ASA PLAVIX AND PREOPERATIVE OPTIMIZATION. John Hann, MD
|
|
|
- Easter McKinney
- 5 years ago
- Views:
Transcription
1 ASA PLAVIX AND PREOPERATIVE OPTIMIZATION John Hann, MD
2 QUESTIONS: WHICH ANTI-PLATELETS DO YOU STOP AND WHEN? yo M with history of stroke on ASA PreOp eval for cataracts surgery yo M with RCRI of 4 on ASA undergoing open cholecystectomy for malignant neoplasm resection yo M with DES in 2007 on ASA and Plavix undergoing laparoscopic cholecystectomy for cholelithiasis yo M with DES on Halloween of 2017 (4 weeks ago) on ASA and Plavix undergoing TURP for BPH yo M with DES in 2012 on ASA and Plavix undergoing malignant, infratentorial neoplasm resection yo M with DES on Thanksgiving of 2017 on ASA and Plavix undergoing cystectomy for urothelial cancer
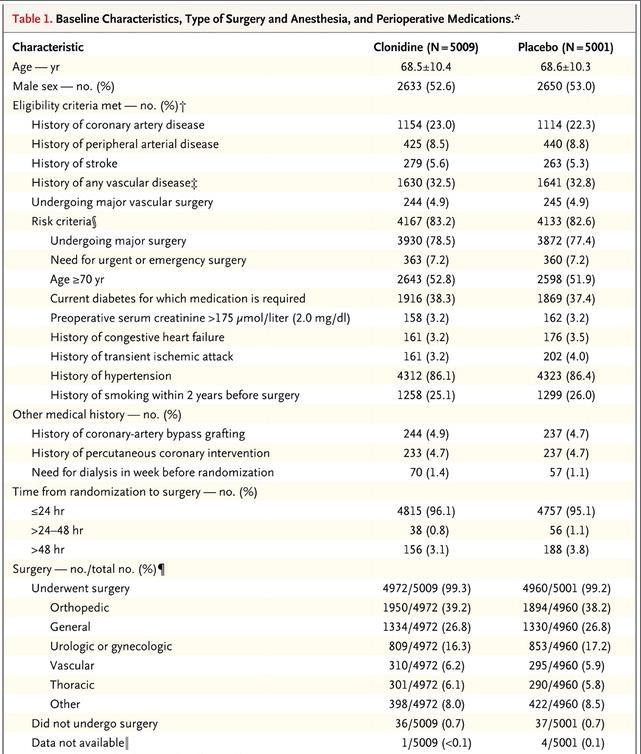
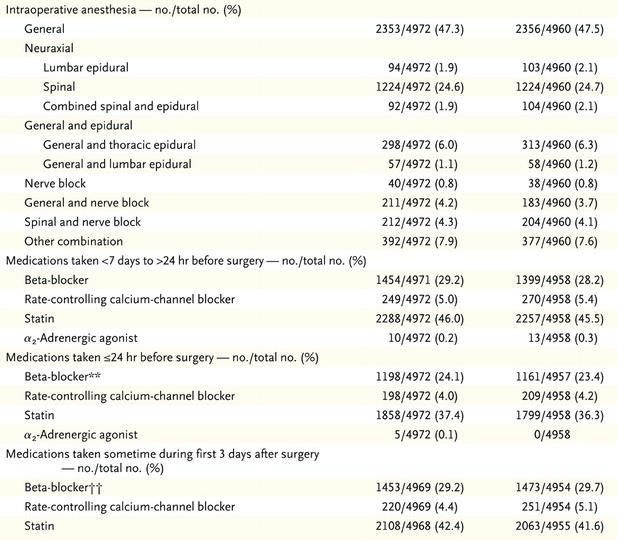
3 POISE-2: PERIOPERATIVE ISCHEMIC EVALUATION international, randomized, controlled trial designed to separately evaluate the effects of aspirin versus placebo and clonidine versus placebo in patients undergoing noncardiac surgery. Clonidine was used vs ASA because of the belief that clonidine may suppress the sympathetic nervous system thus possibly preventing MI it did not. Results showed that Clonididine worsened outcomes Patients also received aspirin or placebo just before surgery and continued receiving it daily throughout the postoperative period. Patients in both ASA strata receive the same trial ASA intervention (ie, either ASA 100 mg or matching placebo). For the first dose prior to surgery (goal 2-4 hours), they take 2 tablets orally. Starting on the day after surgery, patients take 1 tablet daily for 30 days in the Starting Stratum and 7 days in the Continuation Stratum, after which they resume their regular ASA.
4 ELIGIBILITY CRITERIA FOR POISE 2
5 EXCLUSION CRITERIA FOR POISE 2
6
.")
.")
7 Side note: The initiation strata of ASA had lower risk of stroke compared to placebo (3 strokes in ASA vs 12 in placebo). However, in the continuation strata there were more strokes in the ASA group (13 in ASA and 7 in placebo). Combined the data do not show statistically significant differences of combined ASA takers.
8
9
10
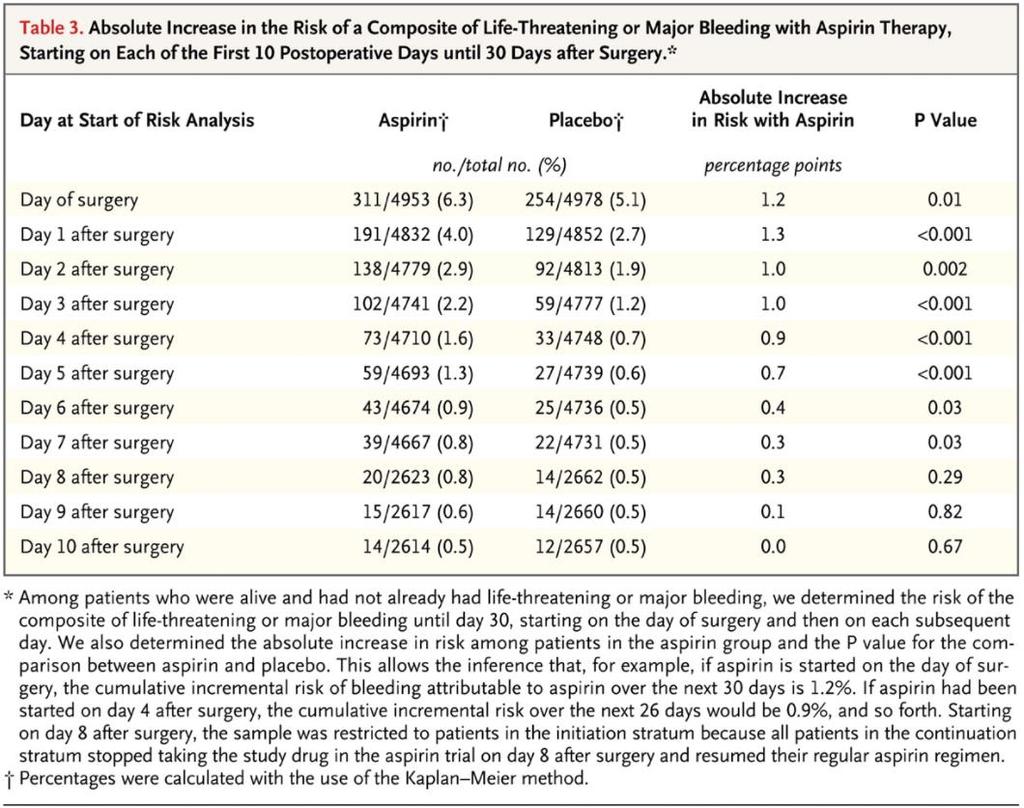
11 CONCLUSION OF THIS STUDY Even for individuals with significantly elevated RCRI, there was no difference in outcomes of those on aspirin and those not on aspirin EXCEPT that those who were not on ASA had an increased risk for major bleeding and dialysis But: There was one important subgroup of participants who were not singled out in the results.
12 WHAT HAPPENS WHEN ASA IS STOPPED IN THE SETTING OF STENT Biondi-Zoccai et al. performed a meta-analyses of 50,279 patients for secondary prevention for coronary artery disease which showed that the cardiac complication rate was three times higher after ASA withdrawal and increased even more in patients with coronary stents. There was, on average, a 10.6-day period between withdrawal from ASA and thrombotic events (8.5 days for coronary symptoms). A survey conducted on 374 interventional cardiologists found that although there is agreement among interventional cardiologists on the optimum delay for surgery after stenting, on the need for BMS or balloon angioplasty alone if early noncardiac surgery is needed, and on treatment of perioperative thrombosis, there is significant inconsistency on the optimum antiplatelet therapy for patients who need surgery early after stent implantation The Poise-2 trial conclusion did not explicitly address this population
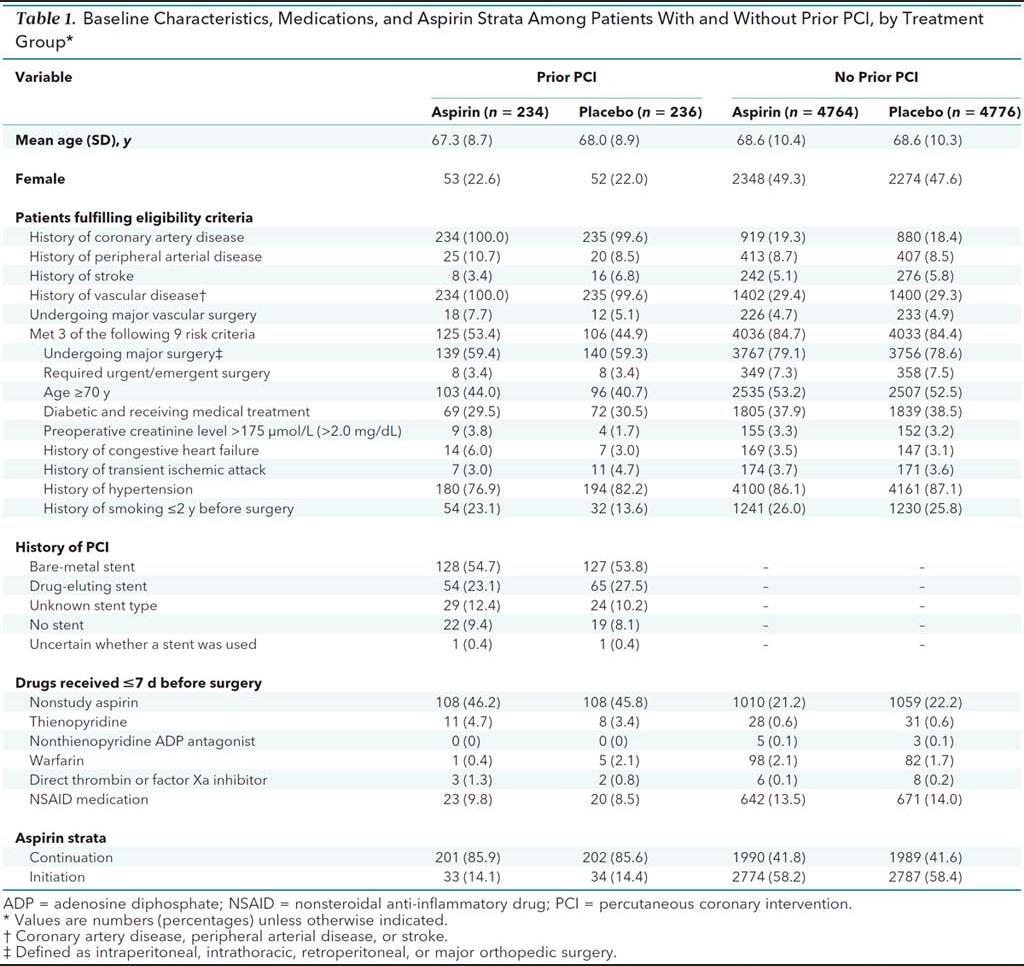
13 THANK YOU AMISH: LOW-DOSE ASPIRIN TO REDUCE THE RISK FOR MYOCARDIAL INFARCTION AMONG PATIENTS WITH CORONARY STENTS UNDERGOING NONCARDIAC SURGERY Approximately 5% to 25% of patients having PCI may require noncardiac surgery within 5 years after stent implantation Cardiovascular adverse events are the leading cause of morbidity and mortality after noncardiac surgery, and myocardial infarction accounts for most of these adverse events
14
15 EFFECT OF ASPIRIN ON RISK FOR COMPOSITE OF DEATH AND NONFATAL MYOCARDIAL INFARCTION AMONG PATIENTS WITH A HISTORY OF PERCUTANEOUS CORONARY INTERVENTION.

16 Uncertainty Uncertainty
17 EFFECT OF ASPIRIN ON RISK FOR MAJOR BLEEDING AMONG PATIENTS WITH A HISTORY OF PERCUTANEOUS CORONARY INTERVENTION.
18
19 The results, then, suggest that for every 1000 patients with prior PCI who have noncardiac surgery, administration of perioperative aspirin would prevent 59 myocardial infarctions (CI, 10 to 108 myocardial infarctions) and cause 8 major bleeding On the basis of this study's findings, 17 patients with prior PCI (95% CI, 9 to 100 patients) would need to be treated with aspirin to prevent 1 myocardial infarction during the perioperative period, the editorialists wrote. If we consider the 22% higher relative risk for major or life-threatening bleeding events associated with aspirin, only surgical procedures with a very high baseline bleeding risk ( 26%) would neutralize aspirin's ischemic benefit. The study included only 470 patients with prior PCI and they had few events, which creates imprecision in the estimates of effect.
20 TAKE HOME FROM THIS SUB GROUP ANALYSIS Patients with prior PCI do have significantly higher risk of MI if ASA is held It is unclear if this population has a higher bleeding risk. Regardless, the bleeding risk of the surgery must be much higher to outweigh the risk of MI
21 HOW LONG TO HOLD ASA If you need to hold ASA, how long should you hold it? Common recommendation are to hold the drug 7 10 days before surgery to ensure that the platelets are functioning once again well. However, mean time for occlusion of stent is approximately 10 days following discontinuation of ASA, so what is optimal time? The following study consisted of 14 healthy, untreated, male volunteers aged years and 58 male and female (all postmenopausal) patients receiving regular treatment with 100 mg aspirin who were scheduled for elective orthopaedic or urological surgery at a major tertiary medical centre.
22
23
24
25
26
27
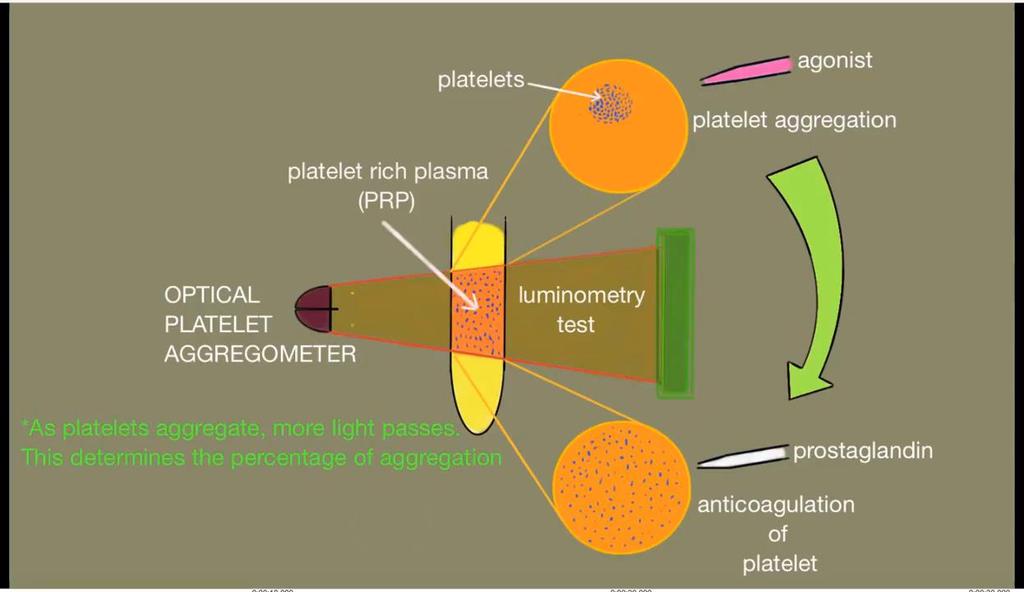
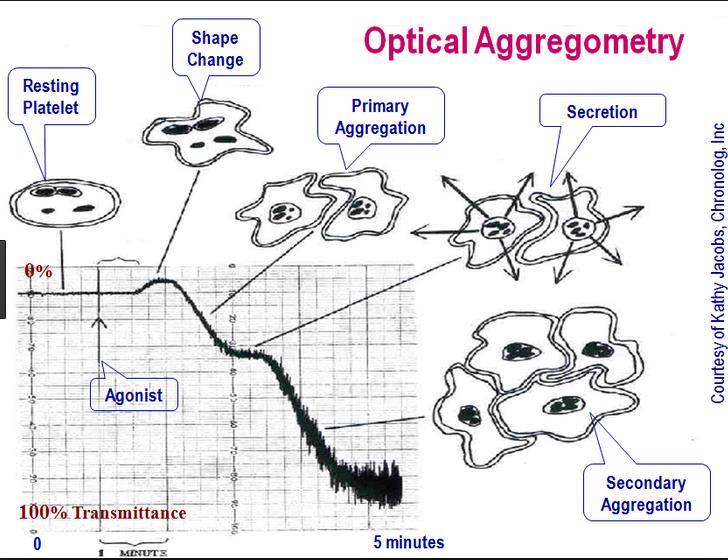
28 CONCLUSIONS The recommendation to wait 7 10 days until platelet function recovers is based on the assumption that aspirin inhibition of platelet COX is irreversible and neutralizes platelets for their whole lifespan. However, in the present study, according to the aggregometry measurements with both agonists, platelet function recovered earlier: after 3 days in volunteers and after 4 days in most patients. To explain this finding, we suggest that the effect of aspirin on megakaryocytes in bone marrow is not permanent, in contrast to platelets that are permanently impaired by the action of aspirin and are later removed from the circulation. Weaknesses of the study: More men then women They chose not to apply the same protocols of the two groups since it would be unethical to do daily blood draws of the patients They did not evaluate the clinical response They had a small sample size.
29 CONCLUSIONS CONTINUED In the majority of the patients treated with aspirin, platelet function recovers in 4 days after aspirin cessation compared with 3 days in healthy volunteers. Despite the fact that platelet function recovers after 4 days in the majority of patients, some patients might nevertheless have delayed recovery. We, therefore, suggest that the duration of aspirin cessation before elective surgical procedures with a high risk of potential bleeding should be 6 days, and that platelets should be monitored by aggregometry if this is not feasible. From the POISE 2: Studies have suggested that hemostasis is unimpaired if at least 20% of the platelets have normal COX-1 activity and 12% of circulating platelets are replaced every 24 hours. Therefore, stopping aspirin 72 or more hours before surgery may be adequate to minimize the risk of perioperative bleeding.
30 PERIOPERATIVE ANTIPLATELET IN THE SETTING OF DES PCI-CURE study (2002) in in which 2658 patients with ACS underwent PCI. Clopidogrel w/ ASA vs ASA alone. 31% reduction (p = 0.002) of cardiovascular mortality or myocardial infarction (MI) rate was observed in the clopidogrel group The difference between both groups appears during the first 3 months, and stays constant or slightly increases up to 12 months. Updated guidelines in 2016: In patients with ACS (NSTE-ACS or STEMI) treated with coronary stent implantation who have tolerated DAPT without a bleeding complication and who are not at high bleeding risk (e.g., prior bleeding on DAPT, coagulopathy, oral anticoagulant use), continuation of DAPT (clopidogrel, prasugrel, or ticagrelor) for longer than 12 months may be reasonable (Class IIb).
31
32 RECOVERY OF PLATELET FUNCTION AFTER DISCONTINUATION OF CLOPIDOGREL TREATMENT IN HEALTHY VOLUNTEERS Flow Cytometry Adenosine diphosphate (ADP, 30 µm)-induced platelet responses were almost completely inhibited by clopidogrel. after discontinuation of clopidogrel treatment, platelet function gradually recovers and that a complete restoration of ADP-induced platelet responses occurs 7 days after the last clopidogrel dose Thus, our data are compatible with the view that the inhibitory effects of clopidogrel are terminated by de novo formed platelets.
33 CLINICAL RELEVANCE: CURE TRIAL CLOPIDOGREL IN UNSTABLE ANGINA TO PREVENT RECURRENT EVENTS In a subgroup analysis of 912 patients who had stopped clopidogrel less than 5 days before CABG surgery in the CURE trial (Yusuf et al 2001) there was increased risk of minor bleeding (5.1% clopidogrel vs 2.4% placebo, p<0.001) and a trend towards an increased risk of major bleeding (9.6% clopidogrel vs 6.3% placebo, p=0.06) among patients in the clopidogrel group compared with placebo. In contrast, there was no excess of major bleeding after CABG surgery among patients who discontinued clopidogrel at least 5 days prior to surgery (4.4% clopidogrel vs 5.3% placebo; p=0.53).
34 CURE TRIAL APPLIED TO CARDIAC CASES, HOWEVER. Evidence to continue Plavix: A study of 647 patients undergoing vascular surgery and receiving DAPT with clopidogrel and ASA up to the day of surgery concluded that maintenance of DAPT is not associated with increased bleeding complications or transfusion requirements Another registry of patients undergoing vascular procedures (carotid endarterectomy, lower extremity bypass, endovascular aneurysm repair, or open abdominal aortic aneurysm repair) found that bleeding, transfusion requirements, and reoperation rates for bleeding were similar among the four patient groups based on an antiplatelet regimen (ASA vs ASA plus clopidogrel vs clopidogrel vs no antiplatelet therapy). Patients undergoing thoracic surgery do not seem to experience increased bleeding while on clopidogrel, but the incidence of perioperative MI is significantly higher among patients with stents discontinuing DAPT in the perioperative period Urological surgery, with the exception of transurethral resection of prostate, can be safely performed while on DAPT However, customary practice among urologists is to stop DAPT before cystoprostatectomy or nephrectomy due to concerns of increased bleeding. 152 In patients undergoing intra-abdominal surgery, data suggest that these operations can be safely performed while continuing DAPT. 153 Evidence to Hold Plavix: Severe complications are eight times more likely after Mohs procedures in patients on DAPT than in control subjects taking ASA monotherapy Patients on DAPT undergoing orthopaedic surgery (especially patients undergoing hip and knee replacement) have an increase in bleeding complications and increased risk of transfusion in the operating theatre or in the first 24 h after operation. 145 Another study concluded that stopping clopidogrel 5 days before operation might decrease the risk of complications, although mortality is not influenced. 146 These findings are in contrast with data from patients undergoing hip fracture surgeries, who demonstrate no increase in transfusion requirements when taking clopidogrel.
35 ACC/AHA RECOMMENDATIONS DIRECTLY FOLLOWING DES Class I 1. Elective noncardiac surgery should be delayed 14 days after balloon angioplasty (Level of Evidence: C) and 30 days after BMS implantation (99 101). (Level of Evidence B) Elective noncardiac surgery should optimally be delayed 365 days after drugeluting stent (DES) implantation ( ). (Level of Evidence: B) Class II 1. In patients in whom noncardiac surgery is required, a consensus decision among treating clinicians as to the relative risks of surgery and discontinuation or continuation of antiplatelet therapy can be useful.. Elective noncardiac surgery after DES implantation may be considered after 180 days if the risk of further delay is greater than the expected risks of ischemia and stent thrombosis
36 TAKE HOME POINTS For elevated risk surgery, even for elevated RCRI, ASA does not improve risk of MI and increases risk of bleed For CAD with Stent, ASA has been proven to be beneficial perioperatively and should be continued in all but the highest risk bleeding surgery ASA usually is out of the system by 5 days, but effects may be resolved in as little as 3 days Plavix should be continued following DES for 180 days minimum, 365 best. Can consider, with discussion with surgeon, continuing Plavix even on higher risk bleeding surgery
37 QUESTIONS: WHICH ANTI-PLATELETS DO YOU STOP AND WHEN? yo M with history of stroke on ASA PreOp eval for cataracts surgery 1. Very low risk bleeding, high risk stroke: Continue ASA yo M with RCRI of 4 on ASA undergoing open cholecystectomy for malignant neoplasm resection 2. Higher risk bleeding (neoplasm), though elevated RCRI, no increased risk of MI, therefore hold ASA yo M with DES in 2007 on ASA and Plavix undergoing laparoscopic cholecystectomy for 3. Low risk surgery bleeding, high risk thrombosis, continue DAPT cholelithiasis yo M with DES on Halloween of 2017 (4 weeks ago) on ASA and Plavix undergoing TURP for BPH 4. Wait 365 days, elevated, but not 20% bleeding, therefore cont ASA, likely hold Plavix 5 days yo M with DES in 2012 on ASA and Plavix undergoing malignant, infratentorial neoplasm resection 5. High bleeding risk, closed space. Hold ASA 3-5 days, Plavix 5 days. Consider agglutination test yo M with DES on Thanksgiving of 2017 on ASA and Plavix undergoing cystectomy for urothelial cancer 6. Tough: too soon for surgery which can wait weeks, but 6-12 months. Best to wait min until 4-6 weeks post stent, then likely consider continue both after discussion of bleeding risk with surgeon.
38 REFERRENCES POISE trial references ASA in patients undergoing noncardiac surgery (POISE-2): Rational for Poise2 study: Duration of platelets: and and and
39 REFERENCES Antithrombotics in the setting of DES AHA guidelines: main.pdf?_tid=0829dad4-c7dc-11e aacb361&acdnat= _b09e0e5b0e59aaff306bfdc4b6b6757d Amish send out article Editorial: Primary article:
40 PLATELET FUNCTION TIME ASA Platelet function recovery after cessation of aspirin: preliminary study of volunteers and surgical patients Zisman, Eliyahu; Erport, Angelika; Kohanovsky, Eugene; Ballagulah, Marc; Cassel, Aliza; Quitt, Miriam; Pizov, Reuven
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Preoperative Management of Patients Receiving Antithrombotics
 Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
COAGULATION, BLEEDING, AND TRANSFUSION IN URGENT AND EMERGENCY CORONARY SURGERY
 COAGULATION, BLEEDING, AND TRANSFUSION IN URGENT AND EMERGENCY CORONARY SURGERY VALTER CASATI, M.D. DIVISION OF CARDIOVASCULAR ANESTHESIA AND INTENSIVE CARE CLINICA S. GAUDENZIO NOVARA (ITALY) ANTIPLATELET
COAGULATION, BLEEDING, AND TRANSFUSION IN URGENT AND EMERGENCY CORONARY SURGERY VALTER CASATI, M.D. DIVISION OF CARDIOVASCULAR ANESTHESIA AND INTENSIVE CARE CLINICA S. GAUDENZIO NOVARA (ITALY) ANTIPLATELET
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Guidelines PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42. Prominent Dutch Cardiovascular Researcher Fired for Scientific Misconduct
 PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
2010, Metzler Helfried
 Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality
 Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
 ACETYL SALICYLIC ACID TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
ACETYL SALICYLIC ACID TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
SESSION 5 2:20 3:35 pm
 SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome'
 'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Scope of the Problem: DAPT and Triple Therapy after Stenting
 Scope of the Problem: DAPT and Triple Therapy after Stenting Kurt Huber, MD, FESC, FACC 3 rd Medical Department Cardiology & Emergency Medicine Wilhelminenhospital Vienna, Austria Session, August 30, 2010,
Scope of the Problem: DAPT and Triple Therapy after Stenting Kurt Huber, MD, FESC, FACC 3 rd Medical Department Cardiology & Emergency Medicine Wilhelminenhospital Vienna, Austria Session, August 30, 2010,
Mayor lung resection in the presence of anti-platelet therapy. Hans-Beat Ris Service de Chirurgie Thoracique CHUV, Lausanne
 Mayor lung resection in the presence of anti-platelet therapy Hans-Beat Ris Service de Chirurgie Thoracique CHUV, Lausanne THORACIC SURGERY IN THE PRESENCE OF ANTI-PLATELET THERAPY Charybdis: Thrombosis
Mayor lung resection in the presence of anti-platelet therapy Hans-Beat Ris Service de Chirurgie Thoracique CHUV, Lausanne THORACIC SURGERY IN THE PRESENCE OF ANTI-PLATELET THERAPY Charybdis: Thrombosis
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
PRASUGREL HYDROCHLORIDE (Effient Eli Lilly Canada Inc.) Indication: Acute Coronary Syndrome
 Indication: Acute Coronary Syndrome") CEDAC FINAL RECOMMENDATION PRASUGREL HYDROCHLORIDE (Effient Eli Lilly Canada Inc.) Indication: Acute Coronary Syndrome Recommendation: The Canadian Expert Drug Advisory Committee (CEDAC) recommends that
CEDAC FINAL RECOMMENDATION PRASUGREL HYDROCHLORIDE (Effient Eli Lilly Canada Inc.) Indication: Acute Coronary Syndrome Recommendation: The Canadian Expert Drug Advisory Committee (CEDAC) recommends that
What hematologists should know about VerifyNow
 What hematologists should know about VerifyNow Hematology fellows conference 12/13/2013 Presenter: Christina Fitzmaurice, MD, MPH Discussant: Daniel Sabath, MD, PhD HMC consult patient 54 yo woman admitted
What hematologists should know about VerifyNow Hematology fellows conference 12/13/2013 Presenter: Christina Fitzmaurice, MD, MPH Discussant: Daniel Sabath, MD, PhD HMC consult patient 54 yo woman admitted
LOW DOSE ASPIRIN CARDIOVASCULAR DISEASE FOR PROPHYLAXIS OF FOR BACKGROUND USE ONLY NOT TO BE USED IN DETAILING
 LOW DOSE ASPIRIN FOR PROPHYLAXIS OF CARDIOVASCULAR DISEASE FOR BACKGROUND USE ONLY NOT TO BE USED IN DETAILING Use of Low Dose Aspirin to Treat and Prevent Cardiovascular Disease In recent decades, aspirin
LOW DOSE ASPIRIN FOR PROPHYLAXIS OF CARDIOVASCULAR DISEASE FOR BACKGROUND USE ONLY NOT TO BE USED IN DETAILING Use of Low Dose Aspirin to Treat and Prevent Cardiovascular Disease In recent decades, aspirin
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
Thrombosis Research active studies
 Thrombosis Research active studies A Pharmacodynamic Study Comparing Prasugrel Versus Ticagrelor in Patients With Coronary Artery Disease Undergoing PCI With CYP2C19 Loss-of-function Genotypes: A Feasibility
Thrombosis Research active studies A Pharmacodynamic Study Comparing Prasugrel Versus Ticagrelor in Patients With Coronary Artery Disease Undergoing PCI With CYP2C19 Loss-of-function Genotypes: A Feasibility
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Anti-platelet therapies and dual inhibition in practice
 Anti-platelet therapies and dual inhibition in practice Therapeutics; Sept. 25 th 2007 Craig Williams, Pharm.D. Associate Professor of Pharmacy Objectives 1. Understand the pharmacology of thienopyridine
Anti-platelet therapies and dual inhibition in practice Therapeutics; Sept. 25 th 2007 Craig Williams, Pharm.D. Associate Professor of Pharmacy Objectives 1. Understand the pharmacology of thienopyridine
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
OUTCOMES WITH LONGTERM DUAL ANTIPLATELET THERAPY AFTER CORONARY ANGIOPLASTY Ashok Kumar Arigonda, K. Nagendra Prasad, O. Hareesh, R.
 INDIAN JOURNAL OF CARDIOVACULAR DIEAE JOURNAL in women (IJCD) 016 VOL 1 IUE 3 ORIGINAL ARTICLE 1 OUTCOME WITH LONGTERM DUAL ANTIPLATELET THERAPY AFTER CORONARY ANGIOPLATY Ashok Kumar Arigonda, K. Nagendra
INDIAN JOURNAL OF CARDIOVACULAR DIEAE JOURNAL in women (IJCD) 016 VOL 1 IUE 3 ORIGINAL ARTICLE 1 OUTCOME WITH LONGTERM DUAL ANTIPLATELET THERAPY AFTER CORONARY ANGIOPLATY Ashok Kumar Arigonda, K. Nagendra
Clopidogrel has been evaluated in clinical trials that included cardiovascular patients
 REVIEW ARTICLE Comparative Benefits of Clopidogrel and Aspirin in High-Risk Patient Populations Lessons From the CAPRIE and CURE Studies Jack Hirsh, CM, MD, FRCPC, FRACP, FRSC, DSc; Deepak L. Bhatt, MD,
REVIEW ARTICLE Comparative Benefits of Clopidogrel and Aspirin in High-Risk Patient Populations Lessons From the CAPRIE and CURE Studies Jack Hirsh, CM, MD, FRCPC, FRACP, FRSC, DSc; Deepak L. Bhatt, MD,
Pocket Guide. Antiplatelet Therapy in the Outpatient Setting 2011 Recommendations. Leadership. Knowledge. Community.
 Pocket Guide Antiplatelet Therapy in the Outpatient Setting 2011 Recommendations For more information, please visit the Canadian Cardiovascular Society (CCS) Antiplatelet Guidelines at www.ccsguidelineprograms.ca.
Pocket Guide Antiplatelet Therapy in the Outpatient Setting 2011 Recommendations For more information, please visit the Canadian Cardiovascular Society (CCS) Antiplatelet Guidelines at www.ccsguidelineprograms.ca.
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation
 HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
Update on Perioperative Medicine. Update on Perioperative Medicine. Question 1: Clinical Risk Prediction. for the Office-based Practitioner
 Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Perioperative Cardiac Management. Emma Sargsyan, MD, FACP
 Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
4/27/2015. Cardiac Events #1 cause of postoperative complications/ mortality- CHF, complete heart block, MI,
 Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Additional Contributor: Glenn Levine (USA).
.") 2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) The Task Force for the Management
2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) The Task Force for the Management
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
6/1/18 LEARNING OBJECTIVES PATIENT POPULATION PRESENTATIONS
 PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
ANTIPLATELET REGIMENS:
 ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
Keeping Coronary Stents Patent in Patients Priya Kumar, M.D. University of North Carolina, Chapel Hill, NC
 Session: L232 Session: L432 Keeping Coronary Stents Patent in Patients Priya Kumar, M.D. University of North Carolina, Chapel Hill, NC Disclosures: This presenter has no financial relationships with commercial
Session: L232 Session: L432 Keeping Coronary Stents Patent in Patients Priya Kumar, M.D. University of North Carolina, Chapel Hill, NC Disclosures: This presenter has no financial relationships with commercial
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Update in Perioperative Anticoagulation and Antiplatelet management
 Update in Perioperative Anticoagulation and Antiplatelet management Grand Rounds October 31, 2014 Brooke Hall, MD Steve Kornfeld, MD Bruce McLellan, MD Nothing to disclose Objectives Describe the updates
Update in Perioperative Anticoagulation and Antiplatelet management Grand Rounds October 31, 2014 Brooke Hall, MD Steve Kornfeld, MD Bruce McLellan, MD Nothing to disclose Objectives Describe the updates
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Anticoagulation Management Around Endoscopy: GI Perspective. Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017
 Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI
 Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI Ομάδες Εργασίας Φεβρουάριος 2016 Ξανθοπούλου Ιωάννα Καρδιολόγος Επιμ Β ΠΓΝΠατρών Nothing to disclose Platelet function testing (PFT) is helpful in identifying
Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI Ομάδες Εργασίας Φεβρουάριος 2016 Ξανθοπούλου Ιωάννα Καρδιολόγος Επιμ Β ΠΓΝΠατρών Nothing to disclose Platelet function testing (PFT) is helpful in identifying
Preoperative Evaluation Guidelines and Work up
 Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
- May Help Increase Appropriate Early Use in Acute Coronary Syndrome Patients -
 MEDIA INVESTORS Ken Dominski John Elicker Bristol-Myers Squibb Bristol-Myers Squibb 609-252-5251 212-546-3775 ken.dominski@bms.com john.elicker@bms.com Amy Ba Felix Lauscher sanofi-aventis sanofi-aventis
MEDIA INVESTORS Ken Dominski John Elicker Bristol-Myers Squibb Bristol-Myers Squibb 609-252-5251 212-546-3775 ken.dominski@bms.com john.elicker@bms.com Amy Ba Felix Lauscher sanofi-aventis sanofi-aventis
WARFARIN: PERI OPERATIVE MANAGEMENT
 WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Is There A LIfe for DES after discontinuation of Clopidogrel
 EMBARGOED UNTIL 3:45pm CT, Sunday, 11/16/14 - FOR MEDIA BACKGROUND ONLY - Do Not Publish Chicago 2014 Is There A LIfe for DES after discontinuation of Clopidogrel Six-month versus 24-month dual antiplatelet
EMBARGOED UNTIL 3:45pm CT, Sunday, 11/16/14 - FOR MEDIA BACKGROUND ONLY - Do Not Publish Chicago 2014 Is There A LIfe for DES after discontinuation of Clopidogrel Six-month versus 24-month dual antiplatelet
Antiplatelet therapy is the mainstay of pharmacological
 Contemporary Reviews in Interventional Cardiology Pretreatment With Antiplatelet Drugs in Invasively Managed Patients With Coronary Artery Disease in the Contemporary Era Review of the Evidence and Practice
Contemporary Reviews in Interventional Cardiology Pretreatment With Antiplatelet Drugs in Invasively Managed Patients With Coronary Artery Disease in the Contemporary Era Review of the Evidence and Practice
Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France
 Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France Disclosures Research grants: Astra-Zeneca, Merck, Novartis, Pfizer, sanofi-aventis, Servier, The MedCo Fees
Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France Disclosures Research grants: Astra-Zeneca, Merck, Novartis, Pfizer, sanofi-aventis, Servier, The MedCo Fees
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author)
 Contact Name and Job Title (author)") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline for Patients on antiplatelet agents undergoing Elective, Non-cardiac
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline for Patients on antiplatelet agents undergoing Elective, Non-cardiac
2018 David Stultz. The Consultant s Job
 The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Plavix duration of effect
 Plavix duration of effect The Borg System is 100 % Plavix duration of effect Jan 20, 2015. If you have had stent placement after balloon angioplasty for coronary artery disease you will be placed on medications
Plavix duration of effect The Borg System is 100 % Plavix duration of effect Jan 20, 2015. If you have had stent placement after balloon angioplasty for coronary artery disease you will be placed on medications
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Controversies in Perioperative Medicine
 Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
NHS Dumfries & Galloway Aspirin Discontinuation Audit May 2011 (updated August 2015)
") Title of Project: NHS Dumfries & Galloway Aspirin Discontinuation Audit May 2011 (updated August 2015) 1 Reason for the review In the UK, low dose aspirin (75mg) is licensed for the prevention of thrombotic
Title of Project: NHS Dumfries & Galloway Aspirin Discontinuation Audit May 2011 (updated August 2015) 1 Reason for the review In the UK, low dose aspirin (75mg) is licensed for the prevention of thrombotic
Updates & Controversies in Perioperative Medicine
 Updates in Perioperative Medicine Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco New Guidelines for Perioperative
Updates in Perioperative Medicine Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco New Guidelines for Perioperative
Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants
 Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants S. Hinan Ahmed, MD Anti-platelet Therapy: Simple Answer Bare metal stent
Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants S. Hinan Ahmed, MD Anti-platelet Therapy: Simple Answer Bare metal stent
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY
 EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
Session Objectives. Clopidogrel Resistance. Clopidogrel (Plavix )
") Session Objectives New Antithrombotics and Real Time Genetic Testing: Their Role in the Vascular Patient Margaret C. Fang, MD, MPH Associate Professor of Medicine Division of Hospital Medicine Medical
Session Objectives New Antithrombotics and Real Time Genetic Testing: Their Role in the Vascular Patient Margaret C. Fang, MD, MPH Associate Professor of Medicine Division of Hospital Medicine Medical
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable?
 SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable? tielle est 2 ré Totielle est interdite. Prof. Marco Roffi Hôpitaux Universitaires de Genève Research funding
SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable? tielle est 2 ré Totielle est interdite. Prof. Marco Roffi Hôpitaux Universitaires de Genève Research funding
Mid-term results from real-world REPARA registry. Felipe Hernandez, on behalf of the REPARA investigators
 Mid-term results from real-world REPARA registry Felipe Hernandez, on behalf of the REPARA investigators Potential conflicts of interest Speaker's name: Felipe Hernandez I have the following potential
Mid-term results from real-world REPARA registry Felipe Hernandez, on behalf of the REPARA investigators Potential conflicts of interest Speaker's name: Felipe Hernandez I have the following potential
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Περιφερική Αρτηριακή Νόσος Νόσος Καρωτίδων
 Νεώτερα δεδομένα στην αντιαιμοπεταλιακή αγωγή που θα επηρεάσουν τις μελλοντικές κατευθυντήριες οδηγίες Περιφερική Αρτηριακή Νόσος Νόσος Καρωτίδων Μιλτιάδης Ματσάγκας, MD, PhD, FEBVS Αναπληρωτής Καθηγητής
Νεώτερα δεδομένα στην αντιαιμοπεταλιακή αγωγή που θα επηρεάσουν τις μελλοντικές κατευθυντήριες οδηγίες Περιφερική Αρτηριακή Νόσος Νόσος Καρωτίδων Μιλτιάδης Ματσάγκας, MD, PhD, FEBVS Αναπληρωτής Καθηγητής
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such