Case study Chest Pain treating angina without a bypass or stent
|
|
|
- Ernest Craig
- 5 years ago
- Views:
Transcription

1 Case study Chest Pain treating angina without a bypass or stent Dr Clare Hawley Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI for Angina Management Programme Hon Lecturer Cardiology University of Bradford for PwSI
2 Declaration of Conflicts of Interests In the past I have received honoraria/expenses for educational talks from: Bayer, Boeheringer Ingelheim, Lundbeck, Menarini, Pfizer and Takeda
3 George is a 58 year old alarm fitter April 2013 seen in RACPC 2 years of typical angina, dismissed as getting old Instructor at gym noticed high heart rates Risk factors: ex smoker, HBP, hyperlipidaemia, Dad MI age 55 Rx: Felodipine MR 5mg od, Simvastatin 40 mg od O/E: No other obvious cause for symptoms ETT: 7 mins got symptoms 2mm ST depression in V4 & 5 Recovery: TWI for 9 mins Diagnosis: Stable angina
4 Medical Management Secondary prevention Antiplatelet Statin Anti anginal GTN Beta blocker Exisiting: Felodipine MR 5mg od Simvastatin 40mg od New: Aspirin 75mg od Atenolol 50mg od GTN spray Remember this was 2013!
5 Angiogram - May 2013 LMS: unobstructed LAD: 30% proximal stenosis D1: 100% occlusion Cx: 70% mid vessel RCA: 95% mid & 95% post left ventricular branch RCA receives collaterals from LAD ECHO: normal LV function Told likely to need 2 stents MDT: Not suitable for stenting No prognostic indication for CABG but could do for symptoms Referred to Angina Management Programme (AMP)
6 More medication Felodipine increased Isosorbide MN added HR 58 bpm BP 138/78 Felodipine MR 10mg od Simvastatin 40mg od Aspirin 75mg od Atenolol 50mg od ISMN 60mg bd GTN spray
7 1 st Visit to AMP Attended with wife Lynne Situation: Chest pain getting worse despite 3 anti-anginals 3-4 episodes per week on exertion & when stressed Episodes lasted at least 15 mins with 9/10 severity Reluctant to use GTN because of headache 2 admissions with normal ECG & no troponin rise Off work, taking no exercise QOL: 50% frightened & frustrated

8 Beliefs & misconceptions Arteries furring up & pain due to build up of pressure Angina damages the heart like a mini heart attack Chest pain is the heart protecting itself People should their best to avoid bringing on angina A stent would fix his CAD & protect from a future heart attack Devastated no chance of stent not keen on bypass
9 What patients think-based on > hour discovery interviews 1 angina damages the heart (50%) like a mini heart attack (40%) angina is due to back pressure on the heart as it struggles to force blood past coronary narrowings the arteries are furring up so it is inevitable that in time they will block completely & that will be it it is important to avoid anything that brings on angina (82%) stents prevent heart attacks & increase life expectancy (90%) 2 1 Chester 2 Kureshi F. BMJ Sept 2014
 Most patients don t really understand their")
10 CHD often presents dramatically (999 or 2ww RACPC) Management focuses on diagnostic investigations & heroic interventions (drugs, stents & bypasses) Chest pain causes fear & anxiety for patients & staff Patient education is often overlooked (not resourced) Most patients don t really understand their angina
11 What our patients & some colleagues don t know about chronic stable angina Angina doesn t damage the heart With the right treatment & lifestyle prognosis is good & mortality low >70% survive 9 years from diagnosis * Feels unpleasant but myocardial ischaemia promotes collateral circulation & ischaemic pre-conditioning Pain due to mix up of pain & messaging nerves Adrenaline makes pain feel worse & endorphins provide relief Symptoms are amplified by psychological factors & can be controlled by better understanding, relaxation & exercise *Henry TD. European Heart Journal 2013
 May improve symptoms & QOL - evidence of benefit is limited Don t improve life expectancy or")
12 The truth about treatments Secondary prevention long term benefit Anti-platelet Statins ACE-I (for some) Anti-anginals for symptom relief only Reduce O 2 demand by reducing heart rate, contractility or vasodilatation rather than increase blood supply (BB, CCB, ISMN, Nicorandil, Ivabradine, Ranolazine) May improve symptoms & QOL - evidence of benefit is limited Don t improve life expectancy or reduce CV events Medical treatment of stable angina. Manolis IJ Cardiology 220(2016)
13 Angioplasty & stents in stable angina Improve symptoms & QOL Fractional Flow Reserve helps inform which lesions to treat But Doesn t reduce death, MI, admissions or further revasc* Technology is improving but still not without risk Procedural complications - MI, CVA Late complications: in stent stenosis (4-20% in 1 st 6 months less if drug eluting) in stent thrombosis (1-2%) Requires dual antiplatelet therapy for up to 12 mo Initial Coronary Stent Implantation With Medical Therapy vs Medical Therapy Alone for Stable Coronary Artery Disease: Meta-analysis of RCTsArch Intern Med. 2012)
14 CABG in stable angina Palliative CABG For symptom control only (70%of procedures) 90% effective 10 years: 40% have angina back Prognostic CABG Improves survival in people with: significant left main stem disease 3 vessel disease + left ventricular dysfunction (LVD) 2 vessel disease involving proximal LAD & LVD But Major surgery - complications occur in 2-4% Post op pain Re do surgery is much less effective & more risky
15 The truth about angina pain Disability is more closely related to health beliefs & misconceptions than the degree of myocardial dysfunction or perfusion * Reaction & response to pain depends on: what we think is happening what we believe the consequences will be personal memories of something similar reactions of others around us The poorly informed make bad healthcare choices Empowered & informed people do better * Foreman RD. Ann Rev Physiol 1999

16 Chester M & Lewin R
17 AMP initial consultation 2 hours with patient & partner Assess the person s symptoms & impact of on QOL Explore what they want & what stops them getting it Establish beliefs & misconceptions about angina Provide education about what angina is & isn t collaterals & ischaemic pre-conditioning pain & somatic nerve pathways importance of fear & anxiety in angina impact of other conditions
18 AMP 4 group sessions Teach people how to control their symptoms Thinking differently about angina (CBT) Using relaxation techniques Exercise - goal setting & pacing Discuss risks & benefits of medication, stents & CABG Motivational interviewing to support healthy lifestyle How to recognise a heart attack & deal with setbacks Refer some on to cardiac rehab programme Follow 6 weeks & 12 months
19 George s story Jan 2014: feeling much better saw cardiologist d/c Dec 2014: just 2 episodes of angina in 6 months, not used GTN, more relaxed about it Attitude to angina -8 to +10 Back at work, attending gym QOL: from 50 to 70% 2017: no admissions, not bypass or stent, off ISMN Win win
20 Chesterfield AMP results are similar to NRAC (unpublished) Referrals come from hospital & GPs (ratio 2:1) 2: 1 males: female Average age mid 60s (range years) True refractory angina + people with a revasc option First 11 cohorts (n=146) 146 started Data for months 15% did not complete 12 mo f/u 22 slots wasted through DNAs
21 Chesterfield AMP QOL & symptoms 98% reported symptoms of angina had improved 90% reported improved QOL on average by 22% 35% reduction in misconceptions score Patient satisfaction with the programme very high best bit was all the information it has taken away the worry I can cope now I understand what is happening I wish I had had this 10 years ago things would have been so different
22 Chesterfield AMP savings 59 had a possible palliative revascularisation option After 12 months 22 of 29 (77%) did not go on to PCI 27 of 30 (90%) did not go on to CABG/re-do CABG Overall reduced hospital activity compared to 12 mo before recruitment with overall savings of 800 pp
23 Self Management Interventions for Chronic Stable Angina 2014 Meta-analysis of 7 short term RCTs showed 1 Fewer episodes of angina & less use of GTN Improved depression scores Fewer admissions & shorter length of stay Bradford Angina Service: showed improvement in symptoms of depression & QOL 2 Specialist Angina Service Royal Brompton & Harefield improved psychosocial outcomes, QoL & drug use 3 1 McGillion. BMC CV Disorders 2014, 14:14 2 Patel P. Br J Cardiol 2016;23: Cheng BCS 2017 poster

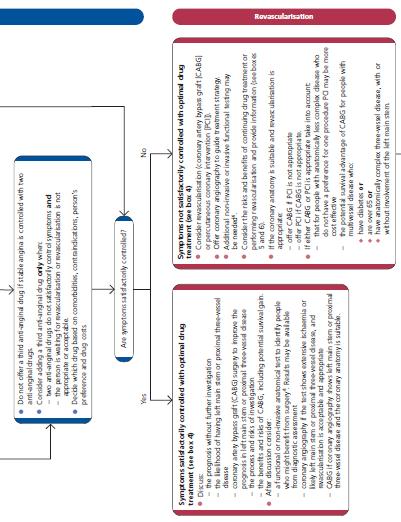


24 NICE 2011 Care pathway
25 Key points Angina is frightening for patients and their families Most patients don t understand their condition People need to know that angina doesn t damage the heart but a sign the heart growing collaterals which will protect it from damage if a heart attack happens in the future Angina Management Programmes which provide education, challenge misconceptions and promote stress management & relaxation to control symptoms empower patients to make healthy lifestyle choices which can reduce the need for investigations, surgery and drugs
Next patient please Dementia Clare Hawley 2018
 Next patient please Dementia Clare Hawley 2018 I have no conflict of interest to declare Dr Clare Hawley Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory Angina Hon Clinical
Next patient please Dementia Clare Hawley 2018 I have no conflict of interest to declare Dr Clare Hawley Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory Angina Hon Clinical
This information explains the advice about the care and treatment of people with stable angina that is set out in NICE clinical guideline 126.
 Information for the public Published: 1 July 2011 nice.org.uk About this information NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and the treatments
Information for the public Published: 1 July 2011 nice.org.uk About this information NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and the treatments
Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126
 Stable angina: management Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Stable angina: management Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Richard Grocott Mason
 Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Ischaemic Heart Disease
 Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Coronary Heart Disease. Iqbal Malik
 Coronary Heart Disease Iqbal Malik Pathophysiology IHD Case chest pain Question -interactive What is the result of the exercise test? 1. negative 2. positive 3. equivocal 4. other Q2 answer STEMI! What
Coronary Heart Disease Iqbal Malik Pathophysiology IHD Case chest pain Question -interactive What is the result of the exercise test? 1. negative 2. positive 3. equivocal 4. other Q2 answer STEMI! What
How to investigate (Cardiac) Chest Pain
 Chest Pain") RCP UPDATE IN MEDICINE 27 th November 2017 How to investigate (Cardiac) Chest Pain Justin Carter Consultant Cardiologist North Tees and Hartlepool NHS Trust The spectrum of coronary disease No Disease
RCP UPDATE IN MEDICINE 27 th November 2017 How to investigate (Cardiac) Chest Pain Justin Carter Consultant Cardiologist North Tees and Hartlepool NHS Trust The spectrum of coronary disease No Disease
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Disclosures. Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin
 Disclosures Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin Servier International, Boehringer Ingelheim Servier International,
Disclosures Speaker s bureau: Research grant: Advisory Board: Servier International, Bayer, Merck Serono, Novartis, Boehringer Ingelheim, Lupin Servier International, Boehringer Ingelheim Servier International,
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines
 Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Review Protocol Patient information
 Review Protocol Patient information What are information needs of patients with stable angina regarding their condition and its management? Adults with a diagnosis of stable angina including people with
Review Protocol Patient information What are information needs of patients with stable angina regarding their condition and its management? Adults with a diagnosis of stable angina including people with
Your heart attack procedure explained
 Patient information Your heart attack procedure explained i Important information for all patients. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk
Patient information Your heart attack procedure explained i Important information for all patients. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011
 Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
Treatment Options for Angina
 Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Current Management of Coronary Artery Disease with Special Emphasis on the Elderly and Diabetic
 Current Management of Coronary Artery Disease with Special Emphasis on the Elderly and Diabetic Dr Albert Ko FRACP, FCSANZ Interventional Cardiologist Ascot Angiography Auckland, New Zealand Diagnosis
Current Management of Coronary Artery Disease with Special Emphasis on the Elderly and Diabetic Dr Albert Ko FRACP, FCSANZ Interventional Cardiologist Ascot Angiography Auckland, New Zealand Diagnosis
Nurse Prescribing in Cardiology. Jan Keenan Consultant Nurse; NMP Lead
 Nurse Prescribing in Cardiology Jan Keenan Consultant Nurse; NMP Lead Jan.keenan@ouh.nhs.uk Objectives Nurse prescribing for cardiology: where are we now? What are nurses prescribing in cardiology? The
Nurse Prescribing in Cardiology Jan Keenan Consultant Nurse; NMP Lead Jan.keenan@ouh.nhs.uk Objectives Nurse prescribing for cardiology: where are we now? What are nurses prescribing in cardiology? The
Treatment of Stable Coronary Artery Disease Pharmacotherapy
 Treatment of Stable Coronary Artery Disease Pharmacotherapy José López-Sendón Hospital Universitario La Paz. Madrid. Spain Conflict of interest: I will discuss off label use and/or investigational use
Treatment of Stable Coronary Artery Disease Pharmacotherapy José López-Sendón Hospital Universitario La Paz. Madrid. Spain Conflict of interest: I will discuss off label use and/or investigational use
The NICE chest pain guideline 1 year on. Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The NICE chest pain guideline 1 year on Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust The Society for Acute Medicine, 5 th International Conference,
The NICE chest pain guideline 1 year on Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust The Society for Acute Medicine, 5 th International Conference,
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Medicines Management Optimisation Achieving your 5 a day post-mi Medication WORKSHOP
 Medicines Management Optimisation Achieving your 5 a day post-mi Medication WORKSHOP What is Medicines Optimisation? the safe and effective use of medicines to enable the best possible outcomes NICE ng
Medicines Management Optimisation Achieving your 5 a day post-mi Medication WORKSHOP What is Medicines Optimisation? the safe and effective use of medicines to enable the best possible outcomes NICE ng
Angioplasty Your quick guide
 Angioplasty Your quick guide Coronary heart disease is the UK s single biggest killer. For over 50 years we ve pioneered research that s transformed the lives of people living with heart and circulatory
Angioplasty Your quick guide Coronary heart disease is the UK s single biggest killer. For over 50 years we ve pioneered research that s transformed the lives of people living with heart and circulatory
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Practical Office Management of Stable Angina
 Practical Office Management of Stable Angina All you need to know about it in 30 minutes Andy Ignaszewski MD FRCPC Head, Division of Cardiology PHC Physician Director, PHC Heart Centre Clinical Professor,
Practical Office Management of Stable Angina All you need to know about it in 30 minutes Andy Ignaszewski MD FRCPC Head, Division of Cardiology PHC Physician Director, PHC Heart Centre Clinical Professor,
Rapid access chest pain clinic (RACPC)
") Rapid access chest pain clinic (RACPC) Context Coronary heart disease (CHD) remains the common cause of death and premture death in the UK with 15% of men and 7% of women dying from the disease. UK death
Rapid access chest pain clinic (RACPC) Context Coronary heart disease (CHD) remains the common cause of death and premture death in the UK with 15% of men and 7% of women dying from the disease. UK death
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
MRCP(UK) PACES. INFORMATION FOR THE CANDIDATE Training Scenario N 001 SAMPLE HOST CENTRE Station 5: BRIEF CLINICAL CONSULTATION
 PACES. INFORMATION FOR THE CANDIDATE Training Scenario N 001 SAMPLE HOST CENTRE Station 5: BRIEF CLINICAL CONSULTATION") INFORMATION FOR THE CANDIDATE MRCP(UK) PACES Station 5: BRIEF CLINICAL CONSULTATION Patient details: Mrs XX aged 45. Your role: You are the doctor in the medical admissions unit. You have 10 minutes with
INFORMATION FOR THE CANDIDATE MRCP(UK) PACES Station 5: BRIEF CLINICAL CONSULTATION Patient details: Mrs XX aged 45. Your role: You are the doctor in the medical admissions unit. You have 10 minutes with
Associate Professor Gerry Devlin
 Associate Professor Gerry Devlin Clinical Cardiologist and Interventional Cardiologist NZ Heart Foundation Hamilton 9:00-9:15 Secondary Prevention of IHD The Challenge of Secondary Prevention Associate
Associate Professor Gerry Devlin Clinical Cardiologist and Interventional Cardiologist NZ Heart Foundation Hamilton 9:00-9:15 Secondary Prevention of IHD The Challenge of Secondary Prevention Associate
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
Cardiac Rehabilitation after Primary Coronary Intervention CONTRA
 DEBATE SESSION Is there a role for cardiac rehabilitation in the modern era of Percutaneous coronary intervention and coronary artery bypass grafting? Cardiac Rehabilitation after Primary Coronary Intervention
DEBATE SESSION Is there a role for cardiac rehabilitation in the modern era of Percutaneous coronary intervention and coronary artery bypass grafting? Cardiac Rehabilitation after Primary Coronary Intervention
Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)?
 or Coronary Artery Bypass Graft Surgery (CABG)?") Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Supporting patients after a heart attack: In hospital In primary care In the community National Heart Foundation of Australia
 Supporting patients after a heart attack: In hospital In primary care In the community Your requests Action plans Information on medicines Stents Follow-up protocols Setting the scene: Mr Charlie Brown
Supporting patients after a heart attack: In hospital In primary care In the community Your requests Action plans Information on medicines Stents Follow-up protocols Setting the scene: Mr Charlie Brown
Can Angioplasty Improve Quality of Life for CAD Patients?
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/can-angioplasty-improve-quality-of-life-for-cadpatients/4000/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/can-angioplasty-improve-quality-of-life-for-cadpatients/4000/
Is it ever too late for cardiovascular prevention and rehabilitation? Prof. Dr. Helmut Gohlke Herz-Zentrum Bad Krozingen, Germany
 Is it ever too late for cardiovascular prevention and rehabilitation? Prof. Dr. Helmut Gohlke Herz-Zentrum Bad Krozingen, Germany The demographic issue Life expectancy is increasing Patients are getting
Is it ever too late for cardiovascular prevention and rehabilitation? Prof. Dr. Helmut Gohlke Herz-Zentrum Bad Krozingen, Germany The demographic issue Life expectancy is increasing Patients are getting
Atherosclerosis Your quick guide
 Atherosclerosis Your quick guide Coronary heart disease is the UK s single biggest killer. For over 50 years we ve pioneered research that s transformed the lives of people living with heart and circulatory
Atherosclerosis Your quick guide Coronary heart disease is the UK s single biggest killer. For over 50 years we ve pioneered research that s transformed the lives of people living with heart and circulatory
Nurse-led Rapid Access Chest Pain Clinic at the Royal Glamorgan Hospital. by Sharon Cassidy/Andrea Gasson
 Nurse-led Rapid Access Chest Pain Clinic at the Royal Glamorgan Hospital by Sharon Cassidy/Andrea Gasson The team consists of :-: Cardiology nurse specialist Sharon Cassidy Part time clinic administrator
Nurse-led Rapid Access Chest Pain Clinic at the Royal Glamorgan Hospital by Sharon Cassidy/Andrea Gasson The team consists of :-: Cardiology nurse specialist Sharon Cassidy Part time clinic administrator
What do the guidelines say?
 Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
More honoured in the breach
 More honoured in the breach.. Bob Lewin CAREARE AND EDUCATION RESEARCH GROUPROUP Cardiac rehabilitation around the world (apart from Austria) is in a mess Austria 1997 90% Holland 60% UK 40% (of angio,,
More honoured in the breach.. Bob Lewin CAREARE AND EDUCATION RESEARCH GROUPROUP Cardiac rehabilitation around the world (apart from Austria) is in a mess Austria 1997 90% Holland 60% UK 40% (of angio,,
Management of the coronary patient in Roberto Ferrari
 Management of the coronary patient in 2011 Roberto Ferrari What is new in treatment of stable CAD? In the era of interventional cardiology, is chronic stable angina a rare disease? Stable angina pectoris
Management of the coronary patient in 2011 Roberto Ferrari What is new in treatment of stable CAD? In the era of interventional cardiology, is chronic stable angina a rare disease? Stable angina pectoris
Women and Vascular Disease
 Women and Vascular Disease KEVIN F. REBECK PA-C VASCULAR TRANSPLANT SURGERY 1 The Scope of the Problem One woman dies every minute from cardiovascular disease in the U.S.! The Scope of the Problem CVD
Women and Vascular Disease KEVIN F. REBECK PA-C VASCULAR TRANSPLANT SURGERY 1 The Scope of the Problem One woman dies every minute from cardiovascular disease in the U.S.! The Scope of the Problem CVD
Diagnosis of CAD S Richard Underwood
 Diagnosis of CAD S Richard Underwood Professor of Cardiac Imaging Royal Brompton Hospital & Imperial College Faculty of Medicine London, UK The history and diagnosis 89% Non-cardiac chest pain 50% Atypical
Diagnosis of CAD S Richard Underwood Professor of Cardiac Imaging Royal Brompton Hospital & Imperial College Faculty of Medicine London, UK The history and diagnosis 89% Non-cardiac chest pain 50% Atypical
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why?
 Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
Stable Angina. An information guide
 TO PROVIDE THE VERY BEST CARE FOR EACH PATIENT ON EVERY OCCASION Stable Angina An information guide Stable Angina About Angina Angina is a condition where people experience chest, stomach, jaw or arm pain
TO PROVIDE THE VERY BEST CARE FOR EACH PATIENT ON EVERY OCCASION Stable Angina An information guide Stable Angina About Angina Angina is a condition where people experience chest, stomach, jaw or arm pain
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
Chest Pain. Dr Robert Huggett Consultant Cardiologist
 Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Heart Attack Your quick guide
 Heart Attack Your quick guide Coronary heart disease is the UK s single biggest killer. For over 50 years we ve pioneered research that s transformed the lives of people living with heart and circulatory
Heart Attack Your quick guide Coronary heart disease is the UK s single biggest killer. For over 50 years we ve pioneered research that s transformed the lives of people living with heart and circulatory
How to successfully manage patients with ischemic heart disease
 Cardiology Update 2013 Satellite symposium A. Menarini Davos, February 14, 2013 How to successfully manage patients with ischemic heart disease François Mach Cardiology Department Geneva University Hospital
Cardiology Update 2013 Satellite symposium A. Menarini Davos, February 14, 2013 How to successfully manage patients with ischemic heart disease François Mach Cardiology Department Geneva University Hospital
Patient characteristics Intervention Comparison Length of followup
 ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
NHS QIS National Measurement of Audit Acute Coronary Syndrome
 NHS QIS National Measurement of Audit Acute Coronary Syndrome Things have changed based on the experience and feedback from the first cycle of measurement and, for the better we think! The Acute Coronary
NHS QIS National Measurement of Audit Acute Coronary Syndrome Things have changed based on the experience and feedback from the first cycle of measurement and, for the better we think! The Acute Coronary
DECISION - CTO. optimal Medical Treatment in patients with. Seung-Jung Park, MD, PhD, FACC for the DECISION-CTO Study investigators
 DECISION - CTO Drug-Eluting stent Implantation versus optimal Medical Treatment in patients with ChronIc Total OccluSION Seung-Jung Park, MD, PhD, FACC for the DECISION-CTO Study investigators Asan Medical
DECISION - CTO Drug-Eluting stent Implantation versus optimal Medical Treatment in patients with ChronIc Total OccluSION Seung-Jung Park, MD, PhD, FACC for the DECISION-CTO Study investigators Asan Medical
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW
 PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
Commissioning for value focus pack
 Commissioning for value focus pack Clinical commissioning group: NHS MILTON KEYNES CCG Focus area: Cardiovascular disease (CVD) pathway Version 2 June 2014 Contents 1. Background and context About the
Commissioning for value focus pack Clinical commissioning group: NHS MILTON KEYNES CCG Focus area: Cardiovascular disease (CVD) pathway Version 2 June 2014 Contents 1. Background and context About the
Maria Angela S. Cruz-Anacleto, MD
 Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
CASE from South Korea
 CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
Post Operative Troponin Leak: David Smyth Christchurch New Zealand
 Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Vorapaxar for the secondary prevention of atherothrombotic events after myocardial infarction Draft scope (pre-referral)
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Vorapaxar for the secondary prevention of atherothrombotic events after myocardial infarction Draft scope (pre-referral)
Cardiovascular risk factor appraisal art or science?
 Cardiovascular risk factor appraisal art or science? Prof. Philip MacCarthy BSc MBChB (Hons) PhD FRCP Consultant Cardiologist Bupa Cromwell Hospital Clinics: Wednesday & Friday PM/Evening What are we trying
Cardiovascular risk factor appraisal art or science? Prof. Philip MacCarthy BSc MBChB (Hons) PhD FRCP Consultant Cardiologist Bupa Cromwell Hospital Clinics: Wednesday & Friday PM/Evening What are we trying
How to Report Effectively on a Nuclear Cardiology Study
 How to Report Effectively on a Nuclear Cardiology Study A/Prof. NATHAN BETTER Cardiologist and Deputy Director of Nuclear Medicine Royal Melbourne Hospital University of Melbourne December 2012 The case
How to Report Effectively on a Nuclear Cardiology Study A/Prof. NATHAN BETTER Cardiologist and Deputy Director of Nuclear Medicine Royal Melbourne Hospital University of Melbourne December 2012 The case
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
TRANSPARENCY COMMITTEE OPINION. 4 November 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 4 November 2009 RANEXA 375 mg extended release tablet Pack of 60 (CIP: 394 370-7) RANEXA 500 mg extended release tablet
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 4 November 2009 RANEXA 375 mg extended release tablet Pack of 60 (CIP: 394 370-7) RANEXA 500 mg extended release tablet
ICD deactivation Patient Journey
 ICD deactivation Patient Journey Julia decourcey Consultant Nurse Kings College Hospital 05.05.10 Internal Cardiac Defibrillator Used in pts at high risk of sudden cardiac death ie EF > 30% Previous survivor
ICD deactivation Patient Journey Julia decourcey Consultant Nurse Kings College Hospital 05.05.10 Internal Cardiac Defibrillator Used in pts at high risk of sudden cardiac death ie EF > 30% Previous survivor
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
CARDIAC REHABILITATION PROGRAMME:- MEDICATION
 CARDIAC REHABILITATION PROGRAMME:- MEDICATION AIM OF THIS SESSION Understand the reasons for taking your medications, Discuss the common side effects associated with these medications - knowing when to
CARDIAC REHABILITATION PROGRAMME:- MEDICATION AIM OF THIS SESSION Understand the reasons for taking your medications, Discuss the common side effects associated with these medications - knowing when to
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Coronary Artery Disease
 Coronary Artery Disease This information is at http://www.nhlbi.nih.gov/health/dci/diseases/cad/cad_all.html and is provided by the NHLBI, one of the Institutes of the National Institutes of Health. To
Coronary Artery Disease This information is at http://www.nhlbi.nih.gov/health/dci/diseases/cad/cad_all.html and is provided by the NHLBI, one of the Institutes of the National Institutes of Health. To
By: Diamond Fernandes BSc, ACSM CES, CSCS To learn more about the author, click below
 By: Diamond Fernandes BSc, ACSM CES, CSCS To learn more about the author, click below http://heartfitclinic.com/diamond-fernandes Special Report The Truth About Heart Tests (Myocardial Perfusion Scans)
By: Diamond Fernandes BSc, ACSM CES, CSCS To learn more about the author, click below http://heartfitclinic.com/diamond-fernandes Special Report The Truth About Heart Tests (Myocardial Perfusion Scans)
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
James M. Kirshenbaum, MD, FACC
 James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
7/27/2017 DISCLOSURES OUTPATIENT MANAGEMENT QUESTION #1 FEATURES OF THIS TALK OF CAD- A PRIMARY CARE PERSPECTIVE
 DISCLOSURES OUTPATIENT MANAGEMENT OF CAD- A PRIMARY CARE PERSPECTIVE I am on the Scientific Advisory Boards with stock option compensation for the following companies: TAI Diagnostics Cricket Health, Inc.
DISCLOSURES OUTPATIENT MANAGEMENT OF CAD- A PRIMARY CARE PERSPECTIVE I am on the Scientific Advisory Boards with stock option compensation for the following companies: TAI Diagnostics Cricket Health, Inc.
Revascularization In HFrEF: Are We Close To The Truth. Ali Almasood
 Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Sheffield guidelines for the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017)
") Sheffield guidelines f the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017) Approved by Sheffield Area Prescribing Committee and Sheffield Teaching Hospitals
Sheffield guidelines f the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017) Approved by Sheffield Area Prescribing Committee and Sheffield Teaching Hospitals
FEATURES OF THIS TALK
 FEATURES OF THIS TALK OUTPATIENT MANAGEMENT OF CAD- A PRIMARY CARE PERSPECTIVE Michael G. Shlipak, MD, MPH Professor of Medicine, Biostatistics, and Epidemiology Chief, General Internal Medicine Covers
FEATURES OF THIS TALK OUTPATIENT MANAGEMENT OF CAD- A PRIMARY CARE PERSPECTIVE Michael G. Shlipak, MD, MPH Professor of Medicine, Biostatistics, and Epidemiology Chief, General Internal Medicine Covers
Debate Should we use FFR? I will say NO.
 Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
FFR in Multivessel Disease
 FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
Percutaneous coronary intervention (angioplasty) +/- rotablation
 +/- rotablation") PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label Why do I need this procedure? If you are coming into hospital for a cardiac procedure
PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label Why do I need this procedure? If you are coming into hospital for a cardiac procedure
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation?
 What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation? Keun-Ho Park, Myung Ho Jeong, Min Goo Lee, Jum Suk Ko,
What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation? Keun-Ho Park, Myung Ho Jeong, Min Goo Lee, Jum Suk Ko,
Cardiology. Self Learning Package. Module 5: Pharmacology: Treatment of Acute Coronary. Prevention
 Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Long-Term Management Of the ACS Patient: State-of-the-Art. Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA
 Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery. Christian Seiler No conflict of interest to declare.
 Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery Christian Seiler No conflict of interest to declare PCI Long-Term Outcome Perioperative Management After Coronary Stenting:
Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery Christian Seiler No conflict of interest to declare PCI Long-Term Outcome Perioperative Management After Coronary Stenting:
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
2/17/2010. Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco
 Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
Stable angina: current guidelines and advances in management
 DRUG REVIEW n Stable angina: current guidelines and advances in management Anoop Shah MRCP and Keith Fox FRCP Our Drug Review discusses the current recommended management of stable angina, focussing on
DRUG REVIEW n Stable angina: current guidelines and advances in management Anoop Shah MRCP and Keith Fox FRCP Our Drug Review discusses the current recommended management of stable angina, focussing on
Physician Self-referral and Health Care Utilization. Rita F. Redberg, MD, MSc Professor of Medicine UCSF Medical Center
 Physician Self-referral and Health Care Utilization Rita F. Redberg, MD, MSc Professor of Medicine UCSF Medical Center Physician self-referral why should we care? Extent of occurrences Impact of physician
Physician Self-referral and Health Care Utilization Rita F. Redberg, MD, MSc Professor of Medicine UCSF Medical Center Physician self-referral why should we care? Extent of occurrences Impact of physician