Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation
|
|
|
- Ashlynn George
- 5 years ago
- Views:
Transcription
1 Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation Hatim Al Lawati MD, FRCPC, FACC Consultant Interventional Cardiology Sultan Qaboos University Hospital Oman
2 Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation DISCLOSURES I, Hatim Al Lawati, have no disclosures relevant to the topic of this presentation. All slides were prepared by myself without any external contribution.

3 Burden of valvular heart diseases - a population-based study - Prevalence of valvular heart diseases in population-based studies >15% with moderate or severe mitral regurgitation Nkomo VT, et al. Lancet 2006; 368:
4 Outcomes in patients with untreated severe chronic mitral regurgitation One year survival was % in operated patients vs % in the non-operated patients (p=0.003) 1 Patients with primary mitral regurgitation have an excess mortality rate of 6.3% per year 2 Within 10-years, the incidence of atrial fibrillation is ~30% and incidence of clinical heart failure is 63% 2 Sudden death accounts for ~25% of deaths in the symptomatic patients with severe mitral regurgitation on medical therapy 3 Patients with secondary (functional) mitral regurgitation (ischemic and non-ischemic) have increased incidence of adverse outcomes at smaller calculated regurgitation orifice area than for primary mitral regurgitation 4 1 Mirabel M, et al. Eur Heart J 2007; 28: Carabello BA. Mod Concepts Cardiovassc Dis 1988; 57: Grigioni F, et al. J Am Coll Cardiol 1999; 34: Nishimura RA, et al. Lancet 2016; 387:
5 Does the presence of functional MR portend worse outcomes? Prognosis of quantitatively determined secondary MR in patients with ischemic and non-ischemic cardiomyopathy Asgar A, et al. J Am Coll Cardiol 2015; 65:
6 Recommendations for the treatment of chronic, severe primary mitral regurgitation ACC/AHA guidelines on the management of valvular heart disease (2017 update) Recommendation COR LOE Mitral valve surgery is recommended for symptomatic patients with chronic severe primary MR and LVEF >30% Mitral valve surgery is recommended for asymptomatic patients with chronic severe primary MR and LVEF 30-60% and/or LVESD >40 mm Mitral valve repair is recommended in preference to MVR when surgical treatment is indicated for patients with chronic severe primary MR involving the AMVL or both leaflets when a successful and durable repair can be accomplished Concomitant MV repair or MVR is indicated in patients with chronic severe primary MR undergoing cardiac surgery for other indications Mitral valve repair is reasonable in asymptomatic patients with chronic severe primary MR with preserved LV (LVEF >60% and LVESD <40 mm) in whom the likelihood of a successful and durable repair without residual MR is >95% with <1% mortality I I I I IIa B B B B B
7 Recommendations for the treatment of chronic, severe primary mitral regurgitation ACC/AHA guidelines on the management of valvular heart disease (2017 update) Recommendation COR LOE Mitral valve surgery is reasonable for asymptomatic patients with chronic severe primary MR and preserved LV function (LVEF >60% and LVESD <40 mm) with a progressive increase in LV size or decrease in LVEF on serial imaging studies Mitral valve repair is reasonable for asymptomatic patients with chronic severe nonrheumatic primary MR with preserved LV function (LVEF >60 and LVESD <40 mm) in whom there is a high likelihood of a successful and durable repair with (1) new onset AF or (2) resting pulmonary hypertension (PASP >50 mmhg) Mitral valve surgery may be considered in symptomatic patients with chronic severe primary MR and LVEF <30% Transcatheter mitral valve repair may considered for severely symptomatic patients (NYHA class III to IV) with chronic severe primary MR who have favorable anatomy for repair procedure and a reasonable life expectancy but who have a prohibitive surgical risk because of severe comorbidities and remain severely symptomatic despite optimal GDMT for heat failure. IIa IIa IIb IIb C B C B
8 Recommendations for the treatment of chronic, severe Secondary mitral regurgitation ACC/AHA guidelines on the management of valvular heart disease (2017 update) Recommendation COR LOE Mitral valve surgery is reasonable for patients with chronic severe secondary MR who are undergoing CABG or AVR It is reasonable to choose chordal-sparing MVR over downsized annuloplasty repair if operation is considered for severely symptomatic patients (NYHA III to IV) with chronic severe ischemic MR and persistent symptoms despite GDMT for HF Mitral valve repair or replacement may be considered for severely symptomatic patients (NYHA III to IV) with chronic severe secondary MR who have persistent symptoms despite optimal GDMT for HF In patients with chronic, moderate, ischemic MR undergoing CABG, the usefulness of mitral valve repair is uncertain Notice no recommendations for catheter-based mitral valve therapies in patients with chronic, severe, symptomatic secondary mitral regurgitation!! IIa IIa IIb IIb C B B B
9 Indications for intervention in severe primary mitral regurgitation ESC guidelines on the management of valvular heart disease (2017) Recommendation COR LOE Mitral valve repair should be the preferred technique when the results are expected to be durable Surgery is indicated in symptomatic patients with LVEF >30% I B Surgery is indicated in asymptomatic patients with LV dysfunction (LVESD >45 mm and/or LVEF <60%) Surgery should be considered in asymptomatic patients with preserved LV function (LVESD <45mm and LVEF >60%) and AF secondary to MR or pulmonary hypertension (PASP >50 mmhg) Surgery should be considered in asymptomatic patients with preserved LVEF (>60%) and LVESD mm when a durable repair is performed in a heart valve center and at least on of the following is present (1) flail leaflet or (2) presence of significant LA dilatation (volume index >60 ml/m 2 BSA) in sinus rhythm I I IIa IIa C B B C
10 Indications for intervention in severe primary mitral regurgitation ESC guidelines on the management of valvular heart disease (2017) Recommendation COR LOE Mitral valve repair should be considered in symptomatic patients with severe LV dysfunction (LVEF <30% and/or LVESD >55 mm) refractory to GDMT when the likelihood of successful repair is low and comorbidity low Mitral valve replacement may be considered in symptomatic patients with severe LV dysfunction (LVEF <30% and/or LVESD >55 mm) refractory to GDMT when the likelihood of successful repair is low and comorbidity low Percutaneous edge-to-edge procedure may be considered in patients with symptomatic severe primary mitral regurgitation who fulfil the echocardiographic criteria for eligibility and are judged inoperable or at high risk by the heart team, avoiding futility IIb IIb IIb C C C
11 Indications for intervention in chronic secondary mitral regurgitation ESC guidelines on the management of valvular heart disease (2017) Recommendation COR LOE Surgery is indicated in patients with severe secondary mitral regurgitation undergoing CABG and LVEF >30% Surgery should be considered in symptomatic patients with severe secondary mitral regurgitation, LVEF <30% but with an option for revascularization and evidence of myocardial viability When revascularization is not indicated, surgery may be considered in patients with severe secondary mitral regurgitation and LVEF >30% who remain symptomatic despite GDMT (including CRT if indicated) and have a low surgical risk When revascularization is not indicated and surgical risk is not low, a percutaneous edge-to-edge procedure may be considered in patients with severe secondary mitral regurgitation and LVEF >30% who remain symptomatic despite GDMT (including CRT if indicated) and who have a suitable valve morphology by echocardiography avoiding futility In patients with severe secondary mitral regurgitation and LVEF <30% who remain symptomatic despite GDMT (including CRT) and who have no option for revascularization, the heat team may consider percutaneous edge-to-edge procedure or valve surgery after careful evaluation for a ventricular assist device or heart transplantation according to individual patient characteristics I IIa IIb IIb IIb C C C C C
12 Re-operation rate vs. Recurrence of significant MR Follow-up studies post standard surgical mitral valve repair technique comparing rates of re-operation and incidence of moderate to severe mitral regurgitation at the last documented follow-up Study/Author Gallinov, et al. Ann Thorac Surg 2000 Tanaka. et al. Am J Cardiol 2003 Flameng, et al. Circulation 2003 N Surgical Technique Re-operation rate % at latest followup (yr) % MR >3+ at latest followup (yr) 197 Carpentier* 5% (5 yr) 9% (1.5 yr) 191 Carpentier* 5.3% (3.7 yr) 7% (3.5 yr) 242 Carpentier* 5.8% (7 yr) 29% (7 yr). *Standard repair with annuloplasty in the vast majority of cases.
13 Is mitral valve repair truly the ultimate panacea? Two-Year Outcomes of Surgical Treatment of Severe Ischemic Mitral Regurgitation Time-to-Event curves for death. The most frequent underlying cause s of death were multisystem organ failure (in 20.8% of patients), Heart failure (in 17.0%) and sepsis (in 13.2%) Goldstein D, et al. N Engl J Med 2016; 374:
 vs. 3.8% in the Replacement group (n=125), p<0.001 Goldstein D, et al. N Engl J Med 2016; 374: 344-353")
14 Is mitral valve repair truly the ultimate panacea? Two-Year Outcomes of Surgical Treatment of Severe Ischemic Mitral Regurgitation Cumulative failure of Mitral-Valve repair or replacement. At 2 years, the rates of moderate to severe MR was 58.8% in the Repair group (n=126) vs. 3.8% in the Replacement group (n=125), p<0.001 Goldstein D, et al. N Engl J Med 2016; 374:

15 The 8 th Emirates Society of Cardiology American College of Cardiology Conference Is mitral valve repair truly the ultimate panacea? Clinical end points, serious adverse events, and hospitalizations at 2 years Goldstein D, et al. N Engl J Med 2016; 374:
16 Characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery Analysis from the Euro Heart Survey One year survival was % in operated patients vs % in the non-operated patients (p=0.003) Factors associated with a decision not to operate Multivariate Analysis P Odds ratio 95% CI LVEF (per 10% decrease) ( ) Aetiology - Ischemic - Non-ischemic ( ) Age (per 10-year increase) ( ) Charlson comorbidity index (per 1 point increase) Degree of Mitral Regurgitation - Grade 4/4 - Grade 3/ ( ) ( ) Mirabel M, et al. Eur Heart J 2007; 28:
, permanent AF, prior ischemic stroke with residual")

17 - Case (1) - 67-year-old female with hypertension, diabetes, chronic kidney disease (egfr= 25 ml/min), permanent AF, prior ischemic stroke with residual right sided motor weakness, recurrent hospitalizations for decompensated HF, severe pulmonary hypertension (PASP ~65 mmhg on 2D transthoracic echocardiography)
 -")

18 - Case (1) -
 -")
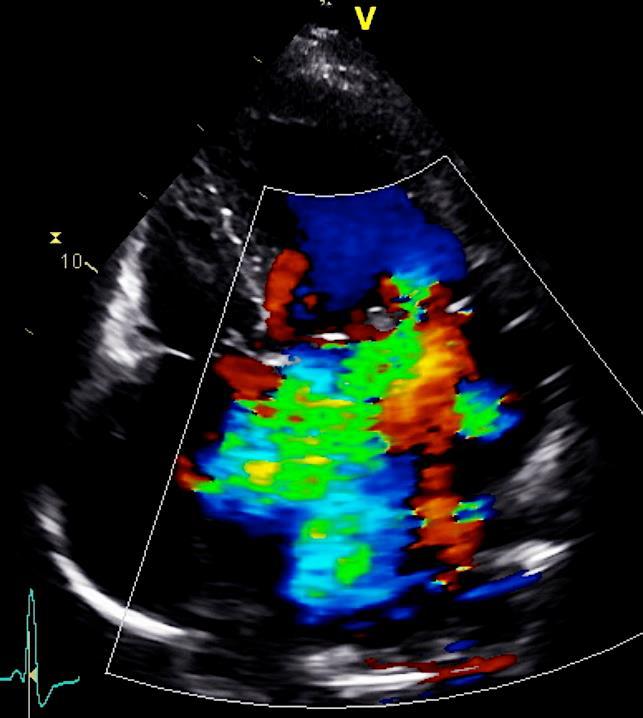
19 - Case (1) -
20 - Case (1) - JA/LA ratio RF 63% RV 84 ml RoA 0.65 cm 2
, chronic kidney disease (egfr= 35 ml/min), permanent AF,")

21 - Case (2) - 55-year-old female with non-ischemic dilated cardiomyopathy with severe LV systolic dysfunction (LVEF ~20%), chronic kidney disease (egfr= 35 ml/min), permanent AF, prior VF arrest post CRT-D implantation, recurrent hospitalizations for decompensated HF despite optimal GDMT, severe pulmonary hypertension (mean PA pressure 50 mmhg from right heart catheterization)
 -")

22 - Case (2) -
23 - Case (1) - MV inflow velocity PV doppler flow & velocities RF 55% RV 60 ml RoA 0.43 cm 2
24 Transcatheter Mitral Valve Repair/Replacement - Device Landscape Coronary sinus annuloplasty Edge-to-Edge MitraClip MitraFlex Direct annuloplasty and basal ventriculoplasty Mitralign Bident GDS Accucinch Valtech Cardioband Quantum Cor (RF) Micardia encor Cardiac Dimensions Carillon Cerclage annuloplasty MV replacement CardiAQ Neovasc Edwards Fortis Micro Interventional Valtech Cardiovalve Valve Xchange Lutter Valve Medtronic Tendyne MitrAssist Mvalve Other approaches MitraSpacer St. Jude leaflet plication Cardiac Implant perc ring NeoChord Babic chords Valtech Vchordal Middle Peak Medical Mardil BACE Mitralis Millipede


25 Transcatheter Mitral Valve Repair - Edge-to-Edge Leaflet Repair - >50,000 implants worldwide MitraClip MitraClip -NT (Abbott Vascular, Santa Clara, CA, USA)





26 Transcatheter Mitral Valve Repair - Edge-to-Edge Leaflet Repair - Systole Diastole Feldman T, et al. N Engl J Med 2011; 364:
 mitral regurgitation at 12 months! Feldman T, et al.")
27 Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Primary efficacy end point at 12 months and major adverse events at 30 days in the intention-to-treat population *Note that in the surgical group, 20% of the patients with complete follow-up data had significant (Grade >3+) mitral regurgitation at 12 months! Feldman T, et al. N Engl J Med 2011; 364:
28 Feldman T, et al. N Engl J Med 2011; 364: Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial -
29 Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Subgroup analyses for the primary end point at 12 months. Shown are the difference in rates of the primary efficacy endpoint (freedom from death, from mitral valve surgery, and from grade 3+ to 4+ mitral regurgitation) between patients in the percutaneous repair group and those in the surgery group for all randomized patients Feldman T, et al. N Engl J Med 2011; 364:

30 Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Secondary End points at 12 months in the intention-to-treat population - Effects on LV remodeling as studies on echocardiography - Feldman T, et al. N Engl J Med 2011; 364:

31 Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Secondary End points at 12 months in the intention-to-treat population - Effects on Quality of Life measures - Feldman T, et al. N Engl J Med 2011; 364:

32 Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Secondary End points at 12 months in the intention-to-treat population - Effects on Quality of Life measures - Feldman T, et al. N Engl J Med 2011; 364:


33 Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation - 5-year results of the EVEREST II trial - Freedom from death Freedom from death, MV surgery or reoperation Freedom from MV surgery or reoperation Feldman T, et al. J Am Coll Cardiol 2015; 66:

34 Feldman T, et al. J Am Coll Cardiol 2015; 66: Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation - 5-year results of the EVEREST II trial - Severity of MR and Heart Failure Symptoms Post- Treatment For patients who survived to 5 years comparisons are seen for: (A) echocardiographic severity of residual MR in 101 of 40 patients in the device and surgery arms, respectively, and (B) New York Heart Association (NYHA) functional class in 105 and 40 patients in the device and surgery arms, respectively, MR= Mitral Regurgitation.

35 Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation - 5-year results of the EVEREST II trial - Secondary MR in heart failure: Interaction between the etiology of MR and the relative success of MV surgery and MitraClip in the Randomized EVEREST II Trial Asgar A, et al. J Am Coll Cardiol 2015; 65:
 http://clinicaltrials.")
36 Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation - The COAPT Trial Study start date: Aug Estimated primary completion date: Jul 2018 (final data collection date for primary outcome measures)
37 Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation - The COAPT Trial - Primary Endpoints: Primary effectiveness (minimum 1-year follow-up on all patients) Recurrent heart failure hospitalizations Primary Safety (1-year) Composite of single leaflet device attachment (SLDA), device embolization, endocarditis requiring surgery, echocardiography core laboratory confirmed mitral stenosis requiring surgery, any device related complications requiring non-elective cardiovascular surgery at 12 months. Secondary Endpoints: Secondary effectiveness MR severity at 12 months Changes in 6MWD at 12 months Change in QoL score (KCCQ) at 12 months Change in LVEDV at 12 months Reduction in NYHA functional class I/II at 12 months Hierarchical composite of death and recurrent HF hospitalizations Recurrent hospitalizations (all cause) Secondary Safety Composite of death (all-cause), stroke, MI, non-elective CV surgery device related complications in device group at 30 days

38 Comparison of Ongoing Randomized Trials of the MitraClip in Patients With Heart Failure and Secondary Mitral Regurgitation Asgar A, et al. J Am Coll Cardiol 2015; 65:

39 Transcatheter Mitral Valve Repair - Indirect Annuloplasty - Carillon Mitral Countour System (Cardiac Dimensions Inc., Kirkland, WA, USA) >600 implants worldwide
 safety after the procedure - Assessment of FMR reduction (quantitative and semi-quantitative evaluation")
40 Percutaneous Mitral Annuloplasty for Functional MR - Results of the CARILLON Mitral Annuloplasty Device European Union (AMADEUS) Study - Primary objective - Evaluate the safety of deploying the CARILLON implant in patients with FMR Secondary objective - Assessment of long-term (6 month) safety after the procedure - Assessment of FMR reduction (quantitative and semi-quantitative evaluation by echocardiography) - Assessment of clinical efficacy through changes in NYHA functional class, exercise tolerance and quality of life Eurointervention Sep 2017; Suppl AA, Vol 13 Courtesy of Prof. M. Haude




41 AMADEUS Study - Effect of the CARILLON device implantation on the severity of mitral regurgitation - Mitral regurgitant JA/LA area ratio Regurgitant Volume Effective regurgitant orifice area Vena contracta Schofer J, et al. Circulation 2009; 120:

 (n/n) At 6 months (n=26) (n/n) P Changes in the 6 min walk distance NYHA class I 0 (0/30) 17 (5/29) 36")
42 Schofer J, et al. Circulation 2009; 120: AMADEUS Study - Effect of the CARILLON device implantation on the severity of mitral regurgitation - Changes in KCCQ score Changes in NYHA classification Baseline (n=30) (n/n) At 1 month (n=29) (n/n) At 6 months (n=26) (n/n) P Changes in the 6 min walk distance NYHA class I 0 (0/30) 17 (5/29) 36 (9/25) II 20 (6/30) 62 (18/29) 52 (13/25) III 73 (22/30) 17 (5/29) 12 (3/25) IV 7 (2/30) 3 (1/29) 0 (0/25) <0.001

43 AMADEUS Study - Effect of the CARILLON device implantation LV remodeling - Hemodynamic changes for 30 implanted patients Schofer J, et al. Circulation 2009; 120:
44 Treatment of functional MR by percutaneous annuloplasty The TITAN Study Comparison of clinical outcome measures between implanted (n=36) and nonimplanted (n=17) patients assessed by 6 MWD and KCCQ Siminiak T, et al. Eur J Heart Fail 2012; 14:
45 The TITAN Study - Echocardiographic Outcomes - Echocardiographic changes in functional MR severity between implanted (n=36) and non-implanted (n=17) patients Siminiak T, et al. Eur J Heart Fail 2012; 14:
46 The TITAN Study - Echocardiographic Outcomes - Echocardiographic changes in LV dimensions between implanted (n=36) and non-implanted (n=17) patients Siminiak T, et al. Eur J Heart Fail 2012; 14:
47 The TITAN II Trial (mxe2) - Echocardiographic Outcomes - 6MWT results showing improvement from baseline at 1, 6 and 12 months in patients receiving an implant (mean + SE of mean) Lipiecki J, et al. Open Heart 2016; 3: e000411
48 The TITAN II Trial (mxe2) - Echocardiographic Outcomes - Quantitative parameters of mitral regurgitation demonstrating improvements from baseline (mean + SE of mean) Plot of mitral annular (A-P) diameter at1, 6, and 12 months, showing mean + SE of mean Lipiecki J, et al. Open Heart Lipiecki 2016; J, et 3: al. e Open Heart 2016; 3: e000411

49 Chordal Replacement - NeoChord DS 1000 system - Vahanian A, et al. Eurointervention 2017; 13: AA22-AA30


50 Chordal Replacement - NeoChord DS 1000 system - Vahanian A, et al. Eurointervention 2017; 13: AA22-AA30


51 Direct Annulplasty - Cardioband - Vahanian A, et al. Eurointervention 2017; 13: AA22-AA30
 Interpid (Medtronic): Feasibility trial (F) HighLife: feasibility trial (G) Caisson: preclinical trials underway (H) Navi Mitral Valved Stent: preclinical trial Patel A, et al.")
52 Transcathter Mitral Valve Replacement - Device Landscape and Stage of Development - (A)CardiAQ valve system: Feasibility Trial (B) FORTIS valve: on hold (C)Tiara: Feasibility trial (D)Tendyne Valve: feasibility trial (E) Interpid (Medtronic): Feasibility trial (F) HighLife: feasibility trial (G) Caisson: preclinical trials underway (H) Navi Mitral Valved Stent: preclinical trial Patel A, et al. Eurointervention 2017; 13: AA31-AA39
53 Guidelines recommendations for catheter-based intervention for chronic, severe mitral regurgitation 2017 Focused update of the 2014 ACC/AHA guidelines on the management of valvular heart disease Recommendation COR LOE Transcatheter mitral valve repair may considered for severely symptomatic patients (NYHA class III to IV) with chronic severe primary MR who have favorable anatomy for repair procedure and a reasonable life expectancy but who have a prohibitive surgical risk because of severe comorbidities and remain severely symptomatic despite optimal GDMT for heat failure. no recommendations for catheter-based mitral valve therapies in patients with chronic, severe, symptomatic secondary mitral regurgitation!! IIb B
54 Guidelines recommendations for catheter-based intervention for chronic, severe mitral regurgitation 2017 ESC guidelines for the management of valvular heart disease Recommendation COR LOE Percutaneous edge-to-edge procedure may be considered in patients with symptomatic severe primary mitral regurgitation who fulfil the echocardiographic criteria for eligibility and are judged inoperable or at high risk by the heart team, avoiding futility When revascularization is not indicated and surgical risk is not low, a percutaneous edge-to-edge procedure may be considered in patients with severe secondary mitral regurgitation and LVEF >30% who remain symptomatic despite GDMT (including CRT if indicated) and who have a suitable valve morphology by echocardiography avoiding futility In patients with severe secondary mitral regurgitation and LVEF <30% who remain symptomatic despite GDMT (including CRT) and who have no option for revascularization, the heat team may consider percutaneous edge-to-edge procedure or valve surgery after careful evaluation for a ventricular assist device or heart transplantation according to individual patient characteristics IIb IIb IIb C C C
55 Contemporary Management of Chronic Severe Mitral Regurgitation Hatim Al Lawati MD, FRCPC, FACC Consultant Interventional Cardiology Sultan Qaboos University Hospital Oman
56 Additional Slides
, permanent AF, prior ischemic stroke with residual")

57 - Case (1) - 67-year-old female with hypertension, diabetes, chronic kidney disease (egfr= 25 ml/min), permanent AF, prior ischemic stroke with residual right sided motor weakness, recurrent hospitalizations for decompensated HF, severe pulmonary hypertension (PASP ~65 mmhg on 2D transthoracic echocardiography)
 -")
58 - Case (1) -
 -")
59 - Case (1) -
 -")


60 - Case (1) - JA/LA ratio RF 63% RV 84 ml RoA 0.65 cm 2



61 - Case (2) - 55-year-old female with non-ischemic dilated cardiomyopathy with severe LV systolic dysfunction (LVEF ~20%), chronic kidney disease (egfr= 35 ml/min), permanent AF, prior VF arrest post CRT-D implantation, recurrent hospitalizations for decompensated HF despite optimal GDMT, severe pulmonary hypertension (mean PA pressure 50 mmhg from right heart catheterization)
62 - Case (2) -


63 - Case (1) - MV inflow velocity PV doppler flow & velocities RF 55% RV 60 ml RoA 0.43 cm 2
64 Indications for percutaneous edge-to-edge treatment in mitral regurgitation Optimal valve morphology Conditionally suitable valve morphology Unsuitable valve morphology Central pathology in segment 2 Pathology in segment 1 or 3 Perforated mitral valve leaflet of cleft No leaflet calcification Mitral valve opening >4 cm 2 Mobile length of the posterior leaflet >10 cm Coaptation depth <11 mm Normal leaflet strength and mobility Flail width <15 mm Flail gap <10 mm Mild calcification outside the grip zone of the clip Mitral valve opening area >3 cm 2 with good residual mobility Mobile lenth of the posterior leaflet 7-10 mm Coaptation depth >11 mm Leaflet restriction in systole (Carpentier IIIB) Flail width >15 mm only with a large ring width and the option for multiple clips Severe calcification in the grip zone Hemodynamically significant mitral stenosis (valve area <3 cm 2, mean gradient >5 mmhg) Mobile length of the posterior leaflet <7 mm Rheumatic leaflet thickening and restriction in systole and diastole (Carpentier IIIA) Barlow s syndrome with multisegment flail leaflets. Boekstegers P, et al. Clin Res Control 2014; 103: 85-96
65 Does the presence of functional MR portend worse outcomes? Relation of frequency and severity of mitral regurgitation to survival among patients with left ventricular systolic dysfunction and heart failure Relation between MR grade and hazard (risk) of death Adjusted survival estimates Schofer J, et al. Circulation 2009; 120:
66 Does the presence of functional MR portend worse outcomes? Relation of frequency and severity of mitral regurgitation to survival among patients with left ventricular systolic dysfunction and heart failure Ischemic Cardiomyopathy Non- Ischemic Cardiomyopathy Schofer J, et al. Circulation 2009; 120:
67 Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Feldman T, et al. N Engl J Med 2011; 364:
68 The 8 th ESC-ACC jointed Conference Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Primary Efficacy End Point at 12 months in the intention-to-treat population Feldman T, et al. N Engl J Med 2011; 364:

69 The 8 th ESC-ACC jointed Conference Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Major Adverse Events at 30 days in the intention-to-treat population Feldman T, et al. N Engl J Med 2011; 364:
70 Contemporary Management of Chronic Severe Mitral Regurgitation.avi format media slides for presentation
71 The 8 th ESC-ACC jointed Conference Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Primary Efficacy end point at 12 months of follow in the intention-to-treat population Event Freedom from death, from surgery for mitral-valve dysfunction, and from grade 3+ or 4+ mitral regurgitation Percutaneous Repair No.(%) Surgery No.(%) P Value 100(55) 65(73) Death 11(6) 5(6) 1.00 Surgery for mitral-valve dysfunction 37(20) 2(2) <0.001 Grade 3+ or 4+ mitral regurgitation 38(21) 18(20) 1.00 Feldman T, et al. N Engl J Med 2011; 364:
72 The 8 th ESC-ACC jointed Conference Percutaneous Repair or Surgery for Mitral Regurgitation - The EVEREST II Trial - Event Major adverse event at 30 days Percutaneous Repair No.(%) Surgery No.(%) P Value Any major adverse event 27(15) 45(48) <0.001 Any major adverse event excluding transfusion 9(5) 9(10) 0.23 Death 2(1) 2(2) 0.89 Myocardial infarction 0 0 NA Re-operation for failed surgical repair or replacement 0 1(1) 0.74 Urgent or emergency cardiovascular surgery for adverse event 4(2) 4(4) 0.57 Major stroke 2(1) 2(2) 0.89 Renal failure 1(<1) Deep wound infection 0 0 NA Mechanical ventilation for >48 hours 0 4(4) 0.02 Gastrointestinal complications requiring surgery 2(1) New onset permanent atrial fibrillation 2(1) Septicemia 0 0 NA Transfusion of >2 units of blood 24(13) 42(45) <0.001 Feldman T, et al. N Engl J Med 2011; 364:

73 The 8 th Emirates Society of Cardiology American College of Cardiology Conference Transcatheter Mitral Valve Repair - Leaflet Repair - Alfieri Stitch MitraClip
Percutaneous Therapy for Mitral Regurgitation: Current and Future Options: Could we do better today?
 Percutaneous Therapy for Mitral Regurgitation: Current and Future Options: Could we do better today? Peter S. Fail, MD, FACC, FACP, FSCAI Director of the Cardiac Catheterization Laboratories and Interventional
Percutaneous Therapy for Mitral Regurgitation: Current and Future Options: Could we do better today? Peter S. Fail, MD, FACC, FACP, FSCAI Director of the Cardiac Catheterization Laboratories and Interventional
Transcatheter Mitral Innovations, Part II. Michael Mack, M.D. Baylor Scott & White Health
 Transcatheter Mitral Innovations, Part II Michael Mack, M.D. Baylor Scott & White Health Conflict of Interest Disclosure Co-PI of the COAPT Trial of MitraClip sponsored by Abbott Vascular Uncompensated
Transcatheter Mitral Innovations, Part II Michael Mack, M.D. Baylor Scott & White Health Conflict of Interest Disclosure Co-PI of the COAPT Trial of MitraClip sponsored by Abbott Vascular Uncompensated
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC
 TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
Emerging Mitral Technologies Where Are We Now? MICHAEL MACK, MD BAYLOR SCOTT & WHITE HEALTH DALLAS, TX
 Emerging Mitral Technologies Where Are We Now? MICHAEL MACK, MD BAYLOR SCOTT & WHITE HEALTH DALLAS, TX Conflict of Interest Disclosure Abbott Vascular- Co PI COAPT Trial Medtronic- Executive Committee
Emerging Mitral Technologies Where Are We Now? MICHAEL MACK, MD BAYLOR SCOTT & WHITE HEALTH DALLAS, TX Conflict of Interest Disclosure Abbott Vascular- Co PI COAPT Trial Medtronic- Executive Committee
Outline 9/17/2016. Advances in Percutaneous Mitral Valve Repair and Replacement. Scope of the Problem and Guidelines
 Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Current status: Percutaneous mitral valve therapy
 Current status: Percutaneous mitral valve therapy Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital ESC Stockholm 2010 Disclosures Research Grants Abbott, Edwards Consultant Abbott, Edwards 2 Percutaneous
Current status: Percutaneous mitral valve therapy Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital ESC Stockholm 2010 Disclosures Research Grants Abbott, Edwards Consultant Abbott, Edwards 2 Percutaneous
Transcatheter Mitral Valve Interventions: Clinical Indications. Didier TCHETCHE, MD. Clinique Pasteur, Toulouse, France.
 Transcatheter Mitral Valve Interventions: Clinical Indications Didier TCHETCHE, MD. Clinique Pasteur, Toulouse, France. Conflicts of interest: -Consultant for Medtronic -Consultant for Cephea Anatomy of
Transcatheter Mitral Valve Interventions: Clinical Indications Didier TCHETCHE, MD. Clinique Pasteur, Toulouse, France. Conflicts of interest: -Consultant for Medtronic -Consultant for Cephea Anatomy of
Disclosure Statement of Financial Interest Saibal Kar, MD, FACC
 MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT
 Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Percutaneous Mitral Valve Repair
 Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Percutaneous Mitral Valve Therapies
 Percutaneous Mitral Valve Therapies Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical School
Percutaneous Mitral Valve Therapies Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical School
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain
 Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain Device Landscape 2010 PERCUTANEOUS TECHNIQUES Percutaneous indirect annuloplasty Percutaneous direct annuloplasty Edge to Edge ( E-Valve ) Non
Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain Device Landscape 2010 PERCUTANEOUS TECHNIQUES Percutaneous indirect annuloplasty Percutaneous direct annuloplasty Edge to Edge ( E-Valve ) Non
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
Percutaneous mitral valve repair/replacement. Jan Van der Heyden MD, PhD St.Antonius Hospital Nieuwegein
 Percutaneous mitral valve repair/replacement Jan Van der Heyden MD, PhD St.Antonius Hospital Nieuwegein Mitral Valve anatomy Difference between AoV and MV Aortic Valve Mitral Valve Transcatheter Mitral
Percutaneous mitral valve repair/replacement Jan Van der Heyden MD, PhD St.Antonius Hospital Nieuwegein Mitral Valve anatomy Difference between AoV and MV Aortic Valve Mitral Valve Transcatheter Mitral
Mitral Valve Disease. James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN
 Mitral Valve Disease James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN Disclosures Affiliation/Financial Relationship Consulting Fees/Honoraria Speaker Bureau Company Abbott, BSC,
Mitral Valve Disease James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN Disclosures Affiliation/Financial Relationship Consulting Fees/Honoraria Speaker Bureau Company Abbott, BSC,
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management
 Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Percutaneous mitral valve repair: current techniques and results
 Percutaneous mitral valve repair: current techniques and results Ted Feldman, M.D., FSCAI, FACC Angioplasty Summit April 25-27 th th 2007 Seoul, Korea Ted Feldman MD, FACC, FSCAI Disclosure Information
Percutaneous mitral valve repair: current techniques and results Ted Feldman, M.D., FSCAI, FACC Angioplasty Summit April 25-27 th th 2007 Seoul, Korea Ted Feldman MD, FACC, FSCAI Disclosure Information
Prognostic Impact of FMR
 Secondary Mitral Valve Regurgitation in Heart Failure, Age 60 Years From Medical Therapy to Surgical Repair to Transcatheter Intervention The Interventionalist s View Samin K Sharma, MD, FACC, FSCAI Director
Secondary Mitral Valve Regurgitation in Heart Failure, Age 60 Years From Medical Therapy to Surgical Repair to Transcatheter Intervention The Interventionalist s View Samin K Sharma, MD, FACC, FSCAI Director
Burden of Mitral Regurgitation (MR) in the US Why is This Important?
 in the US Why is This Important?") Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Mitral Regurgitation
 Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL
 PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Alec Vahanian,FESC, FRCP (Edin.) Bichat Hospital University Paris VII, Paris, France
 Bichat Hospital University Paris VII, Paris, France") Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Percutaneous Mitral Valve Repair
 Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F.
 Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease
 2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ
 Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ Carpentier MV Classification- Leaflet Mobility Normal Increased Decreased Mobility
Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ Carpentier MV Classification- Leaflet Mobility Normal Increased Decreased Mobility
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII
 Bichat hospital University Paris VII") When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream
 Going Mainstream") The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott. Chairperson: M. Haude Panellists: A. Al Nooryani, M.
 Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott Chairperson: M. Haude Panellists: A. Al Nooryani, M. Al Otaiby Session objectives To learn about the clinical patient profile for
Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott Chairperson: M. Haude Panellists: A. Al Nooryani, M. Al Otaiby Session objectives To learn about the clinical patient profile for
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Sergio Berti Ospedale del Cuore Fondazione C.N.R. Reg Toscana Massa/Pisa
 Sergio Berti Ospedale del Cuore Fondazione C.N.R. Reg Toscana Massa/Pisa Prevalence of Valvular Disease The Lancet, Vol. 368, Nkomo, V. T. et al., Burden of valvular heart diseases: a population-based
Sergio Berti Ospedale del Cuore Fondazione C.N.R. Reg Toscana Massa/Pisa Prevalence of Valvular Disease The Lancet, Vol. 368, Nkomo, V. T. et al., Burden of valvular heart diseases: a population-based
Organic mitral regurgitation
 The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
Percutaneous mitral annuloplasty. Francesco Maisano MD, FESC San Raffaele Hospital Milano, Italy
 Percutaneous mitral annuloplasty Francesco Maisano MD, FESC San Raffaele Hospital Milano, Italy Disclosure Consultant for Abbott, Medtronic, St Jude, Edwards, ValtechCardio Founder of 4Tech Surgical techniques
Percutaneous mitral annuloplasty Francesco Maisano MD, FESC San Raffaele Hospital Milano, Italy Disclosure Consultant for Abbott, Medtronic, St Jude, Edwards, ValtechCardio Founder of 4Tech Surgical techniques
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας
 Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Percutaneous Repair for MR:
 Percutaneous Repair for MR: Follow-up and longer term outcomes Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital 16th ANGIOPLASTY SUMMIT TCT Asia Pacific 2011 April 27-29 th Seoul, Korea Ted Feldman
Percutaneous Repair for MR: Follow-up and longer term outcomes Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital 16th ANGIOPLASTY SUMMIT TCT Asia Pacific 2011 April 27-29 th Seoul, Korea Ted Feldman
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Percutaneous Treatment of Mitral Insufficiency: Present and Future
 Percutaneous Treatment of Mitral Insufficiency: Present and Future Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine Seattle, WA
Percutaneous Treatment of Mitral Insufficiency: Present and Future Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine Seattle, WA
Status Of The MitraClip: Trials (EVEREST II & COAPT) & FDA
 & FDA") Status Of The MitraClip: Trials (EVEREST II & COAPT) & FDA Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas, Nevada December 8 11 th, 2013 Ted Feldman MD, FACC, FESC,
Status Of The MitraClip: Trials (EVEREST II & COAPT) & FDA Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas, Nevada December 8 11 th, 2013 Ted Feldman MD, FACC, FESC,
Next Generation Therapies: Aortic, Mitral and Beyond
 Next Generation Therapies: Aortic, Mitral and Beyond Scott M Lilly, MD PhD Medical (Interventional) Director, Structural Heart Program Heart Summit, Lima OH August 26 th, 2017 Next Generation Therapies:
Next Generation Therapies: Aortic, Mitral and Beyond Scott M Lilly, MD PhD Medical (Interventional) Director, Structural Heart Program Heart Summit, Lima OH August 26 th, 2017 Next Generation Therapies:
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
MitraClip World Wide Commercial Experience
 MitraClip World Wide Commercial Experience Valves Repaired. Lives Improved. Carlos G. Hernandez, MBA Sr. Product Manager, Strategic Planning Abbott Vascular October, 2014 MitraClip Transcatheter Mitral
MitraClip World Wide Commercial Experience Valves Repaired. Lives Improved. Carlos G. Hernandez, MBA Sr. Product Manager, Strategic Planning Abbott Vascular October, 2014 MitraClip Transcatheter Mitral
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
GDMT for percutaneous mitral valve repair
 GDMT for percutaneous mitral valve repair Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital The 11th Annual Innovations & Trends in Cardiovascular Care New Brunswick, NJ October 18 th 2014 Ted Feldman
GDMT for percutaneous mitral valve repair Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital The 11th Annual Innovations & Trends in Cardiovascular Care New Brunswick, NJ October 18 th 2014 Ted Feldman
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Get Ready for Percutaneous Mitral Valve Approaches
 Get Ready for Percutaneous Mitral Valve Approaches Paul A. Grayburn, MD Baylor Scott and White Healthcare System The Heart Hospital Baylor Plano and Baylor Heart and Vascular Hospital Dallas, TX HOPE Unmet
Get Ready for Percutaneous Mitral Valve Approaches Paul A. Grayburn, MD Baylor Scott and White Healthcare System The Heart Hospital Baylor Plano and Baylor Heart and Vascular Hospital Dallas, TX HOPE Unmet
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
What Is the Role of Mitral Repair in Heart Failure?
 ASK THE EXPERTS What Is the Role of Mitral Repair in Heart Failure? Experts discuss treatment strategies for patients with mitral regurgitation progressing to heart failure. WITH WILLIAM WEIR, MD; STEPHEN
ASK THE EXPERTS What Is the Role of Mitral Repair in Heart Failure? Experts discuss treatment strategies for patients with mitral regurgitation progressing to heart failure. WITH WILLIAM WEIR, MD; STEPHEN
Transcatheter Mitral Valve for fmr: The Era of Too Many Options
 Transcatheter Mitral Valve for fmr: The Era of Too Many Options Isaac George, M.D. Surgical Director, Structural Heart & Valve Center Assistant Professor of Surgery Columbia University Medical Center Disclosure
Transcatheter Mitral Valve for fmr: The Era of Too Many Options Isaac George, M.D. Surgical Director, Structural Heart & Valve Center Assistant Professor of Surgery Columbia University Medical Center Disclosure
MitraClip in the ICCU: Which Patient will Benefit?
 MitraClip in the ICCU: Which Patient will Benefit? DAVID MEERKIN STRUCTURAL A ND CONGENITAL HEART DISEASE UNIT SHAARE ZEDEK MEDICAL CENTER JERUSALEM Conflict of Interest No relevant disclosures Complex
MitraClip in the ICCU: Which Patient will Benefit? DAVID MEERKIN STRUCTURAL A ND CONGENITAL HEART DISEASE UNIT SHAARE ZEDEK MEDICAL CENTER JERUSALEM Conflict of Interest No relevant disclosures Complex
Truly Endoscopic Robotic mitral valve repair The new frontier
 Truly Endoscopic Robotic mitral valve repair The new frontier T. Sloane Guy, MD, MBA Associate Professor, Dir Robotic Cardiac Surgery Department of Cardiothoracic Surgery roboticheartsurgeon.com Disclaimers
Truly Endoscopic Robotic mitral valve repair The new frontier T. Sloane Guy, MD, MBA Associate Professor, Dir Robotic Cardiac Surgery Department of Cardiothoracic Surgery roboticheartsurgeon.com Disclaimers
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Mitral Regurgitation Epidemiology and Classification
 Subject: Transcatheter Mitral Valve Repair Page: 1 of 23 Last Review Status/Date: December 2015 Transcatheter Mitral Valve Repair Description Transcatheter mitral valve repair is a potential alternative
Subject: Transcatheter Mitral Valve Repair Page: 1 of 23 Last Review Status/Date: December 2015 Transcatheter Mitral Valve Repair Description Transcatheter mitral valve repair is a potential alternative
Percutaneous Mitral Interventions. Alec Vahanian, FESC, FRCP (Edin.) Bichat Hospital, Paris University Paris VII
 Bichat Hospital, Paris University Paris VII") Percutaneous Mitral Interventions Alec Vahanian, FESC, FRCP (Edin.) Bichat Hospital, Paris University Paris VII Rationale for Percutaneous Mitral Valve Interventions Mitral valve disease is frequent and
Percutaneous Mitral Interventions Alec Vahanian, FESC, FRCP (Edin.) Bichat Hospital, Paris University Paris VII Rationale for Percutaneous Mitral Valve Interventions Mitral valve disease is frequent and
Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S.
 ACC 2015 LBCT Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S. A report from the STS/ACC TVT Registry Paul Sorajja, MD, Saibal Kar, MD, Amanda Stebbins,
ACC 2015 LBCT Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S. A report from the STS/ACC TVT Registry Paul Sorajja, MD, Saibal Kar, MD, Amanda Stebbins,
Steven F Bolling Professor of Cardiac Surgery University of Michigan
 Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
Use of MitraClip Beyond Everest Criteria
 Use of MitraClip Beyond Everest Criteria Takashi Matsumoto, MD Sendai Kousei Hospital Sendai, Japan No Disclosure of Financial Interest Introduction The efficacy and safety of the MitraClip therapy was
Use of MitraClip Beyond Everest Criteria Takashi Matsumoto, MD Sendai Kousei Hospital Sendai, Japan No Disclosure of Financial Interest Introduction The efficacy and safety of the MitraClip therapy was
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens
 MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Corrective Surgery in Severe Heart Failure. Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio
 Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Case Report. Percutaneous Mitral Repair with MitraClip as an Adjunct Therapy of Heart Failure. Introduction. Case Report. Keywords
 Percutaneous Mitral Repair with MitraClip as an Adjunct Therapy of Heart Failure Petherson Susano Grativvol, 1,2 Katiuska Massucatti Grativvol, 1,2 Alberto de Paula Nogueira Jr., 1,2 João Eduardo Tinoco
Percutaneous Mitral Repair with MitraClip as an Adjunct Therapy of Heart Failure Petherson Susano Grativvol, 1,2 Katiuska Massucatti Grativvol, 1,2 Alberto de Paula Nogueira Jr., 1,2 João Eduardo Tinoco
Euro Heart Survey New Programme Sentinel Registry Transcatheter Valve Treatment (TCVT) Carlo Di Mario, London, UK President EAPCI
 Carlo Di Mario, London, UK President EAPCI") Euro Heart Survey New Programme 2009-2012 Sentinel Registry Transcatheter Valve Treatment (TCVT) Carlo Di Mario, London, UK President EAPCI Alan Cribier, Rouen, France Andreas Gruentzig Award 2010 Cardiogenic
Euro Heart Survey New Programme 2009-2012 Sentinel Registry Transcatheter Valve Treatment (TCVT) Carlo Di Mario, London, UK President EAPCI Alan Cribier, Rouen, France Andreas Gruentzig Award 2010 Cardiogenic
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Percutaneous Tricuspid Valve Therapies: The Next Frontier? Is the Tricuspid Valve Relevant? Data and Guidelines for TV Interventions
 Percutaneous Tricuspid Valve Therapies: The Next Frontier? Scott M Lilly, MD PhD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Outline Is the Tricuspid Valve Relevant? Data
Percutaneous Tricuspid Valve Therapies: The Next Frontier? Scott M Lilly, MD PhD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Outline Is the Tricuspid Valve Relevant? Data
VALVULOPATIE: NUOVE SOLUZIONI.
 VALVULOPATIE: NUOVE SOLUZIONI www.fisiokinesiterapia.biz Nkomo, Lancet 2006 ELDERLY POPULATION PROJECTION IN USA 65-84 Years Old 85 and Older 77,2 Millions of people 34,8 4,3 30,5 53,8 6,8 47 14,3 62,9
VALVULOPATIE: NUOVE SOLUZIONI www.fisiokinesiterapia.biz Nkomo, Lancet 2006 ELDERLY POPULATION PROJECTION IN USA 65-84 Years Old 85 and Older 77,2 Millions of people 34,8 4,3 30,5 53,8 6,8 47 14,3 62,9
Functional Mitral Regurgitation
 Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
TREATMENT OF SECONDARY MITRAL REGURGITATION VIA PERCUTANEOUS ANNULOPLASTY
 TREATMENT OF SECONDARY MITRAL REGURGITATION VIA PERCUTANEOUS ANNULOPLASTY This symposium took place on 21st May 215 (13:35-14:35), as part of EuroPCR 215; the official annual meeting of the European Association
TREATMENT OF SECONDARY MITRAL REGURGITATION VIA PERCUTANEOUS ANNULOPLASTY This symposium took place on 21st May 215 (13:35-14:35), as part of EuroPCR 215; the official annual meeting of the European Association
Management of Secondary MR : Insights from CTSN Ischemic MR trial; COAPT and MITRA-FR:
 Management of Secondary MR : Insights from CTSN Ischemic MR trial; COAPT and MITRA-FR: Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute,
Management of Secondary MR : Insights from CTSN Ischemic MR trial; COAPT and MITRA-FR: Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute,
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Mitral regurgitation (MR) is the second most
 is the second most") Current Options for Mitral Annuloplasty and Leaflet Repair The benefits and limitations of today s FDA- and CE Mark approved mitral repair technologies. BY ROBERT SCHUELER, MD, AND JAN-MALTE SINNING, MD,
Current Options for Mitral Annuloplasty and Leaflet Repair The benefits and limitations of today s FDA- and CE Mark approved mitral repair technologies. BY ROBERT SCHUELER, MD, AND JAN-MALTE SINNING, MD,
Imaging MV. Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015
 Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
NON SURGICAL TREATMENT OF CARDIAC DISEASE PETER J SABIA, MD FACC ASSOCIATES IN CARDIOLOGY SILVER SPRING, MARYLAND
 NON SURGICAL TREATMENT OF CARDIAC DISEASE PETER J SABIA, MD FACC ASSOCIATES IN CARDIOLOGY SILVER SPRING, MARYLAND TOPICS ATRIAL SEPTAL DEFECT VSD IHSS PERCUTANEOUS AORTIC VALVE PERCUTANEOUS MITRAL VALVE
NON SURGICAL TREATMENT OF CARDIAC DISEASE PETER J SABIA, MD FACC ASSOCIATES IN CARDIOLOGY SILVER SPRING, MARYLAND TOPICS ATRIAL SEPTAL DEFECT VSD IHSS PERCUTANEOUS AORTIC VALVE PERCUTANEOUS MITRAL VALVE
Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical. The Houston Aortic Symposium February 23-25, 2017
 James S. Gammie, MD Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical The Houston Aortic Symposium February 2-25, 2017 Disclosure Statement of Financial Interest Within
James S. Gammie, MD Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical The Houston Aortic Symposium February 2-25, 2017 Disclosure Statement of Financial Interest Within
Index. B B-type natriuretic peptide (BNP), 76
, 76") Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Cases of mitral valve causing mitral regurgitation: the MV prolapse spectrum CASE
 Cases of mitral valve causing mitral regurgitation: the MV prolapse spectrum Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE Mr. M; 50 Year male presents to internist for
Cases of mitral valve causing mitral regurgitation: the MV prolapse spectrum Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE Mr. M; 50 Year male presents to internist for
Update on Transcatheter Mitral Valve Repair and Replacment
 Update on Transcatheter Mitral Valve Repair and Replacment Vinod H. Thourani, MD Professor of Surgery Chair, Department of Cardiac Surgery Medstar Heart and Vascular Washington Hospital Center Georgetown
Update on Transcatheter Mitral Valve Repair and Replacment Vinod H. Thourani, MD Professor of Surgery Chair, Department of Cardiac Surgery Medstar Heart and Vascular Washington Hospital Center Georgetown
Secondary Mitral Regurgitation: When Should We Intervene?
 /19/17 Secondary Mitral Regurgitation: When Should We Intervene? Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
/19/17 Secondary Mitral Regurgitation: When Should We Intervene? Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
Treatment options in ischaemic mitral regurgitation: surgery, clips, devices?
 Treatment options in ischaemic mitral regurgitation: surgery, clips, devices? Francisco Leyva Conflicts of interest: FL has received advisory board fees from Medtronic Inc, Sorin, St Jude Medical and Abbot.
Treatment options in ischaemic mitral regurgitation: surgery, clips, devices? Francisco Leyva Conflicts of interest: FL has received advisory board fees from Medtronic Inc, Sorin, St Jude Medical and Abbot.
The Key Questions in Mitral Valve Interventions. Where Are We in 2018?
 The Key Questions in Mitral Valve Interventions Where Are We in 2018? Gilles D. DREYFUS, MD, FRCS, FESC Professor of Cardiothoracic Surgery 30 GIORNATE CARDIOLOGICHE TORINESI - OCT 2018 Are guidelines
The Key Questions in Mitral Valve Interventions Where Are We in 2018? Gilles D. DREYFUS, MD, FRCS, FESC Professor of Cardiothoracic Surgery 30 GIORNATE CARDIOLOGICHE TORINESI - OCT 2018 Are guidelines
CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ;
 CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ; Επιµορφωτικά Σεµινάρια Ειδικευοµένων Καρδιολογίας 7 Απριλίου 2012 M Chrissoheris MD FACC THV Department HYGEIA Hospital Degenerative MR (DMR) Usually refers to an anatomic
CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ; Επιµορφωτικά Σεµινάρια Ειδικευοµένων Καρδιολογίας 7 Απριλίου 2012 M Chrissoheris MD FACC THV Department HYGEIA Hospital Degenerative MR (DMR) Usually refers to an anatomic
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Management of TR in Patients Undergoing Mitral Interventions
 Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
APOLLO TMVR Trial Update: Case Presentation
 APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας
 Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας Μυτάς Δημήτρης MD, PhD Επιμ Α ΕΣΥ Σισμανόγλειο Γενικό Νοσοκομείο Αττικής Δηλώνω υπεύθυνα ότι η παρούσα ομιλία δεν επιχορηγείται
Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας Μυτάς Δημήτρης MD, PhD Επιμ Α ΕΣΥ Σισμανόγλειο Γενικό Νοσοκομείο Αττικής Δηλώνω υπεύθυνα ότι η παρούσα ομιλία δεν επιχορηγείται