J. Schwitter, MD, FESC Section of Cardiology
|
|
|
- Elisabeth Wells
- 5 years ago
- Views:
Transcription

1 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque


2 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Stress CMR to Guide Complex Revascularization in Stable CAD ESC Meeting Munich, Germany August 28, 2012 Centre de RM Cardiaque
3 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Stress CMR to Guide Complex Revascularization in Stable CAD ESC Meeting Munich, Germany August 28, 2012 Disclosure: - no conflicts of interest - Gd-based contrast media are not approved for CMR in the US and in some European countries
4 CMR in Complicated Revascularizations: Examples CABG: yes or no CABG: 1 vs 2 vs 3 grafts PCI vs CABG PCI and complications CABG and concomitant diseases CABG vs drugs/transplantation
5 CMR in Complicated Revascularizations: Examples CABG: yes or no CABG: 1 vs 2 vs 3 grafts PCI vs CABG PCI and complications CABG and concomitant diseases CABG vs drugs/transplantation



6 septal septal Hibernating Myocardium vs Scar: To Revascularize or Not? LV mass: 205.7g LV scar mass: 46.2g LV scar: 22.5% anterior Subendocardial scar lateral inferior anterior Transmural scar lateral inferior Knuesel et al. Circulation, 2001
7 Characterization of Dysfunctional Myocardium by PET and MR: Relation to Functional Outcome After Revascularization Baseline Follow-up 3% 2% 2% 3% 10% 71% functional improvement 10% 93% 28% Viability 77% PET/MR +/+ PET/MR -/+ PET/MR -/- PET/MR +/- 29% no functional improvement 7% 27% 38% Scar < 4mm, viable rim > 4 mm Recovery of function Scar > 4mm, viable rim < 4 mm Recovery of function P.R. Knuesel et al. Circulation, 2003
8 Hibernating Myocardium vs Scar: To Revascularize or Not? High-Risk Patient: pre-interventional assessment Patient E, 49 years EF 34% Patient S, 62 years 22%




9 Hibernating Myocardium vs Scar: To Revascularize or Not? High-Risk Patient: pre-interventional assessment Large transmural scar No intervention EF 34%




10 Hibernating Myocardium vs Scar: To Revascularize or Not? High-Risk Patient: pre-interventional assessment Small scar Revascularization indicated EF 22% Knuesel, Schwitter et al. Circ. 2003




11 Hibernating Myocardium vs Scar: To Revascularize or Not? High-Risk Patient: pre-interventional assessment EF 22% Pre-operative EF 37% 3 months post-operative Knuesel, Schwitter et al. Circ. 2003
12 CMR in Complicated Revascularizations: Examples CABG: yes or no CABG: 1 vs 2 vs 3 grafts PCI vs CABG PCI and complications CABG and concomitant diseases CABG vs drugs/transplantation
13 Mortality and outcome of patients stratified by number of vessels treated Mortality in patients undergoing CABGs Multivariate Cox proportion regression model N.H. Lopes et al. Eur J Cardiothorac Surg 2008;33:
14 Clinical case 1: CMR for viability assessment 57 y.o male Severe mitral regurgitation LVEF 40%, hypokinesia of the infero-lateral wall Ad coronary angiogram prior to mitral valve repair


15 Clinical case 1: CMR for viability assessment
")
16 Clinical case 1: CMR for viability assessment LGE in the inferior wall (100% transmurality)


17 Clinical case 1: CMR for viability assessment Mitral valve repair CABG LAD CABG CX CABG RCA Time of procedure is reduced
18 CMR in Complicated Revascularizations: Examples CABG: yes or no CABG: 1 vs 2 vs 3 grafts PCI vs CABG PCI and complications CABG and concomitant diseases CABG vs drugs/transplantation
19 MR-IMPACT I (18 centers) MR-IMPACT II (33 centers) Perfusion-CMR all SPECT Gated-SPECT * CMR superior to SPECT p= CMR superior to SPECT p= MR 1- Specificity J. Schwitter et al. Eur Heart J 2008;29: Specificity J. Schwitter et al. JCMR 2012, in press
20 Case 2: CMR for Ischemia Assessment Patient history: Hypertension, high cholesterol CABG x 3 for stable angina 16 years ago LIMA to mid-lad / 2 nd diagonal branch VG to 1 st diagonal branch VG to intermediate branch and 1 st OM branch
21 Case 2: CMR for Ischemia Assessment Recurrence of exertional angina since summer 2009, CCS II Resting ECG normal Stress ECG (bicycle) at 227 W (=10 METs): no angina no ECG changes Sent to private clinic for coronary angiogram
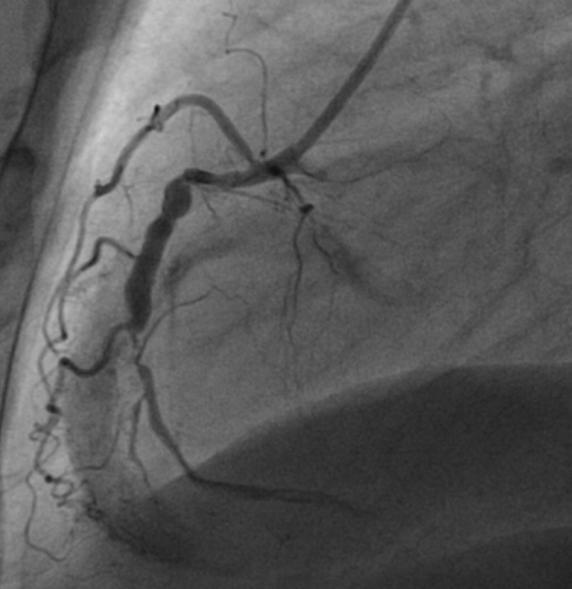
22 Case 2: CMR for Ischemia Assessment Coronary angiogram LIMA graft patent 2 vein grafts occluded LAD: proximally occluded LCX: severe proximal and mid-vessel stenosis RCA: distal 70% stenosis and 70% stenosis of the PLV branch, gives collaterals to LCX and intermediate branch LV-angiogram: LVEF 73%

23 Case 2: CMR for Ischemia Assessment Atrial branch Intermediate LCx Graft OM1


24 Case 2: CMR for Ischemia Assessment Mr R.W. 63 yo
25 Case 2: CMR for Ischemia Assessment Mr R.W. 63 yo First cardiology opinion: CABG re-do because of the lesion complexity, despite good functioning LIMA graft Bifurcation stenosis of the RCA which gives collaterals to the left system Occlusion of the intermediate branch Long and complex lesion of the LCx Sent for second opinion

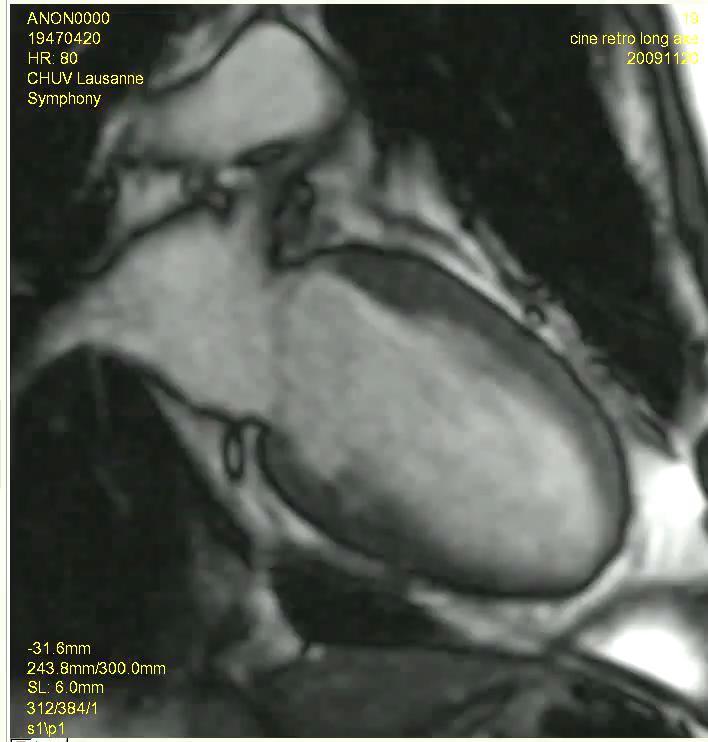
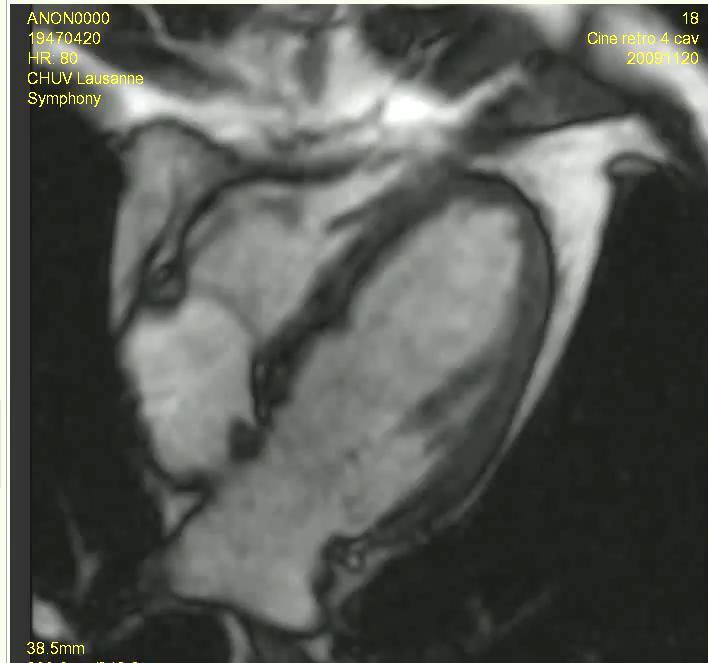
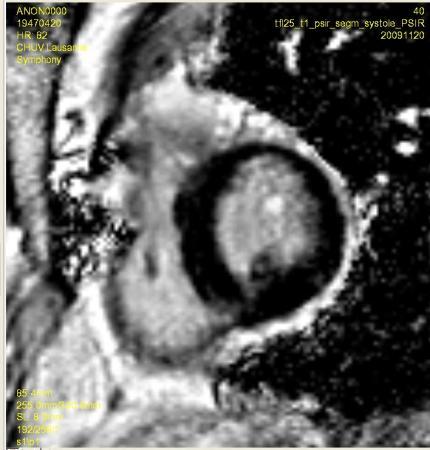
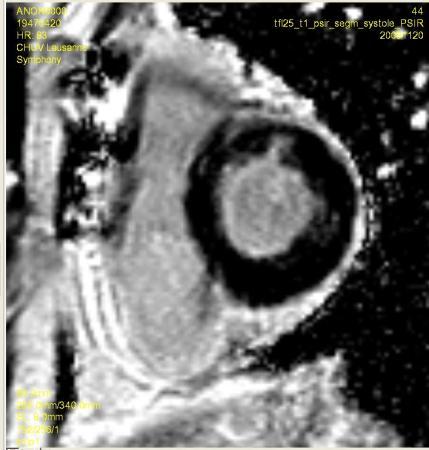
26 Case 2: CMR for Ischemia Assessment CMR 1 Cine: LVEF 58%



27 Case 2: CMR for Ischemia Assessment


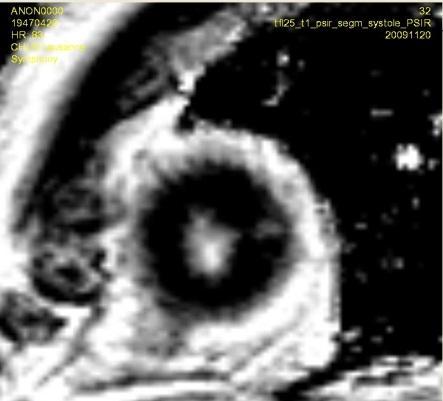
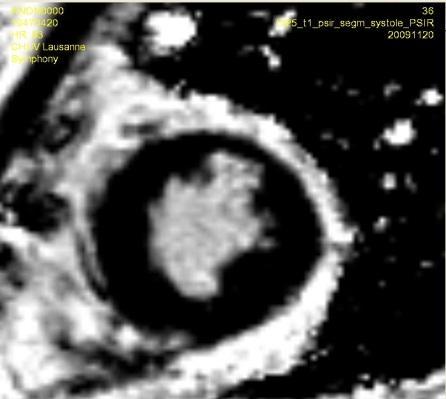
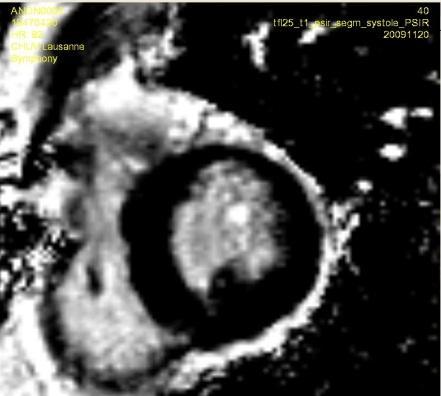
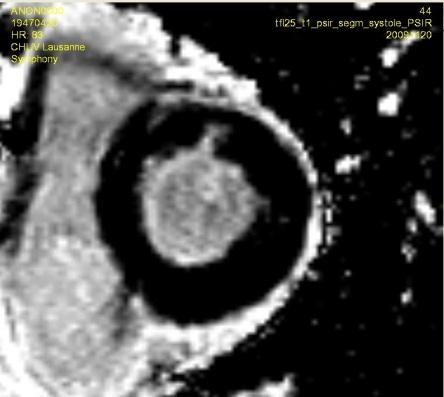
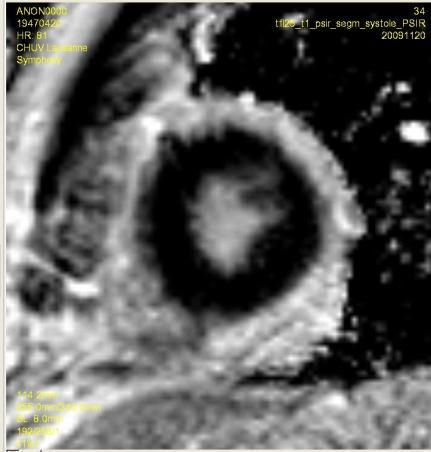
28 LGE PEAK PRE Case 2: CMR for Ischemia Assessment BASE APEX
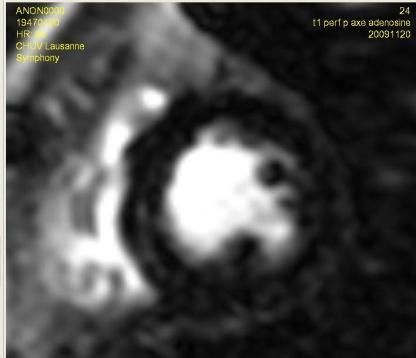
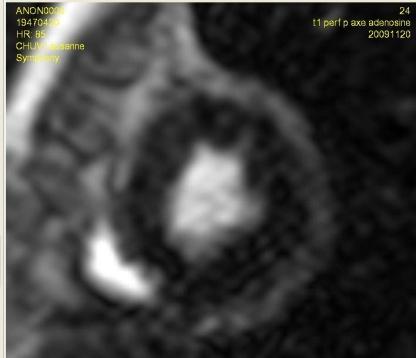
29 Case 2: CMR for Ischemia Assessment Cine: LVEF 58% LGE: small basal-mid anterior subendocardial scar Perfusion: extensive defect in the anterior, anteroseptal and lateral wall No perfusion defect in the RCA territory
30 Case 2: CMR for Ischemia Assessment Cine: LVEF 58% LGE: small basal-mid anterior subendocardial scar Perfusion: extensive defect in the anterior, anteroseptal and lateral wall No perfusion defect in the RCA territory No need for RCA revascularisation Aim for lateral wall revascularisation Remaining graft between OM1 and intermediate should improve anterior wall perfusion PCI is a suitable option
31 Case 2: CMR for Ischemia Assessment Mr R.W. 63 yo Sent for PCI to LCX only LCX angioplasty with stenting of the mid-vessel stenosis Dilatation of the LMS with rotablator, then stenting to the LM-ostial LCX

32 Case 2: CMR for Ischemia Assessment
33 Case 2: CMR for Ischemia Assessment Repeat CMR 1 month after intervention Patient symptom free



34 Case 2: CMR for Ischemia Assessment Mr R.W. 63 yo Cine: LVEF 64% LGE: unchanged small basal anterior scar


35 Case 2: CMR for Ischemia Assessment Mr R.W. 63 yo BASE APEX
36 Case 2: CMR for Ischemia Assessment Mr R.W. 63 yo Take home messages Simple ECG stress test is probably insufficient for ischemia assessment after CABG. Stress imaging is recommended. Accurate assessment of myocardial viability and of the distribution of inducible perfusion defects with CMR is of great value, especially in case of complex coronary lesions It adds a functional assessment to the morphologic angiographic picture, and allows to better targeting PCI (and to avoid unnecessary, potentially dangerous re-op)
37 CMR in Complicated Revascularizations: Examples CABG: yes or no CABG: 1 vs 2 vs 3 grafts PCI vs CABG PCI and complications CABG and concomitant diseases CABG vs drugs/transplantation
38 Case 3: CMR for Complications Assessment 59 y.o male art. hypertension, DM, positive family history known CTO of the RCA Ad PCI of the RCA Failure of anterograde recanalisation of the RCA Locca et al., Circulation, 2007

39 Case 3: CMR for Complications Assessment Retrograde approach via the septal collaterals Implantation of 4 DES TIMI flow 3 at the end of the procedure Locca et al., Circulation, 2007

40 Case 3: CMR for Complications Assessment Retrograde approach via the septal collaterals Implantation of 4 DES TIMI flow 3 at the end of the procedure Locca et al., Circulation, 2007
 - CK-MB: 7.8 g/l (0 6) 48h 48h Edema Necrosis Locca et al.")
41 Case 3: CMR for Complications Assessment unchanged ECG before/after PCI 24h after PCI: - Peak troponin I: 1.19 g/l (0.04) - CK-MB: 7.8 g/l (0 6) 48h 48h Edema Necrosis Locca et al., Circulation, 2007
 - CK-MB: 7.8 g/l (0 6) 48h Edema Necrosis Perforation Locca et al.")
42 Case 3: CMR for Complications Assessment unchanged ECG before/after PCI 24h after PCI: - Peak troponin I: 1.19 g/l (0.04) - CK-MB: 7.8 g/l (0 6) 48h Edema Necrosis Perforation Locca et al., Circulation, 2007
 - CK-MB: 7.8 g/l (0 6) 48h 8 w Edema No Edema Locca et al., Circulation, 2007")
43 Case 3: CMR for Complications Assessment unchanged ECG before/after PCI 24h after PCI: At 24 hours after PCI - Peak troponin I: 1.19 g/l (0.04) - CK-MB: 7.8 g/l (0 6) 48h 8 w Edema No Edema Locca et al., Circulation, 2007



44 Spontaneous Dissection of LCX Not Requiring PCI R. Van 40 40Heeswijk, JACC Cvimaging, in press 30 30
45 CMR in Complicated Revascularizations: Examples CABG: yes or no CABG: 1 vs 2 vs 3 grafts PCI vs CABG PCI and complications CABG and concomitant diseases CABG vs drugs/transplantation
46 Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease 4 year-old boy S/p Switch operation Ostial stenosis of the LCX at the RCA sinus JCMR 2008 E. Valsangiacomo et al.

47 Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease JCMR 2008 E. Valsangiacomo et al.
48 Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease JCMR 2008 E. Valsangiacomo et al.
49 Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease JCMR 2008 E. Valsangiacomo et al.

50 Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease JCMR 2008 E. Valsangiacomo et al.



51 Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease





")
52 Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease Systole forward Flow (black) Diastole retrograde Flow (bright)
53 Flow (L/min) Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease LCX: Diameter ~1.5mm PCI CABG + Replacement of pulmonary valve in aortic position HR: 72 bpm RF: 46% # image


54 Case 4: CMR for Assessment of Coronary Circulation in Congenital Heart Disease Perfusion Pre-CABG LCX: Diameter ~1.5mm Perfusion Post-CABG PCI CABG + Replacement of pulmonary valve in aortic position
55 CMR in Complicated Revascularizations: Examples CABG: yes or no CABG: 1 vs 2 vs 3 grafts PCI vs CABG PCI and complications CABG and concomitant diseases CABG vs drugs/transplantation
56 July 2011 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? 62 y.o male History of inferior MI - RF: DM, HT, hypercholesterolemia, smoking Dyspnea NYHA II On echo: ischemia of anterior and infero-septal wall EF 22% X-ray coronary angiography


57 July 2011 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP?


58 July 2011 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? Ischemia? Ischemia?
59 July 2011 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? 62 y.o male History of inferior MI - RF: DM, HT, hypercholesterolemia, smoking Dyspnea NYHA II On echo: ischemia of anterior and infero-septal wall EF 22% X-ray coronary angiography: 50% LAD, 90% LCX, 50-70% CD Ad CMR: ischemia and viability

60 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? Diastole Systole


61 LV-EF: 14% LVEDVI 365 ml Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP?
62 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? Diastole Systole


63 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP?
64 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP?

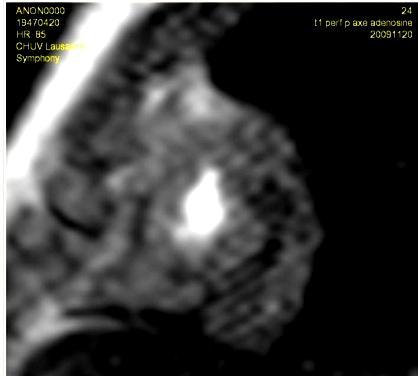
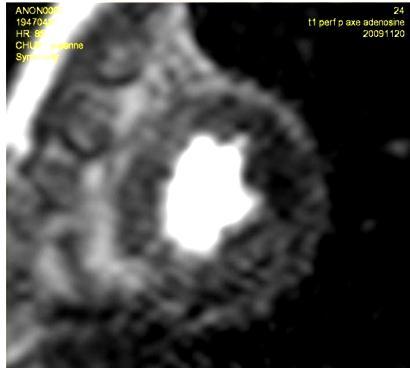
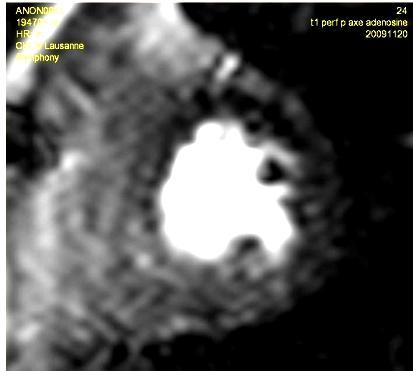
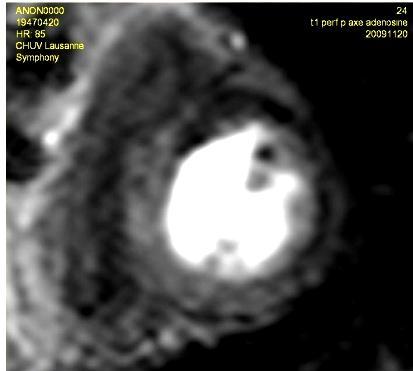
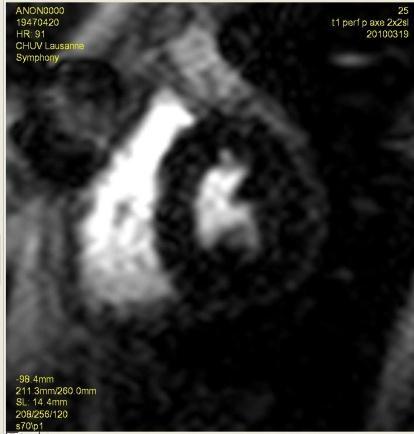
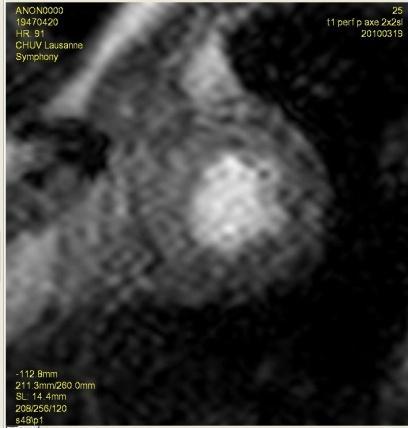
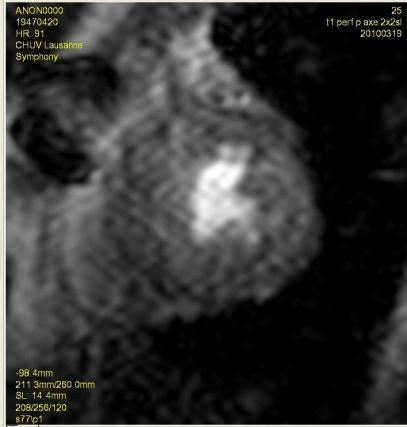
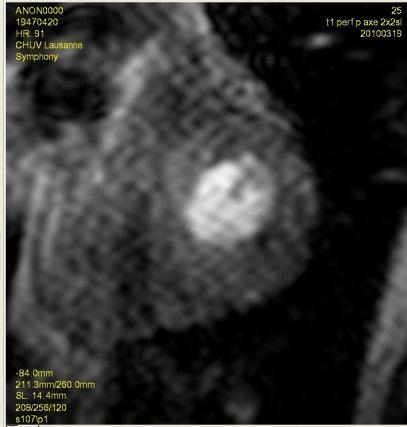
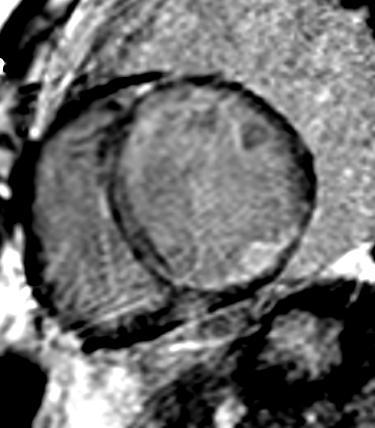
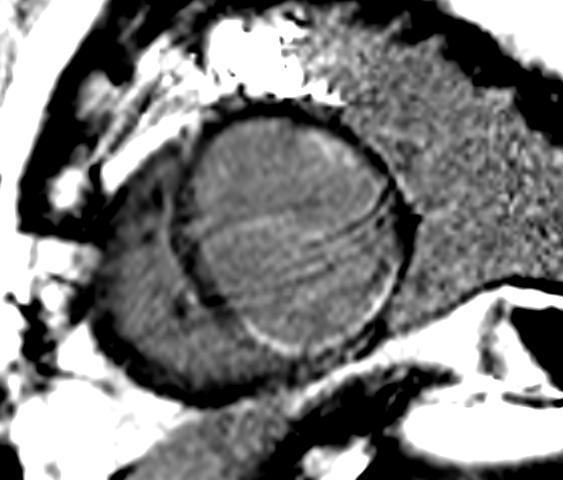
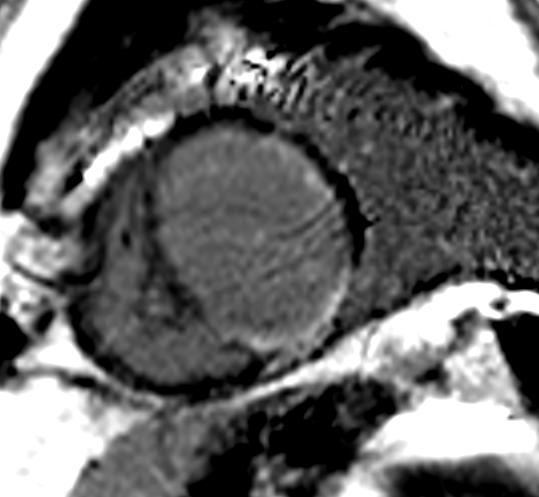
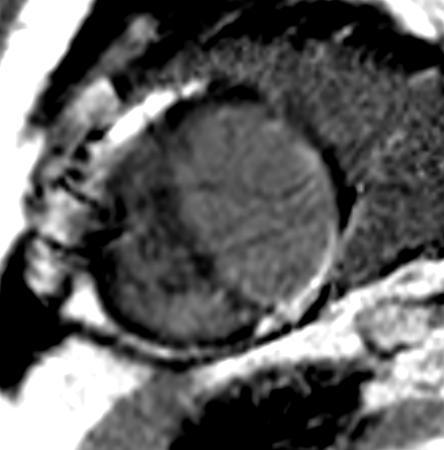
65 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? Pre-contrast Peak First Pass Scar

66 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? Pre-contrast Peak First Pass Ischemia? Scar

67 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? Pre-contrast Peak First Pass Ischemia? Scar


68 Occlusion Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? PCI


69 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP?
70 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP?

71 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP?

72 LV-EF: 20% LVEDV: 372 ml LV Function post-revascularization
73 Case 5: CMR for Assessment of Viability and Ischemia CAD vs dil CMP? 14 g of scar tissue do not explain a LV-EF of 20% The combination of CAD and dil CMP most likely explain the reduced EF, i.e. the heart failure symptoms in this patient No Revascularization Transplantation to discuss (or CRT?)
74 CABG: yes or no CABG: 1 vs 2 vs 3 grafts PCI vs CABG CMR in Complicated Revascularizations PCI and complications CABG and concomitant diseases CABG vs drugs/transplantation CMR can help in decision making by assessing viability, ischemia, and concomitant diseases such as dilative CMP, valvular heart disease etc.
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
Clinical Summary. Live Cases I - IX
 Clinical Summary Live Cases I - IX Case #1 2017/09/16 Age: 66 Target Vessel: RCA proximal Relevant Diagnosis: Single vessel CAD with normal LVEF Coronary Risk Factors: Hypertension, smoke (90py) ECG abnormality:
Clinical Summary Live Cases I - IX Case #1 2017/09/16 Age: 66 Target Vessel: RCA proximal Relevant Diagnosis: Single vessel CAD with normal LVEF Coronary Risk Factors: Hypertension, smoke (90py) ECG abnormality:
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Imaging in Ischemic Heart Disease: Role of Cardiac MRI
 Imaging in Ischemic Heart Disease: Role of Cardiac MRI Chiara Bucciarelli Ducci MD, PhD, FESC, FRCP Consultant Senior Lecturer Cardiologist Bristol Heart Institute, University of Bristol, UK Chair elect,
Imaging in Ischemic Heart Disease: Role of Cardiac MRI Chiara Bucciarelli Ducci MD, PhD, FESC, FRCP Consultant Senior Lecturer Cardiologist Bristol Heart Institute, University of Bristol, UK Chair elect,
Clinical Summary. Live Cases I - IX
 Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Antonio Colombo. Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy. Miracor Symposium. Speaker: 15. Parigi: May 16-19, 2017
 Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
MR Assessment of Myocardial Viability
 MR Assessment of Myocardial Viability Definition of Viability Clinical Metabolism: Presence of glucose uptake Perfusion / Perfusion reserve Morphology: Wall thickness, wall thickening Contractility: Recovery
MR Assessment of Myocardial Viability Definition of Viability Clinical Metabolism: Presence of glucose uptake Perfusion / Perfusion reserve Morphology: Wall thickness, wall thickening Contractility: Recovery
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Pearls & Pitfalls in nuclear cardiology
 Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Imaging and heart failure
 Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Chronic Total Occlusion: A case for coronary artery bypass grafting
 Chronic Total Occlusion: A case for coronary artery bypass grafting Prof. Alfredo R Galassi MD, FESC, FACC, FSCAI Director of Cardiac Catheterization and Interventional Cardiology Unit Department of Medical
Chronic Total Occlusion: A case for coronary artery bypass grafting Prof. Alfredo R Galassi MD, FESC, FACC, FSCAI Director of Cardiac Catheterization and Interventional Cardiology Unit Department of Medical
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium. Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute
 Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
@02-126_Coronary_calcification.ppt. Professor Molecular and Medical Pharmacology
 Assessment of Myocardial Viability Jamshid Maddahi, M.D., FACC, FASNC Professor Molecular and Medical Pharmacology (Nuclear Medicine) and Medicine (Cardiology) David Geffen School of Medicine at UCLA Director,
Assessment of Myocardial Viability Jamshid Maddahi, M.D., FACC, FASNC Professor Molecular and Medical Pharmacology (Nuclear Medicine) and Medicine (Cardiology) David Geffen School of Medicine at UCLA Director,
FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT
 FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT01724957 Dobrin Vassilev MD, PhD Assoc. Prof. in Cardiology Head Cardiology Clinic, Alexandrovska University Hospital Medical
FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT01724957 Dobrin Vassilev MD, PhD Assoc. Prof. in Cardiology Head Cardiology Clinic, Alexandrovska University Hospital Medical
EAE Teaching Course. Magnetic Resonance Imaging. Competitive or Complementary? Sofia, Bulgaria, 5-7 April F.E. Rademakers
 EAE Teaching Course Magnetic Resonance Imaging Competitive or Complementary? Sofia, Bulgaria, 5-7 April 2012 F.E. Rademakers Complementary? Of Course N Engl J Med 2012;366:54-63 Clinical relevance Treatment
EAE Teaching Course Magnetic Resonance Imaging Competitive or Complementary? Sofia, Bulgaria, 5-7 April 2012 F.E. Rademakers Complementary? Of Course N Engl J Med 2012;366:54-63 Clinical relevance Treatment
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System
 Volume 1, Issue 1 Case Report Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System Robert F. Riley * and Bill Lombardi University of Washington Medical Center, Division
Volume 1, Issue 1 Case Report Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System Robert F. Riley * and Bill Lombardi University of Washington Medical Center, Division
Coronary Revascularization in Patients witj Severe LV Dysfunction.: Is the concept of viability still viable?
 Coronary Revascularization in Patients witj Severe LV Dysfunction.: Implications of the STICH trial Is the concept of viability still viable? Banff 2016 3041435-1 Prognosis of Patients With LV Dysfunction
Coronary Revascularization in Patients witj Severe LV Dysfunction.: Implications of the STICH trial Is the concept of viability still viable? Banff 2016 3041435-1 Prognosis of Patients With LV Dysfunction
Coronary Revascularization for Severe LV Dysfunction Is s. Is the concept of viability testing still viable?
 Coronary Revascularization for Severe LV Dysfunction Is s Is the concept of viability testing still viable? Banff 2017 2015 MFMER 3492638-7 Prognosis of Patients With LV Dysfunction and CAD Major determinants
Coronary Revascularization for Severe LV Dysfunction Is s Is the concept of viability testing still viable? Banff 2017 2015 MFMER 3492638-7 Prognosis of Patients With LV Dysfunction and CAD Major determinants
Cardiologic history. Anamnesis. Female BD Risk factors HTN, DM, Dyslipidaemia. Cardiologic Long history. Last admission Heart failure
 Anamnesis Cardiologic history Female BD 29.7.1939 Risk factors HTN, DM, Dyslipidaemia Cardiologic Long history Last admission Heart failure 2004 NSTEMI CX stenosis DES on CX 2012 Acute Pulmonary Oedema
Anamnesis Cardiologic history Female BD 29.7.1939 Risk factors HTN, DM, Dyslipidaemia Cardiologic Long history Last admission Heart failure 2004 NSTEMI CX stenosis DES on CX 2012 Acute Pulmonary Oedema
Current Indications for Cardiac MRI: What You See is What You Get?
 Current Indications for Cardiac MRI: What You See is What You Get? Javier Ganame, MD, PhD, FASE No disclosures Cardiology Update, Niagara, Sept 24th, 2016 The Ideal Diagnostic Technique Easy to apply Accurate
Current Indications for Cardiac MRI: What You See is What You Get? Javier Ganame, MD, PhD, FASE No disclosures Cardiology Update, Niagara, Sept 24th, 2016 The Ideal Diagnostic Technique Easy to apply Accurate
Percutaneous Coronary Interventions Without On-site Cardiac Surgery
 Percutaneous Coronary Interventions Without On-site Cardiac Surgery Hassan Al Zammar, MD,FESC Consultant & Interventional Cardiologist Head of Cardiology Department European Gaza Hospital Palestine European
Percutaneous Coronary Interventions Without On-site Cardiac Surgery Hassan Al Zammar, MD,FESC Consultant & Interventional Cardiologist Head of Cardiology Department European Gaza Hospital Palestine European
Ventricular tachycardia and ischemia. Martin Jan Schalij Department of Cardiology Leiden University Medical Center
 Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Debate Should we use FFR? I will say NO.
 Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium
 FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
Richard Grocott Mason
 Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Patient. Clinical data Indications: Operation date. Comorbidities: Patient code Birth date: / /
 Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
CASE from South Korea
 CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이
 Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Radiologic Assessment of Myocardial Viability
 November 2001 Radiologic Assessment of Myocardial Viability Joshua Moss, Harvard Medical School Year III Patient EF 66yo female with a 3-year history of intermittent chest pain previously relieved by sublingual
November 2001 Radiologic Assessment of Myocardial Viability Joshua Moss, Harvard Medical School Year III Patient EF 66yo female with a 3-year history of intermittent chest pain previously relieved by sublingual
Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center
 CMR Perfusion and Viability A STICH Out of Time? Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center Can Imaging Improve
CMR Perfusion and Viability A STICH Out of Time? Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center Can Imaging Improve
Abnormal, Autoquant Adenosine Myocardial Perfusion Heart Imaging. ID: GOLD Date: Age: 46 Sex: M John Doe Phone (310)
") Background: Reason: preoperative assessment of CAD, Shortness of Breath Symptom: atypical chest pain Risk factors: hypertension Under influence: a beta blocker Medications: digoxin Height: 66 in. Weight:
Background: Reason: preoperative assessment of CAD, Shortness of Breath Symptom: atypical chest pain Risk factors: hypertension Under influence: a beta blocker Medications: digoxin Height: 66 in. Weight:
Chronic Total Occlusions. Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute
 Chronic Total Occlusions Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute Financial Disclosures /see -tee-oh / abbr. Med. Chronic Total Occlusion,
Chronic Total Occlusions Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute Financial Disclosures /see -tee-oh / abbr. Med. Chronic Total Occlusion,
Conflict Disclosures. Vermont Cardiac Network. Outline. Series Learning Objectives 4/27/2016. Scott E. Friedman April 28, 2016
 Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
Flexibility of the COMBO Dual Therapy Stent
 TM CaseSpotlight Flexibility of the COMBO Dual Therapy Stent Doctor Peter den Heijer is an of the Catheterization Laboratory at the Department of Cardiology of the Amphia Ziekenhuis, Breda, The Netherlands.
TM CaseSpotlight Flexibility of the COMBO Dual Therapy Stent Doctor Peter den Heijer is an of the Catheterization Laboratory at the Department of Cardiology of the Amphia Ziekenhuis, Breda, The Netherlands.
Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease
 Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions
 Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Myocardial Infarction
 Myocardial Infarction MI = heart attack Defined as necrosis of heart muscle resulting from ischemia. A very significant cause of death worldwide. of these deaths, 33% -50% die before they can reach the
Myocardial Infarction MI = heart attack Defined as necrosis of heart muscle resulting from ischemia. A very significant cause of death worldwide. of these deaths, 33% -50% die before they can reach the
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Gated blood pool ventriculography: Is there still a role in myocardial viability?
 Gated blood pool ventriculography: Is there still a role in myocardial viability? Oliver C. Alix, MD Adult Clinical and Nuclear Cardiology St. Luke s Medical Centre - Global City Case Presentation A 62-year-old
Gated blood pool ventriculography: Is there still a role in myocardial viability? Oliver C. Alix, MD Adult Clinical and Nuclear Cardiology St. Luke s Medical Centre - Global City Case Presentation A 62-year-old
Basic Coronary Angiography DAVID SHAVELLE MD
 Basic Coronary Angiography DAVID SHAVELLE MD Basic Coronary Angiography: Take Home Points Cardiovascular Medicine Boards and Clinical Practice Understand normal coronary anatomy Understand different imaging
Basic Coronary Angiography DAVID SHAVELLE MD Basic Coronary Angiography: Take Home Points Cardiovascular Medicine Boards and Clinical Practice Understand normal coronary anatomy Understand different imaging
High Risk PCI for Heart Failure
 High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
MRI ACS-ben. Tamás Simor MD, PhD, Med Hab. University of Pécs, Heart Institute
 MRI ACS-ben Tamás Simor MD, PhD, Med Hab Time Course of Changes in Infarct Size, Viable Myocardium, and LV Mass After Reperfused and Nonreperfused MI Blue lines denote reperfused myocardial infarction
MRI ACS-ben Tamás Simor MD, PhD, Med Hab Time Course of Changes in Infarct Size, Viable Myocardium, and LV Mass After Reperfused and Nonreperfused MI Blue lines denote reperfused myocardial infarction
SPECT-CT: Τι πρέπει να γνωρίζει ο Καρδιολόγος
 SPECT-CT: Τι πρέπει να γνωρίζει ο Καρδιολόγος Δρ Αναστασία Κίτσιου Διευθύντρια, Καρδιολογική Κλινική, Σισμανόγλειο ΓΝΑ Chair, Education Committee, Section on Nuclear Cardiology & Cardiac CT, EACVI, ESC
SPECT-CT: Τι πρέπει να γνωρίζει ο Καρδιολόγος Δρ Αναστασία Κίτσιου Διευθύντρια, Καρδιολογική Κλινική, Σισμανόγλειο ΓΝΑ Chair, Education Committee, Section on Nuclear Cardiology & Cardiac CT, EACVI, ESC
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
The new Guidelines: Focus on Chronic Heart Failure
 The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
Ve V rmont rmon Card Car iac d Netw Ne ork tw Scott E. Friedman April 28, 2016
 Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Case Presentation #1
 Case Presentation #1 SCAI Fellows Course December 7, 2013 Barry F Uretsky, MD University of Arkansas for Medical Sciences Central Arkansas Veterans Health System Little Rock, AR Case Presentation #1 65
Case Presentation #1 SCAI Fellows Course December 7, 2013 Barry F Uretsky, MD University of Arkansas for Medical Sciences Central Arkansas Veterans Health System Little Rock, AR Case Presentation #1 65
Dr Felix Keng. Imaging of the heart is technically difficult because: Role of Cardiac MSCT. Current: Cardiac Motion Respiratory Motion
 Siemens Philips Dr Felix Keng GE Toshiba Role of Cardiac MSCT Current: Structural / congenital heart imaging Extra-cardiac / Great vessel imaging Volumes and ejection fractions (cine + gating) Calcium
Siemens Philips Dr Felix Keng GE Toshiba Role of Cardiac MSCT Current: Structural / congenital heart imaging Extra-cardiac / Great vessel imaging Volumes and ejection fractions (cine + gating) Calcium
Percutaneous coronary intervention of RIMA. The real challenge!
 Percutaneous coronary intervention of RIMA The real challenge! Speaker's name: I do not have any potential conflict of interest Clinical Case 76-year old woman Previous History Actual Disease Diabetes
Percutaneous coronary intervention of RIMA The real challenge! Speaker's name: I do not have any potential conflict of interest Clinical Case 76-year old woman Previous History Actual Disease Diabetes
PCI for Left Main Coronary Artery Stenosis. Jean Fajadet Clinique Pasteur, Toulouse, France
 PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
Complex PCI of an LAD/Diagonal bifurcation lesion (Medina 1,1,1) utilizing the DK Crush technique ".
 utilizing the DK Crush technique .") Complex PCI of an LAD/Diagonal bifurcation lesion (Medina 1,1,1) utilizing the DK Crush technique ". "Σύμπλοκη αγγειοπλαστική βλάβης διχασμού LAD/Diagonal (Medina 1,1,1) με την τεχνική DK crush ". Anastasios
Complex PCI of an LAD/Diagonal bifurcation lesion (Medina 1,1,1) utilizing the DK Crush technique ". "Σύμπλοκη αγγειοπλαστική βλάβης διχασμού LAD/Diagonal (Medina 1,1,1) με την τεχνική DK crush ". Anastasios
Disclosures. GETTING TO THE HEART OF THE MATTER WITH MULTIMODALITY CARDIAC IMAGING Organ Review Meeting 25 September. Overview
 GETTING TO THE HEART OF THE MATTER WITH MULTIMODALITY CARDIAC IMAGING Organ Review Meeting 25 September Disclosures None relevant to this presentation Mini Pakkal Assistant Professor of Radiology University
GETTING TO THE HEART OF THE MATTER WITH MULTIMODALITY CARDIAC IMAGING Organ Review Meeting 25 September Disclosures None relevant to this presentation Mini Pakkal Assistant Professor of Radiology University
Alex versus Xience Registry Preliminary report
 Interventional Cardiology Network Alex versus Xience Preliminary report Mariusz Gąsior 1,2, Marek Gierlotka 1, Lech Poloński 1,2 1 3rd Department of Cardiology, Medical University of Silesia Centre tor
Interventional Cardiology Network Alex versus Xience Preliminary report Mariusz Gąsior 1,2, Marek Gierlotka 1, Lech Poloński 1,2 1 3rd Department of Cardiology, Medical University of Silesia Centre tor
Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery. Christian Seiler No conflict of interest to declare.
 Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery Christian Seiler No conflict of interest to declare PCI Long-Term Outcome Perioperative Management After Coronary Stenting:
Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery Christian Seiler No conflict of interest to declare PCI Long-Term Outcome Perioperative Management After Coronary Stenting:
Bifurcation stenting with BVS
 Bifurcation stenting with BVS Breaking the limits or just breaking the struts? Maciej Lesiak Department of Cardiology University Hospital in Poznan, Poland Disclosure Speaker s name: Maciej Lesiak I have
Bifurcation stenting with BVS Breaking the limits or just breaking the struts? Maciej Lesiak Department of Cardiology University Hospital in Poznan, Poland Disclosure Speaker s name: Maciej Lesiak I have
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
The MAIN-COMPARE Study
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Mandatory knowledge about natural history of coronary grafts. P.Sergeant P. Maureira K.U.Leuven, Belgium
 Mandatory knowledge about natural history of coronary grafts P.Sergeant P. Maureira K.U.Leuven, Belgium Types of grafts Arterial ITA/IMA (internal thoracic/mammary artery) Radial artery Gastro-epiploïc
Mandatory knowledge about natural history of coronary grafts P.Sergeant P. Maureira K.U.Leuven, Belgium Types of grafts Arterial ITA/IMA (internal thoracic/mammary artery) Radial artery Gastro-epiploïc
Stress Echo Cases Sunday, October 8, :10 3:30 PM 20 min
 2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E
 When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E Thrombus in STEMI Over 70% of STEMI patients has angiographic evidence of thrombus
When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E Thrombus in STEMI Over 70% of STEMI patients has angiographic evidence of thrombus
Management of High-Risk CAD : Surgeons Perspective
 Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Imaging congestive heart failure: role of coronary computed tomography angiography (CCTA)
") Imaging congestive heart failure: role of coronary computed tomography angiography (CCTA) Gianluca Pontone, MD, PhD, FESC, FSCCT Director of MR Unit Deputy Director of Cardiovascul CT Unit Clinical Cardiology
Imaging congestive heart failure: role of coronary computed tomography angiography (CCTA) Gianluca Pontone, MD, PhD, FESC, FSCCT Director of MR Unit Deputy Director of Cardiovascul CT Unit Clinical Cardiology
What the Cardiologist needs to know from Medical Images
 What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
The role of Magnetic Resonance Imaging in the diagnosis of viability & Coronary Artery Disease
 The role of Magnetic Resonance Imaging in the diagnosis of viability & Coronary Artery Disease G.P. Spanos, MSc, Phd Head of CardioVascular Imaging Tomographia Diagnostic Center Cardiovascular magnetic
The role of Magnetic Resonance Imaging in the diagnosis of viability & Coronary Artery Disease G.P. Spanos, MSc, Phd Head of CardioVascular Imaging Tomographia Diagnostic Center Cardiovascular magnetic
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Typical chest pain with normal ECG
 Typical chest pain with normal ECG F. Mut, C. Bentancourt, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history Male 41 y.o. Overweight, hypertension, high cholesterol,
Typical chest pain with normal ECG F. Mut, C. Bentancourt, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history Male 41 y.o. Overweight, hypertension, high cholesterol,
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Cardiac Care Network of Ontario
 Cardiac Care Network of Ontario Cardiac Wait Times Patient Triage Business Rules December 2016 TABLE OF CONTENTS 1. Introduction... 3 1.1. Document Purpose... 3 1.2. Document Structure... 3 2. Algorithms...
Cardiac Care Network of Ontario Cardiac Wait Times Patient Triage Business Rules December 2016 TABLE OF CONTENTS 1. Introduction... 3 1.1. Document Purpose... 3 1.2. Document Structure... 3 2. Algorithms...
Chronic Total Occlusion: a case for coronary artery bypass grafting
 Chronic Total Occlusion: a case for coronary artery bypass grafting Rune Haaverstad Professor & Chief Dept. of Cardiothoracic Surgery Haukeland University Hospital Bergen, Norway Disclosure Research cooperation
Chronic Total Occlusion: a case for coronary artery bypass grafting Rune Haaverstad Professor & Chief Dept. of Cardiothoracic Surgery Haukeland University Hospital Bergen, Norway Disclosure Research cooperation
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
FRACTIONAL FLOW RESERVE: STANDARD OF CARE
 FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
FFR-guided Jailed Side Branch Intervention
 FFR-guided Jailed Side Branch Intervention - Pressure wire in Bifurcation lesions - Bon-Kwon Koo, MD, PhD Seoul National University Hospital, Seoul, Korea Bifurcation Lesions Bifurcation Lesions Still
FFR-guided Jailed Side Branch Intervention - Pressure wire in Bifurcation lesions - Bon-Kwon Koo, MD, PhD Seoul National University Hospital, Seoul, Korea Bifurcation Lesions Bifurcation Lesions Still
Cardiac Stress MRI: Detection of Ischemia. Disclosures: Dobutamine Stress MR. April 28, 2018
 Cardiac MRI: Detection of Ischemia Cardiac MRI in Today s Clinical Practice Foundations of Cardiovascular Magnetic Resonance Daniel C. Lee, MD, MSc Assistant Professor of Medicine and Radiology Co-Director,
Cardiac MRI: Detection of Ischemia Cardiac MRI in Today s Clinical Practice Foundations of Cardiovascular Magnetic Resonance Daniel C. Lee, MD, MSc Assistant Professor of Medicine and Radiology Co-Director,
FFR vs. icecg in Coronary Bifurcations (FIESTA) - preliminary results. Dobrin Vassilev MD, PhD National Heart Hospital Sofia, Bulgaria
 - preliminary results. Dobrin Vassilev MD, PhD National Heart Hospital Sofia, Bulgaria") FFR vs. icecg in Coronary Bifurcations (FIESTA) - preliminary results Dobrin Vassilev MD, PhD National Heart Hospital Sofia, Bulgaria I would like to express my personal gratitude to Dr. BK Koo for opening
FFR vs. icecg in Coronary Bifurcations (FIESTA) - preliminary results Dobrin Vassilev MD, PhD National Heart Hospital Sofia, Bulgaria I would like to express my personal gratitude to Dr. BK Koo for opening
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr..
 Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Successful revascularization of LCX-CTO via a underlying
 IPS/CTO LIVE 2012 ;@ Asan Medical Center, Seoul, Korea Successful revascularization of LCX-CTO via a underlying collateral l channel The Department of Cardiology, Daini i Okamoto general hospital Masaki
IPS/CTO LIVE 2012 ;@ Asan Medical Center, Seoul, Korea Successful revascularization of LCX-CTO via a underlying collateral l channel The Department of Cardiology, Daini i Okamoto general hospital Masaki
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
RADIATION HEART DISEASE: MANAGEMENT STRATEGIES
 RADIATION HEART DISEASE: MANAGEMENT STRATEGIES AMMAR CHAUDHARY MBChB, ABIM, FRCPC ASSOCIATE CONSULTANT CARDIOLOGIST KING FAISAL SPECIALIST HOSPITAL & RESEARCH CENTER - JEDDAH Scope of the Problem ~ 50
RADIATION HEART DISEASE: MANAGEMENT STRATEGIES AMMAR CHAUDHARY MBChB, ABIM, FRCPC ASSOCIATE CONSULTANT CARDIOLOGIST KING FAISAL SPECIALIST HOSPITAL & RESEARCH CENTER - JEDDAH Scope of the Problem ~ 50
Perfusion, Viability, Edema and Hemorrhage: How it Can (and Should) Change Clinical Practice. Rohan Dharmakumar, Ph.D.
 Change Clinical Practice. Rohan Dharmakumar, Ph.D.") Perfusion, Viability, Edema and Hemorrhage: How it Can (and Should) Change Clinical Practice Rohan Dharmakumar, Ph.D. Director, Translational Cardiac Imaging Research Associate Director, Biomedical Imaging
Perfusion, Viability, Edema and Hemorrhage: How it Can (and Should) Change Clinical Practice Rohan Dharmakumar, Ph.D. Director, Translational Cardiac Imaging Research Associate Director, Biomedical Imaging
Lessons learned From The National PCI Registry
 Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Atypical pain and normal exercise test
 Atypical pain and normal exercise test F. Mut, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history 67-year old male with several coronary risk factors. Atypical
Atypical pain and normal exercise test F. Mut, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history 67-year old male with several coronary risk factors. Atypical
Ischemic heart disease
 Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
National Intervention Council
 National Intervention Council Cardiological Society of India Registry Performa for Coronary, Non- Coronary & Peripheral Interventions Period January 1st 2016 to December 31 st 2016 Dr. (Prof.) N.N. Khanna
National Intervention Council Cardiological Society of India Registry Performa for Coronary, Non- Coronary & Peripheral Interventions Period January 1st 2016 to December 31 st 2016 Dr. (Prof.) N.N. Khanna
Instantaneous Wave-Free Ratio
 Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure