DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES
|
|
|
- Cecil Jackson
- 5 years ago
- Views:
Transcription
1 DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center
2 Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular, Inc. Medtronic NIH Employer-Iowa Heart Center/Mercy-Des Moines
3 Outline Epidemiology Anatomy & Physiology Pathophysiology Risk Factors Natural History of DVT Complications of DVT Diagnosis Treatment Options Guidelines and treatment algorithms Endovascular and Surgical adjuncts to treatment Recommendations
4 Epidemiology and Clinical Significance Annually 900,000 cases of VTE in the US 275,000 new cases annually in the US It is estimated that 684,000 cases of DVT and 434,000 PE with 543,000 fatalities from VTE in the EU 1% incidence with 0.36% mortality in all hospitalized patients
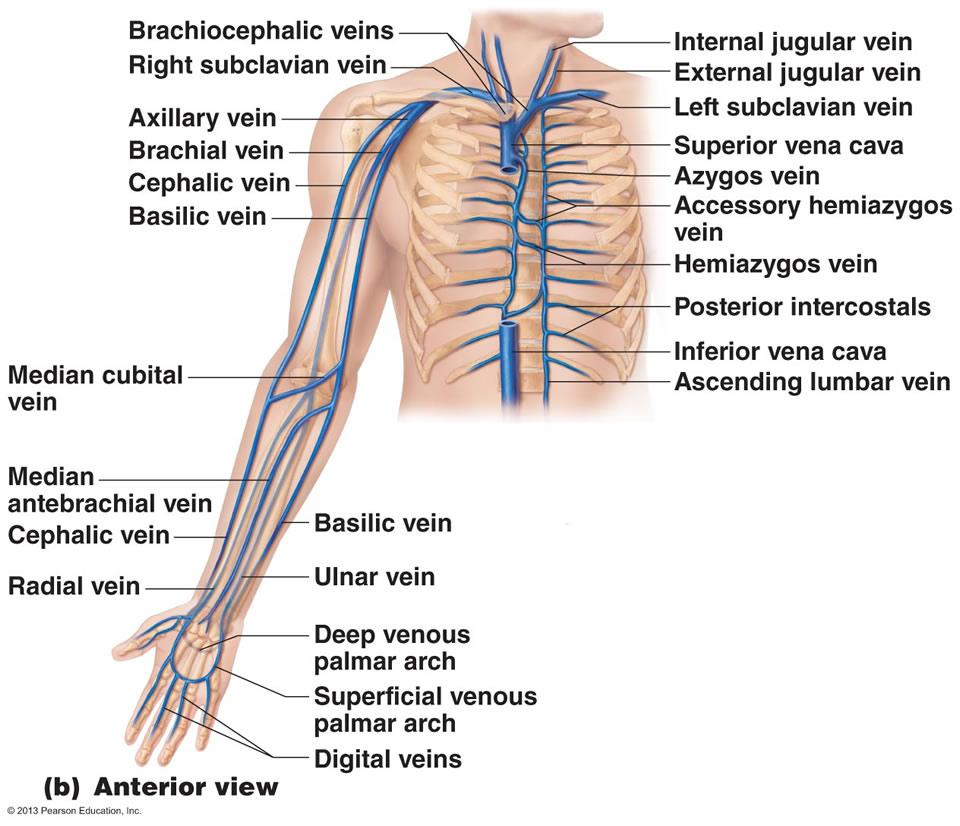
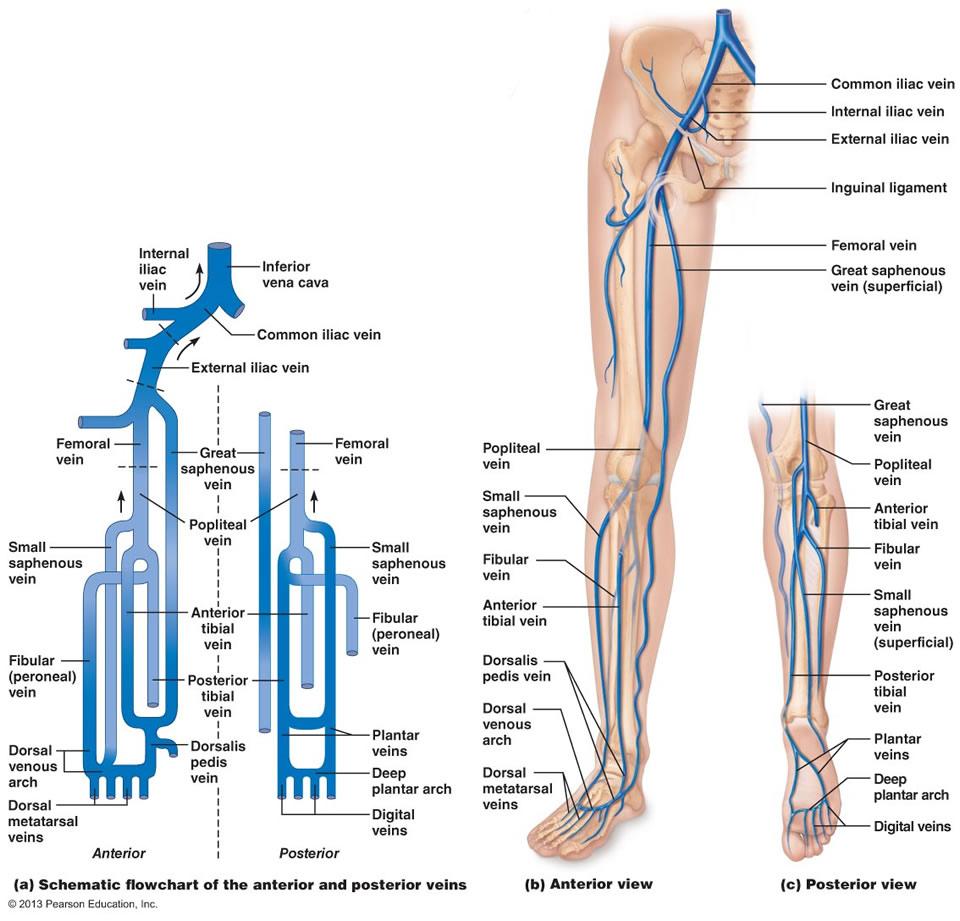
5 ANATOMY The venous anatomy is highly variable compared to the arterial system Components 1. Superficial Veins 2. Deep Veins 3. Perforating Veins
6
7
8
9
10 PHYSIOLOGY 60-70% of blood volume is found in the venous system 80% of this is found in vessels <200 microns in diameter Skeletal muscle related veins are responsive to catecholamines Pressures in the lower extremity venous system are largely determined by gravity and venous system integrity
11 PHYSIOLOGY Venous pressures are increased in the lower extremities Venous flow is pulsatile Valvular closure and integrity are important in blood transport cranially Calf muscle pump creates venous flow Most of the blood flows via the deep system Blood flows from the superficial to the deep veins
12 PATHOPHYSIOLOGY Abnormal functioning of the lower extremity veins results in venous insufficiency Venous insufficiency results from injury to vein walls and valves Tissue changes are a result of prolonged venous hypertension and stasis Inflammation, cellular and molecular modulators result in delayed vascular and cutaneous changes
13 PATHOPHYSIOLOGY OF DVT Virchow s Triad (1850) Stasis Vessel Wall Injury Hypercoagulability Stewart (1974) Thrombosis and inflammation Inflammatory mediators up-regulate procoagulant factors and inhibit fibrinolysis ( Selectins)
14 Pathophysiology of DVT Disturbance in the normal balance of hemostasis and thrombolysis Initial thrombus is composed of RBC and fibrin Subsequent increase in pro-inflammatory factors leading to fibrinolysis and vessel wall fibrosis Clinical effects due to venous obstruction and valvular reflux
15 Complications of DVT Early: Acute Pulmonary Embolism Late: Recurrent Venous thromboembolism (VTE) Post-thrombotic syndrome (PTS)
16 Thrombotic risk factors and Hypercoagulability Congenital Hypercoagulability Factor V Leiden Prothrombin G20210A Protein C Deficiency Protein S Deficiency Antithrombin Factor XI excess Acquired Hypercoagulability Advanced age Antiphospholipid antibodies Malignancy Situational Hypercoagulability Surgery Trauma Pregnancy Oral contraceptives Hormone therapy Adapted from Shalhub S, Meissner M, Therapy in Vascular and Endovascular Surgery, 5 th ed. P. 877.
17
18 Natural History of DVT Proximal extension is variable Recanalization as a normal process of healing as early as 6-12 weeks of an acute event Greater recanalization is seen in patients who present with transient risk factors Prolonged recanalization is proportional to the degree of thrombus burden Greater recurrence of DVT inpatients with diminished recanalization
19 Natural History of DVT Calf veins are the most common site of origin, although 40% arise from the proximal veins In-hospital mortality rate is 5-12% 3 and 5 year mortality rates are 30 and 39% If untreated, 30-50% will develop PE, 10% of which are fatal Incidence of recurrent VTE with treatment is <5%
20 Natural History of DVT 20% of all first time VTE are associated with underlying malignancy 1 in 200 of patients with cancer will develop VTE Most recurrent VTE occurs after anticoagulants have been discontinued ( highest 6 t0 12 after the index event) Cumulative recurrence rates as high as 23%
21 Risk of recurrence is related to the underlying thrombotic risk factors Unprovoked DVT carries a threefold risk of recurrence compared to those with transient risk factors Calf vein DVT have a 23% risk of proximal extension
22 Pulmonary Embolism (PE) Most serious early complication of acute DVT Can occur in up to 50-80% of symptomatic DVT patients Can occur in 7-17% of patients presenting with acute upper extremity DVT Can occur in up to 10% of patients with calf vein DVT ( risk less than 2% for fatal PE)
23 Risk of recurrence of VTE VTE provoked by surgery, 3% at 5 years VTE provoked by transient nonsurgical risk factor, 15% at 5 years Unprovoked VTE not related to cancer, 30% recurrence at 5 years VTE associated with cancer, 15% annual risk of recurrence Distal DVT, ½ risk than after a proximal DVT Second unprovoked DVT/PE, 50% higher
24 Post-thombotic syndrome(pts) Long-term sequelae of LE VTE 29-79% of patients present with some degree of PTS 7-23% have severe manifestations 4-6% develop ulceration Patients who present with recurrent VTE have 6-fold increased incidence of PTS Result from venous hypertension- proximal obstruction and distal reflux


25 Post-Thrombotic Syndrome(PTS)
26 Diagnosis and Clinical Presentation of Acute DVT Calf pain Calf swelling Calf and leg tenderness Prominent superficial veins Pain with foot dorsiflexion (Homan s sign) *Up to 70% of patients with Sx consistent with DVT will not have it, and up to 50% of patients with DVT may lack any specific signs and symptoms
27 Diagnosis and Clinical presentation Variable, ranging from asymptomatic to massive swelling/pitting edema Diagnosis based on clinical probability complemented by objective testing Advanced venous compromise: phlegmasia alba dolens, phlegmasia cerulea dolens


28
29 Differential Diagosis Muscle strain, tear, or twisting injury to the leg 40 percent Leg swelling in a paralyzed limb 9 percent Lymphangitis or lymph obstruction 7 percent Venous insufficiency (reflux) 7 percent Baker's cyst 5 percent Cellulitis 3 percent Knee abnormality 2 percent Unknown 26 percent Hull R, Hirsh J, Circulation, :622.
30
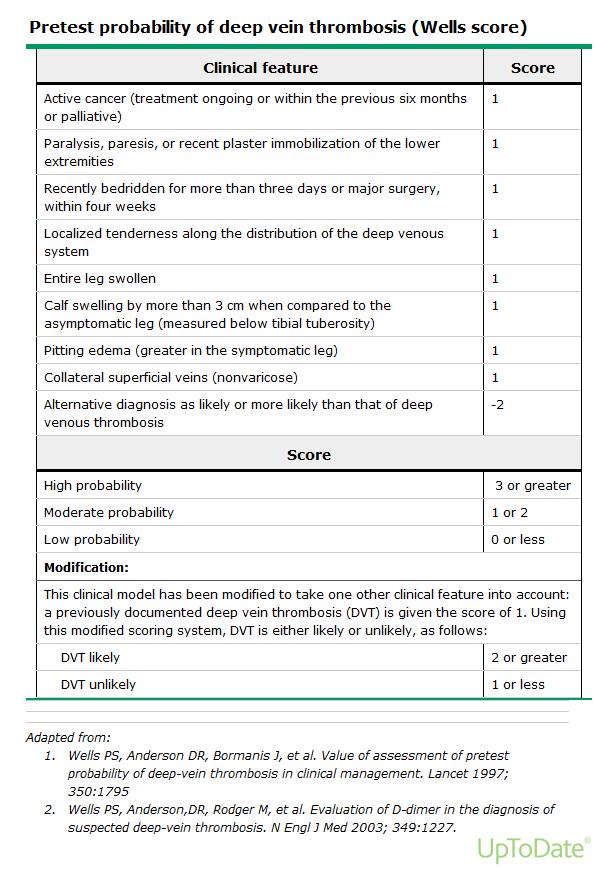
31 Diagnosis Signs and symptoms are nonspecific and of varying specificities Requires confirmatory testing that is resource intensive Duplex ultrasound as the primary diagnostic modality D-Dimer is useful but specificity depends highly on the clinical probability of disease Best strategy incorporates clinical, D-dimer and selective ultrasound evaluation
32 Diagnostic Testing Duplex ultrasound D-Dimer CT venography MR Venography Contrast Venography Impedance plethysmography Isotope Scintigraphy

33 Diagnosis: Compression Ultrasound
34 D-Dimer Products of degradation of cross-linked fibrin by plasmin Reflect the presence of intravascular fibrin, sensitive for thromboembolism Low sensitivity (35%): Elevations seen in DIC, malignancy, post-op states, infection, trauma and pre-eclampsia and with high bilirubin levels Most useful in patients with low pre-test probability of disease and negative result

35 Lohr J and Griffith NM, Rutherford s Vascular Surgery, 7 th ed. p.764

36 Lohr J and Griffith NM. Rutherford s Vascular Surgery, 7 th ed. p. 768.
37 Treatment Extremity elevation- short term Immediate anticoagulation Early Mobilization Compression therapy Limited use of IVC Filter Selective thrombolysis and catheter based interventions
38 Anticoagulation Unfractionated Heparin (UFH) Low Molecular weight heparins (LMWH) Fondaparinux Vitamin K antagonists Direct thrombin inhibitors ( IV Lepirudin, Bivalrudin) Apixaban Rivaroxaban Edoxaban Dabigatran Thrombolysis
39 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015) Shorter duration of initial therapy Role of time-limited and Extended Therapy Recommendations for VTE and malignancy Updates with NOACs Limited role for IVC filters Recommendations for systemic lysis Recommendations for catheter based therapy
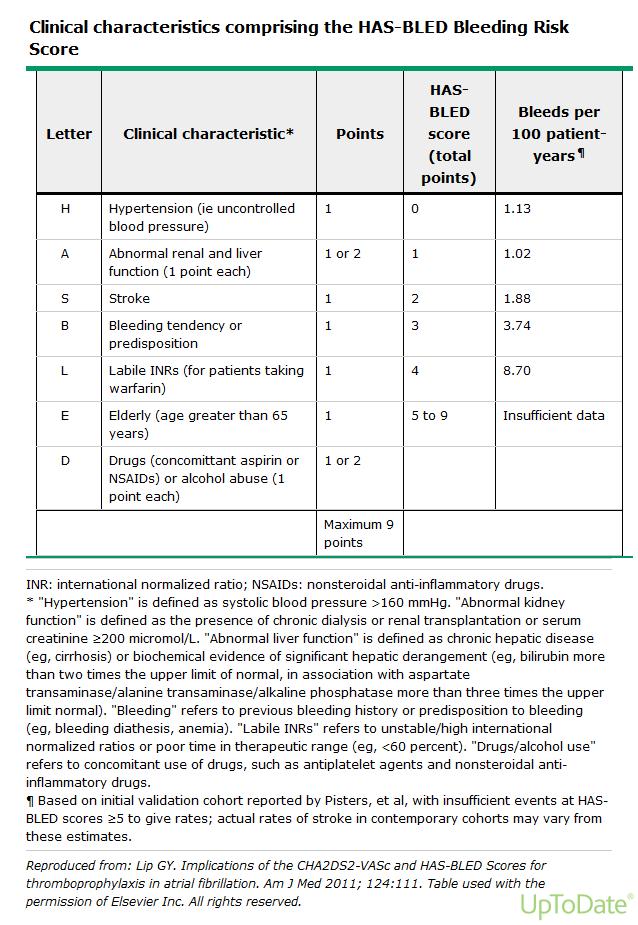
40 Duration of therapy is patient specific Careful risk factor assessment Strong need to evaluate individual patient risks of anticoagulant therapy (HAS BLED) Extended therapy for unprovoked VTE Extended therapy for cancer patients Recommendations for VKA and LMWH and NOACs ( increasing role of new agents)
41 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 Patients with proximal DVT/PE are treated with long-term (3 months) of anticoagulation In absence of cancer, NOACs are suggested over VKA ( and VKA over LMWH) In patients with cancer-associated thrombosis, LMWH is suggested over VKA or NOACs If extended therapy is planned, there is no need to change agent after 3 months
42 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 In patients with proximal DVT/PE provoked by surgery or by nonsurgical transient risk factor, 3 month treatment is recommended. In patients with distal DVT provoked by surgery, 3 month treatment is recommended Patients with UNPROVOKED DVT ( isolated distal or proximal or PE), treatment for AT LEAST 3 months is recommended
43 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 In patients with 1 st episode of UNPROVOKED proximal DVT/PE, with low to moderate bleeding risk, EXTENDED THERAPY ( no stop date) is suggested. In patients with high risk of bleeding, 3 month over extended therapy is recommended. Patients with 2 nd UNPROVOKED VTE with low to moderate bleeding risk, EXTENDED Tx. Those with high bleeding risk, 3 month treatment only is recommended.
44 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 Patients with DVT/PE and cancer, EXTENDED anticoagulation is recommended. ( This is still suggested in high bleeding risk individuals) Patients stopping anticoagulant therapy and without contraindication to ASA, ASA is suggested.
45 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 Patients with distal (calf vein) DVT without severe symptoms or risk for extension, serial imaging for 2 weeks is suggested over anticoagulation. *Pts with high bleeding risk will benefit from serial imaging *Anticoagulation is suggested if patients have severe symptoms, ongoing risk factors for extension or if extension is demonstrated on serial imaging)
46 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 In patients with acute proximal DVT, they suggest anticoagulant therapy alone over catheter directed thrombolysis. Patients with acute DVT/PE treated with anticoagulants, they recommend against the use of an IVC filter. *Patients who are most likely to benefit from CDT who attach a high value to preventing PTS and lower value to complexity, cost and risk of bleeding with CDT are likely to choose CDT over anticoagulation alone.
47 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 Suggest not using compression stockings routinely to prevent PTS. (In patients with acute or chronic symptoms, a trial of compression is justified) In patients with subsegmental PE and no proximal DVT and low risk for recurrent VTE, they suggest clinical surveillance over anticoagulation. (Anticoagulation is suggested in patients with high risk for recurrent VTE)
48 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 In patients with acute PE associated with hypotension without a high bleeding risk, systemic (rather than CDT) is suggested. In patients with high bleeding risk, or failed systemic lysis with shock likely to cause death, catheter assisted thrombus removal is suggested if resources are available.
49 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 Patients with recurrent VTE while on VKA or NOAC, they suggest switching to LMWH at least temporarily. For recurrent VTE while on LMWH, they suggest increasing the dose by ¼ to 1/3.
50 ACCP Guidelines: Antithrombotic Therapy for VTE Disease (Chest Feb 2012, updated Nov 2015 VTE patients who are most likely to benefit from CDT Iliofemoral DVT Symptoms less than 14 days Good functional status Life expectancy greater than 1 year Low risk of bleeding Impending venous related gangrene
51 Table 15: Risk factors for bleeding with, and contraindications to use of thrombolytic therapy (both systemically and locally administered Major Contraindications Structural intracranial disease Previous intracranial hemorrhage Ischemic stroke within 3 months Active bleeding Recent brain or spine surgery Recent head trauma with fracture or brain injury Bleeding diathesis Relative indications Systolic BP>180 Diastolic BP>110 Female Recent bleeding Recent surgery Low BMI Recent invasive procedure Ischemic stroke >3 months Race Ongoing anticoagulation Traumatic CPR Pericarditis/Pericardial fluid DM retinopathy Pregnancy Age > 75 CHEST Guidelines, November 2015.
52
53 Table 11: Risk factors for bleeding with anticoagulant therapy and estimated risk of bleeding Risk Factors Age > 65 Age > 75 Previous bleeding Cancer Metastatic Cancer Renal failure Liver failure Thrombocytopenia Prior stroke Diabetes Anemia Antiplatelet therapy Poor anticoagulant control Recent surgery Frequent falls Alcohol abuse NSAID use Comorbidity & reduced functional capacity Categorization of Risk of Bleeding Low Moderate High 0-3 months 1.6% 3.2% 12.8% > 3 months 0.8%/yr 1.6%/yr >6.5%/yr CHEST Guideline, November 2015.
54 Rationale for Catheter Directed Therapy (CDT) Iliofemoral DVT have greater risk of PTS Large thrombus burden is associated with higher degree of obstruction and vessel wall and valvular injury Lysis requires clot penetration and increased surface area for plasminogen activation Plasminogen in circulation is easily inactivated by alpha 2 macroglobulin and antiplasmin Allows for direct thrombus action and decreased dose of agent needed
55 Catheter Directed Therapy National Venous Registry (Mewissen): 83% resulted in complete lysis of thrombus, and 90% patency and complete lysis at 1 year, with 5-10% bleeding risk Improvements in dosage and technique Adjunctive pharmaco-mechanical therapy
56 Pharmaco-mechanical Therapy (PMT) Comerota ( 2000, 2009) : Improved QOL at 16 and 22 months with CDT/PMT for IFDVT Significant decrease in CEAP class at 12 months Low recurrence rate ( 9% at 35 months) Recurrence was related to degree of lysis (5% in those with <50% residual thrombus and 38% with > 50% residual thrombus)



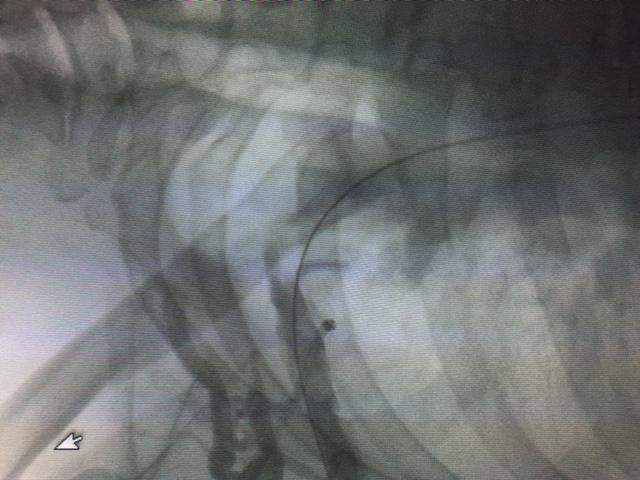
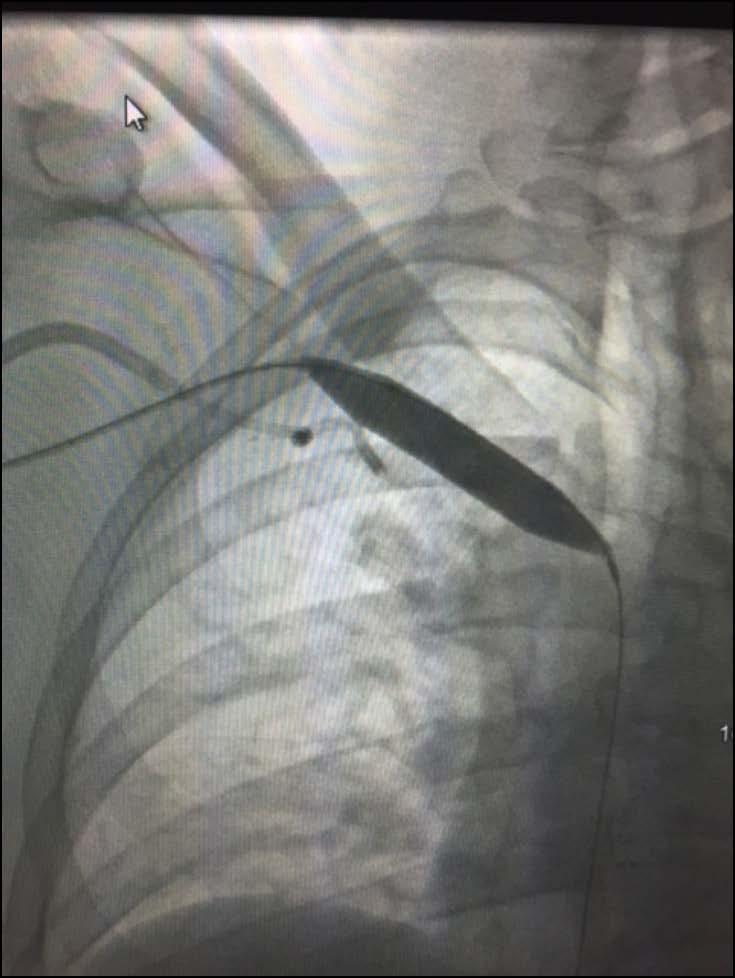
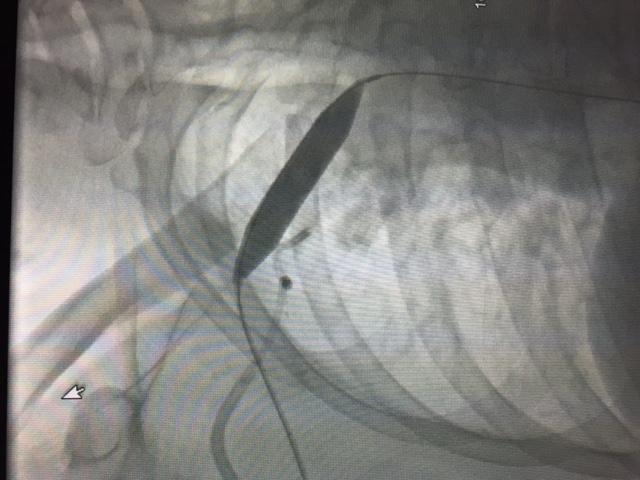
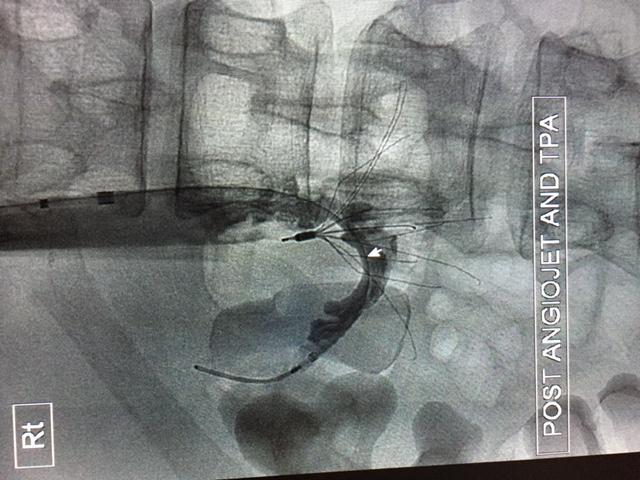
57 Catheter Directed Therapy with PMT

58 Catheter Directed Therapy with PMT


59 Catheter Directed Therapy with PMT

60 Venous Compression :May-Thurners Syndrome Iliofemoral DVT resulting from anatomic compression of the left iliac vein by the overlying right common iliac artery 37-61% risk of edema or DVT



61 Courtesy of Z KRAJCER, MD, and SR ATMAKURI, MD
62 Upper Extremity DVT Accounts for 1-4% of all DVTs in the absence of central venous catheters CVCs increase incidence of DVTs by 2-16% 24% of UE DVTs are spontaneous and related to thoracic outlet compression, often in young healthy individuals PTS can occur in 7-46% of patients and is associated with increased functional disability and decreased QOL

63 Axillo-subclavian DVT (Paget-Schroetter syndrome)

64

65 Management of Paget-Schroetters syndrome

66 Management of Paget-Schroetters syndrome
67 IVC Filter Indicated for DVT/PE where there is a contraindication to anticoagulation Relative indications for failure of anticoagulation, or in cases of recurrent VTE in patients with severe cardiopulmonary compromise Trend towards limited/ highly selective use of IVC filters

68 Aburhama A. The Vein Book. Ed. Bergan J. p.426


69 IVC and renal vein thrombosis

70 IVC and Renal vein thrombosis
71 Surgical Thrombectomy Indicated when catheter based techniques and lytic therapy have failed or are contraindicated in the setting of impending venous gangrene and limb loss Adjunctive arterio-venous fistula and fasciotomy as indicated
72 Conclusions Understanding of venous anatomy and physiology is essential for treatment Appropriate clinical diagnosis based on presentation, clinical probability and confirmatory testing Anticoagulation remains the mainstay of therapy
73 CHEST Guidelines: ú 3 month duration of anticoagulation with preference for NOACs over VKA ú Extended ( no stop date) anticoagulation for unprovoked VTE in patients without high risk for bleeding ú LMWH preferred for cancer-related thrombosis ú Need for regular re-assessment of risks of anticoagulation : INDIVIDUALIZED
74 Conclusion Catheter directed therapy has a role in selected individuals with extensive proximal DVT ( iliofemoral and axillo-subclavian DVT) When used selectively, adjunctive therapies have been shown to improve outcomes and QOL

75 Thank You Thank You
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
 Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
How long to continue anticoagulation after DVT?
 How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach
 Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Venous interventions in DVT
 Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Interventional Treatment VTE: Radiologic Approach
 Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Approach to Thrombosis
 Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales
 John Fletcher Wound Care Association of New South Wales") Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT
 THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT Tara D. Balint, MD FACS Sentara RMH Thursday, June 14, 2018 1 Objectives of treatment for DVT Prevent death from PE Prevent recurrent VTE Prevent post-thrombotic
THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT Tara D. Balint, MD FACS Sentara RMH Thursday, June 14, 2018 1 Objectives of treatment for DVT Prevent death from PE Prevent recurrent VTE Prevent post-thrombotic
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
The Evidence Base for Treating Acute DVT
 The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Intervention for Deep Venous Thrombosis and Pulmonary Embolus
 Intervention for Deep Venous Thrombosis and Pulmonary Embolus Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard
Intervention for Deep Venous Thrombosis and Pulmonary Embolus Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Case 1:
 12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Anticoagulation therapy following endovascular treatment of iliofemoral deep vein thrombosis
 Anticoagulation therapy following endovascular treatment of iliofemoral deep vein thrombosis Tim Sebastian, M.D. University Hospital Zurich Clinic for Angiology Disclosure Speaker name: Tim Sebastian I
Anticoagulation therapy following endovascular treatment of iliofemoral deep vein thrombosis Tim Sebastian, M.D. University Hospital Zurich Clinic for Angiology Disclosure Speaker name: Tim Sebastian I
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT
 VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
Aggressive endovascular management of ilio-femoral DVT. thrombotic syndrome. is the key in preventing post
 CACVS 2017 Aggressive endovascular management of ilio-femoral DVT is the key in preventing post thrombotic syndrome ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HEALTH SYSTEM
CACVS 2017 Aggressive endovascular management of ilio-femoral DVT is the key in preventing post thrombotic syndrome ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HEALTH SYSTEM
DVT and Pulmonary Embolus. Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre
, MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre") DVT and Pulmonary Embolus Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre Overview Structure of deep and superficial venous system of upper
DVT and Pulmonary Embolus Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre Overview Structure of deep and superficial venous system of upper
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
CHAPTER 2 VENOUS THROMBOEMBOLISM
 CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome
 Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome Catherine K. Chang, MD FACS Vascular Surgery San Diego Southern California Permanente Medical Group Acute Deep Venous Thrombosis Incidence & Outcomes
Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome Catherine K. Chang, MD FACS Vascular Surgery San Diego Southern California Permanente Medical Group Acute Deep Venous Thrombosis Incidence & Outcomes
Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium
 Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium Disclosures Honoraria and research support: Daiichi-Sankyo, Boehringer Ingelheim,
Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium Disclosures Honoraria and research support: Daiichi-Sankyo, Boehringer Ingelheim,
Proper Diagnosis of Venous Thromboembolism (VTE)
") Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Disclosures. What is a Specialty Vein Clinic? Prevalence of Venous Disease. Management of Venous Disease: an evidence based approach.
 Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital Foundation Trust
 MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients. David Liff MD Oklahoma Heart Institute Vascular Center
 DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
Duration of Anticoagulant Therapy. Linda R. Kelly PharmD, PhC, CACP September 17, 2016
 Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Diagnosis and management of pulmonary embolism
 Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis. By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan
 Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Treatment of acute thrombosis of axillo-subclavian vein
 Treatment of acute thrombosis of axillo-subclavian vein Yang Jin Park Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine CASE A 32-year-old male patient 3-day history of
Treatment of acute thrombosis of axillo-subclavian vein Yang Jin Park Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine CASE A 32-year-old male patient 3-day history of
DISORDERS OF VENOUS SYSTEM
 DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
This chapter will describe the effectiveness of antithrombotic
 Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Optimal Utilization of Thrombolytics
 April 8-9, 2011 New York LaGuardia Marriott COMPLETE MANAGEMENT OF VENOUS DISEASE Optimal Utilization of Thrombolytics Anthony J. Comerota, MD, FACS, FACC Director, Jobst Vascular Institute Adjunct Professor
April 8-9, 2011 New York LaGuardia Marriott COMPLETE MANAGEMENT OF VENOUS DISEASE Optimal Utilization of Thrombolytics Anthony J. Comerota, MD, FACS, FACC Director, Jobst Vascular Institute Adjunct Professor
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Chronic Iliocaval Venous Occlusive Disease
 none Chronic Iliocaval Venous Occlusive Disease David Rigberg, M.D. Clinical Professor of Surgery Division of Vascular Surgery University of California Los Angeles Chronic Venous Occlusive Disease Chronic
none Chronic Iliocaval Venous Occlusive Disease David Rigberg, M.D. Clinical Professor of Surgery Division of Vascular Surgery University of California Los Angeles Chronic Venous Occlusive Disease Chronic
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
4/23/2009. September 15, 2008
 The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
Michael Meuse, M.D. Vascular and Interventional Radiology
 Michael Meuse, M.D. Vascular and Interventional Radiology Iliac Vein Compression Syndrome Left CIV compressed by right CIA Virchow 1851: DVT L>R May and Thurner 1954: venous spurs Cockett and Thomas 1965:
Michael Meuse, M.D. Vascular and Interventional Radiology Iliac Vein Compression Syndrome Left CIV compressed by right CIA Virchow 1851: DVT L>R May and Thurner 1954: venous spurs Cockett and Thomas 1965:
Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum
 Online Data Supplement Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum Stacey M. Kassutto, C. Jessica Dine, Maryl Kreider, Rupal
Online Data Supplement Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum Stacey M. Kassutto, C. Jessica Dine, Maryl Kreider, Rupal
Anticoagulation Forum: Management of Tiny Clots
 Anticoagulation Forum: Management of Tiny Clots Casey O Connell, MD FACP Associate Professor Jane Anne Nohl Division of Hematology Keck School of Medicine USC DISCLOSURES None 4/11/2017 Objectives Define
Anticoagulation Forum: Management of Tiny Clots Casey O Connell, MD FACP Associate Professor Jane Anne Nohl Division of Hematology Keck School of Medicine USC DISCLOSURES None 4/11/2017 Objectives Define
UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS
 UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS Armando Mansilha MD, PhD, FEBVS 16 th National Congress of the Italian Society of Vascular and Endovascular Surgery Bologna, 2017 Disclosure I have the following
UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS Armando Mansilha MD, PhD, FEBVS 16 th National Congress of the Italian Society of Vascular and Endovascular Surgery Bologna, 2017 Disclosure I have the following
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Management of Iliac and Femoral Thrombosis. Adam Lackey UCH Surgery Grand Rounds November 13, 2006
 Management of Iliac and Femoral Thrombosis Adam Lackey UCH Surgery Grand Rounds November 13, 2006 Overview Definitions/Anatomy Pathogenesis Prevalence Diagnosis Treatment/Prevention Definitions/Anatomy
Management of Iliac and Femoral Thrombosis Adam Lackey UCH Surgery Grand Rounds November 13, 2006 Overview Definitions/Anatomy Pathogenesis Prevalence Diagnosis Treatment/Prevention Definitions/Anatomy
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
10/24/2013. Heparin-Induced Thrombocytopenia (HIT) Anticoagulation Management in ECMO Therapy:
 Anticoagulation Management in ECMO Therapy:") Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of Interventional procedure overview of ultrasound-enhanced, catheterdirected thrombolysis
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of Interventional procedure overview of ultrasound-enhanced, catheterdirected thrombolysis
Copy Here. The Easy One.. What is the Role of Thrombus Removal in Acute Proximal DVT after ATTRACT? Deep Venous Thrombosis Spectrum
 What is the Role of Thrombus Removal in Acute Proximal DVT after ATTRACT? Mitchell J. Silver DO FACC FSVM RPVI Director, Center for Critical Limb Care Riverside Methodist Hospital Ohio Health Heart and
What is the Role of Thrombus Removal in Acute Proximal DVT after ATTRACT? Mitchell J. Silver DO FACC FSVM RPVI Director, Center for Critical Limb Care Riverside Methodist Hospital Ohio Health Heart and
Epidemiology of Thrombosis in Patients with Malignancy. Cancer and Venous Thromboembolism. Chew HK, Arch Int Med, Feb Blom et al, JAMA, Feb 2005
 Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Inferior Vena Cava Filters
 Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
What s New in DVT & PE
 What s New in DVT & PE Mark Buch MD CM CCFP(EM) Attending physician Emergency Department Jewish General Hospital Family Physician and Medical Director GMF Santé Mont-Royal Objectives: Review the diagnostic
What s New in DVT & PE Mark Buch MD CM CCFP(EM) Attending physician Emergency Department Jewish General Hospital Family Physician and Medical Director GMF Santé Mont-Royal Objectives: Review the diagnostic
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range
 Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range") Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS
 TOKUDA HOSPITAL SOFIA DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS MILENA STANEVA, MD, PhD Department of vascular surgery and angiology Venous thromboembolic disease continues to cause significant morbidity
TOKUDA HOSPITAL SOFIA DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS MILENA STANEVA, MD, PhD Department of vascular surgery and angiology Venous thromboembolic disease continues to cause significant morbidity
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON
 Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON How to Prevent and Manage the Post-Thrombotic Syndrome? Jean-Philippe Galanaud Clinical Thromboembolism & Division of GIM Sunnybrook,
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON How to Prevent and Manage the Post-Thrombotic Syndrome? Jean-Philippe Galanaud Clinical Thromboembolism & Division of GIM Sunnybrook,
Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience
 JFICV 2018, Beaune Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience Prof. Romaric LOFFROY, MD, PhD, FCIRSE Chief, Department of Vascular and
JFICV 2018, Beaune Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience Prof. Romaric LOFFROY, MD, PhD, FCIRSE Chief, Department of Vascular and
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Keynote lecture: Oral anticoagulation and DVT
 Keynote lecture: Oral anticoagulation and DVT What is the evidence? Is there a need to anticoagulate every lower leg DVT? Disclosure Speaker name:...sebastian Schellong... I have the following potential
Keynote lecture: Oral anticoagulation and DVT What is the evidence? Is there a need to anticoagulate every lower leg DVT? Disclosure Speaker name:...sebastian Schellong... I have the following potential
UNIVERSITA DI PADOVA. Un tema particolare (II): Le trombosi venose in pediatria
: Le trombosi venose in pediatria") UNIVERSITA DI PADOVA Un tema particolare (II): Le trombosi venose in pediatria Elena Campello Dipartimento di Medicina Università di Padova Bologna, 6 Novembre 2015 Introduction Pediatric thrombosis: -
UNIVERSITA DI PADOVA Un tema particolare (II): Le trombosi venose in pediatria Elena Campello Dipartimento di Medicina Università di Padova Bologna, 6 Novembre 2015 Introduction Pediatric thrombosis: -
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Risk-Based Evaluation and Management of VTE
 12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information
 Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
ED Diagnosis of DVT or tools to rule out DVT in your ED
 ED Diagnosis of DVT or tools to rule out DVT in your ED Ralph Wang UCSF Department of Emergency Medicine 53 yo f c/o left leg swelling recent cholecystectomy its midnight how do you manage this patient?
ED Diagnosis of DVT or tools to rule out DVT in your ED Ralph Wang UCSF Department of Emergency Medicine 53 yo f c/o left leg swelling recent cholecystectomy its midnight how do you manage this patient?
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Thromboembolic Diseases
 Thromboembolic Diseases Incidence, Risk Factors, and Categories Deep venous thrombosis (DVT) and pulmonary embolism (PE), together called venous thromboembolism (VTE), remain a serious health care problem.
Thromboembolic Diseases Incidence, Risk Factors, and Categories Deep venous thrombosis (DVT) and pulmonary embolism (PE), together called venous thromboembolism (VTE), remain a serious health care problem.
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of Interventional procedure overview of ultrasound-enhanced, catheterdirected thrombolysis
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of Interventional procedure overview of ultrasound-enhanced, catheterdirected thrombolysis
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Acoustic Pulse Thrombolysis Treatment
 Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
incidence of cancer-associated thrombosis (CAT) is further increased by additional risk factors such as chemotherapeutic 2
 is further increased by additional risk factors such as chemotherapeutic 2") CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention
 TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention") A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention This handout is a supplemental resource to an educational video activity released on Medscape
A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention This handout is a supplemental resource to an educational video activity released on Medscape
Updates in Coagulation Thrombophilia testing and direct oral anticoagulants. Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017
 Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017 No conflicts of interest Introduction to thrombosis Hemostasis
Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017 No conflicts of interest Introduction to thrombosis Hemostasis
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies
 VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
Prevention and management of venous thromboembolism M. AAPRO
 Prevention and management of venous thromboembolism M. AAPRO Thromboprophylaxisof DVT and PE in AmbulatoryCancerPatients Zurich, February 2017 M. AAPRO Based on a lesson in April 2016 by M. DICATO M.D.,
Prevention and management of venous thromboembolism M. AAPRO Thromboprophylaxisof DVT and PE in AmbulatoryCancerPatients Zurich, February 2017 M. AAPRO Based on a lesson in April 2016 by M. DICATO M.D.,
CPT only copyright 2014 American Medical Association. All rights reserved. 12/23/2014 Page 66 of 593
 Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2015 PQRS OPTIONS FOR INDIVIDUAL MEASURES:
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2015 PQRS OPTIONS FOR INDIVIDUAL MEASURES: