Valve Disease in the Pregnant Patient
|
|
|
- Avice Flynn
- 6 years ago
- Views:
Transcription
1 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com
2 If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If delivered, do not allow breastfeeding.
3 Objectives Understand the normal cardiovascular changes that occur during pregnancy Understand major principles of treatment of valve disease during pregnancy
4 Maternal Cardiac Disease Complicates 1-4 % of pregnancies in US Major cause of nonobstetric maternal morbidity and mortality ~ 16% of maternal deaths Management more complicated than cardiac disease in nonpregnant women Much of data is not recent and is observational
5 Hemodynamic changes in pregnancy Normal changes in Intravascular volumes Cardiac output SVR BP Begin early in pregnancy (weeks 5-8) Impact cardiovascular exam and tests
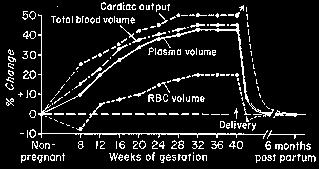
6 Intravascular volumes
7 Labor & Delivery Anxiety, pain, exertion, contractions, bleeding, anesthesia With uterine contraction Displacement of blood into circulation BP Mimic of Valsalva Cardiac output 15-50% in labor 80% post partum
8 Echo Indications Valvular/congenital disease Grade 3 systolic murmur Diastolic murmur Significant dyspnea or CHF signs
9 Predictors of risk Prior cardiac events heart failure, TIA, CVA NYHA functional class >II or cyanosis Valvular or outflow tract obstruction Myocardial dysfunction From Siu SC, Sermer M, et al.circulation. 2001;104:
10 Valvular Heart Disease
11 General Principles Ideally seen prior to pregnancy or early as possible Counseling, including maternal and fetal risks Baseline echo and functional status Adjust medications to optimize fetal risk
12 General Principles High risk lesions correction prior to pregnancy High risk lesion early in pregnancy discuss termination Evaluate once a trimester and for any change in symptoms VanderbiltHeart.com
13 General Principles Cardiac surgery Refractory Class III or IV symptoms Maternal risks nonpregnant patients High risk of fetal distress, IUGR, and fetal demise (19-29%) L & D scheduled and induced when possible with close monitoring
14 Case - 22 year old female Desires to get pregnant. Mild LE edema. PMH: Rheumatic heart disease with severe MR s/p repair 2004 All: NKDA Meds: Multivitamin FH: No cardiac disease Soc: No tobacco, alcohol or illicit drugs PE: 125/ % Normal JVP CTAB Regular, S1, S2, III/VI systolic murmur at LLSB to apex Soft, NT Trace 1+ edema

15 22 year old female

16 22 year old female VanderbiltHeart.com

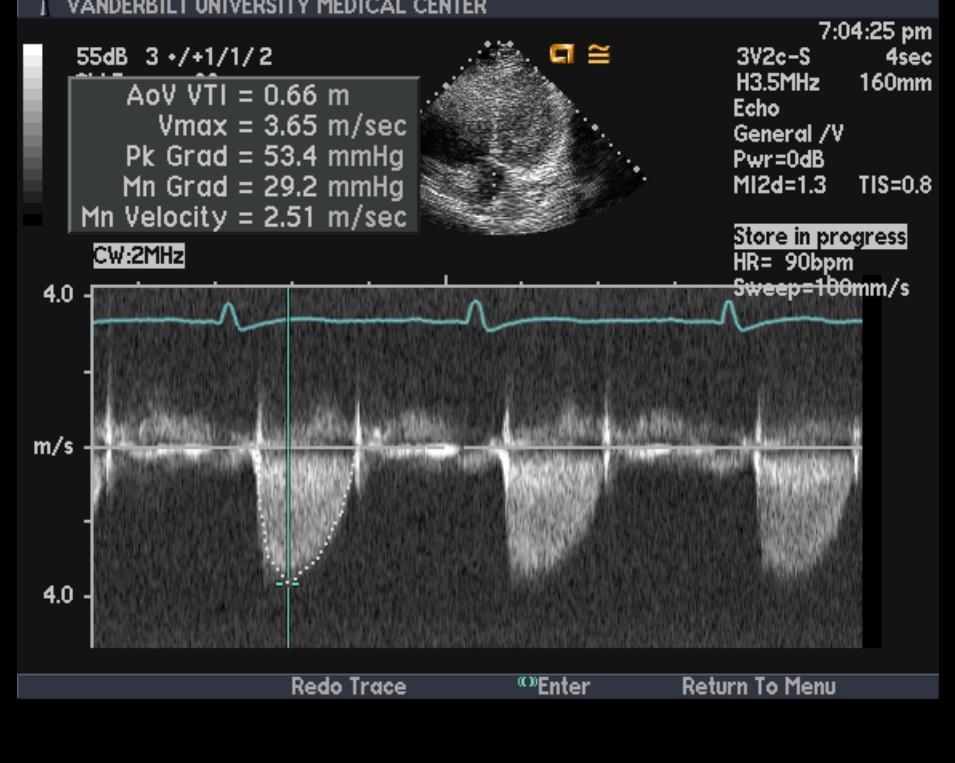
17 22 year old female
18 Mitral Stenosis (Deteriorate in 3 rd trimester and labor) volume LA filling pressures, dyspnea exercise tolerance HR transmitral gradient diastolic filling time CO of 46% with contractions Ramsey, et al. Amer J Perinat 2001;18(5):

19 Severe MS 67% pulmonary edema or arrhythmia Maternal mortality 5% with Class III-IV Fetal mortality 30% with Class IV Heart failure prematurity and IUGR Atrial fibrillation risk of hemodynamic deterioration Anticoagulation VanderbiltHeart.com
20 Mitral Stenosis Medical management Prevention of tachycardia Maintenance of LV preload Diuretics cautiously if needed PA catheters for symptomatic patients Epidural anesthesia better tolerated than general anesthesia
21 Mitral Stenosis Severe MS correct prior to pregnancy Percutaneous balloon valvuloplasty Bridge patient through pregnancy Failed medical management during pregnancy Timing weeks gestation Success rate 95% Symptomatic improvement = surgical correction Fetal complications 5% vs 38% with surgery De Souza, JA, Martinez, et al. J Am Coll Cardiol 2001; 37:900
22 22 year old female Not candidate for valvuloplasty Advised to delay pregnancy Seen by cardiac surgery recommendation for bioprosthetic valve Choose to proceed with pregnancy and delivered without complications


23 Case - 26 year old female Asymptomatic, desires to get pregnant. PMH: Bicuspid AV, HTN, G5P2123 All: NKDA Meds: Multivitamin FH: No cardiac disease Soc: Smokes, no alcohol or illicit drugs PE: 142/ % Normal JVP CTAB Regular, S1, S2, III/VI systolic murmur at USB radiating to neck Soft, NT No edema

24 26 year old female

25 26 year old female
26 Aortic Stenosis Bicuspid valve most common Severe AS Decompensates late 2 nd /early 3 rd trimester Maternal mortality 17% Fetal mortality 32%
27 Aortic Stenosis Medical management Control tachycardia Avoid vasodilation Avoid volume depletion Reduction of physical activity Epidural anesthesia used cautiously due to vasodilatory effects VanderbiltHeart.com
28 Aortic Stenosis Severe AS corrected prior to pregnancy Percutaneous balloon valvuloplasty Prior to pregnancy to delay repair Refractory to medical management Consider with peak gradient > 50mmHg (cath) Bicuspid AV and root dilatation May predispose to aortic dissection Considered a high risk lesion in combination

29 Regurgitant Lesions Chronic mild to moderate MR and AI well tolerated Severe MR or AI corrected prior to pregnancy Close hemodynamic monitoring Diuretics Vasodilator therapy Epidural anesthesia VanderbiltHeart.com
30 Right Sided Valves Pulmonary stenosis well tolerated Balloon valvuloplasty for refractory right sided failure Isolated TR well tolerated
31 Prosthetic Valves


32 Prosthetic Valves DiSaia P. Obstet Gynecol Review 1966;28:
33 Prosthetic Valves Cardiologist involved as early as possible Valve choice Anticoagulation? higher complications with mechanical Pregnancy loss Preterm delivery Maternal cardiac complications? increased degeneration of bioprosthetic valves Sbarouni E, et al. Br Heart J 1994;71:
34 Warfarin > maternal protection (5.7% death or embolic) Crosses placenta fetal death and premature birth Fetal bleeding and cerebral hemorrhage can occur Warfarin embryopathy Nasal hypoplasia, depressed nasal bridge, IUGR, eye defects, punctate epiphyseal dysplasia 1 st trimester exposure CNS abnormalities after any trimester exposure Incidence 5-67% Risk lower with <5mg daily
35 Unfractionated Heparin Safer for the fetus Does not cross the placenta No fetal bleeding or teratogenicity Can cause uteroplacental junction bleeding Risk of maternal thrombocytopenia and osteopenia Thromboembolic complications (12 24%) Target PTT of at least twice the control
36 Low Molecular Weight Heparin Does not cross the placenta Advantages Ease of administration Less thrombocytopenia and osteoporosis More predictable dose response Potential for less monitoring Lower risk of bleeding complications Monitor plasma anti-xa levels 4-6h after morning dose Target level is units/ml
37 Mechanical Aortic Valve Replacement in Young Women Planning on Pregnancy J Am Coll Cardiol. 2012;59(12): doi: /j.jacc VanderbiltHeart.com

38 Recommendations based on risk (differ in US and Europe) High Risk Old generation MV, AF, prior TE? Higher target levels? Add ASA Low Risk New generation MV, AV Elkayam, et al, JACC 2012 Mar 20;59(12): VanderbiltHeart.com
39 Reasonable Strategies 1. LMWH or UFH weeks 6-12 and close to term (week 35-36), with warfarin at other times OR 2. Aggressively dose adjusted UFH throughout OR 3. Aggressively dose adjusted LMWH throughout Decision with patient, OB, and cardiologist
40 Conclusions Hemodynamic changes associated with pregnancy Left sided obstructive lesions, poor functional class, LV dysfunction not well tolerated Prosthetic valve choice/anticoagulation controversial Counseling ideally done prior to pregnancy including maternal and fetal risks Cardiologists involved as early as possible in the care of these patients
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
Congenital Heart Disease Patient and Pregnancy
 Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Images in Cardiovascular Medicine
 Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Pregnancy and Cardiovascular Disease
 Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
Pregnancy and Heart Disease
 Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
Outline. Maternal Congenital Heart Disease in Pregnancy. Maternal congenital heart disease. Cardiovascular disease in pregnancy 10/18/2017
 I have no disclosures or conflicts of interest to report. Maternal Congenital Heart Disease in Pregnancy Jennifer A. Jolley, MD Associate Clinical Professor University of California, Irvine Department
I have no disclosures or conflicts of interest to report. Maternal Congenital Heart Disease in Pregnancy Jennifer A. Jolley, MD Associate Clinical Professor University of California, Irvine Department
Cardiac Disease in Pregnancy
 Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
SESSION D5. The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC
 A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy *C.V. was born the 24th May 1980 Rheumatic fever during
A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy *C.V. was born the 24th May 1980 Rheumatic fever during
Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
 ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
Pregnancy and Heart Disease. Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital
 Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Maternal Cardiac Disease Diagnosis and Management
 Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
Cardiac disease in pre pr gnancy
 IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
Valvular Heart Disease in Pregnancy
 CHAPTER 87 Valvular Heart Disease in Pregnancy M. Panja, S. Basu, D. Kumar Introduction Valvular heart disease in young women is most commonly due to rheumatic heart disease, congenital abnormalities,
CHAPTER 87 Valvular Heart Disease in Pregnancy M. Panja, S. Basu, D. Kumar Introduction Valvular heart disease in young women is most commonly due to rheumatic heart disease, congenital abnormalities,
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Cardiovascular disease complicates 1% to 3% of all
 Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy
 ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη
 Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
 Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Peripartum management of Rheumatic Heart Disease
 Peripartum management of Rheumatic Heart Disease Dr James Sartain Director of Anaesthesia & Perioperative Medicine Cairns & Hinterland Hospital & Health Service Talk outline Why (still) talk about RHD
Peripartum management of Rheumatic Heart Disease Dr James Sartain Director of Anaesthesia & Perioperative Medicine Cairns & Hinterland Hospital & Health Service Talk outline Why (still) talk about RHD
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων
 Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Heidi M. Connolly, M.D. Professor of Medicine Chair for Education Division
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Heidi M. Connolly, M.D. Professor of Medicine Chair for Education Division
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Cardiology. the Sounds: #7 HCM. LV Outflow Obstruction: Aortic Stenosis. (Coming Soon - HCM)
") A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC
 Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC Ebru Ertekin MD, Iris M. Van Hagen MD, Amar M. Salam MD, Titia P.E. Ruys MD PhD, Jolien W. Roos-Hesselink MD
Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC Ebru Ertekin MD, Iris M. Van Hagen MD, Amar M. Salam MD, Titia P.E. Ruys MD PhD, Jolien W. Roos-Hesselink MD
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
What to do when a heart failure patient becomes pregnant
 BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
Case Report A Multidisciplinary Approach to Anesthetic Management of a Parturient with Severe Aortic Stenosis
 Case Reports in Anesthesiology Volume 2015, Article ID 489157, 4 pages http://dx.doi.org/10.1155/2015/489157 Case Report A Multidisciplinary Approach to Anesthetic Management of a Parturient with Severe
Case Reports in Anesthesiology Volume 2015, Article ID 489157, 4 pages http://dx.doi.org/10.1155/2015/489157 Case Report A Multidisciplinary Approach to Anesthetic Management of a Parturient with Severe
Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy
 Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy W. Sia, E. Toor, N. Wahab, J. Windram, R. Khurana Cardiac Problems in Pregnancy Congress
Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy W. Sia, E. Toor, N. Wahab, J. Windram, R. Khurana Cardiac Problems in Pregnancy Congress
3 European Journal of Heart Failure 2016; 18,
 Impella Assisted Cesarean Delivery in a 27 6/7 Weeks Gestation 30 Year Old Female with Newly Diagnosed Cardiomyopathy & Multifocal Incessant Ventricular Tachycardia Brendan J Carry, MD, Jason Costa, MD,
Impella Assisted Cesarean Delivery in a 27 6/7 Weeks Gestation 30 Year Old Female with Newly Diagnosed Cardiomyopathy & Multifocal Incessant Ventricular Tachycardia Brendan J Carry, MD, Jason Costa, MD,
PERIPARTUM CARDIOMYOPATHY
 PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
Adult Congenital Heart Disease: A Growing Problem. Dr. Gary Webb Cincinnati Children s Hospital Heart Institute
 Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Rate of CHD at birth: 4~12/1,000
 Risk assessment and management for the pregnant ACHD woman Suk-Joo Choi Department of Obstetrics and Gynecology Samsung Medical Center Sungkyunkwan k University i School of Medicine i Cardiac diseases
Risk assessment and management for the pregnant ACHD woman Suk-Joo Choi Department of Obstetrics and Gynecology Samsung Medical Center Sungkyunkwan k University i School of Medicine i Cardiac diseases
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Effect of maternal heart disease on pregnancy outcomes
 Expert Review of Obstetrics & Gynecology ISSN: 1747-4108 (Print) 1747-4116 (Online) Journal homepage: http://www.tandfonline.com/loi/ierb20 Effect of maternal heart disease on pregnancy outcomes Emily
Expert Review of Obstetrics & Gynecology ISSN: 1747-4108 (Print) 1747-4116 (Online) Journal homepage: http://www.tandfonline.com/loi/ierb20 Effect of maternal heart disease on pregnancy outcomes Emily
Rheumatic heart disease in pregnancy
 Review Articles Normal cardiovascular changes during pregnancy Hemodynamic changes in pregnancy are profound and begin in the first trimester, the plasma volume increases and approaches to 50% above normal,
Review Articles Normal cardiovascular changes during pregnancy Hemodynamic changes in pregnancy are profound and begin in the first trimester, the plasma volume increases and approaches to 50% above normal,
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Non-cardiac Surgery in Valvular Heart Disease
 Jafar Golshahi, MD; Shahnaz Aram, MD Abstract Background- Valvular heart disease is one of the common complications of acute rheumatic fever, which manifests its clinical complications one or two decades
Jafar Golshahi, MD; Shahnaz Aram, MD Abstract Background- Valvular heart disease is one of the common complications of acute rheumatic fever, which manifests its clinical complications one or two decades
Catherine Nelson-Piercy. Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK
 Cardiac Disease and Pregnancy Catherine Nelson-Piercy Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK Physiological changes in pregnancy Cardiac Output (CO) increases by 40% Further
Cardiac Disease and Pregnancy Catherine Nelson-Piercy Guy s & St Thomas Hospitals & Queen Charlotte s Hospital London, UK Physiological changes in pregnancy Cardiac Output (CO) increases by 40% Further
Hemodynamic Changes in Obstetric Anesthesia. Sonia Vaida PANA, Hershey, April 2009
 Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Hemodynamic Changes in Obstetric Anesthesia Sonia Vaida PANA, Hershey, April 2009 Pregnancy is a normal healthy condition and is simultaneously the most common altered physiologic state to which human
Medical Complications of Pregnancy
 Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Heart Failure treatment during pregnancy
 Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS
 ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη
 The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
The V Wave. January, 2007 Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH. Ref: Kern MJ. Hemodynamic Rounds, 2 nd ed
 The V Wave January, 2007 Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH Ref: Kern MJ. Hemodynamic Rounds, 2 nd ed. 1999. Normal Hemodynamic Values Cardiac index 2.8-4.2 (mean 3.4 L/min/m 2 ) Stroke volume 30-65
The V Wave January, 2007 Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH Ref: Kern MJ. Hemodynamic Rounds, 2 nd ed. 1999. Normal Hemodynamic Values Cardiac index 2.8-4.2 (mean 3.4 L/min/m 2 ) Stroke volume 30-65
The Effect of Valvular Heart Diseases on Maternal and Fetal Outcome of Pregnancy Nada Salih Ameen*,Nawfal Fawzi Anwer**
 THE VALVULAR IRAQI POSTGRADUATE HEART DISEASES MEDICAL AND JOURNAL PREGNANCY The Effect of Valvular Heart Diseases on Maternal and Fetal Outcome of Pregnancy Nada Salih Ameen*,Nawfal Fawzi Anwer** ABSTRACT:
THE VALVULAR IRAQI POSTGRADUATE HEART DISEASES MEDICAL AND JOURNAL PREGNANCY The Effect of Valvular Heart Diseases on Maternal and Fetal Outcome of Pregnancy Nada Salih Ameen*,Nawfal Fawzi Anwer** ABSTRACT:
Susan P. D Anna MSN, APRN BC February 14, 2019
 Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Dr.ssa Loredana Iannetta. Centro Cardiologico Monzino
 Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong
 Pol.Col.Dr.Kasem Ratanasumawong") Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
HEART DISEASE IN PREGNANCY
 HEART DISEASE IN PREGNANCY DR. JOSHI SUYAJNA D. www.suyajna.com VIMS-BELLARY Pre-conceptional counseling a. Objective Risk assessment with» 1. Clarke s table 2. NYHA b. Feasibility of pregnancy care c.
HEART DISEASE IN PREGNANCY DR. JOSHI SUYAJNA D. www.suyajna.com VIMS-BELLARY Pre-conceptional counseling a. Objective Risk assessment with» 1. Clarke s table 2. NYHA b. Feasibility of pregnancy care c.
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
How to Assess Diastolic Dysfunction?
 How to Assess Diastolic Dysfunction? Fausto J Pinto, MD, PhD, FESC, FACC, FASE Lisbon University Dyastolic Dysfunction Impaired relaxation Elevated filling pressures Ischemic heart disease Cardiomyopathies
How to Assess Diastolic Dysfunction? Fausto J Pinto, MD, PhD, FESC, FACC, FASE Lisbon University Dyastolic Dysfunction Impaired relaxation Elevated filling pressures Ischemic heart disease Cardiomyopathies
ThROmbolytIc TherApy of Prosthetic Heart Valve Thrombosis in PREGnancy with Low Dose Slow Infusion of t-pa (TROIA-PREG)
") ThROmbolytIc TherApy of Prosthetic Heart Valve Thrombosis in PREGnancy with Low Dose Slow Infusion of t-pa (TROIA-PREG) Beytullah ÇAKAL, MD Koşuyolu Kartal Heart Training and Research Hospital, Istanbul,
ThROmbolytIc TherApy of Prosthetic Heart Valve Thrombosis in PREGnancy with Low Dose Slow Infusion of t-pa (TROIA-PREG) Beytullah ÇAKAL, MD Koşuyolu Kartal Heart Training and Research Hospital, Istanbul,
Watchman and Structural update..the next frontier. Ari Chanda, MD Cardiology Associates of Fredericksburg
 Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Aortic Stenosis.
 Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Heart failure in pregnancy
 Heart failure in pregnancy PD Dr. med Daniel Tobler Leiter angeborene Herzfehler (GUCH) Universitätsspital Basel! www.heartdiseaseandpregnancy.com Heart failure in pregnancy Agenda! - general considerations
Heart failure in pregnancy PD Dr. med Daniel Tobler Leiter angeborene Herzfehler (GUCH) Universitätsspital Basel! www.heartdiseaseandpregnancy.com Heart failure in pregnancy Agenda! - general considerations
USE OF BALLOON VALVOTOMY AS BRIDGE TO SURGERY FOR SEVERE HIGH RISK MITRAL STENOSIS
 USE OF BALLOON VALVOTOMY AS BRIDGE TO SURGERY FOR SEVERE HIGH RISK MITRAL STENOSIS Prof. Gerald Yonga MBChB, MMed, MBA, FRCP(Edin),FESC, FACC Aga Khan University Hospital Nairobi, Kenya. RHEUMATIC HEART
USE OF BALLOON VALVOTOMY AS BRIDGE TO SURGERY FOR SEVERE HIGH RISK MITRAL STENOSIS Prof. Gerald Yonga MBChB, MMed, MBA, FRCP(Edin),FESC, FACC Aga Khan University Hospital Nairobi, Kenya. RHEUMATIC HEART
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Aortic stenosis and regurgitation
 1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Cardiac Interventions in Pregnancy
 Cardiac Interventions in Pregnancy Introduction 0.2% 4% of all pregnancies are complicated by cardiovascular diseases: At present congenital heart disease in developed countries and rheumatic valvular
Cardiac Interventions in Pregnancy Introduction 0.2% 4% of all pregnancies are complicated by cardiovascular diseases: At present congenital heart disease in developed countries and rheumatic valvular
Pregnancy in Non-Peripartum Cardiomyopathy
 Pregnancy in Non-Peripartum Cardiomyopathy Avraham Shotan, Lubov Vasilenco, Michael Shochat, Mark Kazatsker, David Blondheim, Yaniv Levi, Simcha Meisel, Alicia Vazan Heart Institute, Hillel Yaffe Medical
Pregnancy in Non-Peripartum Cardiomyopathy Avraham Shotan, Lubov Vasilenco, Michael Shochat, Mark Kazatsker, David Blondheim, Yaniv Levi, Simcha Meisel, Alicia Vazan Heart Institute, Hillel Yaffe Medical
How to manage the pregnant woman with heart disease
 How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
How to manage the pregnant woman with heart disease Dr Fiona Walker, The Heart Hospital,UCLH, London Dr Sara Thorne, University Hospital Birmingham Dr Cathy Head, The Heart Hospital, UCLH, London Dr Kate
Središnja medicinska knjižnica
 Središnja medicinska knjižnica Vincelj, J., Sokol, I., Pevec, D., Sutlić, Ž. (2007) Infective endocarditis of aortic valve during pregnancy: A case report. International Journal of Cardiology, [Epub ahead
Središnja medicinska knjižnica Vincelj, J., Sokol, I., Pevec, D., Sutlić, Ž. (2007) Infective endocarditis of aortic valve during pregnancy: A case report. International Journal of Cardiology, [Epub ahead
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic