Pediatric CRRT The Basics
|
|
|
- Gervais Wilson
- 5 years ago
- Views:
Transcription
1 Pediatric CRRT The Basics Patrick Brophy Geoffrey Fleming Jordan Symons Michael Zappitelli 16 th International CRRT Conference San Diego 2011
2 Epidemiology Of and Indications For Pediatric CRRT
3 ACUTE KIDNEY INJURY WHAT IS IT? HOW COMMON? WHO DOES IT HAPPEN TO? WHO GETS IT? CRRT WHAT DO THEY GET? WHO SHOULD GET IT?
 Pediatric RIFLE (prifle) Crit Care.")
4 Pediatric AKI: Definition Past: So many definitions. Risk Injury Failure End-Stage Kidney Disease (RIFLE) Pediatric RIFLE (prifle) Crit Care. 2005; 9(5): Acute Kidney Injury Network definition
5 Pediatric AKI: Incidence in PICU Population & Definition-dependent Cardiac Surgery N = 395 N=395 AKI: 34% No AKI R I F 0 No AKI R I F AKI: 21% Kidney Int Oct;76(8): Anesth Analg 2009;109:45 52 (Aprotinin study)
6 Pediatric AKI: Incidence in PICU Population & Definition-dependent General PICU Most Critically ill children Vasopressors/Ventilated Urinary catheter All PICU Admx SCr baseline All PICU stay>48hrs prifle 82% AKI No AKI R I F Kid Int 2007; 71: SCr Doubling (prifle I) <Doub SCr >=Doub SCr (Rifle I) 70% 60% 58% 4.5% AKI 50% 42% AKI 40% 30% 20% 10% 0% prifle 16% 17% 9% No AKI Stage 1 Stage 2 Stage 3 Pediatr Crit Care Med 2007; 8:29 35 Al-Kandari et al, ASN, 2008

7 Pediatric AKI: Changing Epidemiology Previously: Primary renal diseases Number of Patients Pediatric ARF Causes Unknown AGN Hemoglobinuria Sepsis Hem Cystitis ATN-Dehyrdation Congenital Heart Fluid Overload Neoplasm Low Alb HUS Chronic Renal Dz Congestive heart Rhabdomyolysis ARDS Pyelonephritis Vasculitis Nephrotoxic Med Stickle SH et al: Am J Kid Dis 45:96-101, 2005

8 CRRT Diagnoses
9 RRT Options Hemodialysis, Peritoneal Dialysis, CRRT Each has advantages & disadvantages Choice is guided by Patient Characteristics Disease/Symptoms Hemodynamic stability Goals of therapy Fluid removal Electrolyte correction Both Availability, expertise and cost Pediatr Nephrol (2009) 24:37 48
10 Trends in Pediatric RRT CRRT Increasing 12-US Multicentre ppcrrt Most include Dialysis 60% 50% 40% 30% 20% CRRT PD HD 10% 0% Warady et al, Pediatr Neph 2000, 15:11-3
11 Why CRRT? Reduces hemodynamic instability preventing secondary ischemia Precise Volume control/immediately adaptable Uremic toxin removal Effective control of uremia, hypophosphatemia, hyperkalemia Acid base balance Rapid control of metabolic acidosis Electrolyte management Control of electrolyte imbalances Allows for improved provision of nutritional support Management of sepsis/plasma cytokine filter Safer for patients with head injuries
12 Indications for Pediatric RRT Electrolyte (metabolic) imbalance Uremia with bleeding and or encephalopathy Acuity/Degree of Kidney Injury reduction in GFR/elevated creatinine reduction in urine output Nutritional support Intoxications, Inborn errors of Metabolism (IEM) Fluid Overload (hypervolemia with pulmonary edema/respiratory failure)


13 Fluid Overload P<0.05 Independently associated with mortality in children at CRRT initiation.
14 Timing of Pediatric RRT????????? AKI definition may help. The decision to initiate RRT affected by strongly held physician beliefs Patient characteristics : age, race, illness acuity, and co-morbidities. Considerations Emerging importance of fluid overload prevention. Children develop MODS early in ICU course Maximum number of organ failures occurs within 72 hours of ICU admission (87% of patients) Organizational characteristics Children die with MODS very early in ICU course 88.4% of deaths occur within 7 days of MOSF diagnosis Proulx et al: Crit Care Med 22:1025, 1994
15 Children are not small adults 0 days to 21+ years 2 kg to 200 kg Not present Diabetes Older age Atherosclerotic disease Hypertension Volume of patients Present Size/Access variation Less frequent than adults/less experience Machinery is adapted (not made) for pediatrics Blood priming UF, thermic controls
16 Summary: Pediatric CRRT Epidemiology and Indications Pediatric AKI may be more common than previously described Primary renal disease giving way to MODS CRRT for children continues to expand Advantageous in critically ill child Effective therapy for renal failure Useful in setting of volume overload Best time to start remains uncertain Better AKI definitions will help answer??s
17 CRRT Terminology and Modalities
18 Diffusion vs. Convection Diffusion is solute transport across a semi-permeable membrane - molecules move from an area of higher to an area of lower concentration Effective for small molecule clearance Convection is a process where solutes pass across the semipermeable membrane along with the solvent in response to a positive transmembrane pressure Effectiveness less dependent on molecular size
19 Current Nomenclature for CRRT SCUF: CVVH: CVVHD: CVVHDF: Slow Continuous Ultrafiltration Continuous Veno-Venous Hemofiltration Continuous Veno-Venous Hemodialysis Continuous Veno-Venous Hemodiafiltration
20 CRRT Schematic R SCUF CVVH D CVVHD UF CVVHDF





21 CRRT Machines
22 Convection vs. Diffusion Are there advantages of one type of therapy over another? Solute (MW) Convective Coefficient Diffusion Coefficient Urea (60) 1.01 ± ± 0.07 Creatinine (113) 1.00 ± ± 0.06 Uric Acid (168) 1.01 ± ± 0.04* Vancomycin (1448) 0.84 ± ± 0.04** Cytokines (large) adsorbed minimal clearance *P<0.05, **P<0.01
23 Urea Clearance: CVVHD vs Pre-Dilution CVVH Parakininkas and Greenbaum, Ped Crit Care Med 2004
24 PreDilution CVVH vs CVVHDF: Effect on Solute Clearances Troyanov et al, Nephrol Dial Transplant 2003
25 Urea Clearance (mls/min/1.73 m2) Urea Clearance: CVVH vs CVVHD (Maxvold et al, Crit Care Med April 2000) p = NS 0 CVVH CVVHD BFR = 4 mls/kg/min FRF/Dx FR = 2 l/1.73 m2/hr SAM = 0.3 m2
26 Summary: CRRT Terminology and Modalities CRRT employs physical principles of diffusion and/or convection Nomenclature depends on methods used SCUF, CVVH, CVVHD, CVVHDF All methods that employ solutions are effective at removing small molecules Convection improves large particle removal Still unclear about best modality
27 Vascular Access and Anticoagulation for Pediatric CRRT
28 Why Access function is crucial for therapy Flows obtained will affect adequacy of blood flow for dose delivered and can affect filtercircuit life Downtime from clotted circuits-access is time off therapy
29 Access Considerations Low resistance Resistance ~ 8lη/2r 4 So, the biggest and shortest catheter should be best Vessel size French ~ 3 x diameter of vessel Beside ultrasound nearly universal SVC is bigger than femoral vein
30 Access Considerations Internal Jugular Very accessible Large caliber (SVC) Great flows Low recirculation rate Risk for Pneumothorax Cardiac monitoring may take precedence. Femoral Usually accessible Smaller than SVC Flows may be diminished by: Abdominal Pressures Patient movement Risk for retroperitoneal hemorrhage Higher recirculation rate Subclavian: Many feel current double lumen vas cath are too stiff to make the turn into the SVC and I don t personally use them. Although they are used in some centers. Better for bigger kids likely.

31 376 Patients 1574 circuits Femoral 69% IJ 16% Sub-Clavian 8% Not Specified 7%

32 Circuit Survival Curves by French Size of Catheter 5Fr Demise Hackbarth R et al: IJAIO December 2007
33 Summary: Vascular Access for Pediatric CRRT Put in the largest and shortest catheter when possible Caveat: short femoral catheters have been shown to have high rate of recirc in adult patients. (Little et al. AJKD 2000;36:1135-9) The IJ site is preferable (over femoral) when clinical situation allows Avoid double lumen 5Fr Catheters 2 site single lumen 5Fr catheters ok
34 Anticoagulation Another crucial step in delivering the prescribed dose (reducing downtime) Critically ill patients are at risk for both increased and decreased clot formation simultaneously


35 Heparin acts in conjunction with ATIII on thrombin and F IX, FX, FXII Calcium is necessary for each event in the cascade.

36 The Clot


37 What the filter looks like Hofbauer R et al. Kid Int 1999;56: Heparin Citrate Electron microscopy of polysulfone hemodiafilter with two varieties of anticoagualtion during IHD. Granted, no monitoring of degree of anticoagulation was performed to assess adequacy of response.
38 Anticoagulation Systemic Heparin Goal ACT sec Patient anticoagulated Risk of bleeding Risk for HIT Regional Citrate Goal Circuit ical mmol/L Goal Patient ical mmol/l Risk for Hypocalcemia Alkalosis Hypernatremia
39 138 Patients in multicenter registry study 442 Circuits Circuit survival time evaluated for three anticoagulation strategies Heparin (52% of circuits) Regional Citrate (36% of circuits) No anticoagulation (12% of circuits)
40 Brophy PD et al. Nephrol Dial Transplant. 2005;20: Mean circuit survival (42 and 44 hr) were not different for Hep vs Citrate, but both longer than no anticoagulation (27 hr) At 60 hr, 69% of Hep and Citrate circuits were functional, but only 28% of the noanticoagulation circuits In this analysis circuit survival was not affected by the access size Citrate group had no bleeding complications, 9 Heparin patients with bleeding
41 Citrate Specific Issues Alkalosis 1 mmol Citrate to 3 mmol HCO3 Normocarb protocols may exacerbate (35 meq/l) Hypernatremia Tri-Sodium Citrate infusion Hypocalcemic Citrate Toxicity Incomplete clearance of citrate, usually due to liver dysfunction Rising total calcium, decreasing ical
42 Citrate Specific Issues Alkalosis and Hypernatremia Increase diffusion clearance (increase dialysate flow) Or substitute normal saline for some of the high bicarb containing dialysate Others use pharmacy made citrate solutions with 0.67% Citrate vs 2% standard citrate solution (Tolwani AJ et al. Clin J Am Soc Nephrol 2006;1:79-87)
43 Hypocalcemic Citrate Toxicity Rising Total Calcium Declining ical Usually see with infants (more Qb hence citrate than total clearance) and in those with liver failure Risk for severe hypocalcemia Rx by decreasing citrate, and/or a period of increased clearance (D or UF)
44 Summary: Anticoagulation for Pediatric CRRT Heparin or Citrate is better than no anticoagulation (even in liver failure, DIC, etc) Citrate has fewer bleeding complications Circuit survival means less downtime hence more delivered therapy Pick institutional strategy and learn to use it well Consider citrate as the method of choice
45 Prescribing Pediatric CRRT
46 Prescribing Pediatric CRRT Vascular access Hemofilter Prime Blood pump speed (Q B ) Anticoagulation Ultrafiltration rate Infused fluids CVVH: Pre- and/or post-dilutional replacement CVVHD: Counter-current dialysate CVVHDF: Dialysate and replacement fluid
47 Hemofilter for CRRT Hemofilter size Volume, porosity Membrane material Polysulfone, AN-69, PAES, etc. Tubing set integrated or separate? Open vs. closed systems do you have a choice?
48 Blood Priming the Circuit for Pediatric CRRT Small patient, large extracorporeal volume Albumin Hemodynamic instability Saline Common default approach Self Volume loaded renal failure patient
49 Choosing Q B for Pediatric CRRT Choose blood flow rate (Q B ) of 3-5ml/kg/min, or: 0-10 kg: 25-50ml/min 11-20kg: ml/min 21-50kg: ml/min >50kg: ml/min CRRT device may affect choices for Q B The real determinant the vascular access
50 Ultrafiltration in Pediatric CRRT Choose UF rate to balance input remove excess fluid over time make room for IV fluids and nutrition provide solute clearance by convection SCUF, CVVHD, post-dilution CVVH: UF rate may be limited by blood flow (filtration fraction) Pre-dilution CVVH: High flow of pre-dilution fluid lessens hemoconcentration Remember to consider UF limits of the filter, especially in higher-volume hemofiltration
51 Infused Fluids for Pediatric CRRT SCUF: No infused fluids CVVHD: Counter-current dialysate CVVH: Pre- and/or post-dilution replacement fluid CVVHDF: Dialysate and replacement fluids
52 Rate for Infused Fluid Higher rates increase clearance Lower rates may simplify electrolyte balance and limit protein loss Equations to help choose rate for fluid: ml/kg/hr ml/hr/1.73m 2 May need higher rates to balance citrate delivery
53 Dialysate / Ultrafiltration Rates No Study has identified effective, safe UF or dialysate flow rates in Children. For HEMODIALYSIS NET UF rate of 0.2ml/kg/min is tolerated This extrapolates to 1 ml/kg/ hr (NET UF) over 48 hr of continuous hemofiltration. Donckerwolke Ped Neph 8: ,1994
54 Summary: Prescribing Pediatric CRRT Consider needs for vascular access, hemofilter, priming of circuit, blood pump speed (Q B ), anticoagulation, UF goals, and infused fluids Choices may depend on clinical status of the patient and capabilities at your facility Coordination with all members of the critical care team is essential
55 Solutions for Pediatric CRRT: Dialysis Fluids and Replacement Fluids
56 Characteristics of the Ideal CRRT Solution Physiological Reliable Inexpensive Easy to prepare Simple to store Quick to the bedside Widely available Fully compatible
57 Purpose of CRRT solutions Provide safe and consistent metabolic control To be adaptive to the choice of therapy- CVVH vs CVVHD
58 Options for CRRT Solutions Peritoneal dialysate: Pre-made IV solutions: Saline, Lactated Ringers Multi-bag systems: Custom-made solutions: Local pharmacy; outsource NO MAYBE UNNECESSARY RARELY Commercially available CRRT solutions
59 Evaluation of Errors in Preparation of CRRT Solutions Survey of 3 Pediatric Listserves: Pediatric Critical Care Pediatric Nephrology Pediatric CRRT 31 programs responded to query Barletta JF et.al Pediatr Nephrol Jun;21(6):842-5
60 Prevalence and Consequences of Errors in Solution Preparation 16/31 programs reported errors: 7 errors in replacement solutions 9 errors in dialysate solutions Consequences of improper solutions 2 deaths 1 non lethal cardiac arrest 6 seizures (hypo/hypernatremia) 7 without complications Barletta JF et.al Pediatr Nephrol Jun;21(6):842-5
61 Policy Changes Resulting from Errors in Solutions Changed to Normocarb for either replacement or dialysate (11) Changed to PrismaSate for dialysate (2) Purchased TPN mixer for solutions (2) Chemistry lab check of every bag (3) Bag label check by at least 2 staff (10) Barletta JF et.al Pediatr Nephrol Jun;21(6):842-5
62 What s the Difference Between Dialysate and Replacement Fluid? Dialysate is a Device Replacement Fluid is a Drug
63 CRRT Solutions Many Choices Name Company R / D Bag Size* Flavors Normocarb HF DSI R 3.24 L 2 Prismasate Gambro D 5 L 6 Accusol Baxter D 2.5 L 5 Prismasol Gambro R 5 L 7 Duosol B Braun D 5 L 6 PureFlow NxStage D 5 5 *after mixing
64 Summary: CRRT Solutions Solutions needed to maximize clearance Pharmacy made solutions give greatest flexibility but have increased risks/costs Several industry-made solutions two currently approved for replacement
65 Outcome/ Demographics
66 Pediatric Acute Renal Failure: Ideal Study Design Prospective protocol driven entry criteria to ensure that patients and their respective disease receive similar treatment --- Do not exist! Control for severity of illness, primary and comorbid diseases --- Some information Adequate power to detect effect of an intervention on or an association of a clinical variable with outcome --- Do not exist!
67 Retrospective evaluation of 226 children who received RRT for AKI from Pressor use surrogate marker for patient severity of illness Survival defined at PICU discharge


68
69 Retrospective review of all patients who received CVVH(D) in the Texas Children s Hospital PICU from February 1996 through September 1998 (32 months) Pre-CVVH initiation data: Age Primary disease leading to need for CVVH Co-morbid diseases Reason for CVVH Fluid intake (Fluid In) from PICU admission to CVVH initiation Fluid output (Fluid Out) from PICU admission to CVVH initiation GFR (Schwartz formula) at CVVH initiation
70 Percent Fluid Overload Calculation % FO at CVVH initiation = [ Fluid In - Fluid Out ICU Admit Weight ] * 100% Fluid In = Total Input from ICU admit to CRRT initiation Fluid Out = Total Output from ICU admit to CRRT initiation
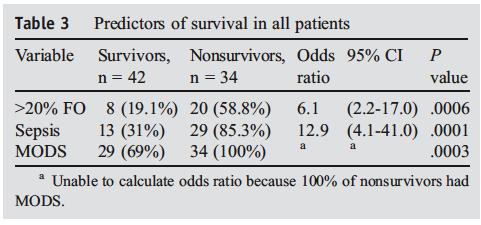
71 22 pt (12 male/10 female) received 23 courses (3028 hrs) of CVVH (n=10) or CVVHD (n=12) over study period. Overall survival was 41% (9/22). Survival in septic patients was 45% (5/11). PRISM scores at ICU admission and CVVH initiation were /- 5.7 and /- 9.0, respectively (p=ns). Conditions leading to CVVH (D) Sepsis (11) Cardiogenic shock (4) Hypovolemic ATN (2) End Stage Heart Disease (2) Hepatic necrosis, viral pneumonia, bowel obstruction and End-Stage Lung Disease (1 each)
72 Survival curve demonstrates that nearly 75% of deaths occurred less than 25 days into the ICU course Cumulative Proportion Surviving Survival Time (days)
73 Lesser % FO at CVVH (D) initiation was associated with improved outcome (p=0.03) Lesser % FO at CVVH (D) initiation was also associated with improved outcome when sample was adjusted for severity of illness (p=0.03; multiple regression analysis) %FO at CVVH Initiation Death p = 0.03 Survival Mean+SE Mean-SE Mean OUTCOME

74 N=113 *p=0.02; **p=0.01
75 N = 77 Group Fluid Overload Hazard Ratio (95% CI) P All Subjects <10% 1 >10% 3.02 ( ) 0.002

76 Kaplan-Meier survival estimates, by percentage fluid overload category

77

78

79
80 The Evolution of Idea to Practice Paradigm:The ppcrrt Registry Group Michael Somers Michelle Baum Cheryl Baker Theresa Mottes Jordan Symons Nancy McAfee Tim Bunchman Rick Hackbarth Dawn Eding Mark Benfield David Askenazi James Fortenberry Kristine Rogers Renee Robinson John Mahan Deepa Chand Francisco Flores Kevin McBryde Steven Alexander Annabelle Chua Douglas Blowey Stuart Goldstein (Founder)
81 Prospective Pediatric CRRT (ppcrrt ) Registry: Phase 1 Design Collect prospective data from 10 pediatric centers treating 15 to 20 patients annually (376 patients over 5 years) Each center follows own institutional practice Patient selection Initiation and termination Anti-coagulation protocols Convection versus diffusion versus hemodiafiltration Fluid composition
82 Overall Survival rate 58%
83
84


85 Seven center study from the ppcrrt Registry 116 patients with MODS PRISM 2 score used to assess patient severity of illness Survival defined at PICU discharge
86 ppcrrt FO Threshold: Multivariate analysis Variable Fluid Overload Group 20% FO vs. <10% FO 20% FO vs. 10%-20% FO 10%-20% FO vs. <10% FO Odds Ratio (Mortality) % Confidence Interval p-value < Oncologic Diagnosis <0.001 Diagnosis of MODS Sepsis Diagnosis Convective CRRT Modality PRISM II PICU Admission IEM/Intoxication Diagnosis Inotrope Number CRRT Initiated to treat FO Age at CRRT Initiation Sex Sutherland S. for the ppcrrt: Am J Kidney Dis Feb;55(2):
87 Mortality Rate 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 36.7% 22.1% 29.4% ppcrrt FO Threshold: Multivariate analysis 43.1% 10% Fluid 10%-20% Fluid Overload Sutherland S. for the ppcrrt: Am J Kidney Dis Feb;55(2): % 29.1% 75.4% 55.8% 65.6% 20% Fluid Overload
88 Stem Cell Transplant: ppcrrt 51 patients in ppcrrt with SCT Mean %FO = %. 45% survival Convection: 17/29 survived (59%) Diffusion: 6/22 (27%), p<0.05 Survival lower in MODS/ventilated patients Flores FX et al: Pediatric Nephrology

89 Percent survival Survival Based on CRRT Modality Pediatric Stem Cell Transplant Recipients P < 0.05 CVVH + CVVHDF CVVHD Flores FX et. al Peds Neph (in Press)
90 ppcrrt & SCT Variable Survivors Non-survivors p Value Patient Admit Age (yr) NS Patient Admit Weight (kg) NS Patients kept dry prior to CRRT initiation No difference in any parameter at CRRT initiation Paw worse for nonsurvivors at CRRT end PRISM 2 at PICU admit PICU Days to CRRT Initiation NS PRISM 2 at CRRT Initiation CRRT Initiation GFR (ml/min/1.73) NS %FO at CRRT Initiation NS No. Inotropes at CRRT Initiation CVP at CRRT Initiation NS Paw at CRRT Initiation (mmh 2 O) NS Paw at End CRRT (mmh 2 O) <0.001 Urine Output (ml/kg/hr) NS CRRT Duration (day) NS Filtration (ml/min/1.73 m 2 ) NS Flores FX et al: Pediatric Nephrology in press

91


92 Ronco, Lancet, 2000 The Ronco Study Improved survival in all patients with convective clearance of 35mL/kg/hr Trend towards improved survival in septic patients with convective clearance of 45mL/kg/hr
93 The ATN Study 1124 adults in the ICU 563 had intensive therapy 561 had less-intensive therapy
94 ATN Study

95 ATN Study
 NEJM 361(17);")
96 Intensity of CRRT in Critically Ill Patients (The RENAL Study) NEJM 361(17); Oct 2009
97 Intensity of CRRT in Critically Ill Patients (The RENAL Study) NEJM 361(17); Oct 2009
98 CRRT Associated Mortality in Major RCT s Borrowed with permission from Claudio Ronco M.D. Clinical Trial Comparison APACHE II Endpoint Mortality Ronco 2000 CRRT dose day 59% Mehta 2001 IHD vs. CRRT 25.5 Hospital 66% Augustine 2004 IHD vs. CRRT - Hospital 68% Saudan 2006 CRRT dose Day 66% Vinsonneau 2006 IHD vs. CRRT day 68% Lins 2008 IHD vs. CRRT 27 Hospital 58% Tolwani 2008 CRRT dose 26 Hospital 60% ATN 2008 Dialysis Dose day 52.5% RENAL 2009 CRRT dose day 45%
99 Pediatric CRRT Associated Mortality Clinical Trial Study design N PRISM Survival Goldstein et al Pediatrics 2001 Gillespie et al. Ped Neph 2004 Foland et al PCCM 2004 Symons et al CJASN 2008 Hayes et al. JCC 2009 Retrospective % Retrospective % Retrospective % ppcrrt Registry % Retrospective
100 BUN at initiation of RRT Predialysis BUN Mortality (%) Early Late Early Late Parson 61 > Fischer Kleinknecht Conger Gettings Bouman Liu >

101 Fluid Accumulation and Survival Bouchard J, et al. Kidney International 2009
102 Fluid Overload in IHD vs. CRRT PICARD study Bouchard J, et al. Kidney International 2009
103 Outcomes after pediatric AKI Hospital Survival of Pediatric AKI 176 / 245 ( 72% ) hospital survival 3-5 year Follow-up Survival Additional 37 children die 139 / 245 (58%) of the original cohort Renal Dysfunction 29 patients 59 % had at least one of the following» HTN, CKD and/ or microalbuminuria 1. Arikan A, et al. Kidney International Hui-Stickle S, et al: Am J Kidney Dis June Askenazi DJ et al. Kidney International January 2006


104 Approach to Pediatric AKI EGDT Defend Blood Pressure Restore & Optimize Perfusion Use inotropes with care Mitigate Inflammatory Injury Optimize RRT Normal Increased risk Damage GFR Kidney failure Death Antecedents Intermediate Stage AKI Outcomes
105 Reference Tools Adqi.net-web site for information on CRRT Crrtonline.com-web site for info on Dr Mehta s meeting Pediatric CRRT with links to other meetings, protocols, industry 5th International Conf on Pediatric CRRT June 19-21, 2008 Orlando, Florida PCRRT list serve (contact Bunchman)
106 Thanks ppcrrt members Dr. Ravi Mehta Bedside ICU and Dialysis Nurses
Renal replacement therapy in Pediatric Acute Kidney Injury
 Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
CRRT in Pediatrics: Indications, Techniques & Outcome. Overview
 CRRT in Pediatrics: Indications, Techniques & Outcome Timothy E. Bunchman Pediatric Nephrology & Transplantation Grand Rapids, MI Overview (Please interrupt me at any time) Access Solutions Anticoagulation
CRRT in Pediatrics: Indications, Techniques & Outcome Timothy E. Bunchman Pediatric Nephrology & Transplantation Grand Rapids, MI Overview (Please interrupt me at any time) Access Solutions Anticoagulation
Technical Considerations for Renal Replacement Therapy in Children
 Technical Considerations for Renal Replacement Therapy in Children Timothy E. Bunchman, MD,* Patrick D. Brophy, MD, and Stuart L. Goldstein, MD Summary: Provision of renal replacement therapy to the critically
Technical Considerations for Renal Replacement Therapy in Children Timothy E. Bunchman, MD,* Patrick D. Brophy, MD, and Stuart L. Goldstein, MD Summary: Provision of renal replacement therapy to the critically
Practice Based Learning in CRRT: The Science and the Art Pediatric Session. David Askenazi Theresa Mottes Scott Sutherland
 Practice Based Learning in CRRT: The Science and the Art Pediatric Session David Askenazi Theresa Mottes Scott Sutherland 1 Objectives Brief Epidemiology Challenges with Pediatric CRRT Indications Prescription
Practice Based Learning in CRRT: The Science and the Art Pediatric Session David Askenazi Theresa Mottes Scott Sutherland 1 Objectives Brief Epidemiology Challenges with Pediatric CRRT Indications Prescription
Clinical Application of CRRT for Infants and Children
 Clinical Application of CRRT for Infants and Children Geoffrey Fleming Daryl Ingram Jordan Symons 22 nd International Conference on Advances in Critical Care Nephrology San Diego 2017 Introduction Pediatric
Clinical Application of CRRT for Infants and Children Geoffrey Fleming Daryl Ingram Jordan Symons 22 nd International Conference on Advances in Critical Care Nephrology San Diego 2017 Introduction Pediatric
Recent advances in CRRT
 Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
Pediatric Continuous Renal Replacement Therapy
 Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
ASN Board Review: Acute Renal Replacement Therapies
 ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
CRRT for the Experience User 1. Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018
 CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of
 Update on CRRT: Pearls for the Clinician Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of Medicine tbunchman@mcvh-vcu.edu
Update on CRRT: Pearls for the Clinician Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of Medicine tbunchman@mcvh-vcu.edu
UAB CRRT Primer Ashita Tolwani, MD, MSc University of Alabama at Birmingham
 UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
CRRT: The Technical Questions Modality & Dose. Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018
 CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Dialysis Dose Prescription and Delivery. William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012
 Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Olistic Approach to Treatment Adequacy in AKI
 Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Renal Replacement Therapy in ICU. Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine
 Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Pediatric AKI in Bad Pediatric CRRT is Hard
 Pediatric AKI in Bad Pediatric CRRT is Hard David Askenazi MD, MSPH Professor of Pediatrics Director Pediatric and Infant Center for Acute Nephrology (PICAN) Potential COI Speaker for Baxter, and the AKI
Pediatric AKI in Bad Pediatric CRRT is Hard David Askenazi MD, MSPH Professor of Pediatrics Director Pediatric and Infant Center for Acute Nephrology (PICAN) Potential COI Speaker for Baxter, and the AKI
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background
 Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background Index: 1. Introduction Pg. 1 1.1 Definitions Pg. 2 1.2 Renal replacement therapy principles Pg. 2 2. Continuous
Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background Index: 1. Introduction Pg. 1 1.1 Definitions Pg. 2 1.2 Renal replacement therapy principles Pg. 2 2. Continuous
MODALITIES of Renal Replacement Therapy in AKI
 MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
Who? Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011
 Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
higher dose with progress in technical equipment. Continuous Dialysis: Dose and Antikoagulation. prescribed and delivered
 1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
Decision making in acute dialysis
 Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
03/19/2019. Michael Zappitelli, MD, MSc Hospital for Sick Children, Toronto. Symposium on Pediatric Dialysis, ADC, Dallas, 2019
 Michael Zappitelli, MD, MSc Hospital for Sick Children, Toronto Symposium on Pediatric Dialysis, ADC, Dallas, 2019 Baxter: Reimbursed for a CRRT workshop to PICU nurses Slides: S. Goldstein D. Askenazi
Michael Zappitelli, MD, MSc Hospital for Sick Children, Toronto Symposium on Pediatric Dialysis, ADC, Dallas, 2019 Baxter: Reimbursed for a CRRT workshop to PICU nurses Slides: S. Goldstein D. Askenazi
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
Essential in Renal Replacement Therapy Pediatrics CRRT
 Essential in Renal Replacement Therapy Pediatrics CRRT Konggrapun Srisuwan MD. Dialysis and Transplantation Program, Department of Pediatrics, Phramongkutklao Hospital Correction of fluid overload in patients
Essential in Renal Replacement Therapy Pediatrics CRRT Konggrapun Srisuwan MD. Dialysis and Transplantation Program, Department of Pediatrics, Phramongkutklao Hospital Correction of fluid overload in patients
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement
 Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Acute Kidney Injury- What Is It and How Do I Treat It?
 Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
UNDERSTANDING THE CRRT MACHINE
 UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
Active UMMC Protocols
 UMMC CRRT 2018 Active UMMC Protocols 1. Standard CRRT Protocol PrismaFlex & NxStage CVVH with Fixed Ratio Regional Citrate Anticoagulation 2. No Anticoagulation Protocol PrismaFlex & NxStage CVVH with
UMMC CRRT 2018 Active UMMC Protocols 1. Standard CRRT Protocol PrismaFlex & NxStage CVVH with Fixed Ratio Regional Citrate Anticoagulation 2. No Anticoagulation Protocol PrismaFlex & NxStage CVVH with
Continuous Renal Replacement Therapy for Children <= 10 kg: A Report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry
 Continuous Renal Replacement Therapy for Children
Continuous Renal Replacement Therapy for Children
Continuous renal replacement therapy. David Connor
 Continuous renal replacement therapy David Connor Overview Classification of AKI Indications Principles Types of CRRT Controversies RIFL criteria Stage GFR Criteria Urine Output Criteria Risk Baseline
Continuous renal replacement therapy David Connor Overview Classification of AKI Indications Principles Types of CRRT Controversies RIFL criteria Stage GFR Criteria Urine Output Criteria Risk Baseline
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 2.0 (March 2017) PICANet Renal Custom Audit Data s Manual Version 2.0 29/03/2017 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 2.0 (March 2017) PICANet Renal Custom Audit Data s Manual Version 2.0 29/03/2017 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
- SLED Sustained Low-Efficiency Dialysis
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy. Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous renal replacement therapy (CRRT) has become the preferred dialysis option to support children with
 has become the preferred dialysis option to support children with") Continuous Renal Replacement Therapy for Children #10 kg: A Report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry David J. Askenazi, MD, MSPH 1, Stuart L. Goldstein, MD 2,
Continuous Renal Replacement Therapy for Children #10 kg: A Report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry David J. Askenazi, MD, MSPH 1, Stuart L. Goldstein, MD 2,
CRRT Procedures. and Guidelines. CRRT: Guidelines
 CRRT Procedures 2013 and Guidelines Guidelines for the utilization of CRRT (Continuous Renal Replacement Therapies) at Monroe Carell Jr. Children s Hospital at Vanderbilt CRRT: Guidelines CRRT Contacts:
CRRT Procedures 2013 and Guidelines Guidelines for the utilization of CRRT (Continuous Renal Replacement Therapies) at Monroe Carell Jr. Children s Hospital at Vanderbilt CRRT: Guidelines CRRT Contacts:
ST. DOMINIC-JACKSON MEMORIAL HOSPITAL JACKSON, MISSISSIPPI. CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) HEPARIN ANTICOAGULATION Page 1 of 5
 HEPARIN ANTICOAGULATION Page 1 of 5") HEPARIN ANTICOAGULATION Page 1 of 5 Pharmacy Mnemonic: CRRTHEP1 PATIENT DATA: DIAGNOSIS: AKI ESRD Other: WEIGHT: Today: kg Admission Weight:: kg Dry Weight: kg Access TYPE: Temporary Dialysis Catheter
HEPARIN ANTICOAGULATION Page 1 of 5 Pharmacy Mnemonic: CRRTHEP1 PATIENT DATA: DIAGNOSIS: AKI ESRD Other: WEIGHT: Today: kg Admission Weight:: kg Dry Weight: kg Access TYPE: Temporary Dialysis Catheter
RENAL FAILURE IN ICU. Jo-Ann Vosloo Department Critical Care SBAH
 RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy
 Cedarville University DigitalCommons@Cedarville Pharmacy Faculty Presentations School of Pharmacy 2-23-2012 Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy Jeb Ballentine
Cedarville University DigitalCommons@Cedarville Pharmacy Faculty Presentations School of Pharmacy 2-23-2012 Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy Jeb Ballentine
Symposium. Principles of Renal Replacement Therapy in Critically ill children- Indian Perspective
 Symposium DOI- 10.21304/2018.0502.00376 in Critically ill children- Indian Perspective Sidharth Kumar Sethi *, Aliza Mittal**, Rupesh Raina***, Manindar Dhaliwal**** * Senior Consultant, Pediatric Nephrology
Symposium DOI- 10.21304/2018.0502.00376 in Critically ill children- Indian Perspective Sidharth Kumar Sethi *, Aliza Mittal**, Rupesh Raina***, Manindar Dhaliwal**** * Senior Consultant, Pediatric Nephrology
oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators
 oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators Heparin-grafted for reduced thrombogenicity Supports renal function POWERED
oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators Heparin-grafted for reduced thrombogenicity Supports renal function POWERED
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
Session 1: Circuit, Anticoagulation and Monitoring. Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019
 Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
CRRT. ICU Fellowship Training Radboudumc
 CRRT ICU Fellowship Training Radboudumc Timing RRT Consider the following: Underlying cause and reversibility. Rapid improvement unlikely with high dose vasopressors and continuous exposure to other risk
CRRT ICU Fellowship Training Radboudumc Timing RRT Consider the following: Underlying cause and reversibility. Rapid improvement unlikely with high dose vasopressors and continuous exposure to other risk
Overview of Pediatric Continuous Renal Replacement Therapy in Acute Kidney Injury
 대한소아신장학회지제 15 권제 2 호 2011년 종설 http://dx.doi.org/10.3339/jkspn.2011.15.2.107 1) Overview of Pediatric Continuous Renal Replacement Therapy in Acute Kidney Injury Se Jin Park, M.D. and Jae Il Shin, M.D.
대한소아신장학회지제 15 권제 2 호 2011년 종설 http://dx.doi.org/10.3339/jkspn.2011.15.2.107 1) Overview of Pediatric Continuous Renal Replacement Therapy in Acute Kidney Injury Se Jin Park, M.D. and Jae Il Shin, M.D.
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Physiology of Blood Purification: Dialysis & Apheresis. Outline. Solute Removal Mechanisms in RRT
 Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Large RCT s s in RRT : What can be learnt for nursing?
 Large RCT s s in RRT : What can be learnt for nursing? Ian Baldwin Dept. of Intensive Care, Austin Hospital Adjunct Professor, RMIT University CRRT 2011 Hilton Bayfront, February 22-25 SanDiego Key Hypothesis
Large RCT s s in RRT : What can be learnt for nursing? Ian Baldwin Dept. of Intensive Care, Austin Hospital Adjunct Professor, RMIT University CRRT 2011 Hilton Bayfront, February 22-25 SanDiego Key Hypothesis
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Paul R. Bowlin, M.D. University of Colorado Denver. May 12 th, 2008
 Paul R. Bowlin, M.D. University of Colorado Denver May 12 th, 2008 Presentation Overview Background / Definitions History Indications for initiation of therapy Outcomes Studies Conclusions Questions Background
Paul R. Bowlin, M.D. University of Colorado Denver May 12 th, 2008 Presentation Overview Background / Definitions History Indications for initiation of therapy Outcomes Studies Conclusions Questions Background
Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience
 Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience Casey N. Gashti, MD, Susana Salcedo, MD, Virginia Robinson, RN, and Roger A. Rodby, MD Background: Renal replacement therapies
Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience Casey N. Gashti, MD, Susana Salcedo, MD, Virginia Robinson, RN, and Roger A. Rodby, MD Background: Renal replacement therapies
CRRT: QUALITY MANAGEMENT SYSTEMS
 CRRT: QUALITY MANAGEMENT SYSTEMS Javier A. Neyra, MD, MSCS Director, Acute Care Nephrology & CRRT Program University of Kentucky Medical Center Disclosures and Funding Disclosures Consulting agreement
CRRT: QUALITY MANAGEMENT SYSTEMS Javier A. Neyra, MD, MSCS Director, Acute Care Nephrology & CRRT Program University of Kentucky Medical Center Disclosures and Funding Disclosures Consulting agreement
Prof Patrick Honoré,MD, PhD,FCCM Intensivist-Nephrologist
 Pro-Con Debate on High Volume Hemofiltration :Burial or Ressurection? The Pro Position 1.-Why Moving From Dose To Membranes? 4.-AN69 Oxiris LPS Adsorptive Membranes in Sepsis 2.- High Cut-Off Membranes
Pro-Con Debate on High Volume Hemofiltration :Burial or Ressurection? The Pro Position 1.-Why Moving From Dose To Membranes? 4.-AN69 Oxiris LPS Adsorptive Membranes in Sepsis 2.- High Cut-Off Membranes
Pediatric AKI & CRRT: Caring for my Patient & Program? David Selewski, MD Theresa Mottes, RN, NP
 Pediatric AKI & CRRT: Caring for my Patient & Program? David Selewski, MD Theresa Mottes, RN, NP Introduction Pediatric AKI is no longer a mystery issue Growing data on epidemiology and outcome Pediatric
Pediatric AKI & CRRT: Caring for my Patient & Program? David Selewski, MD Theresa Mottes, RN, NP Introduction Pediatric AKI is no longer a mystery issue Growing data on epidemiology and outcome Pediatric
Citrate Anticoagulation
 Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done?
 Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done? Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta Disclosure Consulting: Alere, Baxter, Gambro,
Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done? Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta Disclosure Consulting: Alere, Baxter, Gambro,
Renal Replacement Therapy in Acute Renal Failure
 CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
Drug Use in Dialysis
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
(Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
Acute Kidney Injury. Arvind Bagga All India Institute of Medical Sciences New Delhi, India
 Acute Kidney Injury Arvind Bagga All India Institute of Medical Sciences New Delhi, India What is AKI? Sudden loss of renal function, over hrdays, with derangement(s) in fluid balance, acid base & electrolytes
Acute Kidney Injury Arvind Bagga All India Institute of Medical Sciences New Delhi, India What is AKI? Sudden loss of renal function, over hrdays, with derangement(s) in fluid balance, acid base & electrolytes
Continuous renal replacement therapy in children with multiple organ dysfunction syndrome: A case series
 CHALLENGING CLINICAL CASES Vol. 40 (6): 846-852, November - December, 2014 doi: 10.1590/S1677-5538.IBJU.2014.06.18 Continuous renal replacement therapy in children with multiple organ dysfunction syndrome:
CHALLENGING CLINICAL CASES Vol. 40 (6): 846-852, November - December, 2014 doi: 10.1590/S1677-5538.IBJU.2014.06.18 Continuous renal replacement therapy in children with multiple organ dysfunction syndrome:
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Renal replacement therapy in acute kidney injury
 6 February 2009 CONTENTS Renal replacement therapy in acute kidney injury S Jithoo Commentator: CL Quantock Moderator: LW Drummond INTRODUCTION... 3 WHAT IS RENAL REPLACEMENT THERAPY?... 3 MODES OF RENAL
6 February 2009 CONTENTS Renal replacement therapy in acute kidney injury S Jithoo Commentator: CL Quantock Moderator: LW Drummond INTRODUCTION... 3 WHAT IS RENAL REPLACEMENT THERAPY?... 3 MODES OF RENAL
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital
 Renal Dialysis Centre Hong Kong Sanatorium & Hospital") Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD. Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi
 LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD 2008 Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi Effect of acute renal failure requiring renal replacement therapy on
LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD 2008 Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi Effect of acute renal failure requiring renal replacement therapy on
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO
 ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland NO CONFLICT OF INTERESTS Important concept
ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland NO CONFLICT OF INTERESTS Important concept
Continuous renal replacement therapy Gulzar Salman Amlani Aga Khan University, School of Nursing, Karachi.
 Special Communication Continuous renal replacement therapy Gulzar Salman Amlani Aga Khan University, School of Nursing, Karachi. Abstract Acute renal failure refers to sudden deterioration in biochemical
Special Communication Continuous renal replacement therapy Gulzar Salman Amlani Aga Khan University, School of Nursing, Karachi. Abstract Acute renal failure refers to sudden deterioration in biochemical
Blood purification in sepsis
 Blood purification in sepsis Joannes-Boyau O Dept of anesthesiology and intensive care, University Hospital of Bordeaux, France 1 Types of Blood Purification hemofilters regular pore size (MW < 40,000D)
Blood purification in sepsis Joannes-Boyau O Dept of anesthesiology and intensive care, University Hospital of Bordeaux, France 1 Types of Blood Purification hemofilters regular pore size (MW < 40,000D)
Dialysis in the Acute Setting
 Dialysis in the Acute Setting medicine2.missouri.edu/jahm/dialysis-in-the-acute-setting/ October 8, 2015 Kunal Malhotra, MD Division of Nephrology, Department of Medicine, University of Missouri School
Dialysis in the Acute Setting medicine2.missouri.edu/jahm/dialysis-in-the-acute-setting/ October 8, 2015 Kunal Malhotra, MD Division of Nephrology, Department of Medicine, University of Missouri School
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2
 Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
7/17/2017 FSHP 2017 ANNUAL MEETING. Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy
 FSHP Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy Disclosure I do not have (nor does any immediate family member have) a vested interest in or affiliation
FSHP Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy Disclosure I do not have (nor does any immediate family member have) a vested interest in or affiliation
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
Regional Citrate Anticoagulation for RRTs in Critically Ill Patients with AKI
 In-Depth Review Regional Citrate Anticoagulation for RRTs in Critically Ill Patients with AKI Santo Morabito,* Valentina Pistolesi,* Luigi Tritapepe, and Enrico Fiaccadori Abstract Hemorrhagic complications
In-Depth Review Regional Citrate Anticoagulation for RRTs in Critically Ill Patients with AKI Santo Morabito,* Valentina Pistolesi,* Luigi Tritapepe, and Enrico Fiaccadori Abstract Hemorrhagic complications
Aquarius Study Day Adult Pre-Reading Study Pack
 Aquarius Study Day Adult Pre-Reading Study Pack An Introduction to CRRT (Continuous Renal Replacement Therapy) Name Date. Hospital.. Please take the opportunity to read this booklet prior to attending
Aquarius Study Day Adult Pre-Reading Study Pack An Introduction to CRRT (Continuous Renal Replacement Therapy) Name Date. Hospital.. Please take the opportunity to read this booklet prior to attending
404FM.2 CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) USING CITRATE Target Audience: Hospital only ICU. (Based on Gambro and Kalmar Hospital protocols)
 USING CITRATE Target Audience: Hospital only ICU. (Based on Gambro and Kalmar Hospital protocols)") 404FM.2 CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) USING CITRATE Target Audience: Hospital only ICU (Based on Gambro and Kalmar Hospital protocols) CRRT using regional citrate anticoagulation This is
404FM.2 CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) USING CITRATE Target Audience: Hospital only ICU (Based on Gambro and Kalmar Hospital protocols) CRRT using regional citrate anticoagulation This is
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Contrast Induced Nephropathy
 Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Competency assessment in CRRT core curriculum. G07
 Competency assessment in CRRT core curriculum. G07 San Diego 2011 Hilton Bayfront Ian Baldwin R.N. PhD. Austin Hospital RMIT University Australia Heamofiltration Continuous Renal Replacement Therapy (CRRT)
Competency assessment in CRRT core curriculum. G07 San Diego 2011 Hilton Bayfront Ian Baldwin R.N. PhD. Austin Hospital RMIT University Australia Heamofiltration Continuous Renal Replacement Therapy (CRRT)
ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN. Bashir Admani KPA Precongress 24/4/2018
 ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN Bashir Admani KPA Precongress 24/4/2018 Case presentation SP 11month old Presenting complaint: bloody diarrhea, lethargy On exam: dehydration,
ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN Bashir Admani KPA Precongress 24/4/2018 Case presentation SP 11month old Presenting complaint: bloody diarrhea, lethargy On exam: dehydration,
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
James Beck ECS 8 November 2014 Citrate anticoagulation for continuous renal replacement therapy
 Citrate anticoagulation for continuous renal replacement therapy Clinical Problem A 73 year old female patient presented to the Accident and Emergency Department (A&E) with a profound anaemia, acute kidney
Citrate anticoagulation for continuous renal replacement therapy Clinical Problem A 73 year old female patient presented to the Accident and Emergency Department (A&E) with a profound anaemia, acute kidney
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen
 When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
egfr 34 ml/min egfr 130 ml/min Am J Kidney Dis 2002;39(suppl 1):S17-S31
:S17-S31") Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015)
 CITRATE GUIDELINES (Approved May 2015)") Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015) BCU Citrate Guideline v6 Nov 2015 (Approved by CCSC May 15) 1 BCU Critical Care Guideline for Renal Replacement Therapy
Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015) BCU Citrate Guideline v6 Nov 2015 (Approved by CCSC May 15) 1 BCU Critical Care Guideline for Renal Replacement Therapy
Continuous Renal Replacement Therapy in Dogs and Cats
 Continuous Renal Replacement Therapy in Dogs and Cats Mark J. Acierno, MBA, DVM KEYWORDS Continuous renal replacement therapy CRRT Acute kidney injury Dialysis In the early 1900s, a young pharmacologist
Continuous Renal Replacement Therapy in Dogs and Cats Mark J. Acierno, MBA, DVM KEYWORDS Continuous renal replacement therapy CRRT Acute kidney injury Dialysis In the early 1900s, a young pharmacologist
Admission Day 2 Na Potassium Cl Bicarb BUN Cr Hb Hct platelets
 Nithin Karakala Mr. Clark Kent was admitted to the hospital with multiple injuries after an epic battle with the Kryptonians. He was hypotensive at the time of admission. Over the next 24 hours he develops
Nithin Karakala Mr. Clark Kent was admitted to the hospital with multiple injuries after an epic battle with the Kryptonians. He was hypotensive at the time of admission. Over the next 24 hours he develops