HOW TO PERFORM LEFT VENTRICULAR ASSISTANCE IN THE CATHLAB. Andreas Baumbach, MD FESC FRCP Bristol Heart Institute University Hospitals Bristol UK
|
|
|
- Thomas Henderson
- 5 years ago
- Views:
Transcription
1 HOW TO PERFORM LEFT VENTRICULAR ASSISTANCE IN THE CATHLAB Andreas Baumbach, MD FESC FRCP Bristol Heart Institute University Hospitals Bristol UK
2 Disclosure I have no conflicts of interest regarding this presentation
3 Objectives Identification of available technology Establish evidence based indications Practical review of Technology Placement Management Complications Of Intraaortic counterpulsation
4 How to use LV assistance in the Cathlab CARDIOGENIC SHOCK
5 Monday morning 75 yr old man with anterior STEMI admitted to local DGH Chest pain started 4pm, presented 9:30 Hx of Oesophagus -Ca Transfer for primary PCI 10:15

6 On Arrival BP: 60/40 7 * VF arrest and DC shock

7 EBU 4 BMW wire



8

9 Cardiogenic Shock
10 Determinants of Ventricular Function CONTRACTILITY PRELOAD AFTERLOAD STROKE VOLUME - Synergistic LV contraction - LV wall integrity - Valvular competence HEART RATE CARDIAC OUTPUT
11 Management of Acute Ischemic Cardiogenic Shock Inotropic Support Circulatory Support Revascularisation!
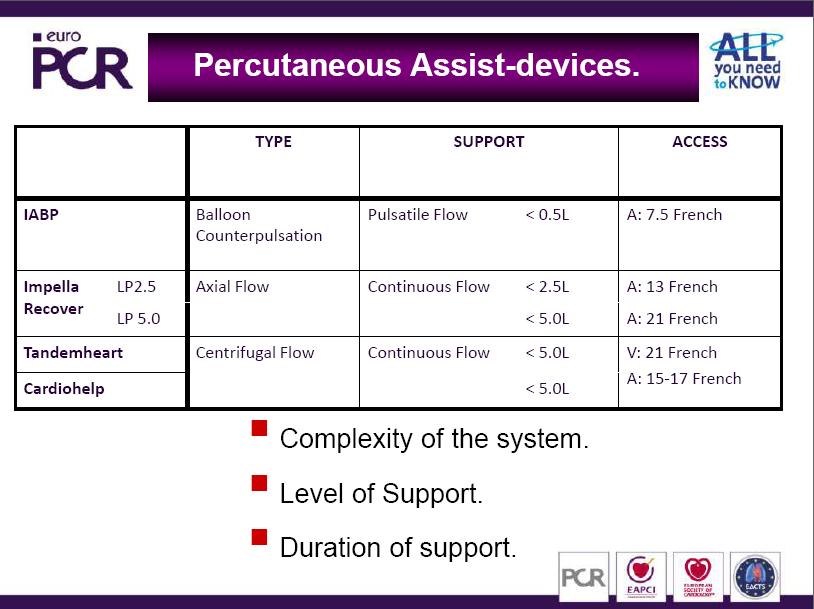
12 Circulatory Support: Options Intraaortic Balloon Counterpulsation Left Ventricular Assist Devices Percutanoeous Implantable Total artificial heart Extracorporeal Circulation

13 Intra-Aortic Balloon Pump Inflatable cc balloon Triggered to inflate with helium immediately after aortic valve closure Triggered to deflate with opening of the aortic valve
14 IABP: INDICATIONS
15 Ideal Candidate for IABP Prerequesite for effect of IABP = contractile reserve Without sufficient contractile reserve correction of preload and afterload cannot result in increased stroke volume and cardiac output!
16 IABP Indications Hemodynamic compromise Cardiogenic shock secondary to AMI with continuing ischemia, VSD, or MR Cardiogenic shock due to transient ischemia, myocarditis, sepsis, drug toxicity, etc. Inability to wean from bypass after cardiac surgery Hemodynamic support while awaiting transplantation adapted from Burkhoff D. Grossman s Cardiac Catheterization, Angiography and Intervention 2006, p. 415
17 IABP Indications Medically refractory ischemia Medically refractory unstable angina Failed PTCA with refractory ischemia Severe arrhythmia owing refractory ischemia adapted from Burkhoff D. Grossman s Cardiac Catheterization, Angiography and Intervention 2006, p. 415
18 IABP Contraindications Significant aortic regurgitation Abdominal aortic aneurysm Aortic dissection Uncontrolled septicemia Uncontrolled bleeding diathesis Severe bilateral peripheral vascular disease uncorrectable by peripheral angioplasty or cross-femoral surgery Bilateral femoral-popliteal bypass grafts for severe peripheral vascular disease adapted from Burkhoff D. Grossman s Cardiac Catheterization, Angiography and Intervention 2006, p. 415
19 LV ASSISTANCE: THE EVIDENCE
20 Assist Devices in STEMI

21 Prophylactic IABP? High-risk PTCA owing to LV dysfunction and/or large territory at risk PTCA during acute myocardial infarction Stabilization in patients with severe aortic stenosis Severe multivessel or left main CAD requiring urgend cardiac or noncardiac surgery Large myocardial infarction adapted from Burkhoff D. Grossman s Cardiac Catheterization, Angiography and Intervention 2006, p. 415

22 CRISP AMI 337 Patients with anterior STEMI NOT in shock IABP vs. no IABP No difference in Infarct size or Microvascular Obstruction CMR Endpoint
23 GUIDELINES

24 ESC GUIDELINES 2010 Acute STEMI

25 Recommendations for Reperfusion Strategies in ST-Segment Elevation Myocardial Infarction Patients ESC Guidelines on Revascularization 2010 Eur Heart J 2010;31: No benefit of IABP in hemodynamic stable patients Increased risk of bleeding and other complications
26 AVAILABLE TECHNOLOGY Courtesy Dr F Eberli, Zurich, EuroPCR 2011





27 IABP Images: Courtesy Datascope


28 Datascope Console Understand the principles!



29 Fluid Filled Systems Pressurized Flushing System Fluid based pressure transmission External pressure transducer Trigger: R-wave of ECG (Aortic pressure) Timing of balloon inflation and deflation according to previous beats Disadvantages: Manual calibration necessary Limited timing accuracy during arrhythmias Pressure Transducer Fluid Filled Tube Images: Courtesy Datascope


30 Fibre Optic Systems Fibre optic manometer in the tip of IAB catheter High fidelity signal transmission at the speed of light Advantages: Artefact free, consistent pressure waves Automatic in vivo calibration High accuracy of automatic timing (arrhythmias!) Smaller catheter size (7F) Images: Courtesy Datascope
31 INTRAAORTIC BALLOON PUMP: HEMODYNAMICS

32 Determinants of Myocardial Oxygen Supply and Demand Supply Demand Coronary Artery Anatomy Diastolic Pressure Diastolic Time Oxygen Extraction Hemoglobin PaO 2 MVO 2 Heart Rate Afterload Preload Contractility

33 Primary Effect of IAB Therapy Supply Demand MVO 2 Supply - IAB Inflation Demand - IAB Deflation
34 Coronary flow IABP Increases Coronary Flow Aortic pressure IABP IABP

35 Intra-Aortic Balloon Pump
36 Intra-Aortic Balloon Pump Decreases Afterload Increases Mean Aortic Pressure Increases Coronary Flow Velocity Reduces Myocardial Oxygen Demand
37 Contractility IABP does not increase contractility of the myocardium. However, the improvement of preload and afterload increases stroke volume and cardiac output.
38 IABP Effects Mean pressure Cardiac output Cerebral perfusion Renal perfusion SVR -> peripheral perfusion

39 Patient With Acute Mitral Insufficiency and Cardiogenic Shock LV = 100/22 mmhg Ao = 100/65/80 mmhg PCWP = a= 25; v= 65; m= 41 mmhg RV = 65/23 mmhg PAP = 65/24/40 mmhg RA = a= 10; v= 9; m= 7 mmhg C.O. = 4.6 L/min. PCWP
40 Decrease of PCWP by IABP in Acute MR IABP off IABP on
41 Effect of IABP in Acute Mitral Insufficiency 100 without 100 with IABP LV ECG LV ECG 50 PCW 50 PCW SEC 1 SEC Decrease of LV Filling Pressure = Decrease of Preload Decrease of Preload Reserve Decrease of Afterload = Decrease of LV Systolic Pressure Grossman s Cardiac Cath 3d edition
42 INTRAAORTIC BALLOON PUMP: INSERTION
 Patient Height (cm) (feet) Datascope Corp.")

43 IABP Catheter: What Size for Which Patient? Manufacturer Balloon Size (mm) Patient Height (cm) (feet) Datascope Corp. 25 <152 < >183 >6 00 Arrow International >183 >6 00 Datascope MEGA 50 ml: Can be used in patients cm Increases blood volume displacment by 25% Courtesy: Datascope

44 The tip of the catheter should be placed at the take of left subclavian artery, i.e. between left main bronchus and aortic knob i.e. between 2 nd and 3 rd rib What is the Correct Position of the IABP Catheter? Too High Ideal Too Low as high as possible in the aorta, but must not touch the roof of the aortic arch After insertion and suturing check correct position by fluoroscopy!!
45

46 Non Femoral Access Brachial artery Axilliary/subclavian access Only very small numbers of patients reported
47 INTRAAORTIC BALLOON PUMP: MANAGEMENT
48 IABP: Early Diastolic Inflation Late Diastolic Deflation 120 Increased early diastolic pressure Increased Coronary Flow mm Hg Decreased late diastolic pressure Increased Systolic Function

49
50 Reasons for Suboptimal Diastolic Augmentation Intra-aortic balloon remains partly in the sheath is only partly unfolded/inflated is positioned too low in the aorta catheter shaft has a kink is leaking low helium concentration arrhythmias

 timing superior to")
51 IABP with Fibre Optic System Datascope CS 300 Timing algorithm of new pumps are excellent. Timing of each individual beat possible. ARROW AutoCAT 2 Wave Automatic (machine) timing superior to manual timing by operator. Images: Courtesy Datascope and ARROW
52 Sheath or Sheathless? 1211 pts, retrospective study 305 sheathless/906 sheath Risk factors for limb ischemia: DM and PAD Pts with DM+PAD+sheath: RR 35! -> Sheathless insertion preferred in pts with DM and PAD Erdogan et al, J Card Surg 2006; 21:342

53 Anticoagulation
54 INTRAAORTIC BALLOON PUMP: COMPLICATIONS
55 Complications Event Hematologic Thrombocytopenia Hemolysis Bleeding Thrombo-embolic events Vascular Limb ischemia Aorto-iliac dissection or perforation Mesenteric ischemia Renal failure Infection Management Thrombocytopenia Secondary to platelet destruction Resolves after removal Thrombo-embolic events Prevention by heparin Bleeding Stop heparin up to 24 hours Limb ischemia Check pulses! Bypass of femoral artery Removal of IABP
56 WEANING
57 Weaning Stepwise reduction of counter pulsation Evaluation of spontaneous circulation Removal of balloon 1:1 1:2 1:4
58 IABP PROPHYLACTIC USE OF IABP
59 Case 2 97year old man Previously fit and well (!) NSTEMI with a moderate Troponin rise Moderately impaired LV function No CV risk factors. Apart from smoking No Family history
60 Initial Treatment ASS/ Clopidogrel/Fondaparinux Beta Blocker, ACE I.V. nitrates But recurrent severe chest pain with widespread ECG changes Referral for invasive assessment

61 Angiogram

62 And the left side


63
64 Strategy Femoral 8F Heparin 5000U i.v. bolus IABP Insertion: Provisional? Prophylactic?

65 BCIS-1 Study
66 LVEF 30% BCIS-1 Jeopardy Score 8 Elective IABP Insertion Randomize PCI No Planned IABP Remove IABP 4-24 hrs. after PCI Hospital Follow-up To discharge or 28 days 6 month follow-up ONS / GROS Am Heart J 2009;158:
 HR 1.")
 HR 0.61 (0.24-1.")
67 Adverse Events (%) BCIS-1: Major Outcomes HR 0.94 ( ) HR 1.86 ( ) HR 0.11 ( ) HR 0.61 ( ) JAMA 2010; 304(8):
 30-day mortality 1.")
68 BCIS-1 Secondary Outcome: 6 month Mortality Routine elective balloon pump insertion before PCI cannot be recommended in patients with severe LV dysfunction and extensive coronary disease 6-month mortality 6.0% (n=300) 30-day mortality 1.3% (n=301)
69 BCIS-1 Follow-up: Results Duration of follow-up (from randomisation): Median 51 months (IQR months) 100 DEATHS (33%)
70 All-cause Mortality by treatment assignment 50% IABP No IABP 40% 30% 20% 10% Hazard ratio 0.66 (95% CI 0.44 to 0.98) 0% IABP No IABP 0 6 m 1 year 2 years 3 years 4 years 5 years Time since randomisation
71 Time-varying Hazard Ratios 4,5 4 3,5 3 2,5 2 1,5 1 0,5 0 6 months 0.63 (0.24 to 1.62) < 1 year 0.68 (0.34 to 1.35) > 1 year 0.65 (0.40 to 1.06) p=0.91 for interaction (<1yr vs. >1yr) overall 0.66 (0.40 to 0.98) 0, IABP Better No planned IABP Better

72
73
74
75
76

77

78

79


80
81 Clinical Course Troponin falling Pain free ECG normalised Patient mobilised on day 1 Patient demands to go home on day 3 Well after 10 days..
82 Outlook
83 Summary IABP is an essential tool for LV support in acute ischaemic cardiogenic shock Knowledge of hemodynamic principles and underlying technology is essential for successful use of IABP The role of LV assist for prevention of complications in high risk interventions has yet to be determined
84 Thank you for your attention
85 Vranx EUROPCR2011

86

87

88
89 Provisional IABP Elective versus provisional intra-aortic balloon pumping in high-risk percutaneous transluminal coronary angioplasty. Briguori C, Sarais C, Pagnotta P, Airoldi F, Liistro F, Sgura, Spanos V, Carlino M, Montorfano M, Di Mario C, Colombo A. Am Heart J 2003;
90 Provisional IABP for PCI N: 133 patients EF<30% Group A: Preprocedural IABP Group B: Conventional PCI Severe hypotension & shock n:11 in group B Brigouri et al Am Heart J 2003
91 IABP Evidence A prospective randomized evaluation of prophylactic intraaortic balloon counterpulsation in high risk patients with acute MI treated with primary angioplasty Stone et al. J Am Coll Cardiol 1997
92 IABP in primary angioplasty Hypothesis: routine use of IABP after primary PCI reduces infarct related artery reocclusion Multicentre, randomised trial High risk patients randomised to 36 to 48hrs IABP or standard care Stone et al. J Am Coll Cardiol 199
93 IABP in primary angioplasty N:1100 Angio for MI N: 908 randomised N: 437 high risk IABP 211 no IABP 226 Established 86% Crossover 13% Stone et al. J Am Coll Cardiol 199
94 IABP in primary angioplasty IABP no IABP Death Re-MI Reoccl Stroke CHF Endpoint Hypo Stone et al. J Am Coll Cardiol 1997
95 Stone et al. J Am Coll Cardiol 1997 IABP in primary angioplasty Complications No difference in hemorrhagic complications or vascular complications Significant difference in stroke This finding may be due to chance.. One intracranial hemorrhage developed after a postinfarction patient was hit in the head with a shovel while robbing the hospital nursery
96 Benchmark Registry June 96-August Hospitals (90%US) patient case records Verified by external audit Ferguson et al. J Am Coll Cardiol 2001; 38:1456
97 Benchmark Registry: Indication Hemodynamic support during/after catheterisation 20.6% Cardiogenic shock 18.8% Weaning from CP bypass 16.1% Preoperative use in high risk pts 13% Refractory unstable angina 12.3% Ferguson et al. J Am Coll Cardiol 2001; 38:1456
98 Benchmark Registry: Complications Major: Limb ischemia, severe bleeding, balloon leak, death due to IABP 2.6% In hospital mortality 21.2% Failed IABP insertion 2.3% Increased risk for major complications: Women Low BSA Older patients PVD Ferguson et al. J Am Coll Cardiol 2001; 38:1456



99 Correct Timing of Balloon Inflation/Deflation Goal = Maximal diastolic augmentation and decrease in aortic end-diastolic pressure. Inflation: Immediately after aortic valve closure. Early Inflation Deflation: Finished just prior to aortic valve opening. Late Deflation Most serious mitakes: Early inflation/late deflation Balloon interferes with LV ejection Increase in LV afterload and MVO 2 Images: Courtesy Datascope
100 IABP Evidence: SHOCK Impact of thrombolysis, intra-aortic balloon pump counterpulsation, and their combination in cardiogenic shock complicating acute myocardial infarction A report from the SHOCK trial registry Sanborn et al. J Am Coll Cardiol 2000;
101 IABP Evidence: SHOCK Background: National registry of MI suggests lower mortality in pts treated with thrombolysis followed by IABP (49%) compared with thrombolysis alone (69%) GUSTO trend towards better outcome Sanborn et al. J Am Coll Cardiol 2000; 36:112
102 SHOCK Registry N: 856 patients with cardiogenic shock in acute MI 36 participating centres Treatment: No thrombolysis / no IABP 33% IABP only 33% Thrombolysis only 15% Thrombolysis and IABP 19% Sanborn et al. J Am Coll Cardiol 2000; 36:112
103 SHOCK Registry: Mortality Cardiogenic shock (LV Failure) No thrombolysis n=564 64% Thrombolysis n=292 54% p=.005 No IABP n=285 77% IABP n=279 52% No IABP n=132 63% IABP n=160 47% p<.0001 no revasc n=233 83% revasc n=52 48% no revasc n=84 76% revasc n=195 41% no revasc n=105 74% revasc n=27 19% no revasc n=51 69% revasc n=109 37% Sanborn et al. J Am Coll Cardiol 2000; 36:112
104 SHOCK Result IABP vs. no IABP mortality after adjustement for revascularisation p=0.313 Use of IABP with or without thrombolysis improves survival in pts with cardiogenic shock because of the higher rate of attempted revascularisation in the IABP group Sanborn et al. J Am Coll Cardiol 2000; 36:1123
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Section 6 Intra Aortic Balloon Pump
 Section 6 Intra Aortic Balloon Pump The Intra Aortic Balloon Pump (IABP) The balloon is synthetic and is made for single use only. It is threaded into the aorta, usually via a femoral approach. The balloon
Section 6 Intra Aortic Balloon Pump The Intra Aortic Balloon Pump (IABP) The balloon is synthetic and is made for single use only. It is threaded into the aorta, usually via a femoral approach. The balloon
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
The Role of Mechanical Circulatory Support in Cardiogenic Shock: When to Utilize
 The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Counterpulsation. John N. Nanas, MD, PhD. Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece
 John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication vs Benefit? Mortality? Morbidity?
 Preoperative intraaortic balloon counterpulsation in high-risk CABG Stefan Klotz, M.D. Preoperative IABP in high-risk CABG Questions?? Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication
Preoperative intraaortic balloon counterpulsation in high-risk CABG Stefan Klotz, M.D. Preoperative IABP in high-risk CABG Questions?? Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication
Principles of intra-aortic balloon pump counterpulsation
 Principles of intra-aortic balloon pump counterpulsation Murli Krishna MBBS FRCA FFPMRCA Kai Zacharowski MD PhD FRCA Key points The primary goal of intraaortic balloon pump (IABP) treatment is to increase
Principles of intra-aortic balloon pump counterpulsation Murli Krishna MBBS FRCA FFPMRCA Kai Zacharowski MD PhD FRCA Key points The primary goal of intraaortic balloon pump (IABP) treatment is to increase
Rhondalyn C. McLean. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume VII, A. Study Purpose and Rationale
 A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
CLINICAL SUPPORT SERVICES DEVELOPING AN IABP PRECEPTOR STRATEGY
 CLINICAL SUPPORT SERVICES DEVELOPING AN IABP PRECEPTOR STRATEGY DATASCOPE IS NOW MAQUET CARDIOVASCULAR Datascope is now MAQUET Cardiovascular In early 2009, the purchase agreement between Datascope and
CLINICAL SUPPORT SERVICES DEVELOPING AN IABP PRECEPTOR STRATEGY DATASCOPE IS NOW MAQUET CARDIOVASCULAR Datascope is now MAQUET Cardiovascular In early 2009, the purchase agreement between Datascope and
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
Guideline compliance, utilization trends
 Guideline compliance, utilization trends and device selection Tilmann Schwab Cardiology / Intensive care Cardiac support IABP LVAD Transluminal l LVAD Cardiac support Emergency cardiac life support (ECLS)
Guideline compliance, utilization trends and device selection Tilmann Schwab Cardiology / Intensive care Cardiac support IABP LVAD Transluminal l LVAD Cardiac support Emergency cardiac life support (ECLS)
CARDIOGENIC SHOCK. Antonio Pesenti. Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI)
") CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention
 Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
IABP SHOCK II trial:
 IABP SHOCK II trial: Randomized comparison of intraaortic balloon counterpulsation versus optimal medical therapy in addition to early revascularization in acute myocardial infarction complicated by cardiogenic
IABP SHOCK II trial: Randomized comparison of intraaortic balloon counterpulsation versus optimal medical therapy in addition to early revascularization in acute myocardial infarction complicated by cardiogenic
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia.
 STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia. PART 1 Systems of care for STEMI. STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis
STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia. PART 1 Systems of care for STEMI. STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση. Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας
 Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
IABP Timing & Fidelity. Pocket Reference Guide
 IABP Timing & Fidelity Pocket Reference Guide Correct IABP Timing A = One complete cardiac cycle R B = Unassisted aortic end diastolic pressure P T C = Unassisted systolic pressure D = Diastolic augmentation
IABP Timing & Fidelity Pocket Reference Guide Correct IABP Timing A = One complete cardiac cycle R B = Unassisted aortic end diastolic pressure P T C = Unassisted systolic pressure D = Diastolic augmentation
Management of Cardiogenic shock. Prof. Christian JM Vrints
 Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
Pre-operative usage of IABP for patients for by pass surgery
 Pre-operative usage of IABP for patients for by pass surgery Mitrev Z, Anguseva T, Hristov N Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 IABP Background Preload Afterload
Pre-operative usage of IABP for patients for by pass surgery Mitrev Z, Anguseva T, Hristov N Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 IABP Background Preload Afterload
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Mechanical Cardiac Support in Acute Heart Failure. Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research
 Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Antonio Colombo. Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy. Miracor Symposium. Speaker: 15. Parigi: May 16-19, 2017
 Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Recovering Hearts. Saving Lives.
 Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
The development of cardiogenic shock portends an extremely poor prognosis. Cardiogenic Shock: A Lethal Complication of Acute Myocardial Infarction
 TREATMENT UPDATE Cardiogenic Shock: A Lethal Complication of Acute Myocardial Infarction David R. Holmes, Jr, MD Mayo Graduate School of Medicine, Mayo Clinic, Rochester, MN Cardiogenic shock is a serious
TREATMENT UPDATE Cardiogenic Shock: A Lethal Complication of Acute Myocardial Infarction David R. Holmes, Jr, MD Mayo Graduate School of Medicine, Mayo Clinic, Rochester, MN Cardiogenic shock is a serious
Ventricular Assisting Devices in the Cathlab. Unrestricted
 Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.)
") A. ADMINISTRATIVE New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.) 1. Facility Code: 2. Facility Name: 3. Procedure Type (Choose only
A. ADMINISTRATIVE New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.) 1. Facility Code: 2. Facility Name: 3. Procedure Type (Choose only
Who is the high risk patient?
 Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Percutaneous mechanical circulatory support for treatment and prevention of hemodynamic instability Engström, A.E.
 UvA-DARE (Digital Academic Repository) Percutaneous mechanical circulatory support for treatment and prevention of hemodynamic instability Engström, A.E. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Percutaneous mechanical circulatory support for treatment and prevention of hemodynamic instability Engström, A.E. Link to publication Citation for published version
Ventricular tachycardia and ischemia. Martin Jan Schalij Department of Cardiology Leiden University Medical Center
 Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
ST-Elevation Myocardial Infarction & Cardiogenic Shock. - What Should We Do?
 ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
Aortic Dissection Causes of Death
 Aortic Dissection Causes of Death Rupture aorta 33.3% Unspecified 33.3% Neurological l deficit it 13.9% Visceral ischemia/kidney failure 11.5% Cardiac tamponade 7.9% (Circulation 2002;105:200-6) Medical
Aortic Dissection Causes of Death Rupture aorta 33.3% Unspecified 33.3% Neurological l deficit it 13.9% Visceral ischemia/kidney failure 11.5% Cardiac tamponade 7.9% (Circulation 2002;105:200-6) Medical
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ
 Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR
 PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
High Risk PCI for Heart Failure
 High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome'
 'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
MODULE 2 THE CLINICAL ENIGMA: RANDOMIZED TRIALS vs CLINICAL PRACTICE. Nico H. J. Pijls, MD, PhD Catharina Hospital Eindhoven The Netherlands
 MODULE 2 THE CLINICAL ENIGMA: RANDOMIZED TRIALS vs CLINICAL PRACTICE Nico H. J. Pijls, MD, PhD Catharina Hospital Eindhoven The Netherlands Disclosure All presenters have a speaker agreement with Maquet
MODULE 2 THE CLINICAL ENIGMA: RANDOMIZED TRIALS vs CLINICAL PRACTICE Nico H. J. Pijls, MD, PhD Catharina Hospital Eindhoven The Netherlands Disclosure All presenters have a speaker agreement with Maquet
The majority of patients with cardiomyopathy
 Selection of Hemodynamic Support: An Approach for Coronary Interventions in Shock and High-Risk PCI The role of hemodynamic support devices in emergent cardiogenic shock and elective high-risk percutaneous
Selection of Hemodynamic Support: An Approach for Coronary Interventions in Shock and High-Risk PCI The role of hemodynamic support devices in emergent cardiogenic shock and elective high-risk percutaneous
Cardiogenic Shock Protocol
 Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA. IMP v4
 1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
A Future for the IABP in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany
 University of Lübeck, Germany") A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
I Was Too Late With Device Placement
 SCAI SHOCK 2018 A Team-Based Course On Cardiogenic Shock General Session # 2 Saturday, October 13, 2018 8:39 8:51 AM Boston Park Plaza - Boston, MA I Was Too Late With Device Placement M Chadi Alraies,
SCAI SHOCK 2018 A Team-Based Course On Cardiogenic Shock General Session # 2 Saturday, October 13, 2018 8:39 8:51 AM Boston Park Plaza - Boston, MA I Was Too Late With Device Placement M Chadi Alraies,
Ted Feldman, M.D., MSCAI FACC FESC
 Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
CVICU EXAM. Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery
 CVICU EXAM 1111 North 3rd Street Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery 1. Nursing standards for a patient on an IABP device include: a. Know results of
CVICU EXAM 1111 North 3rd Street Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery 1. Nursing standards for a patient on an IABP device include: a. Know results of
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
(For items 1-12, each question specifies mark one or mark all that apply.)
") Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Definition. Low-cardiac-output state resulting in life threatening end-organ hypoperfusion. Criteria: MAP 30 mm Hg lower than baseline)
") Definition Low-cardiac-output state resulting in life threatening end-organ hypoperfusion Criteria: 1. Persistent hypotension (SBP
Definition Low-cardiac-output state resulting in life threatening end-organ hypoperfusion Criteria: 1. Persistent hypotension (SBP
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
THE journal OF EXTRA-CORPOREAL TECHNOLOGY ABSTRACT
 Original Article Innovations in Intra-Aortic Balloon Pump Management: Computer Modem Technology John M. Ingram, BS, CCP Cedars Medical Center Miami, Florida Keywords: intra-aortic balloon pump; computer;
Original Article Innovations in Intra-Aortic Balloon Pump Management: Computer Modem Technology John M. Ingram, BS, CCP Cedars Medical Center Miami, Florida Keywords: intra-aortic balloon pump; computer;
Cardiogenic Shock. Dr. JPS Henriques. Academic Medical Center University of Amsterdam The Netherlands
 Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Technique. Technique. Technique. Monitoring 1. Local anesthetic? Aseptic technique Hyper-extend (if radial)
") Critical Care Monitoring Hemodynamic Monitoring Arterial Blood Pressure Cannulate artery Uses 2 Technique Sites Locate artery, prep 3 1 Technique Local anesthetic? Aseptic technique Hyper-extend (if radial)
Critical Care Monitoring Hemodynamic Monitoring Arterial Blood Pressure Cannulate artery Uses 2 Technique Sites Locate artery, prep 3 1 Technique Local anesthetic? Aseptic technique Hyper-extend (if radial)
BEDSIDE ASSESSMENT OF PATIENTS WITH STEMI
 BEDSIDE ASSESSMENT OF PATIENTS WITH STEMI Prof. Maria Dorobantu, PhD, FESC, FACC Emergency Hospital of Bucharest, Romania Presenter Disclosures There are no conflicts/ grants/ disclosures for this presentation.
BEDSIDE ASSESSMENT OF PATIENTS WITH STEMI Prof. Maria Dorobantu, PhD, FESC, FACC Emergency Hospital of Bucharest, Romania Presenter Disclosures There are no conflicts/ grants/ disclosures for this presentation.
Epidemiology of Heart Failure in Adults
 Cardiac Critical Care : Focused on IABP & PCPS Epidemiology of Heart Failure in Adults Prevalence Incidence Mortality 2004 Hospital Cost 2007 2004 Age 20+ (New Cases) All Ages Discharges Age 35+ 2004 All
Cardiac Critical Care : Focused on IABP & PCPS Epidemiology of Heart Failure in Adults Prevalence Incidence Mortality 2004 Hospital Cost 2007 2004 Age 20+ (New Cases) All Ages Discharges Age 35+ 2004 All
Diastolic Augmentation with an External Pulsating Device To Treat Cardiogenic Shock
 Diastolic Augmentation with an External Pulsating Device To Treat Cardiogenic Shock Nickolas Trubov, B.Sc., C.C.P. and Steven J. Phillips, M.D. Mercy Hospital, Des Moines, Iowa 50314 ABSTRACT An 80 cc
Diastolic Augmentation with an External Pulsating Device To Treat Cardiogenic Shock Nickolas Trubov, B.Sc., C.C.P. and Steven J. Phillips, M.D. Mercy Hospital, Des Moines, Iowa 50314 ABSTRACT An 80 cc
Intra-operative Echocardiography: When to Go Back on Pump
 Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Out-of-hospital Cardiac Arrest. Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland
 Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Case - Advanced HF and Shock (INTERMACS 1)
") Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Local Coverage Determination (LCD) for Cardiac Catheterization (L29090)
 for Cardiac Catheterization (L29090)") Local Coverage Determination (LCD) for Cardiac Catheterization (L29090) Contractor Information Contractor Name First Coast Service Options, Inc. Contractor Number 09102 Contractor Type MAC - Part B LCD
Local Coverage Determination (LCD) for Cardiac Catheterization (L29090) Contractor Information Contractor Name First Coast Service Options, Inc. Contractor Number 09102 Contractor Type MAC - Part B LCD
CSC Review Course: Intra Aortic Balloon Pump (IABP) Paula M Davis ARNP, MSN, CCRN-CSC
 Paula M Davis ARNP, MSN, CCRN-CSC") CSC Review Course: Intra Aortic Balloon Pump (IABP) Paula M Davis ARNP, MSN, CCRN-CSC What is an IABP? The Intra-Aortic Balloon Counterpulsation system is a volume displacement device. It should be positioned
CSC Review Course: Intra Aortic Balloon Pump (IABP) Paula M Davis ARNP, MSN, CCRN-CSC What is an IABP? The Intra-Aortic Balloon Counterpulsation system is a volume displacement device. It should be positioned
University of Florida Department of Surgery. CardioThoracic Surgery VA Learning Objectives
 University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
Coronary angiography and PCI
 Coronary arteries Coronary angiography and PCI Samo Granda, Franjo Naji Department of Cardiology Clinical department of internal medicine University clinical centre Maribor Coronary arteries Atherosclerosis
Coronary arteries Coronary angiography and PCI Samo Granda, Franjo Naji Department of Cardiology Clinical department of internal medicine University clinical centre Maribor Coronary arteries Atherosclerosis
Coronary Interventions Indications, Treatment Options and Outcomes
 Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure