Acute Kidney Injury- What Is It and How Do I Treat It?
|
|
|
- Pierce Hardy
- 5 years ago
- Views:
Transcription


1 Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1
2 KDIGO criteria for AKI Increase in serum creatinine of 0.3 mg/dl within 48 hours Increase in serum creatinine of 1.5 times baseline within prior 7 days Urine volume <0.5 ml/kg/hour for more than 6 hours Complications of AKI Fluid overload or pre renal state Hyperkalemia Uremia : pericarditis, altered mental status Metabolic acidosis Distinction of Prerenal vs ATN Urinalysis. Fractional excretion of sodium and, to a lesser degree, the urine sodium concentration. Response to fluid repletion in patients who have evidence of volume depletion, which is the gold standard for the diagnosis prerenal disease. 2
3 Short-term outcomes The outcome of ATN is highly dependent on the severity of comorbid conditions. Uncomplicated ATN is associated with mortality rates of 7 to 23% Mortality of ATN in postoperative or critically ill patients with multisystem organ failure is high as 50 to 80%. Mortality rates increases with the number of failed organ systems Long-term outcomes Long-term outcomes of patients who survive are good. Of a population of 979 critically ill patients with ARF who required RRT (predominately patients with ATN), in-hospital mortality was 69%. Patients who survived to hospital discharge, 6-mo survival was 77%, 1-yr survival was 69%, and 5-yr survival was 50% 59% of surviving patients had no residual renal insufficiency, and only 10% required chronic dialysis therapy. Indications for RRT Pericarditis or pleuritis Progressive uremic encephalopathy or neuropathy (AMS, asterixis, myoclonus, seizures) Bleeding diathesis Fluid overload unresponsive to diuretics Metabolic disturbances refractory to medical therapy (hyperkalemia, metabolic acidosis, hyper- or hypocalcemia, hyperphosphatemia) Sepsis? Toxic overdose of a dialyzable drug 3
4 Goals of RRT Solute clearance Diffusive transport (based on countercurrent flow of blood and dialysate) Convective transport (solvent drag with ultrafiltration) Fluid removal Different modalities Peritoneal dialysis Intermittent hemodialysis Hemofiltration Continuous renal replacement therapy Hybrid methods like SLED Decision of modality determined by catabolic rate, hemodynamic stability, and whether primary goal is fluid or solute removal OUTCOMES : CRRT VS IHD Bellamo ET. AL. have found lower mortality in 24 ICU pt. with ARF treated with CAVHDF/CVVHDF vs IHD Pt. have median APACHE 2 score of Mortality was 49 % in CRRT vs 70 % in IHD. Limitations of study were CRRT was started earlier and patients have lower mean plasma urea. In comparison VAN Bomel Et.AL. have found no difference in mortality with CAVHDF VS IHD (57% VS 41% P=NS). But pt. in CRRT were more sicker. Mehta ET. AL have also found no difference and claims mortality is more associated with underlying disease than on renal failure. 4
5 Improved cardiovascular stability during CRRT therapy in critically ill patients with acute hepatic and renal failure In critically ill patients, in whom DO2(delivery of O2) is impaired, the use of continuous forms of renal replacement therapy is preferred for its improved cardiovascular tolerance compared with daily intermittent machine treatments. Davenport A Et. AL. Crit Care Med 1993 Mar;21(3): IHD VS CAVH/CAHD Thirty-two consecutive, critically ill, mechanically ventilated patients with combined acute hepatic and renal failure were randomized to treatment with either intermittent machine hemofiltration or (CAVH) or (CAVHD). During the first hour of treatment, there was a reduction in cardiac index of 15 +/- 2% during intermittent machine hemofiltration compared with no significant change during the continuous modes of treatment (CAVH/CAVHD) (3 +/- 3%; p <.05). Davenport A Et. AL. Crit Care Med 1993 Mar;21(3): IHD VS CAVH/CAHD This reduction in cardiac output during intermittent machine hemofiltration was associated with a maximum reduction in mean arterial pressure from 82 +/- 2 to 66 +/- 2 mm Hg (p <.001), a reduction in pulmonary artery occlusion pressure of 27 +/- 4%, tissue DO2 of 15 +/- 3%, and tissue oxygen uptake of 12 There was a maximum increase in intracranial pressure of 45 +/- 5% during the first hour of intermittent machine hemofiltration Davenport A Et. AL. Crit Care Med 1993 Mar;21(3):
6 Effect on Mortality CRRT VS INTERMITTENT HD Prospective study by Mehta Et.Al. 166 pt were randomized to intermittent HD VS CVVH in ICU. Principal outcome were ICU and in hosp. mortality, length of stay and recovery of renal function. Continues therapy were associated with an increase in ICU mortality (59.4%vs 41.5%p<0.002) and in hosp. mortality (65.5 % vs 47.6 % p<0.02) Mean ICU length was 16.5 days from time of nephrology consultation and recovery of renal functions was 34.9 and the did not show any difference. Higher APACHE 3 scores and OSF were associated with shorter length of stay secondary to increase mortality. MEHTA ET AL. CRRT VS IHD IN ARF KIDNEY INT. VOL CRRT VS INTERMITTENT HD CRRT was associated with high rates of renal recovery in surviving patients who received adequate trial of therapy with no cross over (92.3 vs 59.4). In addition patients who cross over from CRRT to IHD have higher rates of recovery than those who cross over from IHD to CRRT (15 pt cross over from IHD to CRRT and 17 cross over from CRRT to IHD). Cost of CRRT was $3946 vs $3077 for IHD. MEHTA ET AL. CRRT VS IHD IN ARF KIDNEY INT. VOL CRRT VS INTERMITTENT HD LOS was significantly reduced in patients using CRRT as initial therapy sec. to higher ICU mortality (CRRT 17.1 vs IHD 26.3 days P <0.001). CRRT resulted in lower solute level despite higher BUN levels at start of therapy Complete renal recovery was achieved more frequently in CRRT.This may be secondary to less hemodynamic insults,improved control of azotemia, clearance of middle molecule and reduction in pulmonary and myocardial and GI edema. MEHTA ET AL. CRRT VS IHD IN ARF KIDNEY INT. VOL

7 MEHTA ET AL. CRRT VS IHD IN ARF KIDNEY INT. VOL MEHTA ET AL. CRRT VS IHD IN ARF KIDNEY INT. VOL
8 Limitations Significant differences in groups in several covariates independently associated with mortality including gender, hepatic failure, APACHE II and III scores and number of failed organ systems in each instance biased in favor of intermittent HD. After adjustment of the imbalances in groups the odds of death with continuous therapy was 1.3, P=ns METHA ET. AL. RADOMIZED CLINICAL TRIAL OF CONTINUES VS INTERMITTENT HD IN ARF KIDNEY INT.2001 SEP ;60 (3): Limitations(Cont.) Study has limited statistical power as they assumed a mortality of 70% for control IHD patients. Mortality was infact %. The data showed an overall mortality of 50.6% considerably lower than % rates reported in most studies.this may be secondary to improved level of care of patients or patients with map <70mm were excluded. Mostly using CRRT in reality were excluded i.e. those with Map <70 mm. MEHTA ET AL. CRRT VS IHD IN ARF KIDNEY INT. VOL IHD VS CVVHD In ARF Paganini Et.Al. did a randomized controlled study of 80 critically ill patients with ARF. Pt were randomized after stratification by severity of illness to treatment with CVVHD or IHD. There was no sig. difference in survival or renal recovery. There were greater net volume removal in CVVHD. There were significant drop in mean BP for patients on IHD VS CVVHD but this did not lead to survival advantage. RANDOMIZED CONTROLLED TRIAL COMPARING IHD VS CVVHD IN ARF PAGNINI ET.AL. AJKD 2004 DEC.;44(6)

:875-85 VA Cooperative ATN study, 2008 Pavlesky, N Engl J Med.")
9 Systemic review : impact of dialytic modality on mortality Systemic review and meta-analysis of six eligible trials were done by Tonelli et.al., Univ. Of Alberta, Canada. He found no difference in relative risk of mortality and renal recovery associated with IHD vs CRRT. TONELLI M ET.AL. AJKD 2002 NOV;40 (5): VA Cooperative ATN study, 2008 Pavlesky, N Engl J Med July 3; 359(1):

10 VA cooperative ATN study, 2008 Pavlesky, N Engl J Med July 3; 359(1): Diagnosis and outcome of patients Treated with CRRT The most important factor contributing death was the underlying cause of ARF. Ultimate prognosis depends upon recovery of other organ systems not on ARF per se in patients with ARF and MOF. Lohr Et. Al. found that associated organ failure in the form of respiratory failure,gi dysfunction,chf,sepsis or hypotension were significantly associated with high mortality. Paganini Et.Al Seminar in nephrology vol 17 july Paganini Et.Al Seminar in nephrology vol 17 july

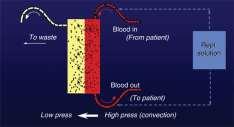
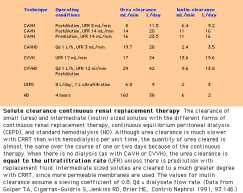
11 Choice of Dialytic Technique The choice of dialytic technique is dependent upon a variety of factors including availability, the expertise of the clinician, hemodynamic stability, and the degree to which solutes and/or fluid must be removed. Do what you know best Choice of Dialytic Technique: Rate of Solute Removal Solute removal occurs primarily by diffusion from the plasma into the dialysate during dialysis and, to a much lesser degree, by convection during ultrafiltration as solvent drag carries small and intermediate sized solutes with the water. Smaller solutes (such as urea and electrolytes) are removed in roughly the same concentration as the plasma with hemofiltration; as a result, the rate of solute clearance is equal to the ultrafiltration rate unless there is concurrent diffusive loss 11
12 Choice of Dialytic Technique: Rate of Solute Removal The rate of solute diffusion is determined by a number of factors including : The surface area and unit solute permeability of the dialysis membrane. The blood and dialysate flow rates which, if increased, maintain a maximum concentration gradient between these two compartments. The duration of dialysis. Choice of Dialytic Technique: Rate of Solute Removal In comparison, the rate of solute removal by ultrafiltration is influenced by: The transmembrane pressure gradient that provides the driving force for ultrafiltration. The surface area and unit water permeability of the dialysis membrane ultrafiltration. The duration of hemofiltration. The blood flow rate, which acts indirectly by moving nonfiltered plasma proteins away from the inner wall of the dialysis membrane; preventing local protein accumulation maintains water permeability. SLED The SLED/EDD technique offers every advantage of CRRT, but does not require any new equipment acquisition The 2008H hemodialysis machine can also be used. Thus, SLED/EDD is well suited for centers in which there is limited support for CRRT. The therapy can be applied to all patients in ARF requiring dialytic support who manifest intolerance to regular hemodialysis. 12
13 SLED Single center experience over 18 months since July 1998 with a hybrid technique named sustained low-efficiency dialysis (SLED), in which standard IHD equipment was used with reduced dialysate and blood flow rates. Sustained low-efficiency dialysis for critically ill patients requiring renal replacement therapy Marshall MR; Golper TA; Shaver MJ; Alam MG; Chatoth DK Kidney Int 2001 Aug;60(2): SLED (Cont.) Twelve-hour treatments were performed nocturnally, allowing unrestricted access to the patient for daytime procedures and tests. 145 SLED treatments were performed in 37 critically ill patients in whom IHD had failed or been withheld. Mean SLED treatment duration was 10.4 hours because 51 SLED treatments were prematurely discontinued sec. to hypotension or clotting. Marshall MR; Golper TA; Shaver MJ; Alam MG; Chatoth DK Sustained low-efficiency dialysis for critically ill patients requiring renal replacement therapy Kidney Int 2001 Aug;60(2): SLED (Cont.) Hemodynamic stability was maintained during most SLED treatments, allowing the achievement of prescribed ultrafiltration goals in most cases with an overall mean of only 240 ml per treatment. Mean delivered double-pool Kt/V of 1.36 per (completed) treatment. Observed hospital mortality was 62.2%, which was not significantly different from the expected mortality as determined from the APACHE II illness severity scoring system. CONCLUSIONS: SLED is a viable alternative to traditional continuous renal replacement therapies for critically ill patients in whom IHD has failed or been withheld. Marshall MR; Golper TA; Shaver MJ; Alam MG; Chatoth DK Sustained low-efficiency dialysis for critically ill patients requiring renal replacement therapy Kidney Int 2001 Aug;60(2):


14 Table 1 Studies of sustained low-efficiency dialysis and extended nocturnal dialysis for treatment of patients with renal failure in the intensive care unit Fliser D and Kielstein JT (2006) Technology Insight: treatment of renal failure in the intensive care unit with extended dialysis Nat Clin Pract Neprol 2: doi: /ncpneph0060 Slow continuous ultrafiltration SCUF is designed to remove up to 6 to 7 L of fluid per day without requiring replacement fluid other than for hyperalimentation. Solute removal is minimal with this technique, being limited by the low ultrafiltration rate and lack of dialysis. Clearance of urea and other small solutes is equal to the ultrafiltration rate of approximately 4 to 5 ml/min. Thus, SCUF is not useful in patients who are uremic or hyperkalemic. SCUF without pump 14
15 SCUF- pump assisted SCUF (Cont.) Either arteriovenous or venovenous access can be used for SCUF. Practical goals are a UFR of 5 ml/min and a Qb of 80 ml/min. If necessary, the UFR can be increased by raising Qb or by adding suction to the filtrate drainage system. The Qb can be raised by increasing the systemic blood pressure or by inserting an extracorporeal blood pump into the circuit ge system. If the UFR is too rapid, ultrafiltration can be slowed by raising the level of the bag into which the ultrafiltrate drains. 15
16 SCUF (Cont.) Low Cardiac out put in CHF activate Renin angiotensin and stimulate Sympathetic nervous system with resultant accumulation of sodium and increased peripheral resistance. Some pt. with advanced CHF will not respond to diuretics. UF intermittently or SCUF breaks this cycle. SCUF (Cont.) Agostine Et.AL.randomized 16 pt. with CHF (NY class II and III) to UF liters for 3-4 hours or lasix 60mg IV followed by 1mg per min for 2 hours. Both treatments produced similar diuresis 3 months later RA pressure,pcwp and body wt. return to baseline in lasix group and they were still low in UF group. Suggest fluid removed by UF shifts the abnormal set point for fluid balance to a more physiological level despite comparable levels of vol. control. Continuous venovenous hemofiltration CVVH is similar to CAVH, except that an extracorporeal blood pump is required that allows the physician to control the flow rates within the system. The blood pump assures a fast and stable Qb that can be set for example, at approximately 250 ml/min. If the hematocrit is 33 percent, then the plasma flow rate will be 167 ml/min. A filtration fraction of 10 percent in this setting results in a UFR of 16.7 ml/min, which is equal to 1 L/h or 24 L/day (four times greater than that with SCUF). 16
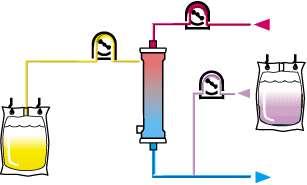
17 Replacement, Pre vs Post dilution CVVH with post-dilution 17

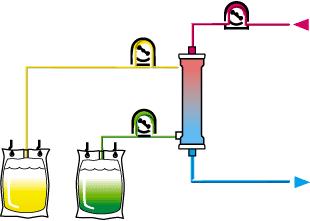
18 PRISMA CVVHDF 18



19 CVVHDF with post-dilution Macias WL Et.Al. Am J Kidney Dis 1991 Oct;18(4):451-8 CVVHDF using regional citrate anticoagulation. ERA EDTA 2003; all rights reserved Cointault O et al. Nephrol. Dial. Transplant. 2004;19:
 varies from 150 to 300 ml/min and the dialysate flow (Qd) from 1 to 2 L/hour Nx Stage machine Antibiotic dosing in critically ill adult")
20 Continuous venovenous hemodialysis CVVHD combines the processes of diffusive and convective clearances. It utilizes a blood pump to maximize the delivery of blood to the extracorporeal device. Under routine operating conditions, the blood flow (Qb) varies from 150 to 300 ml/min and the dialysate flow (Qd) from 1 to 2 L/hour Nx Stage machine Antibiotic dosing in critically ill adult patients receiving CRRT 2005 by the Infectious Diseases Society of America Trotman R L et al. Clin Infect Dis. 2005;41:
21 Conclusion To minimize morbidity, dialysis should generally be started prior to the onset of complications due to renal failure. Sometimes one can also initiate renal replacement therapy in patients in whom excessive volume resuscitation is required (such as hepatic failure), even in the absence of significant azotemia. This is particularly relevant in patients demonstrating hemodynamic instability where volume removal must be performed slowly. Conclusion The apparent advantage of biocompatible dialysis membranes has led to our using them routinely in patients with acute renal failure. More intense delivered doses of dialysis appears to principally benefit patients with acute renal failure and illnesses of intermediate severity. Patients at either extremes of illness (severely ill or not very ill) have much less survival benefit with intense intermittent hemodialysis regimens. 21
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
Who? Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011
 Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Decision making in acute dialysis
 Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Renal Replacement Therapy in Acute Renal Failure
 CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement
 Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Renal Replacement Therapy in ICU. Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine
 Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
RENAL FAILURE IN ICU. Jo-Ann Vosloo Department Critical Care SBAH
 RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
MODALITIES of Renal Replacement Therapy in AKI
 MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
- SLED Sustained Low-Efficiency Dialysis
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
ASN Board Review: Acute Renal Replacement Therapies
 ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
Continuous Renal Replacement Therapy. Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
CRRT: The Technical Questions Modality & Dose. Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018
 CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Recent advances in CRRT
 Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
Paul R. Bowlin, M.D. University of Colorado Denver. May 12 th, 2008
 Paul R. Bowlin, M.D. University of Colorado Denver May 12 th, 2008 Presentation Overview Background / Definitions History Indications for initiation of therapy Outcomes Studies Conclusions Questions Background
Paul R. Bowlin, M.D. University of Colorado Denver May 12 th, 2008 Presentation Overview Background / Definitions History Indications for initiation of therapy Outcomes Studies Conclusions Questions Background
UAB CRRT Primer Ashita Tolwani, MD, MSc University of Alabama at Birmingham
 UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Dialysis Dose Prescription and Delivery. William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012
 Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT for the Experience User 1. Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018
 CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done?
 Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done? Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta Disclosure Consulting: Alere, Baxter, Gambro,
Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done? Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta Disclosure Consulting: Alere, Baxter, Gambro,
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
CRRT. ICU Fellowship Training Radboudumc
 CRRT ICU Fellowship Training Radboudumc Timing RRT Consider the following: Underlying cause and reversibility. Rapid improvement unlikely with high dose vasopressors and continuous exposure to other risk
CRRT ICU Fellowship Training Radboudumc Timing RRT Consider the following: Underlying cause and reversibility. Rapid improvement unlikely with high dose vasopressors and continuous exposure to other risk
[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)
![[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)](/thumbs/92/109602349.jpg "[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)") [1] Levy [3] 183 174 (odds ratio) 5.5 Woodrow [1] 1956 1989 mannitol (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP) McCarthy [2] 1970 1990 insulin-like growth factor-1 (IGF-1) ANP 92
[1] Levy [3] 183 174 (odds ratio) 5.5 Woodrow [1] 1956 1989 mannitol (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP) McCarthy [2] 1970 1990 insulin-like growth factor-1 (IGF-1) ANP 92
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
UNDERSTANDING THE CRRT MACHINE
 UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Pediatric Continuous Renal Replacement Therapy
 Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
Renal replacement therapy in Pediatric Acute Kidney Injury
 Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Physiology of Blood Purification: Dialysis & Apheresis. Outline. Solute Removal Mechanisms in RRT
 Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
higher dose with progress in technical equipment. Continuous Dialysis: Dose and Antikoagulation. prescribed and delivered
 1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
Drug Use in Dialysis
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
(Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
Continuous renal replacement therapy. David Connor
 Continuous renal replacement therapy David Connor Overview Classification of AKI Indications Principles Types of CRRT Controversies RIFL criteria Stage GFR Criteria Urine Output Criteria Risk Baseline
Continuous renal replacement therapy David Connor Overview Classification of AKI Indications Principles Types of CRRT Controversies RIFL criteria Stage GFR Criteria Urine Output Criteria Risk Baseline
Continuous renal replacement therapy Gulzar Salman Amlani Aga Khan University, School of Nursing, Karachi.
 Special Communication Continuous renal replacement therapy Gulzar Salman Amlani Aga Khan University, School of Nursing, Karachi. Abstract Acute renal failure refers to sudden deterioration in biochemical
Special Communication Continuous renal replacement therapy Gulzar Salman Amlani Aga Khan University, School of Nursing, Karachi. Abstract Acute renal failure refers to sudden deterioration in biochemical
Renal replacement therapy in acute kidney injury
 6 February 2009 CONTENTS Renal replacement therapy in acute kidney injury S Jithoo Commentator: CL Quantock Moderator: LW Drummond INTRODUCTION... 3 WHAT IS RENAL REPLACEMENT THERAPY?... 3 MODES OF RENAL
6 February 2009 CONTENTS Renal replacement therapy in acute kidney injury S Jithoo Commentator: CL Quantock Moderator: LW Drummond INTRODUCTION... 3 WHAT IS RENAL REPLACEMENT THERAPY?... 3 MODES OF RENAL
Olistic Approach to Treatment Adequacy in AKI
 Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
CRRT. Sustained low efficiency daily dialysis, SLEDD. Sustained low efficiency daily diafiltration, SLEDD-f. inflammatory cytokine IL-1 IL-6 TNF-
 RRT, renal replacement therapy IHDCRRT CRRT 24 CRRT Sustained low efficiency daily dialysis, SLEDD 6 ~ 12 300 Sustained low efficiency daily diafiltration, SLEDD-f inflammatory cytokine IL-1 IL-6 TNF-
RRT, renal replacement therapy IHDCRRT CRRT 24 CRRT Sustained low efficiency daily dialysis, SLEDD 6 ~ 12 300 Sustained low efficiency daily diafiltration, SLEDD-f inflammatory cytokine IL-1 IL-6 TNF-
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialysis in the Acute Setting
 Dialysis in the Acute Setting medicine2.missouri.edu/jahm/dialysis-in-the-acute-setting/ October 8, 2015 Kunal Malhotra, MD Division of Nephrology, Department of Medicine, University of Missouri School
Dialysis in the Acute Setting medicine2.missouri.edu/jahm/dialysis-in-the-acute-setting/ October 8, 2015 Kunal Malhotra, MD Division of Nephrology, Department of Medicine, University of Missouri School
Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy
 Cedarville University DigitalCommons@Cedarville Pharmacy Faculty Presentations School of Pharmacy 2-23-2012 Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy Jeb Ballentine
Cedarville University DigitalCommons@Cedarville Pharmacy Faculty Presentations School of Pharmacy 2-23-2012 Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy Jeb Ballentine
Citrate Anticoagulation
 Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience
 Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience Casey N. Gashti, MD, Susana Salcedo, MD, Virginia Robinson, RN, and Roger A. Rodby, MD Background: Renal replacement therapies
Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience Casey N. Gashti, MD, Susana Salcedo, MD, Virginia Robinson, RN, and Roger A. Rodby, MD Background: Renal replacement therapies
Practical issues - dosing on extracorporeal circuits
 Practical issues - dosing on extracorporeal circuits Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
Practical issues - dosing on extracorporeal circuits Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen
 When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
Management of the patient with established AKI. Kelly Wright Lead Nurse for AKI King s College Hospital
 Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
Drug dosing in patients with acute kidney injury
 Drug dosing in patients with acute kidney injury They don t know what they are doing Jan Jan T. T. Kielstein Department of of Nephrology and and Hypertension Medical School School Hannover Drug dosing
Drug dosing in patients with acute kidney injury They don t know what they are doing Jan Jan T. T. Kielstein Department of of Nephrology and and Hypertension Medical School School Hannover Drug dosing
ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO
 ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland NO CONFLICT OF INTERESTS Important concept
ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland NO CONFLICT OF INTERESTS Important concept
Renal Physiology Intro to CRRT Concepts. Catherine Jones September 2017
 Renal Physiology Intro to CRRT Concepts Catherine Jones September 2017 Learning Outcomes To revise anatomy & physiology of kidney in health: To understand basic principles of continuous renal replacement
Renal Physiology Intro to CRRT Concepts Catherine Jones September 2017 Learning Outcomes To revise anatomy & physiology of kidney in health: To understand basic principles of continuous renal replacement
CRRT and Drug dosing. Karlee Johnston Lead Pharmacist Division of Critical Care ICU Education June 2017
 CRRT and Drug dosing Karlee Johnston Lead Pharmacist Division of Critical Care ICU Education June 2017 This talk In scope CRRT modalities with regard to medicine Principles of drugs with regard to dialysis
CRRT and Drug dosing Karlee Johnston Lead Pharmacist Division of Critical Care ICU Education June 2017 This talk In scope CRRT modalities with regard to medicine Principles of drugs with regard to dialysis
ACUTE KIDNEY INJURY. Stuart Linas U. Colorado SOM
 ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
Symposium. Principles of Renal Replacement Therapy in Critically ill children- Indian Perspective
 Symposium DOI- 10.21304/2018.0502.00376 in Critically ill children- Indian Perspective Sidharth Kumar Sethi *, Aliza Mittal**, Rupesh Raina***, Manindar Dhaliwal**** * Senior Consultant, Pediatric Nephrology
Symposium DOI- 10.21304/2018.0502.00376 in Critically ill children- Indian Perspective Sidharth Kumar Sethi *, Aliza Mittal**, Rupesh Raina***, Manindar Dhaliwal**** * Senior Consultant, Pediatric Nephrology
egfr 34 ml/min egfr 130 ml/min Am J Kidney Dis 2002;39(suppl 1):S17-S31
:S17-S31") Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Quantification and Dosing of Renal Replacement Therapy in Acute Kidney Injury: A Reappraisal
 In-Depth Review Blood Purif 2017;44:140 155 Received: January 12, 2017 Accepted: April 4, 2017 Published online: June 7, 2017 Quantification and Dosing of Renal Replacement Therapy in Acute Kidney Injury:
In-Depth Review Blood Purif 2017;44:140 155 Received: January 12, 2017 Accepted: April 4, 2017 Published online: June 7, 2017 Quantification and Dosing of Renal Replacement Therapy in Acute Kidney Injury:
Modes of Extracorporeal Therapies For ESRD Patients
 Modes of Extracorporeal Therapies For ESRD Patients Suhail, MD Extracorporeal Therapies: Dialytic Therapies Dialysis: Movement of molecules across a semipermeable membrane (Bi-directional) Movement of
Modes of Extracorporeal Therapies For ESRD Patients Suhail, MD Extracorporeal Therapies: Dialytic Therapies Dialysis: Movement of molecules across a semipermeable membrane (Bi-directional) Movement of
Renal Replacement Therapies in Kidney Disease
 ORIGINAL ARTICLE Sanjiv Mahajan* Chief Medical Officer, Department of Nephrology & Medicine, Safdarjung Hospital & Vardhman Mahavir Medical College, New Delhi, India ABSTRACT Renal replacement therapy
ORIGINAL ARTICLE Sanjiv Mahajan* Chief Medical Officer, Department of Nephrology & Medicine, Safdarjung Hospital & Vardhman Mahavir Medical College, New Delhi, India ABSTRACT Renal replacement therapy
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
HEMODIALFILTRATION LITERATURE REVIEW AND PRACTICE CONSIDERATIONS 1.0 PRACTICE CONSIDERATIONS 2.0 CURRENT LITERATURE REVIEW
 HEMODIALFILTRATION LITERATURE REVIEW AND PRACTICE CONSIDERATIONS This document was prepared at the request of the BC Hemodialysis Committee to provide a brief overview of the literature and to identify
HEMODIALFILTRATION LITERATURE REVIEW AND PRACTICE CONSIDERATIONS This document was prepared at the request of the BC Hemodialysis Committee to provide a brief overview of the literature and to identify
Nutrition in Acute Kidney Injury Enrico Fiaccadori
 Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
ACUTE KIDNEY INJURY IN THE INTENSIVE CARE UNIT
 & ACUTE KIDNEY INJURY IN THE INTENSIVE CARE UNIT Petar Kes*, Nikolina Bašić Jukić Department of Dialysis, University Hospital Centre Zagreb, Kišpatićeva 12, 10000 Zagreb, Croatia * Corresponding author
& ACUTE KIDNEY INJURY IN THE INTENSIVE CARE UNIT Petar Kes*, Nikolina Bašić Jukić Department of Dialysis, University Hospital Centre Zagreb, Kišpatićeva 12, 10000 Zagreb, Croatia * Corresponding author
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital
 Renal Dialysis Centre Hong Kong Sanatorium & Hospital") Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
Contrast Induced Nephropathy
 Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators
 oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators Heparin-grafted for reduced thrombogenicity Supports renal function POWERED
oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators Heparin-grafted for reduced thrombogenicity Supports renal function POWERED
Prof Patrick Honoré,MD, PhD,FCCM Intensivist-Nephrologist
 Pro-Con Debate on High Volume Hemofiltration :Burial or Ressurection? The Pro Position 1.-Why Moving From Dose To Membranes? 4.-AN69 Oxiris LPS Adsorptive Membranes in Sepsis 2.- High Cut-Off Membranes
Pro-Con Debate on High Volume Hemofiltration :Burial or Ressurection? The Pro Position 1.-Why Moving From Dose To Membranes? 4.-AN69 Oxiris LPS Adsorptive Membranes in Sepsis 2.- High Cut-Off Membranes
Large RCT s s in RRT : What can be learnt for nursing?
 Large RCT s s in RRT : What can be learnt for nursing? Ian Baldwin Dept. of Intensive Care, Austin Hospital Adjunct Professor, RMIT University CRRT 2011 Hilton Bayfront, February 22-25 SanDiego Key Hypothesis
Large RCT s s in RRT : What can be learnt for nursing? Ian Baldwin Dept. of Intensive Care, Austin Hospital Adjunct Professor, RMIT University CRRT 2011 Hilton Bayfront, February 22-25 SanDiego Key Hypothesis
Operational characteristics of continuous renal replacement modalities used for critically ill patients with acute kidney injury
 The International Journal of Artificial Organs / Vol. 31 / no. 6, 2008 / pp. 525-534 Review Operational characteristics of continuous renal replacement modalities used for critically ill patients with
The International Journal of Artificial Organs / Vol. 31 / no. 6, 2008 / pp. 525-534 Review Operational characteristics of continuous renal replacement modalities used for critically ill patients with
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
OBJECTVES OF LEARNING
 OBJECTVES OF LEARNING ACUTE RENAL FAILURE AND RENAL REPLACEMENT THERAPY DR.TAI CHENG SHENG RECOGNITION OF DEFINITION OF ARF RECOGNITION OF CAUSE OF ARF RECOGNITION OF PATHOGENESIS OF ARF RECOGNITION OF
OBJECTVES OF LEARNING ACUTE RENAL FAILURE AND RENAL REPLACEMENT THERAPY DR.TAI CHENG SHENG RECOGNITION OF DEFINITION OF ARF RECOGNITION OF CAUSE OF ARF RECOGNITION OF PATHOGENESIS OF ARF RECOGNITION OF
Ana Paula Bernardo. CHP Hospital de Santo António ICBAS/ Universidade do Porto
 Ana Paula Bernardo CHP Hospital de Santo António ICBAS/ Universidade do Porto Clinical relevance of hyperphosphatemia Phosphate handling in dialysis patients Phosphate kinetics in PD peritoneal phosphate
Ana Paula Bernardo CHP Hospital de Santo António ICBAS/ Universidade do Porto Clinical relevance of hyperphosphatemia Phosphate handling in dialysis patients Phosphate kinetics in PD peritoneal phosphate
Clinical Application of CRRT for Infants and Children
 Clinical Application of CRRT for Infants and Children Geoffrey Fleming Daryl Ingram Jordan Symons 22 nd International Conference on Advances in Critical Care Nephrology San Diego 2017 Introduction Pediatric
Clinical Application of CRRT for Infants and Children Geoffrey Fleming Daryl Ingram Jordan Symons 22 nd International Conference on Advances in Critical Care Nephrology San Diego 2017 Introduction Pediatric
Aquarius Study Day Adult Pre-Reading Study Pack
 Aquarius Study Day Adult Pre-Reading Study Pack An Introduction to CRRT (Continuous Renal Replacement Therapy) Name Date. Hospital.. Please take the opportunity to read this booklet prior to attending
Aquarius Study Day Adult Pre-Reading Study Pack An Introduction to CRRT (Continuous Renal Replacement Therapy) Name Date. Hospital.. Please take the opportunity to read this booklet prior to attending
Acute Kidney Injury Care in the Chronic Unit
 Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
Continuous Renal Replacement Therapy in Dogs and Cats
 Continuous Renal Replacement Therapy in Dogs and Cats Mark J. Acierno, MBA, DVM KEYWORDS Continuous renal replacement therapy CRRT Acute kidney injury Dialysis In the early 1900s, a young pharmacologist
Continuous Renal Replacement Therapy in Dogs and Cats Mark J. Acierno, MBA, DVM KEYWORDS Continuous renal replacement therapy CRRT Acute kidney injury Dialysis In the early 1900s, a young pharmacologist
Hemodialysis is a life-sustaining procedure for the treatment of
 The Dialysis Prescription and Urea Modeling Biff F. Palmer Hemodialysis is a life-sustaining procedure for the treatment of patients with end-stage renal disease. In acute renal failure the procedure provides
The Dialysis Prescription and Urea Modeling Biff F. Palmer Hemodialysis is a life-sustaining procedure for the treatment of patients with end-stage renal disease. In acute renal failure the procedure provides
C h a p t e r 3 2 Prevention and Management of Acute Renal Failure in Intensive Care Unit - An Overview
 C h a p t e r 3 2 Prevention and Management of Acute Renal Failure in Intensive Care Unit - An Overview MS Amaresan Emeritus Professor, MGR Medical University, Chennai Acute Renal Failure (ARF) is a common
C h a p t e r 3 2 Prevention and Management of Acute Renal Failure in Intensive Care Unit - An Overview MS Amaresan Emeritus Professor, MGR Medical University, Chennai Acute Renal Failure (ARF) is a common
CONTINUOUS RENAL REPLACEMENT THERAPY
 Acta clin Croat 2000; 39:99-116 Review CONTINUOUS RENAL REPLACEMENT THERAPY Petar Kes Department of Nephrology and Dialysis, Sestre milosrdnice University Hospital, Zagreb, Croatia SUMMARY - Acute renal
Acta clin Croat 2000; 39:99-116 Review CONTINUOUS RENAL REPLACEMENT THERAPY Petar Kes Department of Nephrology and Dialysis, Sestre milosrdnice University Hospital, Zagreb, Croatia SUMMARY - Acute renal
Renal Replacement Therapy
 Chapter 133 Renal Replacement Therapy Claudio Ronco, Zaccaria Ricci, and Stefano Romagnoli Introduction Despite recent advances in acute kidney injury (AKI) definition, diagnosis, and treatment, many aspects
Chapter 133 Renal Replacement Therapy Claudio Ronco, Zaccaria Ricci, and Stefano Romagnoli Introduction Despite recent advances in acute kidney injury (AKI) definition, diagnosis, and treatment, many aspects
7/17/2017 FSHP 2017 ANNUAL MEETING. Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy
 FSHP Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy Disclosure I do not have (nor does any immediate family member have) a vested interest in or affiliation
FSHP Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy Disclosure I do not have (nor does any immediate family member have) a vested interest in or affiliation
Renal Replacement Therapy - Indication and Follow up
 Renal Replacement Therapy - Indication and Follow up Prof Brigadier General Mamun Mostafi FCPS, FRCP Chief Physician Combined Military Hospital Dhaka Bangladesh Primary Functions of the Kidney Removal
Renal Replacement Therapy - Indication and Follow up Prof Brigadier General Mamun Mostafi FCPS, FRCP Chief Physician Combined Military Hospital Dhaka Bangladesh Primary Functions of the Kidney Removal
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
Acute renal failure ARF
 Acute renal failure ARF Definition ARF is a clinical syndrome characterized by an abrupt decline in GFR and the accumulation of nitrogenous waste (BUN & creatinine). The decrease in GFR occurs relatively
Acute renal failure ARF Definition ARF is a clinical syndrome characterized by an abrupt decline in GFR and the accumulation of nitrogenous waste (BUN & creatinine). The decrease in GFR occurs relatively
Continuous Renal Replacement Therapy (CRRT)
") ISPUB.COM The Internet Journal of Anesthesiology Volume 21 Number 1 Continuous Renal Replacement Therapy (CRRT) S Sarkar Citation S Sarkar. Continuous Renal Replacement Therapy (CRRT). The Internet Journal
ISPUB.COM The Internet Journal of Anesthesiology Volume 21 Number 1 Continuous Renal Replacement Therapy (CRRT) S Sarkar Citation S Sarkar. Continuous Renal Replacement Therapy (CRRT). The Internet Journal
ESPEN Congress Vienna Nutritional implications of renal replacement therapy in ICU Nutritional support - how much nitrogen? W.
 ESPEN Congress Vienna 2009 Nutritional implications of renal replacement therapy in ICU Nutritional support - how much nitrogen? W. Druml (Austria) Nutritional Implications of Renal Replacement Therapy
ESPEN Congress Vienna 2009 Nutritional implications of renal replacement therapy in ICU Nutritional support - how much nitrogen? W. Druml (Austria) Nutritional Implications of Renal Replacement Therapy
Solute clearances during continuous venovenous haemofiltration at various ultrafiltration flow rates using Multiflow-100 and HF1000 filters
 Nephrol Dial Transplant (2003) 18: 961 966 DOI: 10.1093/ndt/gfg055 Original Article Solute clearances during continuous venovenous haemofiltration at various ultrafiltration flow rates using Multiflow-100
Nephrol Dial Transplant (2003) 18: 961 966 DOI: 10.1093/ndt/gfg055 Original Article Solute clearances during continuous venovenous haemofiltration at various ultrafiltration flow rates using Multiflow-100
Session 1: Circuit, Anticoagulation and Monitoring. Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019
 Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Cardiorenal Syndrome: What the Clinician Needs to Know. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Cardiorenal Syndrome: What the Clinician Needs to Know William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Renal Hemodynamics in Heart Failure Glomerular
Cardiorenal Syndrome: What the Clinician Needs to Know William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Renal Hemodynamics in Heart Failure Glomerular
When to start a renal replacement therapy in acute kidney injury (AKI) patients: many irons in the fire
 patients: many irons in the fire") Editorial Page 1 of 4 When to start a renal replacement therapy in acute kidney injury (AKI) patients: many irons in the fire Stefano Romagnoli 1,2, Zaccaria Ricci 3 1 Department of Anesthesia and Critical
Editorial Page 1 of 4 When to start a renal replacement therapy in acute kidney injury (AKI) patients: many irons in the fire Stefano Romagnoli 1,2, Zaccaria Ricci 3 1 Department of Anesthesia and Critical
DOSE DIALITICA E OUTCOME: UN PROBLEMA ANCORA APERTO
 DOSE DIALITICA E OUTCOME: UN PROBLEMA ANCORA APERTO Angelo F. Perego Nefrologia e Dialisi Ospedale Vittorio Emanuele III Monselice (PD) ULSS 17 Veneto GDS SIN TRATTAMENTI DEPURATIVI IN AREA CRITICA STAMPA
DOSE DIALITICA E OUTCOME: UN PROBLEMA ANCORA APERTO Angelo F. Perego Nefrologia e Dialisi Ospedale Vittorio Emanuele III Monselice (PD) ULSS 17 Veneto GDS SIN TRATTAMENTI DEPURATIVI IN AREA CRITICA STAMPA
Management of Acute Kidney Injury in the Neonate. Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital
 Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing