Coronary Artery Disease in 2015: Acute Coronary Syndrome and beyond (Primary and Secondary Prevention of CAD)
|
|
|
- Shannon Lucas
- 5 years ago
- Views:
Transcription
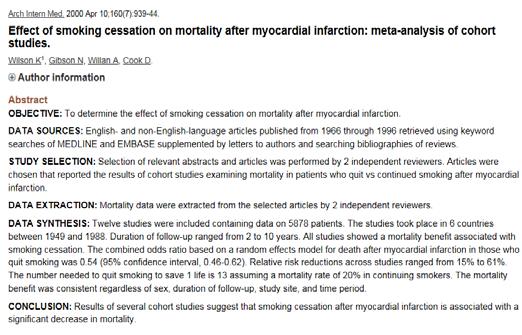
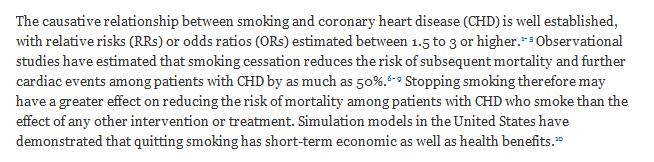
1 Coronary Artery Disease in 2015: Acute Coronary Syndrome and beyond (Primary and Secondary Prevention of CAD) Andrew R. Waxler, MD, FACC Berks Cardiologists, Ltd. President Elect, Berks County Medical Society Cardiology Rep. to PAMED (Specialty Leadership Cabinet) Director, Cardiac Rehab., St. Joseph Medical Center (Reading, PA) 1 Disclosure Dr. Waxler has a financial relationship or interest with a commercial entity that may have a direct interest in the subject matter of this session. Dr. Waxler is a consult and part of a speaker s bureau for Sanofi Pasteur. 2 For a cigarette-smoking patient who has an MI, what is the approximate risk reduction of future MI (over the next several years) that he/she will get from smoking cessation? A. There is no significant change in risk of second MI from smoking cessation at time of first MI B. Only about 10% C. About 25% D. About 50% E. Between % 3 1

2 Based on the most recent (2013) lipid guidelines, which of the following patients do NOT automatically qualify for statin therapy: A. Healthy 37 y.o. woman with LDL 227, no other medical probs B. 54 y.o. man with recent MI and PCI of LAD; his LDL is 65 C. 44 y.o. man with Diabetes and LDL 90; asymptomatic D. Options A and C E. All of the above qualify 4 Which of the following types of patients should receive dual-antiplatelet therapy for 9-12 months following ACS? (ASA/clopid.) A. Patient with ACS treated with Percutaneous Coronary Intervention(PCI)? B. Patient with ACS treated Coronary Artery Bypass Graft (CABG)? C. Patient with ACS treated medically (no PCI or CABG)? D. What about a High-risk patient who has NOT had ACS (ie, DM)? E. A, B, and C F. All of the above 5 We All Know About the Problem 6 2
3 7 8 Vascular Disease: A Generalized and Progressive Process Atherosclerosis Thrombosis Unstable angina ACS MI Ischemic stroke/tia Critical leg ischemia Cardiovascular death Stable angina Intermittent claudication Adapted from Stary HC et a l. Circulation ;92: and Fuster V. Vasc Med ;3:



4 One Method of Diagnosing CAD 10 Cardiac CT 64 Slice Coronary Artery Disease Congenital abnormalities 45 minutes Correlation needed with other studies (stress test or cardiac cath) 11 Sadly, a Common Method of Diagnosing CAD ACS 12 4

.")

5 Hospital Discharges for ACS: UA/NSTEMI vs STEMI USA * ACS 1.67 Million Hospital Discharges ACS MI 700, ,000 USA/NSTEMI NSTEMI 652,000 Discharges per Year STEMI ** 321,000 Discharges per Year Million Discharges per Year * UA=unstable angina. NSTEMI=non ST-segment elevation myocardial infarction (also known as non Q-wave MI). ** STEMI=ST-segment elevation MI (also known as Q-wave MI). American Heart Association. Heart Disease and Stroke Statistics 2005 Update A Dangerous Transition Coronary artery with stable atherosclerosis Coronary artery with ruptured unstable atherosclerotic plaque





6 When there s an elephant on my chest : Don t Do/Watch This Instead, Do This 16 One Often Leads to Another Coronary Atherosclerosis Cardiac catheterization and PCI 17 CAD Starts EARLY 18 6



7 Vascular Disease: A Generalized and Progressive Process Atherosclerosis Thrombosis Unstable angina ACS MI Ischemic stroke/tia Critical leg ischemia Cardiovascular death Stable angina Intermittent claudication Adapted from Stary HC et a l. Circulation ;92: and Fuster V. Vasc Med ;3: Superior doctors prevent the disease. Mediocre doctors treat the disease before evident. Inferior doctors treat the full-blown disease. --Huang Dee: Nai Ching (2600 BC First Chinese Medical Text) 21 7


8 Framingham, Mass



 1999; 100:")
9 National ACC speaker for my upcoming conference 5/2/2015 Circulation. 1999; 100: Circulation. 1998; 97: Framingham Score (CAD event risk) Circulation. 1999; 100:


 5 10 20 40 60 80")
10 28 Lipoprotein (Sub)Classes 0.95 VLDL Chylomicrons IDL Density (g/ml) 1.02 LDL Chylomicron Remnants 1.06 HDL HDL Lp(a) Diameter (nm) 29 10

 Percentage with CHD event 10 9 8 7 WOSCOPS-S 6 5 4 AFCAPS-S AFCAPS-P 3 2 ASCOT-P 1 ASCOT-S 0 2.3 (90) 2.")
11 LDL-C Levels and CAD Risk CAD + Revasc + Stroke (HPS = CAD Only) Solid Shapes = Drug Rx Outline Shapes = Placebo 2 Prevention CAD Events, % S CARE HPS LIPID 1 Prevention AFCAPS WOSCOPS Mean On-Treatment LDL-C Level at Follow-Up, mg/dl Adapted from Am J Cardiol, Vol 82, CM Ballantyne, Low-density lipoproteins and risk for coronary artery disease, pp. 3Q-12Q, Copyright 1998, with permission from Excerpta Medica Inc. Heart Protection Study Collaborative Group. Lancet. 2002;360: Landmark Statin Trials: LDL-C Levels vs Events (primary prevention) Percentage with CHD event WOSCOPS-S AFCAPS-S AFCAPS-P 3 2 ASCOT-P 1 ASCOT-S (90) 2.8 (110) S = statin treated; P = placebo treated 3.4 (130) 3.9 (150) 4.4 (170) 4.9 (190) LDL-C, mmol/l (mg/dl) WOSCOPS-P Primary prevention Pravastatin Lovastatin Atorvastatin 5.4 (210) Modified from Kastelein JJP. Atherosclerosis. 1999;143(suppl 1):S17-S
 Statin (n = 10,269) Placebo (n = 10,267) <100 282 (16.4%) 358 (21.0%) Event Rate Ratio (95% CI) Statin Better Statin Worse 100 129 668 (18.9%) 871 (24.7%) 130 1083 (21.")
12 Heart Protection Study (HPS) 20,536 patients with CAD, other occlusive arterial disease, or DM randomized to simvastatin (40 mg) or placebo for 5.5 years Baseline LDL-C (mg/dl) Statin (n = 10,269) Placebo (n = 10,267) < (16.4%) 358 (21.0%) Event Rate Ratio (95% CI) Statin Better Statin Worse (18.9%) 871 (24.7%) (21.6%) 1356 (26.9%) All patients 2033 (19.8%) 2585 (25.2%) 0.76 ( ) P< CAD=Coronary artery disease, CI=Confidence interval, DM=Diabetes mellitus, HPS Collaborative Group. Lancet 2002;360: Heart Protection Study (5-Year Trial) Simvastatin 40 mg Log CHD Risk Simvastatin 40 mg 26% Reduction in CVD 22% Reduction in CVD LDL-C (mg/dl) Heart Protection Study Collaborative Group. Lancet 2002;360:
13 What Is Desirable Cholesterol? Cholesterol Levels Among Different Human Populations Hazda Inuit!Kung Pygmy San Adult American Hunter-gatherer humans Mean total cholesterol, mg/dl Adapted from O Keefe JH Jr et al. J Am Coll Cardiol. 2004;43: Relationship between LDL-C and Progression Rate Coronary IVUS Progression Trials Median Change In Percent Atheroma Volume (%) REVERSAL atorvastatin A-Plus placebo CAMELOT placebo ACTIVATE placebo REVERSAL pravastatin -0.6 Nissen S. JAMA 2006 ASTEROID rosuvastatin r 2 = 0.95 p< ) Mean Low-Density Lipoprotein Cholesterol (mg/dl)
 1 <70 mg/dl: Therapeutic option for very high-risk patients 1 <100 mg/dl <70 mg/dl AHA/ACC guidelines for")

 plus: multiple major risk factors (especially")
![diabetes); severe and poorly controlled risk factors (eg, cigarette smoking); metabolic syndrome (triglycerides [TG] 200 mg/dl + non HDL-C 130](/docs-images/87/95049518/images/14-3.jpg "mg/dl with HDL-C <40 mg/dl); and acute coronary syndromes. 1 1. Grundy SM et al. Circulation. 2004;110:227 239. 2. Smith SC Jr et al.")
14 Intensive LDL-C Goals for High-Risk Patients Recommended LDL-C treatment goals ATP III Update <100 mg/dl: Patients with CHD or CHD risk equivalents (10-year risk >20%) 1 <70 mg/dl: Therapeutic option for very high-risk patients 1 <100 mg/dl <70 mg/dl AHA/ACC guidelines for patients with CHD*,2 <100 mg/dl: Goal for all patients with CHD,2 <70 mg/dl: A reasonable goal for all patients with CHD, Update If it is not possible to attain LDL-C <70 mg/dl because of a high baseline LDL-C, it generally is possible to achieve LDL-C reductions of >50% with more intensive LDL-C lowering therapy, including drug combinations. *And other forms of atherosclerotic disease. 2 Factors that place a patient at very high risk: established cardiovascular disesase (CVD) plus: multiple major risk factors (especially diabetes); severe and poorly controlled risk factors (eg, cigarette smoking); metabolic syndrome (triglycerides [TG] 200 mg/dl + non HDL-C 130 mg/dl with HDL-C <40 mg/dl); and acute coronary syndromes Grundy SM et al. Circulation. 2004;110: Smith SC Jr et al. Circulation, 2006; 113:

15

16

17

18 52 We ve Come a Long Way Since Back Then But Sadly, Some People Still Haven t Gotten the Message 53 Stopping smoking is easy.i ve done it many times! I don t smoke; the cigarette does! - Said by a patient to Andrew R. Waxler, Internal Medicine intern at UPMC


19 55 Circulation. 1999; 100:


20

21 Clinical Diabetes January 2006 vol. 24 no BMJ 316: , BMJ 316: ,

 PCI (with or without stent) Cath lab CABG Long-term")

.")
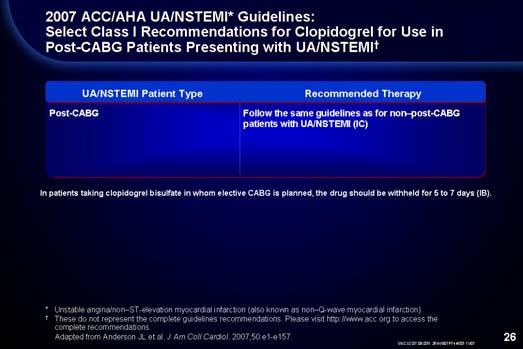
22 64 What about meds for Secondary Prevention? 65 ACC/AHA Treatment Recommendations for the Long-term Management of ACS* ACS (UA/NSTEMI* patients) Medical Management Medical Management (no intervention required) PCI (with or without stent) Cath lab CABG Long-term management 1. ASA 2. Clopid.(?Prasug./Ticag.) 3. ß-blocker 4. ACE Inhibitor 5. Statin * UA/NSTEMI=unstable angina/non ST-segment elevation myocardial infarction (also known as non Q-wave MI). If possible, withhold clopidogrel 5 to 7 days prior to the procedure. 66 Braunwald E, et al. Available at: Accessed February 10,

23 Mechanisms of Action of Oral Antiplatelet Therapies clopidogrel bisulfate ADP dipyridamole ticlopidine HCl ADP phosphodiesterase ADP GP IIb/IIIa (fibrinogen receptor) COX camp Activation collagen thrombin TXA 2 aspirin TXA 2 ADP=adenosine diphosphate, TXA 2 =thromboxane A 2, COX=cyclooxygenase. Schafer AI. Am J Med. 1996;101: Antithrombotic Trialists Collaboration Efficacy of Aspirin Doses on Vascular Events in High-Risk Patients Aspirin Dose # Trials OR* (%) Odds Ratio mg mg mg <75 mg 3 13 Any aspirin Antiplatelet Better Antiplatelet Worse * Odds reduction. Treatment effect P< Adapted with permission from the BMJ Publishing Group. Antithrombotic Trialists Collaboration. BMJ. 2002;324: CURE Primary End Point: MI/Stroke/CV Death Cumulative Hazard Rate Placebo + ASA* Clopidogrel + ASA* 20% Relative Risk Reduction P= N=12,562 The primary outcome occurred in 9.3% of patients in the clopidogrel + ASA group and 11.4% in the placebo + ASA group Months of Follow-Up * Other standard therapies were used as appropriate. PLAVIX Prescribing Information. Adapted with permission (2002) from the Massachusetts Medical Society. The CURE Trial Investigators. N Engl J Med. 2001;345:
24 CURE Patients Treated with PCI * and/or CABG Cumulative Hazard Rate Placebo + ASA (13.8%) Clopidogrel + ASA (11.4%) 18% Relative Risk Reduction (P=0.015 ) * PCI was also referred to as PTCA. Other standard therapies were used as appropriate. Days of Follow-Up In the combined end point of MI, stroke, or CV death. Only first events after randomization were counted in the composite end point. 70 Data on file, Sanofi-Synthelabo Inc. CURE Patients Treated with Medical Therapy 0.20 Without PCI * and/or CABG Cumulative Hazard Rate Placebo + ASA (10.0%) Clopidogrel + ASA (8.1%) 20% Relative Risk Reduction (P= ) Days of Follow-Up * PCI was also referred to as PTCA. Other standard therapies were used as appropriate. In the combined end point of MI, stroke, or CV death. Only first events after randomization were counted in the composite end point. 71 Data on file, Sanofi-Synthelabo Inc. CHARISMA: Overall Population: Primary Efficacy Outcome (MI, Stroke, or CV Death) * 8 Placebo + ASA 7.3% Cumulative event rate (%) Clopidogrel + ASA 6.8% 1 RRR: 7.1% [95% CI: -4.5%, 17.5%] p= Months since randomization * First occurrence of MI, stroke (of any cause), or cardiovascular death. All patients received ASA mg/day. The number of patients followed beyond 30 months decreases rapidly to zero and there are only 21 primary efficacy events that occurred beyond this time (13 clopidogrel and 8 placebo) 1. Adapted from Bhatt DL et al. 2006, in press. 2. Bhatt DL. Presented at ACC
 0.13 Cerebrovascular 4,320 0.84 (0.69, 1.03) 0.09 PAD 2,838 0.87 (0.67, 1.13) 0.29 Multiple RF 3,284 1.20 (0.91, 1.59) 0.20 Overall Population 15,603 0.93 (0.83, 1.05) 0.22 0.4 0.6 0.8 1.")
25 73 CHARISMA: Primary Efficacy Results (MI/Stroke/CV Death)* by Category of Inclusion Criteria Population N RR (95% CI) p value Documented AT 12, (0.77, 0.998) Coronary 5, (0.71, 1.05) 0.13 Cerebrovascular 4, (0.69, 1.03) 0.09 PAD 2, (0.67, 1.13) 0.29 Multiple RF 3, (0.91, 1.59) 0.20 Overall Population 15, (0.83, 1.05) Clopidogrel Better Placebo Better RF=Risk Factors, AT=Atherothrombosis. * First occurrence of MI, stroke (of any cause), or CV Death. Bhatt DL. Presented at ACC ACC/AHA UA/NSTEMI* Guideline Update: Recommendations for Long-Term Medical Therapy Class I Aspirin 75 to 325 mg/day (level of evidence: A) Clopidogrel 75 mg daily (in the absence of contraindications) when ASA is not tolerated because of hypersensitivity or gastrointestinal intolerance (level of evidence: A) The combination of ASA and clopidogrel for 9 months after UA/NSTEMI (level of evidence: B) Beta-blockers in the absence of contraindications (level of evidence: B) Lipid-lowering agents and diet in post-acs and post-revascularization patients with LDL cholesterol >130 mg/dl (level of evidence: A) Lipid-lowering agents if LDL cholesterol level after diet is >100 mg/dl (level of evidence: C) ACE inhibitors for patients with CHF, LV dysfunction (EF <0.40), hypertension, or diabetes (level of evidence: A) * Also known as non Q-wave MI. Braunwald E, et al. Available at: Accessed February 18,

26



27

* 7 6 5 4 3 2 Improved Hospital Adherence 6.0% 5.2% 5.0% 4.")
28 82 CRUSADE Discharge Medication Use Last 12 Months (In patients without contraindications) Utilization of Therapies (%) 100% 80% 60% 40% 20% 93% 89% 64% 86% 69% 0% ASA Beta Blockers ACE- Inhibitors* Any Lipid- Lowering Agent Clopidogrel * LVEF <40%, CHF, DM, HTN. Known hyperlipidemia, TC, LDL. CRUSADE data October 1, 2003-September 30, 2004 (n=40,386) Adapted with permission from CRUSADE Web site. Available at: Accessed March 11, CRUSADE Relationship Between Guidelines Adherence and In-Hospital Mortality In-Hospital Mortality (%)* Improved Hospital Adherence 6.0% 5.2% 5.0% 4.2% % 25 50% 50 75% 75% Hospital Composite Adherence Quartiles * Adjusted figure. Cumulative CRUSADE data (adjusted) through September Adapted with permission from CRUSADE Web site. Available at: Accessed February 10,
 60-85 mg/dl HDL cholesterol")

29 Clinical Outcomes Utilizing Revascularization and Aggressive Guideline-Driven Drug Evaluation - Presented at the ACC meeting, March, 2008, New Orleans, LA - Published NEJM 2007; COURAGE: Risk Factor Goals Variable Goal Smoking Cessation Total Dietary Fat / Saturated Fat <30% calories / <7% calories Dietary Cholesterol <200 mg/day LDL cholesterol (primary goal) mg/dl HDL cholesterol (secondary goal) >40 mg/dl Triglyceride (secondary goal) <150 mg/dl Physical Activity min. moderate intensity 5X/week Body Weight by Body Mass index Initial BMI Weight Loss Goal BMI <25 > % relative weight loss Blood Pressure <130/85 mmhg Diabetes HbAlc <7.0% - Presented at the ACC meeting, March, 2008, New Orleans, LA Published NEJM 2007; COURAGE: Overall Survival 1.0 PCI + OMT OMT Hazard ratio: % CI ( ) P = Years Number at Risk Medical Therapy PCI Presented at the ACC meeting, March, 2008, New Orleans, LA Published NEJM 2007;



 25% 25% 42% 36% - Presented at the ACC meeting,")
30 COURAGE: Long-Term Improvement in Treatment Targets (Group Median ± SE Data) Treatment Targets Baseline 60 Months PCI +OMT OMT PCI +OMT OMT SBP 131 ± ± ± ± 0.92 DBP 74 ± ± ± ± 0.65 Total Cholesterol mg/dl 172 ± ± ± ± 1.64 LDL mg/dl 100 ± ± ± ± 1.21 HDL mg/dl 39 ± ± ± ± 0.75 TG mg/dl 143 ± ± ± ± 4.70 BMI Kg/M² 28.7 ± ± ± ± 0.31 Moderate Activity (5x/week) 25% 25% 42% 36% - Presented at the ACC meeting, March, 2008, New Orleans, LA Published NEJM 2007;

31


32

 that he/she will get from smoking cessation? A.")
33 Keep it Simple; Don t Overthink it 97 Summary CAD remains the number one cause of morbidity and mortality among adults in the USA. There are approximately million episodes of ACS annually. For essentially half a century, we have had data regarding CAD risk factors. We also some very reasonable data demonstrating that interventions do work. Primary and secondary prevention of CAD events can be accomplished but is challenging and may require an astute/aggressive doctor and a motivated patient Keep it simple.remember the basics 98 For a cigarette-smoking patient who has an MI, what is the approximate risk reduction of future MI (over the next several years) that he/she will get from smoking cessation? A. There is no significant change in risk of second MI from smoking cessation at time of first MI B. Only about 10% C. About 25% D. About 50% E. Between % 99 33
34 Based on the most recent (2013) lipid guidelines, which of the following patients do NOT automatically qualify for statin therapy: A. Healthy 37 y.o. woman with LDL 227, no other medical probs B. 54 y.o. man with recent MI and PCI of LAD; his LDL is 65 C. 44 y.o. man with Diabetes and LDL 90; asymptomatic D. Options A and C E. All of the above qualify 100 Which of the following types of patients should receive dual-antiplatelet therapy for 9-12 months following ACS? (ASA/clopid.) A. Patient with ACS treated with Percutaneous Coronary Intervention(PCI)? B. Patient with ACS treated Coronary Artery Bypass Graft (CABG)? C. Patient with ACS treated medically (no PCI or CABG)? D. What about a High-risk patient who has NOT had ACS (ie, DM)? E. A, B, and C F. All of the above
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
COURAGE to Leave Diseased Arteries Alone
 COURAGE to Leave Diseased Arteries Alone Spencer King MD MACC, FSCAI St. Joseph s s Heart and Vascular Institute Professor of Medicine Emeritus Emory Univ. Atlanta, USA Conflict: I am an Interventionalist
COURAGE to Leave Diseased Arteries Alone Spencer King MD MACC, FSCAI St. Joseph s s Heart and Vascular Institute Professor of Medicine Emeritus Emory Univ. Atlanta, USA Conflict: I am an Interventionalist
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
2/17/2010. Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco
 Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
In-Ho Chae. Seoul National University College of Medicine
 The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
How Long Patietns Will Be on Dual Antiplatelet Therapy?
 How Long Patietns Will Be on Dual Antiplatelet Therapy? Ron Waksman,, MD, FACC Professor of Medicine (Cardiology) Georgetown University Associate Director, Division of Cardiology, Washington Hospital Center
How Long Patietns Will Be on Dual Antiplatelet Therapy? Ron Waksman,, MD, FACC Professor of Medicine (Cardiology) Georgetown University Associate Director, Division of Cardiology, Washington Hospital Center
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
ZEUS Trial ezetimibe Ultrasound Study
 Trial The lower, The better Is it True for Plaque Regression? Statin alone versus Combination of Ezetimibe and Statin Juntendo University, Department of Cardiology, Tokyo, Japan Katsumi Miyauchi, Naohisa
Trial The lower, The better Is it True for Plaque Regression? Statin alone versus Combination of Ezetimibe and Statin Juntendo University, Department of Cardiology, Tokyo, Japan Katsumi Miyauchi, Naohisa
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease
 Interventional Cardiology and Cath Labs The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease Manesh R. Patel MD Chief,
Interventional Cardiology and Cath Labs The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease Manesh R. Patel MD Chief,
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options
 Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
STATINS FOR PAD Long - term prognosis
 STATINS FOR PAD Long - term prognosis Prof. Pavel Poredos, MD, PhD Department of Vascular Disease University Medical Centre Ljubljana Slovenia DECLARATION OF CONFLICT OF INTEREST No conflict of interest
STATINS FOR PAD Long - term prognosis Prof. Pavel Poredos, MD, PhD Department of Vascular Disease University Medical Centre Ljubljana Slovenia DECLARATION OF CONFLICT OF INTEREST No conflict of interest
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
James M. Kirshenbaum, MD, FACC
 James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Oral Antiplatelet Therapy in PCI/ACS. Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine
 Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Long-Term Management Of the ACS Patient: State-of-the-Art. Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA
 Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St. Petersburg, Florida
 The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Current Treatment Of Ischemic Heart Disease In the United States: An Overview. By Dr Gary Mo
 Current Treatment Of Ischemic Heart Disease In the United States: An Overview By Dr Gary Mo 1 Ischemic Heart Disease in the US 1. Cardiovascular disease remains the most common cause of death and is responsible
Current Treatment Of Ischemic Heart Disease In the United States: An Overview By Dr Gary Mo 1 Ischemic Heart Disease in the US 1. Cardiovascular disease remains the most common cause of death and is responsible
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Changing lipid-lowering guidelines: whom to treat and how low to go
 European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Optimal medical therapy in patients with stable CAD
 Optimal medical therapy in patients with stable CAD Robert Storey Professor of Cardiology, University of Sheffield and Academic Director and Honorary Consultant Cardiologist, Cardiology and Cardiothoracic
Optimal medical therapy in patients with stable CAD Robert Storey Professor of Cardiology, University of Sheffield and Academic Director and Honorary Consultant Cardiologist, Cardiology and Cardiothoracic
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Clopidogrel and ASA after CABG for NSTEMI
 Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
Treating Lipids for Prevention of CAD in Women: Matching Therapy to Risk
 TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Dr G R Letchuman. Clogged by Cholesterol
 Dr G R Letchuman Clogged by Cholesterol Main message Cholesterol management is all about reducing risk of CV events vs the side effects, hassle and cost of drugs News that it is no longer important to
Dr G R Letchuman Clogged by Cholesterol Main message Cholesterol management is all about reducing risk of CV events vs the side effects, hassle and cost of drugs News that it is no longer important to
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study
 Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
Is there enough evidence for DAPT after endovascular intervention for PAOD?
 Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
Anti-platelet therapies and dual inhibition in practice
 Anti-platelet therapies and dual inhibition in practice Therapeutics; Sept. 25 th 2007 Craig Williams, Pharm.D. Associate Professor of Pharmacy Objectives 1. Understand the pharmacology of thienopyridine
Anti-platelet therapies and dual inhibition in practice Therapeutics; Sept. 25 th 2007 Craig Williams, Pharm.D. Associate Professor of Pharmacy Objectives 1. Understand the pharmacology of thienopyridine
Clopidogrel has been evaluated in clinical trials that included cardiovascular patients
 REVIEW ARTICLE Comparative Benefits of Clopidogrel and Aspirin in High-Risk Patient Populations Lessons From the CAPRIE and CURE Studies Jack Hirsh, CM, MD, FRCPC, FRACP, FRSC, DSc; Deepak L. Bhatt, MD,
REVIEW ARTICLE Comparative Benefits of Clopidogrel and Aspirin in High-Risk Patient Populations Lessons From the CAPRIE and CURE Studies Jack Hirsh, CM, MD, FRCPC, FRACP, FRSC, DSc; Deepak L. Bhatt, MD,
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Traitements associés chez l hypertendu: Statines, Aspirine
 Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Antiplatelet agents treatment
 Session III Comprehensive management of diabetic patients Antiplatelet agents treatment Chonnam National University Hospital Department of Internal Medicine Dong-Hyeok Cho CONTENTS Introduction Prothrombotic
Session III Comprehensive management of diabetic patients Antiplatelet agents treatment Chonnam National University Hospital Department of Internal Medicine Dong-Hyeok Cho CONTENTS Introduction Prothrombotic
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
Best Lipid Treatments
 Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Lessons learned From The National PCI Registry
 Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Supplement materials:
 Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
LAMIS (Livalo in AMI Study)
") JCR 2018. 12. 8 LAMIS (Livalo in AMI Study) Young Joon Hong Division of Cardiology, Chonnam National University Hospital Gwangju, Korea Trend of hypercholesterolemia in Korea < Prevalence of hypercholesterolemia
JCR 2018. 12. 8 LAMIS (Livalo in AMI Study) Young Joon Hong Division of Cardiology, Chonnam National University Hospital Gwangju, Korea Trend of hypercholesterolemia in Korea < Prevalence of hypercholesterolemia
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes?
 Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
FEATURES OF THIS TALK
 FEATURES OF THIS TALK OUTPATIENT MANAGEMENT OF CAD- A PRIMARY CARE PERSPECTIVE Michael G. Shlipak, MD, MPH Professor of Medicine, Biostatistics, and Epidemiology Chief, General Internal Medicine Covers
FEATURES OF THIS TALK OUTPATIENT MANAGEMENT OF CAD- A PRIMARY CARE PERSPECTIVE Michael G. Shlipak, MD, MPH Professor of Medicine, Biostatistics, and Epidemiology Chief, General Internal Medicine Covers
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss