Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University
|
|
|
- Elijah Norton
- 5 years ago
- Views:
Transcription
1 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University
2 COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB

 Kearney PM, et al.")
3 Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult population had hypertension Prevalence of Hypertension by World Region By year 2025, 1.56 billion (29%) are projected to have hypertension Most of the expected increase will be in economically developing regions Number of People With Hypertension (millions) Kearney PM, et al. Lancet. 2005;365:
4 Blood Pressure Classification BP Classification SBP mmhg DBP mmhg Normal <120 and <80 Prehypertension or Stage 1 Hypertension or Stage 2 Hypertension >160 or >100
5 Algorithm for Treatment of Hypertension Lifestyle Modifications Not at Goal Blood Pressure (<140/90 mmhg) (<130/80 mmhg for those with diabetes or chronic kidney disease) Initial Drug Choices Without Compelling Indications With Compelling Indications Stage 1 Hypertension (SBP or DBP mmhg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Stage 2 Hypertension (SBP >160 or DBP >100 mmhg) 2-drug combination for most (usually thiazide-type diuretic and ACEI, or ARB, or BB, or CCB) Drug(s) for the compelling indications Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. Not at Goal Blood Pressure Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with hypertension specialist.

6 Definition of Resistant Hypertension Uncontrolled Hypertension Includes all patients who lack BP control on treatment, including those on inadequate treatment regimens, those with poor adherence, those with undetected secondary hypertension, as well as those with true treatment resistance 1 Uncontrolled Hypertension Resistant Hypertension Resistant Hypertension BP that remains above goal in spite of compliance with full doses of 3 antihypertensive medications of different classes; ideally, 1 of the 3 agents should be a diuretic 1 The treatment plan must include attention to lifestyle measures 2 Includes those patients who achieve BP control but require 4 antihypertensive agents to do so 1 1. Calhoun DA, et al. Circulation. 2008;117:e510-e Mancia G, et al. Eur Heart J. 2007;28:

7 Resistant Hypertension Causes of Pseudoresistant Hypertension 1,2 Suboptimal dosing of antihypertensive agents White coat effect Suboptimal BP measurement technique Physician inertia Lifestyle factors Medications that interfere with BP control Pseudoresistance caused by poor adherence to prescribed medication 1. Calhoun DA, et al. Circulation. 2008;117;e510-e Makris A, et al. Int J Hypertens. 2011;doi: /2011/ Papademetriou V, et al. Int J Hypertens. 2011;doi: /2011/ Secondary Causes of Hypertension 1,2 Obstructive sleep apnea Primary aldosteronism Renal artery stenosis However, a majority of patients with resistant hypertension and no identifiable secondary causes have an activated sympathetic nervous system and increased sympathetic outflow 3 Caution: The Symplicity Renal Denervation System is an Investigational Device. Limited by U.S. law to investigational use.
8 Consequences of Resistant Hypertension Patients with resistant hypertension have approximately 3-fold increased risk for CV events compared with that of patients with controlled hypertension 1 No longitudinal study has specially evaluated the prognosis of resistant hypertension 1 The degree to which CV risk is reduced with treatment is unknown, however the benefits of successful treatment are likely substantial 2 DBP = diastolic blood pressure. 1. Doumas M, et al. Int J Hypertens. 2011;doi: 4061/2011/ Calhoun DA, et al. Circulation. 2008;117:e510-e526.
9 Causes of Resistant Hypertension Improper BP measurement Excess sodium intake Inadequate diuretic therapy Medication Inadequate doses Drug actions and interactions (e.g., nonsteroidal anti-inflammatory drugs (NSAIDs), illicit drugs, sympathomimetics, oral contraceptives) Over-the-counter (OTC) drugs and herbal supplements Excess alcohol intake Identifiable causes of HTN





10 Renal Nerves and the SNS Efferent Sympathetics Afferent Renal Sympathetics Sympathetic signals from the CNS modulate the physiology of the kidneys The kidney is a source of central sympathetic activity, sending signals to the CNS Adapted from Schlaich MP, et al. Hypertension. 2009;54:


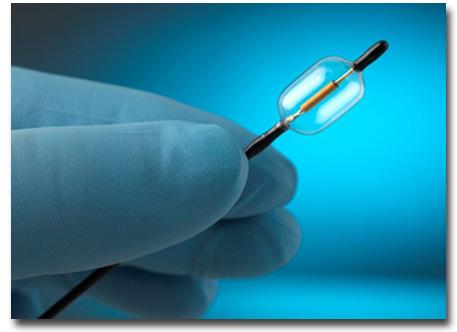
11 Renal Nerve Anatomy Allows a Catheter-Based Approach Standard interventional technique 4-6 two-minute treatments per artery Caution: The Symplicity Renal Denervation System is an Investigational Device. Limited by U.S. law to investigational use. 12
 Continuously monitors temperature and impedance Automatically shuts off")

12 Symplicity Investigational Catheter Device Generator will automatically control RF energy delivery: Power automatically ramped and maintained (5-8W) Continuously monitors temperature and impedance Automatically shuts off after 2 min or when either impedance or temperature exceed program limits 5mm Flexible Tip (self-orienting) 12mm Deflectable Shaft Caution: The Symplicity Renal Denervation System is an Investigational Device. Limited by U.S. law to investigational use.
13


14 St. Jude EnligHTN Boston Scientific/Vessix V2 Covidien OneShot ReCor Paradise

 and adventitial")
15 Six Month Post-Procedure Histology (Porcine Model) Movat s Pentachrome Stain An area of medial injury (yellow) is located between the arrows on the left. An enlargement of the boxed region is shown on the right Findings: minimal intimal thickening and minimal internal elastic lamina injury overlying areas of mild full thickness medial fibrosis (yellow [fibrosis] with green [proteoglycan deposition]) and adventitial fibrosis (yellow) Reproduced with permission from Rippy MK, et. al. Clin Res Cardiol. 2011;doi:101007s

16 Six Month Post-Procedure Nerve Histology (Porcine Model) H&E Nerve from untreated vessel: Periarterial nerve bundle surrounded by a thin fibrous connective tissue sheath (perineurium) Nerve from treated vessel: Periarterial nerve bundle has a hypercellular appearance and the perineurium has a thickened and fibrotic appearance. Nerve from Untreated Vessel Nerve from Treated Vessel Reproduced with permission from Rippy MK, et. al. Clin Res Cardiol. 2011;doi:101007s
17 Symplicity Staged Evaluation in Hypertension and Beyond First-in-Man 1 Symplicity HTN-1 2 Series of Pilot Studies Symplicity HTN-2 3 EU/AU Randomized Clinical Trial USA Symplicity HTN-3 4 US Randomized Clinical Trial Sources: 1. Krum H, et al. Lancet. 2009;373: Symplicity HTN-1 Investigators. Hypertension. 2011;57: GLOBAL Registry EU/AU Other Areas of Research: 4 Insulin Resistance, HF/Cardiorenal, Sleep Apnea, More 3. Symplicity HTN-2 Investigators. Lancet. 2010;376: Data on file, Medtronic.
18 The Symplicity HTN-1 Trial: Overview Design Multicenter (19 sites in Europe, Australia, and the United States), nonrandomized, open-label, proof-of-concept study Population 153 patients with treatment-resistant hypertension Treatment Endovascular catheter-based RDN using the Symplicity Renal Denervation System plus baseline antihypertensive medications Duration 36 months (assessments at 1, 3, 6, 12, 18, 24, and 36 months) Outcome Measures Primary efficacy measure: change in office BP Primary safety measures: based on physical examination, basic blood chemistries, and anatomic assessment of renal vasculature Source: Symplicity HTN-1 Investigators. Hypertension. 2011;57:
19 Symplicity HTN-1 Trial: Key Inclusion/Exclusion Criteria * Inclusion Criteria >18 years of age Elevated office systolic blood pressure (SBP) 160 mm Hg 3 antihypertensive medications (including 1 diuretic) Exclusion Criteria Estimated glomerular filtration rate (egfr) <45 ml/min/1.73m 2 Type 1 diabetes mellitus Known secondary cause of hypertension other than sleep apnea or chronic kidney disease Significant renovascular abnormalities * Inclusion/exclusion criteria in the trial settings were stringent and conservative in order to ensure a homogenous population in clinical practice, individual patient characteristics and physician judgment should guide patient selection Source: Symplicity HTN-1 Investigators. Hypertension. 2011;57:
20 BP change (mmhg) Symplicity HTN-1 Trial Change in Office BP Through 36 Months SBP mmhg Schlaich M, TCT 2012 P<0.01 for from BL for all time points 1 mo (n=143) 3 mo (n=148) 6 mo (n=144) 12 mo (n=132) 24 mo (n=105) Reported as mean with 95% confidence intervals *Number of patients represents data available at time of data-lock 30 mo (n=44) 36 mo (n=34)*
21 % Patients 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Schlaich M, TCT 2012 SYMPLICITY HTN-1 Distribution of SBP Change at Baseline, 1, 12, 24, and 36 Months Baseline 1 mo 12 mo 24 mo 36 mo (n=150) (n=143) (n=132) (n=105) (n=34)* *Number of patients represents data available at time of data-lock 180 mmhg mmhg mmhg < 140 mmhg
22 Conclusions The magnitude of clinical response is significant compared to baseline and sustained through 36 months Average number of medications were similar at each time point Increasing responder rates indicate: Some subjects respond late to RDN No loss of treatment effect out to 36 months The treatment effect was consistent across subgroups (age, diabetes status, and baseline renal function) Observed significant decrease in pulse pressure through 36 months No late adverse events related to RDN were reported through 36 months Schlaich M, TCT 2012 Analysis includes data on patients available through 36 months
23 Symplicity HTN-2 Trial Overview Design Multicenter (24 sites in Europe, Australia, and New Zealand), prospective, randomized, controlled study Population 106 patients with treatment-resistant hypertension Treatment Intervention group (endovascular catheter-based RDN with the Symplicity Renal Denervation System plus baseline antihypertensive medications) Control group (baseline antihypertensive medications alone) Duration 6 months (for the primary endpoint) with follow-up to 3 years Outcome Measures Primary endpoint: between-group changes in average office SBP from baseline to 6 months Secondary endpoints: acute and chronic procedural safety, a composite cardiovascular endpoint, occurrence of 10 mm Hg SBP reductions, achievement of target SBP, change in 24-hour ambulatory BP, and change in home BP Symplicity HTN-2 Investigators. Lancet. 2010;376:
24 Symplicity HTN-2 Trial Key Inclusion/Exclusion Criteria * Inclusion Criteria years of age Elevated office SBP 160 mm Hg (or 150 mm Hg for type 1 diabetics) Documented compliance with 3 antihypertensive medications Exclusion Criteria egfr <45 ml/min/1.73m 2 Type 1 diabetes mellitus Contraindications to MRI Substantial stenotic valvular heart disease Pregnancy or planned pregnancy during the study Myocardial infarction, unstable angina, or cerebrovascular accident in previous 6 mo Hemodynamically or anatomically significant renal artery abnormalities or prior renal artery intervention * Inclusion/exclusion criteria in the trial settings were stringent and conservative in order to ensure a homogenous population in clinical practice, individual patient characteristics and physician judgment should guide patient selection. Symplicity HTN-2 Investigators. Lancet. 2010;376:
25 Symplicity HTN-2 Trial: 1-, 3-, and 6-Month Office BP Reduction * Mean Office BP Change (mm Hg) SBP DBP -50 Symplicity RDN Group Control Group Symplicity RDN Group Control Group Symplicity RDN Group Control Group 1M 3M 6M (Primary Endpoint) * P for changes in SBP and DBP at all time points between Symplicity RDN and control groups; error bars represent 95% CIs. Symplicity HTN-2 Investigators. Lancet. 2010;376:

26 Symplicity HTN-2 Trial: Distribution of Office SBP at 6 Months 1,2 1. Data on file, Medtronic. 2. Symplicity HTN-2 Investigators. Lancet. 2010;376:
27 Change in Office Blood Pressure through 30-Months Post-Procedure* Initial RDN Group Crossover Group SBP DBP SBP DBP Esler M, ASH m 12m 24m 30m -30 P<0.01 at all time points for both groups m 12m 18m 24m n=49 n=47 n=43 n=37 n=35 n=33 n=31 n=26 *Only 7 patients in the Crossover group had available BP data at time of 30m data lock
28 SBP Response Rate Through 30 Months Represents Pooled Data 100% 80% 75% 63% 60% 10 mm Hg 20 mm Hg 84% 77% 80% 68% 70% 71% 64% 53% 40% 20% 0% 6 Months Post 12 Months 18 Months 24 Months 30 Months Procedure Post Procedure Post Procedure Post Procedure Post Procedure n=84 n=80 n=74 n=66 n=44 Esler M, ASH 2013
29 BP Medication Changes Post-Procedure 6 M (n=76) 12 M (n=76) 18 M (n=74) 24 M (n=64) 30 M (n=42) 0% 20% 40% 60% 80% 100% # Med or Dose No Change # Med or Dose Physicians were encouraged to maintain medications and dosages up to the 6-month primary endpoint. Increase: if any or both meds and/or dose increase, Decrease: if any or both meds and/or dose decrease. Values may not total to 100% due to indeterminate modifications, e.g., combination of med/dose increase and decrease. Esler M, ASH 2013
30 Symplicity HTN-2 Trial: Short-Term Procedure Safety No serious device- or procedure-related adverse events Minor complications in 5 of 52 patients: 1 access-site complication (femoral artery pseudoaneurysm); treated with manual compression 1 post-procedural drop in BP 1 urinary tract infection 1 extended hospital admission for assessment of parasthesias 1 case of back pain; treated with pain medication and resolved after 1 month Symplicity HTN-2 Investigators. Lancet. 2010;376:
31 Symplicity HTN-2 Trial: Chronic Safety 43 RDN patients underwent CTA, MRA, or duplex evaluation at 6 months No new vascular abnormalities or stenoses at any site of RF delivery 1 possible progression of a pre-existing stenosis unrelated to RF treatment; no further therapy warranted Serious adverse events at 6 months requiring hospital admission: Composite Cardiovascular Events Hypertensive event unrelated to non-adherence to medication Symplicity RDN Group (n=49) Control Group (n=51) 3 2 Other cardiovascular events 0 0 Other Serious Adverse Events Transient ischemic attack 1 2 Hypertensive crisis after abruptly stopping clonidine 1 0 Hypotensive episode resulting in reduction of medications 1 0 Coronery stent for angina 1 1 Temporary nausea/edema 1 0 Symplicity HTN-2 Investigators. Lancet. 2010;376:

32 Global SYMPLICITY Registry: Real-World Clinical Outcomes Worldwide evaluation of the safety and efficacy of treatment with the Symplicity renal denervation system in real world uncontrolled hypertensive patients Consecutive patients treated in real world population ~ 5000 patients GREAT Registry N=1000 Korea Registry* N=102 South Africa Registry* N=400 Canada and Mexico* Rest of GSR N~3500 ~ 200 Global Sites Minimum 10% randomly assigned to 100% monitoring 30% monitoring to date Follow-up schedule 3mo 6mo 1yr 2yr 3yr 4yr 5yr Mahfoud F, EuroPCR 2013
33 Baseline Patient Characteristics (n=617) Mahfoud F, EuroPCR 2013 * 617 patients treated as of January 11, 2013 Demographics Age (years) 60 ± 13 Gender (% male) 63% Race (% caucasian) 87.5% BMI 30 ± 5.6 Co-Morbidities Diabetes Mellitus II (%) 38% Cardiac Disease (%) 49% egfr (ml/min/1.73 m 2 ) n= ± 53.1 Serum Creatinine (mg/dl) n= ± 1.7 egfr > 45 ml/min/1.73 m 2 97% Blood Pressure Baseline BP (mm Hg) 164/89 ± 23/16 Number of anti-htn medication classes (mean) 4.35 ± 1.34 Diuretic (%) 77% Aldosterone blocker (%) 19% ACE (%) 33% ARB (%) 67% Beta-Blocker (%) 79% Calcium Channel Blocker (%) 74% Alpha-adrenergic blocker (%) 34% Vasodilator (%) 14%
34 Population Characteristics 617 patients treated as of January 11, % with SBP 140 mm Hg Approx 60% of patients treated according to ESC Consensus paper on Renal Denervation 1 SBP 160 mm Hg ( 150 mm Hg Diabetes II), 3+ meds, including diuretic 22% with SBP 180 mm Hg Co-morbidities include Diabetes II 38.2% Renal Disease 30.1% Sleep Apnea 16.3% Hx of Cardiac Disease 49% Heart Failure 9.3% Atrial Fibrillation 11.9% 1 Mahfoud F et al. Expert consensus document from the European Society of Cardiology on catheter-based renal denervation, Eur Heart J April 2013 Mahfoud F, EuroPCR 2013
35 Procedure Detail and Safety Varied Patient Anatomies 98% anatomically eligible Average number renal arteries: 2.16 Mean length of renal artery: 43 +/- 14 mm Mean diameter of artery: 5.7 +/- 1.2 mm Procedure (n=617) 9% incidence of spasm 2 patients with vascular complications Pseudoaneurysm/hematoma No serious adverse events related to delivering RF to the renal artery with the Symplicity Flex catheter Post-Procedure through 6M* No new vascular abnormalities 2 hypertensive crises 1 death deemed unrelated to device or procedure 1 new onset of end-stage renal disease due to nephrotoxic overdose 2 MI *Data collected on all patients who reached either 3 or 6 month follow up Mahfoud F, EuroPCR 2013
36 5 Change in Office BP According to Baseline Measurement 3 Months 6 Months -5 BP change (mmhg) SBP DBP /150* /150* 180 n=274 n=220 n=36 n=135 n=114 n=17 * 150 mm Hg in Type II Diabetes P<.0001 for all values compared to baseline except: Mahfoud F, EuroPCR 2013 p= (SBP 180 mm Hg, 6 mo) p= (DBP 180 mm Hg, 6 mo)
37 Change in ABPM According to Baseline Measurement 0 3 Months 6 Months P <.0001 P=.0020 P <.0001 P=.0021 P=.0195 P=.0619 P <.0001 P=.0183 P <.0001 P=.0256 P=.0156 P= BP change (mmhg) SBP DBP /150* n=104 n=76 * 150 mm Hg in Type II Diabetes n= n=34 160/150* n= n=5 Mahfoud F, EuroPCR 2013
38 Conclusions Preliminary data demonstrated excellent procedural and clinical safety profile of renal denervation in a real world population Majority of patients treated resembled current consensus statements Early look at clinical data showed RDN had a significant reduction in both Office and Ambulatory BP compared to baseline Enrolment and analyses continue to meet goal of establishing procedure safety and efficacy of the Symplicity Flex catheter Mahfoud F, EuroPCR 2013
39 Design Symplicity HTN-3: Overview Multicenter (90 sites in the United States), prospective, randomized, blinded, controlled study Population 530 patients with treatment-resistant hypertension Treatment Treatment group (endovascular catheter-based RDN with the Symplicity Renal Denervation System plus baseline antihypertensive medications) Control group (sham procedure * plus baseline antihypertensive medications) Primary Outcome Measures Change in office SBP from baseline to 6 months Safety * The renal angiogram also acts as the sham procedure for patients in the control group. Data on file, Medtronic.
40 Symplicity HTN-3 Trial: Study Design Office SBP? 160 mmhg Full doses of? 3 meds Initial past 2 wks Screening No plan to change meds for 6 M Initial Screening 2 weeks Home BP & Med Diary Confirmatory Screening ABPM Treatment Renal Angiogram Control 1M 3M 1M 3M 2 weeks Home BP & Med Confirmation 2 weeks 6M Primary Endpoint Home BP & Med Confirmation 6M 12-36M Patient and Research staff assessing BP are blinded to treatment status No changes in medications for 6M 41
41 Symplicity HTN-3 Trial: Exclusion Criteria Hemodynamically or anatomically significant renal artery abnormalities or stenosis (>50%) or prior renal artery intervention egfr < 45 ml/min/1.73m 2 (MDRD formula) In-patient hospitalization for HTN Crisis in past year 24 hour average ABPM SBP <135mm/Hg Type 1 diabetes mellitus Symptomatic orthostatic hypotension in past year Stenotic valvular heart disease for which BP would be hazardous MI, unstable angina, or CVA in the prior 6 months Planned surgery or CV intervention within the next 6 months Known primary pulmonary HTN Known pheochromocytoma, Cushing's disease, coarctation of the aorta, hyperthyroidism or hyperparathyroidism Known alcohol or drug abuse
42 Symplicity HTN-3: Summary Office SBP >160mmHg 3 antihypertensive medications (one must be a diuretic) On stable, 3 full tolerated dose antihypertensive medication regimen for at least 2 weeks No significant renal insufficiency (egfr < 45 ml/min) Meets inclusion/exclusion criteria by general medical review No known renal artery anatomy exclusion (i.e. dual renal arteries, known RA stenosis >50%) Until 6 month primary endpoint: Patients must remain blinded No changes in medication unless medically necessary After 6 mo endpoint, control patients can crossover if still meet all initial criteria
43 Summary We can do a better job with HTN recognition and management Data for renal denervation thus far is very positive Renal denervation is coming (already approved in Europe) for refractory/resistant HTN


44 Questions?
Treating Hypertension With a Catheter..Wait What? COI 5/3/2013. Worldwide Prevalence of Hypertension Is Increasing
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Renal Denervation for Resistant Hypertension
 Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Devices and Long-Term Outcomes of Renal Denervation for Hypertension
 18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
Renal Artery Denervation New Concepts in Hypertension Treatment
 Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Percutaneous Renal Denervation: A New Promise in the Treatment of RHT?
 BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension
 Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Catheter-Based Renal Denervation (RDN)
") Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Byeong-Keuk Kim, MD, PhD. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
What We've Learned from Simplicity HTN-1,2, and Registries
 ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Christopher Valentine, MD
 Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension
 EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Management of Resistant Hypertension in Diabetes
 Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension
 Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Renal Denervation For Hypertension: Status Update
 Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Stephen G. Worthley 1, Gerard T. Wilkins 2, Mark W. Webster 3,Joseph K. Montarello 1, Paul T. Antonis 4, Robert J. Whitbourn 5, Roderic J.
 Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Renal denervation: Current evidence and remaining uncertainties
 Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension
 The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
Renal Sympathetic Denervation for HTN
 Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
The Future of Renal Denervation
 The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης
 Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
MINNEAPOLIS September 12, 2012 Medtronic, Inc. (NYSE: MDT) today announced findings
 today announced findings") NEWS RELEASE Contacts: Wendy Dougherty Jeff Warren Public Relations Investor Relations 707-541-3004 763-505-2696 FOR IMMEDIATE RELEASE HEALTH-ECONOMIC ANALYSIS SUGGESTS MEDTRONIC SYMPLICITY RENAL DENERVATION
NEWS RELEASE Contacts: Wendy Dougherty Jeff Warren Public Relations Investor Relations 707-541-3004 763-505-2696 FOR IMMEDIATE RELEASE HEALTH-ECONOMIC ANALYSIS SUGGESTS MEDTRONIC SYMPLICITY RENAL DENERVATION
Renal Denervation: The Case for Cardiology
 Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION
 CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Transcatheter Renal Denervation and Hong Kong Experience
 Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Layered Approaches to Studying Drug Responses
 Layered Approaches to Studying Drug Responses Brian B Hoffman, MD Chief of Medicine VA Boston Health Care System Professor of Medicine Harvard Medical School Conflict of Interest: US Federal Grant Funding
Layered Approaches to Studying Drug Responses Brian B Hoffman, MD Chief of Medicine VA Boston Health Care System Professor of Medicine Harvard Medical School Conflict of Interest: US Federal Grant Funding
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Update on renal denervation: Latest data
 LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction?
 Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
With an unrestricted educational grant from. The Interventional Treatment of Resistant Hypertension
 With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
Φαρµακευτική θεραπεία υπερτασικών ασθενών. Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική
 Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
SPYRAL HTN ON MED. Disclosure
 Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1
 Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study
 Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial
 Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial Prof Murray Esler Baker IDI Heart and Diabetes Institute, Melbourne
Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial Prof Murray Esler Baker IDI Heart and Diabetes Institute, Melbourne
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich,
 The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Director of the Israeli Institute for Quality in Medicine Israeli Medical Association July 1st, 2016
 The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Preliminary Results of RETREAT
 LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL
 CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
How to Manage Resistant Hypertension Min Su Hyon, MD
 How to Manage Resistant Hypertension Min Su Hyon, MD Cardiovascular Medicine, Internal Medicine Soonchunhyang University College of Medicine Definition Resistant to conventional medical therapy Definition
How to Manage Resistant Hypertension Min Su Hyon, MD Cardiovascular Medicine, Internal Medicine Soonchunhyang University College of Medicine Definition Resistant to conventional medical therapy Definition
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Catheter Based Denervation for Heart Failure
 Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
MP Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension
 Medical Policy Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension BCBSA Ref. Policy: 7.01.136 Last Review: 09/19/2018 Effective Date: 09/19/2018 Section:
Medical Policy Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension BCBSA Ref. Policy: 7.01.136 Last Review: 09/19/2018 Effective Date: 09/19/2018 Section:
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student