HAEMODYNAMIC MONITORING in SEVERE PREECLAMPSIA. Eldrid Langesæter MD PhD Consultant Anaesthesiologist Oslo University Hospital Rikshospitalet
|
|
|
- Ira George
- 5 years ago
- Views:
Transcription

1 HAEMODYNAMIC MONITORING in SEVERE PREECLAMPSIA Eldrid Langesæter MD PhD Consultant Anaesthesiologist Oslo University Hospital Rikshospitalet Stockholm May 2011
2 Rikshospitalet Haemodynamics in severe preeclamspia Ullevål
3 CASE 1 Anxiety, otherwise healthy pregnant woman Remifentanil during labour 1 p.m: Spontanous vaginal delivery 2 p.m: GA for retained placenta hysterical, HR 150, SBP 180 mmhg 1000 ml bleeding
4 CASE 1 3 p.m: Postoperative Circulatory stable Tachycardia > 120 Considered anxious 8.30 p.m Hb7 Platelets 77 Difficulties inserting an arterial line SAP 220 mmhg Volume MgSO4
5 CASE p.m Circulatory collaps, intubated without any medication Hb4 HELLP with liver capsule rupture and DIC

6 AGENDA CMACE Guidelines Haemodynamic monitoring Anaesthetic implications Future research
7
8
9
10
11


12 BJOG 2009 Substandard care 96%
13 GUIDELINES AND RECOMMENDATIONS Evidence based mangement for preeclampsia Dadelszen et al. Frontiers in Bioscience 2007;12: Diagnosis,Evaluation, and Management of the Hypertensive Disorders of Pregnancy J Obst Gyn Can 2008 (3):S1 S48 Guidelines for the management of hypertensive disorders of pregnancy Aust NZJ Obst Gyn 2009;49:242 6
14 GUIDELINES AND RECOMMENDATIONS 1. Treat SAP 160 mmhg 2. MgSO4 Prevent Eclampsia Treat Eclampsia 3. Fluid restriction
15 Martin et al. Obstet Gynecol 2005: Few years ago, obstetricians focused on diastolic blood pressure only Is systolic blood pressure of 160 mmhg an adequate target? Non invasive devices for BP monitoring may underestimate BP in preeclamptic patients
16

17 CMACE

18 CMACE SAP 150 mmhg require effective antihypertensive treatment.


19 NON INVASIVE BLOOD PRESSURE
20 GUIDELINES AND RECOMMENDATIONS 1. Treat SAP 160 mmhg 2. MgSO4 Prevent Eclampsia Treat Eclampsia 3. Fluid restriction

21 Included patients NNT 69
22 MgSO4 Severe hypertension and proteinuria or Mild/moderate hypertension and proteinuria and (1) Severe headache Vision disturbance (blurring, flashing) Severe epigastrial pain or vomiting Papilloedema Signs of clonus Liver tenderness HELLP Platelets < ASAT/ALAT > 70
23 2 years ( )
24 2/210 had prophylactic MgSO4
25 Langesæter ACTA Anaesth Scand 2009
26 GUIDELINES AND RECOMMENDATIONS 1. Treat SAP 160 mmhg 2. MgSO4 Prevent Eclampsia Treat Eclampsia 3.Fluid restriction
27 FLUID RESTRICTION Recommendations based on one study (Evidence level 1)
28 Ganzevoort el al. BJOG 2005;112: patients Randomisation based on diastolic BP Treatment group: Plasma volume expansion and antihypertensive treatment Control group: Antihypertensive treatment Conclusion: No group differences in fetal and maternal outcome
29 ..evidence currently does not support plasma volume expansion as it may promote pulmonary oedema due to capillary leakage with no consistent effect on outcome. (ref. CEMACH)
30 Evidence for recommendation against plasma volume expansion?




31
32 PLASMA VOLUME EXPANSION Old studies using PA cather Belfort et al. BJOG 1989;96: Visser et al. Eur J Obst Gyn Repr Bio 1995;63: Recent studies using eccocardiography Valensise et al. Ultrasound Obst Gyn 2008;31:55 64 Plasma volume expansion and vasodilatation improved maternal and fetal circulation Blood pressure alone is not enough to guide treatment
33 Kuklina et al. Obst Gyn 2009;113:
34 IMPORTANT QUESTIONS Who are at risk for complications? Can recommendations be generalized in this patient group? Is monitoring of blood pressure enough in thehighrisk patients? Canlongtime morbidity and mortality be reduced? Bellamy et al. BMJ 2007; 335(7627) McDonaldet al. Am Heart J 2008; 156 (5):918 30
35 PREDICTORS FOR INCREASED RISK Early onset preeclampsia (< 34 weeks) Valensise et al. Hypertension 2008;52: Increased systemic vascular resistance Valensise et al. BJOG Mei et al. J Obst Gyn Res (2):179 88
 TPR 739 CO 9")
36 Hypertension 2008;52: EARLY (n=75) TPR 1605 CO 4.5 LATE (n=35) TPR 739 CO 9
37 Mei et al. J Obst Gyn Res (2): High TPR 97073% patients Preeclamptic patients are

38 Early PE 1243 vs Late PE 583

39
40 CASE 2 32 years, Nullipara, GA 36.5, BMI 36 Hypertension 14 days Dyspnoe 4 days Ecco cor hypokinesiin septum and apex, left ventricle not dilatated EF (ejection fraction) 27% NYHA IV Hb14.4, platelets , ASAT 81, ALAT 74, haptoglobin < 0.2, U totalprotein/kreatinin ratio 548. SVRI > 5500 dynes.sec.cm 5 Pro BNP > 4000
41 CASE 2 IABP(intraaortic balloon pump) MgSO4 Caesarean section continuous spinal anaesthesia Bleeding 1600 ml, B lynch suture After delivery: no dyspnoe lying flat Ecco cor 6 weeks postpartum: EF 45%, NYHA I II
42
43 Clinica Chimica Acta 2010 Nov 11;411(21 22): sflts the soluble form of the type 1 receptor of the vascular endothelial growth factor (VEGF) Endoglin (seng) an endothelial receptor for transforming growth factor beta PIGF placental growth factor VEGF vascular endothelial growth factor
44 WHY MONITORING CARDIAC OUTPUT? No studies verify a better outcome using CO monitoring in the ICU..we are left with the physiological rationale as primary defense for monitoring Pinsky M. Curr Opin Crit Care 2003
45 CO = HR x SV MAP = CO x SVR
46 The LiDCOplus monitor 2 algorithms PulseCO continuous pulse power analysis LiDCO Measuring SV with lithium dilution technique Calibrated into the PulseCO A peripheral venous and arterial line Recalibration after delivery (?)

47

48



49
50 E.Langesæter A. Pauca


51 Dyer et al. BJA 2010
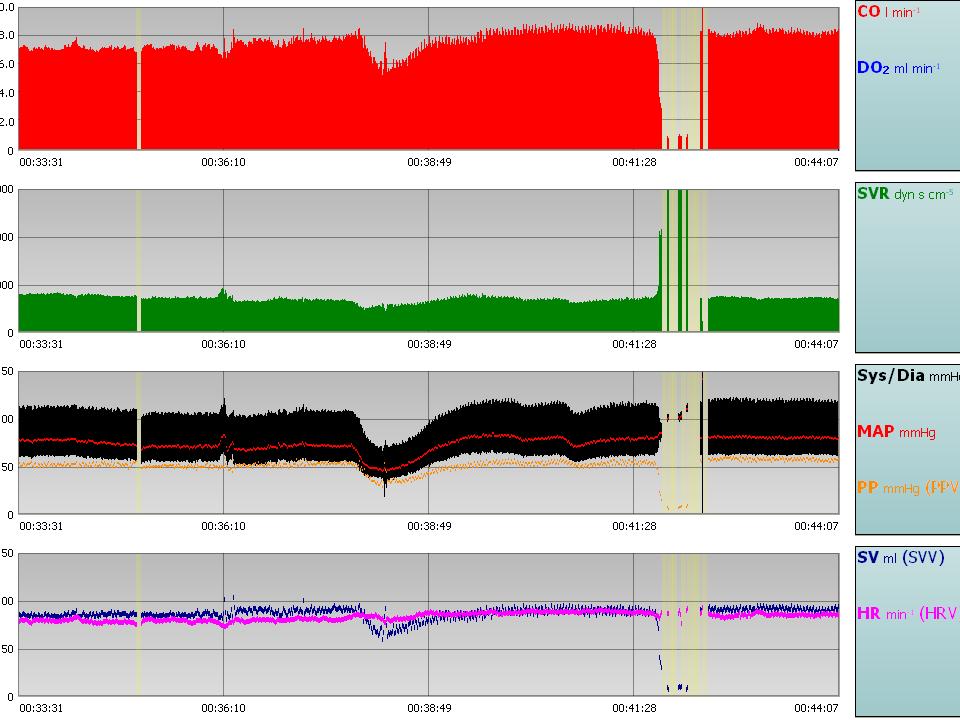
52 2 cases with severe PE the same blood pressure CASE A CASE B BP 193/90 (135) HR 66 BP 189/96 (130) HR 103 CO 5.3 l/min SVR 1900 CO 9.3 l/min SVR 1100
53 POSTPARTUM CASE A BP 145/86 (110) HR 71 SV 49 CO 2.9 l/min SVR 2800 Vasodilatation Plasma volume expansion 10 litre crystalloids (24 hours) CASE B 147/79 (105) HR 64 SV 141 CO 9.0 l/min SVR 900 Diuretics
54 .., calibrated pulse contour or pulse power algorithms may have a valuable future role, because only an arterial and peripheral line are required. Simply measuring cardiac output and blood pressure allows calculation of the systemic vascular resistance, which guides the appropriate use of fluids, diuretics, vasodilators and, occasionally, inotropes.
55 ABORTION GA 21.6 Renal causes or preeclampsia?
56 2 hours before abortion
57 4 hours after abortion
58 20 hours after abortion

59 ANAESTHESIA FOR CAESAREAN SECTION Spinal anaesthesia Oxytocin
60 G. Sharwood Smith & G.B. Drummond
61 12 Healthy all hypotensive after SA 15 PE 4 hypotensive after SA (2 superimposed PE) Spinal catheter L3 4, 16 G Procaine 0.2%, 5 8 ml (C8 T2)


62
63 Langesæter et al. Anesthesiology 2008
64 Evt pas carboto studie
65
66
67 ) m in (L / O C Hemodynamic effects of spinal anesthesia Healthy Preeclampsia m -5) c ċ e s y neṡ (d V R S ) m Hg (m B P S ) (m l V S Time (in seconds) SPINAL ANAESTHESIA 31 women with severe PE 80 healthy pregnant women (unpublished data)
68 OXYTOCIN
69 OXYTOCIN 5 IE i.v Langesæter et al. Int J Gyn Obst 2006;95:46 7 ED95% 0.35 units (not in labour) ED95% 3 units (in labour) Carvalho et al. Obst Gyn 2004;104; Balki et al. Obst Gyn 2006;107:45 50
70 BJA 2008
71 Dyer et al. Anesthesiology 2008;108: IE
72 5/18 women with severe preeclampsia had a decrease in cardiac output after 5 units oxytocin i.v
73 5 units oxytocin i.v 18 women with severe preeclampsia 80 healthy pregnant women

74
75
76

77
78 Anaesthetist involved early Screening with ecco cor (pro BNP) Focus on fluid balance (diuresis) Magnesium Sulphate Antihypertensive treatment postpartum Long time follow up Impact on outcome? Reduced morbidity?
79 Antihypertensive treatment, SAP 150 mmhg MgSO4 and volume Continuous invasive blood pressure monitoring Titrateddoses of oxytocin Continue antihypertensive therapy postpartum SAP < 140 mmhg Labetolol, Adalat Oros 30 mg Diuresis Volume Diuretics if dyspnoe Low treshold for ecco cor
80 FUTURE RESEARCH Predicting risk in womenwithpreeclampsia Useofnon invasive techniques (echocardiography) How to randomise in this heterogenous patient group? Plasma volume expansion? PPCM and PE
81
82 Semin.Perinatol. 2009, 33:
83 ACUTE FATTY LIVER OF PREGNANCY

84 J Am Soc Nephrology 2010
85
86 Visser, Hypertension 1991









87 Young



88
89 Can umbilical ph be used as end point? Umbilical ph Can not be used for evaluation of the best anaesthesia Apgar Not sensitive enough
90 Clark 1989 Cardiac output 6.5 SVR 1129 MAP 93.5 HR 93

91
92
Pre-eclampsia: key issues. Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford
 Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford Antenatal Issues Labour Analgesia Anaesthesia for Delivery High Dependency Care Hypertension systolic >140 mmhg or diastolic
Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford Antenatal Issues Labour Analgesia Anaesthesia for Delivery High Dependency Care Hypertension systolic >140 mmhg or diastolic
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia. RA Dyer Interlaken 2017
 The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
SEVERE PRE-ECLAMPSIA
 DEFINITIONS SEVERE PRE-ECLAMPSIA Pre-eclampsia: pregnancy induced hypertension with significant proteinuria +/- oedema affecting virtually any organ system in the body Severe pre-eclampsia: Diastolic blood
DEFINITIONS SEVERE PRE-ECLAMPSIA Pre-eclampsia: pregnancy induced hypertension with significant proteinuria +/- oedema affecting virtually any organ system in the body Severe pre-eclampsia: Diastolic blood
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY
 CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
Guideline for Management of Severe or Fulminating Pre-Eclampsia
 Guideline for Management of Severe or Fulminating Pre-Eclampsia Originator: Labour Ward Forum, Maternity Services Date Approved: September 2011 Approved by: W&CH Quality & Safety Group Reviewed and ratified
Guideline for Management of Severe or Fulminating Pre-Eclampsia Originator: Labour Ward Forum, Maternity Services Date Approved: September 2011 Approved by: W&CH Quality & Safety Group Reviewed and ratified
Preeclampsia: What s old is new again. Gene Chang, MD Maternal Fetal Medicine
 Preeclampsia: What s old is new again Gene Chang, MD Maternal Fetal Medicine Objectives Define Preeclampsia Review current guidelines Role of proteinuria Timing of delivery Seizure prevention Severe Hypertension
Preeclampsia: What s old is new again Gene Chang, MD Maternal Fetal Medicine Objectives Define Preeclampsia Review current guidelines Role of proteinuria Timing of delivery Seizure prevention Severe Hypertension
INTRAVENOUS HYDRALAZINE POLICY
 PURPOSE INTRAVENOUS HYDRALAZINE POLICY The purpose of this policy is to: provide safe and effective care for women establish a local approach to care that is evidence based and consistent inform good decision
PURPOSE INTRAVENOUS HYDRALAZINE POLICY The purpose of this policy is to: provide safe and effective care for women establish a local approach to care that is evidence based and consistent inform good decision
Endothelial function is impaired in women who had pre-eclampsia
 Endothelial function is impaired in women who had pre-eclampsia Christian Delles, Catriona E Brown, Joanne Flynn, David M Carty Institute of Cardiovascular and Medical Sciences University of Glasgow United
Endothelial function is impaired in women who had pre-eclampsia Christian Delles, Catriona E Brown, Joanne Flynn, David M Carty Institute of Cardiovascular and Medical Sciences University of Glasgow United
Clinical features. Abnormal vasculogenesis and angiogenesis and releasing of antiangiogenic
 Clinical features Abnormal vasculogenesis and angiogenesis and releasing of antiangiogenic factors results in Vasospasm Endothelial dysfunction Etiology of various clinical signs and symptoms So, Preeclampsia
Clinical features Abnormal vasculogenesis and angiogenesis and releasing of antiangiogenic factors results in Vasospasm Endothelial dysfunction Etiology of various clinical signs and symptoms So, Preeclampsia
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient
 Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
You admitted a previously healthy nullipara at 36 weeks gestation who presented with new-onset periorbital edema and is found to have blood pressure
 Preeclampsia Case report You admitted a previously healthy nullipara at 36 weeks gestation who presented with new-onset periorbital edema and is found to have blood pressure readings of 150/100 to 155/105
Preeclampsia Case report You admitted a previously healthy nullipara at 36 weeks gestation who presented with new-onset periorbital edema and is found to have blood pressure readings of 150/100 to 155/105
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM
 MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
What to do when a heart failure patient becomes pregnant
 BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
AWHONN Oregon Section 2014
 AWHONN Oregon Section 2014 Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth Hypertensive in Pregnancy Carol J Harvey, MS, RNC-OB, C-EFM Clinical Specialist Northside
AWHONN Oregon Section 2014 Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth Hypertensive in Pregnancy Carol J Harvey, MS, RNC-OB, C-EFM Clinical Specialist Northside
CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan
 CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth New! Improving Health Care Response to Preeclampsia:
CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth New! Improving Health Care Response to Preeclampsia:
Cardiac Output Monitoring - 6
 Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Continuous Invasive Blood Pressure and Cardiac Output Monitoring during Cesarean Delivery
 PAIN MEDICINE Anesthesiology 2008; 109:856 63 Copyright 2008, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Continuous Invasive Blood Pressure and Cardiac Output Monitoring
PAIN MEDICINE Anesthesiology 2008; 109:856 63 Copyright 2008, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Continuous Invasive Blood Pressure and Cardiac Output Monitoring
Hemodynamic Changes in Obstetric Anesthesia. Sonia Vaida PANA, Hershey, April 2009
 Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
PERIPARTUM CARDIOMYOPATHY
 PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Mercy San Juan Medical Center. Preeclampsia and Other Hypertensive Disorders of Pregnancy
 SUBJECT: Preeclampsia and Other Hypertensive Disorders of Pregnancy DEPARTMENTS: FBC, Emergency Department PURPOSE: To outline the nursing management of inpatients who have preeclampsia or other hypertensive
SUBJECT: Preeclampsia and Other Hypertensive Disorders of Pregnancy DEPARTMENTS: FBC, Emergency Department PURPOSE: To outline the nursing management of inpatients who have preeclampsia or other hypertensive
HST 071. IN SUMMARY PREGNANCY INDUCED HYPERTENSION Classification of Hypertensive Disorders of Pregnancy
 Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY Classification of Hypertensive Disorders of Pregnancy HST
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY Classification of Hypertensive Disorders of Pregnancy HST
How to manage the pregnant woman with heart disease
 How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
Agonistic Autoantibodies to Angiotensin II Type I Receptor Contributes Partly to Placental Ischemia-Induced Cerebrovascular Abnormalities
 Agonistic Autoantibodies to Angiotensin II Type I Receptor Contributes Partly to Placental Ischemia-Induced Cerebrovascular Abnormalities Junie Paula Warrington 1, Fan Fan 1, Babbette B. LaMarca 1, Ralf
Agonistic Autoantibodies to Angiotensin II Type I Receptor Contributes Partly to Placental Ischemia-Induced Cerebrovascular Abnormalities Junie Paula Warrington 1, Fan Fan 1, Babbette B. LaMarca 1, Ralf
Outcomes of Pregnancies at Risk for Hypertensive Complications Managed Using Impedance Cardiography
 Outcomes of Pregnancies at Risk for Hypertensive Complications Managed Using Impedance Cardiography David G. Chaffin, M.D., 1 and Denise G. Webb, RNC, BSN 2 ABSTRACT We assessed the effect of antihypertensive
Outcomes of Pregnancies at Risk for Hypertensive Complications Managed Using Impedance Cardiography David G. Chaffin, M.D., 1 and Denise G. Webb, RNC, BSN 2 ABSTRACT We assessed the effect of antihypertensive
CONTROL OF BLOOD PRESSURE IN PREGNANCY: HOW HIGH IS TOO HIGH? EVELYNE REY, CHU Ste-Justine, Montreal
 CONTROL OF BLOOD PRESSURE IN PREGNANCY: HOW HIGH IS TOO HIGH? EVELYNE REY, CHU Ste-Justine, Montreal CONFLICTS OF INTEREST $: None Others: Canadian guidelines, CHIPS CSIM2015 2 LEARNING OBJECTIVES New
CONTROL OF BLOOD PRESSURE IN PREGNANCY: HOW HIGH IS TOO HIGH? EVELYNE REY, CHU Ste-Justine, Montreal CONFLICTS OF INTEREST $: None Others: Canadian guidelines, CHIPS CSIM2015 2 LEARNING OBJECTIVES New
Drugs used in obstetrics
 Drugs used in obstetrics Drugs used in obstetrics Drugs may be used to modify uterine contractions. These include oxytocic drugs used to stimulate uterine contractions both in induction of labour and to
Drugs used in obstetrics Drugs used in obstetrics Drugs may be used to modify uterine contractions. These include oxytocic drugs used to stimulate uterine contractions both in induction of labour and to
Preeclampsia. &Eclampsia. Hypertensive Disorders of Pregnancy. What we need to know about. Hypertensive Disorders of Pregnancy.
 Preeclampsia &Eclampsia Hypertensive Disorders of Pregnancy Barbara Koop MS, RNC-OB What we need to know about Hypertensive Disorders of Pregnancy Define clinical criteria for: Gestational hypertension,
Preeclampsia &Eclampsia Hypertensive Disorders of Pregnancy Barbara Koop MS, RNC-OB What we need to know about Hypertensive Disorders of Pregnancy Define clinical criteria for: Gestational hypertension,
Continuous monitoring of cardiac output: why and how
 33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Stroke in Pregnancy. Stroke in Pregnancy 6/23/13
 G5#$#Preven*ng#Maternal#Morbidity#and#Mortality#Via# Expanded#Scope#of#Nursing#Prac*ce#As#First#Responder# in#hypertensive#crisis#of#preeclampsia# The$presenter$reports$no$relevant,$influencing$financial$rela5onships.$
G5#$#Preven*ng#Maternal#Morbidity#and#Mortality#Via# Expanded#Scope#of#Nursing#Prac*ce#As#First#Responder# in#hypertensive#crisis#of#preeclampsia# The$presenter$reports$no$relevant,$influencing$financial$rela5onships.$
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Declaration of conflict of interest
 Declaration of conflict of interest Claudio Borghi Lectures fees: Menarini International, Servier International, Recordati International, Ely-Lilly USA, BMS, Boheringer Ingelheim, Novartis Pharma Research
Declaration of conflict of interest Claudio Borghi Lectures fees: Menarini International, Servier International, Recordati International, Ely-Lilly USA, BMS, Boheringer Ingelheim, Novartis Pharma Research
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Peripartum management of Rheumatic Heart Disease
 Peripartum management of Rheumatic Heart Disease Dr James Sartain Director of Anaesthesia & Perioperative Medicine Cairns & Hinterland Hospital & Health Service Talk outline Why (still) talk about RHD
Peripartum management of Rheumatic Heart Disease Dr James Sartain Director of Anaesthesia & Perioperative Medicine Cairns & Hinterland Hospital & Health Service Talk outline Why (still) talk about RHD
Pregnancy and Heart Disease
 Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Magnesium sulfate has an antihypertensive effect on severe pregnancy induced hypertension
 Hypertension Research In Pregnancy 11 S. Takenaka et al. ORIGINAL ARTICLE Magnesium sulfate has an antihypertensive effect on severe pregnancy induced hypertension Shin Takenaka 1, Ryu Matsuoka 2, Daisuke
Hypertension Research In Pregnancy 11 S. Takenaka et al. ORIGINAL ARTICLE Magnesium sulfate has an antihypertensive effect on severe pregnancy induced hypertension Shin Takenaka 1, Ryu Matsuoka 2, Daisuke
SESSION D5. The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Anesthesiology in advanced radical surgery. Bruno Carrara Ospedali Riuniti di Bergamo
 Anesthesiology in advanced radical surgery Bruno Carrara Ospedali Riuniti di Bergamo Anesthetic considerations Anesthesiology in advanced radical surgery Anesthesiologists's task is to minimize the contribution
Anesthesiology in advanced radical surgery Bruno Carrara Ospedali Riuniti di Bergamo Anesthetic considerations Anesthesiology in advanced radical surgery Anesthesiologists's task is to minimize the contribution
Counseling and Long-term Follow up After Gestational Disorders
 Counseling and Long-term Follow up After Gestational Disorders Tanya Melnik, MD Assistant Professor, University of Minnesota Sarina Martini, MD Ob/Gyn Resident, PGY4 University of Minnesota Counseling
Counseling and Long-term Follow up After Gestational Disorders Tanya Melnik, MD Assistant Professor, University of Minnesota Sarina Martini, MD Ob/Gyn Resident, PGY4 University of Minnesota Counseling
LEARNING OBJECTIVES 2/20/2017
 HYPERTENSION IN PREGNANCY: PREVENTING SEVERE MATERNAL MORBIDITY & MORTALITY THROUGH THE IMPLEMENTATION OF EVIDENCED BASED PROTOCOLS Laura Senn, RN, PhD, CNS Sutter Medical Center, Sacramento LEARNING OBJECTIVES
HYPERTENSION IN PREGNANCY: PREVENTING SEVERE MATERNAL MORBIDITY & MORTALITY THROUGH THE IMPLEMENTATION OF EVIDENCED BASED PROTOCOLS Laura Senn, RN, PhD, CNS Sutter Medical Center, Sacramento LEARNING OBJECTIVES
Closed-loop Double-pump Automated System Manual Boluses
 Closed-loop Double-pump Automated System versus Manual Boluses to treat Hypotension during Spinal Anaesthesia for Caesarean Section: randomised controlled trial Dr. Ban Leong SNG MBBS, MMED, FANZCA, FFPMANZCA,
Closed-loop Double-pump Automated System versus Manual Boluses to treat Hypotension during Spinal Anaesthesia for Caesarean Section: randomised controlled trial Dr. Ban Leong SNG MBBS, MMED, FANZCA, FFPMANZCA,
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
Comparision of Intravenous Bolus Phenylephrine and Ephedrine for Prevention of Post Spinal Hypotension in Cesarean Sections
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 7 Ver. II (July. 2015), PP 99-103 www.iosrjournals.org Comparision of Intravenous Bolus Phenylephrine
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 7 Ver. II (July. 2015), PP 99-103 www.iosrjournals.org Comparision of Intravenous Bolus Phenylephrine
Original Research Article
 A COMPARATIVE STUDY OF INTRAVENOUS LABETALOL WITH ORAL ANTIHYPERTENSIVE COMBINATION NIFEDIPINE AND ALPHA-METHYLDOPA IN THE ACUTE MANAGEMENT OF HIGH BLOOD PRESSURE IN SEVERE PREGNANCY-INDUCED HYPERTENSION
A COMPARATIVE STUDY OF INTRAVENOUS LABETALOL WITH ORAL ANTIHYPERTENSIVE COMBINATION NIFEDIPINE AND ALPHA-METHYLDOPA IN THE ACUTE MANAGEMENT OF HIGH BLOOD PRESSURE IN SEVERE PREGNANCY-INDUCED HYPERTENSION
Pregnancy and Neurological Disorders
 Pregnancy and Neurological Disorders Myles Connor NHS Borders and University of Edinburgh, United Kingdom Outline Why is it important? Specific conditions Eclampsia Cerebrovascular disease Epilepsy Idiopathic
Pregnancy and Neurological Disorders Myles Connor NHS Borders and University of Edinburgh, United Kingdom Outline Why is it important? Specific conditions Eclampsia Cerebrovascular disease Epilepsy Idiopathic
Sri Lankan Journal of Anaesthesiology 17(2) : (2009)
 : (2009)") Sri Lankan Journal of Anaesthesiology 17(2) : 55-60 (2009) COMPARISON OF PROPHYLACTIC INTRAMUSCULAR EPHEDRINE WITH PRELOADING VERSUS PRELOADING ALONE IN PREVENTION OF HYPOTENSION DURING ELECTIVE CAESAREAN
Sri Lankan Journal of Anaesthesiology 17(2) : 55-60 (2009) COMPARISON OF PROPHYLACTIC INTRAMUSCULAR EPHEDRINE WITH PRELOADING VERSUS PRELOADING ALONE IN PREVENTION OF HYPOTENSION DURING ELECTIVE CAESAREAN
Admission of patient CVICU and hemodynamic monitoring
 Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
SAFE approach. Unresponsive? Shout or call for help. Open Airway. Not Breathing normally? 30 chest compressions. 2 rescue breaths
 Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Impedance Cardiography (ICG) Application of ICG for Hypertension Management
 Application of ICG for Hypertension Management") Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
Spinal anesthesia without hypotension a myth or reality?
 Spinal anesthesia without hypotension a myth or reality? Peter Poredoš, MD, PhD, DESA peter.poredos@kclj.si University Medical Centre Ljubljana, Slovenia Department for Anesthesiology and Intensive Care
Spinal anesthesia without hypotension a myth or reality? Peter Poredoš, MD, PhD, DESA peter.poredos@kclj.si University Medical Centre Ljubljana, Slovenia Department for Anesthesiology and Intensive Care
Hypertension in Pregnancy. Dr Jenny Myers PhD MRCOG Senior Lecturer, Consultant Obstetrician St Mary s Hospital
 Hypertension in Pregnancy Dr Jenny Myers PhD MRCOG Senior Lecturer, Consultant Obstetrician St Mary s Hospital Maternal Mortality report 2006-8 Pre-eclampsia/eclampsia 2 nd highest cause of direct maternal
Hypertension in Pregnancy Dr Jenny Myers PhD MRCOG Senior Lecturer, Consultant Obstetrician St Mary s Hospital Maternal Mortality report 2006-8 Pre-eclampsia/eclampsia 2 nd highest cause of direct maternal
Comparison of Efficacy and Safety of Intravenous Labetalol Versus Hydralazine for Management of Severe Hypertension in Pregnancy
 https://doi.org/10.1007/s13224-017-1053-9 ORIGINAL ARTICLE Comparison of Efficacy and Safety of Intravenous Labetalol Versus Hydralazine for Management of Severe Hypertension in Pregnancy Purvi Patel 1
https://doi.org/10.1007/s13224-017-1053-9 ORIGINAL ARTICLE Comparison of Efficacy and Safety of Intravenous Labetalol Versus Hydralazine for Management of Severe Hypertension in Pregnancy Purvi Patel 1
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Postpartum hypertension, preeclampsia and eclampsia. Arun Jeyabalan, MD MS University of Pittsburgh
 Postpartum hypertension, preeclampsia and eclampsia Arun Jeyabalan, MD MS University of Pittsburgh Confusing concept Preeclampsia only occurs in pregnancy placenta is required Delivery cures preeclampsia
Postpartum hypertension, preeclampsia and eclampsia Arun Jeyabalan, MD MS University of Pittsburgh Confusing concept Preeclampsia only occurs in pregnancy placenta is required Delivery cures preeclampsia
Pregnancy in women with pulmonary hypertension
 Neth Heart J (2011) 19:504 508 DOI 10.1007/s12471-011-0219-9 SPECIAL ARTICLE Pregnancy in women with pulmonary hypertension P. G. Pieper & E. S. Hoendermis Published online: 9 November 2011 # The Author(s)
Neth Heart J (2011) 19:504 508 DOI 10.1007/s12471-011-0219-9 SPECIAL ARTICLE Pregnancy in women with pulmonary hypertension P. G. Pieper & E. S. Hoendermis Published online: 9 November 2011 # The Author(s)
Cesarean Section Should be Managed: Low Dose / CSE versus High Dose Spinals with Vasopressors
 Cesarean Section Should be Managed: Low Dose / CSE versus High Dose Spinals with Vasopressors Cristian Arzola MD MSc Department of Anesthesia and Pain Management Mount Sinai Hospital and University of
Cesarean Section Should be Managed: Low Dose / CSE versus High Dose Spinals with Vasopressors Cristian Arzola MD MSc Department of Anesthesia and Pain Management Mount Sinai Hospital and University of
Community monitoring of blood pressure and proteinuria Maternity
 Community monitoring of blood pressure and proteinuria V3 Page 1 of 5 Community monitoring of blood pressure and proteinuria Maternity 1. Introduction and who the guideline applies to: This guideline applies
Community monitoring of blood pressure and proteinuria V3 Page 1 of 5 Community monitoring of blood pressure and proteinuria Maternity 1. Introduction and who the guideline applies to: This guideline applies
PHYSIOLOGICAL CHANGES IN PREGNANCY AND OBSTETRIC EMERGENCIES
 PHYSIOLOGICAL CHANGES IN PREGNANCY AND OBSTETRIC EMERGENCIES Shankari Arulkumaran BSc MSc MD MRCOG Consultant Obstetrician and Gynaecologist St Mary s Hospital Imperial College NHS Trust OVERVIEW Obstetric
PHYSIOLOGICAL CHANGES IN PREGNANCY AND OBSTETRIC EMERGENCIES Shankari Arulkumaran BSc MSc MD MRCOG Consultant Obstetrician and Gynaecologist St Mary s Hospital Imperial College NHS Trust OVERVIEW Obstetric
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy
 Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy
 Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy A 44 year old female undergoing 10 hour Cytoreductive (CRS) procedure followed by Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy A 44 year old female undergoing 10 hour Cytoreductive (CRS) procedure followed by Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
Update on Hypertensive Diseases in Pregnancy
 Objectives Update on Hypertensive Diseases in Pregnancy ANNA MCCORMICK, DO MFM FELLOW, MEDICAL COLLEGE OF WISCONSIN At the conclusion of this session, attendees will be able to: Describe the classification
Objectives Update on Hypertensive Diseases in Pregnancy ANNA MCCORMICK, DO MFM FELLOW, MEDICAL COLLEGE OF WISCONSIN At the conclusion of this session, attendees will be able to: Describe the classification
Perioperative management of a patient with left ventricular failure
 Perioperative management of a patient with left ventricular failure Ramkumar Venkateswaran, MD Professor of Anaesthesiology Kasturba Medical College, Manipal University INTRODUCTION Congestive heart failure
Perioperative management of a patient with left ventricular failure Ramkumar Venkateswaran, MD Professor of Anaesthesiology Kasturba Medical College, Manipal University INTRODUCTION Congestive heart failure
Based on 2014 SOGC Guidelines
 Based on 2014 SOGC Guidelines 22nd Edition 2015 1 ICH + gestational hypertension by far the biggest cause of direct maternal deaths New stats coming in 2013 OCR 22nd Edition 2015 2 Diastolic 90 mmhg is
Based on 2014 SOGC Guidelines 22nd Edition 2015 1 ICH + gestational hypertension by far the biggest cause of direct maternal deaths New stats coming in 2013 OCR 22nd Edition 2015 2 Diastolic 90 mmhg is
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Complicated Severe Pre-eclampsia General or regional anaesthesia for caesarean section. Jim Bamber Cambridge University Hospitals
 Complicated Severe Pre-eclampsia General or regional anaesthesia for caesarean section Jim Bamber Cambridge University Hospitals This case presentation has the consent of the patient. You have just finished
Complicated Severe Pre-eclampsia General or regional anaesthesia for caesarean section Jim Bamber Cambridge University Hospitals This case presentation has the consent of the patient. You have just finished
Peripartum kardiomyopati
 Fall 3 Peripartum kardiomyopati Roman A roch 2017 01 26 2 3 Dg. PPCM Symptoms ECG, pro-bnp echocardiography 4 Peripartum cardiomyopathy: a systematic literature review Acta Obstetricia et Gynecologica
Fall 3 Peripartum kardiomyopati Roman A roch 2017 01 26 2 3 Dg. PPCM Symptoms ECG, pro-bnp echocardiography 4 Peripartum cardiomyopathy: a systematic literature review Acta Obstetricia et Gynecologica
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
Case Discussions Cynthia A. Wong, M.D.
 Case Discussions Cynthia A. Wong, M.D. Association des Anesthѐsiologistes du Quѐbec April 2014 CASE 1 Maternal Mortality Lewis G (ed). CEMACH 2007. Saving Mothers Lives 2003-2005 Pregnancy Complications
Case Discussions Cynthia A. Wong, M.D. Association des Anesthѐsiologistes du Quѐbec April 2014 CASE 1 Maternal Mortality Lewis G (ed). CEMACH 2007. Saving Mothers Lives 2003-2005 Pregnancy Complications
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Original Article. Summary. Introduction. M. Mohta, 1 S. Duggal 2 and G. T. Chilkoti 3
 Original Article doi:10.1111/anae.14268 Randomised double-blind comparison of bolus phenylephrine or ephedrine for treatment of hypotension in women with preeclampsia undergoing caesarean section* M. Mohta,
Original Article doi:10.1111/anae.14268 Randomised double-blind comparison of bolus phenylephrine or ephedrine for treatment of hypotension in women with preeclampsia undergoing caesarean section* M. Mohta,
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
Pre-Eclampsia New challenges for the Anaesthetist
 Pre-Eclampsia New challenges for the Anaesthetist OAA 3 day Course Church House Westminster 7/11/2012 Chris Elton Consultant in Obstetric Anaesthesia Leicester Royal Infirmary University Hospitals of Leicester
Pre-Eclampsia New challenges for the Anaesthetist OAA 3 day Course Church House Westminster 7/11/2012 Chris Elton Consultant in Obstetric Anaesthesia Leicester Royal Infirmary University Hospitals of Leicester
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertensive Disorders of Pregnancy Guideline
 Hypertensive Disorders of Pregnancy Guideline Approved by: Senior Director of Operations, Women s & Child Health, GNCH/MCH Facility Chief, Obstetrics/Gynecology, GNCH Facility Chief, Obstetrics/Gynecology,
Hypertensive Disorders of Pregnancy Guideline Approved by: Senior Director of Operations, Women s & Child Health, GNCH/MCH Facility Chief, Obstetrics/Gynecology, GNCH Facility Chief, Obstetrics/Gynecology,
Regional Anaesthesia for Caesarean Section
 Regional Anaesthesia for Caesarean Section "The Best Recipe" Warwick D. Ngan Kee Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong What I will not do. Magic recipes One shoe to fit
Regional Anaesthesia for Caesarean Section "The Best Recipe" Warwick D. Ngan Kee Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong What I will not do. Magic recipes One shoe to fit
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Risk Stratification in Pulmonary Hypertension and Pregnancy
 Risk Stratification in Pulmonary Hypertension and Pregnancy Dr Robin Condliffe Pulmonary Vascular Disease Unit Royal Hallamshire Hospital Sheffield United Kingdom Conflicts of Interest Honorararia Actelion,
Risk Stratification in Pulmonary Hypertension and Pregnancy Dr Robin Condliffe Pulmonary Vascular Disease Unit Royal Hallamshire Hospital Sheffield United Kingdom Conflicts of Interest Honorararia Actelion,
Acute heart failure, beyond conventional treatment: persisting low output
 Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
P215 SPRING 2019: CIRCULATORY SYSTEM Chaps 13, 14 & 15: pp , , , I. Major Functions of the Circulatory System
 P215 SPRING 2019: CIRCULATORY SYSTEM Chaps 13, 14 & 15: pp 360-390, 395-404, 410-428 433-438, 441-445 I. Major Functions of the Circulatory System 1. 2. 3. 4. II. Structure of the Heart 1. atria 2. ventricles
P215 SPRING 2019: CIRCULATORY SYSTEM Chaps 13, 14 & 15: pp 360-390, 395-404, 410-428 433-438, 441-445 I. Major Functions of the Circulatory System 1. 2. 3. 4. II. Structure of the Heart 1. atria 2. ventricles
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
https://www.lucidoc.com/cgi/doc-gw.pl?ref=overlake_p:53602
 Page 1 of 6 Protocol : Severe Hypertension in Obstetrics: Emergent Treatment DocID: 53602 Revision: 7 Status: Official Department: Women's and Infants' Admin Manual(s): Labor and Delivery Mother Baby Unit
Page 1 of 6 Protocol : Severe Hypertension in Obstetrics: Emergent Treatment DocID: 53602 Revision: 7 Status: Official Department: Women's and Infants' Admin Manual(s): Labor and Delivery Mother Baby Unit