ADPKD, what have the last 10 years taught us? Arlene B. Chapman MD Professor of Medicine Director, Section of Nephrology University of Chicago
|
|
|
- Rebecca Horn
- 5 years ago
- Views:
Transcription
1 2016 ADPKD, what have the last 10 years taught us? Arlene B. Chapman MD Professor of Medicine Director, Section of Nephrology University of Chicago
2 2016 Can we TRUMP the cysts?

3 Disclosures Consultant for KADMON, GENZYME, OTSUKA

4 ADPKD 4th leading cause of ESRD No race is favored Dominantly inherited >3,000,000 worldwide Cysts Kidneys Liver Pancreas Spleen Brain Begins in utero Grantham JJ. N Engl J Med. 2008;359:
5 Disorder MIM Frequency Gene Chromosome Protein Length (bp) HEREDITARY RENAL CYSTIC DISEASES ADPKD :700 1:15,000 PKD1 PKD2 16p13.3 4q22.1 Polycystin 1 Polycystin 2 ARPKD :40,000 PKHD1 6p12.2 Polyductin (fibrocystin) TSC :10,000 TSCI 9q34.13 Hamartin TSC2 16p13.3 Tuberin GCKD Not available MCKD :50,000 MCKD1 MCKD2 (UMOD) FJN Protein size (aa) Exon # SNP HNF-1ß 17cen-q21.3 TCF2 protein :100,000 NPHP1 NPHP2/INVS NPHP3 NPHP4 NPHP5/IQCB1 NPHP6/CEP29 0 NPHP7/GLIS2 NPHP8/RPGRI P1L NPHP9/NEK8 1q21 16p12.3 Uromodulin q13 9q31 3q22.1 1p q q p q q11.1 Nephrocystin-1 Inversin Nephrocystin-3 Nephroretinin Nephrocystin-5 Nephrocystin-6 Nephrocystin-7 Nephrocystin-8 Nephrocystin-9 VHL :53,000 VHL 3p25.3 Von hippel lindau

6 Current Ultrasound Diagnostic Criteria for ADPKD Family History < 40 years: 3 cysts bilaterally years: 4 cysts bilaterally 60 years: 8 cysts bilaterally Revised Pei Criteria 2009, 2012 No Family History 20 cysts distributed bilaterally with a consistent phenotype




7



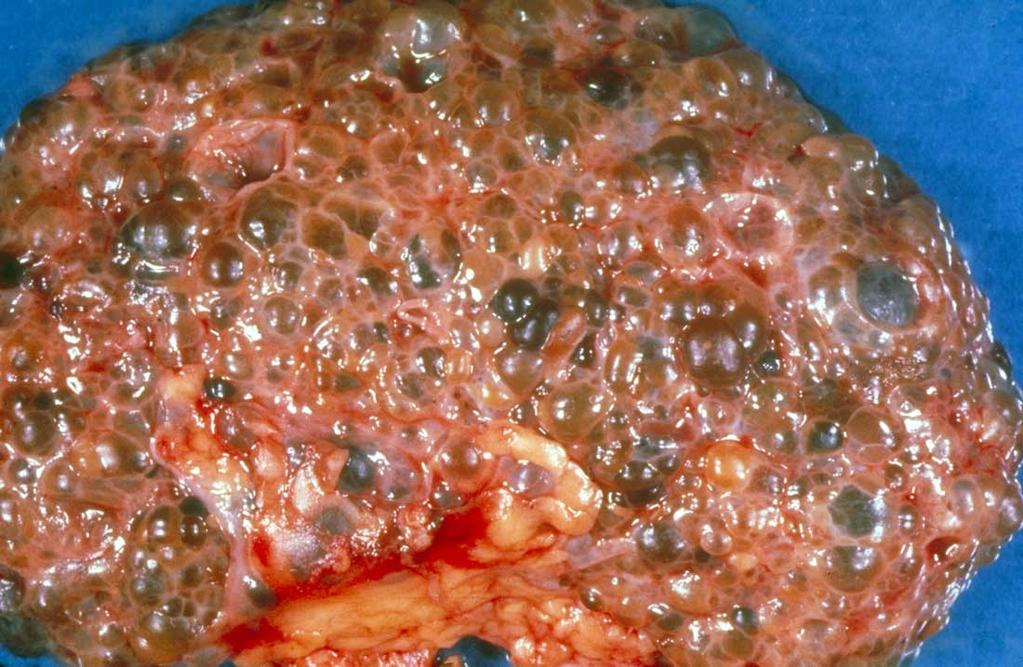
8 Extra-renal Manifestations of ADPKD: Liver Cystic Disease


9
10 Renal Morbidities Associated With ADPKD Chapman A. et.al. American Society of Nephrology Meeting By age 30, over 50% have at least one complication

11 Polycystins 1 and 2 Two genotypes: PKD1 85% ESRD age 55 PKD 2 15% ESRD age 72 Gallagher AR et al. Adv Chronic Kidney Dis. 2010;17:
12 Genetic factors of progression in ADPKD Strong genic and allelic effect on phenotype Cumulative Probability of Survival to ESRD P< Mutation of PKD2: Median age at ESRD: 77.8 yrs Non truncating mutation of PKD1: Median age at ESRD: 65.8 yrs N=1271 Truncating mutation of PKD1: median age at ESRD: 55.1 yrs Cornec-Le Gall E, JASN 2013 Genkyst Cohort update: 2015, non published data
13 Current Results of Genetic Screening in ADPKD Identification of >95% of PKD2 mutations Identification of 85% of PKD1 mutations Cost of sequencing for mutation detection in PKD1/PKD2 is high (>$3,000) and preapproval for insurance coverage is difficult Mutation confirmation in other family members required for potential mutations in PKD1 more so than PKD2 individuals


14

15

16

17 Cell Calcium Is Involved in Promoting Cell Proliferation Torres VE. Adv Chronic Kidney Dis. 2010;17:

18 Mechanism of Fluid Secretion Into Cysts in Response to AVP Wallace DP. Biochim Biophys Acta. 2011;1812: Sullivan LP et al. Physiol Rev. 1998;78:
19 Characteristics of ADPKD That Associate with ESRD Genotype: > 95% PKD1 individuals demonstrate renal cysts by age 30 Hypertension: occurs in 60% with intact renal function by age 30 Proteinuria: is not a common feature of this disease, but has important prognostic implications Gross hematuria: > 50% will have had an episode by age 40 ALL CHARACTERISTICS HAVE NOW BEEN SHOWN TO MEDIATE THEIR RISK THROUGH KIDNEY VOLUME



20 Cyst Burden and Patient Complications in ADPKD Healthy Tissue Cyst Development and Enlargement Vasculature Function Age Signs & Symptoms Urinary Concentrating Defects Hypertension Dull Pain & Discomfort Proteinuria
 100 80 60 40")





21 Kidney function (%) ADPKD Progression Concentrating defect, Hypertension, Proteinuria Pain, Hematuria, Stones, Infections Age (years) Torres Mayo <aupcp
22




23 Inter-observer variability: 2.1% Intra-observer variability:2.4% Day-to-day variability: 2.4%

24 Increased Kidney Volume is Due to Increased Cyst Volume Total Kidney Volume Total Cyst Volume Kidney growth is highly variable and each individual has their own growth curve Measurement variability= Inter-observer 2.1%, Intra-observer 2.4%, Day-to-Day 2.4% Grantham, NEJM CRISP 2006; Chapman Kidney Int 64; , 2003
25

26


27 Average Standardized Unit 1 Change from Baseline Change in Kidney Volume Precedes Change in Kidney Function httkv GFR Years of follow-up p<0.05 for httkv change from baseline; # p<0.05 for GFR change from baseline; httkv=heightadjusted total kidney volume; 1 Percent Change Standardized to a common unit; NIH CRISP Studies; Chapman CJASN 7:479, 2012
28 Sensitivity AUROC = % CI = (0.79, 0.90) Sensitivity = 74% Specificity = 75% Cut Point = 600 (cc/m) Specificity Baseline predictors of CKD Stage 3 endpoint Variable Units AUC Sensitivity Specificity Cut-point 95%CI of AUC P* httkv cc/m (0.79, 0.90) Serum Creatinine mg/dl (0.67, 0.82) 0.02 BUN mg/dl (0.70, 0.83) 0.04 Urine Albumin mg/d (0.61, 0.78) MCP-1 pg/mg (0.68, 0.83) 0.02 Baseline age y (0.59, 0.74) < 0.001

29 Effect of Kidney Growth Rate on Development of ESRD Chapman, AB Unpublished.


30 GFR Compensation for Loss of Parenchyma Loss of Compensated Nephrons Grantham JJ et al. Clin J Am Soc Nephrol. 2006;1:

31 Progressive Rise in Total Kidney Volume Signs and Symptoms of Injury Develop Long Before ADPKD Reaches End Stage Grantham JJ Unpublished.

32 Estimating TKV Using the Ellipsoid Equation W L D Typical values for a cystic kidney L = 15 cm, W = 8 cm, D = 7 cm Volume = 3.14/6 x 15 x 8 x 7 = 440 cc Volume/height = 440 cc/1.73 m = 254 cc/m O Neill WC et al. Am J Kidney Dis. 2005;46:
33 Predicting CKD Stage 3 (iothalamate clearance) utilizing MR and US within 8 years
34 Assessment of TKV and Kidney Length Predictors of CKD Stage 3 in CRISP Participants Method AUC ROC sensitivity specificity Optimal cut point httkv (MR) ml/m % 75.0% 600 ml httkv (US) ml/m % 73.2% 630 ml KL (MR) cm % 92.3% 16.7 cm KL (US) cm % 80.8% 16.8 cm
 20000 10000 8000 6000 Subclass")
 2000 1000 800 600 400 200")

35 Classification by Estimated Rate of Growth (from age and starting HtTKV = 150 ml/m) Subclass 1E > 6% Subclass 1D 4.5 6% 1E 4000 HtTKV (ml/m) Subclass 1C 3 4.5% Subclass 1B 1.5 3% Subclass 1A 1.5% 1C 1A Patient Age (Years) Irazabal. J Am Soc Nephrol 26: , 2015
36 SUMMARY OF CRISP FINDINGS Renal progression in ADPKD is marked by cyst expansion and increases in renal volume prior to loss of renal function Complications including hypertension, gross hematuria, pain, nephrolithiasis, and urinary tract infections occur long before reductions in GFR httkv significantly associates with a decline in GFR and the relationship between httkv and GFR increases with increasing time of followup. HtTKV significantly predicts decline in GFR years before its occurrence

37

38 Baseline TKV and egfr in ADPKD clinical trials 0.35 Ong. A et al. Autosomal dominant polycystic kidney disease: the changing face of clinical management. Lancet vol 385 (2015)
39 Effect of therapeutic interventions Ong. A et al. Autosomal dominant polycystic kidney disease: the changing face of clinical management. Lancet vol 385 (2015)


40 Vasopressin-V 2 Receptor Antagonists Modified from Torres Lancet
41 TOLVAPTAN IN ADPKD Tolvaptan - a highly potent and selective AVP V2 receptor antagonist. Has been shown to slow the progression of PKD in preclinical trials. Currently approved for the treatment of hypervolemic and euvolemic hyponatremia in US Approved in Japan, Canada and Europe as a therapy to slow down the progression of ADPKD in patients with rapidly growing kidneys. LaRiviere WB, Irazabal MV, Torres VE. Novel therapeutic approaches to Autosomal Dominant Polycystic Kidney Disease. Translational research : the journal of laboratory and clinical medicine. 2015;165(4):
42 TEMPO 3:4 TRIAL The Tolvaptan Efficacy and Safety in Management of ADPKD and its Outcomes (TEMPO) 3:4 trial Phase 3, multicenter, randomized, doubleblinded, placebo-controlled, parallel-group clinical study, designed to assess the impact of tolvaptan therapy on the progression of ADPKD. Torres VE, Chapman AB, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med Dec 20;367(25):
43 TEMPO 3:4 TRIAL 1445 ADPKD patients, years, with a TKV >750 ml and CrCL>60 ml/min, across 129 sites worldwide were enrolled in the study between January 2007 and January Tolvaptan group therapy: high dose (120mg/day, n=404), medium dose (90mg/day, n=157), or low dose (60mg/day, n=179). Torres VE, Chapman AB, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med Dec 20;367(25):
44 TEMPO 3:4 TRIAL Primary end point: annual rate of percent change in TKV as measured by MRI. Secondary endpoints: measurable decline renal function, including a composite endpoint of investigator-assessed disease progression. Torres VE, Chapman AB, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med Dec 20;367(25):
45 TEMPO 3:4 TRIAL Results: The intention-to-treat analysis of this study showed that tolvaptan slowed the rate of TKV growth (primary endpoint) by 49% from5.5 to 2.8% per year, and the rate of estimated GFR (egfr) loss on treatment (secondary endpoint) by 26% from 3.70 to 2.72 ml/min/1.73 m2 per year during the median observation period of 3 years. Gansevoort RT, Arici M, Benzing T, et al. Recommendations for the use of tolvaptan in autosomal dominant polycystic kidney disease: a position statement on behalf of the ERA-EDTA Working Groups on Inherited Kidney Disorders and European Renal Best Practice.Nephrology Dialysis Transplantation. 2016;31(3):
46 TEMPO 3:4 TRIAL Over a 3-year period, the increase in total kidney volume in the tolvaptan group was 2.8% per year (95% confidence interval [CI], 2.5 to 3.1), versus 5.5% per year in the placebo group (95% CI, 5.1 to 6.0; P<0.001). Torres VE, Chapman AB, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med Dec 20;367(25):

47 TEMPO 3:4 TRIAL The slope of kidney function (as assessed by means of the reciprocal of the serum creatinine level) from the end of dose escalation to month 36, also favored tolvaptan, Torres VE, Chapman AB, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med Dec 20;367(25):
48 TEMPO 3:4 TRIAL Tolvaptan over placebo had lower rates of worsening kidney function (2 vs. 5 events per 100 person-years of follow-up, P<0.001) Torres VE, Chapman AB, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med Dec 20;367(25):
49 TEMPO 3:4 TRIAL The decrease in kidney pain occurred early and throughout treatment, possibly reflecting a rapid effect on fluid secretion and intracystic pressure. Torres VE, Chapman AB, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med Dec 20;367(25):
50 TEMPO 3:4 TRIAL There were fewer ADPKD-related adverse events in the tolvaptan group but more events related to aquaresis (excretion of electrolytefree water) and hepatic adverse events unrelated to ADPKD, contributing to a higher discontinuation rate (23% vs. 14% in the placebo group). Torres VE, Chapman AB, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med Dec 20;367(25):
51 TEMPO 4:4 EXTENSION TRIAL Two-year open-label extension of the TEMPO 3:4 trial. 976 ADPKD patients received open-label tolvaptan at their highest tolerated dose. Those receiving tolvaptan in TEMPO 3:4 were considered early treatment, and those that received placebo were considered delayed treatment. Torres VE, Chapman AB, Devuyst O,et al. Tolvaptan-treatment of ADPKD confers persistent EGFR improvement: results from the tempo 4:4 extension trial. Nephrol. Dial. Transplant.(2014) 29 (suppl 3): iii5-iii6.
52 TEMPO 4:4 EXTENSION TRIAL Results: Significant improvement in the egfr slope after switching from placebo to tolvaptan (from to ml/min/1.73m2/yr, treatment effect 21%, p=0.048) despite the time difference leading to an increased proportion starting in CKD 3 at TEMPO 4:4 s baseline compared to their own earlier TEMPO 3:4 baseline (37 vs. 15%) Torres VE, Chapman AB, Devuyst O,et al. Tolvaptan-treatment of ADPKD confers persistent EGFR improvement: results from the tempo 4:4 extension trial. Nephrol. Dial. Transplant.(2014) 29 (suppl 3): iii5-iii6.

53 TEMPO 4:4 EXTENSION TRIAL Torres VE, Chapman AB, Devuyst O,et al. Tolvaptan-treatment of ADPKD confers persistent EGFR improvement: results from the tempo 4:4 extension trial. Nephrol. Dial. Transplant.(2014) 29 (suppl 3): iii5-iii6.
54 TEMPO 4:4 EXTENSION TRIAL 5-year early treatment slope (N=554) in TEMPO 3:4 and TEMPO 4:4 combined remained significantly different from the delayed treatment placebo slope (N=422) in TEMPO 3:4 (-2.92 vs ml/min/1.73m2/yr, treatment effect 20%, p<0.0001) (see Figure). Torres VE, Chapman AB, Devuyst O,et al. Tolvaptan-treatment of ADPKD confers persistent EGFR improvement: results from the tempo 4:4 extension trial. Nephrol. Dial. Transplant.(2014) 29 (suppl 3): iii5-iii6.
55 TEMPO 3:4 POST HOC ANALYSIS-1 Patients were randomly assigned 2:1 to splitdose tolvaptan (45/15, 60/30, or 90/30 mg daily as tolerated) or placebo. The primary endpoint was annualized rate of TKV change. Clinically similar beneficial effects of tolvaptan in ADPKD across CKD stages 1-3. Torres VE, Higashihara E, Devuyst O, et al; TEMPO 3:4 Trial Investigators. Effect of Tolvaptan in Autosomal Dominant Polycystic Kidney Disease by CKD Stage: Results from the TEMPO 3:4 Trial. Clin J Am Soc Nephrol Feb 23. pii: CJN
56 TEMPO 3:4 POST HOC ANALYSIS-2 Effects of tolvaptan on albuminuria as a continuous variable. Albuminuria was measured in a spot morning urine sample prior to tolvaptan dosing and expressed as albumin-to-creatinine ratio (ACR). Subjects with higher baseline ACR had higher blood pressure and total kidney volume (TKV) and lower Gansevoort RT, Meijer E, Chapman AB, Czerwiec FS, Devuyst O, Grantham JJ, Higashihara E, Krasa HB, Ouyang J, Perrone RD, Torres VE; TEMPO 3:4 Investigators. Albuminuria and estimated tolvaptan in autosomal-dominant glomerular polycystic kidney disease: results of filtration the TEMPO 3:4 Trial. Nephrol rate Dial Transplant. (egfr) Dec 17. pii: gfv422.
57 TEMPO 3:4 POST HOC ANALYSIS-2 During follow-up, higher baseline ACR was associated with more rapid egfr loss (P < for trend), but not with rate of growth in TKV. During the 3-year trial, ACR rose in placeboand decreased in tolvaptan-treated patients (+0.23 versus mg/mmol). The beneficial effect of tolvaptan on TKV growth and egfr loss was stronger in patients with higher baseline ACR. Gansevoort RT, Meijer E, Chapman AB, Czerwiec FS, Devuyst O, Grantham JJ, Higashihara E, Krasa HB, Ouyang J, Perrone RD, Torres VE; TEMPO 3:4 Investigators. Albuminuria and tolvaptan in autosomal-dominant polycystic kidney disease: results of the TEMPO 3:4 Trial. Nephrol Dial Transplant Dec 17. pii: gfv422.
58 TOLVAPTAN IN VARIOUS LEVELS OF KIDNEY FUNCTION To determine whether the renal hemodynamic effects and pharmacodynamic efficacy of tolvaptan in ADPKD are dependent on GFR. Participants were studied at baseline and after 3 weeks of treatment with tolvaptan given in increasing dosages, if tolerated (doses of 60, 90, and 120mg/d in weeks 1, 2, and 3, respectively). Boertien WE, Meijer E, de Jong PE, et al. Short-term Effects of Tolvaptan in Individuals With Autosomal Dominant Polycystic Kidney Disease at Various Levels of Kidney Function. Am J Kidney Dis Jun;65(6):
59 TOLVAPTAN IN VARIOUS LEVELS OF KIDNEY FUNCTION OUTCOMES: Change in markers for aquaresis (free-water clearance, urine and plasma osmolality, 24-hour urine volume, and plasma copeptin) and kidney injury (TKV and kidney injury biomarkers). Boertien WE, Meijer E, de Jong PE, et al. Short-term Effects of Tolvaptan in Individuals With Autosomal Dominant Polycystic Kidney Disease at Various Levels of Kidney Function. Am J Kidney Dis Jun;65(6):
60 TOLVAPTAN IN VARIOUS LEVELS OF KIDNEY FUNCTION In patients with ADPKD with decreased kidney function, response to tolvaptan is lower for TKV, urinary volume, and osmolality, but larger for fractional free-water clearance. This latter finding suggests that patients with ADPKD with lower GFRs might benefit from long-term treatment with tolvaptan, as has been observed for patients with preserved GFRs. Boertien WE, Meijer E, de Jong PE, et al. Short-term Effects of Tolvaptan in Individuals With Autosomal Dominant Polycystic Kidney Disease at Various Levels of Kidney Function. Am J Kidney Dis Jun;65(6):

61 Changes in Medical Management Age of diagnosis: before 1950: 39 years : 27 years BP medication use 1991:32% 2008:62% ACEI/ARB use: 1991: 7% 2008: 46% SBP/DBP mmhg 1991: 142/ : 133/80 in ADPKD Patch et al, Lancet, 2013
62 Hypotheses Study A: Low (95-110/60-75 mmhg) versus standard ( /70-80 mmhg) BP control will reduce the rate of disease progression measured by change in TKV. Study A and B: Dual blockade of the RAAS with ACE-I and ARB will reduce the rate of disease progression as compared to ACE-I therapy alone. 62
63 Two Clinical Trials: HALT A and B Study A years and healthy baseline egfr > 60 mls/min Study B: years baseline egfr > 25 and < 60 mls/min Outcomes: Primary and secondary differ 63
64 Primary and Secondary Endpoints Primary Study A: Percent change in TKV Study B: Time to death, ESRD or 50% reduction in egfr Secondary Slope of egfr Urine albumin and aldosterone excretion LVMI, RBF and RVR (Study A only) Frequency of all-cause and cardiovascular hospitalizations QOL, pain, PKD related symptoms 64
65 Home BP and Urinary Aldosterone Excretion Levels A B SBP end of study = 13.4 (11.8, 15.0) DBP end of study = 9.3 (7.9, 10.8) NEJM Nov 15, 2014 (online) Low slope=-8.50%/yr Standard slope=-7.39%/yr Diff (95% CI)= (-3.07, 0.60) p=
66 Annualized % Change in TKV Ln(TKV) ml Low slope=5.67%/year Standard slope=6.57%/year Diff (95% CI)=-0.96 (-1.55, -0.24) P=0.006 NEJM Nov 15, 2014 (online) 66
67 egfr Slope Low Low -3.1 ml/min/4 mo Standard -3.1 ml/min/4 mo Standa +0.5 ml/min/4 mo p< ml/min/4 mo p<0.001 Low long term slope = -2.7 ml/min/yr Standard long term slope = -3.1 ml/min/yr p=0.05 Low overall slope = -2.9 ml/min/yr Standard overall slope = -3.0 ml/min/yr p=0.55 NEJM Nov 15, 2014 (online)
68 Conclusions Low blood pressure treatment in young healthy hypertensive ADPKD patients with RAAS blockade is Well tolerated and Safe And results in a 14.2% slower rate of TKV growth over 5 years Reducing proliferation, fluid secretion and normalizing cell-cell interactions are important in ADPKD. Early intervention at specific 68 times of growth may be most beneficial.
69 THANK YOU!
70 Acknowledgements National Institutes of Health PKD Foundation All PKD patients and their families The CRISP and HALT UO1 Consortium Members Boehringer-Ingelheim Pharmaceuticals Inc Merck & Co Inc 70
Autosomal Dominant Polycystic Kidney Disease. Dr. Sameena Iqbal Nephrologist CIUSSS West Island
 Autosomal Dominant Polycystic Kidney Disease Dr. Sameena Iqbal Nephrologist CIUSSS West Island Disclosure Honorarium for Consulting on the Reprise trial from Otsuka Mayo clinic preceptorship for PKD with
Autosomal Dominant Polycystic Kidney Disease Dr. Sameena Iqbal Nephrologist CIUSSS West Island Disclosure Honorarium for Consulting on the Reprise trial from Otsuka Mayo clinic preceptorship for PKD with
Shuma Hirashio 1,2, Shigehiro Doi 1 and Takao Masaki 1*
 Hirashio et al. Renal Replacement Therapy (2018) 4:24 https://doi.org/10.1186/s41100-018-0164-9 CASE REPORT Open Access Magnetic resonance imaging is effective for evaluating the therapeutic effect of
Hirashio et al. Renal Replacement Therapy (2018) 4:24 https://doi.org/10.1186/s41100-018-0164-9 CASE REPORT Open Access Magnetic resonance imaging is effective for evaluating the therapeutic effect of
HHS Public Access Author manuscript Am J Kidney Dis. Author manuscript; available in PMC 2017 July 05.
 HHS Public Access Author manuscript Published in final edited form as: Am J Kidney Dis. 2017 March ; 69(3): 482 484. doi:10.1053/j.ajkd.2016.10.021. Performance of the Chronic Kidney Disease Epidemiology
HHS Public Access Author manuscript Published in final edited form as: Am J Kidney Dis. 2017 March ; 69(3): 482 484. doi:10.1053/j.ajkd.2016.10.021. Performance of the Chronic Kidney Disease Epidemiology
Tolvaptan bei ADPKD: Kritische Beurteilung der Studien
 Tolvaptan bei ADPKD: Kritische Beurteilung der Studien Johannes Mann & Stewart Lambie * KfH Nierenzentrum München Schwabing, Klinik für Nieren- & Hochdruckkrankheiten, Friedrich Alexander Univ. Erlangen-Nürnberg
Tolvaptan bei ADPKD: Kritische Beurteilung der Studien Johannes Mann & Stewart Lambie * KfH Nierenzentrum München Schwabing, Klinik für Nieren- & Hochdruckkrankheiten, Friedrich Alexander Univ. Erlangen-Nürnberg
Nephrology Grand Rounds. Vasishta Tatapudi, MD January 24 th, 2013
 Nephrology Grand Rounds Vasishta Tatapudi, MD January 24 th, 2013 Case Summary Chief complaint: A twenty-six year old African American female veteran presented to ER with left flank pain for two days.
Nephrology Grand Rounds Vasishta Tatapudi, MD January 24 th, 2013 Case Summary Chief complaint: A twenty-six year old African American female veteran presented to ER with left flank pain for two days.
Groningen PKD Expertise Center. Groningen PKD Expertise Center. Groningen PKD Expertise Center. Groningen PKD Expertise Center
 Human polycystic kidney disease. From evolving therapies towards clinical use Prof.dr. Ron T. Gansevoort Chair PKD Expertise Center University Medical Center Groningen The Netherlands Conflict of Interest
Human polycystic kidney disease. From evolving therapies towards clinical use Prof.dr. Ron T. Gansevoort Chair PKD Expertise Center University Medical Center Groningen The Netherlands Conflict of Interest
New Treatments for ADPKD how close are we?
 New Treatments for ADPKD how close are we? Leicester General Hospital 28 Jan 2012 Professor Albert Ong a.ong@sheffield.ac.uk The cystic degeneration of the kidneys, once it reaches the point where it can
New Treatments for ADPKD how close are we? Leicester General Hospital 28 Jan 2012 Professor Albert Ong a.ong@sheffield.ac.uk The cystic degeneration of the kidneys, once it reaches the point where it can
Clinical Experience with Tolvaptan. Prof. Dr. med. O. Devuyst
 Clinical Experience with Tolvaptan Prof. Dr. med. O. Devuyst 1 Outline 1. ADPKD generalities and tolvaptan in ADPKD 2. Who to treat with tolvaptan? How to start? 3. Clinical experience with tolvaptan in
Clinical Experience with Tolvaptan Prof. Dr. med. O. Devuyst 1 Outline 1. ADPKD generalities and tolvaptan in ADPKD 2. Who to treat with tolvaptan? How to start? 3. Clinical experience with tolvaptan in
SUISSE ADPKD Cohort Treatment and Outcomes with Tolvaptan, first in class Vasopressin V2 Antagonist. Hirslanden, 22 March 2018 Stefan Russmann
 SUISSE ADPKD Cohort Treatment and Outcomes with Tolvaptan, first in class Vasopressin V2 Antagonist Hirslanden, 22 March 2018 Stefan Russmann 4 th of July 2004 Database development with outcomes and safety
SUISSE ADPKD Cohort Treatment and Outcomes with Tolvaptan, first in class Vasopressin V2 Antagonist Hirslanden, 22 March 2018 Stefan Russmann 4 th of July 2004 Database development with outcomes and safety
Total Kidney Volume (TKV) in Autosomal Dominant Polycystic Kidney Disease as model for biomarker qualification
 in Autosomal Dominant Polycystic Kidney Disease as model for biomarker qualification") Total Kidney Volume (TKV) in Autosomal Dominant Polycystic Kidney Disease as model for biomarker qualification Roslyn Simms NIHR Clinical Lecturer in Nephrology NIHR Clinical Trials Fellow Monday 23 rd
Total Kidney Volume (TKV) in Autosomal Dominant Polycystic Kidney Disease as model for biomarker qualification Roslyn Simms NIHR Clinical Lecturer in Nephrology NIHR Clinical Trials Fellow Monday 23 rd
Is tolvaptan a promising ally in the treatment strategy of autosomal dominant polycystic kidney disease?
 PERSPECTIVE Port J Nephrol Hypert 2017; 31(4): 243-248 Advance Access publication 4 January 2018 Is tolvaptan a promising ally in the treatment strategy of autosomal dominant polycystic kidney disease?
PERSPECTIVE Port J Nephrol Hypert 2017; 31(4): 243-248 Advance Access publication 4 January 2018 Is tolvaptan a promising ally in the treatment strategy of autosomal dominant polycystic kidney disease?
A New Approach for Evaluating Renal Function and Predicting Risk. William McClellan, MD, MPH Emory University Atlanta
 A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
KDIGO Controversies Conference on Autosomal Dominant Polycystic Kidney Disease (ADPKD)
") KDIGO Controversies Conference on Autosomal Dominant Polycystic Kidney Disease (ADPKD) January 16 19, 2014 Edinburgh, United Kingdom Kidney Disease: Improving Global Outcomes (KDIGO) is an international
KDIGO Controversies Conference on Autosomal Dominant Polycystic Kidney Disease (ADPKD) January 16 19, 2014 Edinburgh, United Kingdom Kidney Disease: Improving Global Outcomes (KDIGO) is an international
Objectives. Pre-dialysis CKD: The Problem. Pre-dialysis CKD: The Problem. Objectives
 The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE
 MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE Introduction Substantial body of prior CKD clinical data characterizes Bard s unique profile Bard has demonstrated
MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE Introduction Substantial body of prior CKD clinical data characterizes Bard s unique profile Bard has demonstrated
Predictors of Autosomal Dominant Polycystic Kidney Disease Progression
 Predictors of Autosomal Dominant Polycystic Kidney Disease Progression Robert W. Schrier,* Godela Brosnahan,* Melissa A. Cadnapaphornchai,* Michel Chonchol,* Keith Friend, Berenice Gitomer,* and Sandro
Predictors of Autosomal Dominant Polycystic Kidney Disease Progression Robert W. Schrier,* Godela Brosnahan,* Melissa A. Cadnapaphornchai,* Michel Chonchol,* Keith Friend, Berenice Gitomer,* and Sandro
Cystic Renal Disease, for USMLE Step One. Howard J. Sachs, MD
 Cystic Renal Disease, for USMLE Step One Howard J. Sachs, MD www.12daysinmarch.com The Major Players Medullary Sponge Kidney (MSK) Polycystic Kidney Disease (PKD) Autosomal Recessive: Childhood Autosomal
Cystic Renal Disease, for USMLE Step One Howard J. Sachs, MD www.12daysinmarch.com The Major Players Medullary Sponge Kidney (MSK) Polycystic Kidney Disease (PKD) Autosomal Recessive: Childhood Autosomal
Age- and height-adjusted total kidney volume growth rate in autosomal dominant polycystic kidney diseases
 https://doi.org/10.1007/s10157-018-1617-8 ORIGINAL ARTICLE Age- and height-adjusted total kidney volume growth rate in autosomal dominant polycystic kidney diseases Eiji Higashihara 1 Kouji Yamamoto 5
https://doi.org/10.1007/s10157-018-1617-8 ORIGINAL ARTICLE Age- and height-adjusted total kidney volume growth rate in autosomal dominant polycystic kidney diseases Eiji Higashihara 1 Kouji Yamamoto 5
Tolvaptan: Slowing Progression of Autosomal Dominant Polycystic Kidney Disease (ADPKD)
") Tolvaptan: Slowing Progression of Autosomal Dominant Polycystic Kidney Disease (ADPKD) Cardiovascular and Renal Drugs Advisory Committee August 5, 2013 Introduction Robert McQuade, PhD Executive Vice President
Tolvaptan: Slowing Progression of Autosomal Dominant Polycystic Kidney Disease (ADPKD) Cardiovascular and Renal Drugs Advisory Committee August 5, 2013 Introduction Robert McQuade, PhD Executive Vice President
clinical investigation see commentary on page 14
 clinical investigation http://www.kidney-international.org 21 International Society of Nephrology see commentary on page 14 A comparison of ultrasound and magnetic resonance imaging shows that kidney length
clinical investigation http://www.kidney-international.org 21 International Society of Nephrology see commentary on page 14 A comparison of ultrasound and magnetic resonance imaging shows that kidney length
Delaying Progression of Renal Complications of Autosomal Dominant Polycystic Kidney Disease by Tolvaptan Inhibition of Arginine Vasopressin
 Delaying Progression of Renal Complications of Autosomal Dominant Polycystic Kidney Disease by Tolvaptan Inhibition of Arginine Vasopressin Briefing Document for 5 August 2013 Advisory Committee Meeting
Delaying Progression of Renal Complications of Autosomal Dominant Polycystic Kidney Disease by Tolvaptan Inhibition of Arginine Vasopressin Briefing Document for 5 August 2013 Advisory Committee Meeting
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Uric acid and CKD. Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George
 Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Tolvaptan in Patients with Autosomal Dominant Polycystic Kidney Disease
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article in Patients with Autosomal Dominant Polycystic Kidney Disease Vicente E. Torres, M.D., Ph.D., Arlene B. Chapman, M.D., Olivier Devuyst,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article in Patients with Autosomal Dominant Polycystic Kidney Disease Vicente E. Torres, M.D., Ph.D., Arlene B. Chapman, M.D., Olivier Devuyst,
tolvaptan 15mg, 30mg, 45mg, 60mg and 90mg tablets (Jinarc ) Otsuka Pharmaceuticals (UK) Ltd SMC No. (1114/15)
 Otsuka Pharmaceuticals (UK) Ltd SMC No. (1114/15)") tolvaptan 15mg, 30mg, 45mg, 60mg and 90mg tablets (Jinarc ) Otsuka Pharmaceuticals (UK) Ltd SMC No. (1114/15) 04 December 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
tolvaptan 15mg, 30mg, 45mg, 60mg and 90mg tablets (Jinarc ) Otsuka Pharmaceuticals (UK) Ltd SMC No. (1114/15) 04 December 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Cost-effectiveness of tolvaptan (Jinarc ) for the treatment of autosomal dominant polycystic kidney disease (ADPKD)
 for the treatment of autosomal dominant polycystic kidney disease (ADPKD)") Cost-effectiveness of tolvaptan (Jinarc ) for the treatment of autosomal dominant polycystic kidney disease (ADPKD) The NCPE has issued a recommendation regarding the cost-effectiveness of tolvaptan (Jinarc
Cost-effectiveness of tolvaptan (Jinarc ) for the treatment of autosomal dominant polycystic kidney disease (ADPKD) The NCPE has issued a recommendation regarding the cost-effectiveness of tolvaptan (Jinarc
A systematic review of the predictors of disease progression in patients with autosomal dominant polycystic kidney disease
 Woon et al. BMC Nephrology DOI 10.1186/s12882-015-0114-5 RESEARCH ARTICLE Open Access A systematic review of the predictors of disease progression in patients with autosomal dominant polycystic kidney
Woon et al. BMC Nephrology DOI 10.1186/s12882-015-0114-5 RESEARCH ARTICLE Open Access A systematic review of the predictors of disease progression in patients with autosomal dominant polycystic kidney
Tolvaptan and Kidney Pain in Patients With Autosomal Dominant Polycystic Kidney Disease: Secondary Analysis From a Randomized Controlled Trial
 Tolvaptan and Kidney Pain in Patients With Autosomal Dominant Polycystic Kidney Disease: Secondary Analysis From a Randomized Controlled Trial Niek F. Casteleijn, University of Groningen Jaime D. Blais,
Tolvaptan and Kidney Pain in Patients With Autosomal Dominant Polycystic Kidney Disease: Secondary Analysis From a Randomized Controlled Trial Niek F. Casteleijn, University of Groningen Jaime D. Blais,
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Case report: a thiazide diuretic to treat polyuria induced by tolvaptan
 Kramers et al. BMC Nephrology (2018) 19:157 https://doi.org/10.1186/s12882-018-0957-7 CASE REPORT Open Access Case report: a thiazide diuretic to treat polyuria induced by tolvaptan Bart J. Kramers *,
Kramers et al. BMC Nephrology (2018) 19:157 https://doi.org/10.1186/s12882-018-0957-7 CASE REPORT Open Access Case report: a thiazide diuretic to treat polyuria induced by tolvaptan Bart J. Kramers *,
Tolvaptan for treating autosomal dominant polycystic kidney disease
 in collaboration with: ERRATUM TO Tolvaptan for treating autosomal dominant polycystic kidney disease 1. The word ********* has been marked as commercial in confidence. a. Section 1.4 (page 13): Hence,
in collaboration with: ERRATUM TO Tolvaptan for treating autosomal dominant polycystic kidney disease 1. The word ********* has been marked as commercial in confidence. a. Section 1.4 (page 13): Hence,
Patient Survey of current water Intake practices in autosomal dominant Polycystic kidney disease: the SIPs survey
 Clinical Kidney Journal, 2017, 1 5 doi: 10.1093/ckj/sfw153 Original Article ORIGINAL ARTICLE Patient Survey of current water Intake practices in autosomal dominant Polycystic kidney disease: the SIPs survey
Clinical Kidney Journal, 2017, 1 5 doi: 10.1093/ckj/sfw153 Original Article ORIGINAL ARTICLE Patient Survey of current water Intake practices in autosomal dominant Polycystic kidney disease: the SIPs survey
The National Quality Standards for Chronic Kidney Disease
 The National Quality Standards for Chronic Kidney Disease Dr Robert Lewis Chief of Service, Wessex Kidney Centre, Portsmouth Specialist Committee Member Quality Standard for Chronic Kidney Disease, NICE
The National Quality Standards for Chronic Kidney Disease Dr Robert Lewis Chief of Service, Wessex Kidney Centre, Portsmouth Specialist Committee Member Quality Standard for Chronic Kidney Disease, NICE
Primary Care Approach to Management of CKD
 Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
microrna Therapeutics Harnessing the power of micrornas to target multiple pathways of disease
 microrna Therapeutics Harnessing the power of micrornas to target multiple pathways of disease January 2018 Safe Harbor Statement Statements contained in this presentation regarding matters that are not
microrna Therapeutics Harnessing the power of micrornas to target multiple pathways of disease January 2018 Safe Harbor Statement Statements contained in this presentation regarding matters that are not
23-Jun-15. Albuminuria Renal and Cardiovascular Consequences A history of progress since ,490,000. Kidney Center, UMC Groningen
 Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Disclosures. Outline. Outline 5/23/17 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Research Introduction
 Research Introduction 9.17.13 Altered metabolism in polycystic kidney disease Telomerase activity in polycystic kidney disease cells Autosomal dominant polycystic kidney disease ADPKD is the most common
Research Introduction 9.17.13 Altered metabolism in polycystic kidney disease Telomerase activity in polycystic kidney disease cells Autosomal dominant polycystic kidney disease ADPKD is the most common
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Disclosures. Outline. Outline 7/27/2017 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Managing patients with renal disease
 Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Samsca. Samsca (tolvaptan) Description
 Description") Subject: Samsca Page: 1 of 5 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: September 20, 2018 Samsca Description Samsca (tolvaptan)
Subject: Samsca Page: 1 of 5 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: September 20, 2018 Samsca Description Samsca (tolvaptan)
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
PRIMARY PHASE 2 ANALYSES FROM CARDINAL: A PHASE 2/3 STUDY OF BARDOXOLONE METHYL IN PATIENTS WITH ALPORT SYNDROME
 PRIMARY PHASE 2 ANALYSES FROM CARDINAL: A PHASE 2/3 STUDY OF BARDOXOLONE METHYL IN PATIENTS WITH ALPORT SYNDROME 217 American Society of Nephrology Meeting Geoffrey A. Block 1, Pablo E. Pergola 2, Lesley
PRIMARY PHASE 2 ANALYSES FROM CARDINAL: A PHASE 2/3 STUDY OF BARDOXOLONE METHYL IN PATIENTS WITH ALPORT SYNDROME 217 American Society of Nephrology Meeting Geoffrey A. Block 1, Pablo E. Pergola 2, Lesley
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Renal Cystic Disease. Dr H Bierman
 Renal Cystic Disease Dr H Bierman Objectives Be able to diagnose renal cystic disease Genetic / non-genetic Be able to describe patterns of various renal cystic disease on routine imaging studies Be able
Renal Cystic Disease Dr H Bierman Objectives Be able to diagnose renal cystic disease Genetic / non-genetic Be able to describe patterns of various renal cystic disease on routine imaging studies Be able
Creatinine & egfr A Clinical Perspective. Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC
 Creatinine & egfr A Clinical Perspective Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC CLINICAL CONDITIONS WHERE ASSESSMENT OF GFR IS IMPORTANT Stevens et al. J Am Soc Nephrol 20: 2305
Creatinine & egfr A Clinical Perspective Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC CLINICAL CONDITIONS WHERE ASSESSMENT OF GFR IS IMPORTANT Stevens et al. J Am Soc Nephrol 20: 2305
Polycystic Kidney Disease
 Polycystic Kidney Disease Theodore I. Steinman, M.D. Clinical Professor of Medicine Harvard Medical School Senior Physician Beth Israel Deaconess Medical Ctr. Brigham and Women s Hospital Disclosures Grant
Polycystic Kidney Disease Theodore I. Steinman, M.D. Clinical Professor of Medicine Harvard Medical School Senior Physician Beth Israel Deaconess Medical Ctr. Brigham and Women s Hospital Disclosures Grant
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Technology appraisal guidance Published: 28 October 2015 nice.org.uk/guidance/ta358
 Tolvaptan for treating autosomal dominant polycystic kidney disease Technology appraisal guidance Published: 28 October 2015 nice.org.uk/guidance/ta358 NICE 2017. All rights reserved. Subject to Notice
Tolvaptan for treating autosomal dominant polycystic kidney disease Technology appraisal guidance Published: 28 October 2015 nice.org.uk/guidance/ta358 NICE 2017. All rights reserved. Subject to Notice
Tolvaptan in Later-Stage Autosomal Dominant Polycystic Kidney Disease
 The new england journal of medicine Original Article Tolvaptan in Later-Stage Autosomal Dominant Polycystic Kidney Disease Vicente E. Torres, M.D., Ph.D., Arlene B. Chapman, M.D., Olivier Devuyst, M.D.,
The new england journal of medicine Original Article Tolvaptan in Later-Stage Autosomal Dominant Polycystic Kidney Disease Vicente E. Torres, M.D., Ph.D., Arlene B. Chapman, M.D., Olivier Devuyst, M.D.,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CARDIO-RENAL SYNDROME
 CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
SPRINT: Consequences for CKD patients
 SPRINT: Consequences for CKD patients 29 e Workshop Nierziekten Papendal 2018 December 12, 2018 MICHAEL ROCCO, MD, MSCE VARDAMAN M. BUCKALEW JR. PROFESSOR OF MEDICINE PROFESSOR OF PUBLIC HEALTH SCIENCES
SPRINT: Consequences for CKD patients 29 e Workshop Nierziekten Papendal 2018 December 12, 2018 MICHAEL ROCCO, MD, MSCE VARDAMAN M. BUCKALEW JR. PROFESSOR OF MEDICINE PROFESSOR OF PUBLIC HEALTH SCIENCES
Volume 15 - Issue 3, Cover Story
 Volume 15 - Issue 3, 2015 - Cover Story ADPKD: Realising Progress Through Patient Empowerment Dr. Richard Sandford, PhD, FRCP ******@***medschl.cam.ac.uk Consultant Clinical Geneticist - Addenbrooke s
Volume 15 - Issue 3, 2015 - Cover Story ADPKD: Realising Progress Through Patient Empowerment Dr. Richard Sandford, PhD, FRCP ******@***medschl.cam.ac.uk Consultant Clinical Geneticist - Addenbrooke s
Acknowledgements. National Kidney Foundation of Connecticut Mark Perazella. Co-PI Slowing the progression of chronic kidney disease to ESRD
 A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Prag. Polycystic kidney disease: ARPKD & ADPKD. Max Christoph Liebau
 Prag Polycystic kidney disease: ARPKD & ADPKD Max Christoph Liebau Department of Pediatrics and Center for Molecular Medicine, University Hospital of Cologne Glasgow, 06th of September 2017 Cystic kidney
Prag Polycystic kidney disease: ARPKD & ADPKD Max Christoph Liebau Department of Pediatrics and Center for Molecular Medicine, University Hospital of Cologne Glasgow, 06th of September 2017 Cystic kidney
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Elevation of Serum Creatinine: When to Screen, When to Refer. Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC
 Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Evaluation of Chronic Kidney Disease KDIGO. Paul E de Jong University Medical Center Groningen The Netherlands
 Evaluation of Chronic Kidney Disease Paul E de Jong University Medical Center Groningen The Netherlands Evaluation and Management of CKD 1. Definition and classification of CKD 2. Definition and impact
Evaluation of Chronic Kidney Disease Paul E de Jong University Medical Center Groningen The Netherlands Evaluation and Management of CKD 1. Definition and classification of CKD 2. Definition and impact
University of Groningen. Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste
 University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
Laura Girardat-Rotar 1, Julia Braun 1, Milo A. Puhan 1, Alison G. Abraham 1,2 and Andreas L. Serra 1,3*
 Girardat-Rotar et al. BMC Nephrology (2017) 18:241 DOI 10.1186/s12882-017-0654-y RESEARCH ARTICLE Open Access Temporal and geographical external validation study and extension of the Mayo Clinic prediction
Girardat-Rotar et al. BMC Nephrology (2017) 18:241 DOI 10.1186/s12882-017-0654-y RESEARCH ARTICLE Open Access Temporal and geographical external validation study and extension of the Mayo Clinic prediction
TREAT THE KIDNEY TO SAVE THE HEART. Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009
 TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Tolvaptan: a Possible Treatment for Autosomal Dominant Polycystic Kidney Disease
 Pacific University CommonKnowledge School of Physician Assistant Studies Theses, Dissertations and Capstone Projects Fall 9-20-2013 Tolvaptan: a Possible Treatment for Autosomal Dominant Polycystic Kidney
Pacific University CommonKnowledge School of Physician Assistant Studies Theses, Dissertations and Capstone Projects Fall 9-20-2013 Tolvaptan: a Possible Treatment for Autosomal Dominant Polycystic Kidney
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Report on the Deliberation Results
 Report on the Deliberation Results March 3, 2014 Evaluation and Licensing Division, Pharmaceutical and Food Safety Bureau Ministry of Health, Labour and Welfare [Brand name] (a) Samsca Tablets 7.5 mg (b)
Report on the Deliberation Results March 3, 2014 Evaluation and Licensing Division, Pharmaceutical and Food Safety Bureau Ministry of Health, Labour and Welfare [Brand name] (a) Samsca Tablets 7.5 mg (b)
Blood Pressure and Atrial Natriuretic Peptide (ANP) Levels in Patients with Autosomal Dominant Polycystic Kidney Disease.
 Levels in Patients with Autosomal Dominant Polycystic Kidney Disease.") Blood Pressure and Atrial Natriuretic Peptide (ANP) Levels in Patients with Autosomal Dominant Polycystic Kidney Disease. Rafie Shakir Al-Khafaji* Ali Hmood Al-Saadi** Haider Kamil Zaidan** * Faculty of
Blood Pressure and Atrial Natriuretic Peptide (ANP) Levels in Patients with Autosomal Dominant Polycystic Kidney Disease. Rafie Shakir Al-Khafaji* Ali Hmood Al-Saadi** Haider Kamil Zaidan** * Faculty of
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Optimal blood pressure targets in chronic kidney disease
 Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
3 generations of ADPKD. 1 long-awaited treatment.
 3 generations of ADPKD. 1 long-awaited treatment. HOPE is finally here now that treatment is available for people with autosomal dominant polycystic kidney disease (ADPKD). JYNARQUE is proven to slow kidney
3 generations of ADPKD. 1 long-awaited treatment. HOPE is finally here now that treatment is available for people with autosomal dominant polycystic kidney disease (ADPKD). JYNARQUE is proven to slow kidney
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
The CARI Guidelines Caring for Australasians with Renal Impairment. Specific management of IgA nephropathy: role of fish oil
 Specific management of IgA nephropathy: role of fish oil Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Early and prolonged treatment with fish oil may retard
Specific management of IgA nephropathy: role of fish oil Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Early and prolonged treatment with fish oil may retard
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Long-term Non-ESRD Kidney Donor Risks. Arthur Matas Dept Surgery University of Minnesota
 Long-term Non-ESRD Kidney Donor Risks Arthur Matas Dept Surgery University of Minnesota Conflict of Interest Disclosure I have no relevant financial relationships to disclose No off label use will be discussed
Long-term Non-ESRD Kidney Donor Risks Arthur Matas Dept Surgery University of Minnesota Conflict of Interest Disclosure I have no relevant financial relationships to disclose No off label use will be discussed
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Masatoshi Kawashima 1, Koji Wada 2, Hiroshi Ohta 2, Rika Moriya 3 and Yoshiharu Aizawa 1. Journal of Occupational Health
 176 J Occup Health, Vol. 54, 2012 J Occup Health 2012; 54: 176 180 Journal of Occupational Health Evaluation of Validity of the Urine Dipstick Test for Identification of Reduced Glomerular Filtration Rate
176 J Occup Health, Vol. 54, 2012 J Occup Health 2012; 54: 176 180 Journal of Occupational Health Evaluation of Validity of the Urine Dipstick Test for Identification of Reduced Glomerular Filtration Rate
Chronic Kidney Disease. Paul Cockwell Queen Elizabeth Hospital Birmingham
 Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Pharmacokinetics and pharmacodynamics of oral tolvaptan in patients with varying degrees of renal function
 http://www.kidney-international.org & 13 International Society of Nephrology OPEN Pharmacokinetics and pharmacodynamics of oral tolvaptan in patients with varying degrees of renal function Susan E. Shoaf
http://www.kidney-international.org & 13 International Society of Nephrology OPEN Pharmacokinetics and pharmacodynamics of oral tolvaptan in patients with varying degrees of renal function Susan E. Shoaf
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?