Preoperative Evaluation. Elizabeth A. Valentine, MD Department of Anesthesia and Critical Care July 5, 2018
|
|
|
- Violet Glenn
- 5 years ago
- Views:
Transcription
1 Preoperative Evaluation Elizabeth A. Valentine, MD Department of Anesthesia and Critical Care July 5, 2018
2 Goals Review important contact information for the Department of Anesthesiology and Critical Care Provide a framework for understanding preoperative medical evaluation (and why it is important) Review major societal recommendations regarding preoperative evaluation and testing 2012 ASA Advisory for Preoperative Evaluation 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
3 HOW DO I CONTACT THE DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE IF I HAVE QUESTIONS ABOUT A CASE?
4 Important Anesthesia Contact Information Anesthesia Scheduler: Sandy Boyer Directors of Preoperative Medicine: Marc Royo, MD MBA Onyi Onuoha, MD MPH Anesthesia Consults: Sandy and Directors of Preoperative Medicine Call Preoperative Medicine Resident (7a-5p): On call resident (evening): Anesthesia Coordinator:
5 What is risk assessment/stratification? What is medical optimization? What is clearance? WHAT IS PREOPERATIVE EVALUATION (AND WHY IS IT IMPORTANT)?
6 Risk Assessment/Stratification The decision to undergo surgery requires a complex weighing risks, benefits, and nonsurgical alternatives for treatment Many factors play into this decision: Surgical risk Medical risk Urgency of the procedure Many vested stakeholders in the decision: Surgical team Medical team Patient and family
7 Risk Assessment/Stratification Risk assessment/stratification attempts to estimate a particular patient s risk, based on surgical and medical factors, to predict likelihood of adverse events There is no such thing clearance of risk There is no safe surgery even a healthy patient undergoing a minor procedure incurs risk!


8 How Can We Estimate Risk?

9 Risk Assessment/Stratification Our goal is to make surgery safer to minimize the modifiable risk Lifestyle changes Diagnostic tests Optimization of medical therapies Procedural interventions Riggs KR, Segal JB. What is the rationale for preoperative medical evaluations? A closer look at surgical risk and common terminology. BJA (6):
10 What is Optimization? Clear outline of what is wrong, and how bad Determination of whether the patient/condition is the best s/he is going to get If not optimized: what is the plan to intervene/improve? If optimized: what is the plan to try to mitigate risk or manage predictable complications?

11 This is a Bad Preop Clearance Note

12 A Little Better

13 If you really want to see an anesthesiologist s head explode Surgeon
14 WHAT SHOULD PREOPERATIVE EVALUATION ENTAIL?
15 Preoperative Evaluation Evaluation of pertinent medical records Patient interview Physical Examination Additional laboratory studies, preoperative testing, and preoperative consultation as dictated by the above Thoughtful decision making about perioperative medication management

16
17 Preoperative Testing Ideally: Cheap High positive and negative predictive values Add to information obtained from clinical history and physical exam Change or modify perioperative decision making to prevent perioperative complications
18 Preoperative Testing Should be ordered for specific indication only Results should clarify questions about preexisting medical condition or establish a relevant new diagnosis in patients with significant risk factors for specific conditions The more tests ordered, the more chance of a false-positive result Wasted time Wasted money Risk for complications
19 Preoperative Testing In the medical population, 50% of clinical diagnoses and nearly 50% of management decisions based on history alone Routine studies contribute to less than 1% of all diagnoses In the surgical world, routine preop screening rarely discovers abnormalities not predicted by history alone, and when detected, results are rarely actionable Sandler G. Costs of unnecessary tests. Br Med J 1979; 2:21-4. Delahunt B, Turnbull PRG. How cost effective are routine preoperative investigations. N Z Med J 1980; 92: Kaplan EB, Sheiner LB, Boeckmann AJ, Roizen MF, Beal SL, Cohen SN, et al. The usefulness of preoperative laboratory screening. JAMA 1985; 253: Narr BJ, Warner ME, Schroeder DR, Warner MA. Outcomes of patients with no laboratory testing before anesthesia and a surgical procedure. Mayo Clin Proc 1997; 72:505-9.
20 Timing of Preoperative Testing Test results should be within 6 months of surgery, provided the patient s medical history has not changed substantially in the interim More recent test results may be desirable when the medical history has changed or when a test results may play a role in the selection of a specific anesthetic technique (e.g., regional anesthesia in the setting of anticoagulation therapy). The American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice Advisory for Preanesthesia Evaluation. Anesthesiology 2012; 116:2-17.
21 Complete Blood Count Clinically asymptomatic anemia has been shown to be present in about 1% of patients but surgically significant anemia in unselected patients is even more rare Should be considered if: Highly invasive procedure/high risk of blood loss Extremes of age History of liver disease History of anemia History of bleeding diatheses Kaplan EB, Sheiner LB, Boeckmann AJ, Roizen MF. Beal SL. Cohen SN, et al. The usefulness of preoperative laboratory screening. JAMA 1985; 253: The American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice Advisory for Preanesthesia Evaluation. Anesthesiology 2012; 116:2-17.
22 Coagulation Studies An unexpected coagulation defect leading to excessive surgical bleeding is extremely unlikely, provided a thorough history (both personal and family) and physical exam is performed Reasonable for patients with: Bleeding diatheses (inherited or iatrogenic) Renal dysfunction Liver dysfunction Undergoing highly invasive procedures Chee YL, Crawford JC, Watson HG, Greaves M. Guidelines on the assessment of bleeding risk prior to surgery or invasive procedures. British J Haematol 2008; 140: The American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice Advisory for Preanesthesia Evaluation. Anesthesiology 2012; 116:2-17.

23 Regional/Neuraxial Anesthesia and Antithrombotic/Antiplatelet Therapy


24 Regional/Neuraxial Anesthesia and Antithrombotic/Antiplatelet Therapy
25 Serum Chemistries Significant electrolyte abnormalities noted on routine screening are extremely rare Increased glucose in patients having noncardiac, nonvascular surgery are associated with increased perioperative cardiovascular mortality compared to normoglycemic patients Consider if: Known endocrine abnormalities Renal dysfunction Liver dysfunction Use of certain medicine/therapies (diuretics, dialysis..) The American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice Advisory for Preanesthesia Evaluation. Anesthesiology 2012; 116:2-17. Wattsman TA, Davies RS. The utility of preoperative laboratory testing in general surgery patients for outpatient procedures. Am Surg 1997; 63: Nordic PG, Vergsma E. Schreiner F, Keratin MD, Fringe HH, Dunkelgrun J, et al. Increased preoperative glucose levels are associated with perioperative mortality in patients undergoing noncardiac, nonvascular surgery. Eur J Endocrinol 2007; 156: Frisch A, Chandra P, Smiley D, Pen L, Rizzo M, Gatcliffe C, et al. Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac
26 Chest Radiograph Abnormalities on chest radiograph are incredibly common but rarely change perioperative outcome or management Exception is to evaluate possible acute processes (pneumonia, decompensated CHF) Joo HS, Wong J, Naik VB, Savodelli GL. The value of screening preoperative chest x-rays: a systematic review. Can J Anesthes 2005; 52:
27 ASA says consider for: Smoking Chest Radiograph Recent upper respiratory infection COPD Cardiac disease ACP suggests CXR may be helpful in patients >50yo who are undergoing AAA repair, upper abdominal, or thoracic surgery AHA adds BMI > 40 kg/m 2 The American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice Advisory for Preanesthesia Evaluation. Anesthesiology 2012; 116:2-17. Smetana GW, Lawrence VA, Cornell JE, American College of Physicians. Preoperative pulmonary risk stratification for noncardiothoracic surgery: a systematic review for the American College of Physicians. Ann Intern Med 2006; 144:581. Poirer P, Alpert MA, Fleisher LA, Thompson PD, Sugerman HJ, Burke LE, et al. Cardiovascular evaluation and management of severely obese patients undergoing surgery: a science advisory from the American Heart Association. Circulation 2009; 120:86-95.
28 Pulmonary Function Testing Range from noninvasive passive or provocative screening tests (e.g., PFTs or spirometry) to invasive assessment of pulmonary function (e.g., ABG, split lung function, right heart catheterization) Incidence of pulmonary complications is higher in patients with preexisting lung disease Preoperative PFTs have not proven to be better predictors than clinical findings in predicting significant postoperative pulmonary complications after surgical procedures not involving lung resection Kroenke K, Lawrence VA, Theroux JF, Tuley MR, Hilsenbeck SG. Postoperative complications after thoracic and major abdominal surgery I patients with and without obstructive lung disease. Chest 1993; 104: Smetana GW, Lawrence VA, Cornell JE. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144: Ivanov A, Yossef J, tailon J, et al. Do pulmonary function tests improve risk stratification before cardiothoracic surgery? J Thor Cardiovasc Surg 2016; 151(4):
29 Risk Factors for Postoperative Pulmonary Complications Patient factors: Advanced age ASA PS 2 or higher Functional dependence COPD Smoking CHF OSA PHTN Surgical Factors: Surgery close to the diaphragm (thoracic and upper abdominal) Emergency surgery Prolonged duration Neurosurgery Head and neck surgery Vascular surgery General anesthesia Smetana GW, Lawrence VA, Cornell JE. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144: Hwang D, Shakir N, Limann B, Sison C, Kalra S, Shulman L, et al. Association of sleep-disordered breathing with postoperative complications. Chest 2008; 133: Ramakrishna G, Sprung J, Ravi BS, Chandrasekaran K, McGoon MD. Impact of pulmonary hypertension on the outcomes of noncardiac surgery: predictors of perioperative morbidity and mortality. J Am Coll Cardiol 2005; 45:
30 UPHS PreOp Testing Guidelines No Testing Duration of acceptability of tests Basic Metabolic Panel CBC CXR EKG Finger Stick (Glucose) Pregnancy PT/PTT/INR T & S UPHS Recommendation NO testing in ASA 1 or 2 regardless of age having a low risk procedure. SIX MONTHS before surgery if the patient s medical history has not changed. In patients having major surgery, taking diuretics, digoxin, potassium supplements, with a history of CKD, or if IV contrast dye will be injected Having major surgery, anemia history, or cirrhosis Not Required In patients with known Diabetes, CAD, CVD, arrhythmias, structural heart disease, or peripheral arterial disease having elevated risk surgery. No age or BMI inclusion. All Diabetics the day of surgery Urine HCG for all females with potential of pregnancy Any patient on anticoagulants, with a bleeding history, or cirrhosis If indicated
31 WHAT ABOUT PREOPERATIVE CARDIAC EVALUATION AND TESTING?
32 Preoperative Cardiac Testing Range from noninvasive (e.g., electrocardiogram or echocardiogram) to invasive (e.g., cardiac catheterization) assessment of cardiac structure, function, and vascularity May be passive or provocative (e.g., stress testing) Clinical characteristics to consider include: cardiovascular risk factors type and invasiveness of surgery The American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice Advisory for Preanesthesia Evaluation. Anesthesiology 2012; 116:2-17.

33

34 Preop ECG

35 Preop Echo: Assessment of LV function
36 Valvular heart disease Preoperative echo is recommended for patients with clinically suspected moderate or greater degree of valvular regurgitation or stenosis if: (1) no prior echo w/in 1y; or (2) significant change in clinical status since last exam. (Class I, LOE C) Valve replacement or repair before noncardiac surgery for patients who meet standard criteria for valve replacement/repair is effective in reducing perioperative risk (Class I, LOE C) Elevated-risk noncardiac surgery w/appropriate monitoring is reasonable in patients with: (1) asymptomatic severe AS; (2) asymptomatic severe MR; (3) asymptomatic severe AI with normal LVEF (Class IIa/b, LOE B/C)
37 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery
38 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery Risk Factors: Age Sex HTN CVD CKD IDDM Obesity.
39 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery Emergency procedure = life or limb is threatened if not in the operating room with no or very limited time for preoperative clinical evaluation, typically within <6 hours. Urgent procedure = life or limb is threatened but there may be time for a limited clinical evaluation, typically between 6 and 24 hours. Time-sensitive procedure = a delay of >1 to 6 weeks to allow for an evaluation and significant changes in management will negatively affect outcome. Elective procedure = the procedure could be delayed for up to 1 year.
40 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery Acute Coronary Syndrome Equivalents: Unstable (active or crescendo angina) coronary syndromes or recent MI Decompensated HF (NYHA Class IV, new onset, worsening) Suspected new or significant worsening of valvular heart disease Unstable arrhythmias (Symptomatic or new ventricular arrhythmias, supraventricular arrhythmias with uncontrolled ventricular rate, High grade AV block, symptomatic bradycardia
41 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery Nishimura RA, Otto CM, Bonow RO, et al AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014; 63:e Yancy CW, Jessup M, Bozkurt B, et al ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e O Gara PT, Kushner FG, Ascheim DD, et al ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:e Fihn SD, Gardin JM, Abrams J, et al ACCF/ AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2012;60:e Fihn SD, Blankenship SC, Alexander KP, et al ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64: Jneid H, Anderson JL, Wright RS, et al ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non- ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60:
42 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery American College of Surgeons NSQIP risk calculator
43 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery Low risk = can proceed to surgery without any further testing

44 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery If elevated risk, it s all about symptomatology and functional capacity

45 Functional capacity > 4 METS
46 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery Elevated risk but moderate/good to excellent functional status = can go to surgery
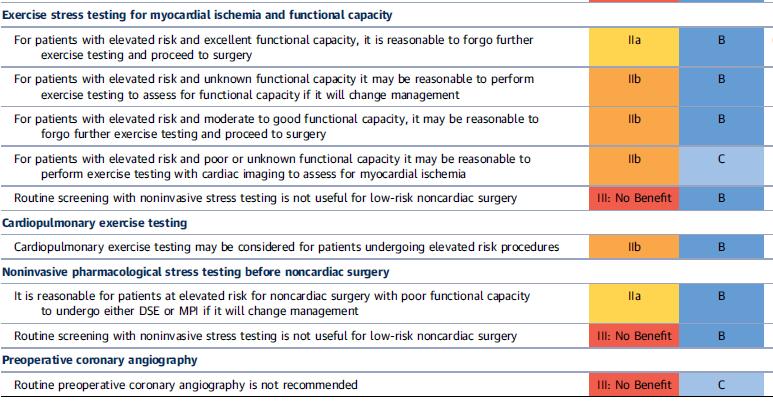
47 2014 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery Elevated risk and poor to unknown functional status = pharmacologic stress IF IT WILL IMPACT CARE
48 Provocative/invasive cardiac testing

49 Should we revascularize everyone preoperatively?
50 Should we revascularize everyone preoperatively? Based largely on the CARP trial, ACC/AHA guidelines do not recommend revascularization for the general population Follow the recommendations found in routine clinical practice guidelines for revascularization (CABG/PCI) There are subsets of populations who benefit from preop revascularization probably worth having cardiology and anesthesia weigh in on perioperative management

51 What if the patient already had a recent cardiac revascularization?
52 Treatment Algorithm for the Timing of Elective Noncardiac Surgery in Patients With Coronary Stents Patients Treated With PCI Undergoing Elective Noncardiac Surgery BMS treated with DAPT DES treated with DAPT 0 d 30 d <30 d since BMS implantation 30 d since BMS implantation Class III: Harm Delay surgery Class I: Proceed with surgery <3 mo since DES implantation 3 mo 6 mo Class III: Harm Delay surgery 3-6 mo since DES implantation, discontinue DAPT; delayed surgery risk is great than stent thrombosis risk Class IIb: Proceeding with surgery may be considered 6 mo since DES implantation, discontinue DAPT Class I: Proceed with surgery

53 Perioperative Management: Timing of Elective Noncardiac Surgery in Patients Treated With PCI and DAPT Levine GN, et al ACC/AHA Guideline Focused Update on Duration of DAPT in Patients with CAD. JACC 2016 & Circulation 2016
54 Conclusions A good history and physical exam will get you far Most extensive workups are unnecessary unless a change in clinical status Determining functional status answers a lot of questions Early multidisciplinary involvement in complex patients can help ensure appropriate optimization We are happy to help answer any questions!
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Preoperative Evaluation Guidelines and Work up
 Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Cardiac Evaluation. Preoperative Cardiac Evaluation Prior to Noncardiac Surgery
 Prior to Noncardiac Surgery Carmine D Amico, D.O. Overview Learning objectives Introduction Procedure risk categorization Preoperative estimation of cardiac risk Stepwise approach to preoperative evaluation
Prior to Noncardiac Surgery Carmine D Amico, D.O. Overview Learning objectives Introduction Procedure risk categorization Preoperative estimation of cardiac risk Stepwise approach to preoperative evaluation
I have no disclosures
 Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT
 PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT Susan H. Noorily, M.D. Clinical Professor of Anesthesiology Medical Director University Preoperative Medicine Center IMPORTANCE Half of all currently
PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT Susan H. Noorily, M.D. Clinical Professor of Anesthesiology Medical Director University Preoperative Medicine Center IMPORTANCE Half of all currently
Perioperative Medicine 2016 Some Answers, Even More Questions
 Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
Guidelines PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42. Prominent Dutch Cardiovascular Researcher Fired for Scientific Misconduct
 PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL
 COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
Pre-operative Evaluations. Objectives. General Considerations. FP Consultation Considerations. CV Credits 7/24/2017. Brian Bachelder, MD Akron, Ohio
 Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
Conflicts of Interest. Evaluation of Cardiac and Pulmonary Risk in the Preop Patient. Introduction. Risk Assessment. Risk Assessment: RCRI
 Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
SESSION 5 2:20 3:35 pm
 SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
PERIOPERATIVE CARDIAC RISK ASSESSMENT. Divya Gollapudi, MD
 PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia preope
 Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
2010, Metzler Helfried
 Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC. DO's and DON'Ts: Reducing unnecessary perioperative investigations
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DO's and DON'Ts: Reducing unnecessary perioperative investigations Emmanuelle Duceppe, MD FRCPC General Internal Medicine University
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DO's and DON'Ts: Reducing unnecessary perioperative investigations Emmanuelle Duceppe, MD FRCPC General Internal Medicine University
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Perioperative Management. Perioperative Management of Cardiovascular Medications
 of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY
 PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
Objectives. Old School. Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction?
 Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
Update in Perioperative Medicine
 Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Preoperative Evaluation of Patients Undergoing Noncardiac Surgery
 Preoperative Evaluation of Patients Undergoing Noncardiac Surgery Shazia Khan, MD Assistant Professor of Clinical Medicine Keck School of Medicine LAC+USC Medical Center Learning Objectives Use a risk
Preoperative Evaluation of Patients Undergoing Noncardiac Surgery Shazia Khan, MD Assistant Professor of Clinical Medicine Keck School of Medicine LAC+USC Medical Center Learning Objectives Use a risk
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Anesthesia for Cardiac Patients for Non Cardiac Surgery. Kimberly Westra DNP, MSN, CRNA
 Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
PAT? WHAT S THAT JEREMY CHAPMAN DO KPN HOSPITALIST
 PAT? WHAT S THAT JEREMY CHAPMAN DO KPN HOSPITALIST My Background 3 years ICU Nursing 1 year Med-Surg Nursing Medical School: Ohio University Heritage College of Osteopathic Medicine Residency: Adena Regional
PAT? WHAT S THAT JEREMY CHAPMAN DO KPN HOSPITALIST My Background 3 years ICU Nursing 1 year Med-Surg Nursing Medical School: Ohio University Heritage College of Osteopathic Medicine Residency: Adena Regional
Preoperative Management. Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
 Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Terry Clifford, MSN, RN, CPAN, CAPA Nurse Manager Perioperative Services Portland, Maine, USA
 Terry Clifford, MSN, RN, CPAN, CAPA Nurse Manager Perioperative Services Portland, Maine, USA Identify and optimize conditions that increase periop morbidity and mortality OR Detect abnormalities that
Terry Clifford, MSN, RN, CPAN, CAPA Nurse Manager Perioperative Services Portland, Maine, USA Identify and optimize conditions that increase periop morbidity and mortality OR Detect abnormalities that
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Clinical Appropriateness Guidelines: Diagnostic Coronary Angiography
 Clinical Appropriateness Guidelines: Diagnostic Coronary Angiography Appropriate Use Criteria Effective Date: January 2, 2018 Proprietary Date of Origin: 08/27/2015 Last revised: 02/23/2017 Last reviewed:
Clinical Appropriateness Guidelines: Diagnostic Coronary Angiography Appropriate Use Criteria Effective Date: January 2, 2018 Proprietary Date of Origin: 08/27/2015 Last revised: 02/23/2017 Last reviewed:
AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIA PRE OPERATIVE SCREENING ASA PHYSICAL STATUS CLASSIFICATION ANESTHESIOLOGISTS
 ANESTHESIA PRE OPERATIVE SCREENING CAPA S 37 TH ANNUAL CONFERENCE PALM SPRINGS OCTOBER 5, 2013 ROBERT F. KOPEL, MD, FACP, FCCP HOAG HOSPITAL ASSISTANT CLINICAL PROFESSOR UCLA SCHOOL OF MEDICINE AMERICAN
ANESTHESIA PRE OPERATIVE SCREENING CAPA S 37 TH ANNUAL CONFERENCE PALM SPRINGS OCTOBER 5, 2013 ROBERT F. KOPEL, MD, FACP, FCCP HOAG HOSPITAL ASSISTANT CLINICAL PROFESSOR UCLA SCHOOL OF MEDICINE AMERICAN
Perioperative Medicine 2017 November 3, Disclosures
 Perioperative Medicine 2017 November 3, 2017 Scott Marsal, MD MSc FACP Chief, Medicine Division Medical Director, Quality & Patient Safety Providence St. Vincent Medical Center Disclosures No conflicts
Perioperative Medicine 2017 November 3, 2017 Scott Marsal, MD MSc FACP Chief, Medicine Division Medical Director, Quality & Patient Safety Providence St. Vincent Medical Center Disclosures No conflicts
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
The goal of preoperative evaluation. Preoperative Testing Before Noncardiac Surgery: Guidelines and Recommendations
 Before Noncardiac Surgery: s and Recommendations MOLLY A. FEELY, MD; C. SCOTT COLLINS, MD; PAUL R. DANIELS, MD; ESAYAS B. KEBEDE, MD; AMINAH JATOI, MD; and KAREN F. MAUCK, MD, MSc, Mayo Clinic, Rochester,
Before Noncardiac Surgery: s and Recommendations MOLLY A. FEELY, MD; C. SCOTT COLLINS, MD; PAUL R. DANIELS, MD; ESAYAS B. KEBEDE, MD; AMINAH JATOI, MD; and KAREN F. MAUCK, MD, MSc, Mayo Clinic, Rochester,
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality
 Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
PREOP EVALUATION AND OPTIMIZATION
 PREOP EVALUATION AND OPTIMIZATION Barry Perlman, PhD, MD System Lead, Anesthesia Physician Best Practice 4/2012 Disclosure of Potential Financial Conflicts of Interest None But am open to any and all offers
PREOP EVALUATION AND OPTIMIZATION Barry Perlman, PhD, MD System Lead, Anesthesia Physician Best Practice 4/2012 Disclosure of Potential Financial Conflicts of Interest None But am open to any and all offers
03/07/ Background. + High Risk Features Are Prevalent in Dialysis Patients
 + When Does Cardiovascular Disease Preclude Consideration of Renal Transplantation? Kul Aggarwal, MD, MRCP (UK), FACC Professor of Clinical Medicine Division of Cardiology University of Missouri & Chief,
+ When Does Cardiovascular Disease Preclude Consideration of Renal Transplantation? Kul Aggarwal, MD, MRCP (UK), FACC Professor of Clinical Medicine Division of Cardiology University of Missouri & Chief,
Perioperative Cardiac Management. Emma Sargsyan, MD, FACP
 Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Heart 101. Objectives. Types of Heart Failure How common is HF? Sign/Symptoms, when to see a doctor? Diagnostic testing
 EXAMING HEART FAILURE: HOW TO RECOGNIZE AND TREAT THE WEAK HEART What is Heart Failure? Treatment of Heart Failure End Stage Heart Failure Munir S. Janmohamed M.D. FACC Assistant Clinical Professor of
EXAMING HEART FAILURE: HOW TO RECOGNIZE AND TREAT THE WEAK HEART What is Heart Failure? Treatment of Heart Failure End Stage Heart Failure Munir S. Janmohamed M.D. FACC Assistant Clinical Professor of
A preoperative evaluation allows us to: learn about the patient. risk stratify them based on their comorbities
 A preoperative evaluation allows us to: learn about the patient risk stratify them based on their comorbities assists in anesthesia preop, intraop and postoperative planning COMPONENTS OF A PREOP Thorough
A preoperative evaluation allows us to: learn about the patient risk stratify them based on their comorbities assists in anesthesia preop, intraop and postoperative planning COMPONENTS OF A PREOP Thorough
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Implementation of a PSH Model in a Preoperative Clinic
 Implementation of a PSH Model in a Preoperative Clinic Les Garson, MD Department of Anesthesiology & Perioperative Care June 27, 2015 Key points for a PSH Pre Op Clinic Culture Change Management Triage
Implementation of a PSH Model in a Preoperative Clinic Les Garson, MD Department of Anesthesiology & Perioperative Care June 27, 2015 Key points for a PSH Pre Op Clinic Culture Change Management Triage
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver
 Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Managing Cardiac & Pulmonary Risk in the Surgical Patient
 Managing Cardiac & Pulmonary Risk in the Surgical Patient Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Preoperative Evaluation Guidelines Cardiac: Fleisher
Managing Cardiac & Pulmonary Risk in the Surgical Patient Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Preoperative Evaluation Guidelines Cardiac: Fleisher
Benefits and Harms of Routine Preoperative Testing: A Comparative Effectiveness Review
 Benefits and Harms of Routine Preoperative Testing: A Comparative Effectiveness Review Brown Evidence- based Practice Center, Brown University School of Public Health Ethan M. Balk, MD, MPH Amy Earley,
Benefits and Harms of Routine Preoperative Testing: A Comparative Effectiveness Review Brown Evidence- based Practice Center, Brown University School of Public Health Ethan M. Balk, MD, MPH Amy Earley,
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Assessment and Diagnosis of Heart Failure
 Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Pre-Operative Services Teaching Rounds 3 Jan 2011
 Pre-Operative Services Teaching Rounds 3 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 3 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013
 Pre-op Assessment by Primary Providers What we really want to know John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013 Outline Discuss anesthesia specific risk Discuss
Pre-op Assessment by Primary Providers What we really want to know John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013 Outline Discuss anesthesia specific risk Discuss
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Patient referral for elective coronary angiography: challenging the current strategy
 Patient referral for elective coronary angiography: challenging the current strategy M. Santos, A. Ferreira, A. P. Sousa, J. Brito, R. Calé, L. Raposo, P. Gonçalves, R. Teles, M. Almeida, M. Mendes Cardiology
Patient referral for elective coronary angiography: challenging the current strategy M. Santos, A. Ferreira, A. P. Sousa, J. Brito, R. Calé, L. Raposo, P. Gonçalves, R. Teles, M. Almeida, M. Mendes Cardiology
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
PRE Operative Care of the High Risk Surgical Patient. Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London
 PRE Operative Care of the High Risk Surgical Patient Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London Perioperative Optimization Shoemaker oxygen delivery goal directed therapy ITS NOT
PRE Operative Care of the High Risk Surgical Patient Dr A T Dewhurst Consultant Anaesthetist St George s Hospital London Perioperative Optimization Shoemaker oxygen delivery goal directed therapy ITS NOT
Cardiac Perioperative Risk Assessment American Heart Association Guidelines
 Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW
 PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Managing Hypertension in the Perioperative Arena
 Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
OP Chest Pain General Data Element List. All Records All Records. All Records All Records All Records. All Records. All Records.
 Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures Chest Pain (CP) Set Measure ID # OP-4 * OP-5 * Measure Short Name Aspirin at Arrival
Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures Chest Pain (CP) Set Measure ID # OP-4 * OP-5 * Measure Short Name Aspirin at Arrival
Cardiac Risk Assessment in the Preoperative period
 Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Does Low Intensity Exercise Improve Physical Performance among Cardiac Survivors? Dr Saari Mohamad Yatim Rehabilitation Physician
 Does Low Intensity Exercise Improve Physical Performance among Cardiac Survivors? Dr Saari Mohamad Yatim Rehabilitation Physician Intro.. Physical inactivity remains a global problem, particularly in clinical
Does Low Intensity Exercise Improve Physical Performance among Cardiac Survivors? Dr Saari Mohamad Yatim Rehabilitation Physician Intro.. Physical inactivity remains a global problem, particularly in clinical
Preoperative Risk. Geoffrey C Zarrella DO FACC. Assessment
 Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Agenda. Disclosures. Surgical Mortality: What is High Risk?
 Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Agenda. Perioperative Cardiac Risk Stratification circa Surgical Mortality: What is High Risk? Presenter Disclosure Information
 9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Pre-op Risk Assessment. Hal Blanks MD FACC
 Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Preoperative Management of Patients Receiving Antithrombotics
 Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
2018 HPN Provider Summary Guide. Adult Cardiology Patients (18 Years and Older) Referral Guidelines
 Referral Guidelines") 12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
Clear for Surgery. What are the components of a good preoperative evaluation? What are not? Preoperative Risk Assessment: an evidence based approach
 Preoperative Risk Assessment: an evidence based approach Daniel M. Swangard, M.D. UCSF Department of Anesthesia & Perioperative Care AIM - May/June 2007 What are the components of a good preoperative evaluation?
Preoperative Risk Assessment: an evidence based approach Daniel M. Swangard, M.D. UCSF Department of Anesthesia & Perioperative Care AIM - May/June 2007 What are the components of a good preoperative evaluation?
AAA CAG CAG. ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac. Group Group AAA AAA.
 13 591 596 2004 AAA CAG CAG 5527 15 CAG ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery CAG 55 34 62CAG 75 CAG 73 63 66 ACC / AHA CAGGroup 1 9 8 Group 225 22 Group
13 591 596 2004 AAA CAG CAG 5527 15 CAG ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery CAG 55 34 62CAG 75 CAG 73 63 66 ACC / AHA CAGGroup 1 9 8 Group 225 22 Group
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
When do you delay surgery?
 Cancer BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University of Chicago I have no disclosures 2 nd leading
Cancer BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University of Chicago I have no disclosures 2 nd leading
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Activated partial thromboplastin time abnormality, perioperative approach to, 104 105 Acute kidney injury, perioperative, 89 99 early
Index Note: Page numbers of article titles are in boldface type. A Activated partial thromboplastin time abnormality, perioperative approach to, 104 105 Acute kidney injury, perioperative, 89 99 early
2018 David Stultz. The Consultant s Job
 The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH
 Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
TAVR : Caring for your patients before and after TAVR
 TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
Perioperative Myocardial Infarction
 Perioperative Myocardial Infarction Which patient should UNDERGO CORONARY ANGIOGRAPHY? The Cardiologists view Hans Rickli, St.Gallen 1 Experience Standards Risk stratification Team approach.. Tightrope
Perioperative Myocardial Infarction Which patient should UNDERGO CORONARY ANGIOGRAPHY? The Cardiologists view Hans Rickli, St.Gallen 1 Experience Standards Risk stratification Team approach.. Tightrope
Preoperative Cardiac Evaluation of Patients With Acute Hip Fracture
 An Original Study Preoperative Cardiac Evaluation of Patients With Acute Hip Fracture Jonathan Cluett, MD, Jill Caplan, MD, and Warren Yu, MD Abstract The goals of the present study were to assess if there
An Original Study Preoperative Cardiac Evaluation of Patients With Acute Hip Fracture Jonathan Cluett, MD, Jill Caplan, MD, and Warren Yu, MD Abstract The goals of the present study were to assess if there
TAB 7: SUB TAB: AMI/CHEST PAIN Specifications & Paper Tools
 TAB 7: SUB TAB: AMI/CHEST PAIN Specifications & Paper Tools Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures Acute Myocardial Infarction
TAB 7: SUB TAB: AMI/CHEST PAIN Specifications & Paper Tools Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures Acute Myocardial Infarction
University of Wisconsin - Madison Cardiovascular Medicine Fellowship Program UW CICU Rotation Goals and Objectives
 Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced