CHALLENGES OF HYPERTENSION IN THE COALFACE
|
|
|
- Francis Page
- 5 years ago
- Views:
Transcription
1 CHALLENGES OF HYPERTENSION IN THE COALFACE Y VERIAVA CENTRE FOR RURAL HEALTH SCHOOL OF CLINICAL MEDICINE FACULTY OF HEALTH SCIENCES UNIVERSITY OF WITWATERSRAND
2 SYSTOLIC AND DIASTOLIC BLOOD PRESSURES (BP) IN 5-YEAR AGE GROUPS IN A REPRESENTATIVE SAMPLE OF THE POPULATION OF NOORD LIMBURG, BELGIUM AGE GROUPS
3 CHALLENGES Goals of lowering blood pressure Blood pressure measurement Risk stratification Modalities of blood pressure treatment Target blood pressure Stage 3 hypertension
4 PREVALENCE OF HYPERTENSION IN SUB-SAHARAN AFRICA OVERALL PREVALENCE 16.2% (95% CI ) (23.3%) RURAL 13.7% URBAN 20.7% GENDER Male 16.8% Female 15.7% Twagirumukiza M et al; J of Hypertension July 2011

5 HYPERTENSION PREVALENCE Twagirumukiza M et al; J of Hypertension; July
6 The total number of hypertensives in SSA was estimated at 75 million in 2008 and at million by Twagirumukiza M et al; J of Hypertension July 2011 Prevalence predicted to increase to 1.5 billion world wide by 2025 He FJ et al; Eur Heart J (Suppl) 2007
7 GLOBAL BURDEN OF BLOOD- PRESSURE RELATED DISEASE 7.6 Million premature deaths (13.5% of global) 92 Million disability adjusted life years (6.9% of global) 54% of stroke and 47% of ischaemic heart disease 80% of attributable burden in low-income and middle-income economies and over half in people aged years Lawes C M M et al; Lancet 2008
8 CLASSIFICATION OF HYPERTENSION STAGE (MMHG) NORMAL HIGH NORMAL GRADE 1 (MILD) SBP and DBP SBP or DBP SBP or DBP GRADE 2 (MODERATE) SBP or DBP GRADE 3 (SEVERE) ISOLATED SYSTOLIC SBP > 180 or DBP > 110
9 BLOOD PRESSURE MEASUREMENT OFFICE OR CLINIC - mercury sphygmomanometer SELF MEASUREMENT: electronic sphygmomanometer AMBULATORY BLOOD PRESSURE MONITORING
10 MEASUREMENT OF BLOOD PRESSURE BP is recorded using an approved device with the patient in a sitting position (with the back supported, arm bared and resting on a surface at heart level) for at least 5 minutes. An appropriate size cuff should be used: a standard cuff (12 cm) for a normal arm and a larger cuff (15 cm) for an arm with a mid-upper circumference >33cm (the bladder within the cuff should encircle 80% of the arm). At the initial consultation BP should be measured in both arms, and if there is any discrepancy is should be taken thereafter in the arm with the higher BP. The systolic BP should be first estimated by palpation to avoid missing the auscultatory gap.

11 TECHNIQUE OF BP MEASUREMENT Kaplan N. Clin Hypt. 10 th ed
12 DIAGNOSIS OF HYPERTENSION. The diagnosis of hypertension may be made if repeat measurements performed on three separate occasions when either the initial SBP is between 140 mm Hg and/or the DBP 90 mm Hg taken over a period of 2 months. Where circumstances permit ABPM should be considered particularly in the absence of TOD.
13 MEASUREMENT OF BLOOD PRESSURE Self-measurement of BP (SBPM) and ambulatory monitoring (ABPM) is recommended for selected target groups and circumstances: suspected white-coat (higher readings in the office compared to outside) or masked hypertension (normal readings in office but higher outside); to guide antihypertensive medication especially in high risk groups e.g. elderly, diabetics; refractory hypertension; to improve compliance to treatment; (SBPM only)
14 RELATIVE EFFECTIVENESS OF CLINIC AND HOME BP MONITORING COMPARED WITH ABPM IN DIAGNOSIS OF HYPERTENSION CLINIC (140/90) VERSUS ABPM (135/85) Sensitivity 74.6%; Specficity 74.6% HOME (135/85) VERSUS ABPM (135/85) Sensitivity 85.7% Specificity 62.4% Hodgkinson J et al; BMJ. 2011
15 One or more, high quality single visit nurse recorded auscultatory blood pressure measurements may be equally as effective as ambulatory blood pressure in predicting target organ damage in a population sample of African ancestry Woodiwiss AJ et al; J Hypertens. 2009
16 BLOOD PRESSURE MEASUREMENT FOR COMMENCEMENT OF ANTIHYPERTENSIVE THERAPY NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE (NICE) ABPM if no target organ damage HBPM if unable to tolerate ABPM AMERICAN HYPERTENSION SOCIETY HBPM SOUTHERN AFRICAN HYPERTENSION SOCIETY Conventional OBPM
17 AUTOMMATED OFFICE BP MEASUREMENT Six readings are taken at 2 minute intervals in a quite room, the initial reading discarded and the remaining 5 are averaged.
18 THE RISK FOR CARDIOVASCULAR DISEASE IN PATIENTS WITH HYPERTENISON IS DETERMINED BY THE PRESENCE OF CARDIOVASCULAR RISK FACTORS TARGET ORGAN DAMAGE AND ASSOCIATED CLINICAL CONDITIONS
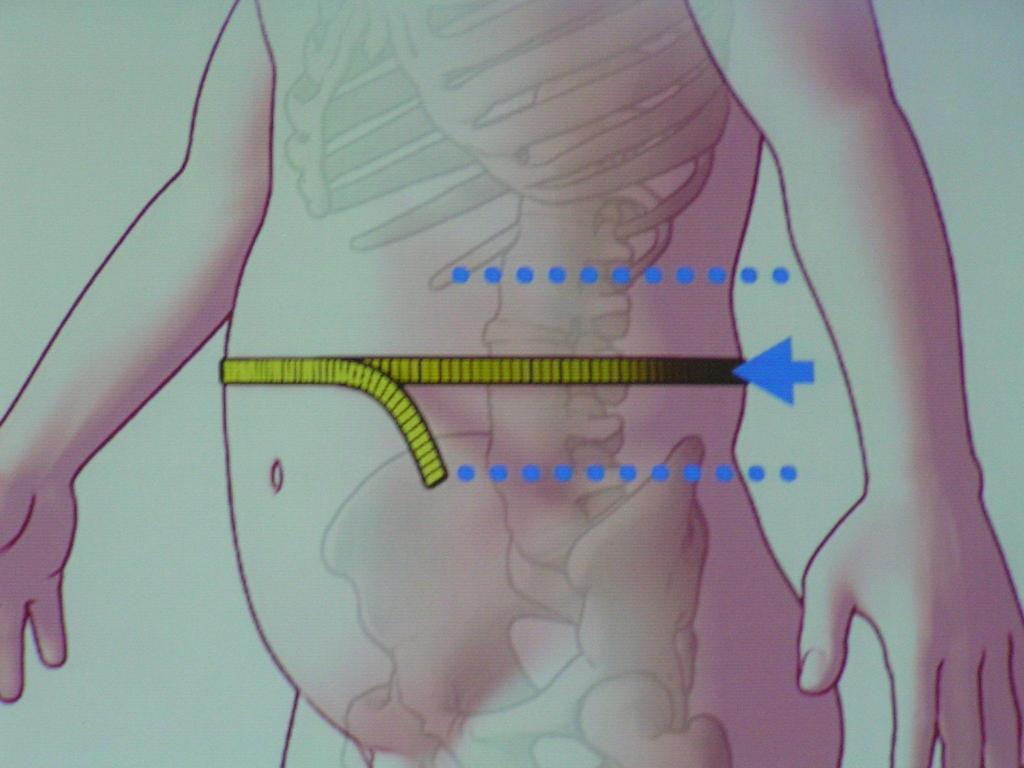
19 MAJOR RISK FACTORS, TARGET ORGAN DAMAGE (TOD) AND ASSOCIATED CLINICAL CONDITIONS (ACC)* MAJOR RISK FACTORS TOD COMPLICATIONS Levels of SBP and DBP Smoking Dyslipidaemia Total cholesterol >5.1 mmol/l, OR LDL >3 mmol/l, OR HDL <1 (men) and <1.2 mmol/l (women) Diabetes mellitus Men >55 years Women >65 years Family history of early-onset CVD: Men aged <55 years Women aged <65 years Waist circumference Men 94 cm Women 80 cm Exceptions are South Asians and Chinese: Men >90 cm and women >80 cm. LVH: based on ECG Sokolow-Lyon >35mm Cornell >2440 mm.ms Microalbuminuria albumin creatinine ratio 3-30 mg/mmol Slightly elevated creatinine: µmol/l (men) µmol/l (women) CHD HF CKD Albuminuria >30 mg/mmol, OR creatinine >133 µmol/l (men) creatinine >124 µmol/l (women) Stroke or TIA Peripheral arterial disease Advanced retinopathy: Haemorrhages, OR Exudates Papilloedema
20
21 ROUTINE INVESTIGATIONS INVESTIGATION FREQUENCY COMMENTS Blood tests Creatinine Yearly if normal From serum creatinine calculate GFR (modified MDRD equation = GFR in ml/min/1.73 m²) Potassium Yearly if normal Glucose (fasting preferred) Yearly if normal Consider GTT in patients with fasting glucose >6.1 mmol/l Random total cholesterol Yearly if normal Measure fasting lipogram if cholesterol >5.1 mmol/l or in high-risk groups ECG (resting) Yearly if normal Refer to SAHS policy brief on LVH Secondary cause suspected Referral as necessary If suspected at first visit or if refractory hypertension exists, additional investigations should be performed If invasive renal, vascular or endocrine investigations are required, refer the patient to the appropriate specialist or subspecialist.
22 THE IDENTIFICATION OF CARDIOVASCULAR RISK FACTORS TARGET ORGAN DAMAGE, AND ASSOCIATED CLINICAL CONDITIONS, STRATIFIES RISK, QUANTIFIES PROGNOSIS, AND ESTABLISHES THE THRESHOLD FOR INTERVENTION
23 STRATIFICATION OF RISK TO QUANTIFY PROGNOSIS(ESH/ECC) GUIDELINES) Blood pressure (mm Hg) Other risk factors and disease history Normal SBP Or DBP High normal SBP or DBP Grade 1 (mild hypertension) SBP or DBP Grade 2 (moderate hypertension) SBP or DBP Grade 3 (severe hypertension) SBP > 180 or DBP> 110 No other risk factors Average risk Average risk Low added risk Moderate added risk High added risk 1-2 risk factors Low added risk Low added risk Moderate added risk Moderate added risk Very high added risk 3 or more risk factors or TOD or diabetes Moderate added risk High added risk High added risk High added risk Very high added risk ACC Very high added risk Very high added risk Very high added risk Very high added risk Very high added risk J Hypertension 2003; 21:
24 CARDIOVASCULAR RISK Low added Moderate added High added Very high added Absolute 10 year risk of cardiovascular disease (%) Absolute risk of fatal cardiovascular disease (%) <15 < >30 >8

25 STRATIFY ACCORDING TO ADDED RISK
26 Measure BP on at least 3 occasions Bp /90-99 mmhg with <3 risk factors, no TOD or complications BP /90-99 mmhg with >3 risk factors, diabetes, TOD or complications BP > 160/100 mmhg Lifestyle modification for 3-6 months Lifestyle modification and commence monotherapy, review in 4-6 weeks Lifestyle modification and commence 2 drug combination, review in 4-6 weeks Not at goal Not at goal Not at goal Add third drug/ optimise doses of drugs
27 MANAGEMENT OF HYPERTENSION LIFE STYLE MODIFICATION DRUG THERAPY
28 Recommended Life style Changes Modification Recommendation Approx BP (mmhg) Weight reduction BMI per 10 kg Dash diet saturated fat and total fat, fruit and vegetables Dietary Na* < 100mmols or 6 gm NaCl /day 2-8 Physical activity Brisk walking for 30mins per day most days Moderation of alcohol No more than 2 Drinks per day 2-4 Tobacco Complete cessation
29 RECOMMENDATIONS First-line drug therapy for uncomplicated hypertension includes low-dose thiazide-like diuretics, calcium channel blockers (CCBs) or angiotensin-converting enzyme inhibitors (ACE- Is) or -angiotensin receptor blockers (ARBs). In black patients either thiazide-like diuretics or CCBs can be used initially, because response rates are better than with ACE-Is.
30 ANTIHYPERTENSIVE DRUGS IN BLACK PATIENTS DIURETICS B BLOCKERS CALCIUM CHANNEL BLOCKERS ACE I/ARB ACE-I/ARB + DIURETICS Effective Less effective Effective Less effective Effective
31 RECOMMENDATIONS ON COMPELLING INDICATIONS FOR A SPECIFIC DRUG CLASS COMPELLING INDICATIONS DRUG CLASS Angina Beta-blocker OR CCB (rate lowering preferred) Prior myocardial infarct Heart failure Left ventricular hypertrophy (confirmed by ECG) Stroke: secondary prevention Diabetes type 1 or 2 with or without evidence of microalbuminuria or proteinuria Beta-blocker AND ACE-1 (ARB if ACE-1 intolerant). Verapamil if Beta-blockers contraindicated. If heart failure, see below ACE-1 (ARB-1 intolerant) AND certain beta-blockers AND aldosterone antagonist For combination ARB and ACE-1 Loop diuretics for volume overload ARB (preferred) OR ACE-1 Low-dose thiazide-like diuretic and ACE-1 or ARB ACE-1 or ARB usually in combination with a diuretic Chronic kidney disease Isolated systolic hypertension ACE-1 OR ARB usually in combination with a diuretic Low-dose thiazide or thiazide-like diuretic OR longacting CCB
32 WHAT IS THE TARGET BLOOD PRESSURE?
33 Targets for BP-lowering treatment STAGE BP LEVEL (mmhg) All stages < 140/90 In isolated systolic hypertension do not lower the DBP to < 65 High-risk patients: < 130/80 Diabetes mellitus Renal disease (macroalbuminuria and/or elevated creatinine) Congestive heart failure Targets should be reached in 3 months
34 TARGET BP CONVENTIONAL Age <80: 140/90 Age >80: 150/90 ABPM /HBPM Age <80:135/85 Age>80:145/85

35 MONOTHERAPY WITH MONOTHERAPY, A TARGET BLOOD PRESSURE OF LESS THAN 140 / 90 mmhg IS RARELY ACHIEVED IN MORE THAN 50% OF HYPERTENSIVE PATIENTS If the target BP is not achieved with the initial agent or monotherapy, what are the options available?
36 OPTIONS AVAILABLE WITH FAILURE OF INITIAL MONOTHERAPY Increase Dose Sequential Monotherapy Combination Therapy
37 ACE I or ARB Thiazide or thiazide-like diuretic CCB
38 BENEFITS OF COMBINATION THERAPY Enhanced antihypertension effect. Improved response rates. Fewer adverse effects. Lessened metabolic effects. Improved outcomes.

39 RATIONALE FOR THE DIURETIC ACE-I or ARB COMBINATION DIURETIC Activation of SNS Activates RAS ACE-I or ARB Attenuates SNS Activation Block RAS Decrease Serum K Increases Serum K
40 ACE-I/ARB + DIURETIC Also - ACE-I s prevent or attenuate the metabolic side effects of diuretics hypokalaemia hyperglycaemia hypercholesterolaemia hyperuricaemia Waeber B et al AmJ Hypertens 1997; 10: 131S-137S
41 RATIONALE FOR ACE I/ARB CALCIUM ANTAGONIST COMBINATION CA Activation of SNS Activation of RAS ACE I /ARB Attenuates Sympathetic activity Blocks RAS
42 STAGE 3 HYPERTENSION Asymptomatic severe hypertension Hypertensive emergency Hypertensive urgency
43 HYPERTENSIVE EMERGENCY Elevation of BP associated with acute and ongoing organ damage to kidneys,brain, heart, eyes or vascular system. Require rapid (within minutes to a few hours) lowering of BP to safe levels. Treatment: Hospitalisation in an intensive care unit. Intravenous antihypertensive therapy.
44 HYPERTENSIVE EMERGENCY Hypertensive encephalopathy Unstable angina/myocardial infarction Acute left ventricular failure with severe pulmonary redema Excessive circulating catecholamines Pheochromocytoma Food or drug administration with monoamine oxidase inhibitors Eclampsia and severe pre-eclampsia Acute nephritis with encephalopathy Acute aortic dissection
45 INTRAVENOUS AND ORAL DRUGS FOR HYPERTENSION EMERGENCY Drug Dose Indications and precautions Effect on BP Intravenous Nitroglycerin (glyceryl trinitrate) 5-10 μg/min Especially useful for myocardial ischaemia BP lowering occurs in 2 5 minutes Dihydralazine 10 mg every minutes until either BP is controlled or a maximum of 50 mg given Avoid in patients with myocardial ischaemia BP lowering occurs In 10 minutes Sodium nitroprusside μg/kg/min diluted in 5% dextrose and adjust dose as necessary Admission to intensive care unit An intra-arterial BP line is desirable BP control is immediate Labetalol 2 mg/min to a total dose of 1-2 mg/kg Use where emergency caused by phaeochromocytoma Caution in acute pulmonary oedema Furosemide mg Acts only for 6 hours Potentiates all of the above drugs
46 INTRAVENOUS AND ORAL DRUGS FOR HYPERTENSION EMERGENCY (CONTINUTED) Drug Dose Indications and precautions Effect on BP ORAL (USE ONLY IF IV DRUGS ARE NOT AVAILABLE) Nifedipine Long-acting only Long-acting CCBs must be used to prevent rapid and dangerous BP reduction Preferred in black persons Check dosage according to CCB brand used Captopril 6.25 mg as a test dose Increase to 25 mg if BP Lowering is not obtained in minutes Other rapidly acting ACE-1 may be used starting with a low test dose DO NOT USE if bilateral renal artery stenosis is suspected DO NOT USE if pregnancy is suspected BP lowering in Minutes
47 THANK YOU
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Summary of recommendations
 Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
ESSENTIAL HYPERTENSION
 E S S E N T I A L H Y P E R T E N S I O N Elevated blood pressure is one of the most important causes of cardiovascular disease. J A Ker MB ChB, MMed, MD Professor and Deputy Dean Faculty of Health Sciences
E S S E N T I A L H Y P E R T E N S I O N Elevated blood pressure is one of the most important causes of cardiovascular disease. J A Ker MB ChB, MMed, MD Professor and Deputy Dean Faculty of Health Sciences
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
What s New? Hypertension Canada Guidelines for the Management of Hypertension
 What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127
 Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Prevention of Cardiovascular Disease
 Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
This Protocol is applicable to Class 1, 2, and Class 3 applicants. Resting ECG shall be performed at the following intervals:
 SCHEDULE 34: PROTOCOL ON ELECTROCARDIOGRAMS ( ECG ) 1. Applicability This Protocol is applicable to Class 1, 2, and Class 3 applicants. 2. Resting ECG Resting ECG shall be perfmed at the following intervals:
SCHEDULE 34: PROTOCOL ON ELECTROCARDIOGRAMS ( ECG ) 1. Applicability This Protocol is applicable to Class 1, 2, and Class 3 applicants. 2. Resting ECG Resting ECG shall be perfmed at the following intervals:
How Low Do We Go? Update on Hypertension
 How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
What is hypertension?
 HYPERTENSION What is hypertension? Abnormally elevated arterial blood pressure that is usually indicated by an adult systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90
HYPERTENSION What is hypertension? Abnormally elevated arterial blood pressure that is usually indicated by an adult systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90
Presentation of hypertensive emergency
 Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL
 CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
Hypertension Clinical case scenarios for primary care
 Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
IMET 2000 PAL International Medical Education Trust Palestine What the GP Should Know about Hypertension
 What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist Impact of Age on Blood Pressure Prevalence of HTN according to Age Fast
What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist Impact of Age on Blood Pressure Prevalence of HTN according to Age Fast
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
2020 HYPERTENSION HIGHLIGHTS
 2020 HYPERTENSION HIGHLIGHTS A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension BLOOD PRESSURE MEASUREMENT TECHNIQUE
2020 HYPERTENSION HIGHLIGHTS A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension BLOOD PRESSURE MEASUREMENT TECHNIQUE
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors.
 Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Banks E, Crouch SR, Korda RJ, et al. Absolute risk of cardiovascular
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Banks E, Crouch SR, Korda RJ, et al. Absolute risk of cardiovascular
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
major public health burden
 HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
HTN talk_l Davis_ /28/2018
 1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Annual Update Hypertension Canada Guidelines for the Management of Hypertension (FULL VERSION)
") Annual Update 2017 Hypertension Canada Guidelines for the Management of Hypertension (FULL VERSION) TABLE OF CONTENTS 2017 Hypertension Canada Guidelines for the Management of Hypertension Diagnosis &
Annual Update 2017 Hypertension Canada Guidelines for the Management of Hypertension (FULL VERSION) TABLE OF CONTENTS 2017 Hypertension Canada Guidelines for the Management of Hypertension Diagnosis &
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Chronic Benefit Application Form Cardiovascular Disease and Diabetes
 Chronic Benefit Application Form Cardiovascular Disease and Diabetes 19 West Street, Houghton, South Africa, 2198 Postnet Suite 411, Private Bag X1, Melrose Arch, 2076 Tel: +27 (11) 715 3000 Fax: +27 (11)
Chronic Benefit Application Form Cardiovascular Disease and Diabetes 19 West Street, Houghton, South Africa, 2198 Postnet Suite 411, Private Bag X1, Melrose Arch, 2076 Tel: +27 (11) 715 3000 Fax: +27 (11)
TIP. Documentation and coding guide. Disease definitions* Prevalence and statistics associated with HTN**
 Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Approach to Management of Hypertension. Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc
 Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Impact of Recent Hypertension Guidelines on Clinical Practice
 C H A P T E R 144 Impact of Recent Hypertension Guidelines on Clinical Practice NK Soni, VB Jindal The movement towards evidence-based healthcare has been gaining ground quickly over the past few years,
C H A P T E R 144 Impact of Recent Hypertension Guidelines on Clinical Practice NK Soni, VB Jindal The movement towards evidence-based healthcare has been gaining ground quickly over the past few years,
Blood Pressure Acre Surgery Diviash Thakrar
 Blood Pressure Acre Surgery Diviash Thakrar Why Are We Doing This? 1. Improve education for patients within the practice 2. Allow us use this for general health promotion Raise money for charity 3. Raise
Blood Pressure Acre Surgery Diviash Thakrar Why Are We Doing This? 1. Improve education for patients within the practice 2. Allow us use this for general health promotion Raise money for charity 3. Raise
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
NICE BHS Hypertension guidelines 2011 update
 NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM
 MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Primary hypertension in adults
 Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Primary and Secondary Prevention of Cardiovascular Disease. Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group
 Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
CVD Risk of Hypertension. Regina Giblin CVD Clinical Development Coordinator
 CVD Risk of Hypertension Regina Giblin CVD Clinical Development Coordinator CVD Clinical Development Coordinator In-house education for your team: Regina Giblin giblinr@bhf.org.uk Often interactive with
CVD Risk of Hypertension Regina Giblin CVD Clinical Development Coordinator CVD Clinical Development Coordinator In-house education for your team: Regina Giblin giblinr@bhf.org.uk Often interactive with
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Patrick Kay, General and Interventional Cardiologist Auckland or healthpoint.co.nz
 Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Coronary Artery Disease Clinical Practice Guidelines
 Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical