Valvular Guidelines: The Past, the Present, the Future
|
|
|
- MargaretMargaret Malone
- 5 years ago
- Views:
Transcription

1 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief, JAMA Cardiology No Relationships to Disclose

2


3 The evidence base is limited by an inadequate number of randomized clinical trials
4 Hence, virtually all of the recommendations are based on expert consensus (Level C)

5
6 Stages of Valvular Heart Disease Stage A B C D Definition Risk of valve disease (BAV, MVP, RF, CHF) Mild - moderate asymptomatic disease Severe valve disease but asymptomatic C1: Normal LV function C2: Depressed LV function Severe, symptomatic valve disease
7 Mitral regurgitation Degenerative MR: primary valve disease Functional MR: primary myocardial disease
8 Mitral regurgitation Degenerative MR: primary valve disease Functional MR: primary myocardial disease

9 Mitral regurgitation Indications for mitral valve surgery for degenerative MR?

10 Mitral regurgitation Indications for mitral valve surgery for degenerative MR?
11 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? MR Severity: RV = 68 ml RF = 60% ERO = 0.48 cm 2
12 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? MR Severity: RV = 68 ml RF = 60% ERO = 0.48 cm 2 Severe MR: > 60 ml > 50% > 0.4 cm 2
13 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients class I
14 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction class I class I
15 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction LVEF <60% class I class I
16 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction LVEF <60% LVSD >40mm class I class I
17 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction Pulmonary hypertension class I class I class IIa
18 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction Pulmonary hypertension PASP >50 mmhg at rest class I class I class IIa
19 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction Pulmonary hypertension Atrial fibrillation class I class I class IIa class IIa
20 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction Pulmonary hypertension Atrial fibrillation Normal LV function, repair feasible? class I class I class IIa class IIa?
21 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction Pulmonary hypertension Atrial fibrillation Normal LV function, repair feasible? MV repair to improve survival? class I class I class IIa class IIa?

22 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction Pulmonary hypertension Atrial fibrillation Normal LV function, repair feasible? MV repair to improve survival? What is the natural history? class I class I class IIa class IIa?
23 Mitral regurgitation Indications for mitral valve surgery for degenerative MR? Symptomatic patients Asymptomatic patients LV systolic dysfunction Pulmonary hypertension Atrial fibrillation Normal LV function, repair feasible? class I class I class IIa class IIa Asymptomatic severe degenerative MR: 66% come to surgery in 5 years because of symptoms, LV dysfunction, pulmonary hypertension or AF Long-term postoperative survival is worse if surgery is performed after patients become symptomatic
24 Surgery for Acquired Cardiovascular Disease J Thorac Cardiovasc Surg 2003;125:
25 Survival (percent) Surgery for Acquired Cardiovascular Disease Mitral Regurgitation Survival After Mitral Valve Surgery n=488 J Thorac Cardiovasc Surg 2003;125: Expected 64% 20 p< Time (years) 14 David et al, J Thorac Cardiovasc Surg 2003;126:
26 Survival (percent) Surgery for Acquired Cardiovascular Disease 100 Mitral Regurgitation Survival After Mitral Valve Surgery FC I-II 81% n=488 J Thorac Cardiovasc Surg 2003;125: FC III-IV 58% 20 p< Time (years) David et al, J Thorac Cardiovasc Surg 2003;126:
27 Mitral regurgitation Indications for MV repair for asymptomatic degenerative MR: Chronic severe MR Preserved LV function Experienced surgical center Likelihood of durable repair without residual MR > 95% class IIa

28 Mitral regurgitation Indications for MV repair for asymptomatic degenerative MR: Chronic severe MR Preserved LV function Experienced surgical center Likelihood of durable repair without residual MR > 95% Preserved LV function Likelihood of durable repair and low risk for surgery, and LA dilatation >60 ml/m2 -- or -- Exercise PAP >60 mmhg class IIa class IIb
29 Mitral regurgitation Indications for MV repair for asymptomatic degenerative MR:! Chronic severe MR Preserved LV function Experienced surgical center Likelihood of durable repair without residual MR > 95%. Repair better than mitral valve replacement Patients should be referred to centers experienced in repair class IIa class I
30 Mitral regurgitation Indications for transcatheter MV repair for severe degenerative MR: Chronic severe MR Severely symptomatic Prohibited surgical risk Reasonable life expectancy class IIb

31 Mitral regurgitation Primary MR: primary valve disease Secondary MR: primary myocardial disease
32 Mitral regurgitation Primary MR: primary valve disease Secondary MR: primary myocardial disease Diagnostic dilemmas Therapeutic dilemmas


33 Imprecision in grading severity of secondary MR What is severe secondary MR?
")
34 Survival (percent) 100 Survival After MI p<0.001 MI without MR ERO 1-19 ERO 20 61% 47% 29% Time (years) Grigioni et al. Circulation 2001;103:
35 Hospital-Free Survival (%) Ischemic or Nonischemic Cardiomyopathy No FMR Mild-Mod FMR 51% 20 0 p< ERO >20 Severe FMR Time (years) 24% 11% 6 7 Rossi et al. Heart 2011;97:

 No FMR Mild-Mod FMR Severe FMR 6 7")
36 Hospital-Free Survival (%) Ischemic or Nonischemic Cardiomyopathy p< EF 34% LVSD 51 mm EF 33% LVSD 53 mm EF 29% LVSD 57 mm Time (years) No FMR Mild-Mod FMR Severe FMR 6 7 Rossi et al. Heart 2011;97: % 24% 11%
37 Mortality (percent) 800 Ischemic Cardiomyopathy p<0.001 p<0.001 Mod-Severe MR 55% Mild MR 47% No MR 30% Time (years) Deja et al. Circulation 2012;125: Deja et al. Circulation 2012
")
38 Mortality (percent) 800 Ischemic Cardiomyopathy p<0.001 p<0.001 EF 25% ESVI 90 ml/m 2 EF 27% ESVI 80 ml/m 2 EF 30% ESVI 73 ml/m 2 Mod-Severe MR Mild MR No MR Time (years) Deja et al. Circulation 2012;125: Deja et al. Circulation 2012
39 Prevalence of MR in Patients with LV Dysfunction N Prevalence MR Yiu et al Circulation % Grigioni et al Circulation % Koelling et al Am Heart J % Trichon et al Am J Cardiol % Robbins et al Am J Cardiol % Cleland et al N Engl J Med % Grayburn et al J Am Coll Cardiol % Bursi et al Circulation % Acker et al J Thorac CV Surg % Di Mauro et al Ann Thorac Surg % Rossi et al Heart % Deja et al Circulation % Onishi et al Circ Heart Fail % * Patients with moderate to severe MR * * *
40 Secondary mitral regurgitation: a marker of a sicker LV - or - a contributor to a sicker LV?
41 Secondary mitral regurgitation: a marker of a sicker LV - or - a therapeutic target? Therapies that produce beneficial reverse remodeling also reduce severity of functional MR
42 Secondary mitral regurgitation Guideline-directed medical therapy for heart failure, including CRT class I
43 Secondary mitral regurgitation Guideline-directed medical therapy for heart failure, including CRT Indications for mitral valve surgery: class I Patients with severe MR undergoing CABG or AVR class IIa
44 Secondary mitral regurgitation Guideline-directed medical therapy for heart failure, including CRT Indications for mitral valve surgery: class I Patients with severe MR undergoing CABG or AVR Severe MR, persistent symptoms despite optimal medical therapy, including CRT class IIa class IIb

45 Secondary mitral regurgitation Guideline-directed medical therapy for heart failure, including CRT Indications for mitral valve surgery: Patients with severe MR undergoing CABG or AVR Severe MR, persistent symptoms despite optimal medical therapy, including CRT Patients with moderate MR undergoing CABG or AVR class I class IIa class IIb class IIb


46 Baseline Optimized Medical Therapy and Biventricular Pacing
47
48 Secondary mitral regurgitation Indications for transcatheter MV repair for severe secondary MR: Severe secondary MR Severely symptomatic Prohibited or high surgical risk Reasonable life expectancy class IIb
49 Prevalence of MR in Patients with LV Dysfunction N Prevalence MR Yiu et al Circulation % Grigioni et al Circulation % Koelling et al Am Heart J % Trichon et al Am J Cardiol % Robbins et al Am J Cardiol % Cleland et al N Engl J Med % Grayburn et al J Am Coll Cardiol % Bursi et al Circulation % Acker et al J Thorac CV Surg % Di Mauro et al Ann Thorac Surg % Rossi et al Heart % Deja et al Circulation % Onishi et al Circ Heart Fail % * Patients with moderate to severe MR * * *
50 Percent Moderate-Severe Mitral Valve Disease ARIC, CHS, CARDIA (n=11,911) Lancet 2006;368: Olmstead County (n=16,501) ,412 subjects < Age Nkomo et al, Lancet 2006;368:
51 Percent Moderate-Severe Aortic Valve Disease ARIC, CHS, CARDIA (n=11,911) Lancet 2006;368: Olmstead County (n=16,501) 28,412 subjects < Age Nkomo et al, Lancet 2006;368:
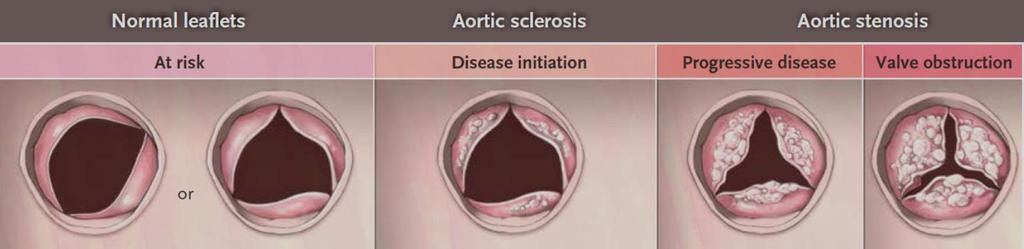
52 Aortic Stenosis Rheumatic AS Congenital AS Calcific AS from Bonow and Braunwald, Valvular Heart Disease Braunwald s Heart Disease, 7th ed, 2004
53 Aortic Stenosis Rheumatic AS Congenital AS Age >60 All patients Men 47% 51% Calcific AS Roberts and Ko, Circulation 2005;111: from Bonow and Braunwald, Valvular Heart Disease Braunwald s Heart Disease, 7th ed, 2004



54 Aortic Stenosis Rheumatic AS Congenital AS Age >80 All patients Men 28% 32% Calcific AS Roberts and Ko, Circulation 2005;111: from Bonow and Braunwald, Valvular Heart Disease Braunwald s Heart Disease, 7th ed, 2004
55

56
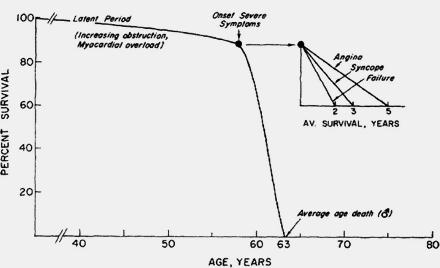
57 Ross and Braunwald, Am J Circulation 1968;38:V-61
58 the grave prognosis that appears to accompany the onset of certain symptoms Ross and Braunwald, Am J Circulation 1968;38:V-61
59 Ross and Braunwald, Am J Circulation 1968;38:V-61

60 Ross and Braunwald, Am J Circulation 1968;38:V-61
 Bach et al, Circ Cardiovasc Qual Outcomes")
61 Survival (percent) Aortic Stenosis Survival of Symptomatic Patients Circ Cardiovasc 100 Qual Outcomes 2009;2: % Time (months) Bach et al, Circ Cardiovasc Qual Outcomes 2009;2:
62 Aortic Stenosis Indications for AVR Symptomatic patients with severe AS class I if it is likely that the symptoms are cardiac in origin
63 Aortic Stenosis Management challenges: The asymptomatic patient with severe AS Low-flow, low gradient severe AS Indications for TAVR
64 Aortic Stenosis Management challenges: The asymptomatic patient with severe AS Low-flow, low gradient severe AS Indications for TAVR
65 Aortic Stenosis Management challenges: The asymptomatic patient with severe AS Low-flow, low gradient severe AS Indications for TAVR Are asymptomatic patients with severe AS really asymptomatic?

66 Aortic stenosis Indications for valve replacement Exercise test results: Symptoms Hypotension class I class IIa How are symptoms determined? Everyone has symptoms on stress test Are the symptoms cardiac in origin? What level of exercise? How is hypotension defined? Less than 20 mmhg increase (?)
67 Aortic stenosis Indications for valve replacement Exercise test results: Symptoms Hypotension class I class IIa Should asymptomatic patients with severe AS undergo AVR? when they are really asymptomatic?


68 Vmax: 4.6 m/s Mean Δ: 52 mmhg AVA: 0.7 sq cm Severe AS: >4.0 m/s >40 mmhg <1.0 sq cm

69 Aortic Stenosis 84 year old man with severe AS Watchful waiting? * More data (more testing)? Aortic valve replacement? * Wait until he develops symptoms in 5-6 years and then recommend TAVR?
70 Event-Free Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Vmax > 4.0 m/s Average hospital mortality: 8.8% Low volume centers: 13.0% High volume centers: 6.0% Otto Time (years) Otto et al. Circulation 1997;95:
71 Event-Free Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Vmax > 4.0 m/s Average hospital mortality: 8.8% Low volume centers: 13.0% High volume centers: 6.0% Otto Rosenhek Time (years) Otto et al. Circulation 1997;95: Rosenhek et al. N Engl J Med 2000;343:
72 Event-Free Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Vmax > 4.0 m/s Average hospital mortality: 8.8% Low volume centers: 13.0% High volume centers: 6.0% Otto Rosenhek Pellikka Time (years) Otto et al. Circulation 1997;95: Rosenhek et al. N Engl J Med 2000;343: Pellikka et al. Circulation 2005;111:
73 Event-Free Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Vmax > 4.0 m/s Average hospital mortality: 8.8% Low volume centers: 13.0% Stewart High volume centers: 6.0% Otto Rosenhek Pellikka Time (years) Otto et al. Circulation 1997;95: Rosenhek et al. N Engl J Med 2000;343: Pellikka et al. Circulation 2005;111: Stewart et al. Eur Heart J 2010;31:
74 Event-Free Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Vmax > 4.0 m/s Average hospital mortality: 8.8% Low volume centers: 13.0% Rosenhek High n=128 volume centers: 6.0% Time (years) Rosenhek et al. N Engl J Med 2000;343:
75 Event-Free Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Average hospital mortality: 8.8% Low volume centers: 13.0% High n=198 volume centers: 6.0% p<0.001 Vmax m/s Vmax m/s Vmax >5.5 m/s Time (years) Rosenhek et al. Circulation 2010;121:
76 Aortic Stenosis Management challenges: The asymptomatic patient with severe AS Low-flow, low gradient severe AS Indications for TAVR What is the risk of death while waiting for symptoms to trigger AVR?
77 Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Average hospital mortality: 8.8% Low volume centers: 13.0% High volume centers: 6.0% Pai Time (years) Pai et al. Ann Thorac Surg 2006;82:
78 Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Kang Average hospital mortality: 8.8% Low volume centers: 13.0% High volume centers: 6.0% Pai Time (years) Pai et al. Ann Thorac Surg 2006;82: Kang et al. Circulation 2010;121:
79 Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Kang Average hospital mortality: 8.8% Low volume centers: 13.0% High volume centers: 6.0% Nistri Pai Time (years) Pai et al. Ann Thorac Surg 2006;82: Kang et al. Circulation 2010;121: Nistri et al. Am J Cardiol 2012;109;
80 Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Kang Average hospital mortality: 8.8% 60 Taniguchi Low volume centers: 13.0% High volume centers: 6.0% Nistri Pai Time (years) Pai et al. Ann Thorac Surg 2006;82: Kang et al. Circulation 2010;121: Nistri et al. Am J Cardiol 2012;109; Taniguchi et al. J Am Coll Cardiol 2105;66:
81 Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Average hospital mortality: 8.8% 60 Taniguchi Low volume centers: 13.0% High volume centers: 6.0% Time (years) Taniguchi et al. J Am Coll Cardiol 2105;66:
82 Survival (%) Natural History of Severe Asymptomatic AS Medicare 80 data Average hospital mortality: 8.8% AVR (n=291) Low volume centers: 13.0% Conservative (n=291) High volume centers: 6.0% 85% 74% Taniguchi 31% of patients who developed symptoms did not have AVR 17 deaths Time (years) Taniguchi et al. J Am Coll Cardiol 2105;66:
83 Asymptomatic Aortic Stenosis Indications for valve replacement: Very severe AS: Vmax 5 m/s class IIa
84 Asymptomatic Aortic Stenosis Indications for valve replacement: Very severe AS: Vmax 5 m/s Rapid progression and low surgical risk class IIa class IIb
85 Asymptomatic Aortic Stenosis Indications for valve replacement: Very severe AS: Vmax 5 m/s Rapid progression and low surgical risk class IIa class IIb Very severe AS: Vmax >5.5 m/s class IIa
86 Asymptomatic Aortic Stenosis Indications for valve replacement: Very severe AS: Vmax 5 m/s Rapid progression and low surgical risk class IIa class IIb Very severe AS: Vmax >5.5 m/s Severe valve calcification and rate of progression 0.3 m/s / year class IIa class IIa
87 Asymptomatic Aortic Stenosis Indications for valve replacement: Very severe AS: Vmax 5 m/s Rapid progression and low surgical risk class IIa class IIb Very severe AS: Vmax >5.5 m/s Severe valve calcification and rate of progression 0.3 m/s / year Markedly elevated BNP Increase in gradient with exercise >20 mmhg Excessive LVH class IIa class IIa class IIb

88 Asymptomatic Aortic Stenosis Indications for valve replacement: The ACC/AHA and ESC/EACTS guidelines have lowered the threshold for surgery in asymptomatic patients with AS Severity of AS Severity of calcification Left ventricular function Exercise response

89 Asymptomatic Aortic Stenosis Indications for valve replacement: The ACC/AHA and ESC/EACTS guidelines have lowered the threshold for surgery in asymptomatic patients with AS Severity of AS Severity of calcification Left ventricular function Exercise response BNP?

90 Survival (percent) Asymptomatic AS with Normal EF n=562 p<0.001 BNP ratio 83% <1.0 66% % % Time (years) Clavel et al, J Am Coll Cardiol 2014;63:
91 Aortic stenosis Management challenges: The asymptomatic patient with severe AS Low-flow, low gradient severe AS Indications for TAVR

92 Low Gradient Aortic Stenosis LV Dysfunction Normal LV Function Diastole Dobutamine: Echocardiography or Catheterization Treat hypertension Catheterization Valve calcification Advanced imaging Clinical skills Systole from Pibarot and Dumesnill, J Am Coll Cardiol 2012:60:
93 Low Flow, Low Gradient Aortic Stenosis Indications for valve replacement: Reduced EF: Dobutamine study showing: Vmax >4 m/s or Mean Δ >40 mmhg or AVA 1 sq cm class IIa Reduced EF: With contractile reserve class IIa
94 Low Flow, Low Gradient Aortic Stenosis Indications for valve replacement: Reduced EF: Dobutamine study showing: Vmax >4 m/s or Mean Δ >40 mmhg or AVA 1 sq cm Normal EF: Only if clinical, anatomic and hemodynamic data support severe AS Reduced EF: With contractile reserve class IIa class IIa class IIa
95 Low Flow, Low Gradient Aortic Stenosis Indications for valve replacement: Reduced EF: Dobutamine study showing: Vmax >4 m/s or Mean Δ >40 mmhg or AVA 1 sq cm Normal EF: Only if clinical, anatomic and hemodynamic data support severe AS Reduced EF: With contractile reserve Normal EF: Only after thorough confirmation of severe AS class IIa class IIa class IIa class IIa


96 Aortic stenosis Management challenges: The asymptomatic patient with severe AS Low-flow, low gradient severe AS Indications for TAVR
97 Intervention for Severe AS Indications for TAVR vs surgical AVR: Evaluation by a Heart Team class I
98 Intervention for Severe AS Indications for TAVR vs surgical AVR: Evaluation by a Heart Team Surgical AVR for patients at low or intermediate risk class I class I
99 Intervention for Severe AS Indications for TAVR vs surgical AVR: Evaluation by a Heart Team Surgical AVR for patients at low or intermediate risk TAVR for patients with prohibitive surgical risk and life expectancy >12 months class I class I class I
100 Intervention for Severe AS Indications for TAVR vs surgical AVR:?? Evaluation by a Heart Team Surgical AVR for patients at low or intermediate risk TAVR as alternative? TAVR for patients with prohibitive surgical risk and life expectancy >12 months TAVR alternative for patients at high surgical risk class I? class I class I class I class IIa


101
102 TAVR Now TAVR has been truly transformative Surgical AVR remains the standard with proven durability and safety for most patients TAVR provides treatment options for patients who previously had no options other than a predictably very poor short term outcome TAVR is an alternative to SAVR in patients at high or intermediate surgical risk The threshold for TAVR is declining in clinical trials, registries and clinical practice All patients want this Determining when to withhold TAVR is difficult
103 TAVR in the Future Guidelines will need to adapt to the rapidly evolving TAVR evidence base TAVR in intermediate and low risk surgical patients Availability of TAVR is likely to inform new indications for valve replacement Moderate AS in primary cardiomyopathy Asymptomatic severe AS? Judgment of the Heart Team remains essential in patient selection for TAVR Appropriate use criteria and performance measures are needed to define quality


104 Aortic stenosis is a simple mechanical fault which, if severe enough, imposes a heavy burden on the left ventricle and sooner or later overcomes it. it s not simple any more Wood P, Am J Cardiol 1958;1:


105 Valvular heart disease: Have the guidelines filled the gap?
Secondary Mitral Regurgitation: When Should We Intervene?
 /19/17 Secondary Mitral Regurgitation: When Should We Intervene? Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
/19/17 Secondary Mitral Regurgitation: When Should We Intervene? Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
Severe Asymptomatic Aortic Stenosis
 Severe Asymptomatic Aortic Stenosis The Clinician s Perspective Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
Severe Asymptomatic Aortic Stenosis The Clinician s Perspective Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
MitraClip: Why, How, and For Whom?
 MitraClip: Why, How, and For Whom? Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief, JAMA Cardiology
MitraClip: Why, How, and For Whom? Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief, JAMA Cardiology
Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines. Christophe Tribouilloy Amiens, France
 Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines Christophe Tribouilloy Amiens, France I have no financial relationships to disclose related
Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines Christophe Tribouilloy Amiens, France I have no financial relationships to disclose related
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Mitral Regurgitation
 Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC
 TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Welcome 17 Michigan TAVR Participating Hospitals!
 Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease
 2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies
 Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern
Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern
Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
 Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F.
 Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis in the Elderly: Difficulties for the Clinician. Are Symptoms Due to Aortic Stenosis?
 Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France
 Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Ischemic Mitral Valve Disease: Repair, Replace or Ignore?
 Ischemic Mitral Valve Disease: Repair, Replace or Ignore? Fabio B. Jatene Full Professor of Cardiovascular Surgery, Medical School, University of São Paulo, Brazil DISCLOSURE I have no financial relationship
Ischemic Mitral Valve Disease: Repair, Replace or Ignore? Fabio B. Jatene Full Professor of Cardiovascular Surgery, Medical School, University of São Paulo, Brazil DISCLOSURE I have no financial relationship
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease Transcatheter Valve Therapies. October 2016 Brian Whisenant MD
 Valvular Heart Disease Transcatheter Valve Therapies October 2016 Brian Whisenant MD Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Valvular Heart Disease Transcatheter Valve Therapies October 2016 Brian Whisenant MD Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Michigan Society of Echocardiography 30 th Year Jubilee
 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
What is the Role of Surgical Repair in 2012
 What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
I have financial relationships to disclose Honoraria from: Edwards
 I have financial relationships to disclose Honoraria from: Edwards Mitral Valve Annuloplasty in Ischemic Mitral regurgitation Jean François Avierinos Hôpital Timone Marseille August 28, 2012 Ischemic MR
I have financial relationships to disclose Honoraria from: Edwards Mitral Valve Annuloplasty in Ischemic Mitral regurgitation Jean François Avierinos Hôpital Timone Marseille August 28, 2012 Ischemic MR
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Secondary MR joint with the mitral academy. What is new in our understanding of this disease? Luc Pierard University Hospital, Liège
 Secondary MR joint with the mitral academy What is new in our understanding of this disease? Luc Pierard University Hospital, Liège Faculty disclosure Luc Pierard I have no financial relationships to disclose.
Secondary MR joint with the mitral academy What is new in our understanding of this disease? Luc Pierard University Hospital, Liège Faculty disclosure Luc Pierard I have no financial relationships to disclose.
Management of Heart Failure in Adult with Congenital Heart Disease
 Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons
 Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Objectives. Systolic Heart Failure: Definitions. Heart Failure: Historical Perspective 2/7/2009
 Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Outline 9/17/2016. Advances in Percutaneous Mitral Valve Repair and Replacement. Scope of the Problem and Guidelines
 Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Aortic Stenosis.
 Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation
 Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation Hatim Al Lawati MD, FRCPC, FACC Consultant Interventional Cardiology Sultan Qaboos University
Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation Hatim Al Lawati MD, FRCPC, FACC Consultant Interventional Cardiology Sultan Qaboos University
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Steven F Bolling Professor of Cardiac Surgery University of Michigan
 Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Aortic stenosis with concomitant mitral regurgitation
 Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT
 Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Affecting the elderly Requiring new approaches. Echocardiographic Evaluation of Hemodynamic Severity. Increasing prevalence Mostly degenerative
 Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes
 Original Article Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes Andrea Colli, Eleonora Bizzotto, Laura Besola, Dario Gregori, Francesca Toto, Erica Manzan,
Original Article Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes Andrea Colli, Eleonora Bizzotto, Laura Besola, Dario Gregori, Francesca Toto, Erica Manzan,
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère asymptomatique de type dégénérative?
 Réunion d automne de la SSC à Lucerne le 24.11.2011 Incertitudes dans le travail cardiologique quotidien Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère
Réunion d automne de la SSC à Lucerne le 24.11.2011 Incertitudes dans le travail cardiologique quotidien Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère
Imaging in dilated cardiomyopathy : factors associated with a poor outcome
 Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
Which Type of Secondary Tricuspid Regurgitation Accompanying Mitral Valve Disease Should Be Surgically Treated?
 Ann Thorac Cardiovasc Surg 2013; 19: 428 434 Online January 31, 2013 doi: 10.5761/atcs.oa.12.01929 Original Article Which Type of Secondary Tricuspid Regurgitation Accompanying Mitral Valve Disease Should
Ann Thorac Cardiovasc Surg 2013; 19: 428 434 Online January 31, 2013 doi: 10.5761/atcs.oa.12.01929 Original Article Which Type of Secondary Tricuspid Regurgitation Accompanying Mitral Valve Disease Should
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative
 Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Surgical Indications of Infective Endocarditis in Children
 2016 Annual Spring Scientific Conference of the KSC April 15-16, 2016 Surgical Indications of Infective Endocarditis in Children Cheul Lee, MD Pediatric and Congenital Cardiac Surgery Seoul St. Mary s
2016 Annual Spring Scientific Conference of the KSC April 15-16, 2016 Surgical Indications of Infective Endocarditis in Children Cheul Lee, MD Pediatric and Congenital Cardiac Surgery Seoul St. Mary s
Burden of Mitral Regurgitation (MR) in the US Why is This Important?
 in the US Why is This Important?") Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Exercise PHT in valvular heart disease. Julien Magne CHU Limoges, France
 Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
CARDIOLOGY GRAND ROUNDS
 CARDIOLOGY GRAND ROUNDS Presentation: Mitral Disease Speakers: Robert S. Farivar, MD, PhD Chief, Cardiothoracic Surgery, Abbott Northwestern Hospital Chairman, Allina Cardiothoracic; Minneapolis Heart
CARDIOLOGY GRAND ROUNDS Presentation: Mitral Disease Speakers: Robert S. Farivar, MD, PhD Chief, Cardiothoracic Surgery, Abbott Northwestern Hospital Chairman, Allina Cardiothoracic; Minneapolis Heart
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL
 PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Corrective Surgery in Severe Heart Failure. Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio
 Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott. Chairperson: M. Haude Panellists: A. Al Nooryani, M.
 Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott Chairperson: M. Haude Panellists: A. Al Nooryani, M. Al Otaiby Session objectives To learn about the clinical patient profile for
Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott Chairperson: M. Haude Panellists: A. Al Nooryani, M. Al Otaiby Session objectives To learn about the clinical patient profile for
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
03/07/ Background. + High Risk Features Are Prevalent in Dialysis Patients
 + When Does Cardiovascular Disease Preclude Consideration of Renal Transplantation? Kul Aggarwal, MD, MRCP (UK), FACC Professor of Clinical Medicine Division of Cardiology University of Missouri & Chief,
+ When Does Cardiovascular Disease Preclude Consideration of Renal Transplantation? Kul Aggarwal, MD, MRCP (UK), FACC Professor of Clinical Medicine Division of Cardiology University of Missouri & Chief,
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ
 Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ Carpentier MV Classification- Leaflet Mobility Normal Increased Decreased Mobility
Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ Carpentier MV Classification- Leaflet Mobility Normal Increased Decreased Mobility
Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ;
 Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
ESC / EACTS new valvular guidelines- Update
 ESC / EACTS new valvular guidelines- Update Yaron Shapira, MD The Dan Sheingarten echocardiography & valve clinic Rabin Medical Center, Beilinson Hospital, Petah-Tiqva Tel-Aviv University ESC valve guidelines
ESC / EACTS new valvular guidelines- Update Yaron Shapira, MD The Dan Sheingarten echocardiography & valve clinic Rabin Medical Center, Beilinson Hospital, Petah-Tiqva Tel-Aviv University ESC valve guidelines
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of