Cook
Exceptions to the Rules: Abdominal and Thoracic Aneurysms
 Exceptions to the Rules: Abdominal and Thoracic Aneurysms Jason Bayne MD, FRCSC Vascular Surgery Jewish General Hospital Assistant Professor, Program Director McGill University Objectives Risk factors
Exceptions to the Rules: Abdominal and Thoracic Aneurysms Jason Bayne MD, FRCSC Vascular Surgery Jewish General Hospital Assistant Professor, Program Director McGill University Objectives Risk factors
State of Art Hybrid Approach
 State of Art Hybrid Approach for Complex Aorta Diseases Won Ho Kim, MD Division of Cardiology, Eulji University Hospital Eulji University School of Medicine, Daejeon, Korea Introduction.Hybrid procedure
State of Art Hybrid Approach for Complex Aorta Diseases Won Ho Kim, MD Division of Cardiology, Eulji University Hospital Eulji University School of Medicine, Daejeon, Korea Introduction.Hybrid procedure
UC SF. Disclosures. Thoracic Endovascular Aortic Repair 4/24/2009. Management of Acute Dissections: Is There Still a Role for Open Surgery?
 UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Optimal Treatment of Chronic Dissection
 Optimal Treatment of Chronic Dissection Chun-Che Shih 施俊哲 MD, Ph.D. Chief, Professor Institute of Clinical Medicine National Yang Ming University Division of Cardiovascular Surgery Taipei Veterans General
Optimal Treatment of Chronic Dissection Chun-Che Shih 施俊哲 MD, Ph.D. Chief, Professor Institute of Clinical Medicine National Yang Ming University Division of Cardiovascular Surgery Taipei Veterans General
Abdominal Aortic Aneurysm - Part 1. Learning Objectives. Disclosure. University of Toronto Division of Vascular Surgery
 University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR
 Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Aortic Arch pathology options: Open,Hybrid, fenestration, Chimney or branched stent-graft?
 Aortic Arch pathology options: Open,Hybrid, fenestration, Chimney or branched stent-graft? Chang Shu, M.D., Ph.D Vascular Surgery Center National Center for Cardiovascular Diseases. Fuwai Hospital, CAMS
Aortic Arch pathology options: Open,Hybrid, fenestration, Chimney or branched stent-graft? Chang Shu, M.D., Ph.D Vascular Surgery Center National Center for Cardiovascular Diseases. Fuwai Hospital, CAMS
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX
 FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
Title. Different arch branched devices are available, is morphology the. main criteria of choice? Ciro Ferrer, MD
 Different arch branched devices are available, is morphology the Title main criteria of choice? Ciro Ferrer, MD Vascular Surgery Unit Sapienza University of Rome Disclosure Speaker name: Ciro Ferrer Proctoring/speaking
Different arch branched devices are available, is morphology the Title main criteria of choice? Ciro Ferrer, MD Vascular Surgery Unit Sapienza University of Rome Disclosure Speaker name: Ciro Ferrer Proctoring/speaking
Endovascular aortic stent grafts have forever
 Identifying the Appropriate Thoracic Device Size How to correctly size a thoracic device in diameter, landing zone, and length. BY MICHAEL E. BARFIELD, MD, AND THOMAS S. MALDONADO, MD Endovascular aortic
Identifying the Appropriate Thoracic Device Size How to correctly size a thoracic device in diameter, landing zone, and length. BY MICHAEL E. BARFIELD, MD, AND THOMAS S. MALDONADO, MD Endovascular aortic
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Current State of Thoracic Branch Devices and Ongoing Clinical Trials
 Current State of Thoracic Branch Devices and Ongoing Clinical Trials Hiroo Takayama, MD, PhD Associate Professor of Surgery Director of Cardiovascular Institute Co-Director of Aortic Center NY Presbyterian/Columbia
Current State of Thoracic Branch Devices and Ongoing Clinical Trials Hiroo Takayama, MD, PhD Associate Professor of Surgery Director of Cardiovascular Institute Co-Director of Aortic Center NY Presbyterian/Columbia
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY
 SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation
 Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Development of a Branched LSA Endograft & Ascending Aorta Endograft
 Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES
 CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES A SERIES OF THREE CASE REPORTS Joel Sousa Department of Department of Angiology and Vascular Surgery Hospital S. João, Porto,
CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES A SERIES OF THREE CASE REPORTS Joel Sousa Department of Department of Angiology and Vascular Surgery Hospital S. João, Porto,
Durability of The Endurant Stent-Graft through 5 Years
 Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
symptomatic aneurysms or aneurysms that grow >1cm/yr
 1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion
 Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair
 583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
Disclosures. EVAR follow-up: actual recommendation. EVAR follow-up: critical issues
 Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan
 The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
THE THE MORE MORE NATURAL APPROACH TO OPTIMAL FIT
 THE THE MORE MORE NATURAL APPROACH Natural Approach TO Optimal Fit TO OPTIMAL FIT Conformability without Compromise THE STANDARD IN Conformability AND Designed for flexibility and conformability in tortuous
THE THE MORE MORE NATURAL APPROACH Natural Approach TO Optimal Fit TO OPTIMAL FIT Conformability without Compromise THE STANDARD IN Conformability AND Designed for flexibility and conformability in tortuous
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
Anatomical challenges in EVAR
 Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Distal Arch and Descending Aorta: What Is the Optimal Therapy in 2017?
 Distal Arch and Descending Aorta: What Is the Optimal Therapy in 2017? Eric E. Roselli, MD Chief, Adult Cardiac Surgery Director, Aorta Center Heart and Vascular Institute, Cleveland Clinic Disclosures
Distal Arch and Descending Aorta: What Is the Optimal Therapy in 2017? Eric E. Roselli, MD Chief, Adult Cardiac Surgery Director, Aorta Center Heart and Vascular Institute, Cleveland Clinic Disclosures
Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
 Young-Guk Ko, M.D., Dangas G, J Am Coll Cardiol Intv 2012;5:1071 All-cause Mortality Dangas Severance G, J Am Coll Cardiovascular Cardiol Intv Hospital, 2012;5:1071 Yonsei University Health System Aneurysm-related
Young-Guk Ko, M.D., Dangas G, J Am Coll Cardiol Intv 2012;5:1071 All-cause Mortality Dangas Severance G, J Am Coll Cardiovascular Cardiol Intv Hospital, 2012;5:1071 Yonsei University Health System Aneurysm-related
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Description. Section: Surgery Effective Date: April 15, Subsection: Surgery Original Policy Date: December 6, 2012 Subject:
 Last Review Status/Date: March 2015 Page: 1 of 6 Description Wireless sensors implanted in an aortic aneurysm sac after endovascular repair are being investigated to measure post procedural pressure. It
Last Review Status/Date: March 2015 Page: 1 of 6 Description Wireless sensors implanted in an aortic aneurysm sac after endovascular repair are being investigated to measure post procedural pressure. It
Advances in Treatment of Traumatic Aortic Transection
 Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
FLEXIBLE, BALOON EXPANDABLE
 EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
INCRAFT system: Update from the Pivotal INSPIRATION Study
 INCRAFT system: Update from the Pivotal INSPIRATION Study Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh
INCRAFT system: Update from the Pivotal INSPIRATION Study Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh
No Disclosure. Aortic Dissection in Japan. This. The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair
 No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
P Paraplegia abdominal aortic aneurysm repair, 52 paraparesis, 52 pathophysiology, 51 rates and endografts, 51 two-stage approach, 129
 A AAA. See Abdominal aortic aneurysm (AAA) Abdominal aortic aneurysm (AAA). See also Abdominal aortic pathologies advantage, IVUS, 20 asymptomatic infrarenal, 154 device selection and treatment, 19 20
A AAA. See Abdominal aortic aneurysm (AAA) Abdominal aortic aneurysm (AAA). See also Abdominal aortic pathologies advantage, IVUS, 20 asymptomatic infrarenal, 154 device selection and treatment, 19 20
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients
 ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
Objective assessment of current stent grafts: which graft for which lesion. Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France
 Objective assessment of current stent grafts: which graft for which lesion Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France Conflict of interest: none 1 Introduction Different diseases
Objective assessment of current stent grafts: which graft for which lesion Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France Conflict of interest: none 1 Introduction Different diseases
EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED.
 EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED. A/Prof. B. Patrice Mwipatayi MD, MMed (Surg), MClinEd (Melb), FCS, FRACS Department of Vascular Surgery, Royal
EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED. A/Prof. B. Patrice Mwipatayi MD, MMed (Surg), MClinEd (Melb), FCS, FRACS Department of Vascular Surgery, Royal
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy. Johannes Lammer Medical University Vienna, Austria
 Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability. Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands
 GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
Clinical experience with a new thoracic stent graft system (Ankura TM ). Procedural analysis, 30 days and 6-month results in a single center study
. Procedural analysis, 30 days and 6-month results in a single center study") Clinical experience with a new thoracic stent graft system (Ankura TM ). Procedural analysis, 30 days and 6-month results in a single center study Theodoros Kratimenos, MD Consultant, Interventional Radiologist
Clinical experience with a new thoracic stent graft system (Ankura TM ). Procedural analysis, 30 days and 6-month results in a single center study Theodoros Kratimenos, MD Consultant, Interventional Radiologist
Optimizing Accuracy of Aortic Stent Grafts in Short Necks
 Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Arch Repair with the Bolton Medical RelayBranch Thoracic Stent-graft system: Multicenter experience
 Arch Repair with the Bolton Medical RelayBranch Thoracic Stent-graft system: Multicenter experience Joost van Herwaarden, MD, PhD University Medical Center, Utrecht Disclosure I have the following potential
Arch Repair with the Bolton Medical RelayBranch Thoracic Stent-graft system: Multicenter experience Joost van Herwaarden, MD, PhD University Medical Center, Utrecht Disclosure I have the following potential
Jean M. Panneton, MD, FRCSC, FACS. Professor of Surgery, Chief & Program Director Division of Vascular Surgery. Norfolk, VA
 Jean M. Panneton, MD, FRCSC, FACS Professor of Surgery, Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School Norfolk, VA The Houston Aortic Symposium Houston TX, February
Jean M. Panneton, MD, FRCSC, FACS Professor of Surgery, Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School Norfolk, VA The Houston Aortic Symposium Houston TX, February
Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft
 MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
Toward Total Endovascular Therapy of the Aorta. Adam W. Beck, MD. Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy
 Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Hostile Neck During EVAR, The Role Of Endoanchores
 Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
Anatomical applicability of current off-the-shelf branched endografts in thoracoabdominal aortic aneurysms managed by open surgery.
 Leipzig Interventional Course Update on clinical trials Tuesday, January 30 th, 2018 Anatomical applicability of current off-the-shelf branched endografts in thoracoabdominal aortic aneurysms managed by
Leipzig Interventional Course Update on clinical trials Tuesday, January 30 th, 2018 Anatomical applicability of current off-the-shelf branched endografts in thoracoabdominal aortic aneurysms managed by
Endovascular options of treating iliac aneurysms
 Endovascular options of treating iliac aneurysms Marek Majewski Department of Vascular Surgery of P. Desgranges Henri Mondor Hospital University Paris XII Créteil, France Common Iliac Artery Aneurysms
Endovascular options of treating iliac aneurysms Marek Majewski Department of Vascular Surgery of P. Desgranges Henri Mondor Hospital University Paris XII Créteil, France Common Iliac Artery Aneurysms
Hostile Proximal Neck: A New Conformable EVAR Device
 Hostile Proximal Neck: A New Conformable EVAR Device Young-Guk Ko, M.D., Seoul, Korea Currently Available Devices for EVAR in Korea, 2018 Zenith Flex, Cook Endurant IIs, Medtronic INCRAFT, Cordis AFX2,
Hostile Proximal Neck: A New Conformable EVAR Device Young-Guk Ko, M.D., Seoul, Korea Currently Available Devices for EVAR in Korea, 2018 Zenith Flex, Cook Endurant IIs, Medtronic INCRAFT, Cordis AFX2,
Aortic stents, types, selection, tricks in deployment.
 Aortic stents, types, selection, tricks in deployment. Hamdy Soliman.M.D,FSCAI Consultant of Cardiology&Head of Endovascular Unit National Heart Institute Endovascular Treatment of Thoracic Aortic Aneurysms
Aortic stents, types, selection, tricks in deployment. Hamdy Soliman.M.D,FSCAI Consultant of Cardiology&Head of Endovascular Unit National Heart Institute Endovascular Treatment of Thoracic Aortic Aneurysms
Management of Acute Aortic Syndromes. M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria
 Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts
 Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Complications of endovascular aneurysm repair of the thoracic and abdominal aorta: evaluation and management
 Review Article Complications of endovascular aneurysm repair of the thoracic and abdominal aorta: evaluation and management Dania Daye, T. Gregory Walker Department of Radiology, Massachusetts General
Review Article Complications of endovascular aneurysm repair of the thoracic and abdominal aorta: evaluation and management Dania Daye, T. Gregory Walker Department of Radiology, Massachusetts General
Description. Section: Surgery Effective Date: October 15, 2016 Subsection: Surgery Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 30 Description Thoracic endovascular aneurysm repair (TEVAR) involves the percutaneous placement of a stent graft in the descending thoracic or thoracoabdominal
Last Review Status/Date: September 2016 Page: 1 of 30 Description Thoracic endovascular aneurysm repair (TEVAR) involves the percutaneous placement of a stent graft in the descending thoracic or thoracoabdominal
Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2017 Origination: 5/2006 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2017 Origination: 5/2006 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2018 Origination: 5/2006 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2018 Origination: 5/2006 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
I have the following financial relationships to disclose:
 Novel Approaches to Endovascular Management of Aortic Aneurysms Rodney A White, MD Medical Director, Vascular Services MemorialCare Heart & Vascular Institute Long Beach Memorial Hospital Long Beach, California
Novel Approaches to Endovascular Management of Aortic Aneurysms Rodney A White, MD Medical Director, Vascular Services MemorialCare Heart & Vascular Institute Long Beach Memorial Hospital Long Beach, California
How to manage the left subclavian and left vertebral artery during TEVAR
 How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
DISCLOSURES ISOLATED DTA LESION? TYPE B DISSECTIONS TREATMENT OPTIONS
 Endovascular Repair of Aortic Arch Pathologies; What is available/possible in the U.S. in 2018? Kaiser Permanente Endovascular Symposium 6/2/18 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery
Endovascular Repair of Aortic Arch Pathologies; What is available/possible in the U.S. in 2018? Kaiser Permanente Endovascular Symposium 6/2/18 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies. Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018
 Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Development of Stent Graft. Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection.
 Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
DIFFICULT ACCESS REMAINS A CONTRAINDICATION FOR EVAR APOSTOLOS K. TASSIOPOULOS, MD, FACS PROFESSOR AND CHIEF DIVISION OF VASCULAR SURGERY
 DIFFICULT ACCESS REMAINS A CONTRAINDICATION FOR EVAR APOSTOLOS K. TASSIOPOULOS, MD, FACS PROFESSOR AND CHIEF DIVISION OF VASCULAR SURGERY Disclosures Speaker Bureau: - Medtronic - Cook Medical - Bolton
DIFFICULT ACCESS REMAINS A CONTRAINDICATION FOR EVAR APOSTOLOS K. TASSIOPOULOS, MD, FACS PROFESSOR AND CHIEF DIVISION OF VASCULAR SURGERY Disclosures Speaker Bureau: - Medtronic - Cook Medical - Bolton
Associate Professor Walter W. Buckley Endowed Chair in Research Cleveland Clinic Lerner College of Medicine-CWRU. Houston Aortic Symposium 2017
 Matthew J. Eagleton, MD Associate Professor Walter W. Buckley Endowed Chair in Research Cleveland Clinic Lerner College of Medicine-CWRU Houston Aortic Symposium 2017 Aortica: Advisory Board Centerline
Matthew J. Eagleton, MD Associate Professor Walter W. Buckley Endowed Chair in Research Cleveland Clinic Lerner College of Medicine-CWRU Houston Aortic Symposium 2017 Aortica: Advisory Board Centerline
Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND
 Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND Thoracic Aortic Trauma In USA and CANADA 7500-8000 die of blunt thoracic aortic
Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND Thoracic Aortic Trauma In USA and CANADA 7500-8000 die of blunt thoracic aortic
Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques
 Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques Tariq Almerey MD, January Moore BA, Houssam Farres MD, Richard Agnew MD, W. Andrew Oldenburg MD, Albert Hakaim MD Department of Vascular
Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques Tariq Almerey MD, January Moore BA, Houssam Farres MD, Richard Agnew MD, W. Andrew Oldenburg MD, Albert Hakaim MD Department of Vascular
UC SF An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.
 Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.") An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,