How to deal with hypotension on dialysis? CME Basics in Nephrology SGN-SSN Interlaken 2016
|
|
|
- Suzan Simon
- 5 years ago
- Views:
Transcription
1 How to deal with hypotension on dialysis? CME Basics in Nephrology SGN-SSN Interlaken 2016 PD Dr. med. Andreas Kistler Leitender Arzt Nephrologie und Dialyse Kantonsspital Frauenfeld
2 Intradialytic hypotension is a frequent problem......yet there is no simple solution to it......and the evidence-base for most preventive measures is scarce. 2
3 Mr. Ivo Dieter Höfler (I.D.H.) 68 yo male patient with DNP on HD for 4y with a number of comorbidities... Diabetic retinopathy Ischemic heart disease (nstemi 6y ago) Peripheral arterial disease Right calf amputee for infected diabetic ulcer Obesity (BMI 33) 3
4 Mr. Ivo Dieter Höfler (I.D.H.) Time BP 13:05 152/68 13:10 146/65 13:40 139/67 14:10 126/61 14:40 128/59 15:10 125/60 15:40 103/61 15:45 99/56 15:48 93/54 15:53 114/63 16:02 108/60 15:17 112/62 16:32 109/60 16:47 113/63 lightheaded, nausea 4
5 Does this patient have intradialytic hypotension? Yes No Don t know It depends 5
6 Why bother about IDH? Because of the annoying alarms Because it causes dyscomfort to the patient Because the nurse asks me to change the prescription Because it negatively affects dialysis efficacy All of the above All of the above plus......because of the consequences of IDH 6
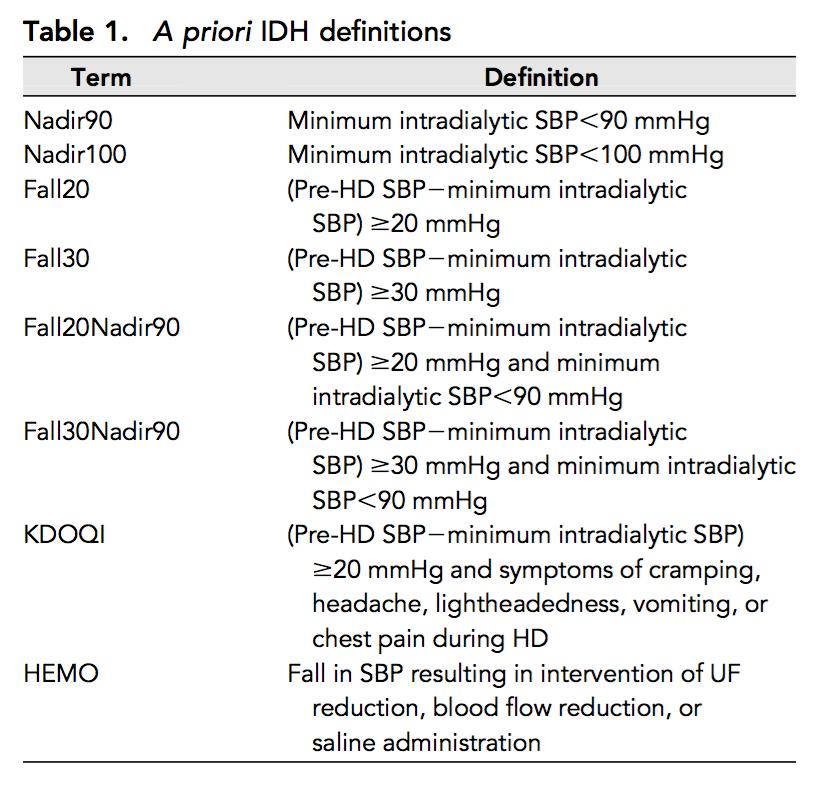
7 Definition of IDH KDOQI: decrease in systolic blood pressure by 20 mmhg or MAP by 10 mmhg associated with symptoms that include: abdominal discomfort; yawning; sighing; nausea; vomiting; muscle cramps; restlessness; dizziness or fainting; and anxiety HEMO: Fall in BP resulting in intervention of UF reduction, bood flow reduction or saline administration EBPG guidelines on hemodynamic instability:...no evidence based recommendation regarding the definition of IDH can be given...both a reduction in BP, as well as clinical symptoms with need for nursing intervention should be present in order to accept the presence of IDH Many different definitions in different studies... 7
8 8
9 9
10 Does this patient have intradialytic hypotension? Yes No Don t know It depends...on the definition 10
11 Mr. Ivo Dieter Höfler (I.D.H.) Time BP 13:05 152/68 13:10 146/65 13:40 139/67 14:10 126/61 14:40 128/59 15:10 125/60 15:40 103/61 15:45 87/48 15:48 89/54 15:53 114/63 16:02 108/60 15:17 112/62 16:32 109/60 16:47 113/63 lightheaded, nausea 11
12 Why bother about IDH? Because of the annoying alarms Because it causes dyscomfort to the patient Because the nurse asks me to change the prescription Because it negatively affects dialysis efficacy All of the above All of the above plus......because of the consequences of IDH 12
13 Pathophysiology Fluid removal Reduction of intravascular volume vascular refilling vasoconstriction Maintenance of Blood pressure cardiac response 13
14 low RRF IDWG High salt and fluid intake Medications Vascular calcification Autonomic dysfunction Eating (splanchnic pooling) Dialysate temperature Endotoxins Target weight too low Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling Dialysate composition Anemia Low albumin Ischemic heart disease Hypertensive cardiopathy Myocardial stunning Systolic and diastolic dysfunction impaired vasoconstriction IDH Impaired cardiac response 14
15 Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling impaired vasoconstriction IDH Impaired cardiac response 15
16 Consequences of IDH Mortality Access thrombosis Inadequate dialysis Organ hypoperfusion brain heart gut Kidneys (RRF) 16
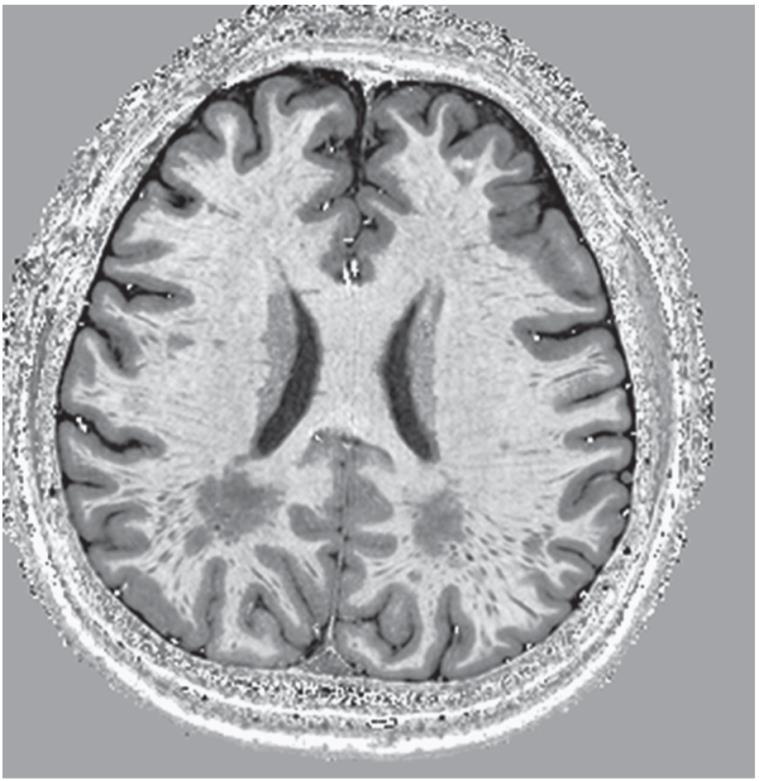
17 Consequences of IDH: brain 17
18 Consequences of IDH: heart 18
19 Consequences of IDH: heart 19
20 Gut and beyond: endotoxinemia 20
21 low RRF IDWG High salt and fluid intake Medications Vascular calcification Autonomic dysfunction Eating (splanchnic pooling) Dialysate temperature Endotoxins Target weight too low Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling Dialysate composition Anemia Low albumin Ischemic heart disease Hypertensive cardiopathy Myocardial stunning Systolic and diastolic dysfunction impaired vasoconstriction IDH Impaired cardiac response 21
22 How to deal with IDH? Acute management Preventive measures 22
23 Mr. Ivo Dieter Höfler (I.D.H.) Before calling you, the nurse reacted to the hypotensive episode by: Stopping ultrafiltration Placing the patient in Trendelenburg position Slowig blood flow rate to 100ml/min Infusing a bolus of 250ml substituate Did she react correclty? 23
24 Mr. Ivo Dieter Höfler (I.D.H.) Before calling you, the nurse reacted to the hypotensive episode by: Stopping ultrafiltration Placing the patient in Trendelenburg position Slowig blood flow rate to 100ml/min Infusing a bolus of 250ml substituate Oxygen! 24
25 Why is blood flow often lowered with IDH? Misconception that access flow depends on dialyzer blood flow In parallel plate dialyzers, extracorporeal blood volume depended on blood flow BF reduction lowered TMP and hence UF rate in the era before UF control was standard BF reduction reduced acetate delivery to the patient in the era of acetate buffering With cuprophane membranes, slowing BF reduced contact to the bio-incompatible, complement activating membrane When higher dialysate temperatures and lower dialysate Na were standart, a reduction of BF lowered temperature and increased Na of blood returning to the patient 25
26 What actions will you take at this point? You raise the dialysis Na concentration in the prescription You raise the target weight by 1 kg You raise the target weight if there is no edema You adjust dry weight depending of BCM results You tell the patient to drink less You limit the ultrafiltration rate to 10ml/h/kg You stop antihypertensives before dialysis You prescribe Midodrine (Gutron) 10 drops before dialysis 26
27 low RRF IDWG High salt and fluid intake Medications Vascular calcification Autonomic dysfunction Eating (splanchnic pooling) Dialysate temperature Endotoxins Target weight too low Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling Dialysate composition Anemia Low albumin Ischemic heart disease Hypertensive cardiopathy Myocardial stunning Systolic and diastolic dysfunction impaired vasoconstriction IDH Impaired cardiac response 27
28 Dry weight the lowest tolerated postdialysis weight achieved via gradual change in postdialysis weight at which there are minimal signs or symptoms of hypovolemia or hypervolemia Agarwal and Singh 28
29 All-cause mortality Cardiovascular mortality 29
30 How to assess dry weight? Clinical assessment 30
31 31

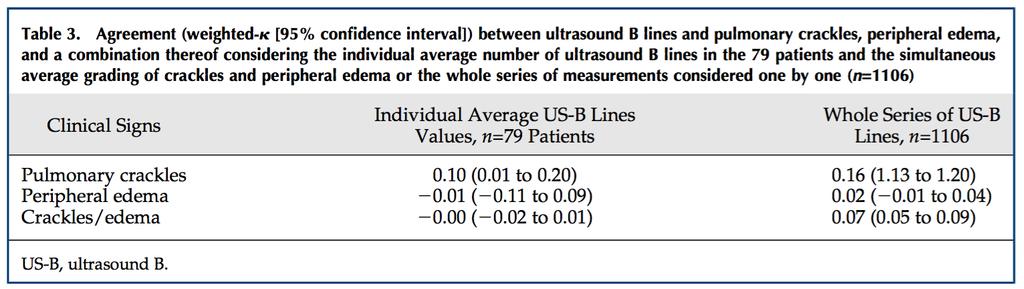
32 How to assess dry weight? Clinical assessment Lung ultrasound 32
33 How to assess dry weight? Clinical assessment Lung ultrasound Chest X-ray 33
34 How to assess dry weight? Clinical assessment Lung ultrasound Chest X-ray Inferior vena cava ultrasound 34
35 How to assess dry weight? Clinical assessment Lung ultrasound Chest X-ray Inferior vena cava ultrasound Bioimpedance 35

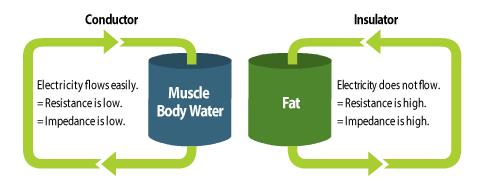


36 Bioimpedance 36
37 BCM-guided treatment and outcomes 37
38 How to assess dry weight? Clinical assessment Lung ultrasound Chest X-ray Inferior vena cava ultrasound Bioimpedance Online blood volume monitoring 38

39 Blood volume monitoring 39
40 Blood volume monitoring Nesrallah, ASAIO Journal 2008; 54:

41 Blood volume monitoring Nesrallah, ASAIO Journal 2008; 54:
42 Assessment of dry weight will usually rely on a combination of clinical assessment, history taking, technical tools as available and some trial and error 42
43 low RRF IDWG High salt and fluid intake Medications Vascular calcification Autonomic dysfunction Eating (splanchnic pooling) Dialysate temperature Endotoxins Target weight too low Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling Dialysate composition Anemia Low albumin Ischemic heart disease Hypertensive cardiopathy Myocardial stunning Systolic and diastolic dysfunction impaired vasoconstriction IDH Impaired cardiac response 43
44 low RRF IDWG High salt and fluid intake Medications Vascular calcification Autonomic dysfunction Eating (splanchnic pooling) Dialysate temperature Endotoxins Target weight too low Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling Dialysate composition Anemia Low albumin Ischemic heart disease Hypertensive cardiopathy Myocardial stunning Systolic and diastolic dysfunction impaired vasoconstriction IDH Impaired cardiac response 44
45 200ml x 3 = 600ml 45
46 46
47 47
48 low RRF IDWG High salt and fluid intake Medications Vascular calcification Autonomic dysfunction Eating (splanchnic pooling) Dialysate temperature Endotoxins Target weight too low Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling Dialysate composition Anemia Low albumin Ischemic heart disease Hypertensive cardiopathy Myocardial stunning Systolic and diastolic dysfunction impaired vasoconstriction IDH Impaired cardiac response 48
49 Dialysate composition (Acetate) Na + Ca 2+ Mg 2+ 49
50 Dialysate composition (Acetate) Na + Ca 2+ Mg 2+ Acute effect: - hemodynamic stability Chronic effect: - Na loading - Thirst - Higher IDWG 50
51 Endpoint: IDH Advantage only for stepwise profiling Considerable heterogeneity of studies 51
52 low RRF IDWG High salt and fluid intake Medications Vascular calcification Autonomic dysfunction Eating (splanchnic pooling) Dialysate temperature Endotoxins Target weight too low Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling Dialysate composition Anemia Low albumin Ischemic heart disease Hypertensive cardiopathy Myocardial stunning Systolic and diastolic dysfunction impaired vasoconstriction IDH Impaired cardiac response 52
53 low RRF IDWG High salt and fluid intake Medications Vascular calcification Autonomic dysfunction Eating (splanchnic pooling) Dialysate temperature Endotoxins Target weight too low Excessive fluid removal Reduction of intravascular volume Impaired vascular refilling Dialysate composition Anemia Low albumin Ischemic heart disease Hypertensive cardiopathy Myocardial stunning Systolic and diastolic dysfunction impaired vasoconstriction IDH Impaired cardiac response 53

54 Eating on HD Eating before or during HD should be discouraged in IHD prone patients But consider the risk of malnutrition! 54
55 Dialysate temperature 55
56 56
57 Medication review Aspirin cardio 100mg Calcitriol 0.5mcg Ca-acetate 400mg Sevelamer 800mg Fluvstatin 80mg Bisoprolol 5mg Losartan 100mg Amlodipin 10mg Doxazosin 4mg Insulin Special Scheme Gabapentin 300mg After Dialysis 57
58 Blood pressure in HD patients IDH is just part of the story......we measure BP only during 12 of 168 hours Consider orthostatic effects (particularly in DM) We have to make many trade offs when treating HD patients... Consider pharmacokinetics of antihypertensive medications! 58
59 59
60 Medication adjustments: suggestion Aspirin cardio 100mg Calcitriol 0.5mcg Ca-acetate 400mg Sevelamer 800mg Fluvstatin 80mg Bisoprolol 5mg Lisinopril 10mg Amlodipin 10mg Doxazosin 4mg (0-0-1 on HD days) Insulin Special Scheme Gabapentin 300mg After Dialysis 60

61 10mg = 30 drops Midodrine, low temperature dialysate or both 61
62 What actions will you take at this point? You raise the dialysis Na concentration in the prescription You raise the target weight by 1 kg You raise the target weight if there is no edema You adjust dry weight depending of BCM results You tell the patient to drink less You limit the ultrafiltration rate to 10ml/h/kg You stop antihypertensives before dialysis You prescribe Midodrine (Gutron) 10 drops before dialysis 62
63 Summary: how to deal with IDH? First line interventions: Reassess target weight But don t rely on clinical signs of hypervolemia only! Review and adjust antihypertensive agents But keep in mind BP between dialyses! Try to lower IDWG Max out diuretics if RRF Salt restriction No eating during dialysis 63
64 Summary: how to deal with IDH? Second line interventions: Assess for cardiac disease Cool dialysate Consider Na profiling Consider online blood volume measurement Consider HDF Consider Midodrine Consider longer dialysis time 64
65 Summary: how to deal with IDH? Third line interventions: Consider frequent HD (some consider it first line, but ask the patient and the SVK...) Consider modality change 65
66 Questions? 66
02/28/2018. To reduce morbidity, mortality and treatment loss associated with chronic volume overload in hemodialysis patients
 Lisa Koester Renal Nurse Practitioner Washington University School of Medicine St. Louis, MO To reduce morbidity, mortality and treatment loss associated with chronic volume overload in hemodialysis patients
Lisa Koester Renal Nurse Practitioner Washington University School of Medicine St. Louis, MO To reduce morbidity, mortality and treatment loss associated with chronic volume overload in hemodialysis patients
THE INTRADIALYTIC BIOFEEDBACKS AND THE CARDIOVASCULAR STABILITY IN HYPOTENSION- PRONE PATIENTS Antonio Santoro, Bologna, Italy
 THE INTRADIALYTIC BIOFEEDBACKS AND THE CARDIOVASCULAR STABILITY IN HYPOTENSION- PRONE PATIENTS Antonio Santoro, Bologna, Italy Chair: Walter H. Hörl, Vienna, Austria Wojciech Zaluska, Lublin, Poland Prof.
THE INTRADIALYTIC BIOFEEDBACKS AND THE CARDIOVASCULAR STABILITY IN HYPOTENSION- PRONE PATIENTS Antonio Santoro, Bologna, Italy Chair: Walter H. Hörl, Vienna, Austria Wojciech Zaluska, Lublin, Poland Prof.
DEFINITIONS FOR FLUID STATUS & TARGET WEIGHT
 Home Dialysis Interest Group HEALTHCARE TEAM TOOL DEFINITIONS FOR STATUS & TARGET WEIGHT BALANCED EXCESS DEFICIT Illustrations provided by: 1 BALANCE OF THE HOME HEMODIALYSIS PATIENT Dialysis Weight**
Home Dialysis Interest Group HEALTHCARE TEAM TOOL DEFINITIONS FOR STATUS & TARGET WEIGHT BALANCED EXCESS DEFICIT Illustrations provided by: 1 BALANCE OF THE HOME HEMODIALYSIS PATIENT Dialysis Weight**
FLUID MANAGEMENT IN DIALYSIS: STRATEGIES FOR SUCCESS
 FLUID MANAGEMENT IN DIALYSIS: STRATEGIES FOR SUCCESS Quality Insights Renal Network 3 October 2, 2014 Laura D. Byham-Gray, PhD, RD Professor & Director Master of Science in Clinical Nutrition Rutgers University
FLUID MANAGEMENT IN DIALYSIS: STRATEGIES FOR SUCCESS Quality Insights Renal Network 3 October 2, 2014 Laura D. Byham-Gray, PhD, RD Professor & Director Master of Science in Clinical Nutrition Rutgers University
However, Adverse Events Do Still Occur During Dialysis, Which May Be Because Of Technical Problems With The Extracorporeal Treatment, Often Combined W
 Incidence of Intradialytic Hypotension in Patients on Hemodialysis in Al Kindy Teaching Hospital Dr. *Consultant Physician Nephrologist/Head Of Faculty Of Medicine/Al Kindy College Of Medicine Abstract
Incidence of Intradialytic Hypotension in Patients on Hemodialysis in Al Kindy Teaching Hospital Dr. *Consultant Physician Nephrologist/Head Of Faculty Of Medicine/Al Kindy College Of Medicine Abstract
Sodium elimination and dialysate sodium. How much? Does it matter?
 Sodium elimination and dialysate sodium How much? Does it matter? A. Bock Nephrologie Dialysis visit Aarau 3.12.2013 90 kg dialysis patient: 5 kg over dry weight Recent dyspnea. Minimal leg edema RBV in
Sodium elimination and dialysate sodium How much? Does it matter? A. Bock Nephrologie Dialysis visit Aarau 3.12.2013 90 kg dialysis patient: 5 kg over dry weight Recent dyspnea. Minimal leg edema RBV in
Striking the Optimal Balance in
 Not Too fast, Not Too Slow: Striking the Optimal Balance in Hemodialysis Fluid Management ANNA/ IPRO Spring Symposium May 24, 2018 Jennifer E. Flythe, MD, MPH Assistant Professor of Medicine University
Not Too fast, Not Too Slow: Striking the Optimal Balance in Hemodialysis Fluid Management ANNA/ IPRO Spring Symposium May 24, 2018 Jennifer E. Flythe, MD, MPH Assistant Professor of Medicine University
St George Hospital Renal Department: INTERNAL ONLY
 HYPOTENSION AND HAEMODIALYSIS THE BOTTOM LINE 1. Prevention of hypotension during haemodialysis (IDH) 2. Treatment of hypotension during haemodialysis (IDH) 3. Withholding dialysis when SBP
HYPOTENSION AND HAEMODIALYSIS THE BOTTOM LINE 1. Prevention of hypotension during haemodialysis (IDH) 2. Treatment of hypotension during haemodialysis (IDH) 3. Withholding dialysis when SBP
Achieving Equilibrium in ESRD Patients
 Achieving Equilibrium in ESRD Patients -Marc Richards MD -South Florida Kidney Disease and HTN Specialists -Chief of Medicine, BRRH -BRRH Grand Rounds: April 18 th, 2017 Outline Dialysis prescription Adequacy
Achieving Equilibrium in ESRD Patients -Marc Richards MD -South Florida Kidney Disease and HTN Specialists -Chief of Medicine, BRRH -BRRH Grand Rounds: April 18 th, 2017 Outline Dialysis prescription Adequacy
Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University
 Hypertension in Hemodialysis Patient Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University Mechanism of HTN in HD patients Volume-dependent HTN ECV expansion. Volume-independent HTN
Hypertension in Hemodialysis Patient Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University Mechanism of HTN in HD patients Volume-dependent HTN ECV expansion. Volume-independent HTN
Low Blood Pressure During Dialysis (Intradialytic Hypotension (IDH))
)") Low Blood Pressure During Dialysis (Intradialytic Hypotension (IDH)) By Dori Schatell, Medical Education Institute One of the main jobs of dialysis is to remove excess water from your body. Seems pretty
Low Blood Pressure During Dialysis (Intradialytic Hypotension (IDH)) By Dori Schatell, Medical Education Institute One of the main jobs of dialysis is to remove excess water from your body. Seems pretty
Challenges to Manage Blood Pressure in ESRD and Heart Failure Patients
 Challenges to Manage Blood Pressure in ESRD and Heart Failure Patients Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health San Antonio 2nd Annual Cardiorenal Connections Meeting, April 28,
Challenges to Manage Blood Pressure in ESRD and Heart Failure Patients Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health San Antonio 2nd Annual Cardiorenal Connections Meeting, April 28,
Hemocontrol. Management of Intradialytic Hypotension
 Hemocontrol Management of Intradialytic Hypotension Dialysis Complications Cramps 31% Headache 18% Vomiting 1% Nephrologische Praxen Rostock 1998-1999 Dialysis n=6,508 Hypotension 50% BP = CO X SVR Potential
Hemocontrol Management of Intradialytic Hypotension Dialysis Complications Cramps 31% Headache 18% Vomiting 1% Nephrologische Praxen Rostock 1998-1999 Dialysis n=6,508 Hypotension 50% BP = CO X SVR Potential
Volume control in maintenance hemodialysis: how to keep your patient dry? Dr. Luc Radermacher
 Volume control in maintenance hemodialysis: how to keep your patient dry? Dr. Luc Radermacher Fluid balance in HD Weight HD HD HD Hypervolaemia DW Euvolaemia Hypovolaemia Mo Tu We Th Fr Sa Su Mo Chonic
Volume control in maintenance hemodialysis: how to keep your patient dry? Dr. Luc Radermacher Fluid balance in HD Weight HD HD HD Hypervolaemia DW Euvolaemia Hypovolaemia Mo Tu We Th Fr Sa Su Mo Chonic
Understanding Kt/V and Volume Control
 Understanding Kt/V and Volume Control Its practical use to determine dialysis and improve outcomes Caroline Williams RD May 23, 2017 Volume Control in Dialysis Patients Pathogenesis In the 1960s and early
Understanding Kt/V and Volume Control Its practical use to determine dialysis and improve outcomes Caroline Williams RD May 23, 2017 Volume Control in Dialysis Patients Pathogenesis In the 1960s and early
Strategies to assess and manage hypervolemia The invisible threat in dialysis
 Strategies to assess and manage hypervolemia The invisible threat in dialysis Rajiv Agarwal MD Professor of Medicine, Indiana University School of Medicine Volume excess is common and costly. Admission
Strategies to assess and manage hypervolemia The invisible threat in dialysis Rajiv Agarwal MD Professor of Medicine, Indiana University School of Medicine Volume excess is common and costly. Admission
Innovations in Cardio/Renal Patient Care. Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health at San Antonio Spring Symposium 2018
 Innovations in Cardio/Renal Patient Care Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health at San Antonio Spring Symposium 2018 Percent of Patients CVD = cardiovascular disease; ASHD =
Innovations in Cardio/Renal Patient Care Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health at San Antonio Spring Symposium 2018 Percent of Patients CVD = cardiovascular disease; ASHD =
UNIVERSITY OF CALGARY. Blood Volume Monitoring Guided Ultrafiltration Biofeedback on the Reduction of
 UNIVERSITY OF CALGARY Blood Volume Monitoring Guided Ultrafiltration Biofeedback on the Reduction of Intradialytic Hypotensive Episodes in Hemodialysis by Kelvin Cheuk-Wai Leung A THESIS SUBMITTED TO THE
UNIVERSITY OF CALGARY Blood Volume Monitoring Guided Ultrafiltration Biofeedback on the Reduction of Intradialytic Hypotensive Episodes in Hemodialysis by Kelvin Cheuk-Wai Leung A THESIS SUBMITTED TO THE
Get Healthy Stay Healthy
 Hypertension Management WHAT IS HYPERTENSION (HIGH BLOOD PRESSURE)? Blood pressure is a measure of how hard the blood pushes against the walls of your arteries as it moves through your body. It is normal
Hypertension Management WHAT IS HYPERTENSION (HIGH BLOOD PRESSURE)? Blood pressure is a measure of how hard the blood pushes against the walls of your arteries as it moves through your body. It is normal
Crit-Line Monitor. Frequently Asked Questions
 Crit-Line Monitor Frequently Asked Questions Crit-Line Monitor Frequently Asked Questions 1 What is the indication for use of the Crit-Line monitor? The Crit-Line Monitor III is used to non-invasively
Crit-Line Monitor Frequently Asked Questions Crit-Line Monitor Frequently Asked Questions 1 What is the indication for use of the Crit-Line monitor? The Crit-Line Monitor III is used to non-invasively
There are no shortcuts to Dialysis
 There are no shortcuts to Dialysis 1 Outcomes John Sweeny Wednesday, March 21 st, 2018 (3:10 pm 4:10 pm) 2 Quality in Hemodialysis Quality Health Care is the degree to which health services increases the
There are no shortcuts to Dialysis 1 Outcomes John Sweeny Wednesday, March 21 st, 2018 (3:10 pm 4:10 pm) 2 Quality in Hemodialysis Quality Health Care is the degree to which health services increases the
RJ Picciano BA, CHT, OCDT, CHBT Fluid Management Coordinator Centers for Dialysis Care, Cleveland Ohio BONENT President
 FLUID MANAGEMENT: WHAT THE NEPHROLOGY TECHNICIAN CAN DO TO HELP? RJ Picciano BA, CHT, OCDT, CHBT Fluid Management Coordinator Centers for Dialysis Care, Cleveland Ohio BONENT President Lori Poole MSN,
FLUID MANAGEMENT: WHAT THE NEPHROLOGY TECHNICIAN CAN DO TO HELP? RJ Picciano BA, CHT, OCDT, CHBT Fluid Management Coordinator Centers for Dialysis Care, Cleveland Ohio BONENT President Lori Poole MSN,
Assessment of dry weight by monitoring changes in blood volume during hemodialysis using Crit-Line
 Kidney International, Vol. 68 (25), pp. 854 861 Assessment of dry weight by monitoring changes in blood volume during hemodialysis using Crit-Line HECTOR J. RODRIGUEZ,REGINA DOMENICI,ANNE DIROLL, and IRINA
Kidney International, Vol. 68 (25), pp. 854 861 Assessment of dry weight by monitoring changes in blood volume during hemodialysis using Crit-Line HECTOR J. RODRIGUEZ,REGINA DOMENICI,ANNE DIROLL, and IRINA
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Hypertension AN OVERVIEW
 AN OVERVIEW Hypertension Your doctor has determined that you have high blood pressure, or hypertension. Although high blood pressure is never really cured, it can be controlled by early detection, lifestyle
AN OVERVIEW Hypertension Your doctor has determined that you have high blood pressure, or hypertension. Although high blood pressure is never really cured, it can be controlled by early detection, lifestyle
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Achieve. Achieve. More Effective. Dialysis Treatment
 Achieve More Effective Achieve Dialysis Treatment The Crit-Line monitor measures the following: Real-time, lab-equivalent, non-invasive hematocrit (HCT) Real-time percent changes in intravascular blood
Achieve More Effective Achieve Dialysis Treatment The Crit-Line monitor measures the following: Real-time, lab-equivalent, non-invasive hematocrit (HCT) Real-time percent changes in intravascular blood
On Referral to our Unit
 Case Presentation By Samah Ibrahim Abdel Meguid Idris, MD Internal Medicine & Nephrology Consultant Head of Hemodialysis Unit Ahmed Maher Hospital, Alexandria Patient Data MEA 27-year-old male patient
Case Presentation By Samah Ibrahim Abdel Meguid Idris, MD Internal Medicine & Nephrology Consultant Head of Hemodialysis Unit Ahmed Maher Hospital, Alexandria Patient Data MEA 27-year-old male patient
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE
 IT S NOT THAT SIMPLE") POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
Attending Rounds. Attending Rounds: A Patient with Intradialytic Hypotension
 Attending Rounds Attending Rounds: A Patient with Intradialytic Hypotension Robert F. Reilly Abstract Intradialytic hypotension is the most common adverse event that occurs during the hemodialysis procedure.
Attending Rounds Attending Rounds: A Patient with Intradialytic Hypotension Robert F. Reilly Abstract Intradialytic hypotension is the most common adverse event that occurs during the hemodialysis procedure.
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Online HD monitoring (BVM, OCM, BTM, etc.): Useful tools or fancy toys?
: Useful tools or fancy toys?") Online HD monitoring (BVM, OCM, BTM, etc.): Useful tools or fancy toys? Patrice Ambühl Basics in SSN/SGN Meeting, December 4 2013 patrice.ambuehl@waid.zuerich.ch Nephrologie Therapeutical dilemma Ultrafiltra
Online HD monitoring (BVM, OCM, BTM, etc.): Useful tools or fancy toys? Patrice Ambühl Basics in SSN/SGN Meeting, December 4 2013 patrice.ambuehl@waid.zuerich.ch Nephrologie Therapeutical dilemma Ultrafiltra
Dialysis: the long case
 Dialysis: the long case Prof Mark Brown St George Public Hospital, Kogarah The case SD 1. What significant things have been omitted from the history? 2. Physical findings 70 RTA; mitral regurg murmur;
Dialysis: the long case Prof Mark Brown St George Public Hospital, Kogarah The case SD 1. What significant things have been omitted from the history? 2. Physical findings 70 RTA; mitral regurg murmur;
Iraqi JMS. Effect of Dialysate Temperature on Hemodynamic Stability among Hemodialysis Patients. Tarik A. Hussein 1 FICMS, Arif S.
 Iraqi JMS Published by Al-Nahrain College of Medicine ISSN 1681-6579 Email: iraqijms@colmed-alnahrain.edu.iq http://www.colmed-nahrain.edu.iq Effect of Dialysate Temperature on Hemodynamic Stability among
Iraqi JMS Published by Al-Nahrain College of Medicine ISSN 1681-6579 Email: iraqijms@colmed-alnahrain.edu.iq http://www.colmed-nahrain.edu.iq Effect of Dialysate Temperature on Hemodynamic Stability among
Olistic Approach to Treatment Adequacy in AKI
 Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
major public health burden
 HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
Dialysis in frail and Elderly
 Dialysis in frail and Elderly Dr Shibu Jacob, Assistant Professor, Christian Medical College, Vellore. ISHDCON April 2,2017 Complications during dialysis and soon after? How to minimise these? Should
Dialysis in frail and Elderly Dr Shibu Jacob, Assistant Professor, Christian Medical College, Vellore. ISHDCON April 2,2017 Complications during dialysis and soon after? How to minimise these? Should
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
28-Feb-10 Reza Sabagh
 DIALYSIS EQUIPMENTS (DIALYSIS MACHINE & R.O) Nursing Conference on Dialysis Tehran 1 The standard dialysis machines are designed for performing chronic and acute hemodialysis. They can be used in home
DIALYSIS EQUIPMENTS (DIALYSIS MACHINE & R.O) Nursing Conference on Dialysis Tehran 1 The standard dialysis machines are designed for performing chronic and acute hemodialysis. They can be used in home
CSI (Clinical Scenario Investigation): Hyperkalemia
: Hyperkalemia") CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
The relationship between symptoms and blood pressure during maintenance hemodialysis
 Hemodialysis International 2015; : The relationship between symptoms and blood pressure during maintenance hemodialysis David J. MEREDITH, 1,2 Christopher W. PUGH, 1,2 Sheera SUTHERLAND, 2 Lionel TARASSENKO,
Hemodialysis International 2015; : The relationship between symptoms and blood pressure during maintenance hemodialysis David J. MEREDITH, 1,2 Christopher W. PUGH, 1,2 Sheera SUTHERLAND, 2 Lionel TARASSENKO,
Oxford Kidney Unit Your blood pressure and dialysis Information for patients
 Oxford Kidney Unit Your blood pressure and dialysis Information for patients If you are on dialysis, this leaflet will provide you with information on how manage your blood pressure. What is blood pressure?
Oxford Kidney Unit Your blood pressure and dialysis Information for patients If you are on dialysis, this leaflet will provide you with information on how manage your blood pressure. What is blood pressure?
Dialysis induced cardiac and brain injury
 Dialysis induced cardiac and brain injury Dr Nick Selby Consultant Nephrologist, Royal Derby Hospital, UK How can dialysis hurt patients? Wasting Inflammation Infection Cognitive loss, depression Increased
Dialysis induced cardiac and brain injury Dr Nick Selby Consultant Nephrologist, Royal Derby Hospital, UK How can dialysis hurt patients? Wasting Inflammation Infection Cognitive loss, depression Increased
Understanding Your Fluid Status During Dialysis and the Crit-Line. IV Monitor
 Understanding Your Fluid Status During Dialysis and the Crit-Line IV Monitor IV 1 Understanding Your Fluid Status During Hemodialysis Welcome to understanding your fluid status during hemodialysis. This
Understanding Your Fluid Status During Dialysis and the Crit-Line IV Monitor IV 1 Understanding Your Fluid Status During Hemodialysis Welcome to understanding your fluid status during hemodialysis. This
Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld
 Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld andreas.kistler@stgag.ch www.nephrologie-thurgau.ch Mr. Hyper K. Lemia charged with serial murder Bild entfernt (copyright)
Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld andreas.kistler@stgag.ch www.nephrologie-thurgau.ch Mr. Hyper K. Lemia charged with serial murder Bild entfernt (copyright)
HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI
 HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI high-flux Hemodiafiltration (HDF) Combination of two dialysis techniques, hemodialysis and hemofiltration:
HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI high-flux Hemodiafiltration (HDF) Combination of two dialysis techniques, hemodialysis and hemofiltration:
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Haemodiafiltration - the case against. Prof Peter G Kerr Professor/Director of Nephrology Monash Health
 Haemodiafiltration - the case against Prof Peter G Kerr Professor/Director of Nephrology Monash Health Know your opposition.. Haemodiafiltration NB: pre or post-dilution What is HDF how is it different
Haemodiafiltration - the case against Prof Peter G Kerr Professor/Director of Nephrology Monash Health Know your opposition.. Haemodiafiltration NB: pre or post-dilution What is HDF how is it different
Care of the Critically Unwell Patient. fluids
 Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
DIALYSIS THE VIEW FROM THE OTHER SIDE
 DIALYSIS THE VIEW FROM THE OTHER SIDE Myriam Farah, MD, FRCPC Fellow in Hemodialysis Division of Nephrology, University of British Columbia October 2011 OBJECTIVES 1. Identify the limitations of conventional
DIALYSIS THE VIEW FROM THE OTHER SIDE Myriam Farah, MD, FRCPC Fellow in Hemodialysis Division of Nephrology, University of British Columbia October 2011 OBJECTIVES 1. Identify the limitations of conventional
Causes of Intradialytic hypotension(idh)
") fluid management Causes of Intradialytic hypotension(idh) Excessive fluid removal Ultrafiltration rate > 0.35 ml/min/kg Patient-related factors Autonomic neuropathy (e.g. DM, Uremia) Antihypertensive medications
fluid management Causes of Intradialytic hypotension(idh) Excessive fluid removal Ultrafiltration rate > 0.35 ml/min/kg Patient-related factors Autonomic neuropathy (e.g. DM, Uremia) Antihypertensive medications
Cardiac Emergencies. Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington
 Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
EFFECT OF ONLINE HAEMODIAFILTRATION ON ALL- CAUSE MORTALITY AND CARDIOVASCULAR OUTCOMES Ercan Ok, Izmir, Turkey
 EFFECT OF ONLINE HAEMODIAFILTRATION ON ALL- CAUSE MORTALITY AND CARDIOVASCULAR OUTCOMES Ercan Ok, Izmir, Turkey Chair: Walter H. Hörl, Vienna, Austria Wojciech Zaluska, Lublin, Poland Prof Ercan Ok Division
EFFECT OF ONLINE HAEMODIAFILTRATION ON ALL- CAUSE MORTALITY AND CARDIOVASCULAR OUTCOMES Ercan Ok, Izmir, Turkey Chair: Walter H. Hörl, Vienna, Austria Wojciech Zaluska, Lublin, Poland Prof Ercan Ok Division
Vital Sign Variations with Complications during Dialysis among End-Stage Renal Disease Patients
 ORIGINAL ARTICLE Vital Sign Variations with Complications during Dialysis among End-Stage Renal Disease Patients ABSTRACT Abdul Rehman Qureshi 1, Naureen Durrani 2 and Naila Asif 3 Objective: To analyse
ORIGINAL ARTICLE Vital Sign Variations with Complications during Dialysis among End-Stage Renal Disease Patients ABSTRACT Abdul Rehman Qureshi 1, Naureen Durrani 2 and Naila Asif 3 Objective: To analyse
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen
 Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Module 10 Troubleshooting Guide
 Module 10 Troubleshooting Guide Your safety and wellbeing are our priority. Issues can occur during your treatment and it is important that you recognize the symptoms. This guide will teach you how to
Module 10 Troubleshooting Guide Your safety and wellbeing are our priority. Issues can occur during your treatment and it is important that you recognize the symptoms. This guide will teach you how to
Clinical judgment is the most important element in overhydration assessment of chronic hemodialysis patients
 Clin Exp Nephrol (2013) 17:563 568 DOI 10.1007/s10157-012-0745-9 ORIGINAL ARTICLE Clinical judgment is the most important element in overhydration assessment of chronic hemodialysis patients Radovan Vasko
Clin Exp Nephrol (2013) 17:563 568 DOI 10.1007/s10157-012-0745-9 ORIGINAL ARTICLE Clinical judgment is the most important element in overhydration assessment of chronic hemodialysis patients Radovan Vasko
Wednesday September 20 th CMT Regional Study Day. Dr Colin Mason, Consultant DME, Addenbrooke s Hospital
 Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Questions to ask your Doctor
 Questions to ask your Doctor What is my current blood pressure? What are my target blood pressure numbers? What blood pressure medication(s) am I currently taking? How is this drug different from what
Questions to ask your Doctor What is my current blood pressure? What are my target blood pressure numbers? What blood pressure medication(s) am I currently taking? How is this drug different from what
Hypertension and Hyperlipidemia. University of Illinois at Chicago College of Nursing
 Hypertension and Hyperlipidemia University of Illinois at Chicago College of Nursing 1 Learning Objectives 1. Provide a basic level of knowledge regarding hypertension and hyperlipidemia and care coordinators/
Hypertension and Hyperlipidemia University of Illinois at Chicago College of Nursing 1 Learning Objectives 1. Provide a basic level of knowledge regarding hypertension and hyperlipidemia and care coordinators/
Sodium ramping reduces hypotension and symptoms during haemodialysis
 ORIGINAL ARTICLE Key words: Blood pressure; Hemodialysis solutions; Kidney failure, chronic; Renal dialysis; Sodium!!"#!"#$! HL Tang SH Wong KH Chu W Lee A Cheuk CMK Tang ILL Kong KS Fung WK Tsang HWH
ORIGINAL ARTICLE Key words: Blood pressure; Hemodialysis solutions; Kidney failure, chronic; Renal dialysis; Sodium!!"#!"#$! HL Tang SH Wong KH Chu W Lee A Cheuk CMK Tang ILL Kong KS Fung WK Tsang HWH
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
2016 Annual Dialysis Conference Michelle Hofmann RN, BSN, CNN Renal Clinical Educator - Home
 Fluid Management 2016 Annual Dialysis Conference Michelle Hofmann RN, BSN, CNN Renal Clinical Educator - Home Objectives Define euvolemia Determine factors which contribute to fluid imbalance Discuss strategies
Fluid Management 2016 Annual Dialysis Conference Michelle Hofmann RN, BSN, CNN Renal Clinical Educator - Home Objectives Define euvolemia Determine factors which contribute to fluid imbalance Discuss strategies
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypotension During Haemodialysis: Aetiology, Risk Factors and Outcome
 ORIGINAL ARTICLE Hypotension During Haemodialysis: Aetiology, Risk Factors and Outcome *N Mahmood 1, MMU Hassan 2, F Mahmood 3, S Bari4 Background: Hypotension during hemodialysis is common. In some patients,
ORIGINAL ARTICLE Hypotension During Haemodialysis: Aetiology, Risk Factors and Outcome *N Mahmood 1, MMU Hassan 2, F Mahmood 3, S Bari4 Background: Hypotension during hemodialysis is common. In some patients,
Hemodynamic Instability in HD patients: Dialysis Hypotension Prof Ali BAŞÇI MD FERA Ege University Medical School
 Hemodynamic Instability in HD patients: Dialysis Hypotension Prof Ali BAŞÇI MD FERA Ege University Medical School Relationship between blood pressure and mortality in patients treated with volume control
Hemodynamic Instability in HD patients: Dialysis Hypotension Prof Ali BAŞÇI MD FERA Ege University Medical School Relationship between blood pressure and mortality in patients treated with volume control
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Assessment and Management of Hypertension in Patients on Dialysis
 Assessment and Management of Hypertension in Patients on Dialysis Rajiv Agarwal,* Joseph Flynn, Velvie Pogue, Mahboob Rahman, Efrain Reisin, and Matthew R. Weir *Division of Nephrology, Department of Medicine,
Assessment and Management of Hypertension in Patients on Dialysis Rajiv Agarwal,* Joseph Flynn, Velvie Pogue, Mahboob Rahman, Efrain Reisin, and Matthew R. Weir *Division of Nephrology, Department of Medicine,
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
What is Hypertension?
 What is Hypertension? What is hypertension? Hypertension is also known as high blood pressure. Our blood needs to be under pressure to make it move around the body, but when it is too high this causes
What is Hypertension? What is hypertension? Hypertension is also known as high blood pressure. Our blood needs to be under pressure to make it move around the body, but when it is too high this causes
PREVALENCE AND TYPES OF INTRA-DIALYTIC COMPLICATIONS IN PATIENTS DIALYSING AT THE UNIVERSITY OF BENIN TEACHING HOSPITAL
 PREVALENCE AND TYPES OF INTRA-DIALYTIC COMPLICATIONS IN PATIENTS DIALYSING AT THE UNIVERSITY OF BENIN TEACHING HOSPITAL ADEJUMO OA, OLOKOR AB, IYAWE IO, OKAKA EI, UNUIGBE EI, OJOGWU LI Presented at Nigerian
PREVALENCE AND TYPES OF INTRA-DIALYTIC COMPLICATIONS IN PATIENTS DIALYSING AT THE UNIVERSITY OF BENIN TEACHING HOSPITAL ADEJUMO OA, OLOKOR AB, IYAWE IO, OKAKA EI, UNUIGBE EI, OJOGWU LI Presented at Nigerian
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
HIGH BLOOD. PRESSURE What you need to know BECAUSE...CARING COMES NATURALLY TO US
 HIGH BLOOD PRESSURE What you need to know BECAUSE...CARING COMES NATURALLY TO US What is Blood Pressure We all need blood pressure to stay alive. Without it, blood can t flow through our bodies to supply
HIGH BLOOD PRESSURE What you need to know BECAUSE...CARING COMES NATURALLY TO US What is Blood Pressure We all need blood pressure to stay alive. Without it, blood can t flow through our bodies to supply
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
2019 Home Hemodialysis Standing Orders
 2019 Home Hemodialysis Standing Orders 1. Nutrition Standards of Care: A. Follow P&P Nutrition Standards of Care 2. Laboratory Tests: A. Drawn On Admission: 1. Renal Function Panel (BMP, PO 4 and Albumin)
2019 Home Hemodialysis Standing Orders 1. Nutrition Standards of Care: A. Follow P&P Nutrition Standards of Care 2. Laboratory Tests: A. Drawn On Admission: 1. Renal Function Panel (BMP, PO 4 and Albumin)
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Critical Thinking. Beat the Clock!
 Critical Thinking Beat the Clock! Critical Thinking Making good choices by using information from several sources o Training o Policies and procedures o Communicating/collaborating with other dialysis
Critical Thinking Beat the Clock! Critical Thinking Making good choices by using information from several sources o Training o Policies and procedures o Communicating/collaborating with other dialysis
Snapshot. What kinds of things make you feel stressed out? What do you do to calm back down? Do you have any good tricks for de-stressing??
 Snapshot What kinds of things make you feel stressed out? What do you do to calm back down? Do you have any good tricks for de-stressing?? Welcome back! Agenda - Introduction to blood pressure - Blood
Snapshot What kinds of things make you feel stressed out? What do you do to calm back down? Do you have any good tricks for de-stressing?? Welcome back! Agenda - Introduction to blood pressure - Blood
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Treatment of the Medically Compromised Patient
 Treatment of the Medically Compromised Patient Nashville Area Continuing Dental Education Series November 3, 2010 Harry J. Brown, MD Chief Medical Officer, Nashville Area Outline General Principles Specific
Treatment of the Medically Compromised Patient Nashville Area Continuing Dental Education Series November 3, 2010 Harry J. Brown, MD Chief Medical Officer, Nashville Area Outline General Principles Specific
Mechanisms and Treatment of Intradialytic Hypertension
 Review Advances in CKD 2016 Published online: January 15, 2016 Peter Noel Van Buren a Jula K. Inrig b a University of Texas Southwestern Medical Center, Department of Internal Medicine and Division of
Review Advances in CKD 2016 Published online: January 15, 2016 Peter Noel Van Buren a Jula K. Inrig b a University of Texas Southwestern Medical Center, Department of Internal Medicine and Division of
Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST)
 and Inappropriate Sinus Tachycardia (IST)") Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST) Ahmad Hersi, MBBS, MSc, FRCPC Professor of Cardiac Sciences Consultant
Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST) Ahmad Hersi, MBBS, MSc, FRCPC Professor of Cardiac Sciences Consultant
Volume Management 2/25/2017. Disclosures statement: Objectives. To discuss evaluation of hypervolemia in peritoneal dialysis patients
 Volume Management Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 14, 2017 Disclosures statement: Consultant: Allena, Becker Professional Education Grant
Volume Management Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 14, 2017 Disclosures statement: Consultant: Allena, Becker Professional Education Grant
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Diagnosing and Treating Neurogenic Orthostatic Hypotension: A Case Study
 Diagnosing and Treating Neurogenic Orthostatic Hypotension: A Case Study Learning Objectives: Illustrate how to accurately diagnose noh Employ scales and questionnaires in combination with cardiovascular
Diagnosing and Treating Neurogenic Orthostatic Hypotension: A Case Study Learning Objectives: Illustrate how to accurately diagnose noh Employ scales and questionnaires in combination with cardiovascular
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
High Blood Pressure. Do You Have High Blood Pressure? What Is Blood Pressure?
 High Blood Pressure You can have high blood pressure, or hypertension, and still feel just fine. That s because high blood pressure often does not cause signs of illness that you can see or feel. But,
High Blood Pressure You can have high blood pressure, or hypertension, and still feel just fine. That s because high blood pressure often does not cause signs of illness that you can see or feel. But,
Contempo GIMSI Cosa cambia alla luce della letteratura in tema di terapia farmacologica
 Contempo GIMSI 2015-2017 Cosa cambia alla luce della letteratura in tema di terapia farmacologica Dott.ssa Diana Solari Centro Aritmologico e Sincope Unit, Lavagna www.gimsi.it POST 2 (Prevention of Syncope
Contempo GIMSI 2015-2017 Cosa cambia alla luce della letteratura in tema di terapia farmacologica Dott.ssa Diana Solari Centro Aritmologico e Sincope Unit, Lavagna www.gimsi.it POST 2 (Prevention of Syncope
INTRADIALYTIC DOPAMINE THERAPY IN MAINTENANCE HEMODIALYSIS PATIENTS WITH PERSISTENT HYPOTENSION
 Original Article 22 INTRADIALYTIC DOPAMINE THERAPY IN MAINTENANCE HEMODIALYSIS PATIENTS WITH PERSISTENT HYPOTENSION Wen-Yuan Chiu, Horng-Rong Chang *, Zyh-Zan Lin **, Enny Halim, Jong-Da Lian * Intradialytic
Original Article 22 INTRADIALYTIC DOPAMINE THERAPY IN MAINTENANCE HEMODIALYSIS PATIENTS WITH PERSISTENT HYPOTENSION Wen-Yuan Chiu, Horng-Rong Chang *, Zyh-Zan Lin **, Enny Halim, Jong-Da Lian * Intradialytic
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Dialysis Technicians Can Positively Influence Patient Outcomes
 Dialysis Technicians Can Positively Influence Patient Outcomes CMS expectations for clinical management of dialysis patients The role direct care staff play and strategies for improving patient clinical
Dialysis Technicians Can Positively Influence Patient Outcomes CMS expectations for clinical management of dialysis patients The role direct care staff play and strategies for improving patient clinical
Blood Pressure Fox Chapter 14 part 2
 Vert Phys PCB3743 Blood Pressure Fox Chapter 14 part 2 T. Houpt, Ph.D. 1 Cardiac Output and Blood Pressure How to Measure Blood Pressure Contribution of vascular resistance to blood pressure Cardiovascular
Vert Phys PCB3743 Blood Pressure Fox Chapter 14 part 2 T. Houpt, Ph.D. 1 Cardiac Output and Blood Pressure How to Measure Blood Pressure Contribution of vascular resistance to blood pressure Cardiovascular