Transfusion Medicine III
|
|
|
- Irma Arnold
- 5 years ago
- Views:
Transcription



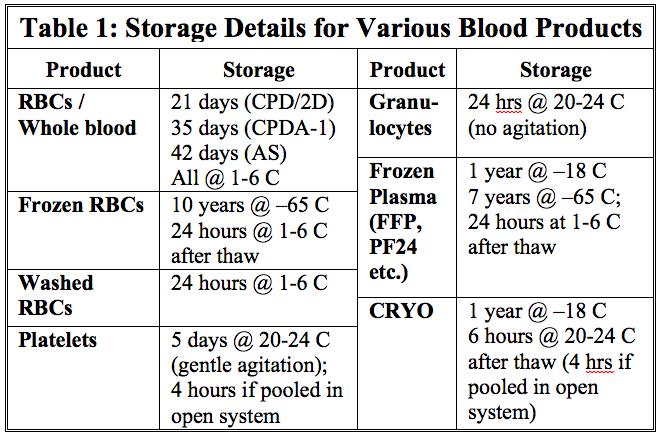
1 Transfusion Medicine III Blood Products from Collection to Use D. Joe Chaffin, MD Loma Linda University 3/5/2019


2 FFP WB RBC
3
 ACD (70 ml) Shelf Life (RBC) Labeled RBCs in 35 Day Shelf Life Wait 24 hours >75% survival CPDA-1 (70")
4 Anticoagulant/Preservatives Why we need 21 Day Shelf Life Prevent clotting Keep cells fresh CPD (70 ml) CP2D (70 ml) ACD (70 ml) Shelf Life (RBC) Labeled RBCs in 35 Day Shelf Life Wait 24 hours >75% survival CPDA-1 (70 ml)
5 RBC Shelf Life CPD 21 ACD-A 21 CP2D 21 CPDA-1 35 AS
6 Anticoagulant/Preservatives Why we need 21 Day Shelf Life Prevent clotting Keep cells fresh CPD (70 ml) CP2D (70 ml) ACD (70 ml) Shelf Life (RBC) Labeled RBCs in 35 Day Shelf Life Wait 24 hours >75% survival CPDA-1 (70 ml)
 AS RBC HCT: 50-60%")
* AS-7 (SOLX)* LR * = Has")
7 21 Day Shelf Life 42 Day Shelf Life CPD RBC HCT: 60-80% AS (110 ml) AS RBC HCT: 50-60% CP2D RBC Types: AS-1 (Adsol)* AS-3 (Nutricel) AS-5 (Optisol)* AS-7 (SOLX)* LR * = Has mannitol
8 RBC Shelf Life CPD 21 ACD-A 21 CP2D 21 CPDA-1 35 AS
9 /LLU LLUPathology

10 Whole Blood Gimme some whole blood! WHADDYA MEAN, WHOLE BLOOD? WB Definitions Matter!

11 Whole Blood WB WB Low-titer ABO abs Leukoreduced but platelet-rich Warm, fresh Unmodified Untested Cold, stored
12 Whole Blood Indication for Group O, low-titer, cold whole blood: - Trauma massive transfusion (universal) Appears safe so far Cold PLTs may have better immediate activity Other forms - Reconstituted: Exchange transfusions (neonates) Storage length depends on anticoagulant WB - Always at 1-6 C
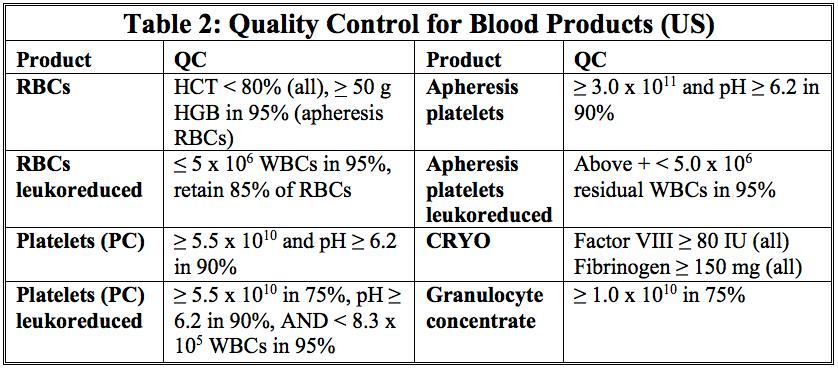
13 Red Blood Cells 5.9 M units/yr as of 2014 (declining) Volume: Contents: 350 ml (incl. additive) RBCs ( ml) Plasma (< 50 ml) WBCs (10 9 ) and PLTs Anticoagulant/preservative Additive solution (110 ml) mg iron RBC

14 Consumption/Delivery VO2 DO2 DO 2 : Oxygen delivery (supply) DO2 independence DO 2 = CO x CaO g/dl? Cardiac Output Arterial O 2 HR x SV Hgb O 2 + plasma O 2 Unless below critical DO2, RBCs have minimal effect! RBC VO 2 = Oxygen consumption DO 2 = Oxygen delivery
15 Why Use? Insufficient O 2 delivery due to carrying capacity - Acute hemorrhage (>30% of BV) - Hemolysis - Marrow failure Replace malformed RBCs in Sickle Cell Disease Exchange coated RBCs in neonates with HDFN RBC

16 Stable hospitalized patients: 7 g/dl Ortho/Cardiac surg: 8 g/dl or symptoms Chronic CV disease: 8 g/dl Others with no recommendation: - Acute coronary syndrome - Marked thrombocytopenia - Chronic anemias RBC Source: Carson JL et al, JAMA 2016
17 Why NOT to Use Smaller acute hemorrhages - 1L (20%) OK with saline Nutritional anemias - Folate, B12, iron RBC
18 Effect in non-bleeding Pts RBC RBC 24% 8 g/dl 21% 7 g/dl 15 min 15 min Hematocrit Hemoglobin RBC
19 Storage Depends on anticoagulant - 42 days with additives Always at 1-6 C Shipping - Temperature range 1-10 C RBC
20 Compatible Fluids NaCl (0.9%, not 0.45%) ABO compatible plasma 5% albumin Plasma-Lyte 148, Plasma-Lyte-A, Normosol-R ph 7.4 NOT: - LR (3 meq Ca2+/L), antibiotics, other meds, TPN RBC


21 Platelets

22 Platelets: Two Options >90% Multiple products Limits exposure WB <10% Pooled product Trauma
23 Apheresis Platelets Volume: ml (or more) Contents: PLTs (>3.0 x in 90%) Plasma ( ml) WBCs (< 5.0 x 10 6 ) ph > 6.2 (90%) PLTs
24 WBD-Platelets Volume: ml each Contents: PLTs (>5.5 x in 90%) Plasma (40-60 ml) WBCs (~10 7 ) ph > 6.2 (90%) PLTs

25 Typical Conversions 4-6 of these (Whole blood) One of these (Apheresis) PLTs PLTs PLTs PLTs AD PLTs PLTs PLTs PLTs AD PLTs AD PLTs AD PLTs AD PLTs
 Increased risks (?")
26 Thrombocytopenia Might bleed" vs. IS bleeding debate - Answered in Heme/Onc (prophylactic helps) Increased risks (? higher threshold): - Fever - Sepsis - Thrombocytopathy - Splenomegaly? PLTs - Coagulopathy?

27 No bleeding or risk factors: <10K Elective CVC placement: <20K Elective lumbar puncture: <50K Major non-neuraxial surgery: <50K No prophylaxis for CPB PLTs Source: Kaufman RM et al, Ann Int Med 2015
 - Count is not predictive of bleeding - Skill of operator IS predictive! - Cranial bleed?")
28 Controversial Liver biopsy/endoscopy/regional anesthesia? - 50K common (sometimes 100K!) - Count is not predictive of bleeding - Skill of operator IS predictive! - Cranial bleed? - Data suggesting worse if on anti-plt - Cranial surg/pulm or eye hemorrhage? PLTs - No rec; typically 100K used
 Cardiopulmonary bypass, ECMO")
29 Thrombocytopathy Prophylactic not indicated! Congenital defects Drugs (ASA, clopidogrel) Cardiopulmonary bypass, ECMO Metabolic effects - Renal failure PLTs
 Post-transfusion")
30 When NOT to Give Thrombotic Thrombocytopenic Purpura/HUS Heparin-induced thrombocytopenia, type II Immune Thrombocytopenic Purpura (ITP) Post-transfusion Purpura (PTP) PLTs
31 How Much? WBD-PLTs 1 per 10 Kg - Usually 4-6 at a time - Pooled at blood center or hospital AD-PLTs 1 bag per dose Smaller doses may be ok ml/kg in neonates PLTs

32 Expected Effect > 20-30,000 is eyeball ok Corrected Count Increment for standard eval One hour post count is standard - But 10 minute counts can be magical! No bump at 10 min usually = antibodies Bump at 10 min but not at 1 hr = nonimmune PLTs
33 Platelet Storage 5 days, 20-24C, gentle agitation - AD, WBD (unpooled) - WBD (pooled by blood center) - 7 day option with Verax (later) 4 hours: Transfusion service pooling Shipping: C, < 24 hours without agitation PLTs

34 ABO-Identical PLT Transfusion anti-b Plasma anti-b PLTs A + A+ RBCs A Pos Recipient A Pos Donor
35 Major-incompatible PLT Transfusion anti-b Plasma anti-a anti-b Risk: Decreased response PLTs A + O+ RBCs O Pos Recipient A Pos Donor
36 Minor-incompatible PLT Transfusion anti-a anti-b Plasma anti-b Risk: Patient RBC hemolysis PLTs O + A+ Consider titers RBCs for anti-a, -B A Pos Recipient O Pos Donor
37 ABO-Identical, Rh incompatible PLT Transfusion AD PLTs: ml of RBCs! Plasma A + PLTs A- A Pos Donor RBCs A NEG Recipient Risk: Patient anti-d Risk ~1% Consider RhIg for child-bearing aged females



38 Sterility Testing ALL Platelets must have! Culture-based (AD, pooled WBD) - 24 hour wait required - BacT/ALERT Pre-issue (Verax PGD pre-issue) Gram stain, swirling, etc no good! Pathogen reduced platelets (next) PLTs

39 The Future Pathogen-reduced platelets PLTs

40 Modified Products Leukocyte Reduced Products Irradiated products Frozen products Washed products
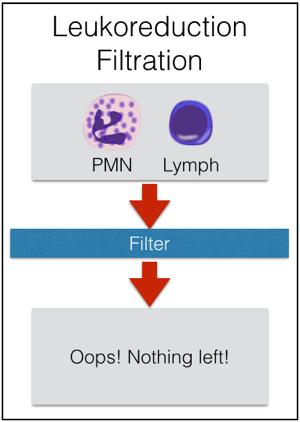
41 Leukocyte Reduced Products < 5.0 x 10 6 WBC (95% of tested) LR-RBCs < 8.3 x 10 5 WBC (95% of tested) LR-PLTs LR-AD-PLTs 5 x 10 6 / 6 bags = 8.3 x 10 5 per bag
42 Leukocyte Reduced Products Prestorage - < 3 days after collection - Various methods Pretransfusion - Bedside ; rarely done now - Old studies often included
43 Leukocyte Reduced Products Established benefits: - Febrile transfusion reactions - HLA immunization - CMV transmission

44 Leukocyte Reduced Products Reduce Febrile Transfusion Reactions - Removes WBC that can either: Secrete cytokines in bag Interact with recipient WBCs

45 Leukocyte Reduced Products Reduce HLA immunization risk - Foreign HLA antigens require donor lymphocytes for processing - Leukoreduction prevents this interaction

46 Leukocyte Reduced Products Reduce CMV transmission - CMV only in WBCs (monocytes) - Removal of WBCs = reduction of CMV risk - About 1-4% risk with LR or CMV products - See podcast (/047)
47 Leukocyte Reduced Products It also works to prevent: - Reperfusion injury after cardiac bypass It might work to prevent: - Immunosuppression (TRIM) - Septic transfusion reactions - Prion disease (vcjd)

48 Washed Blood Products Remove plasma from cellular products 1-2 L saline / 99% of plasma 1 to several hours Shelf life - RBCs: 24 hours - Platelets: 4 hours
49 Why Wash Blood? Remove harmful plasma proteins - Pt with IgA deficiency with anti-iga - Pt with haptoglobin deficiency - Antibodies ABO antibodies in minor PLT incompatibility Neonatal alloimmune thrombocytopenia Remove unwanted plasma electrolytes (K+)
50 Frozen Red Cells Long-term storage of valuable RBCs Protect with glycerol (40% most common) Remove before transfusion Hemolysis is risk if not removed Why? - Patients with high-frequency antibodies - Donors with rare phenotypes - Autologous units for later use
 - At least 2 years at 80 C - Not FDA-licensed Photo courtesy LifeStream Blood")
51 Frozen Blood Products Red cells - 10 years at 65 C - 24 hours at 1-6 C after deglycerolizing Platelets (in DMSO) - At least 2 years at 80 C - Not FDA-licensed Photo courtesy LifeStream Blood Bank


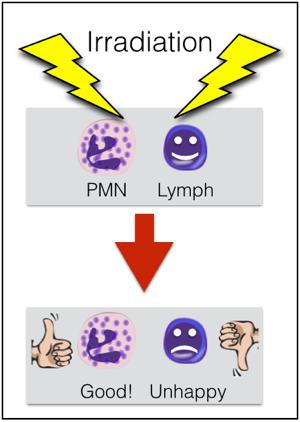
52 Irradiation 2500 cgy targeted to center of bag, 1500 cgy to all parts Targets T-lymphocytes to prevent TA-GVHD


53 Maximum 28 day shelf life after irradiation
54 Who Needs Irradiated Products? Immunosuppressed patients - Stem cell/marrow transplant recipients - T-cell defects (including drugs) - Aplastic anemia Fetuses or premature neonates Patients with Hodgkins Disease Granulocyte recipients 1st-degree relatives or HLA-matched
 LR is NOT interchangeable!")
55 Miscellaneous Not for CMV prevention Not for stem cell infusions (duh!) LR is NOT interchangeable! - We don t know minimum threshold Not Good Enough!


56 Fresh Frozen Plasma Whole blood-derived Apheresis-derived - 1 o collection or concurrent FFP
57 Fresh Frozen Plasma Volume: Contents: ml All coagulation factors >500 mg fibrinogen 1 IU/mL of all others Lysed RBCs and WBCs No QC required FFP
58 Relationship between INR and coagulation factors 100 % 60 ml/kg FFP = 4 L fresh plasma zone of normal hemostasis 50 % 30 % 15 ml/kg FFP zone of anticoagulation INR Slide courtesy Dr. Jeannie Callum
59 FFP 200mL FFP 200mL INR ! Each unit is about 7% of total PV Plasma Volume 3 L INR 1.7


60
61 FFP Indications Bleeding/operative patients with coagulopathy from multiple factor deficiencies - Hepatic failure (avoid prophyaxis) - Dilution, consumption Bleeding patients needing urgent reversal of warfarin effect - 4 factor PCC may be better choice ($$) FFP
62 FFP Indications Trauma massive transfusion - 1:1 RBC:FFP ratio - PROPPR study published 2015 (no difference in mortality, less exsanguination) Transfusion/exchange in TTP Factor-specific coagulopathies without a factor concentrate (V, XI) FFP

63 FFP Contraindications Volume expansion Heparin reversal Specific concentrate available Prophylaxis with mild INR elevations Nutrition, wound healing, etc. FFP

64 FFP Preparation Pre-storage - Plasma at 18 C within 8 hours - WHY? To preserve Factors and - 1 year at -18 C, 7 years at -65 C Pre-transfusion - Thaw at C - Keep at 1-6 C for 24 hours FFP
65 Dosage and Effect Two at a time common (inadequate!) FFP FFP ml/kg is appropriate 20-30% factor increase per dose Transient effect (FVII t 1/2 = 4 hrs!) ABO compatible (no crossmatch) Rh doesn t matter FFP FFP FFP
66 Plasma Variants-Frozen Plasma frozen within 24 hours Plasma Cryoprecipitate-reduced -Majority of FFP -FFP after CRYO PF24 -Use just like FFP -Store/thaw = FFP -Can t make CRYO P-CR - FVIII, FBG, vwf -Refractory TTP -Store/thaw = FFP
67 Plasma Variants-Liquid Thawed Plasma Liquid Plasma PF24 -FFP/PF24 >24 hrs -1-6C up to 5 days -Use = FFP LP -Never Frozen -Use in trauma/mt -Expires 26 days -Store 1-6C
68 Cryoprecipitate Volume: Contents: ~15 ml each > 150 mg fibrinogen > 80 IU Factor VIII IU vwf IU Factor XIII Fibronectin Easy! Us. > 250 mg


69 CRYO Preparation FBG FVIII vwf Thaw overnight 1-6C Spin Drain Pool and Freeze 18C
70 Cryoprecipitate Uses Fibrinogen deficiency - Target at least 150 mg/dl - Approx mg in 10 bags Thrombocytopathy in renal failure (2 nd line-ddavp) Topical glue (infrequent now) vwd treatment (2 nd line after Humate-P) - 1 bag per 10 Kg q 8 hours
71 Cryoprecipitate Store like FFP ( 18 C for 1 year) Thaw like FFP (30-37 C) Keep UNLIKE FFP - 6 hours at C - 4 hours if pooled with open system ABO, Rh compatibility irrelevant (but many match ABO)
72 Myths CRYO = small volume FFP - No FVII - Can t replace FFP in vol-sensitive More fibrinogen in CRYO than FFP - Not possible - Just more concentrated
73 Granulocyte Concentrate Volume: Contents: ml > 1 x neutrophils ml RBCs (needs XM) ~1 x platelets Plasma

74 Granulocyte Concentrate Large studies show no proven effect RING suggests at least 4.0 x for effect Potential recipients: - Preemies with sepsis/infections - Transplant patients with infections - CGD/LAD patients Stimulate donors (G-CSF +/- steroids)

75 Granulocyte Concentrate Indications: - Neutropenia (<500/uL), reversible - Fever hrs - Proven bacterial/fungal infx - Unresponsive to antibiotics 24 hours at C, no agitation


76 XM ABO/Rh YES Antibodies NO

77 DDAVP Treats vwf deficiency and may help: - Uremic thrombocytopathy - vwd - Mild Hemophilia A - Hepatic thrombocytopathy
 effect in: - Acute major bleeding - Urgent surgical procedure Cost: Up to")
78 Prothrombin Complex Concentrate Pharmaceutical concentrate of Vitamin-K factors - II, VII, IX, X - Current form ( K-centra ) contains all 4 factors Indicated to reverse VKA (warfarin) effect in: - Acute major bleeding - Urgent surgical procedure Cost: Up to ~$6000/dose
79
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
UKGS TRANSFUSION SERVICE PRODUCTS AND AVAILABILITY
 Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
The ABC s of Blood Components. Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service
SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service") The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
ADULT TRANSFUSION GUIDELINES ORDERED COMPONENT
 ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
Blood Component Therapy
 Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Risk of ID transmission. Patient Blood Management - Blood Safety and Component Utilization. Transfusion and Cancer 4/9/2014
 Patient Blood Management - Blood Safety and Component Utilization Lowell Tilzer M.D. Pathology and Lab Medicine Kansas University Med Center Risk of ID transmission Pre NAT Post NAT HIV 1:607,000 ~1:2.5
Patient Blood Management - Blood Safety and Component Utilization Lowell Tilzer M.D. Pathology and Lab Medicine Kansas University Med Center Risk of ID transmission Pre NAT Post NAT HIV 1:607,000 ~1:2.5
Transfusion Medicine Best Practices: Indications for Blood Components
 Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Learning Objectives. Blood Component Therapy. Blood Component Therapy. Apheresis Technology. Red Cells
 Learning Objectives Blood Component Therapy Jeffrey Jhang, MD Assistant Professor of Clinical Pathology College of Physicians and Surgeons New York, NY 1. Know how components are prepared by whole blood
Learning Objectives Blood Component Therapy Jeffrey Jhang, MD Assistant Professor of Clinical Pathology College of Physicians and Surgeons New York, NY 1. Know how components are prepared by whole blood
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
New Advances in Transfusion EM I LY CO BERLY, M D
 New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created
 Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created By: Bray, Karen Last Approved Time: 7/22/2016 12:41:34
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created By: Bray, Karen Last Approved Time: 7/22/2016 12:41:34
CMC Medical Staff Transfusion Guidelines. Table of Contents edition INTRODUCTION:
 CMC Medical Staff Transfusion Guidelines 2014 edition INTRODUCTION: The CMC Blood Component and Transfusion Guidelines have been approved by the multidisciplinary Transfusion Committee. These are based
CMC Medical Staff Transfusion Guidelines 2014 edition INTRODUCTION: The CMC Blood Component and Transfusion Guidelines have been approved by the multidisciplinary Transfusion Committee. These are based
Blood Product Modifications: Leukofiltration, Irradiation and Washing
 1. Leukocyte Reduction Definitions and Standards: o Process also known as leukoreduction, or leukofiltration o Applicable AABB Standards, 25th ed. Leukocyte-reduced RBCs At least 85% of original RBCs
1. Leukocyte Reduction Definitions and Standards: o Process also known as leukoreduction, or leukofiltration o Applicable AABB Standards, 25th ed. Leukocyte-reduced RBCs At least 85% of original RBCs
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Blood Product Utilization A Mythbusters! Style Review. Amanda Haynes, DO 4/28/18
 Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Blood Components Transfusion Criteria
 Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
POLICY NO. Printed copies are for reference only. Please refer to the electronic copy for the latest version.
 Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
BLOOD TRANSFUSION. Dr Lumka Ntabeni
 BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Guidelines for Use of Canine Blood Components
 Guidelines for Use of Canine Blood Components Cryoprecipitate This product is prepared by a controlled thaw of fresh frozen plasma, resulting in a concentration of Factor VIII, Factor XIII, vwf and some
Guidelines for Use of Canine Blood Components Cryoprecipitate This product is prepared by a controlled thaw of fresh frozen plasma, resulting in a concentration of Factor VIII, Factor XIII, vwf and some
Pretransfusion Testing
 Pretransfusion Testing Blood transfusion services The immunohematologic testing needed for By proper patient blood typing, component Dr. selection Reham and Talaat compatibility testing. Which Blood ensure
Pretransfusion Testing Blood transfusion services The immunohematologic testing needed for By proper patient blood typing, component Dr. selection Reham and Talaat compatibility testing. Which Blood ensure
Transfusion: indications (RBC, platelets, granulocytes, plasma)
") Transfusion: indications (RBC, platelets, granulocytes, plasma) BHS Educational Course: course n 5 22/3/2014 Timothy Devos (KU Leuven) Indications for the transfusion of erythrocytes General rules only
Transfusion: indications (RBC, platelets, granulocytes, plasma) BHS Educational Course: course n 5 22/3/2014 Timothy Devos (KU Leuven) Indications for the transfusion of erythrocytes General rules only
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Specific Requirements
 Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Blood Transfusion. What is blood transfusion? What are blood banks? When is a blood transfusion needed? Who can donate blood?
 What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
Recent advances in donor screening, blood testing
 TRANSFUSION PRACTICE Guidelines for assessing appropriateness of pediatric transfusion Susan D. Roseff, Naomi L.C. Luban, and Catherine S. Manno Recent advances in donor screening, blood testing before
TRANSFUSION PRACTICE Guidelines for assessing appropriateness of pediatric transfusion Susan D. Roseff, Naomi L.C. Luban, and Catherine S. Manno Recent advances in donor screening, blood testing before
Chapter 13 The Blood
 Chapter 13 The Blood Copyright 2015 Wolters Kluwer Health Lippincott Williams & Wilkins Overview Key Terms agglutination erythrocyte lymphocyte albumin fibrin megakaryocyte anemia hematocrit monocyte antigen
Chapter 13 The Blood Copyright 2015 Wolters Kluwer Health Lippincott Williams & Wilkins Overview Key Terms agglutination erythrocyte lymphocyte albumin fibrin megakaryocyte anemia hematocrit monocyte antigen
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference
 Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Transfusion Therapy & Safety. Mary Grabowski, RN, BSN, BSIA Transfusion Safety Officer PSONEC Fundamentals September, 2015
 Transfusion Therapy & Safety Mary Grabowski, RN, BSN, BSIA Transfusion Safety Officer PSONEC Fundamentals September, 2015 Topics Blood Components Special Processing/Attributes Irradiation Leukoreduction
Transfusion Therapy & Safety Mary Grabowski, RN, BSN, BSIA Transfusion Safety Officer PSONEC Fundamentals September, 2015 Topics Blood Components Special Processing/Attributes Irradiation Leukoreduction
What is an Apheresis Donation?
 What are Platelets? Platelets are colorless, irregularly shaped bodies found in blood. The primary role of platelets is to prevent bleeding in injured blood vessel walls by forming an aggregate at the
What are Platelets? Platelets are colorless, irregularly shaped bodies found in blood. The primary role of platelets is to prevent bleeding in injured blood vessel walls by forming an aggregate at the
Consent Laboratory Transfuse RBC
 Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
A Compendium of Transfusion Practice Guidelines
 A Compendium of Transfusion Practice Guidelines First Edition 2010 Authors: NurJehan Quraishy, MD (Chair), Western Lake Erie Region Gary Bachowski, MD, PhD, North Central Region Richard J. Benjamin, MD,
A Compendium of Transfusion Practice Guidelines First Edition 2010 Authors: NurJehan Quraishy, MD (Chair), Western Lake Erie Region Gary Bachowski, MD, PhD, North Central Region Richard J. Benjamin, MD,
Unit 5: Blood Transfusion
 Unit 5: Blood Transfusion Blood transfusion (BT) therapy: Involves transfusing whole blood or blood components (specific portion or fraction of blood lacking in patient). Learn the concepts behind blood
Unit 5: Blood Transfusion Blood transfusion (BT) therapy: Involves transfusing whole blood or blood components (specific portion or fraction of blood lacking in patient). Learn the concepts behind blood
CIRCULAR OF INFORMATION
 CIRCULAR OF INFORMATION FOR THE USE OF HUMAN BLOOD AND BLOOD COMPONENTS This Circular was prepared jointly by AABB, the American Red Cross, America s Blood Centers, and the Armed Services Blood Program.
CIRCULAR OF INFORMATION FOR THE USE OF HUMAN BLOOD AND BLOOD COMPONENTS This Circular was prepared jointly by AABB, the American Red Cross, America s Blood Centers, and the Armed Services Blood Program.
Transfusion Medicine Kris0ne Kra1s, M.D.
 Transfusion Medicine Kris0ne Kra1s, M.D. Transfusion Medicine Outline Blood groups Introduc0on ABO system Rh system Other systems Blood transfusion Blood products Indica0ons Tes0ng Dangers Transfusion
Transfusion Medicine Kris0ne Kra1s, M.D. Transfusion Medicine Outline Blood groups Introduc0on ABO system Rh system Other systems Blood transfusion Blood products Indica0ons Tes0ng Dangers Transfusion
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
The primary goal of collection
 7 Blood and Components 7 The primary goal of collection centers is to ensure that processes involved in the collection, preparation, storage, and shipment of blood and components result in a blood or blood
7 Blood and Components 7 The primary goal of collection centers is to ensure that processes involved in the collection, preparation, storage, and shipment of blood and components result in a blood or blood
Blood Products & Transfusion. Karim Rafaat, M.D.
 Blood Products & Transfusion Karim Rafaat, M.D. Compatibility Testing Compatibility testing involves three separate procedures involving both donor and recipient blood. 1. ABO & Rh blood type identification
Blood Products & Transfusion Karim Rafaat, M.D. Compatibility Testing Compatibility testing involves three separate procedures involving both donor and recipient blood. 1. ABO & Rh blood type identification
PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal
 PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal Dragoslav Domanovič, MD. PhD. Blood transfusion centre of Slovenia, Ljubljana FFP - definition Fresh
PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal Dragoslav Domanovič, MD. PhD. Blood transfusion centre of Slovenia, Ljubljana FFP - definition Fresh
An Approach to the Patient Refractory to Platelets Transfusion. Harold Alvarez, MD
 Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
When should I transfuse platelets and plasma for children? Dr Liz Chalmers. Consultant Paediatric Haematologist Royal Hospital for Children Glasgow
 When should I transfuse platelets and plasma for children? Dr Liz Chalmers Consultant Paediatric Haematologist Royal Hospital for Children Glasgow When should I transfuse platelets and plasma in children?
When should I transfuse platelets and plasma for children? Dr Liz Chalmers Consultant Paediatric Haematologist Royal Hospital for Children Glasgow When should I transfuse platelets and plasma in children?
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Blood Banking and Transfusion Medicine
 Immunohematology Blood Banking and Transfusion Medicine A science that deals with the principles of blood collection, storage, and transfusion It covers the areas of: ü Donor selection and blood donation
Immunohematology Blood Banking and Transfusion Medicine A science that deals with the principles of blood collection, storage, and transfusion It covers the areas of: ü Donor selection and blood donation
Jovona Powelson, B.S. MLT (ASCP) Director of Laboratories
 Director of Laboratories") Jovona Powelson, B.S. MLT (ASCP) Director of Laboratories Blood Products From the Donor to You Objectives Deliver a brief virtual tour of a blood center. Describe the number of donors needed to meet the
Jovona Powelson, B.S. MLT (ASCP) Director of Laboratories Blood Products From the Donor to You Objectives Deliver a brief virtual tour of a blood center. Describe the number of donors needed to meet the
TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER?
 TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER? 1. Fatal blood transfusion reactions are most likely the result of: a. Circulatory overload b. ABO incompatible blood due to patient identification
TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER? 1. Fatal blood transfusion reactions are most likely the result of: a. Circulatory overload b. ABO incompatible blood due to patient identification
Transfusion Medicine Potpourri. BUMC - Phoenix Internal Medicine Residents September 29, 2015
 Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Update KEMC Nov 5, 2014
 Transfusion Medicine Update KEMC Nov 5, 2014 Allison Collins MD FRCPC Ontario Regional Blood Coordinating Network Physician Clinical Project Coordinator Disclosure I have no conflict of interest with this
Transfusion Medicine Update KEMC Nov 5, 2014 Allison Collins MD FRCPC Ontario Regional Blood Coordinating Network Physician Clinical Project Coordinator Disclosure I have no conflict of interest with this
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Clinical Applications: Donor and Cellular Therapy. Jay S. Raval, MD University of North Carolina Chapel Hill, NC
 Clinical Applications: Donor and Cellular Therapy Jay S. Raval, MD University of North Carolina Chapel Hill, NC None Conflicts of Interest Objectives Donor Collections of Red Blood Cells (RBCs), Plasma,
Clinical Applications: Donor and Cellular Therapy Jay S. Raval, MD University of North Carolina Chapel Hill, NC None Conflicts of Interest Objectives Donor Collections of Red Blood Cells (RBCs), Plasma,
QUICK REFERENCE Clinical Practice Guide on Red Blood Cell Transfusion
 QUICK REFERENCE 2012 Clinical Practice Guide on Red Blood Cell Transfusion Presented by the American Society of Hematology, adapted from Red Blood Cell Transfusion: A Clinical Practice Guideline from the
QUICK REFERENCE 2012 Clinical Practice Guide on Red Blood Cell Transfusion Presented by the American Society of Hematology, adapted from Red Blood Cell Transfusion: A Clinical Practice Guideline from the
Bloodborne Pathogen CEU Training Course $ HOUR RUSH ORDER PROCESSING FEE ADDITIONAL $50.00
 Registration form Bloodborne Pathogen CEU Training Course $100.00 48 HOUR RUSH ORDER PROCESSING FEE ADDITIONAL $50.00 Start and finish dates: You will have 90 days from this date in order to complete this
Registration form Bloodborne Pathogen CEU Training Course $100.00 48 HOUR RUSH ORDER PROCESSING FEE ADDITIONAL $50.00 Start and finish dates: You will have 90 days from this date in order to complete this
12 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
 Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
TRANSFUSIONS WHY DO WE EVEN CARE?????
 TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
Special Requirements Lab Matters. 21 st June Barrie Ferguson
 Special Requirements Lab Matters. 21 st June 2017 Barrie Ferguson Special requirements Patients requiring Methylene Blue or Solvent Detergent treated Fresh Frozen Plasma Patients requiring apheresis platelets
Special Requirements Lab Matters. 21 st June 2017 Barrie Ferguson Special requirements Patients requiring Methylene Blue or Solvent Detergent treated Fresh Frozen Plasma Patients requiring apheresis platelets
BMTCN REVIEW COURSE PRE-TRANSPLANT CARE
 BMTCN REVIEW COURSE PRE-TRANSPLANT CARE Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to edit the Master Experts
BMTCN REVIEW COURSE PRE-TRANSPLANT CARE Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to edit the Master Experts
Transfusion Reactions. Directed by M-azad March 2012
 Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
COMPLICATIONS OF BLOOD TRANSFUSIONS. :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan
 COMPLICATIONS OF BLOOD TRANSFUSIONS :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan COMPLICATIONS OF TRANSFUSIONS Transfusion reaction may result from either : A. Immune transfusion reaction. B. Non
COMPLICATIONS OF BLOOD TRANSFUSIONS :Prepared by Dr. Nawal Mogales & Dr. Mohammed Aqlan COMPLICATIONS OF TRANSFUSIONS Transfusion reaction may result from either : A. Immune transfusion reaction. B. Non
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy. Megan Boysen Osborn, MD, MHPE
 Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
FOR THE USE OF HUMAN BLOOD AND BLOOD COMPONENTS
 CIRCULAR OF INFORMATION FOR THE USE OF HUMAN BLOOD AND BLOOD COMPONENTS This Circular was prepared jointly by AABB, the American Red Cross, America s Blood Centers, and the Armed Services Blood Program.
CIRCULAR OF INFORMATION FOR THE USE OF HUMAN BLOOD AND BLOOD COMPONENTS This Circular was prepared jointly by AABB, the American Red Cross, America s Blood Centers, and the Armed Services Blood Program.
TRANSFUSION MEDICINE. Table 1 Advantages and Disadvantages of Preoperative Autologous Donation. Directed Donation
 X TRANSFUSION MEDICINE Harvey G. Klein, MD* Transfusion medicine has evolved from the empirical administration of blood to a laboratory-based clinical discipline. 1 The discovery of blood group antigens
X TRANSFUSION MEDICINE Harvey G. Klein, MD* Transfusion medicine has evolved from the empirical administration of blood to a laboratory-based clinical discipline. 1 The discovery of blood group antigens
Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital
 Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Practice Guidelines for Blood Transfusion
 Republic of Yemen The Ministry of Health and Population Commission Revolution General Hospital Hodeidah The National Center for Blood Transfusion and research Practice Guidelines for Blood Transfusion
Republic of Yemen The Ministry of Health and Population Commission Revolution General Hospital Hodeidah The National Center for Blood Transfusion and research Practice Guidelines for Blood Transfusion
CASE STUDIES IN CLINICAL APPLICATIONS OF THERAPEUTIC PLASMA EXCHANGE
 CASE STUDIES IN CLINICAL APPLICATIONS OF THERAPEUTIC PLASMA EXCHANGE Eric Rosa, MLS (ASCP) CM Medical Laboratory Scientist Transfusion Service April 18, 2018 Objectives Explain the process of a therapeutic
CASE STUDIES IN CLINICAL APPLICATIONS OF THERAPEUTIC PLASMA EXCHANGE Eric Rosa, MLS (ASCP) CM Medical Laboratory Scientist Transfusion Service April 18, 2018 Objectives Explain the process of a therapeutic
Hematology. The Study of blood
 Hematology The Study of blood Average adult = 8-10 pints of blood Composition: PLASMA liquid portion of blood without cellular components Serum plasma after a blood clot is formed Cellular elements are
Hematology The Study of blood Average adult = 8-10 pints of blood Composition: PLASMA liquid portion of blood without cellular components Serum plasma after a blood clot is formed Cellular elements are
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR
 MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT
 Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT History Why is blood transfusion involved? What tests are performed in blood transfusion and why? What does a protocol look
Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT History Why is blood transfusion involved? What tests are performed in blood transfusion and why? What does a protocol look
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Immunological transfusion reactions
 Immunological transfusion reactions Immunological transfusion reactions can be hemolytic or non-hemolytic in nature. Both types can be separated into acute (those occurring immediately after transfusion)
Immunological transfusion reactions Immunological transfusion reactions can be hemolytic or non-hemolytic in nature. Both types can be separated into acute (those occurring immediately after transfusion)
TRANSFUSION MEDICINE UPDATE & REVIEW TOO MUCH OF A GOOD THING? YELENA KIER, DO
 TRANSFUSION MEDICINE UPDATE & REVIEW TOO MUCH OF A GOOD THING? YELENA KIER, DO DISCLOSURES No Disclosures/Conflicts of interest OVERVIEW Brief overview of history of transfusion medicine Review of blood
TRANSFUSION MEDICINE UPDATE & REVIEW TOO MUCH OF A GOOD THING? YELENA KIER, DO DISCLOSURES No Disclosures/Conflicts of interest OVERVIEW Brief overview of history of transfusion medicine Review of blood
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
CIRCULAR. of information. For the use of Labile Blood Products. Edition
 For the use of Labile Blood Products CIRCULAR of information july 2009 Edition WARNING: The risk of transmitting known and unknown infectious disease agents is present in the transfusion of labile blood
For the use of Labile Blood Products CIRCULAR of information july 2009 Edition WARNING: The risk of transmitting known and unknown infectious disease agents is present in the transfusion of labile blood
Review. Blood Components for Hemostasis. RBC Transfusion. Karen W. Eldin, MD 1, and Jun Teruya, MD, DSc 1,2 ABSTRACT
 Blood Components for Hemostasis Karen W. Eldin, MD 1, and Jun Teruya, MD, DSc 1,2 ABSTRACT We present an overview of revised indications and doses for routinely transfused blood components. Targeted blood
Blood Components for Hemostasis Karen W. Eldin, MD 1, and Jun Teruya, MD, DSc 1,2 ABSTRACT We present an overview of revised indications and doses for routinely transfused blood components. Targeted blood
HEMATOLOGIC DISORDERS
 Blood HEMATOLOGIC DISORDERS Disorders of RBCs (erythrocytes) are the anemias. Anemias result from: decreased supply of RBCs, the volume of packed RBCs, the quantity of hgb. The end result of each of these
Blood HEMATOLOGIC DISORDERS Disorders of RBCs (erythrocytes) are the anemias. Anemias result from: decreased supply of RBCs, the volume of packed RBCs, the quantity of hgb. The end result of each of these
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress TRANSFUSIONS CONTAINING RED BLOOD CELLS Ann E. Hohenhaus, DVM Diplomate, ACVIM (Oncology and Internal Medicine)
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress TRANSFUSIONS CONTAINING RED BLOOD CELLS Ann E. Hohenhaus, DVM Diplomate, ACVIM (Oncology and Internal Medicine)
Blood Component Information. CIRCULAR OF INFORMATION An extension of blood component labels
 Blood Component Information CIRCULAR OF INFORMATION An extension of blood component labels 2009 Copyright Australian Red Cross Blood Service 2009 Last updated April 2009 Apart from any fair dealing for
Blood Component Information CIRCULAR OF INFORMATION An extension of blood component labels 2009 Copyright Australian Red Cross Blood Service 2009 Last updated April 2009 Apart from any fair dealing for
BLOOD TRANSFUSION GUIDELINES
 BLOOD TRANSFUSION GUIDELINES rational and safe practices Kartika W. Taroeno-Hariadi Hematology and Medical Oncology,Department of Internal Medicine Faculty of Medicine,Public Health, and Nursing Universitas
BLOOD TRANSFUSION GUIDELINES rational and safe practices Kartika W. Taroeno-Hariadi Hematology and Medical Oncology,Department of Internal Medicine Faculty of Medicine,Public Health, and Nursing Universitas
From donor biology to donor health protection: Three (very) short stories
 short stories") From donor biology to donor health protection: Three (very) short stories Steven L. Spitalnik, M.D. Laboratory of Transfusion Biology Potential Conflicts of Interest Hemanext: Tioma, Inc: Advisory Board
From donor biology to donor health protection: Three (very) short stories Steven L. Spitalnik, M.D. Laboratory of Transfusion Biology Potential Conflicts of Interest Hemanext: Tioma, Inc: Advisory Board
Laboratory Empowerment. Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance
 Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
CURRENT COURSE OFFERINGS
 The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
For more information about how to cite these materials visit
 Author(s): Robertson Davenport, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Robertson Davenport, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC
 RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
ACCEPTABLE UNIVERSAL BLOOD PRODUCTS FOR RESUSCITATION?
 ACCEPTABLE UNIVERSAL BLOOD PRODUCTS FOR RESUSCITATION? Paul M. Ness, M.D. Professor Pathology, Medicine, and Oncology The Johns Hopkins Medical Ins tu ons Bal more, Maryland, USA BLOOD BANK BUREAUCRATS
ACCEPTABLE UNIVERSAL BLOOD PRODUCTS FOR RESUSCITATION? Paul M. Ness, M.D. Professor Pathology, Medicine, and Oncology The Johns Hopkins Medical Ins tu ons Bal more, Maryland, USA BLOOD BANK BUREAUCRATS