Optimizing Cholesterol Lowering Therapy in Patients who Report Statin Adverse Events
|
|
|
- Rosalyn Strickland
- 5 years ago
- Views:
Transcription
1 Optimizing Cholesterol Lowering Therapy in Patients who Report Statin Adverse Events Robert S. Rosenson MD FACC, FACP, FAHA, FESC, FCCP, FNLA Professor of Medicine (Cardiology) Icahn School of Medicine at Mount Sinai New York, NY USA Co-Editor-in-Chief, Cardiovascular Drugs and Therapy Section Editor, Lipids, UpToDate Section Editor, Journal of the American College of Cardiology
2 Disclosures Research Grants to Institution: Akcea, Amgen, Astra Zeneca, Eli Lilly, Medicines Company, Regeneron, Sanofi Advisory Boards: Amgen, Easy Vitals, Regeneron, Sanofi Honoraria: Akcea, Kowa Royalties: UpToDate, Inc.
3 Cumulative risk for MI, CHD events, and all-cause mortality following MI 24,566 Medicare beneficiaries 65.5 years of age who had a MI between 2007 and 2011 and filled a high intensity statin, betablocker, ACE-I or ARB, and prescription antiplatelet agent (ie, intensively medically managed) within 30 days following hospital discharge Calculated the incidence of MI, CHD events, and all-cause mortality from 30 days after hospital discharge through December 31, 2012 Event rates for these beneficiaries were compared to two groups: 49,132 age, race-ethnicity, sex, and calendar-year matched beneficiaries each from (1) The general Medicare population (2) Medicare beneficiaries with diabetes Muntner P, Colantonio LD, Rosenson RS. Abstract P3634. European Heart Journal 2016;37(Abstract Supplement):731
4 Despite intensive medical management, substantial residual risk remains following MI Myocardial infarction, % Intensive medical management General Medicare population Medicare population with diabetes Primary myocardial infarction, % Intensive medical management General Medicare population Medicare population with diabetes Coronary heart disease events, % Intensive medical management General Medicare population Medicare population with diabetes All-cause mortality, % Intensive medical management General Medicare population Medicare population with diabetes Follow-up, years Follow-up, years Muntner P, Colantonio LD, Rosenson RS. Abstract P3634. European Heart Journal 2016;37(Abstract Supplement):731
5 Clinical benefit of lower LDL-C is determined by absolute exposure to lower LDL 80 Proportional reduction in risk of CHD, % Magnitude of exposure to lower LDL-C (mmol/l) Mendelian randomization studies Median follow-up: 52 years (N = 194,427) Prospective cohort studies Median follow-up: 12 years (N = 403,501) Randomized controlled trials Median follow-up: 5 years (N = 196,552) Ference BA, et al. Eur Heart J 2017 [Epub ahead of print] doi: /eurheartj/ehx144
6 Underutilization of statin therapy for secondary prevention Registry Years N Statin prescribed Inclusion criteria PINNACLE ,029,633 72% Adults with confirmed ASCVD TRIUMPH ,271 91% + 23% Adults hospitalized with ACS, discharged alive, no contraindications to statin PREMIER + TRIUMPH ,748 88% /33% Adults hospitalized with ACS, discharged alive GWTG ,396 89% /38% Adults hospitalized with ACS, prescribed lipid-lowering therapy at discharge Any statin therapy Maximally potent statin at hospital discharge (rosuvastatin mg or atorvastatin 80 mg) Any statin therapy at hospital discharge Statin at 75% of the target dose at hospital discharge Intensive lipid-lowering therapy 1. Maddox TM, et al. J Am Coll Cardiol 2014;64: Arnold SV, et al. J Am Coll Cardiol 2013;62: Arnold SV, et al. Circulation 2014;129: Javed U, et al. Am Heart J 2011;161: Hirsh BJ, Smilowitz NR, Rosenson RS, Fuster V, Sperling LS. J Am Coll Cardiol 2015;66:
7 What characteristics are associated with continued high adherence to statin therapy? a. Participation in cardiac rehabilitation b. More frequent outpatient cardiology visits c. Low income subsidy d. Use of internet e. Choice a, b and c Correct answer: d Colantonio LD, et al. JAMA Cardiol 2017 [Epub ahead of print] doi: /jamacardio
 in Medicare beneficiaries,<75 years Evidence-based")

8 Change in statin intensity pre- and posthospitalization for acute coronary syndrome, POST-HOSPITALIZATION PRE-HOSPITALIZATION 16.8% High-intensity statin 53.1% Low/moderateintensity statin Hospitalization for ACS (MI or unstable angina requiring coronary intervention) in Medicare beneficiaries,<75 years Evidence-based guideline therapy Biomarker-(LDL-C) directed therapy or insufficient posthospitalization transition 27.0% 73.0% High-intensity statin 11.5% change over 365 days post discharge Low/moderateintensity statin 30.1% No statin 88.5% did not change over 365 days post discharge No change in therapy Rosenson RS, et al. J Am Coll Cardiol 2015; 65:
9 Type of statin filled after hospital discharge for myocardial infarction, MarketScan beneficiaries <65 years of age Medicare beneficiaries years of age Rosenson RS, et al. J Am Coll Cardiol 2017;69:

10 Trends in the use of high-intensity statin therapy Rosenson RS, et al. J Am Coll Cardiol 2017;69:
11 Adherence to statin therapy for secondary prevention of CAD in registry databases Interview with medication review Proportion of days covered 80% Proportion of days covered 50% Continuation without >60-day gap Medication possession ratio 80% CAD, coronary artery disease Registry Years N Hirsh BJ, Smilowitz NR, Rosenson RS, Fuster V, Sperling LS. J Am Coll Cardiol 2015;66: Statin adherence PREMIER , % KPCO ,596 74% CMS Chronic Condition Data Warehouse , % Medicare Part D Enrolees , % PharmMetrics Patient Centric Database 5 MedStat MarketScan Commercial Claims and Encounters Database + Medicare Supplemental and Coordination of Benefit Database ,331 50% , % Inclusion criteria Adults hospitalized with ACS, discharged alive, no contraindications to statin Patients in Kaiser CAD registry with prior MI, PCI, or CABG Medicare beneficiaries with CHDrelated hospitalization, filled prescriptions for antihypertensive, initiation of statin therapy within 90 days of hospital discharge Medicare Part D enrollees with diabetes Statin naïve adults with a prior cardiac event and 1 prescription for atorvastatin or simvastatin Patients who initiated statin treatment within 6 months of hospitalization for cardiovascular disease Follow-Up (Years) 1. Ho PM, et al. Arch Intern Med 2006;166: Ho PM, et al. Am Heart J 208;155: Muntner P, et al. Am J Cardiol 2014;114: Yang Y, et al. Clin Ther 2009;31: , Discussion Foody JM, et al. Curr Med Res Opin 2008;24: Ye X, et al. Clin Ther 2007;29:
:890-895. doi:10.1001/jamacardio.2017.0911")
12 Adherence to High-Intensity Statins Following a Myocardial Infarction Hospitalization Among Medicare Beneficiaries Colantonio LD, Huang L, Monda KL, Bittner V, Serban MC, Taylor B, Brown TM, Glasser SP, Muntner P, Rosenson RS. JAMA Cardiol. 2017;2(8): doi: /jamacardio
13 What are the healthcare consequences of statin downtitration/discontinuation? a. Financial savings from reduced medication costs b. Higher risk of cardiovascular events c. Financial costs increase as a consequence of more outpatient visits/hospitalization costs d. Choices: a,b,c e. Choices: b,c Correct answer: e
14 Side effects are commonly reported by people taking statins 16,362 currently active REGARDS participants 14,224 have completed the statin survey 7,803 reported having ever taken a statin 1,874 (24%) reported experiencing side effects Of those experiencing side effects, 1,075 (57%) discontinued their statin Of those who discontinued a statin, 73% did not want a rechallenge Tanner RM, et al. AHA Session EP. APS.P266. T2015/2015
15 Statin-associated muscle symptoms Incidence, % Study On statin On placebo STOMP NHANES *CoQ *GAUSS Analysis of 42 clinical trials with 56,059 patients *Patients with a history of statin-associated muscle symptoms; non-statin users 1. Parker BA, et al. Circulation 2013;127:96 103; 2. Buettner C, et al. J Gen Intern Med 2008;23: ; 3. Taylor BA, et al. Atherosclerosis 2015;238: ; 4. Nissen SE, et al. JAMA 2016;315: ; 5. Ganga HV, et al. Am Heart J 2014;168:6 15
16 Nocebo effect influence of blinding and unblinding on reported statin-related AEs ASCOT-LLA Atorvastatin 10 mg qd versus matching placebo 5.5 years follow-up During the blinded phase (median 3.3 years follow-up), there was no significant difference between atorvastatin and placebo in the proportion of patients reporting muscle-related symptoms % vs 2.00% per annum However, during the unblinded phase (median 2.3 years follow-up), statin users reported a 41% excess of muscle-related symptoms compared with non-users (P=0.006) % vs 1.00% per annum Muscle-related symptoms and statin intolerance have been attributed to a nocebo effect subjective symptoms largely influenced by media hype about statins 2 Gupta A, et al. Lancet 2017; pii: S (17) [Epub ahead of print]; Tobert J, Newman C. J Clin Lipidol 2016;10:
17 Claims-based algorithm for the assessment of statin intolerance and clinical events Developed using claims data from 134,863 Medicare beneficiaries who initiated statin therapy between 2007 and Statin intolerance within 365 days after initiation based on clinical rationale and data availability. Those with statin intolerance were compared with those with high adherence to statins (proportion of days covered 80% following statin initiation). Colantonio LD, Kent ST, Huang L, Chen L, Monda KL, Serban MC, Manthripragada A, Kilgore ML, Rosenson RS, Muntner P. Cardiovasc Drugs Ther. 2016;30:
18 Algorithm Definitions of Statin Intolerance Definition 1: 1. Statin discontinuation with the initiation of ezetimibe; 2. Initiation of ezetimibe within 7 days before or after down-titrating statin dose; 3. A claim for rhabdomyolysis followed by statin down-titration discontinuation; 4. An inpatient or outpatient claim for adverse effect of an antihyperlipidemic agent followed by statin down-titration or discontinuation; and 5. Fills for 3 types of statins within one year. Definition 2: Included components of Definition 1 and down-titration of statin therapy. Definition 3: Included components of Definitions 1 and 2 and discontinuation of statin therapy. Colantonio LD, Kent ST, Huang L, Chen L, Monda KL, Serban MC, Manthripragada A, Kilgore ML, Rosenson RS, Muntner P. Cardiovasc Drugs Ther. 2016;30:
19 Is Statin Intolerance Associated with Recurrent MI, CHD Events and Mortality? Medicare beneficiaries initiating moderate/high intensity statins after myocardial infarction ( ). Exposure: statin intolerance by Definition 1 (n=1,741) versus high adherence to statins (n=55,567). Outcomes: Recurrent myocardial infarction, Coronary heart disease events, and All-cause mortality. Medicare expenditures were also analyzed. Serban MC, Colantonio LD, Manthripragada A, Monda KL, Bittner V, Banach M, Chen L, Huang L, Dent R, Kent ST, Muntner P, Rosenson, RS. J Am Coll Cardiol 2017;69:
 Exposure: statin SDD (n=1,741) versus high adherence to statins (n=55,567) Outcomes Recurrent myocardial")
20 Is statin switch/down-titration/discontinuation (SDD) associated with recurrent MI, CHD events and mortality? Medicare beneficiaries initiating moderate/high intensity statins after MI ( ) Exposure: statin SDD (n=1,741) versus high adherence to statins (n=55,567) Outcomes Recurrent myocardial infarction Coronary heart disease events All-cause mortality Composition of SDD group Switching between 3 types of statin within 1 year after initiation (59.3%) Switching from statins to ezetimibe monotherapy (17.0%) Having ICD-9 codes for rhabdomyolysis followed by statin down-titration or discontinuation (11.4%) Down-titrating statins and initiating ezetimibe (11.1%) SDD, switch/down-titration/discontinuation Having ICD-9 codes for antihyperlipidemic adverse event followed by statin down-titration or discontinuation (1.2%) Serban MC, Colantonio LD, Manthrigrapagada AD, Monda KL,, Bittner VA, Banach M, Chen L, Huang L, Dent RD Kent ST, Muntner P, Rosenson RS. J Am Coll Cardiol 2017;69:
21 Clinical outcomes associated with statin SDD High adherence (n=55,567) Statin SDD (n=1,741) Recurrent myocardial infarction Events 4, CHD, coronary heart disease; CI, confidence interval. Incidence rates are presented per 1,000 person-years *Includes adjustment for age, race/ethnicity, sex, and history of diabetes, chronic kidney disease, stroke, heart failure, antihypertensive medication use and adherence, and Charlson comorbidity index p-value Incidence rate (95% CI) 30.1 (29.2, 31.0) 41.1 (35.4, 46.8) <0.001 Hazard ratio (95% CI)* 1 (reference) 1.50 (1.30, 1.73) <0.001 CHD events Events 5, Incidence rate (95% CI) 43.8 (42.7, 44.9) 62.5 (55.3, 69.8) <0.001 Hazard ratio (95% CI)* 1 (reference) 1.51 (1.34, 1.70) <0.001 All-cause mortality Events 13, Incidence rate (95% CI) 94.2 (92.6, 95.7) 79.9 (72.1, 87.6) Hazard ratio (95% CI)* 1 (reference) 0.96 (0.87, 1.06) SDD, switch/down-titration/discontinuation Serban MC, Colantonio LD, Manthripragada A, Monda KL, Bittner V, Banach M, Chen L, Huang L, Dent R, Kent ST, Muntner P, Rosenson, RS. J Am Coll Cardiol 2017;69:
22 Excess risk from statin SDD Statin SDD 1.65% Myocardial infarction (n = 105,329) 50% increased risk for recurrent MI* 51% increased risk for CHD* High adherence 52.8% SDD, switch/down-titration/discontinuation *Excess risk compared with high adherence after multivariable adjustment Serban MC, Colantonio LD, Manthripragada A, Monda KL, Bittner V, Banach M, Chen L, Huang L, Dent R, Kent ST, Muntner P, Rosenson, RS. J Am Coll Cardiol 2017;69:
23 Continued Statin Prescriptions After Adverse Reactions and Patient Outcomes: A Cohort Study Organ System Distribution of the First Documented Adverse Reaction Among Study Patients, by Continuation of Statin Prescriptions During the First 12 Months After the Presumed Adverse Reaction* Adverse Reaction Category All Patients (n=28,266) Patients With Continued Statin Prescriptions Yes (n=19, 989) No (n= 8277) Myalgia or myopathy 6943 (24.6) 4903 (24.5) 2040 (24.7) Muscuskeletal and connective tissue disorders other than myalgia or myopathy General disorders and administration site conditions 5044 (17.8) 3594 (18.0) 1450 (17.5) 3521 (12.5) 2517 ( (12.1) Hepatobiliary disorders 2965 (10.5) 2036 (10.2) 929 (11.2) Drug intolerance 2223 (7.9) 1489 (7.5) 734 (8.9) Gastrointestinal disorders 2517 (8.9) 1809 (9.1) 708 (8.6) Nervous system disorders 1021 (3.6) 751 (3.8) 270 (3.3) Other 4032 (14.3) 2890 (14.5) 1142 (13.8) * Values are numbers (percentages). Adverse reactions were classified according to the Medical Dictionary for Regulatory Activities. A single adverse reaction could be classified only in a single category. Includes generalized weakness, cold sweats, and lack of energy. Includes intolerance and decreased tolerance. Zhao et al. Ann Intern Med 2017.
24 Continued Statin Prescriptions After Adverse Reactions and Patient Outcomes: A Cohort Study Inverse probability weighted cumulative incidence curves: continued versus discontinued statin prescriptions during the first 12 months after the presumed adverse reaction Zhao et al. Ann Intern Med CV = cardiovascular. A. The composite primary outcome (P < , weighted log-rank test). B. Death (P < , weighted log-rank test). C. CV events (P = 0.047, weighted log-rank test).
25 Summary Underutilization of evidence-based (IA) recommendations remains a major healthcare challenge in the United States even for the highest-risk patients hospitalized for a CHD event Down-titration or discontinuation of high intensity statins is common following hospitalization for MI Maintaining high adherence to high or low/moderate intensity statins is associated with lower risk for CVD hospitalization and all-cause mortality Strategies for improved adherence require health system factors, provider behavior and patient factors including early identification of statin intolerance using validated tools
26 What is the best approach to evaluate and prevent statin adverse muscle events? a. Recommend coenzyme Q10 for all statin users b. Recommend vitamin D supplementation for all statin users. c. Assess symptoms using validated clinical tool. d. Communicate with patients regarding concerns/fears of statin therapy. e. Encourage use of internet for assessment of adverse events f. Choice: c,d Correct answer: f Colantonio LD, et al. JAMA Cardiol 2017 [Epub ahead of print] doi: /jamacardio
27 Statin-Intolerance The true incidence of statin intolerance has been questioned due to conflicting rates of muscle-related symptoms, isolated case reports of cognitive impairment and other rare adverse events in observational studies and randomized trials. Statin associated muscle symptoms accounts for 90% of statin intolerance Diagnosis of statin intolerance is primarily based on subjective patient complaints. Statin intolerance may be complete (inability to tolerate any statin at any dosage) or partial (ability to tolerate low or intermittent dosing of statin).
28 Non-Specificity of Self-Reported SAMS STOMP: 9.4% (4.6% on placebo) NHANES: 22% (16.7% non-statin users) *CoQ10: 36% (29% on placebo) *GAUSS-3: 43% (27% on placebo) Analysis of 42 clinical trials with 56,059 patients: 13% (13% on placebo) * Patients with a history of SAMS Parker et al. 2013; Buettner et al. 2008; Taylor et al. 2015; Nissen et al. 2016; Ganga et al. 2014
29 Definition Of Statin-Associated Muscle Symptoms (SAMS) NLA 2015 Statement Myalgia unexplained muscle discomfort often described as flu-like symptoms with normal CK level Myopathy muscle weakness Myositis muscle inflammation often with muscle enzyme elevations Myonecrosis elevation in muscle enzymes, severity graded by elevation of CK level above pre-treatment baseline levels or ULN. Clinical rhabdomyolysis muscle injury with myoglobinuria and/or acute renal failure Rosenson RS, Baker SL, Jacobson TA, Kopecky SL, Parker NA. J Clin Lipidol 2014;8 (suppl 3):S58-71
30 Clinical Predictors Of Risk Older age, Asian race and gender (F>M) Exercise Comorbidity (hypothyroidism, hyeruricemia, alcohol overconsumption) Statin dose History of muscle pain with another lipid-lowering therapy Family history of muscular symptoms with lipid-lowering agents Concomitant medications (CYP3A4 with simvastatin, inhibitors of CYP3A4 and SLCO1B1 including azole antifungals, ritonavir, verapamil and diltiazem; gemfibrozil) Modified after Feng, Wilke and Baye. Pharmacogenomics 2012;13:
31 What is the Spectrum of Myalgia Symptoms? Muscle aches Muscle soreness Muscle stiffness Muscle tenderness Muscle cramps with or shortly after exercise. Not typically nocturnal cramping Rosenson RS, Baker SL, Jacobson TA, Kopecky SL, Parker NA. J Clin Lipidol 2014;8 (suppl 3):S58-71
32 Clinical Scoring Index For The Accurate Diagnosis Of SAMS Clinical symptoms (new or increased unexplained muscle symptoms Regional distribution/pattern Symmetric pelvic/ thigh aches 3 Symmetric calf aches 2 Symmetric upper proximal aches 2 Non-Specific asymmetric, intermittent 1 Temporal pattern Symptoms onset < 4 weeks 3 Symptoms onset 4-12 weeks 2 Symptoms-onset > 12 weeks 1 Dechallenge Improves upon withdrawal (< 2 weeks) 2 Improves upon withdrawal ( 2-4 weeks) 1 Does not improve 0 Challenge Same symptoms recurs upon re-challenge <4 weeks 3 Same symptoms recur upon re-challenge 4-12 weeks 1 Rosenson RS, Baker SL, Jacobson TA, Kopecky SL, Parker NA. J Clin Lipidol 2014;8 (suppl 3):S58-71
33 Clinical Scoring Index For The Accurate Diagnosis Of SAMS SAMS Clinical Index Score Probably 9-11 Possible 5-8 Unlikely <5 Rosenson RS, Baker SL, Jacobson TA, Kopecky SL, Parker NA. J Clin Lipidol 2014;8 (suppl3):s58-71 Revised after Rosenson RS, Sanchez R, Taylor B, Jacobson T. Cardiovasc Drugs Ther 2017; Taylor BA, Sanchez RJ, Jacobson TA, Chibedi deroche D, Manvelian G, Baccara-Dinet MT, Khan I, Rosenson RS. JACC 2017; 70:

34 Taylor BA, Sanchez RJ, Jacobson TA, Chibedi-De-Roche D, Manvelian G, Baccara-Dinet MT, Khan I, Rosenson RS. J Am Coll Cardiol. 2017;70:
35 Genetic Variations and SAMS Genetic variations may influence both an individual s therapeutic response to statins and propensity for SAMS SLCO1B1 reported to mediate hepatic transport of statins SNP rs has been associated with an increased risk of SAMS in simvastatin treated patients Increase of statin exposure by SLC01B1 c.521cc genotype (%) Serum [statin] associated with coding variant rs (Val174Ala) in SLCO1B1 gene Niemi M, et al. Pharmacol. Rev. 2011; 63: Brunham LR, et al. Pharmacogenics J. 2012; 12: SLCO1B1 = solute carrier organic anion transporter family, member 1B1
36 Sample Selection SAMS was confirmed in 149 adult Caucasians; 622 controls were on stable doses of statins in other evolocumab trials or were screen fails for SAMS in the GAUSS-3 study. STUDY PHENOTYPE SUBJECTS (N) SAMPLES (n) GENOTYPED* (n) GAUSS-3 Statin Rechallenge for Intolerance SAMS Confirmed Statin Rechallenge for Intolerance Screen Fails Cases (N=149) RUTHERFORD RUTHERFORD-2 HeFH on a Stable Dose of Statin + other lipid-lowering therapies HeFH on a Stable Dose of Statin + other lipid-lowering therapies Controls (N=622) LAPLACE-TIMI 57 Stable Dose of Statins *All samples meeting consent review and QC parameters were analyzed. Adult Caucasians selected from 159 total cases and 747 total controls.


37 Manhattan Plot Identifies 3 Genome-Wide Significant Loci of SAMS GW Suggestive MGAT5 ATP5O/MRPS6 KCNJ2/SOX9 GW Significant
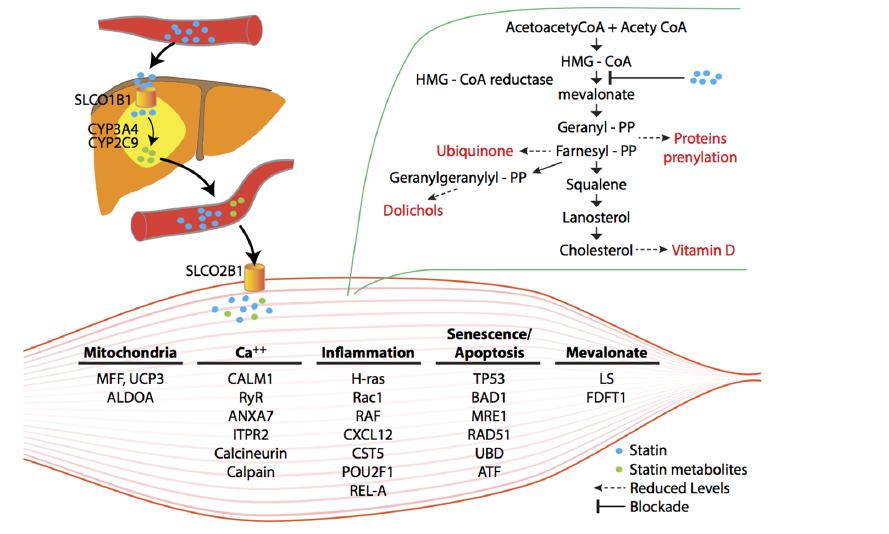
38 Biology of MRPS6 / ATP5O MRPS6 gene: Mitochondrial Ribosomal Protein S6 Translation of ribosomal proteins variants associated with CHD and early onset MI ATP5O gene: Mitochondrial ATP synthase Complex V ATP production via mitochondrial respiratory chain essential component of cellular energetics Mitochondria may provide a link between statins and SAMS, as statins potentially alter mitochondrial function by decreasing mitochondrial DNA, complex III activity, and oxidative phosphorylation Stroes ES, et al. Eur Heart J 2015; 36:
39 Functional annotation clustering of DEGs seen in the muscle of patients eperiencing statin myalgia (DA VID functional annotation clustering) Process Number of genes P= * FDR# Annotation Cluster 1: Protein Catabolism (Enrichment Score 6.89) Proteolysis involved in protein catabolic process E-5 1.9E-5 Cellular protein catabolic process E-5 2.2E-5 Protein catabolic process E-5 4.8E-5 Modification-dependent protein catabolic process E-5 6.9E-5 Ubi conjugation pathway E-5 1.4E-4 Cellular macromolecule catabolic process E-5 2.6E-4 Proteolysis E-2 1.3E-1 Annotation Cluster 2: Protein Ubiquitination (Enrichment Score 3.89) Small conjugating protein ligase activity E-2 3.7E-2 Ubiquitin-protein ligase activity E-3 5.0E-2 Acid-amino acid ligase activity E-2 2.6E-1 Annotation Cluster 3: Nuclear and Organelle Proteins (Enrichment Score 3.91) Nuclear lumen E-3 2.0E-2 Organelle E-2 2.7E-1 Intracellular organelle lumen E-2 2.8E-1 Membrane enclosed lumen E-2 4.5E-1 Functional clustering of 391 DEGs using DAVID Bioinformatics Resource (Version 6.7) accessed 9/28/2016 ( * P value adjusted for multiple comparisons (Benjamini-Hochberg). # FDR = False Discovery Rate
40

41

42 Clinical Pharmacokinetics of Statins Rosenson RS, et al. JACC 2017;70:

43 Nutrceuticals Lowering LDL-C in SAMS Patients Rosenson RS, et al. JACC 2017;70:
44 Nissen SE, Sroes E, Dent-Acosta RE, Rosenson RS, Lehman S, Sattar N, Preiss D, Bruckert E, Češka R, Lepor N, Ballantyne CM, Gouni-Berthold I, Elliott M, Brennan DM, Wasserman SM, Somaratne R, Scott R, Stein EA.JAMA 2016;315: GAUSS 3: Study design: two double-blind phases Phase A 511 patients with a history of intolerance to multiple statins due to muscle-related adverse effects 10 weeks Atorvastatin 20 mg Placebo 10 weeks Atorvastatin 20 mg Placebo Phase B 24 weeks Participants entered Phase B only if they had muscle symptoms on atorvastatin, but not placebo, or CK 10 x ULN during statin treatment Monthly SC evolocumab 420 mg 2 1 Daily oral ezetimibe 10 mg
45 Phase A: study drug discontinuation events Intolerable muscle symptoms N=491 On atorvastatin, but not placebo 209 (42.6%)* On placebo, but not atorvastatin 130 (26.5%) On both placebo and atorvastatin 48 (9.8%) No symptoms on either treatment 85 (17.3%) Did not complete Phase A 20/511 Bypassed Phase A due to CK elevation 10 x ULN 19 (3.9%)* *218 of these 228 patients proceeded to Phase B Nissen SE, Sroes E, Dent-Acosta RE, Rosenson RS, Lehman S, Sattar N, Preiss D, Bruckert E, Češka R, Lepor N, Ballantyne CM, Gouni-Berthold I, Elliott M, Brennan DM, Wasserman SM, Somaratne R, Scott R, Stein EA.JAMA 2016;315:
46 Phase B: Adverse effects and drug discontinuations Ezetimibe (n=73) Evolocumab (n=145) Total muscle-related events 21 (28.8%) 30 (20.7%) Myalgia, muscle pain or weakness 17 (23.3%) 25(17.2%) Investigator reported CK Increase 1 (1.4%) 4 (2.8%) Discontinuation of treatment for any reason Discontinuation of oral treatment 14 (19.2%) 23 (15.9%) Discontinued SC drug treatment 4 (5.5%) 7 (4.8%) Discontinuation of treatment for muscle symptoms Discontinued oral drug treatment 5 (6.8%) 11 (7.6%) Discontinued SC drug treatment 0 (0%) 1 (0.7%) Nissen SE, Sroes E, Dent-Acosta RE, Rosenson RS, Lehman S, Sattar N, Preiss D, Bruckert E, Češka R, Lepor N, Ballantyne CM, Gouni-Berthold I, Elliott M, Brennan DM, Wasserman SM, Somaratne R, Scott R, Stein EA. JAMA 2016;315:
 Alirocumab 75/150 mg SC Q2W + placebo PO QD administered via single 1 ml injection using prefilled pen for self-administration N=100 N=50 Per-protocol dose")
47 ODYSSEY ALTERNATIVE Study Design Statin intolerant patients* (by medical history) with LDL-C 70 mg/dl (very-high CV risk) or 100 mg/dl (moderate/ high risk) Placebo PO QD + Placebo SC Q2W R N=100 Double-Blind Treatment Period (24 Weeks) Alirocumab 75/150 mg SC Q2W + placebo PO QD administered via single 1 ml injection using prefilled pen for self-administration N=100 N=50 Per-protocol dose possible depending on W8 LDL-C Ezetimibe 10 mg PO QD + placebo SC Q2W Atorvastatin 20 mg PO QD + placebo SC Q2W OLTP/8 week FU Assessments W -4 W0 W4 W8 W12 W16 W24 Patients discontinued if muscle-related AEs reported with placebos during run-in Per-protocol dose increase if Week 8 LDL-C 70 or 100 mg/dl (depending on CV risk) Primary endpoint (LDL-C % change from baseline, ALI and EZE only) Safety analysis (all groups) 4-week single-blind placebo run-in follows 2-week washout of statins, ezetimibe and red yeast rice. OLTP: Alirocumab open-label treatment period; W, Week. Moriarty PM, et al. J Clin Lipidol. 2015
48 Fewer Skeletal Muscle AEs with Alirocumab than with Atorvastatin Kaplan-Meier estimates for time to first skeletal muscle event Cumulative probability of event Atorvastatin Ezetimibe Alirocumab Cox model analysis: HR ATV vs ALI = 1.63 (95% CI: 1.01 to 2.62), nominal P=0.042 HR EZE vs ALI = 1.41 (95% CI: 0.94 to 2.13), nominal P= Week Pre-defined category including myalgia, muscle spasms, muscular weakness, musculoskeletal stiffness, muscle fatigue. ALI, alirocumab; ATV, atorvastatin, EZE, ezetimibe.
49 Conclusions Statins are highly efficacious cholesterol lowering therapies with proven benefits in lowering cardiovascular events The inability to tolerate statins results in a higher cardiovascular event rate, more hospitalizations and more health care expenditures Strategies to accurately identify SAMS is an important healthcare challenge that involves validated screening tools and genetic markers Non-statin agents provide options for LDL-C lowering
PCSK9 inhibition across a wide spectrum of patients: One size fits all?
 PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Update on PCSK9 inhibitors and Statin Intolerance
 Update on PCSK9 inhibitors and Statin Intolerance Dr Amrish Agrawal MD, DM Card, MRCP UK, FRCP(Glas.), FRCP(Edin.) Fellow Cardiology (Australia), FCSI Consultant Cardiologist Ass. Professor of Medicine
Update on PCSK9 inhibitors and Statin Intolerance Dr Amrish Agrawal MD, DM Card, MRCP UK, FRCP(Glas.), FRCP(Edin.) Fellow Cardiology (Australia), FCSI Consultant Cardiologist Ass. Professor of Medicine
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Challenges in lipid management
 Challenges in lipid management Milan Gupta MD, FRCPC, FACC State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University of Toronto
Challenges in lipid management Milan Gupta MD, FRCPC, FACC State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University of Toronto
Pharmacology Challenges: Managing Statin Myalgia
 Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Evan A. Stein 1, David Sullivan 2, Anders G. Olsson 3, Rob Scott 4, Jae B. Kim 4, Allen Xue 4, Thomas Liu 4, Scott M. Wasserman 4
 Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, Double-blind, Placebo and Ezetimibe Controlled Study Evan A. Stein 1, David Sullivan
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, Double-blind, Placebo and Ezetimibe Controlled Study Evan A. Stein 1, David Sullivan
March 30, 2014, Joint ACC/JAMA Late-breaking Clinical Trials Session 402 American College of Cardiology, Washington DC
 A Phase 3 Double-blind, Randomized Study to Assess Safety and Efficacy of Evolocumab (AMG 145) in Hypercholesterolemic Subjects Unable to Tolerate an Effective Dose of Statin Erik Stroes 1, David Colquhoun
A Phase 3 Double-blind, Randomized Study to Assess Safety and Efficacy of Evolocumab (AMG 145) in Hypercholesterolemic Subjects Unable to Tolerate an Effective Dose of Statin Erik Stroes 1, David Colquhoun
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Praluent. Praluent (alirocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin intolerance. Pr Franck Boccara, MD, PhD Cardiologie, INSERM UMRS938 CHU St Antoine, UPMC, Paris, France
 Statin intolerance Pr Franck Boccara, MD, PhD Cardiologie, INSERM UMRS938 CHU St Antoine, UPMC, Paris, France Disclosure Statement of Financial Interest I currently have, or have had over the last two
Statin intolerance Pr Franck Boccara, MD, PhD Cardiologie, INSERM UMRS938 CHU St Antoine, UPMC, Paris, France Disclosure Statement of Financial Interest I currently have, or have had over the last two
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a
: Results from a") Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, d Double-blind, bli Placebo- Controlled Study Evan A. Stein 1, David Sullivan 2,
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, d Double-blind, bli Placebo- Controlled Study Evan A. Stein 1, David Sullivan 2,
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Case Study. Case Study. Case Study
 Case Study Patrick M Moriarty, M.D., Professor of Medicine Director of Clinical Pharmacology and the Atherosclerosis/Lipoprotein-apheresis Center University of Kansas Medical Center Aurora May 4 th 2018
Case Study Patrick M Moriarty, M.D., Professor of Medicine Director of Clinical Pharmacology and the Atherosclerosis/Lipoprotein-apheresis Center University of Kansas Medical Center Aurora May 4 th 2018
Praluent (alirocumab)
") Praluent (alirocumab) Policy Number: 5.01.600 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Praluent
Praluent (alirocumab) Policy Number: 5.01.600 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Praluent
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Anne Carol Goldberg, MD, FACP, FAHA, FNLA Washington University, St. Louis, MO USA
 Efficacy and Safety of Bempedoic Acid Added to Maximally Tolerated Statins in Patients with Hypercholesterolemia and High Cardiovascular Risk: The CLEAR Wisdom Trial Anne Carol Goldberg, MD, FACP, FAHA,
Efficacy and Safety of Bempedoic Acid Added to Maximally Tolerated Statins in Patients with Hypercholesterolemia and High Cardiovascular Risk: The CLEAR Wisdom Trial Anne Carol Goldberg, MD, FACP, FAHA,
2/23/2018. Management of Hyperlipidemia Update on Guidelines and Novel Therapies. Burden of Heart Disease in U.S.
 Management of Hyperlipidemia Update on Guidelines and Novel Therapies SHARATH SUBRAMANIAN, MD, FACC February 24, 2018 Disclosures : None Burden of Heart Disease in U.S. https://www.cdc.gov/nchs/images/databriefs/251
Management of Hyperlipidemia Update on Guidelines and Novel Therapies SHARATH SUBRAMANIAN, MD, FACC February 24, 2018 Disclosures : None Burden of Heart Disease in U.S. https://www.cdc.gov/nchs/images/databriefs/251
Statins ARE Enough For The Prevention of CVD! Professor Kausik Ray Imperial College London, UK
 1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/
1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
PCSK9 Inhibitors: A View of Clinical Studies
 PCSK9 Inhibitors: A View of Clinical Studies Slide deck kindly donated for website use by Professor Raul D. Santos Lipid Clinic InCor-HCFMUSP Sao Paulo, Brazil PCSK9 Inhibitors : A View of Clinical Studies
PCSK9 Inhibitors: A View of Clinical Studies Slide deck kindly donated for website use by Professor Raul D. Santos Lipid Clinic InCor-HCFMUSP Sao Paulo, Brazil PCSK9 Inhibitors : A View of Clinical Studies
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Industry Relationships and Institutional Affiliations
 Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated daily statin: results from the ODYSSEY COMBO II study Christopher
Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated daily statin: results from the ODYSSEY COMBO II study Christopher
EVOLOCUMAB Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378
 Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP
 STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP Peter P. Toth, MD, PhD, FAAFP, FICA, FNLA, FCCP, FAHA, FACC Director of Preventative Cardiology CGH Medical Center, Sterling, Illinois
STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP Peter P. Toth, MD, PhD, FAAFP, FICA, FNLA, FCCP, FAHA, FACC Director of Preventative Cardiology CGH Medical Center, Sterling, Illinois
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
Guidelines on Lowering LDL-C Levels
 Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
LDL How Low can (should) you Go and be Safe
 you Go and be Safe") LDL How Low can (should) you Go and be Safe Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Definition of Low LDL National Health and
LDL How Low can (should) you Go and be Safe Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Definition of Low LDL National Health and
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Quality ID #438: Statin Therapy for the Prevention and Treatment of Cardiovascular Disease National Quality Strategy Domain: Effective Clinical Care
 Quality ID #438: Statin Therapy for the Prevention and Treatment of Cardiovascular Disease National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Quality ID #438: Statin Therapy for the Prevention and Treatment of Cardiovascular Disease National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Clinical Policy: Evolocumab (Repatha) Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
The University of Mississippi School of Pharmacy
 LONG TERM PERSISTENCE WITH ACEI/ARB THERAPY AFTER ACUTE MYOCARDIAL INFARCTION: AN ANALYSIS OF THE 2006-2007 MEDICARE 5% NATIONAL SAMPLE DATA Lokhandwala T. MS, Yang Y. PhD, Thumula V. MS, Bentley J.P.
LONG TERM PERSISTENCE WITH ACEI/ARB THERAPY AFTER ACUTE MYOCARDIAL INFARCTION: AN ANALYSIS OF THE 2006-2007 MEDICARE 5% NATIONAL SAMPLE DATA Lokhandwala T. MS, Yang Y. PhD, Thumula V. MS, Bentley J.P.
MS Sabatine, RP Giugliano, AC Keech, PS Sever, SA Murphy and TR Pedersen, for the FOURIER Steering Committee & Investigators
 Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Repatha (evolocumab) Policy Number: Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019
 Policy Number: Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019") Repatha (evolocumab) Policy Number: 5.01.601 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Repatha
Repatha (evolocumab) Policy Number: 5.01.601 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Repatha
Management of LDL as a Risk Factor. Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil
 Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies
 Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Should I use statins?
 I know the trials in heart failure but how do I manage my patient? Should I use statins? Aldo P Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Disclosures Aldo P Maggioni served as a member of
I know the trials in heart failure but how do I manage my patient? Should I use statins? Aldo P Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Disclosures Aldo P Maggioni served as a member of
Cholesterol; what are the future lipid targets?
 Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
The ACCELERATE Trial
 The ACCELERATE Trial Impact of the Cholesteryl Ester Transfer Protein Inhibitor Evacetrapib on Cardiovascular Outcome Stephen J Nicholls for the ACCELERATE investigators Disclosure Research support: AstraZeneca,
The ACCELERATE Trial Impact of the Cholesteryl Ester Transfer Protein Inhibitor Evacetrapib on Cardiovascular Outcome Stephen J Nicholls for the ACCELERATE investigators Disclosure Research support: AstraZeneca,
1 DOS CME Course 2011
 Statin Myopathy February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 Case 1 50 y/o woman with hyperlipidemia presents with one year history of deep
Statin Myopathy February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 Case 1 50 y/o woman with hyperlipidemia presents with one year history of deep
Randomized Comparison of the Safety, Tolerability, and Efficacy of Long-term Administration of AMG 145: 52-Week Results From the OSLER Study
 Randomized Comparison of the Safety, Tolerability, and Efficacy of Long-term Administration of AMG 145: 52-Week Results From the OSLER Study Michael J Koren 1, Robert P Giugliano 2, Frederick Raal 3, David
Randomized Comparison of the Safety, Tolerability, and Efficacy of Long-term Administration of AMG 145: 52-Week Results From the OSLER Study Michael J Koren 1, Robert P Giugliano 2, Frederick Raal 3, David
Familial hypercholesterolaemia in children and adolescents
 Familial hypercholesterolaemia in children and adolescents Rationale and recommendations for early identification and treatment European Atherosclerosis Society Consensus Panel Slide deck adapted from:
Familial hypercholesterolaemia in children and adolescents Rationale and recommendations for early identification and treatment European Atherosclerosis Society Consensus Panel Slide deck adapted from:
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials?
 PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials? Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis
PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials? Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis
Long-term safety, tolerability and efficacy of alirocumab in high cardiovascular risk patients: ODYSSEY LONG TERM
 Long-term safety, tolerability and efficacy of alirocumab in high cardiovascular risk patients: ODYSSEY LONG TERM Efficacy by subgroup, and safety when LDL-C
Long-term safety, tolerability and efficacy of alirocumab in high cardiovascular risk patients: ODYSSEY LONG TERM Efficacy by subgroup, and safety when LDL-C
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
NEWS BRIEFING Diabetes and Cardiovascular Disease. Moderated by: Robert Eckel, MD University of Colorado
 NEWS BRIEFING Diabetes and Cardiovascular Disease Moderated by: Robert Eckel, MD University of Colorado 1 EMBARGO POLICY All recordings are for personal use only and not for rebroadcast online or in any
NEWS BRIEFING Diabetes and Cardiovascular Disease Moderated by: Robert Eckel, MD University of Colorado 1 EMBARGO POLICY All recordings are for personal use only and not for rebroadcast online or in any
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Cholesterol targets and therapy Thomas C. Andrews, MD, FACC
 Cholesterol targets and therapy Thomas C. Andrews, MD, FACC 2 Statins in secondary prevention Still first line therapy! First line therapy: high intensity statin Dose individualized based on baseline LDL
Cholesterol targets and therapy Thomas C. Andrews, MD, FACC 2 Statins in secondary prevention Still first line therapy! First line therapy: high intensity statin Dose individualized based on baseline LDL
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia
 : 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
: 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
Efficacy and Safety of Alirocumab in Patients with Hypercholesterolemia not on Statin Therapy: the ODYSSEY CHOICE II Study
 Efficacy and Safety of Alirocumab in Patients with Hypercholesterolemia not on Statin Therapy: the ODYSSEY CHOICE II Study Erik Stroes, 1 John Guyton, 2 Michel Farnier, 3 Norman Lepor, 4 Fernando Civeira,
Efficacy and Safety of Alirocumab in Patients with Hypercholesterolemia not on Statin Therapy: the ODYSSEY CHOICE II Study Erik Stroes, 1 John Guyton, 2 Michel Farnier, 3 Norman Lepor, 4 Fernando Civeira,
Clinical Policy: Alirocumab (Praluent) Reference Number: CP.CPA.268 Effective Date: Last Review Date: 11.17
 Reference Number: CP.CPA.268 Effective Date: Last Review Date: 11.17") Clinical Policy: (Praluent) Reference Number: CP.CPA.268 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for
Clinical Policy: (Praluent) Reference Number: CP.CPA.268 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for
RISK FACTORS AND DRUG TO STATIN-INDUCED MYOPATHY
 RISK FACTORS AND DRUG INTERACTION PREDISPOSING TO STATIN-INDUCED MYOPATHY Assist. Prof. Dr. Verawan Uchaipichat Clinical Pharmacy Department Khon Kaen University Advanced Pharmacotherapy 2012 Updated d
RISK FACTORS AND DRUG INTERACTION PREDISPOSING TO STATIN-INDUCED MYOPATHY Assist. Prof. Dr. Verawan Uchaipichat Clinical Pharmacy Department Khon Kaen University Advanced Pharmacotherapy 2012 Updated d
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
PCSK9 Inhibitors DRUG POLICY BENEFIT APPLICATION
 DRUG POLICY BENEFIT APPLICATION PCSK9 Inhibitors Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
DRUG POLICY BENEFIT APPLICATION PCSK9 Inhibitors Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study
 Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
EVIDENCE TO DATE EVOLOCUMAB (REPATHA)
") and Clinical Outcomes in Patients with Cardiovascular Disease, March 2017 1 CLINICAL QUESTION In patients with atherosclerotic cardiovascular disease and LDL >1.8mmol/L or non-hdl > 2.6mmol/L, how does
and Clinical Outcomes in Patients with Cardiovascular Disease, March 2017 1 CLINICAL QUESTION In patients with atherosclerotic cardiovascular disease and LDL >1.8mmol/L or non-hdl > 2.6mmol/L, how does
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Juxtapid (lomitapide)
") Juxtapid (lomitapide) Policy Number: 5.01.599 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Juxtapid
Juxtapid (lomitapide) Policy Number: 5.01.599 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Juxtapid
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2
 Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Educational Objectives. Disease Trajectories and CVD Risk Reduction. Hypercholesterolemia Support for LDL-C Causality
 Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements