Chronic Total Occlusions Opening the Way. Reginald Low MD Chief, Division of Cardiovascular Medicine University of California, Davis
|
|
|
- Toby Wright
- 5 years ago
- Views:
Transcription
1 Chronic Total Occlusions Opening the Way Reginald Low MD Chief, Division of Cardiovascular Medicine University of California, Davis
2 Disclosures Abbott Vascular Consultant Boston Scientific Consultant Direct Flow Medical Consultant
3 Chronic Total Occlusion Clinical Definition Complete coronary arterial obstruction with TIMI flow 0 for longer than 3 months







4 CTO Prevalence and Treatment Pa,ents with Coronary Artery Disease N = 14,439 Treatment of Pa,ents with CTOs N = 1,697 CTO 18.4% Medical Therapy 44% CABG 26% Non- CTO PCI 20% A>empted CTO- PCI 10% Fefer et al. JACC 2012.


5 Variability in Current Treatment CTO-PCI attempt rate varied among hospitals from 1% to 16% CTO treatment strategies in 3 Canadian centers *p < 0.001; **p = NS; p < Fefer et al. JACC 2012.

6 PCI Utilization Disproportionately Low in CTOs 50% 40% 30% 20% 10% CAD Treatment Strategies PCI CABG Med Rx 0% CTO N=1,612 No CTO N=1,475 BARI Registry Substudy Christofferson et al. Am J Cardiol 2005.
7 CABG is Not Always an Option SYNTAX CTO Substudy 266 CTO pa,ents randomized to receive CABG Bypassed 68% Not Bypassed 32% Reason not bypassed: Not intended to treat (n=12) Diseased (n=11) Inadequate conduit (n=2) Too small (n=19) Unable to find (n=1) Other (n=36) ITT, per lesion. 49.6% overall complete revascularization in CTO subset. Courtesy Patrick Serruys, Syntax CTO substudy, TCT 2008.
8 Benefits of Revascularization Quality of Life QuanVty of Life

9 Quantity of Life Ischemia Cardiac Death Rate % 1-5% 5-10% 11-20% >20% % Ischemic Burden Hachamovitch et al Circula3on. 2003; 107:

10 Quality of Life after PCI QOL BeWer QOL Worse Asx I II III IV 30 points! Baseline 1 Year McNulty et al AHA 2012
11 Rationale for CTO Revascularization Improve symptoms Improve coronary blood flow - O 2 Supply Increase long-term survival Improve left ventricular function Improve electrical stability of myocardium - reduce predisposition for arrhythmic event Increase tolerance of progressive coronary artery disease - provide collaterals
12 Chronic Total Occlusion Percutaneous recanalization of Chronic Total occlusions Most challenging procedure in the Cardiac Cath Lab Technically difficult to treat Time intensive Complex procedure Significant contrast load Complications Historic success rate ~ 50% Success rates now - > 90%


 in fibrous stroma Calcium Dense")

13 Anatomy and Histopathology Thrombotic occlusion, thrombus organization & tissue aging Histologically one-half of CTOs are <99% stenotic No relationship between severity of histopathic lumen stenosis and plaque composition or lesion age Atherosclerotic plaque of CTO Intra and extracellular lipid Smooth muscle cells Extracellular matrix (predominate type I and III) in fibrous stroma Calcium Dense concentration of collagen rich fibrous tissue at proximal and distal ends - columnlike lesion of calcified fibrous tissue Large - 59% of all CTO Small - 41% of all CTO




14 Comparison of CTO Tissues Differential Elastance of Adventitia and Fibrous Plaque Adventitia Plaque Emery et al. LuMend, Inc.
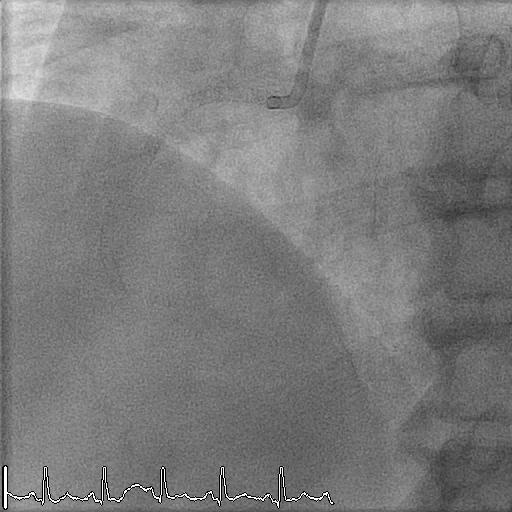
15 Contralateral Injection

16 Remodeling Immediate 6 Months
17 The CTO Toolbox Devices to facilitate Antegrade wire escalavon Antegrade dissecvon/re- entry Retrograde wire escalavon Retrograde dissecvon/re- entry ComplicaVon Management Guides, balloons, catheters, wires and specialty devices
18 Specialty CTO Asahi Wires Torque response, drilling, anti-trap Straight Tip ASAHI MIRACLEBROS 3 Interrogate lesion - transmits lesion information Tapered Tip ASAHI CONFIANZA 9 ASAHI MIRACLEBROS 4.5 ASAHI MIRACLEBROS 6 ASAHI MIRACLEBROS 12 Increasing Support ASAHI CONFIANZA PRO 9 ASAHI CONFIANZA PRO 12


19 Newer Specialty CTO Asahi Wires cm Polymer Sleeve & SLIP COAT 16cm Radio-opaque spring coil Stainless Steel Core Fielder XT PTFE Coating 11cm Spring Coil 3cm Radio-opaque Coil Stainless Steel Core Fielder FC 20cm Polymer Sleeve & SLIP COAT PTFE Coating ASAHI SION


20 Corsair Catheter Collateral Crossing and Support Catheter Hydrophilic Polymer Coating 60cm Balloon Microcatheter Flexible tapered tip of ASAHI Corsair contributes excellent channel tracking and also effectively works for super-selective tip injection
21 Antegrade Toolbox WIRES Sob,tapered, jacketed IniVal probing- crossing wire SVff, non- tapered, jacketed Complex lesion crossing wire SUPPORT Microcatheter SVffen wire and facilitate quick wire exchange Guide Extension and Support SVff, tapered, non- jacketed SVff PenetraVng wire
22 Retrograde and Ancillary Toolbox RETROGRADE Same wires as antegrade Externalization guidewires Snares ANCILLARY Doddering device Specialty balloons (small, long) 8 Fr 23-45cm femoral sheaths 90 cm guides (retrograde) Hemostasis valves PERFORATION KIT Pericardiocentisis tray Covered stent Occlusion coils, coil pusher, delivery catheter





23 Evolution of CTO-PCI Increasing Success Rates Related to Technique Evolution 2004 Antegrade Wires and IVUS Rudimentary Retrograde Early Antegrade DissecVon Re- Entry 2012 Hybrid









24 New Approach to Treat CTOs The Hybrid Strategy Retrograde Techniques Antegrade Dissec,on Re- Entry Antegrade Wiring FOUR ANGIOGRAPHIC CHARACTERISTICS DICTATE STRATEGY Proximal cap ambiguity Lesion length Quality of distal target Suitability of interventional collaterals HYBRID STRATEGY PRINCIPLES Consistent evaluation approach Emphasizes procedural safety, success, and efficiency Minimizes radiation and contrast Quick transition to alternate plans when failure mode occurs




")

 Dissection")

25 The Hybrid Algorithm Clear Proximal Cap Good Distal Target YES NO Antegrade Retrograde YES NO Length < 20mm YES NO Wire Escalation FAIL Dissection Re- Entry (CrossBoss - Stingray ) Wire Escalation FAIL Dissection Re- Entry (Reverse CART) FAIL FAIL Dissection Re-Entry (Reverse CART) Dissection Re-Entry (CrossBoss - Stingray )


26 Hybrid CTO Registry Results Most Successful Strategy for Complex Lesions Success Hybrid N=194 CTO lesions Success Japanese CTO N=528 lesions Success Royal Brompton N=269 lesions % Cases J- CTO 0-1 J- CTO 2 J- CTO 3 Daniels D, TCT2013 More Complex Lesions
 250 Contrast (cc) Data on procedure Vme from J- CTO was not")
27 Procedural Efficiency Lowest procedure time and contrast used in Hybrid Registry p< p< Hybrid CTO N=194 lesions European CTO N=1983 lesions Japanese CTO N=528 lesions 0 Procedure Time (minutes) 250 Contrast (cc) Data on procedure Vme from J- CTO was not published. Presented by Daniels, D at TCT Gallasi et al. EurointervenVon 2011;7:472-49
28 Hybrid CTO Registry Results Complex Lesions Crossed Quickly in More Cases JCTO 2 Lesions Crossed in Less Than 30 Minutes % % Cases % 0 Hybrid Registry Japanese CTO Registry Daniels D, CTO/LM Summit 2013
29

30 Antegrade Wire Escalation Soft-tipped polymerjacketed Excellent Steerability Poor Penetration Moderate stifftipped polymerjacketed Good Steerability Moderate Penetration Excellent Penetration Easier Perforation Heavy tipped non-polymerjacketed

31 Ostial LAD CTO





32 Antegrade Dissection Re-Entry CTO crossing through the subintimal space, advancing across the occlusion, re-entering into the distal true lumen





33 Coronary CTO Crossing and Re-entry System CrossBoss Catheter Designed to quickly and safely deliver a guidewire via true lumen or subinvmal pathways 1 2 SVngray Catheter Designed to accurately target and re- enter the true lumen from a subinvmal posivon 3

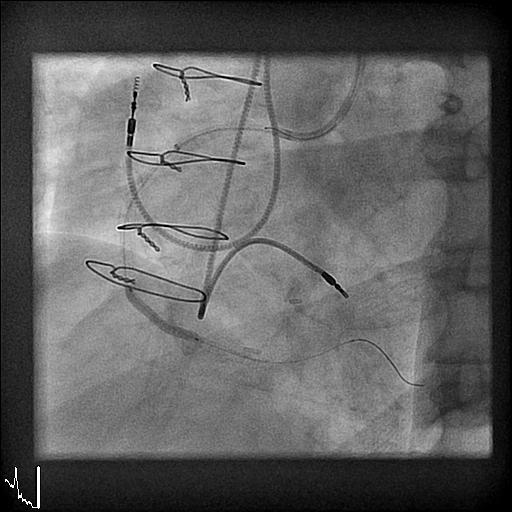
34 Antegrade Dissection Re-entry Procedure


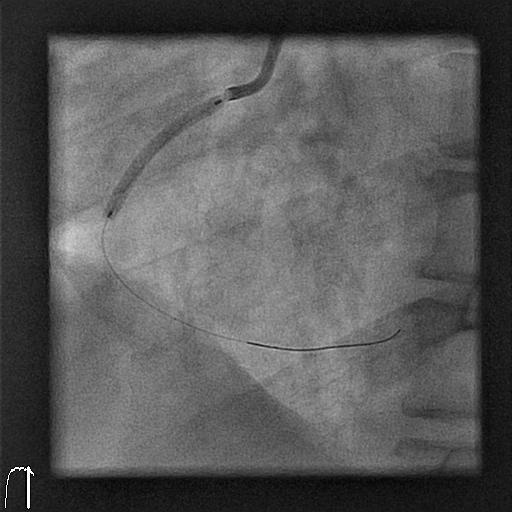
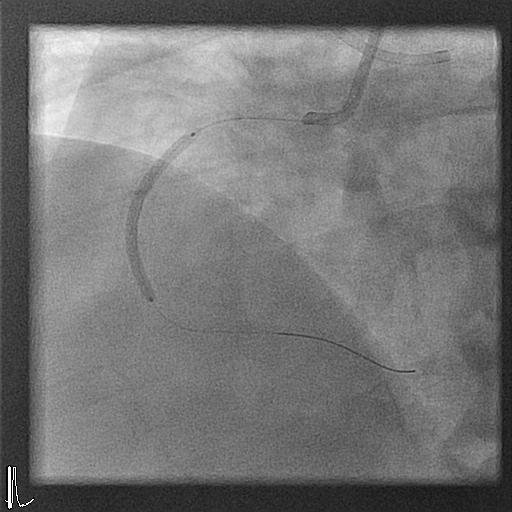
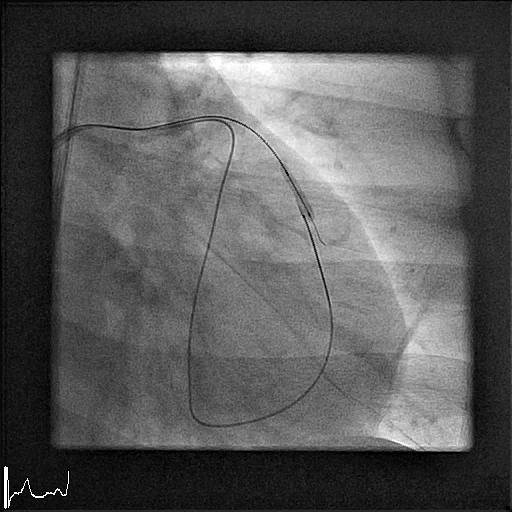
35 CTO of the RCA Contralateral injecvon of the L è R collaterals

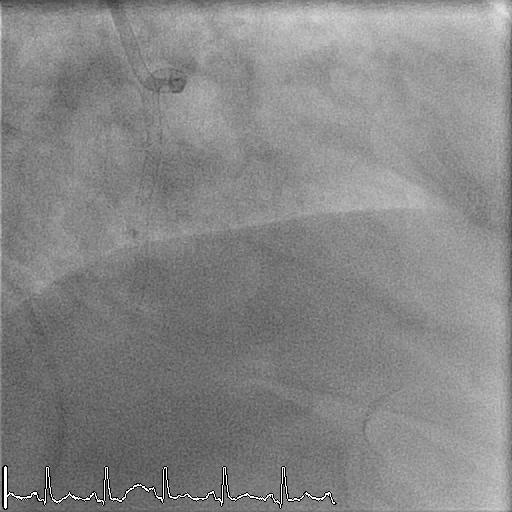
36 CrossBoss Catheter
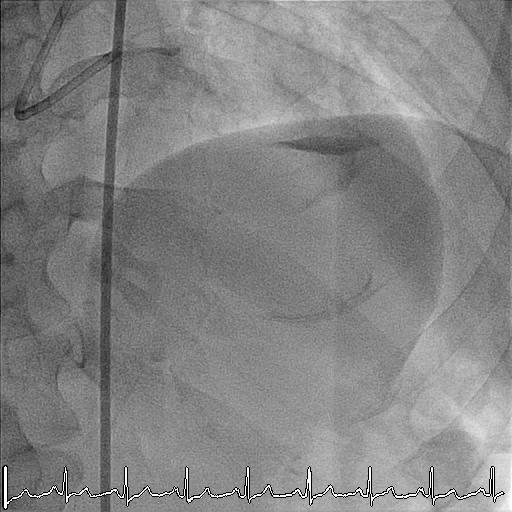
37 Angioplasty and Stenting

38 Final Angiography
39
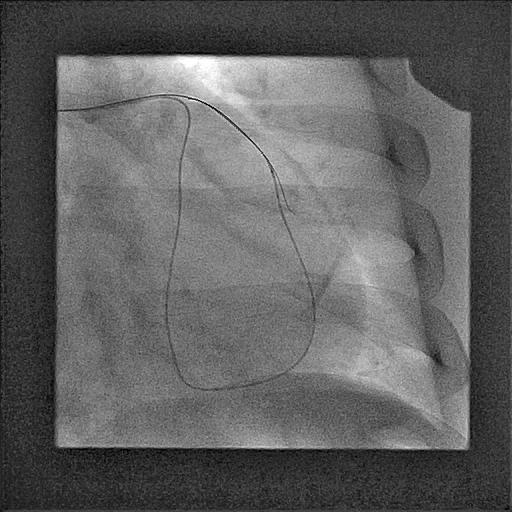
40 Re-reattempt at RCA CTO

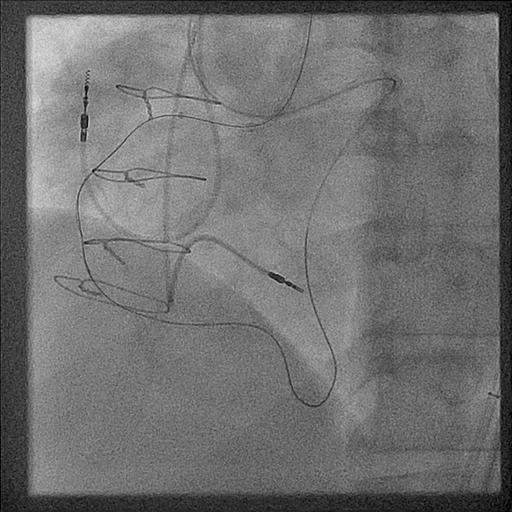
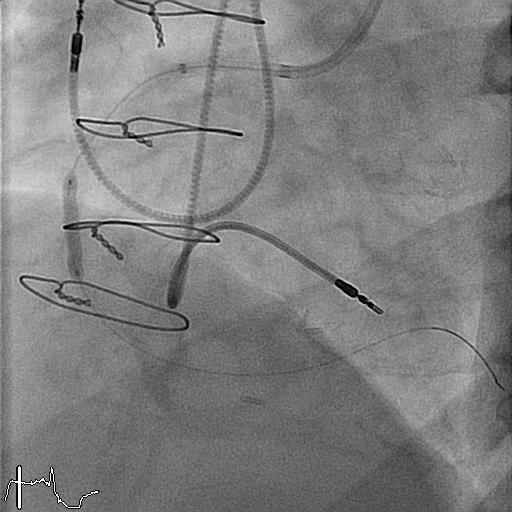
41 Simultaneous RCA & LCA Injections
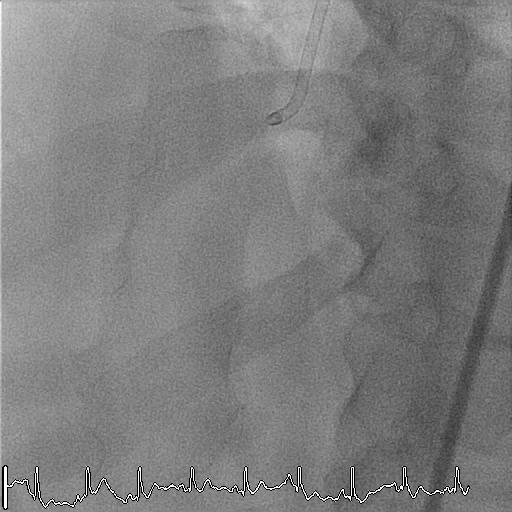
42 CrossBoss Catheter - Subintimal
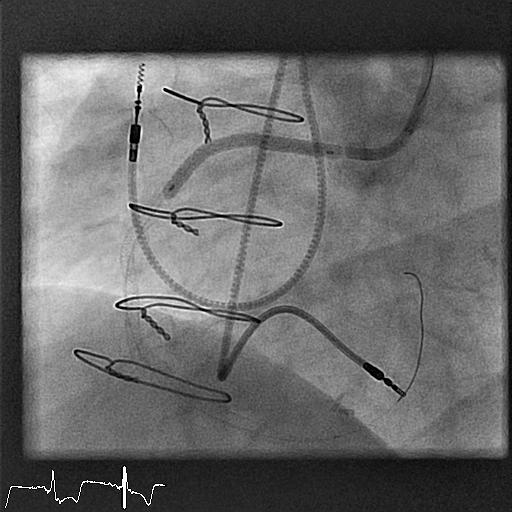
43 Wire redirection and advancement of CrossBoss

44 Wire redirection and advancement of CrossBoss
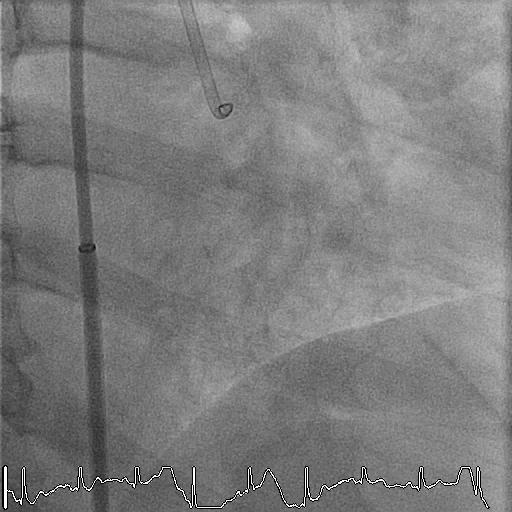
45 Stingray Positioning for Reentry Incorrect PosiVon Correct PosiVon
46 Stingray wiring into true lumen

47 Stingray wiring into true lumen
48 Exchange for Corsair and workhorse wire
49 PTCA of lesion

50 Stenting of lesion with DES
51 Final Angiography



52 Retrograde Techniques Retrograde collateral wiring EssenVal tools for retrograde 1. Microcatheters 2. Wires IllustraVon by Dr. J C SpraW / VascularPerspecVves,



53 Retrograde Techniques Once septal collaterals allow access to distal cap... the distal cap should then be tackled like proximal cap. Follow the Hybrid approach. Images provided by Boston Scientific. Results from case studies are not predictive of results in other cases. Results in other cases may vary.


54 Retrograde Techniques Dissection Re-Entry Techniques: Reverse CART IllustraVon by Dr. J C SpraW / VascularPerspecVves,

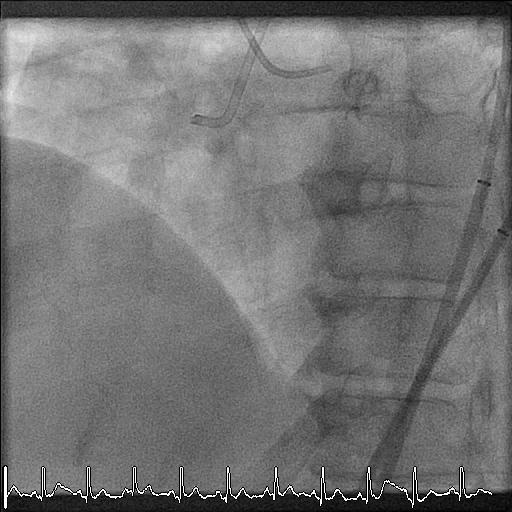
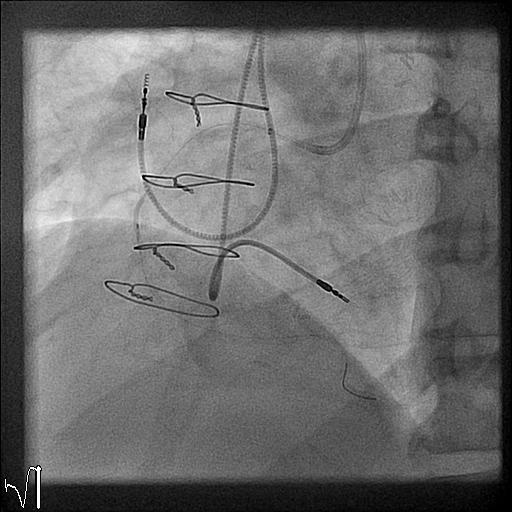
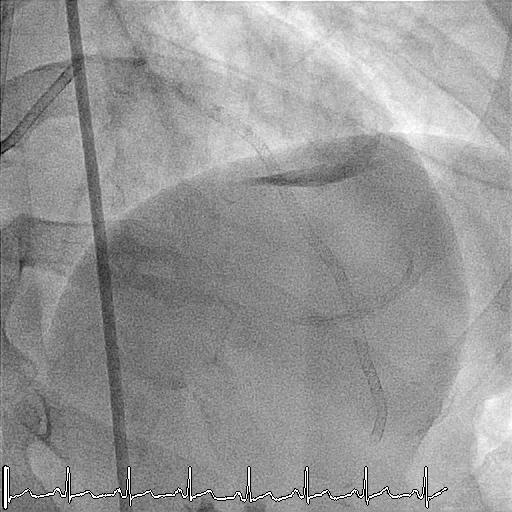
55 CTO of the RCA Retrograde Approach

56 CTO of the RCA - Retrograde IdenVfy an appropriate septal collateral

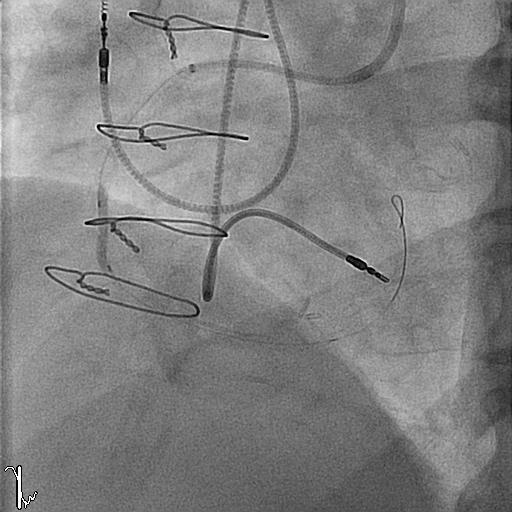
57 Septal channel wiring In real time

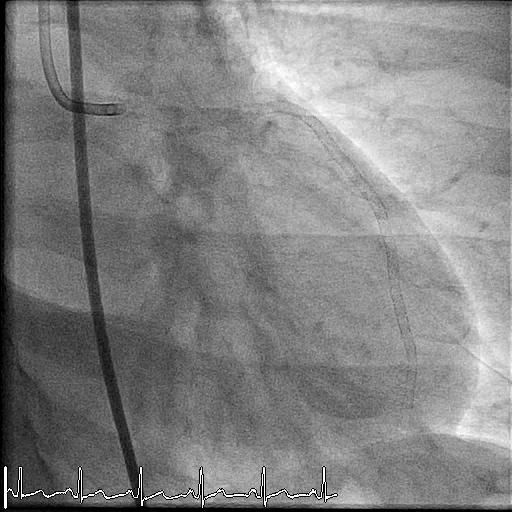
58 CTO of the RCA - Retrograde

59 CTO of the RCA - Retrograde
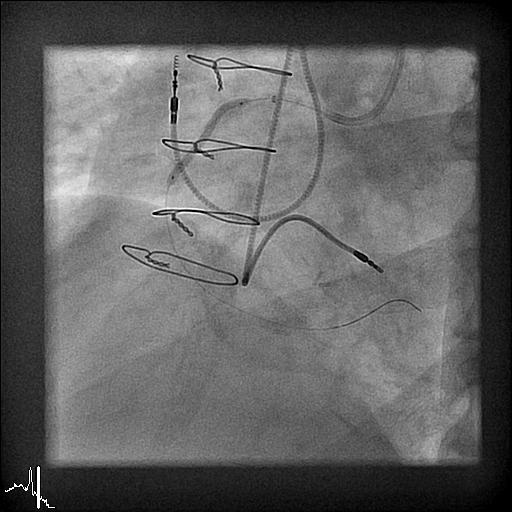
60 Successive Balloon Angioplasty
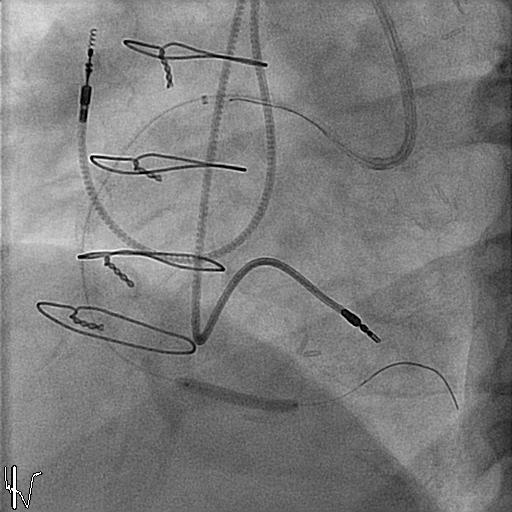
61 Multiple drug-eluting stents placed

62 Initial and Final Angiography
63 Patient 56 yo male Hypertension, hyperlipidemia MI 2006 MI 2014 Exertional angina and shortness of breath Anterior wall ischemia with viability LVEF 45% ASA, clopidogrel, metoprolol, isorsorbide dinitrate, atorvastatin, losartan CTO attempted with LAD dissection Referred for CABG

64 Initial Angiograms demonstrating mid LAD CTO


65 Initial Angiograms demonstrating mid LAD CTO

66 Evidence of septal perforator collateral to the distal LAD

67 Corsair into the septal with distal tip injections and successful wiring into distal LAD

68 Advancing Corsair and preparing antegrade system

69 Attempting to cross occlusion to proximal true lumen with retrograde system
70 Advancing antegrade and retrograde wires and confirming position in orthogonal views
71 Advancing Corsair in preparation for Reverse CART procedure
72 Performing Reverse CART technique
73 Retrograde advancement of the Corsair and wiring of guide catheter
74 Retrograde Corsair into guide catheter to externalize wire
75 Sequential Predilation
76 Multiple DES deployed

77 High pressure post dilation
78 Final angiograms
79 Conclusions Pt is doing well in follow up with complete relief of symptoms Discontinued his long acting nitrates Increasing his exercise tolerance Quit smoking!
80
81 Complications CTO Angioplasty (n=2007) Non-CTO Angioplasty (n=2007) P Death 1.3% 0.8% 0.13 Q-wave myocardial infarction 0.5% 0.6% 0.67 Non-Q wave myocardial infarction 1.9% 2.4% 0.27 Urgent bypass graft surgery 0.7% 1.1% 0.25 Urgent repeat PCI 1.5% 2.0% 0.23 Major adverse cardiac events 3.8% 3.7% 0.39 Stroke 0.01% 0.1% 0.63 Vascular complication 1.7% 2.5% 0.80 Suero JA JACC 2001;38:409


82 Complications Death and MI Shearing off collateral circulation Injure proximal vessel or side branch Perforation Air embolism Thrombus Arrhythmia Emergency CABG Proximal vessel injury or side branch Guidewire fracture or entrapment Perforation Subacute vessel closure Contrast nephropathy Radiation skin injury
83 Complications Major Complications Death 0.8% Emergency CABG 0.3% Q wave MI 0.2% Minor Complications Tamponade 1.1% Aortic Dissection 0.4% Acute Occlusion 0.8% Subacute Occlusion 0.4% Side branch compromise 2.6% Coronary perforation Type I 9.0% Type II 1.1% Toyohashi Heart Center - CTO Summit 2007

84 Procedural Success Rates Over Time Operators with Retrograde Skills >90% Success Retrograde Operators Antegrade Operators Dartmouth North Cascade MulVcenter CTO Registry, Thompson CA, Lombardi WL
85 Is CTO-PCI for you? ü PCI aggressive YOU ü YOUR INSTITUTION Two reliable PCI labs with good imaging ü Technically accomplished ü Demonstrable excellent PCI outcomes ü Do complex angioplasty(rotablator IVUS, curng balloon) ü Willing to change old habits ü Comfortable being uncomfortable ü Okay with failure ü ü ü ü A team that is comfortable with complex PCI EnthusiasVc core of nurse/technicians Efficient, flexible, pavent- centered flow CTO partner and supporvve pracvce ü CTO- commiwed work strategy
86 Summary Successful PCI of Chronic Total Occlusion may Relieve symptoms Improve LV function Improve survival Improve electrical stability Enhance tolerance for progressive CAD Assess Risk / Benefit for each patient Consider clinical, angiographic and technical factors Essentials of a CTO program Knowledge of histopathology Equipment knowledge and selection Techniques - Guidewire, parallel wire, side branch, retrograde, etc. Specialty devices - Tornus, Cross Boss, Stingray Balloon, Corsair, etc High resolution imaging, contra-lateral injection, orthogonal views Operator, patient, staff, scheduling commitment to CTO program

87 Thank You University of California Davis Medical Center
Fielder XT: Initial and. Department of Cardiology, Asan Medical Center, Ulsan University of college of medicine
 Fielder XT: Initial and Professional Use for CTO Seung-Whan Lee, MD, PhD D t t f C di l A M di l C t Department of Cardiology, Asan Medical Center, Ulsan University of college of medicine Plastic-Jacket
Fielder XT: Initial and Professional Use for CTO Seung-Whan Lee, MD, PhD D t t f C di l A M di l C t Department of Cardiology, Asan Medical Center, Ulsan University of college of medicine Plastic-Jacket
Angioplasty Summit TCTAP Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D
 Angioplasty Summit TCTAP 2010 Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D Introduction CTO-PCI has been technically and technologically evolved over the past two
Angioplasty Summit TCTAP 2010 Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D Introduction CTO-PCI has been technically and technologically evolved over the past two
Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD Toyohashi Heart Center, Japan
 Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD, Japan Retrograde Approach for Coronary CTO Collateral channels A. bypass graft B. epicardial collateral C. septal perforator Retrograde wiring techniques
Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD, Japan Retrograde Approach for Coronary CTO Collateral channels A. bypass graft B. epicardial collateral C. septal perforator Retrograde wiring techniques
Antegrade techniques for CTO recanalization. Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist
 Antegrade techniques for CTO recanalization Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist can CTOs be reliably opened by PCI? Meta-Analysis of 18,061 Patients Patel V, J Am Coll
Antegrade techniques for CTO recanalization Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist can CTOs be reliably opened by PCI? Meta-Analysis of 18,061 Patients Patel V, J Am Coll
Educational Objectives. Conflict of Interest Disclosure. TIMI Flow Classification TIMI= Thrombolysis in Myocardial Infarction TIMI 0 Flow
 Educational Objectives Percutaneous Coronary Interventions (PCI) in Chronic Total Occlusions (CTO s) The Last Frontier Ramon L. Lloret, MD, FACC, FSCAI At the end of this talk, attendees will: Understand
Educational Objectives Percutaneous Coronary Interventions (PCI) in Chronic Total Occlusions (CTO s) The Last Frontier Ramon L. Lloret, MD, FACC, FSCAI At the end of this talk, attendees will: Understand
Chronic Total Occlusions. Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute
 Chronic Total Occlusions Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute Financial Disclosures /see -tee-oh / abbr. Med. Chronic Total Occlusion,
Chronic Total Occlusions Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute Financial Disclosures /see -tee-oh / abbr. Med. Chronic Total Occlusion,
Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System
 Volume 1, Issue 1 Case Report Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System Robert F. Riley * and Bill Lombardi University of Washington Medical Center, Division
Volume 1, Issue 1 Case Report Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System Robert F. Riley * and Bill Lombardi University of Washington Medical Center, Division
Chronic Total Occlusions (CTO): The Final Fron er of Coronary Interven on CTO PCI
: The Final Fron er of Coronary Interven on CTO PCI") Chronic Total Occlusions (CTO): The Final Fron er of Coronary Interven on Christopher D. Nielsen, M.D. Director, Adult Cardiac Cath Labs Medical University of South Carolina CTO PCI What is a CTO and how
Chronic Total Occlusions (CTO): The Final Fron er of Coronary Interven on Christopher D. Nielsen, M.D. Director, Adult Cardiac Cath Labs Medical University of South Carolina CTO PCI What is a CTO and how
Clinical Considerations for CTO
 38 RCTs Clinical Considerations for CTO 18,000 pts Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD FACC, FSCAI Director, Interventional Cardiology Research
38 RCTs Clinical Considerations for CTO 18,000 pts Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD FACC, FSCAI Director, Interventional Cardiology Research
Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
 Catheterization and Cardiovascular Interventions 78:395 399 (2011) Case Reports Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
Catheterization and Cardiovascular Interventions 78:395 399 (2011) Case Reports Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
THE PROXIMAL LAD VIA SVG IN PATIENT AFTER CABG. Cardiovascular department Tokyo, Japan
 SUCCESSFUL RECANALIZATION OF CTO IN THE PROXIMAL LAD VIA SVG IN PATIENT AFTER CABG St. Lukes International Hospital Cardiovascular department Tokyo, Japan Hitoshi Anzai MD M.D. Present illness 64 YRS-OLD
SUCCESSFUL RECANALIZATION OF CTO IN THE PROXIMAL LAD VIA SVG IN PATIENT AFTER CABG St. Lukes International Hospital Cardiovascular department Tokyo, Japan Hitoshi Anzai MD M.D. Present illness 64 YRS-OLD
Illustration of the hybrid approach to chronic total occlusion crossing
 case report Illustration of the hybrid approach to chronic total occlusion crossing The hybrid approach to coronary chronic total occlusions advocates using all feasible crossing techniques in a manner
case report Illustration of the hybrid approach to chronic total occlusion crossing The hybrid approach to coronary chronic total occlusions advocates using all feasible crossing techniques in a manner
For Personal Use. Copyright HMP 2013
 Case Report J INVASIVE CARDIOL 2013;25(2):E39-E41 A Case With Successful Retrograde Stent Delivery via AC Branch for Tortuous Right Coronary Artery Yoshiki Uehara, MD, PhD, Mitsuyuki Shimizu, MD, PhD,
Case Report J INVASIVE CARDIOL 2013;25(2):E39-E41 A Case With Successful Retrograde Stent Delivery via AC Branch for Tortuous Right Coronary Artery Yoshiki Uehara, MD, PhD, Mitsuyuki Shimizu, MD, PhD,
-Wire Based Strategies- Step by Step Instructions. Yasumi Igarashi M.D. Ph.D. JCHO Hokkaido Hospital
 -Wire Based Strategies- Step by Step Instructions Yasumi Igarashi M.D. Ph.D. JCHO Hokkaido Hospital Disclosure Statement of Financial Interest I,Yasumi Igarashi, DO NOT have a financial interest/ arrangement
-Wire Based Strategies- Step by Step Instructions Yasumi Igarashi M.D. Ph.D. JCHO Hokkaido Hospital Disclosure Statement of Financial Interest I,Yasumi Igarashi, DO NOT have a financial interest/ arrangement
CTO Re vascularization in 2013
 CTO Re vascularization in 2013 Is it safe to use/stent the sub intimal space? Dimitri Karmpaliotis, MD, FACC, FSCAI Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia Dimitri.karmpaliotis@piedmont.org
CTO Re vascularization in 2013 Is it safe to use/stent the sub intimal space? Dimitri Karmpaliotis, MD, FACC, FSCAI Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia Dimitri.karmpaliotis@piedmont.org
Clinical Considerations for CTO Revascularization
 Clinical Considerations for CTO Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD, FACC, FSCAI Chief Medical Officer Cordis Cardiology Johnson & Johnson
Clinical Considerations for CTO Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD, FACC, FSCAI Chief Medical Officer Cordis Cardiology Johnson & Johnson
Elements of CTO PCI. Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center
 Elements of CTO PCI Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center Disclosures Consultant- Bridgepoint Medical Systems Speakers Honorarium- WL Gore Inc.
Elements of CTO PCI Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center Disclosures Consultant- Bridgepoint Medical Systems Speakers Honorarium- WL Gore Inc.
Patient. Clinical data Indications: Operation date. Comorbidities: Patient code Birth date: / /
 Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
Guidewire Selection. Making the Most Out of My Guidewire: LINC 2016: Leipzig Interventional Course Leipzig, Germany January 26-29, 2016
 Making the Most Out of My Guidewire: Guidewire Selection LINC 2016: Leipzig Interventional Course Leipzig, Germany January 26-29, 2016 Brian DeRubertis, MD, FACS Associate Professor of Surgery Division
Making the Most Out of My Guidewire: Guidewire Selection LINC 2016: Leipzig Interventional Course Leipzig, Germany January 26-29, 2016 Brian DeRubertis, MD, FACS Associate Professor of Surgery Division
PCI for Chronic Total Occlusions
 PCI for Chronic Total Occlusions Chronic Total Occlusions 20-40% of patients with CAD Why should we open? Rationale for CTO Revascularization Relief of symtomatic ischemia and angina Increase long-term
PCI for Chronic Total Occlusions Chronic Total Occlusions 20-40% of patients with CAD Why should we open? Rationale for CTO Revascularization Relief of symtomatic ischemia and angina Increase long-term
Interventional Cardiology
 Interventional Cardiology Retrograde approach to successfully treat antegrade failure due to subintimal hematoma of a right coronary artery chronic total occlusion Use of antegrade dissection re-entry
Interventional Cardiology Retrograde approach to successfully treat antegrade failure due to subintimal hematoma of a right coronary artery chronic total occlusion Use of antegrade dissection re-entry
Copyright HMP Communications
 Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Fighting Through a Heavy Calcified RCA-CTO; Required Retrograde Approach Two Times in the Difficulty of Passing Devices Through
 Fighting Through a Heavy Calcified RCA-CTO; Required Retrograde Approach Two Times in the Difficulty of Passing Devices Through The Department of Cardiology Dai-ni Okamoto General Hospital Masaki Tanabe
Fighting Through a Heavy Calcified RCA-CTO; Required Retrograde Approach Two Times in the Difficulty of Passing Devices Through The Department of Cardiology Dai-ni Okamoto General Hospital Masaki Tanabe
Modified Reverse CART technique in a near-ostial
 Modified Reverse CART technique in a near-ostial RCA CTO Dr. Vincent O.H. Kwok MB BS (HK) FRCP (Lond( Lond, Edin, Glasg) ) FACC FSCAI Consultant Cardiologist & Director Cardiac Catheterization & Intervention
Modified Reverse CART technique in a near-ostial RCA CTO Dr. Vincent O.H. Kwok MB BS (HK) FRCP (Lond( Lond, Edin, Glasg) ) FACC FSCAI Consultant Cardiologist & Director Cardiac Catheterization & Intervention
New Devices Pedro Pinto Cardoso
 New Devices Pedro Pinto Cardoso HSM, CHLN, CALM for CTOs Guidewires Microcatheters Radiofrequency Pharmacotherapy Pedro Pinto Cardoso, Serviço de Cardiologia HSM CHLN New Guidewires SENTAI family Samurai
New Devices Pedro Pinto Cardoso HSM, CHLN, CALM for CTOs Guidewires Microcatheters Radiofrequency Pharmacotherapy Pedro Pinto Cardoso, Serviço de Cardiologia HSM CHLN New Guidewires SENTAI family Samurai
PCI for Chronic Total Occlusions
 PCI for Chronic Total Occlusions Chronic Total Occlusions Why not Medical Treatment? Medical Treatment CTO in 891 pts over 24 years High 10% Mortality Low 2 % 1 year 10 years Puma JA, et al. JACC 1994;23:390A
PCI for Chronic Total Occlusions Chronic Total Occlusions Why not Medical Treatment? Medical Treatment CTO in 891 pts over 24 years High 10% Mortality Low 2 % 1 year 10 years Puma JA, et al. JACC 1994;23:390A
The Case of the successful PCI for the ostium CTO lesion of the RCA by the retrograde approach
 The Case of the successful PCI for the ostium CTO lesion of the RCA by the retrograde approach NAGOYA KYORITSU HOSPITAL DAISUKE KAMOI K.KAWASHIMA, Y.KAWAMURA, M.TANAKA T.AOYAMA Case : 58y.o. Male CC: CCSⅡ
The Case of the successful PCI for the ostium CTO lesion of the RCA by the retrograde approach NAGOYA KYORITSU HOSPITAL DAISUKE KAMOI K.KAWASHIMA, Y.KAWAMURA, M.TANAKA T.AOYAMA Case : 58y.o. Male CC: CCSⅡ
Excimer Laser for Coronary Intervention: Case Study RADIAL APPROACH: CORONARY LASER ATHERECTOMY FOR CTO OF THE LAD FOLLOWED BY PTCA NO STENTING
 Excimer Laser for Coronary Intervention: Case Study RADIAL APPROACH: CORONARY LASER ATHERECTOMY FOR CTO OF THE LAD FOLLOWED BY PTCA NO STENTING 1 2013 Spectranetics. All Rights Reserved. Approved for External
Excimer Laser for Coronary Intervention: Case Study RADIAL APPROACH: CORONARY LASER ATHERECTOMY FOR CTO OF THE LAD FOLLOWED BY PTCA NO STENTING 1 2013 Spectranetics. All Rights Reserved. Approved for External
Lessons for Successful Subintimal Angioplasty in SFA CTO
 Lessons for Successful Subintimal Angioplasty in SFA CTO John R. Laird Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center CTOs in the Periphery Presence of Total Occlusion
Lessons for Successful Subintimal Angioplasty in SFA CTO John R. Laird Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center CTOs in the Periphery Presence of Total Occlusion
Retrograde approach: a practical guide for maximizing procedural success
 SPECIAL FOCUS y Chronic total occlusions review Retrograde approach: a practical guide for maximizing procedural success The aim of this article is to focus on the practical aspects of performing retrograde
SPECIAL FOCUS y Chronic total occlusions review Retrograde approach: a practical guide for maximizing procedural success The aim of this article is to focus on the practical aspects of performing retrograde
HKSTENT 2012: 2012/3/3-4 11:47 12:17 CTO Complication
 HKSTENT 2012: 2012/3/3-4 11:47 12:17 CTO Complication SATORU SUMITSUJI MD. FACC. Specially Appointed Associate Professor Advanced Cardiovascular Therapeutics, Osaka University Director of Heart Center,
HKSTENT 2012: 2012/3/3-4 11:47 12:17 CTO Complication SATORU SUMITSUJI MD. FACC. Specially Appointed Associate Professor Advanced Cardiovascular Therapeutics, Osaka University Director of Heart Center,
CTO Angioplasty Lessons from the Summit
 CTO Angioplasty Lessons from the Summit Gregg W. Stone, MD Columbia University Medical Center The Cardiovascular Research Foundation New York City The 1 st International CTO Summit January 2004 47 faculty
CTO Angioplasty Lessons from the Summit Gregg W. Stone, MD Columbia University Medical Center The Cardiovascular Research Foundation New York City The 1 st International CTO Summit January 2004 47 faculty
CTO PCI. Yangsoo Jang, MD, PhD, FACC. Medicine, Yonsei University Health System,
 Expert Review on CTO PCI Yangsoo Jang, MD, PhD, FACC Yonsei University College of Medicine, Yonsei University Health System, Cardiology Division Easy CTO vs. Tough CTO Usual guiding g catheters in PCI
Expert Review on CTO PCI Yangsoo Jang, MD, PhD, FACC Yonsei University College of Medicine, Yonsei University Health System, Cardiology Division Easy CTO vs. Tough CTO Usual guiding g catheters in PCI
Percutanous revascularization of chronic total occlusion of diabetic patients at Iraqi center for heart diseases, a single center experience 2012
 www.muthjm.com Muthanna Medical Journal 2015; 2(2):76-82 Percutanous revascularization of chronic total occlusion of diabetic patients at Iraqi center for heart diseases, a single center experience 2012
www.muthjm.com Muthanna Medical Journal 2015; 2(2):76-82 Percutanous revascularization of chronic total occlusion of diabetic patients at Iraqi center for heart diseases, a single center experience 2012
Complication management and long-term outcome after percutaneous coronary intervention
 Complication management and long-term outcome after percutaneous coronary intervention ESC meeting 2012, Munich, Germany Session: Chronic total occlusion: a challenge for percutaneous coronary intervention
Complication management and long-term outcome after percutaneous coronary intervention ESC meeting 2012, Munich, Germany Session: Chronic total occlusion: a challenge for percutaneous coronary intervention
Radiation Safety Abbott Vascular. All rights reserved.
 Radiation Safety More and more complex cases are performed Complexity Index and Fluoroscopy Time 2 3 Collimators / Distances The intensity of scattered radiation is a function of exposed field size Use
Radiation Safety More and more complex cases are performed Complexity Index and Fluoroscopy Time 2 3 Collimators / Distances The intensity of scattered radiation is a function of exposed field size Use
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Hybrid algorithm for chronic total occlusion percutaneous coronary intervention
 SPECIAL FOCUS y Chronic total occlusions commentary Hybrid algorithm for chronic total occlusion percutaneous coronary intervention The emphasis [of the hybrid approach] is on procedural efficiency, recommending
SPECIAL FOCUS y Chronic total occlusions commentary Hybrid algorithm for chronic total occlusion percutaneous coronary intervention The emphasis [of the hybrid approach] is on procedural efficiency, recommending
Successful revascularization of LCX-CTO via a underlying
 IPS/CTO LIVE 2012 ;@ Asan Medical Center, Seoul, Korea Successful revascularization of LCX-CTO via a underlying collateral l channel The Department of Cardiology, Daini i Okamoto general hospital Masaki
IPS/CTO LIVE 2012 ;@ Asan Medical Center, Seoul, Korea Successful revascularization of LCX-CTO via a underlying collateral l channel The Department of Cardiology, Daini i Okamoto general hospital Masaki
CTO: Technique and Tools
 CTO: Technique and Tools S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Associate Editor: Cath Cardiov Interventions UT
CTO: Technique and Tools S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Associate Editor: Cath Cardiov Interventions UT
Optimal Revascularization in Multivessel Disease and Coronary CTO. Dr Simon Walsh MD FRCP FSCAI Consultant Cardiologist Belfast Trust
 Optimal Revascularization in Multivessel Disease and Coronary CTO Dr Simon Walsh MD FRCP FSCAI Consultant Cardiologist Belfast Trust Potential Conflicts of Interest Speaker's name: Simon Walsh Consulting
Optimal Revascularization in Multivessel Disease and Coronary CTO Dr Simon Walsh MD FRCP FSCAI Consultant Cardiologist Belfast Trust Potential Conflicts of Interest Speaker's name: Simon Walsh Consulting
Guide Wires design and selection Abbott Vascular. All rights reserved.
 Guide Wires design and selection the cardiac catheter was...the key in the lock Cournand AF, Nobel lecture December 11, 1956; nowadays, the coronary guidewire is the master key to all locks Colombo et
Guide Wires design and selection the cardiac catheter was...the key in the lock Cournand AF, Nobel lecture December 11, 1956; nowadays, the coronary guidewire is the master key to all locks Colombo et
CHRONIC TOTAL OCCLUSION IN PATIENTS AFTER CORONARY ARTERY BYPASS GRAFTING: A REVIEW OF POSSIBLE INTERVENTIONS AND RESULTS WITH A CASE STUDY
 CHRONIC TOTAL OCCLUSION IN PATIENTS AFTER CORONARY ARTERY BYPASS GRAFTING: A REVIEW OF POSSIBLE INTERVENTIONS AND RESULTS WITH A CASE STUDY *Sergey N. Furkalo Department of Endovascular Surgery and Angiography,
CHRONIC TOTAL OCCLUSION IN PATIENTS AFTER CORONARY ARTERY BYPASS GRAFTING: A REVIEW OF POSSIBLE INTERVENTIONS AND RESULTS WITH A CASE STUDY *Sergey N. Furkalo Department of Endovascular Surgery and Angiography,
Endovascular Approach to CTOs: Crossing methods and Devices
 Endovascular Approach to CTOs: Crossing methods and Devices Anish J. Thomas, MD FACC FSCAI Interventional Cardiology Vascular/Endovascular Medicine SSM Heart Institute St. Louis, MO Disclosure Consultant:
Endovascular Approach to CTOs: Crossing methods and Devices Anish J. Thomas, MD FACC FSCAI Interventional Cardiology Vascular/Endovascular Medicine SSM Heart Institute St. Louis, MO Disclosure Consultant:
Coronary artery Dissection. Dr TP Singh MD,DM
 Coronary artery Dissection Dr TP Singh MD,DM 52 M,Non HT, Non DM,Acute IWMI lysed within 4 hours D2 Coronary angiography RCA mid 90% discrete hazy stenosis LAD non significant ifi disease, LCx Normal Taken
Coronary artery Dissection Dr TP Singh MD,DM 52 M,Non HT, Non DM,Acute IWMI lysed within 4 hours D2 Coronary angiography RCA mid 90% discrete hazy stenosis LAD non significant ifi disease, LCx Normal Taken
Bifurcation stenting with BVS
 Bifurcation stenting with BVS Breaking the limits or just breaking the struts? Maciej Lesiak Department of Cardiology University Hospital in Poznan, Poland Disclosure Speaker s name: Maciej Lesiak I have
Bifurcation stenting with BVS Breaking the limits or just breaking the struts? Maciej Lesiak Department of Cardiology University Hospital in Poznan, Poland Disclosure Speaker s name: Maciej Lesiak I have
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
Algorithm and Tools for the Uncrossable CTO
 Algorithm and Tools for the Uncrossable CTO David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Algorithm and Tools for the Uncrossable CTO David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Annals of Vascular Diseases Advance Published Date: June 2, Horie K, et al.
 2016 Annals of Vascular Diseases doi:10.3400/avd.cr.16-00007 Case Report Recanalization of a Heavily Calcified Chronic Total Occlusion in a Femoropopliteal Artery Using a Wingman Crossing Catheter Kazunori
2016 Annals of Vascular Diseases doi:10.3400/avd.cr.16-00007 Case Report Recanalization of a Heavily Calcified Chronic Total Occlusion in a Femoropopliteal Artery Using a Wingman Crossing Catheter Kazunori
Appropriate Device Selection for Endovascular Procedures
 Appropriate Device Selection for Endovascular Procedures Thomas M. Shimshak, MD Florida Hospital Heartland Medical Center Sebring, Florida Disclosures Speaker s Bureau: Abbott Vascular Boston Scientific
Appropriate Device Selection for Endovascular Procedures Thomas M. Shimshak, MD Florida Hospital Heartland Medical Center Sebring, Florida Disclosures Speaker s Bureau: Abbott Vascular Boston Scientific
Coronary Artery Perforation Angioplasty Summit Seoul April 30, 2005
 Coronary Artery Perforation Angioplasty Summit Seoul April 30, 2005 James R. Margolis, M.D. Miami International Cardiology Consultants Miami, Florida USA Introduction In the stent era, coronary artery
Coronary Artery Perforation Angioplasty Summit Seoul April 30, 2005 James R. Margolis, M.D. Miami International Cardiology Consultants Miami, Florida USA Introduction In the stent era, coronary artery
Chronic Total Occlusion: A case for coronary artery bypass grafting
 Chronic Total Occlusion: A case for coronary artery bypass grafting Prof. Alfredo R Galassi MD, FESC, FACC, FSCAI Director of Cardiac Catheterization and Interventional Cardiology Unit Department of Medical
Chronic Total Occlusion: A case for coronary artery bypass grafting Prof. Alfredo R Galassi MD, FESC, FACC, FSCAI Director of Cardiac Catheterization and Interventional Cardiology Unit Department of Medical
Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries
 MEET 2013 Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HOSPITAL AND MEDICAL CENTER READING, PA USA Chronic
MEET 2013 Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HOSPITAL AND MEDICAL CENTER READING, PA USA Chronic
Chronic Total Occlusion (CTO) Technologies
 Technologies") to receive our latest news and key activities. Chronic Total Occlusion (CTO) Technologies Re-open vital channels LinkedIn page Follow us on CORDIS EMEA OUTBACK LTD Re-Entry Catheter True Lumen Re-Entry
to receive our latest news and key activities. Chronic Total Occlusion (CTO) Technologies Re-open vital channels LinkedIn page Follow us on CORDIS EMEA OUTBACK LTD Re-Entry Catheter True Lumen Re-Entry
Selection and Use of Basic Equipment : Guiding Catheters, Wires and Balloons
 SCAI Interventional Cardiology Fall Fellows Course 2014 Selection and Use of Basic Equipment : Guiding Catheters, Wires and Balloons December 7, 2014 8:30 am John S. Douglas Jr, MD Professor of Medicine
SCAI Interventional Cardiology Fall Fellows Course 2014 Selection and Use of Basic Equipment : Guiding Catheters, Wires and Balloons December 7, 2014 8:30 am John S. Douglas Jr, MD Professor of Medicine
RECOMMENDED INSTRUCTIONS FOR USE
 Rapid Exchange PTCA Dilatation Catheter RECOMMENDED INSTRUCTIONS FOR USE Available in diameters 1.25mm to 4.5mm and in lengths 09mm to 40mm Caution: This device should be used only by physicians trained
Rapid Exchange PTCA Dilatation Catheter RECOMMENDED INSTRUCTIONS FOR USE Available in diameters 1.25mm to 4.5mm and in lengths 09mm to 40mm Caution: This device should be used only by physicians trained
Euro-Asia CTO Club Can we Implement Japanese Techniques in Europe?
 Euro-Asia CTO Club Can we Implement Japanese Techniques in Europe? T. Lefèvre,, Massy, France Background Despite continuous improvement, PTCA of chronic total occlusion remains a real technical challenge.
Euro-Asia CTO Club Can we Implement Japanese Techniques in Europe? T. Lefèvre,, Massy, France Background Despite continuous improvement, PTCA of chronic total occlusion remains a real technical challenge.
Total occlusion at ostial Left internal mammary graft with successful angioplasty and longterm patency result
 DOI 10.7603/s40602-014-0017-x ASEAN Heart Journal http://www.aseanheartjournal.org/ Vol. 22, no. 1, 116 121 (2014) ISSN: 2315-4551 Case Report Total occlusion at ostial Left internal mammary graft with
DOI 10.7603/s40602-014-0017-x ASEAN Heart Journal http://www.aseanheartjournal.org/ Vol. 22, no. 1, 116 121 (2014) ISSN: 2315-4551 Case Report Total occlusion at ostial Left internal mammary graft with
MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION
 MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION C. Graidis, D. Dimitriadis, A. Ntatsios, V. Karasavvides Euromedica Kyanous Stavros, Thessaloniki.
MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION C. Graidis, D. Dimitriadis, A. Ntatsios, V. Karasavvides Euromedica Kyanous Stavros, Thessaloniki.
Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut
 Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct Professor Emory University School of Medicine Indication
Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct Professor Emory University School of Medicine Indication
SCAI Fall Fellows Course Subclavian/Innominate Case Presentation
 SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
UC SF. Introduction: Retrograde Access. Pedal Access: When to Do It How Does it Fare. Introduction: Retrograde Access. Introduction: Retrograde Access
 Introduction: Retrograde Access Pedal Access: When to Do It How Does it Fare Wide spread application of endovascular techniques to infrageniculate arterial occlusive disease Technical failure rate of crossing
Introduction: Retrograde Access Pedal Access: When to Do It How Does it Fare Wide spread application of endovascular techniques to infrageniculate arterial occlusive disease Technical failure rate of crossing
Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)?
 or Coronary Artery Bypass Graft Surgery (CABG)?") Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Effectiveness of IVUS in Complex Cases
 Effectiveness of IVUS in Complex Cases Satoru Sumituji,M.D. Rinku General Medical Center IVUS is can provide images of the vessel wall and the tissue around the vessel which cannot be viewed by angiography.
Effectiveness of IVUS in Complex Cases Satoru Sumituji,M.D. Rinku General Medical Center IVUS is can provide images of the vessel wall and the tissue around the vessel which cannot be viewed by angiography.
CPT Code Details
 CPT Code 93572 Details Code Descriptor Intravascular Doppler velocity and/or pressure derived coronary flow reserve measurement (coronary vessel or graft) during coronary angiography including pharmacologically
CPT Code 93572 Details Code Descriptor Intravascular Doppler velocity and/or pressure derived coronary flow reserve measurement (coronary vessel or graft) during coronary angiography including pharmacologically
When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E
 When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E Thrombus in STEMI Over 70% of STEMI patients has angiographic evidence of thrombus
When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E Thrombus in STEMI Over 70% of STEMI patients has angiographic evidence of thrombus
Chronic Total Occlusion (CTO) Technologies. Re-open vital channels
 Technologies. Re-open vital channels") Chronic Total Occlusion (CTO) Technologies Re-open vital channels OUTBACK LTD Re-Entry Catheter True Lumen Re-Entry Technology Get back into the true lumen with ease and precision There are a number of
Chronic Total Occlusion (CTO) Technologies Re-open vital channels OUTBACK LTD Re-Entry Catheter True Lumen Re-Entry Technology Get back into the true lumen with ease and precision There are a number of
Late Breaking Clinical Trials: The Consistent CTO study
 Late Breaking Clinical Trials: The Consistent CTO study CONventional antegrade vs Sub-Intimal Synergy stenting in Chronic Total Occlusions Dr Simon Walsh on behalf of the Consistent CTO Investigators Introduction
Late Breaking Clinical Trials: The Consistent CTO study CONventional antegrade vs Sub-Intimal Synergy stenting in Chronic Total Occlusions Dr Simon Walsh on behalf of the Consistent CTO Investigators Introduction
Procedure planning for chronic total occlusion percutaneous coronary intervention
 SPECIAL FOCUS y Chronic total occlusions review Procedure planning for chronic total occlusion percutaneous coronary intervention To maximize procedure success, chronic total occlusion percutaneous coronary
SPECIAL FOCUS y Chronic total occlusions review Procedure planning for chronic total occlusion percutaneous coronary intervention To maximize procedure success, chronic total occlusion percutaneous coronary
Αγγειοπλαστική σε Nόσο Στελέχους: Που βρισκόμαστε. Βάιος Τζίφος Δ/ντής Τμήματος Επεμβατικής Καρδιολογίας Τομέας Καρδιάς Ερρίκος Ντυνάν Hospital Center
 Αγγειοπλαστική σε Nόσο Στελέχους: Που βρισκόμαστε. Βάιος Τζίφος Δ/ντής Τμήματος Επεμβατικής Καρδιολογίας Τομέας Καρδιάς Ερρίκος Ντυνάν Hospital Center Δεν έχω οικονομική σχέση με φαρμακευτική εταιρία.
Αγγειοπλαστική σε Nόσο Στελέχους: Που βρισκόμαστε. Βάιος Τζίφος Δ/ντής Τμήματος Επεμβατικής Καρδιολογίας Τομέας Καρδιάς Ερρίκος Ντυνάν Hospital Center Δεν έχω οικονομική σχέση με φαρμακευτική εταιρία.
ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions
 Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES
 MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES PUSHING BOUNDARIES Terumo Interventional Systems is committed to your success with innovative procedural solutions and ongoing support for your most challenging
MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES PUSHING BOUNDARIES Terumo Interventional Systems is committed to your success with innovative procedural solutions and ongoing support for your most challenging
The Role of the Retrograde Approach in Percutaneous Coronary Interventions for Chronic Total Occlusions : Insights from the Japanese Retrograde
 Interventional Cardiology The Role of the Retrograde Approach in Percutaneous Coronary Interventions for Chronic Total Occlusions : Insights from the Japanese Retrograde Summit Registry Background: Percutaneous
Interventional Cardiology The Role of the Retrograde Approach in Percutaneous Coronary Interventions for Chronic Total Occlusions : Insights from the Japanese Retrograde Summit Registry Background: Percutaneous
Between Coronary Angiography and Fractional Flow Reserve
 Visual-Functional Mismatch Between Coronary Angiography and Fractional Flow Reserve Seung-Jung Park, MD., PhD. University of Ulsan, College of Medicine Asan Medical Center, Seoul, Korea Visual - Functional
Visual-Functional Mismatch Between Coronary Angiography and Fractional Flow Reserve Seung-Jung Park, MD., PhD. University of Ulsan, College of Medicine Asan Medical Center, Seoul, Korea Visual - Functional
STEMI ST Elevation Myocardial Infarction
 STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
Chronic Total Occlusions Current Techniques and future directions. International Journal of Cardiology
 ÔØ Å ÒÙ Ö ÔØ Chronic Total Occlusions Current Techniques and future directions George Touma, David Ramsay, James Weaver PII: S2352-9067(15)00017-2 DOI: doi: 10.1016/j.ijcha.2015.02.002 Reference: IJCHA
ÔØ Å ÒÙ Ö ÔØ Chronic Total Occlusions Current Techniques and future directions George Touma, David Ramsay, James Weaver PII: S2352-9067(15)00017-2 DOI: doi: 10.1016/j.ijcha.2015.02.002 Reference: IJCHA
Antonio Colombo. Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy. Miracor Symposium. Speaker: 15. Parigi: May 16-19, 2017
 Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Percutaneous Coronary Interventions Without On-site Cardiac Surgery
 Percutaneous Coronary Interventions Without On-site Cardiac Surgery Hassan Al Zammar, MD,FESC Consultant & Interventional Cardiologist Head of Cardiology Department European Gaza Hospital Palestine European
Percutaneous Coronary Interventions Without On-site Cardiac Surgery Hassan Al Zammar, MD,FESC Consultant & Interventional Cardiologist Head of Cardiology Department European Gaza Hospital Palestine European
DISRUPT CAD. Todd J. Brinton, MD Clinical Associate Professor of Medicine Adjunct Professor of Bioengineering Stanford University
 DISRUPT CAD A multicenter, prospective, single-arm study of percutaneous Lithoplasty prior to stent implantation in heavily calcified coronary lesions Todd J. Brinton, MD Clinical Associate Professor of
DISRUPT CAD A multicenter, prospective, single-arm study of percutaneous Lithoplasty prior to stent implantation in heavily calcified coronary lesions Todd J. Brinton, MD Clinical Associate Professor of
Carotid Artery Stenting
 Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Breakage and retention of wire fragments
 Case Report Hellenic J Cardiol 2011; 52: 79-83 Septal Wire Entrapment During Recanalisation of a Chronic Total Occlusion with the Retrograde Approach Georgios Sianos, Michail I. Papafaklis 1st Cardiology
Case Report Hellenic J Cardiol 2011; 52: 79-83 Septal Wire Entrapment During Recanalisation of a Chronic Total Occlusion with the Retrograde Approach Georgios Sianos, Michail I. Papafaklis 1st Cardiology
NCVD-PCI Registry. Percutaneous Coronary Intervention (PCI) Registry, MALAYSIA c/o National Heart Association of Malaysia
 Registry, MALAYSIA c/o National Heart Association of Malaysia") NCVD-PCI Registry National Cardiovascular Disease Database (NCVD) National Cardiovascular Disease Database (NCVD) Percutaneous Coronary Intervention (PCI) Registry, MALAYSIA c/o National Heart Association
NCVD-PCI Registry National Cardiovascular Disease Database (NCVD) National Cardiovascular Disease Database (NCVD) Percutaneous Coronary Intervention (PCI) Registry, MALAYSIA c/o National Heart Association
Disclosures. Tips and Tricks for Tibial Intervention. Tibial intervention overview
 Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
PCI TO CHRONIC TOTAL OCCLUSION, LIAQUAT NATIONAL HOSPITAL EXPERINCE
 SUMMARY PCI TO CHRONIC TOTAL OCCLUSION, LIAQUAT NATIONAL HOSPITAL EXPERINCE INTRODUCTION GHAZALA IRFAN*, MANSOOR AHMAD**, DAD JAN BALOCH @, ABDUL RASHEED @@ BACKGROUND PCI of chronic total occlusion represents
SUMMARY PCI TO CHRONIC TOTAL OCCLUSION, LIAQUAT NATIONAL HOSPITAL EXPERINCE INTRODUCTION GHAZALA IRFAN*, MANSOOR AHMAD**, DAD JAN BALOCH @, ABDUL RASHEED @@ BACKGROUND PCI of chronic total occlusion represents
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
REBEL. Platinum Chromium Coronary Stent System. Patient Information Guide
 REBEL Patient Information Guide REBEL PATIENT INFORMATION GUIDE You have recently had a REBEL bare metal stent implanted in the coronary arteries of your heart. The following information is important for
REBEL Patient Information Guide REBEL PATIENT INFORMATION GUIDE You have recently had a REBEL bare metal stent implanted in the coronary arteries of your heart. The following information is important for
The Retrograde Technique for Recanalization of Chronic Total Occlusions
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 1, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2011.10.011 STATE-OF-THE-ART
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 1, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2011.10.011 STATE-OF-THE-ART
Making the difference with Live Image Guidance
 Interventional Cardiology AlluraClarity Making the difference with Live Image Guidance Diagnosis and treatment of coronary artery diseases and atherosclerosis Where/who The First Bethune Hospital of Jilin
Interventional Cardiology AlluraClarity Making the difference with Live Image Guidance Diagnosis and treatment of coronary artery diseases and atherosclerosis Where/who The First Bethune Hospital of Jilin
Contrast-induced nephropathy (CIN) is a serious complication
 is a serious complication") Case Reports Successful Complete Revascularization With PCI Using Super-Low Volume of Contrast Medium in a Patient With Three-Vessel Disease Including 2 Chronic Total Occlusions With Severe Renal Dysfunction
Case Reports Successful Complete Revascularization With PCI Using Super-Low Volume of Contrast Medium in a Patient With Three-Vessel Disease Including 2 Chronic Total Occlusions With Severe Renal Dysfunction
IVUS Analysis. Myeong-Ki. Hong, MD, PhD. Cardiac Center, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea
 IVUS Analysis Myeong-Ki Hong, MD, PhD Cardiac Center, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Intimal disease (plaque) is dense and will appear white Media is made of
IVUS Analysis Myeong-Ki Hong, MD, PhD Cardiac Center, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Intimal disease (plaque) is dense and will appear white Media is made of
Coronary Interventions Indications, Treatment Options and Outcomes
 Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Debate Should we use FFR? I will say NO.
 Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Chronic Total Occlusion: a case for coronary artery bypass grafting
 Chronic Total Occlusion: a case for coronary artery bypass grafting Rune Haaverstad Professor & Chief Dept. of Cardiothoracic Surgery Haukeland University Hospital Bergen, Norway Disclosure Research cooperation
Chronic Total Occlusion: a case for coronary artery bypass grafting Rune Haaverstad Professor & Chief Dept. of Cardiothoracic Surgery Haukeland University Hospital Bergen, Norway Disclosure Research cooperation
TOSCA-5. Total Occlusion Studies in Coronary Arteries - 5. phase-2 placebo controlled study of MZ- 004 collagenase
 Total Occlusion Studies in Coronary Arteries - 5 phase-2 placebo controlled study of MZ- 004 collagenase C.E. Buller, J.J. Graham, A. Bagai, H. Wijeysundera for the Investigators Disclosures consultant
Total Occlusion Studies in Coronary Arteries - 5 phase-2 placebo controlled study of MZ- 004 collagenase C.E. Buller, J.J. Graham, A. Bagai, H. Wijeysundera for the Investigators Disclosures consultant
BSIC, Manchester, September 15, Gerald S. Werner, MD, FESC, FACC Klinikum Darmstadt, Germany
 BSIC, Manchester, September 15, 2006 Gerald S. Werner, MD, FESC, FACC Klinikum Darmstadt, Germany BSIC, Manchester, September 15, 2006 Chronic total occlusions update A European perspective Gerald S. Werner,
BSIC, Manchester, September 15, 2006 Gerald S. Werner, MD, FESC, FACC Klinikum Darmstadt, Germany BSIC, Manchester, September 15, 2006 Chronic total occlusions update A European perspective Gerald S. Werner,
Clinical Summary. Live Cases I - IX
 Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG