PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014
|
|
|
- Reynold Stone
- 5 years ago
- Views:
Transcription


1 PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL
2 Conflict of Interest Bayer Healthcare Speakers Bureau AstraZeneca Speakers Bureau Off-label Use I will discuss experimental therapies in this talk, covering Drug Eluting Stents and Drug Eluting Balloons currently in PAD and CLI clinical trials
3 PAD Clinical Manifestations Chronic Peripheral Arterial Disease Claudication, symptoms vary Critical Limb Ischemia Gangrene Acute Limb Ischemia Cold Foot
4 2011 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Peripheral Artery Disease (Updating the 2005 Guideline) A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines J Am Coll Cardiol. 2011;58(19): doi: /j.jacc
5 The American College of Cardiology Foundation and American Heart Association (ACCF/AHA) in collaboration with the Society of Vascular Medicine, Society for Vascular Surgery, and Society of Interventional Radiology The prevalence of PAD remains very high and is likely to increase, especially with an aging, more obese, and more diabetic population. New guidelines are intended to: facilitate the identification of PAD patients earlier use of effective measures of prevention, such as smoking cessation and antiplatelet therapy highlight effective treatment strategies supported by clinical outcome data Short-term risk and cost of PAD are high. extremely common patients outcomes over one to five years are as adverse, or worse, as patients who suffer with STEMI the costs are equal to or higher than treating patients with STEMI.
6 Lower Extremity PAD: Class 1 Recommendations The resting ABI should be used to establish the lower extremity PAD diagnosis in patients with suspected lower extremity PAD, defined as individuals with 1 or more of the following (Level of Evidence: B): exertional leg symptoms non-healing wounds age 65 years and older or 50 years and older with a history of smoking or diabetes. The ABI should be measured in both legs in all new patients with PAD of any severity to confirm the diagnosis of lower extremity PAD and establish a baseline. (Level of Evidence: B)
7 Lower Extremity PAD: Class 1 Recommendations The TBI should be used to establish the lower extremity PAD diagnosis in patients in whom lower extremity PAD is clinically suspected but in whom the ABI test is not reliable due to noncompressible vessels (usually patients with long-standing diabetes or advanced age). (Level of Evidence: B) Leg segmental pressure measurements are useful to establish the lower extremity PAD diagnosis when anatomic localization of lower extremity PAD is required to create a therapeutic plan. (Level of Evidence: B) ABI results should be uniformly reported with non-compressible values defined as greater than 1.40, normal values 1.00 to 1.40, borderline 0.91 to 0.99, and abnormal 0.90 or less (24). (Level of Evidence: B) * * = NEW RECOMMENDATION
8 Recommendations for Smoking Cessation: Class 1 Recommendation Smokers or former smokers should be asked about status of tobacco use at every visit. (Level of Evidence: A)* Patients should be assisted with counseling and developing a plan for quitting that may include pharmacotherapy and/or referral to a smoking cessation program. (Level of Evidence: A)* Individuals with lower extremity PAD who smoke cigarettes or use other forms of tobacco should be advised by each of their clinicians to stop smoking and offered behavioral and pharmacological treatment. (Level of Evidence: C) In the absence of contraindication or other compelling clinical indication, 1 or more of the following pharmacological therapies should be offered: varenicline, bupropion, and nicotine replacement therapy. (Level of Evidence: A)* * = NEW RECOMMENDATION
9 2011 Focused Update Recommendations: Antiplatelet Therapy Class I Antiplatelet therapy is indicated to reduce the risk of MI, stroke, and vascular death in individuals with symptomatic atherosclerotic lower extremity PAD, including those with intermittent claudication or CLI, prior lower extremity revascularization (endovascular or surgical), or prior amputation for lower extremity ischemia. (Level of Evidence: A) Aspirin, typically in daily doses of 75 to 325 mg, is recommended as safe and effective antiplatelet therapy to reduce the risk of MI, stroke, or vascular death in individuals with symptomatic atherosclerotic lower extremity PAD, including those with intermittent claudication or CLI, prior lower extremity revascularization (endovascular or surgical), or prior amputation for lower extremity ischemia. (Level of Evidence: B)
10 2011 Focused Update Recommendations: Antiplatelet Therapy Class 1 Clopidogrel (75 mg per day) is recommended as a safe and effective alternative antiplatelet therapy to aspirin to reduce the risk of MI, ischemic stroke, or vascular death in individuals with symptomatic atherosclerotic lower extremity PAD, including those with intermittent claudication or critical limb ischemia, prior lower extremity revascularization (endovascular or surgical), or prior amputation for lower extremity ischemia. (Level of Evidence: B) Class 2a Antiplatelet therapy can be useful to reduce the risk of MI, stroke, or vascular death in asymptomatic individuals with an ABI less than or equal to (Level of Evidence: C)
11 2011 Focused Update Recommendations: Antiplatelet Therapy Class 2b The usefulness of antiplatelet therapy to reduce the risk of MI, stroke, or vascular death in asymptomatic individuals with borderline abnormal ABI, defined as 0.91 to 0.99, is not well established. (Level of Evidence: A) The combination of aspirin and clopidogrel may be considered to reduce the risk of cardiovascular events in patients with symptomatic atherosclerotic lower extremity PAD, including those with intermittent claudication or CLI, prior lower extremity revascularization (endovascular or surgical), or prior amputation for lower extremity ischemia and who are not at increased risk of bleeding and who are at high perceived cardiovascular risk. (Level of Evidence: B)
12 2011 Focused Update Recommendations: Antiplatelet Therapy Class 3: No benefit In the absence of any other proven indication for warfarin, its addition to antiplatelet therapy to reduce the risk of adverse cardiovascular ischemic events in individuals with atherosclerotic lower extremity PAD is of no benefit and is potentially harmful due to increased risk of major bleeding. (Level of Evidence: B)
13 Medical Management of PAD Statins: Reduce your risk factor of heart attack and stroke. Goals: LDL <100 and lower for prior MI, CVA, DM2, smokers High blood pressure medications: Goal: Non-diabetics <140/90, Diabetics <130/80 mm Hg. Consider ACEI/ARB s first-line Medication to control blood sugar. Medications to prevent blood clots: Aspirin or clopidogrel (Plavix). Symptom-relief medications: Cilostazol (Pletal) Pentoxifylline (Trental, however, it's generally less effective).
14 Rutherford Categories and Fontaine Stages of PAD PAD Classification Clinical Symptom Rutherford Fontaine Asymptomatic Asymptomatic 0 I Intermittent claudication Critical limb ischemia Mild claudication 1 IIa Moderate claudication Severe claudication Ischemic rest pain 2 IIb 3 IIb 4 III Minor tissue loss 5 IV Ulceration or gangrene 6 IV
15 Prognosis for CLI Patients Within 3 months of presentation: death in 9% MI in 1% stroke in 1% amputation in 12% persistent CLI in 18% 1-year mortality: 21.0% 2-year mortality: 31.6%



16 CLI = Multi-level arterial obstrcution

17 Limb Ischemia Straight line flow Intact Plantar Arch LIMB SALVAGE Appropriate Surveillance Do whatever it takes to get a pulse!!!!!
18 Recommendations for Critical Limb Ischemia (CLI) : Endovascular and Open Surgical Treatment for Limb Salvage Class I For individuals with combined inflow and outflow disease with critical limb ischemia, inflow lesions should be addressed first. (Level of Evidence: C) For individuals with combined inflow and outflow disease in whom symptoms of critical limb ischemia or infection persist after inflow revascularization, an outflow revascularization procedure should be performed. (Level of Evidence: B) If it is unclear whether hemodynamically significant inflow disease exists, intra-arterial pressure measurements across lesions should be measured before and after the administration of a vasodilator. (Level of Evidence: C)
19 Recommendations for Critical Limb Ischemia: Endovascular and Open Surgical Treatment for Limb Salvage Class 2a For patients with limb-threatening lower extremity ischemia and an estimated life expectancy of 2 years or less or in patients in whom an autogenous vein conduit is not available, balloon angioplasty is reasonable to perform when possible as the initial procedure to improve distal blood flow. (Level of Evidence: B) For patients with limb-threatening ischemia and an estimated life expectancy of more than 2 years, bypass surgery, when possible and when an autogenous vein conduit is available, is reasonable to perform as the initial treatment to improve distal blood flow. (Level of Evidence: B)


20 Management of Limb Ischemia Surgical Endovascular
21 Outcome of Fem-pop Surgery for CLI Pooled data, 1194 saphenous vein 5 year primary patency 80% in claudicants 66% in critical ischemia Results with PTFE 75% in claudicants 47% in critical ischemia JAMA 1995: 274:71

22 The Dirty Little Secret: Poor Healing
23 InfraInguinal Surgery: Outcomes Wound Infection 10-30% Myocardial Infarction % Early graft failure 0-24% Acute leg ischemia % Op. Mortality 1.3-6% Surgical Revision rate > 20% TASC J Vasc Surg 2000




24 Vascular Access for Endovascular Intervention Antegrade Puncture Popliteal access Pedal Punctures



25 Endovascular Lesion Crossing Devices


26 Endovascular Lesion Modification Devices (Rotational/Orbital Atherectomy 2.1 mm 3.0 mm


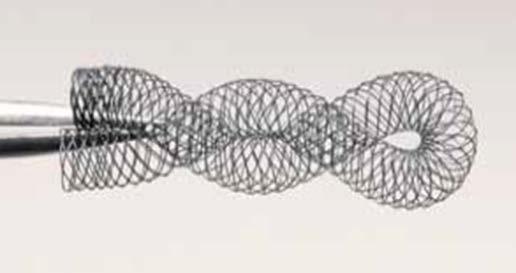


27 Endovascular Devices to Increase Patency (Stents/Cryoplasty)
28 What about Drug-eluting stents in CLI Revascularization? The PaRADISE (PReventing Amputations using Drug eluting StEnts) Trial J Am Coll Cardiol. 2010;55(15): doi: /j.jacc
29 The PARADISE Trial Patient Flow Diagram (A) Clinical outcomes. (B) Angiographic outcomes. RS = binary restenosis TO = total occlusion. J Am Coll Cardiol. 2010;55(15): , doi: /j.jacc
 and 2 overlapping 3.5-mm Cypher drug-eluting stents (DES). (C) The patient returned 17 months later with rest pain.")
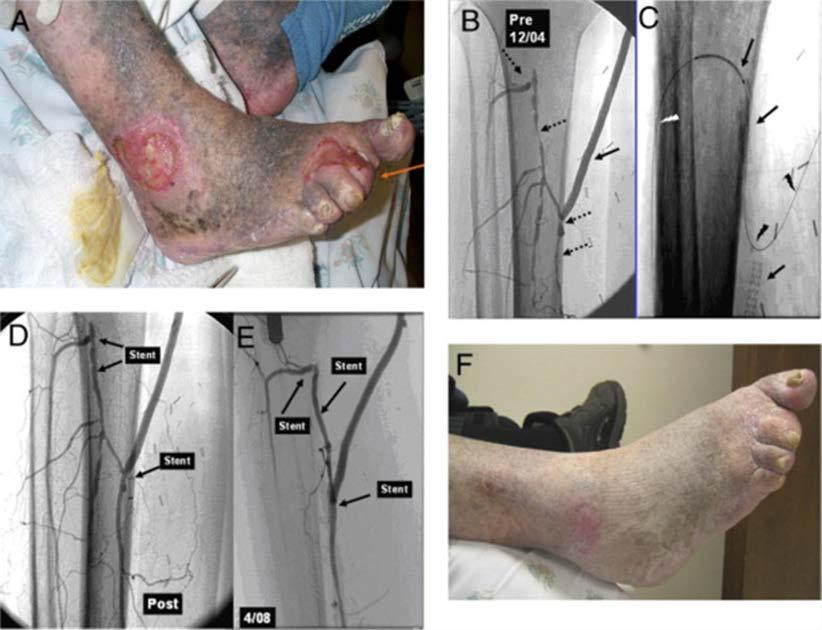
30 Bare-Metal In-Stent Restenosis Successfully Treated With DES (A) An 87-year-old patient, Rutherford 5 CLI. The arrow indicates popliteal artery occlusion. (B) After placing a proximal 4.0 mm bare-metal stent (BMS) and 2 overlapping 3.5-mm Cypher drug-eluting stents (DES). (C) The patient returned 17 months later with rest pain. Note in-stent restenosis of the BMS (dotted brackets) and the patent DES (solid brackets). (D) Incidental angiography 18 months after treating in-stent restenosis with a 3.5-mm 23- mm Cypher stent.
31
32 Rate of Major Amputations in Patients Treated With Below-the-Knee Drug-Eluting Stents (A) 1 cumulative incidence of amputation curve and confidence limits. (B) 1 (cumulative incidence of amputation) stratified according to entry Rutherford category. All-Cause Mortality in Patients Treated With Below-the- Knee Drug-Eluting Stents (A) Kaplan-Meier survival curve with confidence limits. (B) Kaplan-Meier survival curves stratified according to entry Rutherford category.
33 Preventing Leg Amputations in Critical Limb Ischemia With Belowthe-Knee Drug-Eluting Stents: The PaRADISE (PReventing Amputations using Drug eluting StEnts) Trial J Am Coll Cardiol. 2010;55(15): doi: /j.jacc The PaRADISE Trial Amputation-Free Survival Kaplan-Meier amputation-free survival curve (combined death and major amputation).

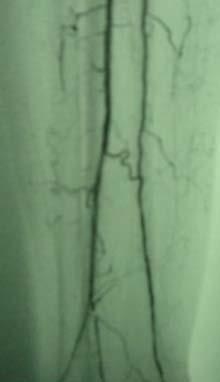
34 68-YEAR-OLD MAN WITH LEFT 5TH TOE GANGRENE: ANTEGRADE PUNCTURE COMMON FEMORAL SUPERFICIAL FEMORAL PROFUNDA FEMORAL

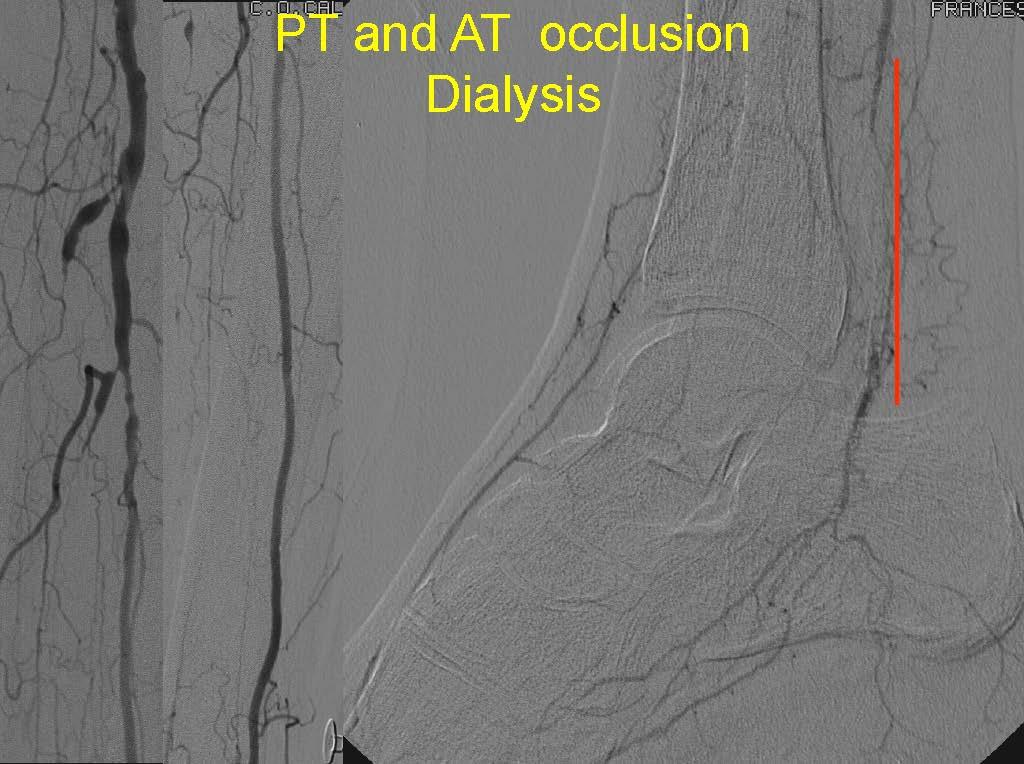
35 68-YEAR-OLD MAN WITH LEFT 5TH TOE GANGRENE: POPLITEAL AND TIBIAL DISEASE POPLITEAL POSTERIOR TIBIAL? ANTERIOR TIBIAL POSTERIOR TIBIAL? ANTERIOR TIBIAL? PERONEAL PERONEAL

36 68-YEAR-OLD MAN WITH LEFT 5TH TOE GANGRENE: FOOT DISEASE PERONEAL POSTERIOR TIBIAL ANTERIOR TIBIAL CLI = 3 vessel disease BTK

37 STEP 1: SUBINTIMAL ANGIOPLASTY LEADING TO EXTENSIVE DISSECTION COVERING POSTERIOR TIBIAL ARTERY OSTIUM PRE PTA POST PTA


38 STEP 2: RETROGRADE POSTERIOR TIBIAL ARTERY ACCESS FOR INTRALUMINAL RE- ENTRY IN THE POPLITEAL POSTERIOR TIBIAL POSTERIOR TIBIAL 19G NEEDLE V WIRE

39 STEP 3: RESIDUAL DISSECTIONS AFTER EXTENSIVE BALLOON-ONLY ANGIOPLASTY WITH 2.5 TO 5.0 MM BALLOONS AT 4 ATM POPLITEAL POSTERIOR TIBIAL POSTERIOR TIBIAL PERONEAL PLANTAR
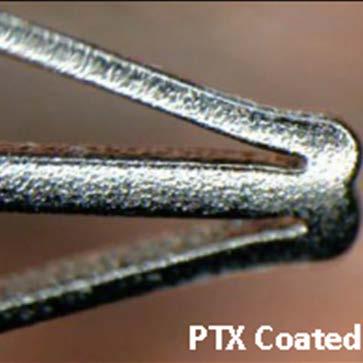
40 Drug Eluting Balloon Technology 2014

41
42
43
44
45
46
47
48
 or angioplasty (n = 111).")
49 Randomized Trial of IN.PACT Admiral DCB vs PTA for Atherosclerotic Lesions in the SFA and/or PPA 331 patients from Europe and the US received a drug-eluting balloon (DEB; n = 220) or angioplasty (n = 111). ITT Analysis at 1 Year DEB (n = 220) Angioplasty (n = 111) P Value Primary Patency 82.2% 52.4% <0.001 Clinically Driven TLR 2.4% 20.6% <0.001 The primary safety composite (freedom from 30-day device- and procedurerelated death and from target limb major amputation and clinically driven TVR through 12 months) was higher in the DEB arm. Conclusion: The IN.PACT Admiral DEB achieves substantially better primary patency at 1 year compared with angioplasty. Tepe G. Charing Cross International Symposium 2014; London, United Kingdom.
50 Exercise and Revascularization vs Exercise Alone ERASE
51 Endovascular Revascularization Benefits PAD Patients When Added to Exercise Therapy 212 PAD patients stable intermittent claudication + vascular obstruction > 50% randomized to supervised exercise therapy with (n = 106) or without (n = 106) endovascular revascularization. Walking distances and quality of life measured. Improvements From Combination Therapy vs. Exercise Therapy Alone at 1 Year Mean Difference 95% CI P Value Maximum Walking Distance, m Pain-free Walking Distance, m < VascuQuol < Conclusion: The combination of endovascular revascularization plus supervised exercise therapy in patients with peripheral artery disease (PAD) and intermittent claudication results in greater improvements in maximum walking distance and quality of life compared with exercise therapy alone. Kruidenier LM, et al. J Vasc Interv Radiol. 2011;22:

52 Additional Supervised Exercise Therapy After a Percutaneous Vascular Intervention for PAD 70 pts randomized to angioplasty with or without exercise therapy. Exercise consisted of 2 to 3 30-minute weekly sessions with a physiotherapist plus encouragement to walk every day. Claudication Distance at 6 Months Angioplasty Alone (n = 27) Angioplasty + Exercise (n = 34) P Value Absolute, m ± ± Functional, m ± ± Conclusion: For PAD patients, supplementing percutaneous intervention with supervised exercise is more effective at improving walking ability than angioplasty alone. Kruidenier LM, et al. J Vasc Interv Radiol. 2011;22:
53 Summary New consensus guidelines for PAD evaluation and treatment recently published 2011 Focus on Smoking Cessation, Counseling and Drug Rx Focus on appropriate Antiplatelet Rx Continue Rx that matters: Statins, BP Rx, DM2 Rx, ACEI s Endo and Surgical Revascularization are both options Many endovascular technologies exist to modify lesions and improve patency Lesion Specific Device Selection Likely Contributes to Better Outcomes Newer endovascular technology may offer better long-term patency outcomes Drug Eluting Balloon reduces restenosis rates significantly at 1 year Supervised Exercise 2-3 days per week improves outcomes with endovascular revascularization more than revascularization alone
54 Thank You Questions?
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC
 Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
The present status of selfexpanding. for CLI: Why and when to use. Sean P Lyden MD Cleveland Clinic Cleveland, Ohio
 The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment
: Presentation, Diagnosis, and Treatment") Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment Prepared and Presented by Jon Manocchio, Pharm D Blanchard Valley Hospital October 2011 Introduction PAD is a condition that is
Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment Prepared and Presented by Jon Manocchio, Pharm D Blanchard Valley Hospital October 2011 Introduction PAD is a condition that is
Critical Limb Ischemia A Collaborative Approach to Patient Care. Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017
 Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Treatment Strategies For Patients with Peripheral Artery Disease
 Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
Limb Salvage in Diabetic Ischemic Foot. Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017
 Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Interventional Treatment First for CLI
 Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria
 Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria") Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Evidence-Based Optimal Treatment for SFA Disease
 Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Disclosures. Tips and Tricks for Tibial Intervention. Tibial intervention overview
 Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Guidelines for Management of Peripheral Arterial Disease
 Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Disclosures. Talking Points. An initial strategy of open bypass is better for some CLI patients, and we can define who they are
 An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome
 Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Hypothesis: When compared to conventional balloon angioplasty, cryoplasty post-dilation decreases the risk of SFA nses in-stent restenosis
 Cryoplasty or Conventional Balloon Post-dilation of Nitinol Stents For Revascularization of Peripheral Arterial Segments Background: Diabetes mellitus is associated with increased risk of in-stent restenosis
Cryoplasty or Conventional Balloon Post-dilation of Nitinol Stents For Revascularization of Peripheral Arterial Segments Background: Diabetes mellitus is associated with increased risk of in-stent restenosis
Peripheral arterial disease for primary care Ed Aboian, MD
 Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the on-label use of
 IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the on-label use of referenced technologies as well as current standards of care
IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the on-label use of referenced technologies as well as current standards of care
Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA. Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE
 PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel
 Case Reports in Vascular Medicine Volume 2015, Article ID 725168, 4 pages http://dx.doi.org/10.1155/2015/725168 Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel Alexander
Case Reports in Vascular Medicine Volume 2015, Article ID 725168, 4 pages http://dx.doi.org/10.1155/2015/725168 Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel Alexander
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
DCB use in fem-pop lesions of patients with CLI (RCC 4-5): subgroup analysis of IN.PACT Global 12-month outcomes
: subgroup analysis of IN.PACT Global 12-month outcomes") DCB use in fem-pop lesions of patients with CLI (RCC 4-5): subgroup analysis of IN.PACT Global 12-month outcomes Carlos Mena, MD FACC FSCAI Associate Professor of Medicine - Cardiology Director Cardiac
DCB use in fem-pop lesions of patients with CLI (RCC 4-5): subgroup analysis of IN.PACT Global 12-month outcomes Carlos Mena, MD FACC FSCAI Associate Professor of Medicine - Cardiology Director Cardiac
Case Discussion. Disclosures. Critical Limb Ischemia: A Selective Approach to Revascularization Works Best 4/28/2012. None. 58 yo M, DM, CAD, HTN
 Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More. Spence M Taylor, M.D.
 Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Olive registry: 3-years outcome of BTK intervention in Japan. Osamu Iida, MD Kansai Rosai Hospital Amagasaki, Hyogo, Japan
 Olive registry: 3-years outcome of BTK intervention in Japan Osamu Iida, MD Kansai Rosai Hospital Amagasaki, Hyogo, Japan What is the optimal treatment for the patient with critical limb ischemia (CLI)?
Olive registry: 3-years outcome of BTK intervention in Japan Osamu Iida, MD Kansai Rosai Hospital Amagasaki, Hyogo, Japan What is the optimal treatment for the patient with critical limb ischemia (CLI)?
Drug-Coated Balloon Treatment for Patients with Intermittent Claudication: Insights from the IN.PACT Global Full Clinical Cohort
 Drug-Coated Balloon Treatment for Patients with Intermittent Claudication: Insights from the IN.PACT Global Full Clinical Cohort a.o. Univ. Prof. Dr. Marianne Brodmann Medical University of Graz Graz,
Drug-Coated Balloon Treatment for Patients with Intermittent Claudication: Insights from the IN.PACT Global Full Clinical Cohort a.o. Univ. Prof. Dr. Marianne Brodmann Medical University of Graz Graz,
Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD
 Seung-Whan Lee, MD, PhD") Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD Asan Medical Center, Heart Institute, University of Ulsan College of Medicine, Werk et al. Circulation Cardiovasc Intervent 2012
Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD Asan Medical Center, Heart Institute, University of Ulsan College of Medicine, Werk et al. Circulation Cardiovasc Intervent 2012
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
The incidence of peripheral artery disease (PAD)
") Pharmacologic Options for Treating Restenosis The role of cilostazol in the treatment of patients with infrainguinal lesions. By Osamu Iida, MD, and Yoshimitsu Soga, MD The incidence of peripheral artery
Pharmacologic Options for Treating Restenosis The role of cilostazol in the treatment of patients with infrainguinal lesions. By Osamu Iida, MD, and Yoshimitsu Soga, MD The incidence of peripheral artery
The essentials for BTK procedures: wires, balloons, what else
 A comprehensive approach to diabetic patient Tx The essentials for BTK procedures: wires, balloons, what else Dai-Do Do Clinical and Interventional Angiology Cardiovascular Department Disclosure Speaker
A comprehensive approach to diabetic patient Tx The essentials for BTK procedures: wires, balloons, what else Dai-Do Do Clinical and Interventional Angiology Cardiovascular Department Disclosure Speaker
DCB in my practice: How the evidence influences my strategy. Yang-Jin Park
 DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
Update from Korea on the Lutonix SFA registry 12 month data
 Update from Korea on the Lutonix SFA registry 12 month data Prospective, Multicenter, Post-Market Registy Assessing the Clinical Use and Safety of the Lutonix Drug Coated Balloon in Femoropopliteal Arteries
Update from Korea on the Lutonix SFA registry 12 month data Prospective, Multicenter, Post-Market Registy Assessing the Clinical Use and Safety of the Lutonix Drug Coated Balloon in Femoropopliteal Arteries
Disclosures. TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Purpose of Practice Guidelines
 TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
LIBERTY 360 Study. 15-Jun-2018 Data 1. Olinic Dm, et al. Int Angiol. 2018;37:
 LIBERTY 360 Study LIBERTY is a prospective, observational, multi-center study to evaluate procedural and long-term clinical and economic outcomes of endovascular device interventions in patients with symptomatic
LIBERTY 360 Study LIBERTY is a prospective, observational, multi-center study to evaluate procedural and long-term clinical and economic outcomes of endovascular device interventions in patients with symptomatic
How Do We Optimize the Medical Therapy of Patients with Critical Limb Ischemia?
 How Do We Optimize the Medical Therapy of Patients with Critical Limb Ischemia? Ehrin J. Armstrong, MD MSc MAS Director, Interventional Cardiology Director, Vascular Laboratory VA Eastern Colorado Healthcare
How Do We Optimize the Medical Therapy of Patients with Critical Limb Ischemia? Ehrin J. Armstrong, MD MSc MAS Director, Interventional Cardiology Director, Vascular Laboratory VA Eastern Colorado Healthcare
Leg arteries : MANAGEMENT and STRATEGY
 Leg arteries : MANAGEMENT and STRATEGY Prof E. Ducasse Unit of vascular surgery BORDEAUX ESVB May 14th 2011 BARD Symposium CLI : definition Fontaine Rutherford ABI Symptoms class category Asymptomatic
Leg arteries : MANAGEMENT and STRATEGY Prof E. Ducasse Unit of vascular surgery BORDEAUX ESVB May 14th 2011 BARD Symposium CLI : definition Fontaine Rutherford ABI Symptoms class category Asymptomatic
Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD
 Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD Faculty Disclosure Thomas Zeller, MD For the 12 months preceding this presentation, I disclose the following types of
Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD Faculty Disclosure Thomas Zeller, MD For the 12 months preceding this presentation, I disclose the following types of
Disclosures. Objectives. Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach. Christopher D. Owens, MD 4/23/2009
 Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA
 Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA Disclosures John R. Laird Within the past 12 months, I or my spouse/partner have had a
Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA Disclosures John R. Laird Within the past 12 months, I or my spouse/partner have had a
Christian Wissgott MD, PhD Assistant Director, Radiology Westküstenkliniken Heide
 2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
Outcomes Of DCB Use In Real World Registries: 2 Year Results From The INPACT Global Registry
 Outcomes Of DCB Use In Real World Registries: 2 Year Results From The INPACT Global Registry Marianne Brodmann, MD Head of the Clinical Division of Angiology Department of Internal Medicine Medical University
Outcomes Of DCB Use In Real World Registries: 2 Year Results From The INPACT Global Registry Marianne Brodmann, MD Head of the Clinical Division of Angiology Department of Internal Medicine Medical University
4/14/2016. Faculty Disclosure. Drug-eluting technology in the SFA and Popliteal. Typical SFA Disease Pattern. Why Peripheral Artery Disease Matters
 Drug-eluting technology in the SFA and Popliteal David Paul Slovut, MD, PhD Associate Professor of Medicine and Surgery Co-director of TAVR program Director of Advanced Intervention Faculty Disclosure
Drug-eluting technology in the SFA and Popliteal David Paul Slovut, MD, PhD Associate Professor of Medicine and Surgery Co-director of TAVR program Director of Advanced Intervention Faculty Disclosure
Medical Therapy for Peripheral Artery Disease
 Medical Therapy for Peripheral Artery Disease Beau M. Hawkins, MD, FSCAI University of Oklahoma Health Sciences Center, Oklahoma City, OK Sahil A. Parikh, MD, FSCAI Columbia University Medical Center,
Medical Therapy for Peripheral Artery Disease Beau M. Hawkins, MD, FSCAI University of Oklahoma Health Sciences Center, Oklahoma City, OK Sahil A. Parikh, MD, FSCAI Columbia University Medical Center,
Current Status of Endovascular Therapies for Critical Limb Ischemia
 Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Garland Green, MD Interventional Cardiologist. Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management
 Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Step by step Hybrid procedures in peripheral obstructive disease. Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery
 Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Specificities for infrapopliteal stents
 Specificities for infrapopliteal stents Nicolas Diehm, M.D. Swiss Cardiovascular Center Clinical and Interventional Angiology University Hospital Bern, Switzerland Disclosures Speaker`s Bureau: MEDRAD,
Specificities for infrapopliteal stents Nicolas Diehm, M.D. Swiss Cardiovascular Center Clinical and Interventional Angiology University Hospital Bern, Switzerland Disclosures Speaker`s Bureau: MEDRAD,
Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis
 Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis Osamu Iida, MD From the Kansai Rosai Hospital Cardiovascular Center, Amagasaki City, Japan. ABSTRACT: Approximately
Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis Osamu Iida, MD From the Kansai Rosai Hospital Cardiovascular Center, Amagasaki City, Japan. ABSTRACT: Approximately
Disclosures. In-Stent Restenosis: The Tail IS Wagging the Dog 4/15/2016. Restenosis: The Continuing Challenge for Peripheral Vascular Intervention
 In-Stent Restenosis: The Tail IS Wagging the Dog Disclosures NONE Michael S. Conte MD Division of Vascular and Endovascular Surgery UCSF Heart and Vascular Center UCSF Vascular Symposium 2016 IF YOU WERE
In-Stent Restenosis: The Tail IS Wagging the Dog Disclosures NONE Michael S. Conte MD Division of Vascular and Endovascular Surgery UCSF Heart and Vascular Center UCSF Vascular Symposium 2016 IF YOU WERE
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia
 Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Recent Advances in Peripheral Salvage
 Recent Advances in Peripheral Salvage Dr Shaiful Azmi Yahaya, MD, MMed, FNHAM, FAsCC, FAPSIC Consultant Cardiologist and Peripheral Interventionist, Institut Jantung Negara Disclosure I am proctoring for
Recent Advances in Peripheral Salvage Dr Shaiful Azmi Yahaya, MD, MMed, FNHAM, FAsCC, FAPSIC Consultant Cardiologist and Peripheral Interventionist, Institut Jantung Negara Disclosure I am proctoring for
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
Distal By-Pass procedures can reduce limb loss
 Conventional treatment of the diabetic foot Distal By-Pass procedures can reduce limb loss Dr. Nikolaos Melas, PhD Vascular and Endovascular Surgeon Military Doctor Associate in 1st department of Surgery,
Conventional treatment of the diabetic foot Distal By-Pass procedures can reduce limb loss Dr. Nikolaos Melas, PhD Vascular and Endovascular Surgeon Military Doctor Associate in 1st department of Surgery,
Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can
 Rafael Malgor, MD Assistant Professor of Surgery The University of Oklahoma, Tulsa Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can Background Lower extremity anatomy (below the
Rafael Malgor, MD Assistant Professor of Surgery The University of Oklahoma, Tulsa Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can Background Lower extremity anatomy (below the
Angiosome concept myth or truth? Does it make a real difference in real world cases?
 Angiosome concept myth or truth? Does it make a real difference in real world cases? Osamu Iida, MD, FACC Kansai Rosai Hospital Amagasaki, Hyogo, Japan Disclosure Speaker name:... I have the following
Angiosome concept myth or truth? Does it make a real difference in real world cases? Osamu Iida, MD, FACC Kansai Rosai Hospital Amagasaki, Hyogo, Japan Disclosure Speaker name:... I have the following
12-month Outcomes of Post Dilatation in the IN.PACT Global CTO Cohort. Gunnar Tepe, MD RodMed Clinic Rosenheim Rosenheim, Germany
 12-month Outcomes of Post Dilatation in the IN.PACT Global CTO Cohort Gunnar Tepe, MD RodMed Clinic Rosenheim Rosenheim, Germany Disclosure Speaker name: Gunnar Tepe I have the following potential conflicts
12-month Outcomes of Post Dilatation in the IN.PACT Global CTO Cohort Gunnar Tepe, MD RodMed Clinic Rosenheim Rosenheim, Germany Disclosure Speaker name: Gunnar Tepe I have the following potential conflicts
Endovascular treatment of infrapopliteal arteries: angioplasty vs stent in the drug-eluting era
 Eur Radiol (2014) 24:793 798 DOI 10.1007/s00330-014-3094-0 VASCULAR-INTERVENTIONAL Endovascular treatment of infrapopliteal arteries: angioplasty vs stent in the drug-eluting era Fabrizio Fanelli & Alessandro
Eur Radiol (2014) 24:793 798 DOI 10.1007/s00330-014-3094-0 VASCULAR-INTERVENTIONAL Endovascular treatment of infrapopliteal arteries: angioplasty vs stent in the drug-eluting era Fabrizio Fanelli & Alessandro
What s New in the Management of Peripheral Arterial Disease
 What s New in the Management of Peripheral Arterial Disease Sibu P. Saha, MD, MBA Professor of Surgery Chairman, Directors Council Gill Heart Institute University of Kentucky Lexington, KY Disclosure My
What s New in the Management of Peripheral Arterial Disease Sibu P. Saha, MD, MBA Professor of Surgery Chairman, Directors Council Gill Heart Institute University of Kentucky Lexington, KY Disclosure My
Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data)
") Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data) (Angiolite BTK DES, IVascular) P. Goverde MD, K. Taeymans MD, K. Lauwers MD Vascular Clinic ZNA Antwerp,Belgium
Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data) (Angiolite BTK DES, IVascular) P. Goverde MD, K. Taeymans MD, K. Lauwers MD Vascular Clinic ZNA Antwerp,Belgium
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures
 Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
John E. Campbell, MD. Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Copyright HMP Communications
 Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Peripheral Arterial Disease: A Practical Approach
 Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler Jones, MD September 14, 2016
 PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
Larry Diaz, MD, FSCAI Mehdi H. Shishehbor, DO, FSCAI
 PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
LIMB SALVAGE IN THE DIABETIC PATIENT
 LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts
 Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts Dr Steven Kum MBBS MMed FRCS FAMS Vascular & Endovascular Surgeon Vascular Centre Department of Surgery Changi
Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts Dr Steven Kum MBBS MMed FRCS FAMS Vascular & Endovascular Surgeon Vascular Centre Department of Surgery Changi
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step -
 Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
One Year after In.Pact Deep: Lessons learned from a failed trial. Prof. Dr. Thomas Zeller
 One Year after In.Pact Deep: Lessons learned from a failed trial Prof. Dr. Thomas Zeller Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: x Consulting:
One Year after In.Pact Deep: Lessons learned from a failed trial Prof. Dr. Thomas Zeller Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: x Consulting:
Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, Japan
 Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, Japan Disclosure Hiroshi Ando, MD Kasukabe Chuo General Hospital I have the following potential conflicts of interest to report: Consulting Employment
Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, Japan Disclosure Hiroshi Ando, MD Kasukabe Chuo General Hospital I have the following potential conflicts of interest to report: Consulting Employment
Use of Laser In BTK Disease (CLI)
") Use of Laser In BTK Disease (CLI) Click to edit academic affiliation, practice or hospital logo(s) of preference. Product and/or sponsor logos not permitted, per CME guidelines. Richard Kovach, MD, FACC,
Use of Laser In BTK Disease (CLI) Click to edit academic affiliation, practice or hospital logo(s) of preference. Product and/or sponsor logos not permitted, per CME guidelines. Richard Kovach, MD, FACC,
Fabrizio Fanelli, MD, EBIR Director Vascular and Interventional Radiology Department "Careggi " University Hospital Florence - Italy
 Don t Use Risky and Embolizing Drug Coated Balloons Below The Knee! Fabrizio Fanelli, MD, EBIR Director Vascular and Interventional Radiology Department "Careggi " University Hospital Florence - Italy
Don t Use Risky and Embolizing Drug Coated Balloons Below The Knee! Fabrizio Fanelli, MD, EBIR Director Vascular and Interventional Radiology Department "Careggi " University Hospital Florence - Italy
9/7/2018. Disclosures. CV and Limb Events in PAD. Challenges to Revascularization. Challenges. Answering the Challenge
 Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Promise and limitations of DCB in long lesions What Have we Learned from Clinical Trials? Ramon L. Varcoe, MBBS, MS, FRACS, PhD
 Promise and limitations of DCB in long lesions What Have we Learned from Clinical Trials? Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor of Vascular Surgery University of New South Wales Sydney,
Promise and limitations of DCB in long lesions What Have we Learned from Clinical Trials? Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor of Vascular Surgery University of New South Wales Sydney,
Present & future of below the knee stenting
 Session 5 Below the knee arteries & limb salvage Present & future of below the knee stenting M. Bosiers K. Deloose P. Peeters 1 PRESENT Clinical perspective whom to treat CRITICAL LIMB ISCHEMIA (CLI) 0
Session 5 Below the knee arteries & limb salvage Present & future of below the knee stenting M. Bosiers K. Deloose P. Peeters 1 PRESENT Clinical perspective whom to treat CRITICAL LIMB ISCHEMIA (CLI) 0
DEB in Periphery: What we Know Till Now
 DEB in Periphery: What we Know Till Now Karl-Ludwig Schulte Vascular Center Berlin Ev. Hospital Königin Elisabeth St. Gertrauden Hospital Charité, CC13, Humboldt-University Berlin www.vascular-center-berlin.com
DEB in Periphery: What we Know Till Now Karl-Ludwig Schulte Vascular Center Berlin Ev. Hospital Königin Elisabeth St. Gertrauden Hospital Charité, CC13, Humboldt-University Berlin www.vascular-center-berlin.com
Peripheral Arterial Disease Extremity
 Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
TOBA II 12-Month Results Tack Optimized Balloon Angioplasty
 TOBA II 12-Month Results Tack Optimized Balloon Angioplasty William Gray, MD System Chief, Cardiovascular Division Main Line Health, Philadelphia, PA Dissection: The Primary Mechanism of Angioplasty Lesions
TOBA II 12-Month Results Tack Optimized Balloon Angioplasty William Gray, MD System Chief, Cardiovascular Division Main Line Health, Philadelphia, PA Dissection: The Primary Mechanism of Angioplasty Lesions
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital
 Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Femoropopliteal Above-Knee Bypass: The True Results
 Femoropopliteal Above-Knee Bypass: The True Results Lise Pyndt Jørgensen, Camilla Rasmussen & Torben V Schroeder Rigshospitalet and University of Copenhagen, DENMARK Treatment options in the femoropopliteal
Femoropopliteal Above-Knee Bypass: The True Results Lise Pyndt Jørgensen, Camilla Rasmussen & Torben V Schroeder Rigshospitalet and University of Copenhagen, DENMARK Treatment options in the femoropopliteal
Dealing with Calcification in BTK Arteries: Is Lithoplasty the Answer?
 Dealing with Calcification in BTK Arteries: Is Lithoplasty the Answer? Andrew Holden, MBChB, FRANZCR, EBIR Director of Interventional Radiology Auckland, New Zealand LINC 2017 January 25 th 2017 Disclosure
Dealing with Calcification in BTK Arteries: Is Lithoplasty the Answer? Andrew Holden, MBChB, FRANZCR, EBIR Director of Interventional Radiology Auckland, New Zealand LINC 2017 January 25 th 2017 Disclosure
Introduction to Peripheral Arterial Disease. Stacey Clegg, MD Interventional Cardiology August
 Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Superficial Femoral Artery Intervention: The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA
 : The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA Peripheral arterial disease (PAD) of the superficial femoral artery (SFA) is the most common cause of intermittent claudication
: The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA Peripheral arterial disease (PAD) of the superficial femoral artery (SFA) is the most common cause of intermittent claudication
Are DES and DEB worth the cost in BTK interventions?
 Are DES and DEB worth the cost in BTK interventions? Thomas Zeller, MD University Heart-Center Freiburg-Bad Krozingen Bad Krozingen, Germany -1- My Disclosures: Advisory Board: Medtronic-Invatec, Gore,
Are DES and DEB worth the cost in BTK interventions? Thomas Zeller, MD University Heart-Center Freiburg-Bad Krozingen Bad Krozingen, Germany -1- My Disclosures: Advisory Board: Medtronic-Invatec, Gore,
Perfusion Assessment in Chronic Wounds
 Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Efficacy of DEB in Calcification and Subintimal Angioplasty
 Efficacy of DEB in Calcification and Subintimal Angioplasty Seung-Woon Rha, MD, PhD, FACC, FAHA, FSCAI, FESC, FAPSIC Div of Cardiovascular Intervention and Research Cardiovascular Center, Korea University
Efficacy of DEB in Calcification and Subintimal Angioplasty Seung-Woon Rha, MD, PhD, FACC, FAHA, FSCAI, FESC, FAPSIC Div of Cardiovascular Intervention and Research Cardiovascular Center, Korea University
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options
 Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI
 Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention