Causes of Intradialytic hypotension(idh)
|
|
|
- Ophelia Maxwell
- 5 years ago
- Views:
Transcription
1 fluid management
2 Causes of Intradialytic hypotension(idh) Excessive fluid removal Ultrafiltration rate > 0.35 ml/min/kg Patient-related factors Autonomic neuropathy (e.g. DM, Uremia) Antihypertensive medications Sympathetic failure RAS and arginine-vasopressin syst. sensitivity Food ingestion(splanchnic vasodilation) Tissue ischemia(adenosine mediated) Bacterial sepsis Impaired Intradialytic venous pooling Vasoconstriction. Core body temp.anemia Decrease in plasma vol. > 20% Reduced plasma refilling rate Reduced ECV Hemorrhage Intradialytic Hypotension Dialysis-related factors Heart problems Myocardial Infarction.Structural heart dis Arrythmias Pericardial tamponade Hemolysis Dialyzer Rxn Air embolism Acetate dalysate (adenosine-mediated).low dialysate Na &/or ionized Ca conc Complemant activation (C3a and C5a-mediated) Cytokine generation(il-1 and NO-mediated)
3 Water movement during standard hemodialysis Intracellular fluid Extracellular fluid Dialyzer step3 Water movement Osmolality Osmolality mosm/kg mosm/kg Osmolality mosm/kg 320 Falling to 290mosm/ kg as diffusion occurs Compensatory refilling step1 280 step2 Loss of urea and water


4 Fluid removal Plasma refilling
5 Fluid removal Fluid removal Na Low Na meq/l Na Increased risk of hypotension
6 urea removed by dialyzer urea sequestration in tissue fluid Effluent Dialysate Increased intracellular osmolarity Inffluent Dialysate fluid Na
7 Fluid removal Plasma refilling Na Na >145 meq/l Na
8 Pathophysiological Changes Induced by Low and High Dialysate Change Low Na+ Dialysate High Na+ Dialysate Decrease in ECF Osmolality Increase in ECF Osmolality H20 from EC to IC Increased Renin & Aldosterone Decreased ECV/ Increased ICV H20 from IC to EC Decreased Renin & Aldosterone Increased ECV/ Decreased ICV
9 Intradialytic hypotension (IDH):.definition Decrease in SBP 20 mm Hg or MAP < 10 mm Hg, associated with clinical events and need for nursing. intervention Intervention may be IV saline administration,.trendelenburg position Asymptomatic SBP <90 mm Hg should be.considered as hypotension 1, EBPG, NDT , K/DOQI Am J Kidney Dis. 2005
10 .Complications of recurrent IDH Reduced efficiency of dialysis. Compartmentalization leading to sequestration of uremic toxins. Reduced time on dialysis. Organ ischemia. Brain: cerebro-vascular events. Gut: ischemia, gram negative sepsis.
11 Salt & volume overload Vascular Space Interstitial Space Cardiac Output SNS activity Renin angiotensin activity Blood Pressure Inappropriate Vascular resistance
12 Clinical Significance In 17% of all treatments, intradialytic hypotension seen. 25% are free of intradialytic hypotension 75% of all patients has had at least 1 episode. 16% of all patients had more than 1x/week on average. These patients had higher mortality rate, higher admission rates and longer hospital stays. Dialysis facility was an independent predictor. Older patients Longer dialysis vintage Diabetes Lowe pre-dialysis blood pressure Higher Uf goal In essence, the BP depends on: 1) Cardiac reserve 2) Intravascular volume and Uf rate 3) Vascular tone In a study of 1137 patients over 44,801 treatments among 13 outpatient dialysis facilities. Sands, J. et al. 2014, Intradialytic hypotension: Frequency, sources of variation and correlation with clinical outcome. Hemodialysis International, 18:
13 Patients at risk of IDH 65 years or older age DM Patients with CVD: LVH and diastolic dysfunction with or without CHF LV systolic dysfunction and CHF Valvular heart disease Pericardial disease (constrictive pericarditis or pericardial effusion) Poor nutritional status and hypoalbuminemia Hyperphosphatemia Uremic neuropathy or autonomic dysfunction due to other causes Severe anemia Patients requiring high volume ultrafiltration; more than expected interdialytic weight gain Patients with predialysis SBP of <100 mm Hg
14 HYPOTENSION AVOIDANCE Hemodialysis-induced Cardiac Dysfunction Is Associated with an Acute.Reduction in Global and Segmental Myocardial Blood Flow Ref: Christopher W.Mclntyre james o.burton Nicholas M. Selby, Lucia leccisolti Shvan korsheed, Christopher S.R Beker and Paolo G. camici Hemodialysis-Induced Repetitive Myocardial Injury Results in Global and Segmental Reduction in Systolic Cardiac Function. Ref: JAMES O.BURTON, HELEN J.JEFFERIES,NICHOLAS M.SELBY, AND CHRISTOPHER W. MCINTYPE,CHIN J SEC NEPHRED ,2009
. dry weight. Refraining fromcardiac foodtreatment intake operform evaluation. options duringodialysis.")
15 EBPG guideline on haemodynamic instability o o o o o o o First-line approach Second-line Third-line approach approach DietaryoTry counselling (sodium to assess objective methods (only if other restriction). dry weight. Refraining fromcardiac foodtreatment intake operform evaluation. options duringodialysis. failed) Gradual reductionhave of dialysate Clinicaltemperature reassessment dry fromof 36.5 C weight.downward (lowest oconsider 35 C) midodrine. or Use of isothermic bicarbonate as oconsider treatment (possible l-carnitine dialysis buffer. supplementation. alternative: convective oconsider peritoneal dialysis. Use of treatments). a dialysate oconsider temperature of 36.5 C. individualized blood Check volume dosing controlled and timing of feedback. oprolong dialysis antihypertensive agents time and/or increase dialysis frequency. oprescribe a dialysate calcium concentration of 1.50 mmol/l. Kooman J, Basci A et al. Nephrol Dial Transplant May;22 Suppl 2:ii22-44.

 Temperature setting of at least 1 degree from the actual body temperature seem to help.")
16 Dialysate Temperature Vasoconstriction to maintain BP Vasodilation to lower temperature Raises the body core temperature Drops the BP A reduction in dialysate temperature from 36.7 to 34.4 decreased the frequency of IDH from 0.58 to 0.05 episodes per treatment in a study of 7 patients with frequent IDH. (Sherman, 1985) Temperature setting of at least 1 degree from the actual body temperature seem to help. Multiple similar study results in the efficacy of lower dialysate temp.



17 Principles of fluid management practice Retained fluid & salt Goal Vascular stability Remove fluid without adverse events Prevent Long term CVDShort term hypotension- BTMDialysate temp- PRR UFR<12.4 ml/kg/hruf profilesdt frequency- Avoid Saline- Monitoring BP (frequency)cardiac (Apex)- Target Weight :(IDWT) Fluid assessment1/12 BCM 1/12- f: Fresenius MEA Nephrology Academy and EDTNA 2017 Evaluate
 Quantification of")

18 Body Composition Monitoring- BCM :BCM assists in the assessment of the following clinical parameters Monthly review (pre-dialysis) Quantification of fluid status Over hydration Total body water(v) Assessment of body composition Lean tissue mass Adipose tissue mass Ref: Fresenius MEA Nephrology Academy and EDTNA 217
19 ?Why all the Physiology Stuff Gain of water (5% Dextrose) 5% Dex 1L 5% dextrose infused into the intravascular compartment (ECF) will redistribute throughout the whole body water space of which only 3.5L is intravascular space. Therefore you would need to infuse 13l of 5% dextrose to increase the plasma volume by 1L Plasma ICF Interstitial
20 ?Why all the Physiology Stuff Gain of water & electrolytes eg 0.9% NaCl Na+ & Cl- at concentration of 150 mmol/l Osmolality matches that inside the cells therefore no net change in the osmolality and no net movement of water.into the cells so fluid remains in the extracellular space 0.9% NaCl Plasma ICF Interstitial
21 Why all the Physiology Stuff? - Pop Quiz IV infusion of Colloids (solutions containing high molecular weight molcules/proteins eg Gel fusion) Where does it go? A) Intravascular/Plasma space Gelofusion Plasma ICF Interstitial
22 Why all the Physiology Stuff? - Pop Quiz IV infusion of Colloids (solutions containing high molecular weight molcules/proteins eg Gelofusion) Where does it go? B) Draws fluid in (plasma. expander) Gelofusion Plasma ICF Interstitial

23 Factores affecting Plasma refilling PR Measures to reduce risk Blood Volume PR UF PR Ref: Fresenius MEA Nephrology Academy and EDTNA 2017 Reduce IDWG decrease UFR Prolong dialysis time decrease UFR Increase dialysis frequency decrease UFR Limb exercise Increase PRR Ultrafiltration profiling Increase PRR Balance PRR and UFR Avoid saline boluses Increase PRR
24 Summary Safe Uf rate is <12.4 ml/kg/hr. Remind patients to drink less liquids. Discuss with the patient/physician to increase dialysis time. Low dialysate temperature in place? Monitor for changes in MAP. Pre-emptive holding of Uf for 10 minutes until MAP better? Saline, hypertonic saline, 20% dextrose, albumin as per local procedures and physician orders. Na profiling: Pros vs. Cons Uf profile review Holding BP medications pre-dialysis Discuss with physicians re: midodrine, caffeine, Zoloft Role of Blood Volume Monitoring? Always think of acute issues Is Peritoneal Dialysis an option?
25 THANKS FOR YOUR ATTENTION
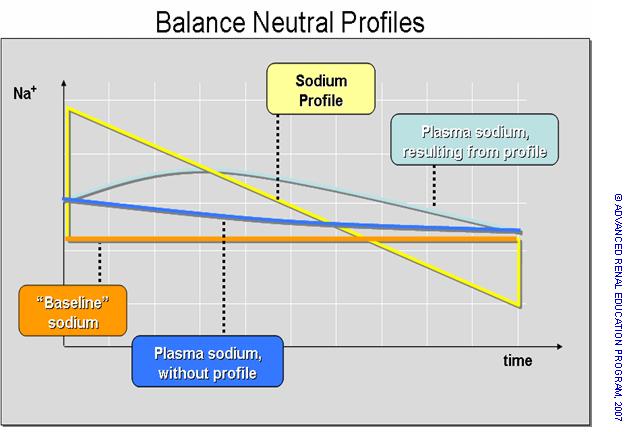
26 Different patterns of sodium modeling meq/lit Na concentration meq/lit Hours after dialysis initiation
27
28
29
30 Goals of UF Profiling Provide adequate ultrafiltration (UF) Minimize symptoms related to hypovolemia Enhance plasma refill Allow the patient to reach estimated dry weight (EDW) Plasma refill: Refilling of the blood compartment, or vascular space from the surrounding tissue spaces Hypovolemia: Decreased blood volume leads to decreased cardiac output which can cause hypotension
31 Profiling Ultrafiltration: Allows the patient to reach their estimated dry weight (EDW) Helps prevent symptoms Allows refilling of vascular fluid volume from the interstitial space (plasma refill) Allows higher volume fluid removal at times when fluid is more readily available Prevents hypotension 31
32 A patient weight gains typically of 3-4 kg and experiences moderate to severe leg cramps during the last 30 minutes of treatment 32
33 Patient tolerates fluid removal (higher UF) at the beginning of treatment Systolic BP Symptoms are relieved at the end of treatment with a lower UF UF Profile Time in Minutes 33
34 220 Systolic BP Fluid overloaded 200 patients benefit from 180 aggressive UF at 1.8 Kg/h 160 the beginning of the treatment Step profiles allow for 80 dramatic decreases in UF. 60 Lower UF at the 40 middle and end of treatment will reduce the patient s symptoms UF Profile Time in Minutes 34
35 Second patient arrives with a systolic blood pressure of 85 and a weight gain of 3 Kg. If her SBP falls below 75 she becomes symptomatic 35
36 220 Less UF should be used at the beginning of 200while the SBP treatment is low. 180 Increase the UF during periods when the SBP 160is higher Systolic BP Decrease the UF toward the end of treatment as the patient approaches her dry weight to prevent symptoms Time in Minutes 36
37 220 Using a Step Profile, you can create multiple minimum UF periods which will allow plasma refill to occur. Decrease the UF toward the end of treatment as the patient approaches her dry weight to prevent symptoms Systolic BP Time in Minutes 37
38 A woman patient is hypertensive and diabetic. She has large fluid gains of 4-6 Kg between treatments and has symptoms of hypotension about 45 minutes into the treatment as well as mid and late treatment 38
39 Assessment and Plan Assessment: Large fluid gains Severe hypotensive episodes Poor plasma refill Plan Support plasma refill, especially during the first part of the treatment Prevent hypovolemia Consider conductivity profiling in addition to UF profiling 39
40 Utilize a Conductivity profile to support solute removal Systolic BP Arrows indicate plasma refill times Time in Minutes 40
41 220 UF and Conductivity Profiling can be used simultaneously with similar step curves 200 Systolic BP Time in Minutes 41
42 Systolic BP UF and Conductivity Profiling 100 can be used simultaneously with 80 similar progressive curves Time in Minutes 42
43 Clinical case study Name: Nasser Tabkhi Unit: Smarrt company Topic: Patient with Intradialytic episodic Hypotension
44 contents Background Laboratory Test Clinical problems Management outcome
45 Background A man with 68 years old, on hemodialysis since 2011 diabetic nephropathy hypertension vascular disease LVH diabetic retinopathy lungs were not clear to auscultation cardiac rhythm was regular Dialysis duration= 4 hours The single pool Kt/V on this man was 1.21 his dry weight was 82.5 kg average interdialytic weight gain was 5 kg per treatment

46 LABORATORY TEST BUN = 45 (mg/dl) cr = 9 (mg/dl) Hemoglobin= 11.5 g/dl Albumin = 3.4 g/dl Calcium = 8.9 mg/dl Phosphor = 6.5 mg/dl PTH = 558 pg/ml KT/V= 1.2
47 CLINICAL PROBLEM Large fluid gains Severe hypotensive episodes Poor plasma refill between treatments he had symptoms of hypotension about 45 minutes into the treatment as well as mid and late treatment At the beginning of dialysis session his BP= 160/74 after half an hour BP= 105/60 after one hour BP = 95/6 then BP decreased to 85/42
48 management Plan A Saline was administered Ultrafiltration was stopped Trendelenburg position Cool dialysate solution Dry weight was adjusted Counseling with nutritionist on limiting salt intake but they were not effective and Despite this intervention after starting uf again, the patient developed another episode of IDH Plan B Support plasma refill, during of the treatment Consider UF profiling and if necessary in addition to sodium profiling
49 Outcome to prevent episodic hypotension: By using Step UF and Sodium modeling(increasing osmolality of extra cellular space ) we create multiple minimum UF periods which will allow plasma refilling. Considering patient s cardiovascular and diabetes disorders and problems related to plasma refilling patient s BP has been stabled around 130/60 mmhg
50 Na profile Uf profile 220 Using a Step Profile, you can create multiple minimum UF periods which will allow plasma refill to occur. Decrease the UF toward during of treatment as the patient approaches her dry weight to prevent symptoms Systolic BP Time in Minutes


51
52 Subclinical Negative Impact Brain Ischemia: MRI have shown pathologic changes with dialysis, worse with intradialytic hypotension (IDH) Brain white matter ischemic injury from loss of axons and myelin (McIntyre, Seminars in Dialysis, 2010) Cardiac Stunning: Echo during dialysis confirms the presence of LV regional wall motion abnormality (Chesterton, Hemodialysis International, 2010) Episodic IDH is thought to exacerbate evolving myocardial injury. Cardiac muscles receive coronary flow during diastole and most HD patients have a widened pulse pressure. Gut Stunning: Non-occlusive mesenteric ischemia is associated with frequent IDH. (Daugirdas, AJKD, 2001). Mesenteric ischemia may also allow bacterial endotoxins to be introduced into the circulation, causing vasodilation and reduced cardiac contractility. (McIntyre, Seminars in Dialysis, 2010)
53 References Heinrich, W.L. & Victor, R.G., Autonomic Neuropathy and Hemodynamic Stability in End-Stage Renal Disease Patients, Principles and Practice in Dialysis, Williams and Wilkins, Baltimore, Wilson, S., Alvarez, D., A Primer on Ultrafiltration Profiling and Sodium Modeling for Dialysis Patients, Contemporary Dialysis and Nephrology, April 2000, pp Bonomini, V., Coli, L., Scolari, M.P., Profiling Dialysis: A New Approach to Dialysis Intolerance, Nephron 1997; 75:1-6 Leunissen, K.M.L., Kooman, J.P., van der Sande, F.M., van Kuijk, W.H.M., Hypotension and Ultrafiltration Physiology in Dialysis, Blood Purif 2000; 18: Oliver, M.J., Edwards, L.J., Churchill, Impact of Sodium and Ultrafiltration Profiling on Hemodialysis Related Symptoms, J Am Soc Nephrol 12: Jensen, B.M., Dobbe, S. A., Squillace, D.P., McCarthy, J.T., (April 1994) Clinical Benefits of High and Variable Sodium Concentration Dialysate in Hemodialysis Patients, ANNA Journal, Vol. 21, No
54 References Gambro Basics 1 Gambro Education 1994 Petitclerc, T. and Jacobs, C. Dialysis sodium concentration: what is optimal and can it be individualized?, Nephrol Dial Transplant Editorial Comments1995, Coli, L., Ursino, M., Dalmastri, V., Volpe, F., LaManna, G., Avanzolini, G., Stefoni, S., Bonomini, V., A simple mathematical model applied to selection of the sodium profile during profiled haemdialysis, Nephrol Dial Transplant (1998) 13: Donauer,J., Kolblin, D., Bek, M., Krause, A., Bohler, J., Ultrafiltration Profiling and Measurement of Reletive Blood Volume as Strategies to Reduce Hemodialysis-Related Side Effects, AJKD, Vol 36, No 1 (July), 2000:pp Stiller, S., Bonnie-Schorn, E., Grassmann, A., Uhlenbusch-Korwer, Mann, A Critical Review of Sodium Profiling for Hemodialysis, Seminars in Dialysis, Vol 14, No 5 (September-October) 2001 pp Locatelli, F., DiFilippo, S., Manzoni, C., Corti, M., Andrulli, S., Pontoriero, G., Monitoring sodium removal and delivered dialysis by conductivity, The International Journal of Artificial Organs/Vol. 18/no. 11, 1995/pp
55 THANK YOU 55
How to deal with hypotension on dialysis? CME Basics in Nephrology SGN-SSN Interlaken 2016
 How to deal with hypotension on dialysis? CME Basics in Nephrology SGN-SSN Interlaken 2016 PD Dr. med. Andreas Kistler Leitender Arzt Nephrologie und Dialyse Kantonsspital Frauenfeld www.spital-thurgau.ch
How to deal with hypotension on dialysis? CME Basics in Nephrology SGN-SSN Interlaken 2016 PD Dr. med. Andreas Kistler Leitender Arzt Nephrologie und Dialyse Kantonsspital Frauenfeld www.spital-thurgau.ch
St George Hospital Renal Department: INTERNAL ONLY
 HYPOTENSION AND HAEMODIALYSIS THE BOTTOM LINE 1. Prevention of hypotension during haemodialysis (IDH) 2. Treatment of hypotension during haemodialysis (IDH) 3. Withholding dialysis when SBP
HYPOTENSION AND HAEMODIALYSIS THE BOTTOM LINE 1. Prevention of hypotension during haemodialysis (IDH) 2. Treatment of hypotension during haemodialysis (IDH) 3. Withholding dialysis when SBP
Challenges to Manage Blood Pressure in ESRD and Heart Failure Patients
 Challenges to Manage Blood Pressure in ESRD and Heart Failure Patients Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health San Antonio 2nd Annual Cardiorenal Connections Meeting, April 28,
Challenges to Manage Blood Pressure in ESRD and Heart Failure Patients Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health San Antonio 2nd Annual Cardiorenal Connections Meeting, April 28,
Haemodiafiltration - the case against. Prof Peter G Kerr Professor/Director of Nephrology Monash Health
 Haemodiafiltration - the case against Prof Peter G Kerr Professor/Director of Nephrology Monash Health Know your opposition.. Haemodiafiltration NB: pre or post-dilution What is HDF how is it different
Haemodiafiltration - the case against Prof Peter G Kerr Professor/Director of Nephrology Monash Health Know your opposition.. Haemodiafiltration NB: pre or post-dilution What is HDF how is it different
Hypotension During Haemodialysis: Aetiology, Risk Factors and Outcome
 ORIGINAL ARTICLE Hypotension During Haemodialysis: Aetiology, Risk Factors and Outcome *N Mahmood 1, MMU Hassan 2, F Mahmood 3, S Bari4 Background: Hypotension during hemodialysis is common. In some patients,
ORIGINAL ARTICLE Hypotension During Haemodialysis: Aetiology, Risk Factors and Outcome *N Mahmood 1, MMU Hassan 2, F Mahmood 3, S Bari4 Background: Hypotension during hemodialysis is common. In some patients,
Iraqi JMS. Effect of Dialysate Temperature on Hemodynamic Stability among Hemodialysis Patients. Tarik A. Hussein 1 FICMS, Arif S.
 Iraqi JMS Published by Al-Nahrain College of Medicine ISSN 1681-6579 Email: iraqijms@colmed-alnahrain.edu.iq http://www.colmed-nahrain.edu.iq Effect of Dialysate Temperature on Hemodynamic Stability among
Iraqi JMS Published by Al-Nahrain College of Medicine ISSN 1681-6579 Email: iraqijms@colmed-alnahrain.edu.iq http://www.colmed-nahrain.edu.iq Effect of Dialysate Temperature on Hemodynamic Stability among
Sodium elimination and dialysate sodium. How much? Does it matter?
 Sodium elimination and dialysate sodium How much? Does it matter? A. Bock Nephrologie Dialysis visit Aarau 3.12.2013 90 kg dialysis patient: 5 kg over dry weight Recent dyspnea. Minimal leg edema RBV in
Sodium elimination and dialysate sodium How much? Does it matter? A. Bock Nephrologie Dialysis visit Aarau 3.12.2013 90 kg dialysis patient: 5 kg over dry weight Recent dyspnea. Minimal leg edema RBV in
02/28/2018. To reduce morbidity, mortality and treatment loss associated with chronic volume overload in hemodialysis patients
 Lisa Koester Renal Nurse Practitioner Washington University School of Medicine St. Louis, MO To reduce morbidity, mortality and treatment loss associated with chronic volume overload in hemodialysis patients
Lisa Koester Renal Nurse Practitioner Washington University School of Medicine St. Louis, MO To reduce morbidity, mortality and treatment loss associated with chronic volume overload in hemodialysis patients
The goal of dialysis for patients with chronic renal failure is to
 Dialysate Composition in Hemodialysis and Peritoneal Dialysis Biff F. Palmer The goal of dialysis for patients with chronic renal failure is to restore the composition of the body s fluid environment toward
Dialysate Composition in Hemodialysis and Peritoneal Dialysis Biff F. Palmer The goal of dialysis for patients with chronic renal failure is to restore the composition of the body s fluid environment toward
Low Blood Pressure During Dialysis (Intradialytic Hypotension (IDH))
)") Low Blood Pressure During Dialysis (Intradialytic Hypotension (IDH)) By Dori Schatell, Medical Education Institute One of the main jobs of dialysis is to remove excess water from your body. Seems pretty
Low Blood Pressure During Dialysis (Intradialytic Hypotension (IDH)) By Dori Schatell, Medical Education Institute One of the main jobs of dialysis is to remove excess water from your body. Seems pretty
Striking the Optimal Balance in
 Not Too fast, Not Too Slow: Striking the Optimal Balance in Hemodialysis Fluid Management ANNA/ IPRO Spring Symposium May 24, 2018 Jennifer E. Flythe, MD, MPH Assistant Professor of Medicine University
Not Too fast, Not Too Slow: Striking the Optimal Balance in Hemodialysis Fluid Management ANNA/ IPRO Spring Symposium May 24, 2018 Jennifer E. Flythe, MD, MPH Assistant Professor of Medicine University
FLUID MANAGEMENT IN DIALYSIS: STRATEGIES FOR SUCCESS
 FLUID MANAGEMENT IN DIALYSIS: STRATEGIES FOR SUCCESS Quality Insights Renal Network 3 October 2, 2014 Laura D. Byham-Gray, PhD, RD Professor & Director Master of Science in Clinical Nutrition Rutgers University
FLUID MANAGEMENT IN DIALYSIS: STRATEGIES FOR SUCCESS Quality Insights Renal Network 3 October 2, 2014 Laura D. Byham-Gray, PhD, RD Professor & Director Master of Science in Clinical Nutrition Rutgers University
THE INTRADIALYTIC BIOFEEDBACKS AND THE CARDIOVASCULAR STABILITY IN HYPOTENSION- PRONE PATIENTS Antonio Santoro, Bologna, Italy
 THE INTRADIALYTIC BIOFEEDBACKS AND THE CARDIOVASCULAR STABILITY IN HYPOTENSION- PRONE PATIENTS Antonio Santoro, Bologna, Italy Chair: Walter H. Hörl, Vienna, Austria Wojciech Zaluska, Lublin, Poland Prof.
THE INTRADIALYTIC BIOFEEDBACKS AND THE CARDIOVASCULAR STABILITY IN HYPOTENSION- PRONE PATIENTS Antonio Santoro, Bologna, Italy Chair: Walter H. Hörl, Vienna, Austria Wojciech Zaluska, Lublin, Poland Prof.
Achieving Equilibrium in ESRD Patients
 Achieving Equilibrium in ESRD Patients -Marc Richards MD -South Florida Kidney Disease and HTN Specialists -Chief of Medicine, BRRH -BRRH Grand Rounds: April 18 th, 2017 Outline Dialysis prescription Adequacy
Achieving Equilibrium in ESRD Patients -Marc Richards MD -South Florida Kidney Disease and HTN Specialists -Chief of Medicine, BRRH -BRRH Grand Rounds: April 18 th, 2017 Outline Dialysis prescription Adequacy
Understanding Kt/V and Volume Control
 Understanding Kt/V and Volume Control Its practical use to determine dialysis and improve outcomes Caroline Williams RD May 23, 2017 Volume Control in Dialysis Patients Pathogenesis In the 1960s and early
Understanding Kt/V and Volume Control Its practical use to determine dialysis and improve outcomes Caroline Williams RD May 23, 2017 Volume Control in Dialysis Patients Pathogenesis In the 1960s and early
Sodium ramping reduces hypotension and symptoms during haemodialysis
 ORIGINAL ARTICLE Key words: Blood pressure; Hemodialysis solutions; Kidney failure, chronic; Renal dialysis; Sodium!!"#!"#$! HL Tang SH Wong KH Chu W Lee A Cheuk CMK Tang ILL Kong KS Fung WK Tsang HWH
ORIGINAL ARTICLE Key words: Blood pressure; Hemodialysis solutions; Kidney failure, chronic; Renal dialysis; Sodium!!"#!"#$! HL Tang SH Wong KH Chu W Lee A Cheuk CMK Tang ILL Kong KS Fung WK Tsang HWH
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
HTA ET DIALYSE DR ALAIN GUERIN
 HTA ET DIALYSE DR ALAIN GUERIN Cardiovascular Disease Mortality General Population vs ESRD Dialysis Patients 100 Annual CVD Mortality (%) 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age
HTA ET DIALYSE DR ALAIN GUERIN Cardiovascular Disease Mortality General Population vs ESRD Dialysis Patients 100 Annual CVD Mortality (%) 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age
Nephrology Dialysis Transplantation
 Nephrol Dial Transplant (1996) 11 [Suppl 8]: 10-15 Nephrology Dialysis Transplantation Urea, sodium, and water changes in profiling dialysis H. Mann and S. Stiller ntroduction Control of osmolarity, as
Nephrol Dial Transplant (1996) 11 [Suppl 8]: 10-15 Nephrology Dialysis Transplantation Urea, sodium, and water changes in profiling dialysis H. Mann and S. Stiller ntroduction Control of osmolarity, as
On Referral to our Unit
 Case Presentation By Samah Ibrahim Abdel Meguid Idris, MD Internal Medicine & Nephrology Consultant Head of Hemodialysis Unit Ahmed Maher Hospital, Alexandria Patient Data MEA 27-year-old male patient
Case Presentation By Samah Ibrahim Abdel Meguid Idris, MD Internal Medicine & Nephrology Consultant Head of Hemodialysis Unit Ahmed Maher Hospital, Alexandria Patient Data MEA 27-year-old male patient
Hemodialysis is a life-sustaining procedure for the treatment of
 The Dialysis Prescription and Urea Modeling Biff F. Palmer Hemodialysis is a life-sustaining procedure for the treatment of patients with end-stage renal disease. In acute renal failure the procedure provides
The Dialysis Prescription and Urea Modeling Biff F. Palmer Hemodialysis is a life-sustaining procedure for the treatment of patients with end-stage renal disease. In acute renal failure the procedure provides
Dialysis induced cardiac and brain injury
 Dialysis induced cardiac and brain injury Dr Nick Selby Consultant Nephrologist, Royal Derby Hospital, UK How can dialysis hurt patients? Wasting Inflammation Infection Cognitive loss, depression Increased
Dialysis induced cardiac and brain injury Dr Nick Selby Consultant Nephrologist, Royal Derby Hospital, UK How can dialysis hurt patients? Wasting Inflammation Infection Cognitive loss, depression Increased
Online HD monitoring (BVM, OCM, BTM, etc.): Useful tools or fancy toys?
: Useful tools or fancy toys?") Online HD monitoring (BVM, OCM, BTM, etc.): Useful tools or fancy toys? Patrice Ambühl Basics in SSN/SGN Meeting, December 4 2013 patrice.ambuehl@waid.zuerich.ch Nephrologie Therapeutical dilemma Ultrafiltra
Online HD monitoring (BVM, OCM, BTM, etc.): Useful tools or fancy toys? Patrice Ambühl Basics in SSN/SGN Meeting, December 4 2013 patrice.ambuehl@waid.zuerich.ch Nephrologie Therapeutical dilemma Ultrafiltra
Strategies to assess and manage hypervolemia The invisible threat in dialysis
 Strategies to assess and manage hypervolemia The invisible threat in dialysis Rajiv Agarwal MD Professor of Medicine, Indiana University School of Medicine Volume excess is common and costly. Admission
Strategies to assess and manage hypervolemia The invisible threat in dialysis Rajiv Agarwal MD Professor of Medicine, Indiana University School of Medicine Volume excess is common and costly. Admission
Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University
 Hypertension in Hemodialysis Patient Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University Mechanism of HTN in HD patients Volume-dependent HTN ECV expansion. Volume-independent HTN
Hypertension in Hemodialysis Patient Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University Mechanism of HTN in HD patients Volume-dependent HTN ECV expansion. Volume-independent HTN
The Association between Hypoalbuminemia and Intradialytic Hypotension in Heamodialysis Patients
 The Egyptian Journal of Hospital Medicine (Apr. 2016) Vol. 63, Page 185-194 The Association between Hypoalbuminemia and Intradialytic Hypotension in Heamodialysis Patients Ezzat A. Al-Etreby, Ayaman Abd
The Egyptian Journal of Hospital Medicine (Apr. 2016) Vol. 63, Page 185-194 The Association between Hypoalbuminemia and Intradialytic Hypotension in Heamodialysis Patients Ezzat A. Al-Etreby, Ayaman Abd
DEFINITIONS FOR FLUID STATUS & TARGET WEIGHT
 Home Dialysis Interest Group HEALTHCARE TEAM TOOL DEFINITIONS FOR STATUS & TARGET WEIGHT BALANCED EXCESS DEFICIT Illustrations provided by: 1 BALANCE OF THE HOME HEMODIALYSIS PATIENT Dialysis Weight**
Home Dialysis Interest Group HEALTHCARE TEAM TOOL DEFINITIONS FOR STATUS & TARGET WEIGHT BALANCED EXCESS DEFICIT Illustrations provided by: 1 BALANCE OF THE HOME HEMODIALYSIS PATIENT Dialysis Weight**
However, Adverse Events Do Still Occur During Dialysis, Which May Be Because Of Technical Problems With The Extracorporeal Treatment, Often Combined W
 Incidence of Intradialytic Hypotension in Patients on Hemodialysis in Al Kindy Teaching Hospital Dr. *Consultant Physician Nephrologist/Head Of Faculty Of Medicine/Al Kindy College Of Medicine Abstract
Incidence of Intradialytic Hypotension in Patients on Hemodialysis in Al Kindy Teaching Hospital Dr. *Consultant Physician Nephrologist/Head Of Faculty Of Medicine/Al Kindy College Of Medicine Abstract
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Cardiovascular Complications of Dialysis In Children. Why is this important? Why is this Important? 01/26/2017. Dr Daljit Hothi
 Cardiovascular Complications of Dialysis In Children Dr Daljit Hothi Great Ormond Street Hospital, London Why is this important? 100 90 Why is this Important? Long Term Survival of Childhood Onset ESRD
Cardiovascular Complications of Dialysis In Children Dr Daljit Hothi Great Ormond Street Hospital, London Why is this important? 100 90 Why is this Important? Long Term Survival of Childhood Onset ESRD
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
UNIVERSITY OF CALGARY. Blood Volume Monitoring Guided Ultrafiltration Biofeedback on the Reduction of
 UNIVERSITY OF CALGARY Blood Volume Monitoring Guided Ultrafiltration Biofeedback on the Reduction of Intradialytic Hypotensive Episodes in Hemodialysis by Kelvin Cheuk-Wai Leung A THESIS SUBMITTED TO THE
UNIVERSITY OF CALGARY Blood Volume Monitoring Guided Ultrafiltration Biofeedback on the Reduction of Intradialytic Hypotensive Episodes in Hemodialysis by Kelvin Cheuk-Wai Leung A THESIS SUBMITTED TO THE
Chapter 2 Peritoneal Equilibration Testing and Application
 Chapter 2 Peritoneal Equilibration Testing and Application Francisco J. Cano Case Presentation FW, a recently diagnosed patient with CKD Stage 5, is a 6-year-old boy who has been recommended to initiate
Chapter 2 Peritoneal Equilibration Testing and Application Francisco J. Cano Case Presentation FW, a recently diagnosed patient with CKD Stage 5, is a 6-year-old boy who has been recommended to initiate
Cardiovascular Disease in CKD. Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center
 Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Hemocontrol. Management of Intradialytic Hypotension
 Hemocontrol Management of Intradialytic Hypotension Dialysis Complications Cramps 31% Headache 18% Vomiting 1% Nephrologische Praxen Rostock 1998-1999 Dialysis n=6,508 Hypotension 50% BP = CO X SVR Potential
Hemocontrol Management of Intradialytic Hypotension Dialysis Complications Cramps 31% Headache 18% Vomiting 1% Nephrologische Praxen Rostock 1998-1999 Dialysis n=6,508 Hypotension 50% BP = CO X SVR Potential
Chapter 9. Body Fluid Compartments. Body Fluid Compartments. Blood Volume. Blood Volume. Viscosity. Circulatory Adaptations to Exercise Part 4
 Body Fluid Compartments Chapter 9 Circulatory Adaptations to Exercise Part 4 Total body fluids (40 L) Intracellular fluid (ICF) 25 L Fluid of each cell (75 trillion) Constituents inside cell vary Extracellular
Body Fluid Compartments Chapter 9 Circulatory Adaptations to Exercise Part 4 Total body fluids (40 L) Intracellular fluid (ICF) 25 L Fluid of each cell (75 trillion) Constituents inside cell vary Extracellular
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
ASN DIALYSIS ADVISORY GROUP ASN DIALYSIS CURRICULUM
 ASN DIALYSIS ADVISORY GROUP ASN DIALYSIS CURRICULUM Medical Management of Home Hemodialysis Patients Brent W. Miller, MD Professor of Medicine Washington University School of Medicine Saint Louis, Missouri
ASN DIALYSIS ADVISORY GROUP ASN DIALYSIS CURRICULUM Medical Management of Home Hemodialysis Patients Brent W. Miller, MD Professor of Medicine Washington University School of Medicine Saint Louis, Missouri
A Randomized, Controlled Trial of Albumin versus Saline for the Treatment of Intradialytic Hypotension
 J Am Soc Nephrol 15: 487 492, 2004 A Randomized, Controlled Trial of Albumin versus Saline for the Treatment of Intradialytic Hypotension GREG A. KNOLL,* JENNY A. GRABOWSKI, GEOFFREY F. DERVIN, and KEITH
J Am Soc Nephrol 15: 487 492, 2004 A Randomized, Controlled Trial of Albumin versus Saline for the Treatment of Intradialytic Hypotension GREG A. KNOLL,* JENNY A. GRABOWSKI, GEOFFREY F. DERVIN, and KEITH
Hemodialysis: slightly beyond basics Dialysate calcium and magnesium concentrations
 Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Attending Rounds. Attending Rounds: A Patient with Intradialytic Hypotension
 Attending Rounds Attending Rounds: A Patient with Intradialytic Hypotension Robert F. Reilly Abstract Intradialytic hypotension is the most common adverse event that occurs during the hemodialysis procedure.
Attending Rounds Attending Rounds: A Patient with Intradialytic Hypotension Robert F. Reilly Abstract Intradialytic hypotension is the most common adverse event that occurs during the hemodialysis procedure.
Contrast Induced Nephropathy
 Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Vital Sign Variations with Complications during Dialysis among End-Stage Renal Disease Patients
 ORIGINAL ARTICLE Vital Sign Variations with Complications during Dialysis among End-Stage Renal Disease Patients ABSTRACT Abdul Rehman Qureshi 1, Naureen Durrani 2 and Naila Asif 3 Objective: To analyse
ORIGINAL ARTICLE Vital Sign Variations with Complications during Dialysis among End-Stage Renal Disease Patients ABSTRACT Abdul Rehman Qureshi 1, Naureen Durrani 2 and Naila Asif 3 Objective: To analyse
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury Care in the Chronic Unit
 Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
AJNT. Original Article
 . 2012 Sep;5(3):129-34 Original Article AJNT Applying Sodium Profile with or without Ultrafiltration Profile Failed to Show Beneficial Effects on the Incidence of Intradialytic Hypotension in Susceptible
. 2012 Sep;5(3):129-34 Original Article AJNT Applying Sodium Profile with or without Ultrafiltration Profile Failed to Show Beneficial Effects on the Incidence of Intradialytic Hypotension in Susceptible
The main determinants of intradialysis hypertension during dialysis in chronic hemodialysis patients; a single-center study
 J Renal Inj Prev. 2018; 7(3): 152-159. http://journalrip.com Journal of Renal Injury Prevention DOI: 10.15171/jrip.2018.38 The main determinants of intradialysis hypertension during dialysis in chronic
J Renal Inj Prev. 2018; 7(3): 152-159. http://journalrip.com Journal of Renal Injury Prevention DOI: 10.15171/jrip.2018.38 The main determinants of intradialysis hypertension during dialysis in chronic
Predilution hemodiafiltration displays no hemodynamic advantage over low-flux hemodialysis under matched conditions
 Kidney International, Vol. 67 (2005), pp. 1601 1608 Predilution hemodiafiltration displays no hemodynamic advantage over low-flux hemodialysis under matched conditions NIKOLAOS KARAMPERIS,ERIK SLOTH, and
Kidney International, Vol. 67 (2005), pp. 1601 1608 Predilution hemodiafiltration displays no hemodynamic advantage over low-flux hemodialysis under matched conditions NIKOLAOS KARAMPERIS,ERIK SLOTH, and
Characteristics of hypotension-prone haemodialysis patients: is there a critical relative blood volume?
 Nephrol Dial Transplant (2003) 18: 1353 1360 DOI: 10.1093/ndt/gfg171 Original Article Characteristics of hypotension-prone haemodialysis patients: is there a critical relative blood volume? Claudia Barth
Nephrol Dial Transplant (2003) 18: 1353 1360 DOI: 10.1093/ndt/gfg171 Original Article Characteristics of hypotension-prone haemodialysis patients: is there a critical relative blood volume? Claudia Barth
Left ventricular hypertrophy: why does it happen?
 Nephrol Dial Transplant (2003) 18 [Suppl 8]: viii2 viii6 DOI: 10.1093/ndt/gfg1083 Left ventricular hypertrophy: why does it happen? Gerard M. London Department of Nephrology and Dialysis, Manhes Hospital,
Nephrol Dial Transplant (2003) 18 [Suppl 8]: viii2 viii6 DOI: 10.1093/ndt/gfg1083 Left ventricular hypertrophy: why does it happen? Gerard M. London Department of Nephrology and Dialysis, Manhes Hospital,
Innovations in Cardio/Renal Patient Care. Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health at San Antonio Spring Symposium 2018
 Innovations in Cardio/Renal Patient Care Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health at San Antonio Spring Symposium 2018 Percent of Patients CVD = cardiovascular disease; ASHD =
Innovations in Cardio/Renal Patient Care Shweta Bansal, MD, FASN Associate Professor of Medicine UT Health at San Antonio Spring Symposium 2018 Percent of Patients CVD = cardiovascular disease; ASHD =
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
Sodium removal during pre-dilution haemofiltration
 Nephrol Dial Transplant (2003) 18 [Suppl 7]: vii31 vii36 DOI: 10.1093/ndt/gfg1076 Sodium removal during pre-dilution haemofiltration Salvatore Di Filippo, Celestina Manzoni, Simeone Andrulli, Francesca
Nephrol Dial Transplant (2003) 18 [Suppl 7]: vii31 vii36 DOI: 10.1093/ndt/gfg1076 Sodium removal during pre-dilution haemofiltration Salvatore Di Filippo, Celestina Manzoni, Simeone Andrulli, Francesca
28-Feb-10 Reza Sabagh
 DIALYSIS EQUIPMENTS (DIALYSIS MACHINE & R.O) Nursing Conference on Dialysis Tehran 1 The standard dialysis machines are designed for performing chronic and acute hemodialysis. They can be used in home
DIALYSIS EQUIPMENTS (DIALYSIS MACHINE & R.O) Nursing Conference on Dialysis Tehran 1 The standard dialysis machines are designed for performing chronic and acute hemodialysis. They can be used in home
Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are
 Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Achieve. Achieve. More Effective. Dialysis Treatment
 Achieve More Effective Achieve Dialysis Treatment The Crit-Line monitor measures the following: Real-time, lab-equivalent, non-invasive hematocrit (HCT) Real-time percent changes in intravascular blood
Achieve More Effective Achieve Dialysis Treatment The Crit-Line monitor measures the following: Real-time, lab-equivalent, non-invasive hematocrit (HCT) Real-time percent changes in intravascular blood
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Plasma sodium as a predictor of death and non-osmotic sodium storage
 An update on sodium in CKD stage 5D Plasma sodium as a predictor of death and non-osmotic sodium storage Prof. Mustafa ARICI, MD Hacettepe University Faculty of Medicine Ankara-TURKEY 2 (new) questions...
An update on sodium in CKD stage 5D Plasma sodium as a predictor of death and non-osmotic sodium storage Prof. Mustafa ARICI, MD Hacettepe University Faculty of Medicine Ankara-TURKEY 2 (new) questions...
The Cardiorenal Syndrome in Heart Failure
 The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
Nephrology Unit- CHU Liège- Ulg- Belgium
 Are the complications of arteriovenous fistulas associated with an abnormal Ankle-Brachial Index in Hemodialysis? A 4y study P. Xhignesse, A. Saint-Remy, B. Dubois, JC. Philips, JM. Krzesinski Nephrology
Are the complications of arteriovenous fistulas associated with an abnormal Ankle-Brachial Index in Hemodialysis? A 4y study P. Xhignesse, A. Saint-Remy, B. Dubois, JC. Philips, JM. Krzesinski Nephrology
2016 Annual Dialysis Conference Michelle Hofmann RN, BSN, CNN Renal Clinical Educator - Home
 Fluid Management 2016 Annual Dialysis Conference Michelle Hofmann RN, BSN, CNN Renal Clinical Educator - Home Objectives Define euvolemia Determine factors which contribute to fluid imbalance Discuss strategies
Fluid Management 2016 Annual Dialysis Conference Michelle Hofmann RN, BSN, CNN Renal Clinical Educator - Home Objectives Define euvolemia Determine factors which contribute to fluid imbalance Discuss strategies
The evaluation of relationship between blood pressure and dialysate Na concentration in chronic hemodialysis patients
 J Renal Inj Prev. 2016; 5(3): 118-122. Journal of Renal Injury Prevention DOI: 10.15171/jrip.2016.25 The evaluation of relationship between blood pressure and dialysate Na concentration in chronic hemodialysis
J Renal Inj Prev. 2016; 5(3): 118-122. Journal of Renal Injury Prevention DOI: 10.15171/jrip.2016.25 The evaluation of relationship between blood pressure and dialysate Na concentration in chronic hemodialysis
Ultrafiltration Programs : Clinical Experiences
 Ultrafiltration Programs : Clinical Experiences By : Kay Woodruff, RN, BS, CNN, Divisional Clinical Specialist Lisa Miller Hedin, RN, CNN, Senior Clinical Specialist Introduction The purpose of this article
Ultrafiltration Programs : Clinical Experiences By : Kay Woodruff, RN, BS, CNN, Divisional Clinical Specialist Lisa Miller Hedin, RN, CNN, Senior Clinical Specialist Introduction The purpose of this article
Hemodiafiltration: principles and advantages over conventional HD. Rukshana Shroff Great Ormond Street Hospital for Children London, UK
 Hemodiafiltration: principles and advantages over conventional HD Rukshana Shroff Great Ormond Street Hospital for Children London, UK Effectiveness of RRT modalities Mcfarlane, Seminars in dialysis, 2009
Hemodiafiltration: principles and advantages over conventional HD Rukshana Shroff Great Ormond Street Hospital for Children London, UK Effectiveness of RRT modalities Mcfarlane, Seminars in dialysis, 2009
Cardiorenal Syndrome
 Cardiorenal Syndrome Peenida Skulratanasak, M.D. Division of Nephrology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University Definition of Cardiorenal syndrome (CRS) Structural
Cardiorenal Syndrome Peenida Skulratanasak, M.D. Division of Nephrology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University Definition of Cardiorenal syndrome (CRS) Structural
RJ Picciano BA, CHT, OCDT, CHBT Fluid Management Coordinator Centers for Dialysis Care, Cleveland Ohio BONENT President
 FLUID MANAGEMENT: WHAT THE NEPHROLOGY TECHNICIAN CAN DO TO HELP? RJ Picciano BA, CHT, OCDT, CHBT Fluid Management Coordinator Centers for Dialysis Care, Cleveland Ohio BONENT President Lori Poole MSN,
FLUID MANAGEMENT: WHAT THE NEPHROLOGY TECHNICIAN CAN DO TO HELP? RJ Picciano BA, CHT, OCDT, CHBT Fluid Management Coordinator Centers for Dialysis Care, Cleveland Ohio BONENT President Lori Poole MSN,
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Acute Kidney Injury. APSN JSN CME for Nephrology Trainees May Professor Robert Walker
 Acute Kidney Injury APSN JSN CME for Nephrology Trainees May 2017 Professor Robert Walker Kidney International (2017) 91, 1033 1046; http://dx.doi.org/10.1016/ j.kint.2016.09.051 Case for discussion 55year
Acute Kidney Injury APSN JSN CME for Nephrology Trainees May 2017 Professor Robert Walker Kidney International (2017) 91, 1033 1046; http://dx.doi.org/10.1016/ j.kint.2016.09.051 Case for discussion 55year
Advances in Peritoneal Dialysis, Vol. 29, 2013
 Advances in Peritoneal Dialysis, Vol. 29, 2013 Takeyuki Hiramatsu, 1 Takahiro Hayasaki, 1 Akinori Hobo, 1 Shinji Furuta, 1 Koki Kabu, 2 Yukio Tonozuka, 2 Yoshiyasu Iida 1 Icodextrin Eliminates Phosphate
Advances in Peritoneal Dialysis, Vol. 29, 2013 Takeyuki Hiramatsu, 1 Takahiro Hayasaki, 1 Akinori Hobo, 1 Shinji Furuta, 1 Koki Kabu, 2 Yukio Tonozuka, 2 Yoshiyasu Iida 1 Icodextrin Eliminates Phosphate
Blood Pressure Fox Chapter 14 part 2
 Vert Phys PCB3743 Blood Pressure Fox Chapter 14 part 2 T. Houpt, Ph.D. 1 Cardiac Output and Blood Pressure How to Measure Blood Pressure Contribution of vascular resistance to blood pressure Cardiovascular
Vert Phys PCB3743 Blood Pressure Fox Chapter 14 part 2 T. Houpt, Ph.D. 1 Cardiac Output and Blood Pressure How to Measure Blood Pressure Contribution of vascular resistance to blood pressure Cardiovascular
Drug Use in Dialysis
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
(Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS
 FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
Future Perspectives in Peritoneal Dialysis
 Future Perspectives in Peritoneal Dialysis Dialysis Initiatives Nefrologen Meeting September 21, 2017 Joanne M. Bargman MD FRCPC Director, Peritoneal Dialysis Program University Health Network Professor
Future Perspectives in Peritoneal Dialysis Dialysis Initiatives Nefrologen Meeting September 21, 2017 Joanne M. Bargman MD FRCPC Director, Peritoneal Dialysis Program University Health Network Professor
Fluid and electrolyte balance, imbalance
 Fluid and electrolyte balance, imbalance Body fluid The fluids are distributed throughout the body in various compartments. Body fluid is composed primarily of water Water is the solvent in which all solutes
Fluid and electrolyte balance, imbalance Body fluid The fluids are distributed throughout the body in various compartments. Body fluid is composed primarily of water Water is the solvent in which all solutes
PREVALENCE AND TYPES OF INTRA-DIALYTIC COMPLICATIONS IN PATIENTS DIALYSING AT THE UNIVERSITY OF BENIN TEACHING HOSPITAL
 PREVALENCE AND TYPES OF INTRA-DIALYTIC COMPLICATIONS IN PATIENTS DIALYSING AT THE UNIVERSITY OF BENIN TEACHING HOSPITAL ADEJUMO OA, OLOKOR AB, IYAWE IO, OKAKA EI, UNUIGBE EI, OJOGWU LI Presented at Nigerian
PREVALENCE AND TYPES OF INTRA-DIALYTIC COMPLICATIONS IN PATIENTS DIALYSING AT THE UNIVERSITY OF BENIN TEACHING HOSPITAL ADEJUMO OA, OLOKOR AB, IYAWE IO, OKAKA EI, UNUIGBE EI, OJOGWU LI Presented at Nigerian
Efficacy of stepwise sodium profile versus individualized dialysate sodium in blood pressure control among hemodialysis patients
 Original Article Efficacy of stepwise profile versus individualized dialysate in control among hemodialysis patients Nahid Shahgholian 1, Maryam Sadat Hashemi 2, Shahrzade Shahidi 3 ABSTRACT Background:
Original Article Efficacy of stepwise profile versus individualized dialysate in control among hemodialysis patients Nahid Shahgholian 1, Maryam Sadat Hashemi 2, Shahrzade Shahidi 3 ABSTRACT Background:
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
INTRADIALYTIC DOPAMINE THERAPY IN MAINTENANCE HEMODIALYSIS PATIENTS WITH PERSISTENT HYPOTENSION
 Original Article 22 INTRADIALYTIC DOPAMINE THERAPY IN MAINTENANCE HEMODIALYSIS PATIENTS WITH PERSISTENT HYPOTENSION Wen-Yuan Chiu, Horng-Rong Chang *, Zyh-Zan Lin **, Enny Halim, Jong-Da Lian * Intradialytic
Original Article 22 INTRADIALYTIC DOPAMINE THERAPY IN MAINTENANCE HEMODIALYSIS PATIENTS WITH PERSISTENT HYPOTENSION Wen-Yuan Chiu, Horng-Rong Chang *, Zyh-Zan Lin **, Enny Halim, Jong-Da Lian * Intradialytic
OT Exam 3, August 19, 2002 Page 1 of 6. Occupational Therapy Physiology, Summer Examination 3. August 19, 2002
 Page 1 of 6 Occupational Therapy Physiology, Summer 2002 Examination 3 August 19, 2002 There are 20 questions and each question is worth 5 points for a total of 100 points. Dr. Heckman's section is questions
Page 1 of 6 Occupational Therapy Physiology, Summer 2002 Examination 3 August 19, 2002 There are 20 questions and each question is worth 5 points for a total of 100 points. Dr. Heckman's section is questions
There are no shortcuts to Dialysis
 There are no shortcuts to Dialysis 1 Outcomes John Sweeny Wednesday, March 21 st, 2018 (3:10 pm 4:10 pm) 2 Quality in Hemodialysis Quality Health Care is the degree to which health services increases the
There are no shortcuts to Dialysis 1 Outcomes John Sweeny Wednesday, March 21 st, 2018 (3:10 pm 4:10 pm) 2 Quality in Hemodialysis Quality Health Care is the degree to which health services increases the
The Triple Threat. Cardiac Care in the NT Annual Workshop 2017 is proudly supported by:
 The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Acute Kidney Injury- What Is It and How Do I Treat It?
 Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Intradialytic hypertension is a marker of volume excess
 Nephrol Dial Transplant (2010) 1 of 6 doi: 10.1093/ndt/gfq210 NDT Advance Access published April 16, 2010 Original Article Intradialytic hypertension is a marker of volume excess Rajiv Agarwal 1,2 and
Nephrol Dial Transplant (2010) 1 of 6 doi: 10.1093/ndt/gfq210 NDT Advance Access published April 16, 2010 Original Article Intradialytic hypertension is a marker of volume excess Rajiv Agarwal 1,2 and
BIOL 2402 Fluid/Electrolyte Regulation
 Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
Vasopressin secretion by hypertonic saline infusion during hemodialysis: effect of cardiopulmonary recirculation
 Nephrol Dial Transplant (2011) 0: 1 8 doi: 10.1093/ndt/gfr272 NDT Advance Access published June 1, 2011 Original Article Vasopressin secretion by hypertonic saline infusion during hemodialysis: effect
Nephrol Dial Transplant (2011) 0: 1 8 doi: 10.1093/ndt/gfr272 NDT Advance Access published June 1, 2011 Original Article Vasopressin secretion by hypertonic saline infusion during hemodialysis: effect
Hemodynamic Instability in HD patients: Dialysis Hypotension Prof Ali BAŞÇI MD FERA Ege University Medical School
 Hemodynamic Instability in HD patients: Dialysis Hypotension Prof Ali BAŞÇI MD FERA Ege University Medical School Relationship between blood pressure and mortality in patients treated with volume control
Hemodynamic Instability in HD patients: Dialysis Hypotension Prof Ali BAŞÇI MD FERA Ege University Medical School Relationship between blood pressure and mortality in patients treated with volume control
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum