Pregnancy and Heart Disease
|
|
|
- Dwight Douglas
- 5 years ago
- Views:
Transcription



1 Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER

2 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al.

3 Pregnancy and the Heart 2% of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk to mother and fetus 2011 MFMER
4 Pregnancy Physiologic Changes Blood volumes (% control) Gestational age (weeks) Plasma Whole blood Erythrocytes Am J Physiol MFMER

5 Hemodynamic Changes >40% in blood volume in SVR and PVR in HR 30% CO Little change in BP Usually well tolerated 2011 MFMER

6 Hemodynamic Changes Labor and Delivery CO 60-80% HR and BP changes Volume changes blood volume with uterine contraction venous return Volume loss during delivery 2011 MFMER

7 Advise Against Pregnancy Severe pulmonary arterial HT Severe obstructive lesions AS, MS, PS, HCM, Coarct 2011 MFMER

8 Advise Against Pregnancy Severe pulmonary arterial HT Severe obstructive lesions AS, MS, PS, HCM, Coarct Ventricular dysfunction Class III or IV CHF, EF <40% Prior peripartum cardiomyopathy Dilated or unstable aorta Marfan with aorta mm Severe cyanosis 2011 MFMER
9 Heart Disease in Pregnancy Prepregnancy evaluation Pregnancy Multidisciplinary care Peripartum OB, anesthesia, IE prophylaxis Postpartum 2011 MFMER
10

11 35-Year-Old Female Progressive dyspnea 3 weeks post partum 1st pregnancy Previously asymptomatic no CV history Exam JVP of 13 cm Diffuse apical impulse, gr 2 apical HSM S3 and S4 at apex Crackles both lung bases ECG sinus tachycardia 2011 MFMER
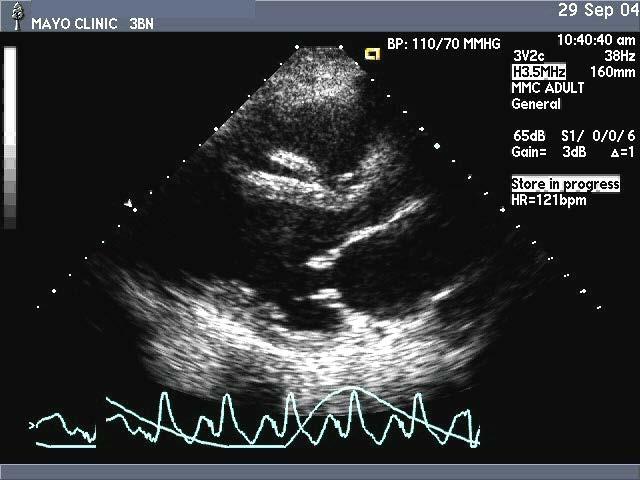
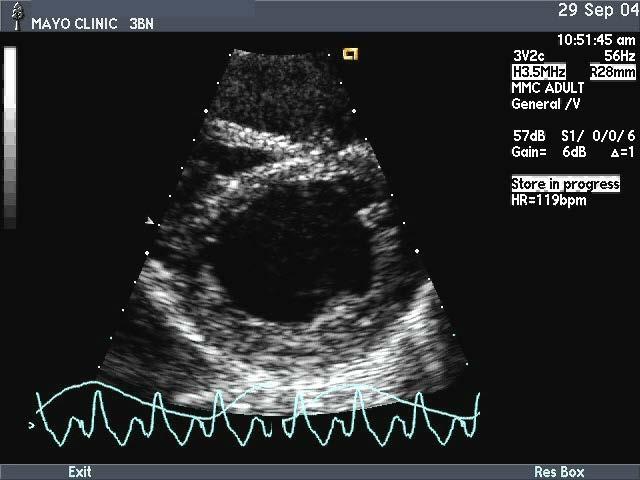
12 35-Year-Old Female 2011 MFMER

13 35-Year-Old Female Progressive CHF symptoms despite diuretics, digoxin, ACE inhibitor, beta-blocker, warfarin Echo global LV dysfunction, EF 25% Symptoms persist, SBP 100 mmhg 2011 MFMER
14 What would you suggest next? Bromocriptine 2011 MFMER
15 Peripartum Cardiomyopathy 50 Delivery 40 Patients (%) Month antepartum Month postpartum NEJM 312:1432, 1985
 South Africa 1 in 1000 Haiti 1 in 300 frequency Age >30 yr Multifetal pregnancy Multiparity Tocolytic Black women HT, DM, smoking")
16 Peripartum Cardiomyopathy New diagnosis of HF due to LV dysfunction Last trimester 6 mos postpartum Diagnosis of exclusion Incidence varies U.S. 1 in 3200 deliveries (1350/year) South Africa 1 in 1000 Haiti 1 in 300 frequency Age >30 yr Multifetal pregnancy Multiparity Tocolytic Black women HT, DM, smoking Elkayam: JACC, 2011

17 Peripartum Cardiomyopathy Pathophysiology Defective antioxidant defense mechanism Prolactin/bromocriptine Viral infection Autoimmune response Genetic susceptibility Sliwa et al: Eur J Heart Fail, 2010

18 Peripartum Cardiomyopathy Defective Antioxidant Defense Mechanism Due to oxidative stress levels of activated cathepsin D total prolactin and angiostatic 16 kda prolactin Inhibits endothelial cell proliferation and migration, induces apoptosis, disrupts capillary structures, promotes vasoconstriction and impairs cardiomyocyte function Suppression of prolactin production by bromocriptine, prevents onset of PPCM in mouse Sliwa et al: Circulation, 2010

19 Peripartum Cardiomyopathy Management Standard CHF Rx O 2, ACE, diuretic, iv NTG inotrope for CO Bromocriptine - blocks prolactin release EF in PPCM vs standard Rx 2.5 mg BID for 2 wk, then 2.5 mg QD for 6 wks with standard HF therapy Anticoagulation for EF <35%, or bromocriptine VAD or transplantation

20 Peripartum Cardiomyopathy Prognosis Variable Major cause of preg related death in US Mortality 6 mos and 2 yr 10 and 28% Sliwa et al: Eur J Heart Fail, 2010

21 Peripartum Cardiomyopathy Prognosis Variable Major cause of preg related death in US Mortality 6 mos and 2 yr 10 and 28% mortality with EF >6 mos postpartum ~50% improve in 6 months 20-40% normalize EF Recurrence with recurrent pregnancy Sliwa et al: Eur J Heart Fail, 2010

22 CHF in Pregnancy Conservative salt, bedrest Limited medical therapy Digoxin, hydralazine Diuretic if necessary Aldosterone antagonists Antiandrogenic effect in first trimester 2011 MFMER


23 Cardiac Drugs in Pregnancy ACE Inhibitors contraindicated in pregnancy 30% fetal morbidity with administration after week 14 Fetal renal tubular dysplasia, neonatal renal failure Oligohydramnios, cranial ossification, IUGR Cooper et al: N Engl J Med st trimester ACE risk of congenital malformations CV and CNS malformations AT II blocker contraindicated Safe during lactation
24


25 20-Year-Old Female Pre-pregnancy counseling FH of Marfan, dissection, ectopia lentis Asymptomatic Ao root 41 mm 2011 MFMER
26 What would you recommend? Avoid pregnancy 2011 MFMER

 Oxytocin implicated in dissection 2011")
27 Pregnancy in Marfan Preexisting medial changes Changes with pregnancy Physiologic, hormonal Unpredictable maternal risk Dissection, rupture, IE, CHF Fetal - 50% inheritance (AD) Oxytocin implicated in dissection 2011 MFMER

28 Preconceptual Counseling In addition to routine obstetric screening Detailed CV history, FH, medications and exam Echo aorta and valves Aortic imaging Aorta >45 mm no pregnancy Aorta 40 mm reasonable if low risk Aorta mm individualize Genetics, prenatal diagnosis ESC GUCH Guidelines 2010
29 Pregnancy in Aortic Disorders Recommendations During pregnancy Beta-blocker, regular ao imaging (individualize) Fetal echo Peripartum Facilitated vaginal delivery C-section for ao >40 mm or size IE prophylaxis Postpartum FU - dissection risk persists Future eval of lactation risk Management similar with other aortic disorders 2011 MFMER
30

31 29-Year-Old Female 29 weeks pregnant Presents to ED with palpitations and lightheadedness No past CV history BP 100/50, HR 160 Alert No murmurs Lungs clear 2011 MFMER
32 2011 MFMER

33 What would you recommend? iv adenosine 2011 MFMER

34 SVT in Pregnancy Hemodynamic compromise DC cardioversion fetal HR/mortality Acute symptoms Adenosine - bradycardia 2011 MFMER

35 Recurrent SVT in Pregnancy Beta blocker Calcium channel blocker Sotalol Flecainide Amiodarone - CI by manufacturer Monitor neonatal ECG and thyroid Excreted in breast milk Ablation 2011 MFMER
36


37 30-Year-Old Female 33 weeks pregnant, dyspnea Mean gradient = 15 mmhg What would you do next? 2011 MFMER

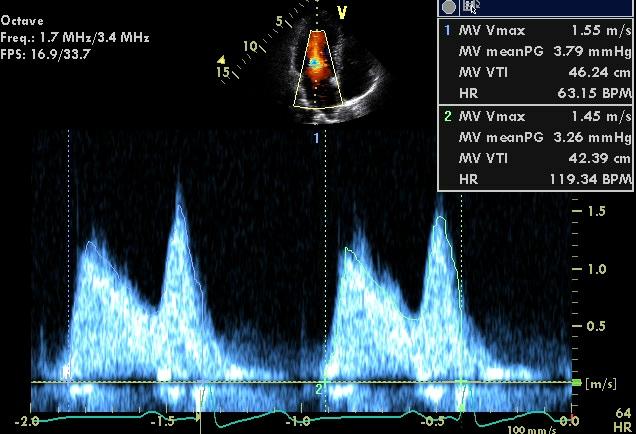

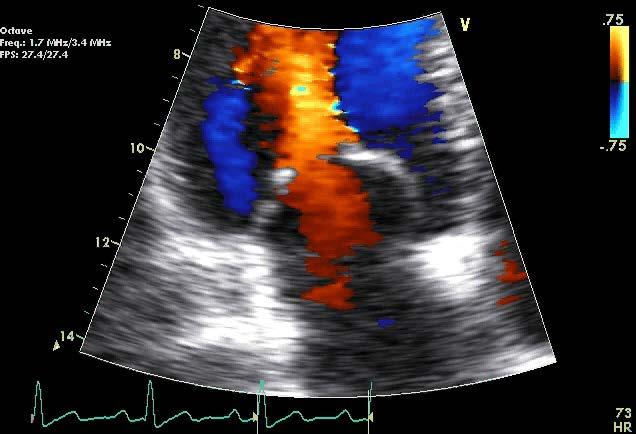
38 30-Year-Old Female Beta-blocker MG = 4 mmhg at HR MFMER


39 Mitral Stenosis in Pregnancy HR diastolic filling SV Reflex HR Further in LA pressure AF Pulmonary Edema 2011 MFMER
40 Mitral Stenosis Management in Pregnancy β blockade, maintain NSR Anticoagulation, diuretics Balloon valvotomy Surgical valvotomy or MVR 2011 MFMER

41


42 VHD in Pregnancy Tissue Prosthesis degeneration in young Reoperation risk Possible accelerated degeneration in pregnancy 2011 MFMER



43 Anticoagulation in Pregnancy Mechanical Prosthesis AC options suboptimal thrombosis risk clotting factor, plt adhesion fibrinolysis, prot S activity High mortality Limited options
44 ESC VHD Guidelines European Heart Journal 2012 Warfarin favored AC therapy during 2 nd and 3rd trimesters until the 36th wk Warfarin is favored during the first trimester if dose is <5 mg/24 hr, after patient approval Close AC monitoring advised when UFH used



45 Pregnancy and the Heart CVD 1-2% of pregnancies CHD most common SHD Doesn t preclude pregnancy risk to mother and fetus Individual assessment Preferably prior to conception 2011 MFMER

46 Questions or Comments?
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Pregnancy in Marfan Syndrome and Bicuspid Aortic Valve Related Aortopathy
 Pregnancy in Marfan Syndrome and Bicuspid Aortic Valve Related Aortopathy Heidi M. Connolly, MD Cardiac Problems in Pregnancy Venice Italy, February 2014 No Disclosures 2012 MFMER slide-1 Regitz-Zagrosek
Pregnancy in Marfan Syndrome and Bicuspid Aortic Valve Related Aortopathy Heidi M. Connolly, MD Cardiac Problems in Pregnancy Venice Italy, February 2014 No Disclosures 2012 MFMER slide-1 Regitz-Zagrosek
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Congenital Heart Disease Patient and Pregnancy
 Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Peripartum kardiomyopati
 Fall 3 Peripartum kardiomyopati Roman A roch 2017 01 26 2 3 Dg. PPCM Symptoms ECG, pro-bnp echocardiography 4 Peripartum cardiomyopathy: a systematic literature review Acta Obstetricia et Gynecologica
Fall 3 Peripartum kardiomyopati Roman A roch 2017 01 26 2 3 Dg. PPCM Symptoms ECG, pro-bnp echocardiography 4 Peripartum cardiomyopathy: a systematic literature review Acta Obstetricia et Gynecologica
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy
 ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Pregnancy and Heart Disease. Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital
 Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Cardiovascular Disease
 Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Heidi M. Connolly, M.D. Professor of Medicine Chair for Education Division
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Heidi M. Connolly, M.D. Professor of Medicine Chair for Education Division
SESSION D5. The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Susan P. D Anna MSN, APRN BC February 14, 2019
 Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
Cardiac disease in pre pr gnancy
 IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
Heart Failure treatment during pregnancy
 Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Maternal Cardiac Disease Diagnosis and Management
 Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
What to do when a heart failure patient becomes pregnant
 BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
PREGNANCY IN PATIENTS WITH A SYSTEMIC RV
 PREGNANCY IN PATIENTS WITH A SYSTEMIC RV Carole A. Warnes MD, FRCP Professor of Medicine, Mayo Clinic No disclosures 2013 MFMER slide-1 PREGNANCY : SYSTEMIC RV D - transposition after atrial switch procedure
PREGNANCY IN PATIENTS WITH A SYSTEMIC RV Carole A. Warnes MD, FRCP Professor of Medicine, Mayo Clinic No disclosures 2013 MFMER slide-1 PREGNANCY : SYSTEMIC RV D - transposition after atrial switch procedure
Catherine Nelson-Piercy. Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK
 Cardiac Disease and Pregnancy Catherine Nelson-Piercy Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK Physiological changes in pregnancy Cardiac Output (CO) increases by 40% Further
Cardiac Disease and Pregnancy Catherine Nelson-Piercy Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK Physiological changes in pregnancy Cardiac Output (CO) increases by 40% Further
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
Cardiac Disease in Pregnancy
 Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
How to manage the pregnant woman with heart disease
 How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Peripartum cardiomyopathy: Challenges and perspectives
 Prof. Petar M. Seferović, MD, PhD, FESC, FESC Board member, Heart Failure Association of the ESC Peripartum cardiomyopathy: Challenges and perspectives Director, Department of Cardiology, Clinical Center
Prof. Petar M. Seferović, MD, PhD, FESC, FESC Board member, Heart Failure Association of the ESC Peripartum cardiomyopathy: Challenges and perspectives Director, Department of Cardiology, Clinical Center
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων
 Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Peripartum cardiomyopathy: review and practice guidelines. Hanan ALBackr Associate Professor King Saud university, King Fahad Cardaic center -Riyadh
 Peripartum cardiomyopathy: review and practice guidelines Hanan ALBackr Associate Professor King Saud university, King Fahad Cardaic center -Riyadh Outlines Definition of PPCM Dignostic Critaria for peripartum
Peripartum cardiomyopathy: review and practice guidelines Hanan ALBackr Associate Professor King Saud university, King Fahad Cardaic center -Riyadh Outlines Definition of PPCM Dignostic Critaria for peripartum
3 European Journal of Heart Failure 2016; 18,
 Impella Assisted Cesarean Delivery in a 27 6/7 Weeks Gestation 30 Year Old Female with Newly Diagnosed Cardiomyopathy & Multifocal Incessant Ventricular Tachycardia Brendan J Carry, MD, Jason Costa, MD,
Impella Assisted Cesarean Delivery in a 27 6/7 Weeks Gestation 30 Year Old Female with Newly Diagnosed Cardiomyopathy & Multifocal Incessant Ventricular Tachycardia Brendan J Carry, MD, Jason Costa, MD,
How pregnancy impacts adult cyanotic congenital heart disease
 How pregnancy impacts adult cyanotic congenital heart disease Magalie Ladouceur Adult Congenital Heart Disease Unit, Hôpital Européen Georges Pompidou, Centre de reference des Malformations Cardiaques
How pregnancy impacts adult cyanotic congenital heart disease Magalie Ladouceur Adult Congenital Heart Disease Unit, Hôpital Européen Georges Pompidou, Centre de reference des Malformations Cardiaques
Outline. Maternal Congenital Heart Disease in Pregnancy. Maternal congenital heart disease. Cardiovascular disease in pregnancy 10/18/2017
 I have no disclosures or conflicts of interest to report. Maternal Congenital Heart Disease in Pregnancy Jennifer A. Jolley, MD Associate Clinical Professor University of California, Irvine Department
I have no disclosures or conflicts of interest to report. Maternal Congenital Heart Disease in Pregnancy Jennifer A. Jolley, MD Associate Clinical Professor University of California, Irvine Department
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Images in Cardiovascular Medicine
 Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Heart disease complicating pregnancy management strategies
 www.slcog.lk/sljog LEADING ARTICLE Heart disease complicating pregnancy management strategies Priyadharshan P¹ Introduction Heart disease is the third most common cause of maternal death and the leading
www.slcog.lk/sljog LEADING ARTICLE Heart disease complicating pregnancy management strategies Priyadharshan P¹ Introduction Heart disease is the third most common cause of maternal death and the leading
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease. Pregnancy and Cardiovascular Disease MCQ
 Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη
 The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY
 CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Familial Aggregation of Dilated Cardiomyopathy in Patients with Peripartum Cardiomyopathy
 Familial Aggregation of Dilated Cardiomyopathy in Patients with Peripartum Cardiomyopathy Tibazarwa K 1, Sliwa K 1, Wonkam A 2, Mayosi BM 1 1 Hatter Cardiovascular Research Institute, Department of Medicine,
Familial Aggregation of Dilated Cardiomyopathy in Patients with Peripartum Cardiomyopathy Tibazarwa K 1, Sliwa K 1, Wonkam A 2, Mayosi BM 1 1 Hatter Cardiovascular Research Institute, Department of Medicine,
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Acute Pulmonary edema Secondary to CARDIAC FAILURE NON COMPACTED LEFT VENTRICLE in Pregnancy
 Acute Pulmonary edema Secondary to CARDIAC FAILURE NON COMPACTED LEFT VENTRICLE in Pregnancy Dr Anisha Gala, Consultant Obstetrician Dr. Tarakeswari S HOD, Dept of Obstetric Medicine, Fernandez Hospitals
Acute Pulmonary edema Secondary to CARDIAC FAILURE NON COMPACTED LEFT VENTRICLE in Pregnancy Dr Anisha Gala, Consultant Obstetrician Dr. Tarakeswari S HOD, Dept of Obstetric Medicine, Fernandez Hospitals
Innovation therapy in Heart Failure
 Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Steel vs Alcohol. Or Neither. Management of Hypertrophic Cardiomyopathy. Josh Doll, MD January 24, 2015
 Steel vs Alcohol Or Neither Management of Hypertrophic Cardiomyopathy Josh Doll, MD January 24, 2015 47yo Male, Mr. L Severe progressive dyspnea on exertion and weight gain Previous avid Cross-Fit participant
Steel vs Alcohol Or Neither Management of Hypertrophic Cardiomyopathy Josh Doll, MD January 24, 2015 47yo Male, Mr. L Severe progressive dyspnea on exertion and weight gain Previous avid Cross-Fit participant
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pregnancy and cyanotic congenital heart disease. A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain
 Hospital Vall d Hebron Barcelona, Spain") Pregnancy and cyanotic congenital heart disease A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain I have nothing to disclose. Pregnancy and cyanotic congenital
Pregnancy and cyanotic congenital heart disease A. Pijuan Domènech (U. de C. Congènites de l Adult) Hospital Vall d Hebron Barcelona, Spain I have nothing to disclose. Pregnancy and cyanotic congenital
Hemodynamic Changes in Obstetric Anesthesia. Sonia Vaida PANA, Hershey, April 2009
 Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Risk of Subsequent Pregnancy in Women with a History of Peripartum Cardiomyopathy Uri Elkayam, MD
 Risk of Subsequent Pregnancy in Women with a History of Peripartum Cardiomyopathy Uri Elkayam, MD Professor of Medicine / Cardiology Professor of Obstetrics and Gynecology University of Southern California
Risk of Subsequent Pregnancy in Women with a History of Peripartum Cardiomyopathy Uri Elkayam, MD Professor of Medicine / Cardiology Professor of Obstetrics and Gynecology University of Southern California
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Peripartum Anesthetic Management in Patients with Left Ventricular Hypertrabeculation
 Peripartum Anesthetic Management in Patients with Left Ventricular Hypertrabeculation Marissa L. Kauss, M.D. Fellow, Cardiovascular Anesthesia Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Peripartum Anesthetic Management in Patients with Left Ventricular Hypertrabeculation Marissa L. Kauss, M.D. Fellow, Cardiovascular Anesthesia Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Atrial Fibrillation. Epidemiology. Goals 11/12/2012. Faithful marker for age and underlying cardiopulmonary disease
 Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
Cardiomyopathies lessons learnt
 Maternal Deaths from Cardiomyopathies lessons learnt Dr Sarah Vause St Mary s Hospital, Manchester Mrs Thomas Jefferson Mumtaz Mahal Charlotte Bronte Mrs Beeton Cardiomyopathy Dilated - acquired
Maternal Deaths from Cardiomyopathies lessons learnt Dr Sarah Vause St Mary s Hospital, Manchester Mrs Thomas Jefferson Mumtaz Mahal Charlotte Bronte Mrs Beeton Cardiomyopathy Dilated - acquired
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong
 Pol.Col.Dr.Kasem Ratanasumawong") Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Medical Complications of Pregnancy
 Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
PERIPARTUM CARDIOMYOPATHY
 PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM
 MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
What s New in the AF Guidelines
 Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Peripartum Cardiomyopathy
 Peripartum Cardiomyopathy Denise Hilfiker-Kleiner Kardiologie & Angiologie MHH, Hannover Nothing to disclose Peri- or Postpartum Cardiomyopathy Peri- or postpartum cardiomyopathy (PPCM) is a disorder of
Peripartum Cardiomyopathy Denise Hilfiker-Kleiner Kardiologie & Angiologie MHH, Hannover Nothing to disclose Peri- or Postpartum Cardiomyopathy Peri- or postpartum cardiomyopathy (PPCM) is a disorder of
Cardiovascular disease complicates 1% to 3% of all
 Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Heart failure in pregnancy
 Heart failure in pregnancy PD Dr. med Daniel Tobler Leiter angeborene Herzfehler (GUCH) Universitätsspital Basel! www.heartdiseaseandpregnancy.com Heart failure in pregnancy Agenda! - general considerations
Heart failure in pregnancy PD Dr. med Daniel Tobler Leiter angeborene Herzfehler (GUCH) Universitätsspital Basel! www.heartdiseaseandpregnancy.com Heart failure in pregnancy Agenda! - general considerations
Is it HF secondary to rheumatic heart disease???
 Is it HF secondary to rheumatic heart disease??? Is mitral regurg. Is complication of CHF??? Cardiomyopathy Definition The term cardiomyopathy is purely descriptive, meaning disease of the heart muscle
Is it HF secondary to rheumatic heart disease??? Is mitral regurg. Is complication of CHF??? Cardiomyopathy Definition The term cardiomyopathy is purely descriptive, meaning disease of the heart muscle
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη
 Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Amiodarone Prescribing and Monitoring: Back to the Future
 Amiodarone Prescribing and Monitoring: Back to the Future Subha L. Varahan, MD, FHRS, CCDS Electrophysiologist Oklahoma Heart Hospital Oklahoma City, OK Friday, February, 8 th, 2019 Iodinated benzofuran
Amiodarone Prescribing and Monitoring: Back to the Future Subha L. Varahan, MD, FHRS, CCDS Electrophysiologist Oklahoma Heart Hospital Oklahoma City, OK Friday, February, 8 th, 2019 Iodinated benzofuran
Objectives. Medical Complications of Pregnancy. Potential Conflicts: None. Common Complicating Medical Conditions that Precede Pregnancy
 Medical Complications of Potential Conflicts: None Ellen W. Seely, M.D. Director of Clinical Research Endocrine-Hypertension Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Medical Complications of Potential Conflicts: None Ellen W. Seely, M.D. Director of Clinical Research Endocrine-Hypertension Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Imaging Cardiovascular Disease in Pregnancy
 Imaging Cardiovascular Disease in Pregnancy Karen Ordovas MD, MAS Associate Professor of Radiology and Medicine Director of Cardiac Imaging University of California San Francisco Cardiac MRI during pregnancy
Imaging Cardiovascular Disease in Pregnancy Karen Ordovas MD, MAS Associate Professor of Radiology and Medicine Director of Cardiac Imaging University of California San Francisco Cardiac MRI during pregnancy
Cardiomyopathy. Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement
 Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Peripartum management of Rheumatic Heart Disease
 Peripartum management of Rheumatic Heart Disease Dr James Sartain Director of Anaesthesia & Perioperative Medicine Cairns & Hinterland Hospital & Health Service Talk outline Why (still) talk about RHD
Peripartum management of Rheumatic Heart Disease Dr James Sartain Director of Anaesthesia & Perioperative Medicine Cairns & Hinterland Hospital & Health Service Talk outline Why (still) talk about RHD
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Pregnancy in Non-Peripartum Cardiomyopathy
 Pregnancy in Non-Peripartum Cardiomyopathy Avraham Shotan, Lubov Vasilenco, Michael Shochat, Mark Kazatsker, David Blondheim, Yaniv Levi, Simcha Meisel, Alicia Vazan Heart Institute, Hillel Yaffe Medical
Pregnancy in Non-Peripartum Cardiomyopathy Avraham Shotan, Lubov Vasilenco, Michael Shochat, Mark Kazatsker, David Blondheim, Yaniv Levi, Simcha Meisel, Alicia Vazan Heart Institute, Hillel Yaffe Medical
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
CKD Satellite Symposium
 CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
Takotsubo cardiomyopathy. Joseph L. Blackshear, MD Professor of Medicine Mayo Clinic College of Medicine Mayo Clinic Florida
 Takotsubo cardiomyopathy Joseph L. Blackshear, MD Professor of Medicine Mayo Clinic College of Medicine Mayo Clinic Florida 79 year old woman, pre chemo echo for esophageal cancer Post chemo, dehydration,
Takotsubo cardiomyopathy Joseph L. Blackshear, MD Professor of Medicine Mayo Clinic College of Medicine Mayo Clinic Florida 79 year old woman, pre chemo echo for esophageal cancer Post chemo, dehydration,
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,