Transcatheter Renal Denervation and Hong Kong Experience
|
|
|
- Clarence Norman
- 5 years ago
- Views:
Transcription
1 Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart Diseases 1
2 A Major Public Health Burden Astonishing prevalence 1 in 3 adults 1 B people worldwide 1.6 B by 2025 Single largest contributor to death Dramatically increases risk of heart attack, stroke, heart failure, kidney failure & insulin resistance 2

 = Potentially a")
3 Drugs Work, But Not as Well as We Hope 30% Untreated 35% Treated but Uncontrolled Current approach failing Physician inertia Patient compliance Resistant HTN 35% Treated & Controlled Renal Denervation (RDN) = Potentially a compliance-independent therapy 3









4 Renal Sympathetic Connection Role of kidneys & sympathetic nervous system in development & progression of HTN is well established Pharmaceuticals modify physiology at intermediate steps in pathway RDN attempts to break the cycle at its source 4

5 Renal Sympathetic Nerve Activity: Kidney as Origin & Recipient of Central Sympathetic Drive Vasoconstriction Contractility Heart rate Efferent Nerves Afferent Nerves Blood Pressure Renin Release RAAS activation Sodium Retention Renal Blood Flow Schlaich et al. Hypertension. 2009;54(6):
6 Renal Sympathetic Nerve Activity: Kidney as Origin & Recipient of Central Sympathetic Drive Vasoconstriction Atherosclerosis Efferent Nerves Afferent Nerves Contractility Heart rate Hypertrophy Arrhythmia Heart Failure Blood Pressure + Increase co-morbidities Renin Release RAAS activation Sodium Retention Renal Blood Flow Kidney function Schlaich et al. Hypertension. 2009;54(6):
7 Renal Sympathetic Nerve Activity: RDN Disrupts Renal Nerves, Lowering SNS Activity Vasoconstriction Atherosclerosis Efferent Nerves Afferent Nerves -- Renal Denervation (RDN)-- Contractility Heart rate Hypertrophy Arrhythmia Heart Failure Blood Pressure - Decrease co-morbidities + Increase co-morbidities Renin Release RAAS activation Sodium Retention Renal Blood Flow Kidney function Schlaich et al. Hypertension. 2009;54(6):
8 VALIDATION OF PHYSIOLOGY


9 Proof of Principle Central Sympathetic Nerve Activity Muscle Sympathetic Nerve Activity (MSNA) Renal Sympathetic Nerve Activity Norepinephrine Spillover
10 Reduction of Renal Contribution to Central Sympathetic Drive: MSNA in Resistant Hypertension Patient * 59 year old male on 7 HTN meds MSNA (burst/min) BP (mmhg) Baseline /107 1 mo 41 (-27%) 141/90 (-20/-17) 12 mo 19 (-66%) 127/81 (-34/-26) * Improvement in cardiac baroreflex sensitivity after renal denervation ( msec/mmhg) Schlaich et al. NEJM. 2009; 36(9):
11 Proof of Principle: Related Changes in Underlying Physiology Baseline 1 mo Office BP (mmhg) 161/ /90 Renal NE spillover (ng/min) - left kidney % - right kidney % Total body NE spillover (ng/min) % Plasma Renin (μg/l/hr) % Renal Plasma flow (ml/min) % LV Mass (cmri) dropped 7% (from 78.8 to 73.1 g/m 2 ) from baseline to 12 months Schlaich et al. NEJM. 2009; 36(9):
12 Renal Norepinephrine Spillover: 10 cases Mean total renal norepinephrine spillover 47%, p=0.023 (95% CI: 28 65%) Mean total body NE spillover 28%, p=0.043 (95% CI: 4 52%) Example Case: Left: 75 % reduction Right: 85 % reduction Esler et al. J Htn. 2009;27(suppl 4):s167. Schlaich et al. J Htn. 2009;27(suppl 4):s154.
13 Concept Validated by Surgical History 1952 Effective, but significant morbidity 13
14 A common question How will the kidney function without sympathetic control? Transplanted kidneys lack innervation Yet effectively maintain fluid and electrolyte balance Establishes that sympathetic component of control represents overdrive system, rather than foundation of basic renal function Blaufox et al. N Engl J Med. 1969;280(2):


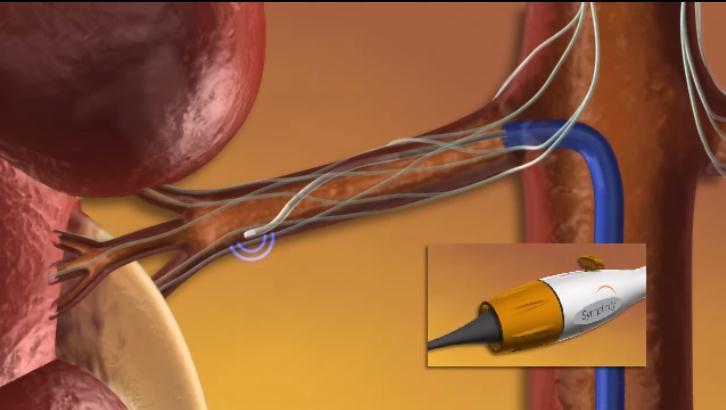
15 Renal Anatomy Allows a Catheter-Based Approach Vessel Lumen Media Adventitia Renal Nerves Arise from T10-L2 Follow the renal artery to the kidney Primarily lie within the adventitia The only location that renal efferent & afferent nerves travel together 15


16 Symplicity Catheter System Low profile, electrode tipped catheter Delivers RF energy to treatment site Proprietary RF generator - Low power - Automated - Built-in safety control algorithms Standard interventional technique 40-minutes from first to last RF delivery
17
18 Renal Denervation: Preclinical Evidence

19 Renal Tissue NE (pg/mg) Renal Denervation Preclinical Efficacy and Safety Extensive research in >300 swine Effectiveness: Significant reduction in renal tissue NE Safety: Verification testing included angiography, gross pathology, histopathology, & clinical pathology at 7, 30, 60, and 180 days Intact endothelium by 7 days Vascular healing observed at 30 and 60 days; by 180 days, arteries were well healed (no inflammatory cells) treatment sites were considered sterile and stable No stenosis or luminal reduction seen in any treated artery through 180 days Data on file. Medtronic, Inc. P< P=1.0


20 Vascular Safety Documented by Preclinical Studies Studied in >300 swine Angiography and pathology at 7, 30, 60 & 180 days No stenosis or luminal reduction seen in treated arteries RF Generator algorithm optimized to minimize vascular injury 21
 Nerve from treated vessel:")

21 Six Month Post-Procedure Nerve Histology (Porcine Model) H&E Nerve from untreated vessel: Periarterial nerve bundle surrounded by a thin fibrous connective tissue sheath (perineurium) Nerve from treated vessel: Periarterial nerve bundle has a hypercellular appearance and the perineurium has a thickened and fibrotic appearance. Nerve from Untreated Vessel Nerve from Treated Vessel Rippy MK, et. al. Clin Res Cardiol. 2011;doi:101007s
22 Staged Clinical Evaluation Symplicity HTN-1 First-in-Man Series of Pilot studies Symplicity HTN-2 EU/AU Randomized Clinical Trial USA Symplicity HTN-3 US Randomized Clinical Trial (upcoming) EU/AU Other Areas of Research: Insulin Resistance, HF/Cardiorenal, Sleep Apnea, More 23

23 Relevant studies Lancet published electronically on Nov 17,
 -")
24 Symplicity HTN-1 Lancet. 2009;373: Hypertension. 2011;57: Initial Cohort Reported in the Lancet, 2009: -First-in-man, non-randomized -Cohort of 45 patients with resistant HTN (SBP 160 mmhg on 3 anti-htn drugs, including a diuretic; egfr 45 ml/min) - 12-month data \ Expanded Cohort This Report (Symplicity HTN-1): -Expanded cohort of patients (n=153) -24 and 36 -month follow-up Symplicity HTN-1 Investigators. Hypertension. 2011;57: Sobotka P, ACC 2012
25 Baseline Patient Characteristics (n=153) Demographics Age (years) 57 ± 11 Gender (% female) 39% Race (% non-caucasian) 5% Co-morbidities Diabetes Mellitus II (%) 31% CAD (%) 22% Hyperlipidemia (%) 68% egfr (ml/min/1.73m 2 ) 83 ± 20 Blood Pressure Baseline BP (mmhg) 176/98 ± 17/15 Number of anti-htn meds (mean) 5.1 ± 1.4 Diuretic (%) 95% Aldosterone blocker(%) 22% ACE/ARB (%) 91% Direct Renin Inhibitor 14% Beta-blocker (%) 82% Calcium channel blocker (%) 75% Centrally acting sympatholytic (%) 33% Vasodilator (%) 19% Alpha-1 blocker 19% Symplicity HTN-1 Investigators. Hypertension. 2011;57:
26 Procedure Detail & Safety (n=153) 38 minute median procedure time Average of 4 ablations per artery Intravenous narcotics & sedatives used to manage pain during delivery of RF energy No catheter or generator malfunctions No major complications Minor complications 4/153: 1 renal artery dissection during catheter delivery (prior to RF energy), no sequelae 3 access site complications, treated without further sequelae Symplicity HTN-1 Investigators. Hypertension. 2011;57:
 P<0.")
27 Change in Office BP Through 36 Months BP change (mmhg) P<0.01 for from BL for all time points
 (N=143) (N=130) (N=59) (N=24) Sobotka P, ACC")
28 % Patients Distribution of SBP Change at Baseline, 1, 12, 24, and 36 Months (N=150) (N=143) (N=130) (N=59) (N=24) Sobotka P, ACC 2012
29 Response Rate Among 1-Month Non-responders (n=45) 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Responder was defined as an office SBP reduction 10 mmhg 58% 57% 64% 82% 100% 1 Month 3 Months 6 Months 12 Months 24 Months 36 Months (N=45) (N=45) (N=44) (N=39) (N=17) (N=8) Sobotka P, ACC 2012
30 BP change (mmhg) Sobotka P, ACC 2012 Change in Office BP by Age 12 Months 24 Months 36 Months N=97 N=33 N=44 N=15 N=21 N=3
 Non-DM (N=86) DM (N=17) Non-DM (N=42) DM (N=8) Non-DM (N=16)")
31 BP change (mmhg) Sobotka P, ACC 2012 Change in Office BP in Diabetic and Non-Diabetic Patients 12 Months 24 Months 36 Months DM (N=44) Non-DM (N=86) DM (N=17) Non-DM (N=42) DM (N=8) Non-DM (N=16)
32 BP change (mmhg) Change in Office BP by Baseline Renal function 12 Months 24 Months 36 Months egfr (N=9) egfr >60 (N=115) egfr (N=5) egfr >60 (N=51) egfr (N=1) egfr >60 (N=22) Sobotka P, ACC 2012
 Renal Function Over Time")
33 egfr (ml/min/1.73m 2 ) Renal Function Over Time Sobotka P, ACC 2012
34 Chronic Safety Out to 3 Years One progression of a pre-existing stenosis unrelated to RF treatment (stented without further sequelae) One new moderate stenosis which was not hemodynamically relevant and no treatment 3 deaths within the follow-up period; all unrelated to the device or therapy No hypotensive events that required hospitalization There were no observed changes in mean electrolytes or egfr to 18 months Symplicity HTN-1 Investigators. Hypertension. 2011;57: Sobotka P, ACC 2012
35 Conclusions from Symplicity HTN-1 The magnitude of clinical response is significant and sustained through 3 years Increasing responder rates indicate: no loss of treatment effect out to 36 months BP non-response at 6 months does not predict failure to respond at 12 months or later The treatment effect was consistent across subgroups (age, diabetes status, and baseline renal function) No late adverse events were seen Sobotka P, ACC 2012
36 Symplicity HTN-2 Lancet. 2010;376: Purpose: To demonstrate the effectiveness of catheter-based renal denervation for reducing blood pressure in patients with uncontrolled hypertension in a prospective, randomized, controlled, clinical trial Patients: 106 patients randomized 1:1 to treatment with renal denervation vs. control Clinical Sites: 24 centers in Europe, Australia, & New Zealand (67% were designated hypertension centers of excellence) Symplicity HTN-2 Investigators. Lancet. 2010;376:
37 Symplicity HTN-2 Trial Treatment-resistant HTN population BL OBP 178/97 mmhg 49 RDN, 51 Control Age 58 years BMI 31 kg/m² 40% with Diabetes egfr 77* Avg # meds 5.2 RDN and Control groups generally well-matched Inclusion Criteria: Office SBP 160 mmhg ( 150 mmhg with type II diabetes mellitus) Stable drug regimen of 3+ more anti-htn medications Age years Exclusion Criteria: Hemodynamically or anatomically significant renal artery abnormalities or prior renal artery intervention egfr < 45 ml/min/1.73m 2 (MDRD formula) Type 1 diabetes mellitus Contraindication to MRI Stenotic valvular heart disease for which reduction of BP would be hazardous MI, unstable angina, or CVA in the prior 6 months *MDRD, ml/min/1.73m 2 Symplicity HTN-2 Investigators. Lancet. 2010;376:
38 Patient Disposition Assessed for Eligibility (n=190) Screening Excluded Prior to Randomization (n=84) BP<160 after 2-weeks of compliance confirmation (n=36; 19%) Ineligible anatomy (n=30; 16%) Declined participation (n=10; 5%) Other exclusion criteria discovered after consent (n=8; 4%) Randomized (n=106) Allocation Allocated to RDN (n=52) Allocated to Control (n = 54) Follow-up No Six-Month Primary Endpoint Visit (n = 3) Reasons: Withdrew consent (n=1) Missed visit (n=2) No Six-Month Primary Endpoint Visit (n = 3) Reasons: Withdrew consent (n=2) Lost to follow-up (n=1) Analysis Analyzed (n = 49) Analyzed (n = 51) Symplicity HTN-2 Investigators. Lancet. 2010;376:
 84% of RDN patients had 10 mmhg reduction in SBP 10% of RDN patients had no reduction in SBP Symplicity HTN-2 Investigators. Lancet. 2010;376:1903-1909.")
39 Primary Endpoint: 6-Month Office BP from Baseline to 6 Months (mmhg) Diastolic Systolic Diastolic Systolic 33/11 mmhg difference between RDN and Control (p<0.0001) 84% of RDN patients had 10 mmhg reduction in SBP 10% of RDN patients had no reduction in SBP Symplicity HTN-2 Investigators. Lancet. 2010;376:
40 Home & 24 Hour Ambulatory BP Home BP Change BP (mmhg) Change (mmhg) Systolic Diastolic Diastolic Systolic 24-h ABPM: Analysis on technically sufficient (>70% of readings) paired baseline and 6-month RDN (n=20): -11/-7 mmhg (SD 15/11; p=0.006 SBP change, p=0.014 for DBP change) Control (n=25): -3/ -1 mmhg (SD 19/12; p=0.51 for systolic, p=0.75 for diastolic) Symplicity HTN-2 Investigators. Lancet. 2010;376:
41 Procedural Safety One renal artery dissection from injection of contrast into renal artery wall during dye angiography. The lesion was stented without further consequences One hospitalization prolonged in a crossover patient due to hypotension following the RDN procedure. IV fluids administered, anti-hypertensive medications decreased and patient discharge without further incident No radiofrequency-related renal artery stenosis or aneurysm occurred in either Randomised group Minor adverse events (full cohort) 1 femoral artery pseudoaneurysm treated with manual compression 1 postprocedural drop in BP resulting in a reduction in medication 1 urinary tract infection 1 prolonged hospitalization for evaluation of paraesthesias 1 back pain treated with pain medications and resolved after 1 month 6-month renal imaging (n=43) showed no vascular abnormalities at any RF treatment site 1 MRA indicates possible progression of a pre-existing stenosis unrelated to RF treatment (no further therapy warranted) Esler M, ACC 2012
42 Systolic BP (mmhg) Office BP 18 months Post Procedure 220 Randomization Primary Endpoint reached* 183 (n = 54) 191 (n = 37) (n = 52) 166 (n = 35) 167 (n = 33) 162 (n = 31) 147 (n = 49) 151 (n = 47) 145 (n = 43) Baseline *Patients randomized to control were offered RDN following the primary endpoint assessment. Only patients still meeting entry criteria (SBP 160 mmhg) were included in this analysis (n=37) Esler M, ESC 2012


43 (mm Hg) (mm Hg) Change in Office Blood Pressure Through 18 Months* 10 RDN Group Crossover Group Series1 SBP Series2 DBP SBP DBP month N=49 12 months N=47 *Post Procedure follow up Esler M, ESC months N=43 6 months N=35 P-values < 0.01 at each time point compared to pre procedure values for each group 12 months N=33 18 months N=31


44 Renal Function Over Time *egfr ml/min/1.73m 2 Esler M, ESC 2012 Renal function parameters were not obtained beyond 12 months follow up

45 mm Hg Change in Pulse Pressure Post Procedure N=49 N=35 N=47 N=33 N=43 N=31 *P<.01 from pre procedure values at all time points Esler M, ESC 2012
 All p-values at each time point are compared to pre procedure HR Esler")
46 BPM Heart Rate Over Time *p <.01 (6, 12m), p=.02 (18m) p=ns (6, 18m), p<.01 (12m) All p-values at each time point are compared to pre procedure HR Esler M, ESC 2012

47 Physicians were allowed to change medication following the 6-month primary endpoint Reasons for medication changes were unknown and may be related to a variety of confounding factors Increase: if both meds/dose increase, or if meds no change and dose increase, or if dose no change and meds increase; Decrease: if both meds/dose decrease, or if meds no change and dose decrease, or if dose no change and meds decrease; Indeterminate: All other combinations Esler M, ESC 2012 Medication Change Analysis to 18 Months Post Procedure
48 Safety Through 18 months Post Procedure No device-related SAEs No vascular complications at any site of RF delivery No clinically significant changes to egfr for RDN or crossover groups at 12 months post RDN* 2 hypotensive events that required hospitalization: 1 in crossover cohort and 1 in RDN cohort 10 hypertensive events (in 8 patients) requiring hospitalization through 18 months post RDN in combined cohort 1 mild transient acute renal failure Patient admitted with elevated K+, meds temporarily discontinued (Co-Amilofruse, perindopril, metformin). IV fluids administered and K+ decreased. Patient discharged and remained off perindopril 2 deaths within the follow-up period; all unrelated to the device or therapy *Renal function parameters were not obtained beyond 12 months follow up
49 Symplicity HTN-2 Baseline Medications RDN (n=52) Control (n=54) p-value Number Anti-HTN medications 5.2 ± ± % patients on HTN meds >5 years 71% 78% 0.51 % percent patients on 5 medications 67% 57% 0.32 % patients on drug class: ACEi/ARB 96% 94% >0.99 Direct renin inhibitor 15% 19% 0.80 Beta-adrenergic blocker 83% 69% 0.12 Calcium channel blocker 79% 83% 0.62 Diuretic 89% 91% 0.76 Aldosterone antagonist 17% 17% >0.99 Vasodilator 15% 17% >0.99 Alpha-1 adrenergic blocker 33% 19% 0.12 Centrally acting sympatholytic 52% 52% >0.99 Symplicity HTN-2 Investigators. Lancet. 2010;376:
50 Symplicity HTN-2 Medication Changes at 6 months Despite protocol guidance to maintain medications, some medication changes were required: RDN (n=49) Control (n=51) P-value # Med Dose Decrease (%) 10 (20%) 3 (6%) 0.04 # Med Dose Increase (%) 4 (8%) 6 (12%) 0.74 Censoring BP after medication increases: Renal Denervation Reduction of 31/12 ± 22/11 mmhg (p< for SBP & DBP) Control Change of 0/-1 ± 20/10 mmhg (p=0.90 & p=0.61 for SBP & DBP, respectively) Symplicity HTN-2 Investigators. Lancet. 2010;376:
51 Symplicity HTN-2 Renal Function (6 months) Δ Renal Function (baseline - 6M) RDN Mean ± SD (n) Control Mean ± SD (n) Difference (95% CI) p-value egfr (MDRD) (ml/min/1.73m 2 ) 0 ± 11 (49) 1 ± 12 (51) -1 (-5, 4) 0.76 Serum Creatinine (mg/dl) 0.0 ± 0.2 (49) 0.0 ± 0.1 (51) 0.0 (-0.1, 0.1) 0.66 Cystatin-C (mg/l) 0.1 ± 0.2 (37) 0.0 ± 0.1 (40) 0.0 (-0.0, 0.1) 0.31 Symplicity HTN-2 Investigators. Lancet. 2010;376:
52 Symplicity HTN-2 Other Safety (6 months) Composite CV Events RDN (n=49) Control (n=51) Hypertensive event unrelated to non-adherence to medication 3 2 Other CV events 0 0 Other Serious AEs Transient ischemic attack 1 2 Hypertensive event after abruptly stopping clonidine 1 0 Hypotensive episode resulting in reduction of medications 1 0 Coronary stent for angina 1 1 Temporary nausea/edema 1 0 Symplicity HTN-2 Investigators. Lancet. 2010;376:


53 Symplicity HTN-2 Trial Distribution of Office SBP Post-RDN Treated with RDN Crossover group Treated after 6 M follow up Esler M, ACC 2012
54 Medication Change Analysis to 18 Months Post Procedure RDN (n=47) 6 month 12 months 18 months Decrease (# Meds or Dose) 18.6% (8/43) 23.3% (10/43) 25.6% (11/43) Increase (# Meds or Dose) 9.3% (4/43) 9.3% (4/43) 20.9% (9/43) No Change 67.4% (29/43) 53.5% (23/43) 37.2% (16/43) Indeterminate 4.7% (2/43) 14.0% (6/43) 16.3% (7/43) Crossover (n=35) 6 months post-rdn 12 months post-rdn 18 months post-rdn Decrease (# Meds or Dose) 15.2% (5/33) 24.2% (8/33) 20.0% (6/30) Increase (# Meds or Dose) 12.1% (4/33) 30.3% (10/33) 23.3% (7/30) No Change 66.7% (22/33) 27.3% (9/33) 30.0% (9/30) Indeterminate 6.1% (2/33) 18.2% (6/33) 26.7% (8/30) Physicians were allowed to change medication following the 6-month primary endpoint Reasons for medication changes were unknown and may be related to a variety of confounding factors Increase: if both meds/dose increase, or if meds no change and dose increase, or if dose no change and meds increase; Decrease: if both meds/dose decrease, or if meds no change and dose decrease, or if dose no change and meds decrease; Indeterminate: All other combinations
55 Conclusions Subjects in both groups had blood pressure reductions which were significant and sustained through 18 months of follow up Physicians were allowed to change medications following the 6-month primary endpoint. Reasons for changes were mostly unknown but may be related to a variety of confounding factors Pulse pressure improved and heart rate was stable or dropped following treatment with the Symplicity renal denervation system At 18 months follow-up there are no device-related serious adverse effects and no detrimental effects on the renal vasculature following treatment Esler M, ESC 2012
56 59 Equipment and Lab Setup
57 Equipment Set-up Symplicity Catheter and Generator Dispersive electrode (Ground pad) 6 Fr Renal guide catheter (45-55cm) (RDC or LIMA) and introducer sheath Guidewire (0.014, non-hydrophilic) Tuohy (RHV) Non-ionic contrast (dilute to 50:50) Heparinized saline flush bag (pressurized) Radiopaque ruler Common medications to have available: Heparin Fentanyl / Morphine or similar Midazolam (Dormicum, Versed) or similar Nitroglycerine Atropine 60
 Deflectable Shaft")
58 Catheter Tip Features 5mm 12mm Flexible Tip (self-orienting) Deflectable Shaft 61



59 Catheter Handle Features Deflect tip by pulling lever towards back of handle Straighten tip by pushing lever towards front of handle 62 Shaft & electrode can rotate independent from handle body Handle rotator has tactile click every 45 Dot on rotator gives relative rotational reference
60 Assessing Renal Anatomy 63

61 Renal Angiogram 64 Eligible Anatomy: Absence of flow limiting obstructions Diameter 4mm in targeted area Length 20mm




62 Renal Angiogram Prudently limit contrast dye exposure 50/50 dilution of contrast and use of DSA or biplane may help Verify entire kidney fills with contrast Unfilled kidney sections may indicate multiple main arteries Accessory Vessel Partially Supplies Lower Portions of the Kidney Lower Pole Not Completely Filling on Selective Injection


63 Oblique Angiographic Views Changing from AP to oblique and cranial views can provide optimal assessment of artery length AP projection ~20% LAO projection 66


64 Guide Catheter Selection Typical: RDC-1 Alternate: LIMA Once suitable anatomy is confirmed, upsize to 6Fr (or larger) introducer and guide Consider guide shape based on renal anatomy (LIMA for inferior takeoffs) 67
65 Intra-Procedural Patient Management and Monitoring 68
66 Patient Management Premedication Aspirin mg on the day of procedure, then for one month after operation Anxiolytic and Amnesic Midazolam (Dormicum, Versed) or similar recommended, often administered before groin access. 3-5mg or more may be required. Anticoagulation Heparin: target ACT >250 sec Continuously flush guide catheter with heparinized saline during the procedure Pain Management Patients may experience transient visceral pain during each ablation Fentanyl or Morphine (or similar) 2-5 minutes before first ablation; as needed thereafter mg may be required. Vasodilatation IA nitroglycerine through renal guide is recommended before treating each artery 69
67 Vital Signs During Procedure 70 Blood Pressure Pain medications, nitroglycerine, valsalva maneuvers during therapy, and changes of heart rate can all reduce BP during procedure Fluid resuscitation for hypotension Atropine for bradycardia or block associated with hypotension Heart Rate Pain medications, valsalva maneuvers during therapy, and pain can cause bradycardia Atropine for bradycardia or block associated with hypotension Oxygenation Pain medications and anxiolytic may reduce quality of respiration and oxygenation Monitor respiratory rate and pulse oximetry

68 Symplicity Catheter & Generator 71


69 Targeting Renal Nerves Nerves arise from T10-L2 The nerves arborize around the artery and primarily lie within the adventitia Vessel Lumen Media Adventitia 72 Renal Nerves
: Distal: Inferior and inferolateral locations Proximal: Superior and superolateral locations Avoid purely lateral treatments (possible electrode movement with respiration) 73 PULL, ROTATE,")
70 Targeting Renal Nerves Treat distal to proximal 4-6 focal treatments 2 min per treatment 5 mm between locations Stable, unique locations Circumferential coverage Common strategy (dependent on renal anatomy): Distal: Inferior and inferolateral locations Proximal: Superior and superolateral locations Avoid purely lateral treatments (possible electrode movement with respiration) 73 PULL, ROTATE, ASSESS new location and prior treatment site

 to position catheter within vessel Position electrode 5mm proximal")
71 Delivering Symplicity Catheter Fully straighten tip of catheter. NEVER advance the catheter while the tip is deflected DO NOT cross recently treated sites Deliver Symplicity Catheter through the renal guide catheter Use the catheter shaft (not handle) to position catheter within vessel Position electrode 5mm proximal to renal bifurcation 74

72 Positioning Catheter With electrode advanced to most distal treatment site, use handle lever to deflect catheter tip against vessel wall 75 Good wall contact is important for the proper delivery of energy First deflect slightly Rotate to superior or inferior hemisphere Continue to deflect until electrode is well apposed to the vessel wall May not need to use handle lever to deflect tip in tortuous anatomy or proximal locations


 76")
73 Wall Contact Sufficient Wall Contact Excessive Wall Contact (avoid distending vessel wall with electrode) 76



74 Example Treatment Sites Distal locations in straight vessels may require more deflection to achieve vessel wall contact Because of added guide catheter support, proximal locations may require less deflection to achieve vessel wall contact 77
 may indicate")

75 Optimizing Treatment Sites: Impedance may be used to confirm stable wall contact: Higher impedance may indicate better wall contact Stable impedance over a respiratory cycle (Δ < ohms) may indicate consistent wall contact Abnormally high impedance may indicate electrode is in a side-branch Impedance 78 * Impedance varies by patient and vessel. Care should be taken to notice range of available impedance readings within each vessel
76 Initiate First Treatment Meds: IA nitroglycerine Fentanyl or morphine (or similar) Sufficient anticoagulation (confirm ACT > 250) Document each treatment site using cine Initiate energy delivery: Stabilize catheter do not move during treatment Press foot pedal (or RF button) once to activate catheter Do not inject contrast during active treatment (alters impedance) Generator will automatically control RF energy delivery: Power automatically ramped and maintained (5-8W) Continuously monitors temperature and impedance Automatically shuts off after 2 min or when either impedance or temperature exceed program limits To manually stop RF delivery, depress foot pedal or press RF button once 79

77 Repeat for Additional Treatment Sites Reposition electrode for next treatment: Retract Symplicity Catheter proximal (using catheter shaft) If needed, straighten catheter tip using handle lever Deflect electrode to make contact with vessel wall, using visual and impedance feedback Rotate electrode to appropriate treatment location Optionally, using physician discretion, the tip may remain deflected while positioning electrode for next treatment (rotating and retracting) Allow 5 mm between treatment sites ( ~3 electrode lengths) Secondary shaft marker may help identify 5mm spacing Initial treatment location Secondary 5 mm shaft marker (~3 electrode lengths) 80 New treatment location
78 Switching Sides / Ending Procedure Straighten tip, then remove Symplicity Catheter from patient Perform renal artery angiogram (cine) of treated artery Prudently limit dye exposure If coagulum or clot are present on electrode, gently wipe with a sterile gauze pad dampened with sterile saline Confirm ACT > 250 sec Repeat entire procedure on opposite renal artery if required After treating both kidneys: Remove ground pad from patient 81


")

79 Areas to Avoid There is no clinical experience treating near any areas of visible atherosclerosis, calcification, or fibromuscular dysplasia. Avoid treating areas of visible disease. There is no clinical experience treating in vessels with renal artery aneurysms Atherosclerosis (Ostial Stenosis) Calcification Fibromuscular Dysplasia (FMD) Avoid treating in segment with stenosis Avoid energy delivery to area with visible calcification Avoid treating in segment with FMD 82



80 Pre-Procedure Angiographic Appearance: Typical 1 Month Follow-Up Acute Post-Procedure 83




81 Angiographic Appearance: Less Common Pre-Procedure 1 Month Follow-up Acute Post-Procedure * Increased vessel reactivity, such as spasm, may be encountered when treating in areas with reduced blood flow, such as dual renal arteries or beyond significant renal artery branch points 84

82 Multiple sites of edema and spasm
83 Post-Procedure Care Manage femoral access site per standard protocol Be attentive to preventing groin access complications Be attentive to radiocontrast nephropathy prophylaxis (hydrate well) 86
84 Expanding Indications of TRenD
85 RENAL DENERVATION & INSULIN RESISTANCE
86 RDN and Insulin Resistance Three separate publications with data on changes of IR post denervation Schlaich Euglycemic clamp in 2 resistant HTN patients with polycystic ovarian syndrome Warsaw HOMA + HgbA1c in 10 patients with resistant HTN with sleep apnea Homburg HOMA in 37 patients with resistant HTN Schlaich. J Hypertens. 2011;29: Witkowski A, et al. Hypertension. 2011;58: Mahfoud et al. Circulation. 2011;123:
87 Improvement in Fasting Plasma Glucose and Insulin Sensitivity in 2 patients with rhtn + PCOS Schlaich. J Hypertens. 2011;29:
88 Insulin Resistance and HgbA1c Significant decrease in plasma glucose concentration 2 hours after glucose challenge at 6 months BL median: 7.0 mmol/dl at baseline (IQR: ) 6-month median: 6.4 mmol/dl (IQR: ) P<0.05 Significant decrease in HgbA1C level at 6 months BL median: 6.1% (IQR: 5.9%-6.7%) 6-month median: 5.6% (IQR: 5.4%-6.5%) P<0.05 Witkowski A, et al. Hypertension. 2011;58:
 Renal Denervation Group (n=37) Control Group (n=13) Age, y 59.7±1.4 58.7±1.6 62.5±2.9 0.228 Sex (female), n (%) 13 (26) 8 (21) 5 (38) 0.")
89 Treatment-resistant HTN population 37 RDN, 13 Control Age 60 years BMI 31 kg/m² 16% with Diabetes 52% either impaired fasting glucose or impaired glucose tolerance RDN and Control groups generally well-matched All Patients (n=50) Renal Denervation Group (n=37) Control Group (n=13) Age, y 59.7± ± ± Sex (female), n (%) 13 (26) 8 (21) 5 (38) Type 2 diabetes mellitus, n (%) 20 (40) 13 (35) 7 (54) On medication, n (%) 16 (32) 12 (32) 4 (31) Body mass index, kg/m ± ± ± Weight, kg 94.0± ± ± egfr, ml min m ± ± ± Heart rate, bpm 70.9± ± ± Systolic blood pressure, mm Hg 178±3 177±3 184± Diastolic blood pressure, mm Hg 96±2 96±6 94± Antihypertensive drugs, n 5.6± ± ± Fasting glucose, mg/dl 121±4 118±3 129± Glucose level at 60 min, OGTT, mg/dl 219±10 221±10 215± Glucose level at 120 min, OGTT, mg/dl 186±11 184±13 190± Impaired fasting glycemia, OGTT, n (%) 8 (16) 5 (13) 3 (23) Impaired glucose tolerance, OGTT, n (%) 18 (36) 15 (40) 3 (23) Diabetes mellitus, OGTT, n (%) 8 (16) 5 (13) 3 (23) Hemoglobin A 1C, % 6.0± ± ± Insulin, miu/ml 19.3± ± ± C peptide, ng/ml 4.9± ± ± HOMA-IR 5.7± ± ± IS QUICKI 0.32± ± ± P Mahfoud et al. Circulation. 2011;123:
90 Change in fasting C-peptide (ng/ml) Change in HOMA-IR (ng/ml) Change in fasting glucose (mg/dl) Change in fasting insulin (mlu/ml) RDN Group Showed Improvements In Several Key Insulin Resistance Markers Fasting Glucose 1 month 3 months p=0.402 p= p=0.043 p=0.039 p for interaction (ANOVA)= Fasting Insulin 1 month 3 months p=0.129 p= p=0.036 p=0.006 p for interaction (ANOVA)=0.016 Renal denervation (n=37) Control (n=13) Fasting C-peptide HOMA-IR 1 month 3 months p= p= p=0.006 p= p for interaction (ANOVA)=0.031 Mahfoud et al. Circulation. 2011;123: month 3 months p=0.085 p= p=0.008 p=0.001 p for interaction (ANOVA)=0.003
91 Patients (%) Change in Status from Baseline to 3 months: 1) Diabetes 2) Impaired Glucose Tolerance or Impaired Fasting Glucose (IGT/IFG) 3) Normal Glucose Tolerance (NGT) Renal denervation (n=37) Control group (n=13) Diabetes % 6% 23% IGT, IFG, or both NGT 80 n=3 38% % n=4 51% 46% n=2 38% % 43% 31% n=1 24% 0 Baseline 3 months Baseline 3 months Mahfoud et al. Circulation. 2011;123:
92 Possible Physiologic Explanations? Sympathetic hyperactivity: Shifts blood from striated skeletal muscle to visceral tissue 1 Visceral tissue is less insulin sensitive than striated muscle 1 Sympathetic activity increases glucagon secretion 2 Inhibition of the sympathetic nervous system by moxonidine has been shown to improve glucose metabolism 2 1 Julius S et al, Blood Press. 1992;1: Yakubu-Madus et al, Diabetes. 1999;48:
93 RENAL DENERVATION & Heart Failure
94 RDN and Heart Failure A recent publication with data on changes to LVH post denervation Mathias Brandt et al Evaulated BP and cardiac structure and function following renal denervation. Brandt et al. J Am Coll Cardiol. 2012;59:901 9


95 Treatment-resistant HTN population 46 RDN, 18 Control Evaulated BP and cardiac structure and function via echo and baseline, 1 mo & 6 mo RDN Group: Mean age 63 years BMI 28.6 kg/m² 46% with Diabetes 4.7 mean anti-htn meds Incidence LVH 63% by echo Brandt et al. J Am Coll Cardiol. 2012;59:901 9


96 RDN Group: in SBP, DBP, & Pulse Pressure at 1 & 6 Mo RDN SBP Histogram at 1 & 6 mo RDN & Control SBP at 1 & 6 Mo RDN & Control DBP at 1 & 6 Mo RDN & Control PP at 1 & 6 Mo Brandt et al. J Am Coll Cardiol. 2012;59:901 9

97 RDN Impact on Cardiac Structure & Fxn: (1) LV Mass Index (2) EF (3) Improved Diastolic Dysfunction - Myocardial Relaxation - End-Diastolic Pressures E/E & LA size Brandt et al. J Am Coll Cardiol. 2012;59:901 9
 Brandt et al. J Am Coll Cardiol.")
98 LVMI Reduction after RDN Effect driven by LVMI reduction among patients with LVH at baseline (no appreciable change in LVMI in patients without LVMI at baseline) Brandt et al. J Am Coll Cardiol. 2012;59:901 9

99 LVMI by BP Response Tier LVMI decreases in every group, but correlates with magnitude of BP reduction LV mass regression occurred also in 5 of 6 RD nonresponders, supporting the notion of BP-independent effects of RD on LVH Brandt et al. J Am Coll Cardiol. 2012;59:901 9
100 SYMPLICITY HF Study Goal Evaluate safety of the Symplicity Catheter System and efficacy of renal denervation for improving cardiac & renal function in patients who have Chronic Heart Failure with Renal impairment Study Design Multicenter prospective, non-randomized, open-label study Enrollment 40 subjects NYHA Class II-III, EF<40%, egfr ml/min/1.73m 2 ~ 8 sites in Australia and Europe Major Assessments: Cardiac ventricular function by Echocardiography - 6 & 12 months Renal function by GFR - 1, 3, 6, & 12 months
101 Objectives: Assess procedural and long term safety of renal denervation Evaluate effectiveness of renal denervation on clinical outcomes Establish procedural benchmarking & physician practice patterns Evaluate the effect of geographical variations in patients and procedural characteristics on clinical outcomes Perform Quality of Life analysis First enrollment February 2 nd, 2012 Scope: Over 200 sites world wide; at least 5000 patients Prospective, single-arm, open-label, non-interventional registry In accordance with Instructions For Use Geographies with commercial availability of Medtronic Symplicity Renal Denervation System
102 Study Design SYMPLICITY HTN-3 Multi-center, prospective, blinded, randomized controlled trial Study Objective To demonstrate that catheter-based renal denervation is a safe and effective treatment for uncontrolled hypertension Study Population Uncontrolled hypertension population SBP 160 mmhg despite maximally tolerated doses of 3 antihypertensive medication classes Without significant renal impairment (egfr > 45mL/min) 530 randomized subjects at 90 sites Randomization (2:1) All patients maintained on baseline meds for 6 months This study is actively enrolling patients
103 Conclusions Transcatheter renal denervation, based on the described neural pathophysiology of essential hypertension, affirms the crucial relevance of renal nerves in the maintenance of BP in patients with hypertension. Transcatheter renal denervation is the latest breakthrough in the area of non-pharmaceutical treatment of essential hypertension. It produces significant reductions in BP in patients with treatment-resistant essential hypertension, The magnitude of BP reduction is predictable. The technique was applied without major complications. 106
104 Conclusions At present, this therapy is mainly reserved for those patients whose blood pressure cannot be controlled (SBP >160mmHg) with three or more medications And in those whose blood pressure cannot be controlled due to intolerance of anti-hypertensive drugs Its role in milder forms of hypertension remains to be explored
105 Conclusions Its long term results and its application in other areas still require more studies and long term follow-up but its initial results are very encouraging Good drug compliance and modification of life style (diet, exercise, body weight control) are the most important elements for good blood pressure control in all patients with essential hypertension
Renal Sympathetic Denervation for HTN
 Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Catheter-Based Renal Denervation (RDN)
") Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
What We've Learned from Simplicity HTN-1,2, and Registries
 ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
Devices and Long-Term Outcomes of Renal Denervation for Hypertension
 18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension
 Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Renal Artery Denervation New Concepts in Hypertension Treatment
 Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
Autumn Meeting Birmingham. Renal Denervation
 Autumn Meeting Birmingham Renal Denervation Andreas Baumbach, MD, FRCP, FESC Consultant Cardiologist, hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol Renal Denervation BACKGROUND
Autumn Meeting Birmingham Renal Denervation Andreas Baumbach, MD, FRCP, FESC Consultant Cardiologist, hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol Renal Denervation BACKGROUND
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension
 Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION
 CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
With an unrestricted educational grant from. The Interventional Treatment of Resistant Hypertension
 With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
noradrenaline spillover and systemic blood pressure in patients with resistant hypertension
 Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Percutaneous Renal Denervation: A New Promise in the Treatment of RHT?
 BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension
 EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
Renal denervation: Current evidence and remaining uncertainties
 Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Treating Hypertension With a Catheter..Wait What? COI 5/3/2013. Worldwide Prevalence of Hypertension Is Increasing
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Renal Denervation for Resistant Hypertension
 Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Renal Denervation. Henry Krum MBBS PhD FRACP. Centre of Cardiovascular Research & Monash University/Alfred Hospital;
 Renal Denervation Henry Krum MBBS PhD FRACP Centre of Cardiovascular Research & Education in Therapeutics, Monash University/Alfred Hospital; Alfred Heart Centre, The Alfred Hospital, Melbourne Australia
Renal Denervation Henry Krum MBBS PhD FRACP Centre of Cardiovascular Research & Education in Therapeutics, Monash University/Alfred Hospital; Alfred Heart Centre, The Alfred Hospital, Melbourne Australia
Byeong-Keuk Kim, MD, PhD. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Stephen G. Worthley 1, Gerard T. Wilkins 2, Mark W. Webster 3,Joseph K. Montarello 1, Paul T. Antonis 4, Robert J. Whitbourn 5, Roderic J.
 Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Catheter Based Denervation for Heart Failure
 Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich,
 The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial
 Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial Prof Murray Esler Baker IDI Heart and Diabetes Institute, Melbourne
Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial Prof Murray Esler Baker IDI Heart and Diabetes Institute, Melbourne
Management of Resistant Hypertension in Diabetes
 Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications
 Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications Uta C. Hoppe, MD, FESC Dep. of Internal Medicine II Paracelsus University Salzburg Austria Disclosures Within
Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications Uta C. Hoppe, MD, FESC Dep. of Internal Medicine II Paracelsus University Salzburg Austria Disclosures Within
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1
 Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Transcatheter Perivascular Alcohol- Mediated Renal Denervation
 Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
The Future of Renal Denervation
 The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension
 The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Evidence of Baroreflex Activation Therapy s Mechanism of Action
 Evidence of Baroreflex Activation Therapy s Mechanism of Action Edoardo Gronda, MD, FESC Heart Failure Research Center IRCCS MultiMedica Cardiovascular Department Sesto S. Giovanni (Milano) Italy Agenda
Evidence of Baroreflex Activation Therapy s Mechanism of Action Edoardo Gronda, MD, FESC Heart Failure Research Center IRCCS MultiMedica Cardiovascular Department Sesto S. Giovanni (Milano) Italy Agenda
Renal denervation for treatment of resistant hypertension
 Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Update on renal denervation: Latest data
 LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
Φαρµακευτική θεραπεία υπερτασικών ασθενών. Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική
 Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.
 Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Disclosures for Dr. Bhatt
 Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Christopher Valentine, MD
 Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
MINNEAPOLIS September 12, 2012 Medtronic, Inc. (NYSE: MDT) today announced findings
 today announced findings") NEWS RELEASE Contacts: Wendy Dougherty Jeff Warren Public Relations Investor Relations 707-541-3004 763-505-2696 FOR IMMEDIATE RELEASE HEALTH-ECONOMIC ANALYSIS SUGGESTS MEDTRONIC SYMPLICITY RENAL DENERVATION
NEWS RELEASE Contacts: Wendy Dougherty Jeff Warren Public Relations Investor Relations 707-541-3004 763-505-2696 FOR IMMEDIATE RELEASE HEALTH-ECONOMIC ANALYSIS SUGGESTS MEDTRONIC SYMPLICITY RENAL DENERVATION
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Renal sympathetic denervation as a potential treatment for hypertension
 Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital
Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension: the Heart Vs the Kidney. George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi
 Hypertension: the Heart Vs the Kidney George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi 24 th Feb, 2017 Travel facilitation from Novartis Disclaimer Systolic blood pressure (SBP) of at least
Hypertension: the Heart Vs the Kidney George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi 24 th Feb, 2017 Travel facilitation from Novartis Disclaimer Systolic blood pressure (SBP) of at least
OLOMOUC I Registry. The effect of renal denervation in patients with advanced heart failure:
 The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Registry M. Táborský, M. Lazárová, J. Václavík, D. Richter, D. Vindiš, M. Kamasová, A. Louis, J. Jarkovský * I.IKK FNOL,
The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Registry M. Táborský, M. Lazárová, J. Václavík, D. Richter, D. Vindiš, M. Kamasová, A. Louis, J. Jarkovský * I.IKK FNOL,
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Renal Denervation: The Case for Cardiology
 Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Renal Denervation For Hypertension: Status Update
 Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
SPYRAL HTN ON MED. Disclosure
 Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES
 CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Individual Study Table Referring to Part of Dossier: Volume: Page:
 Synopsis Abbott Laboratories Name of Study Drug: Paricalcitol Capsules (ABT-358) (Zemplar ) Name of Active Ingredient: Paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For
Synopsis Abbott Laboratories Name of Study Drug: Paricalcitol Capsules (ABT-358) (Zemplar ) Name of Active Ingredient: Paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Renal Sympathetic Denervation Using an Irrigated Radiofrequency Ablation Catheter for the Management of Drug-Resistant Hypertension
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 7, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2012.01.027
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 7, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2012.01.027
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Cardiovascular Diseases in CKD
 1 Cardiovascular Diseases in CKD Hung-Chun Chen, MD, PhD. Kaohsiung Medical University Taiwan Society of Nephrology 1 2 High Prevalence of CVD in CKD & ESRD Foley RN et al, AJKD 1998; 32(suppl 3):S112-9
1 Cardiovascular Diseases in CKD Hung-Chun Chen, MD, PhD. Kaohsiung Medical University Taiwan Society of Nephrology 1 2 High Prevalence of CVD in CKD & ESRD Foley RN et al, AJKD 1998; 32(suppl 3):S112-9
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease
 Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease Michelle P Kao, Donald S Ang, Steve Gandy, Chim C Lang, Allan D Struthers Division of
Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease Michelle P Kao, Donald S Ang, Steve Gandy, Chim C Lang, Allan D Struthers Division of
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study
 Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Vascular disease. Structural evaluation of vascular disease. Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital
 Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Phase 3 investigation of aprocitentan for resistant hypertension management. Investor Webcast June 2018
 Phase 3 investigation of aprocitentan for resistant hypertension management Investor Webcast June 2018 The following information contains certain forward-looking statements, relating to the company s business,
Phase 3 investigation of aprocitentan for resistant hypertension management Investor Webcast June 2018 The following information contains certain forward-looking statements, relating to the company s business,
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
WPCCS May2013. Mr Ian Williams Consultant Vascular Surgeon UHW. Consultant Cardiologist UHW
 Peripheral Vascular Disease WPCCS May2013 Mr Ian Williams Consultant Vascular Surgeon UHW Prof Julian Halcox Prof Julian Halcox Consultant Cardiologist UHW Case 1? Ischaemic Legs History 85 years lady?varicose
Peripheral Vascular Disease WPCCS May2013 Mr Ian Williams Consultant Vascular Surgeon UHW Prof Julian Halcox Prof Julian Halcox Consultant Cardiologist UHW Case 1? Ischaemic Legs History 85 years lady?varicose
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis
 Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
When should you treat blood pressure in the young?
 ESC Stockholm - Dilemmas in Cardiovascular Disease Prevention in the Young: 30 th August 2010 When should you treat blood pressure in the young? Bryan Williams MD FRCP FAHA FESC Professor of Medicine Department
ESC Stockholm - Dilemmas in Cardiovascular Disease Prevention in the Young: 30 th August 2010 When should you treat blood pressure in the young? Bryan Williams MD FRCP FAHA FESC Professor of Medicine Department
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Prof. Andrzej Wiecek Department of Nephrology, Endocrinology and Metabolic Diseases Medical University of Silesia Katowice, Poland.
 What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Preliminary Results of RETREAT
 LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality
 Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs