Colorectal Surgery Benign Anal Conditions...
|
|
|
- Neal Merritt
- 6 years ago
- Views:
Transcription
1 Colorectal Surgery Benign Anal Conditions... Lee Dvorkin Consultant General, Colorectal & Laparoscopic Surgeon, NMUH Clinical Lead for General Surgery, NMH Senior Clinical Lecturer, UCLH Associate Professor of Surgery, SGU

2 The next 45 minutes... 7 common conditions Fissure in ano Haemorrhoids Fistulae Pilonidal sinus Pruritus ani Rectal prolapse Faecal Incontinence

3

4 Anal fissure Ischaemic ulcer Posterior midline anal canal
5 Aetiology Constipation Postpartum females (anterior fissure) Crohn s (multiple fissures) Internal anal sphincter spasm
6 Presentation Severe pain on defaecation Blood pr
 38 % headaches Diltiazem (2 %) Botulinum toxin")
7 Management (Medical) Dietary (Movicol) GTN ( %) 38 % headaches Diltiazem (2 %) Botulinum toxin A

8 Surgery... Caution!
9 Surgery Anal stretch (Incontinence > 30 %) Lateral internal sphincterotomy Morbidity % flatus incontinence % mucus discharge Low recurrence
10 Caution Post partum women & women with low pressure fissures Advancement flap as opposed to spincterotomy ( to avoid incontinence)


11
12 Haemorrhoids Common 50 % population > 50 years Vascular cushions (functional importance in maintenance of continence)


13 XXXX Piles


14 Piles?
15 Haemorrhoids aetiology Straining at stool Prolonged perineal descent (sitting on the loo) Familial tendency Poor connective tissue support
")
16 Presentation PR bleed Prolapse Discomfort Pain suggests thrombosis Bleeding > 35 (exclude Ca)
17 Treatment Depends on severity and symptoms First degree: doesn t descend, may bleed Second degree: protrudes below dentate line, return spontaneously Third degree: requires manual reduction Forth degree: irreducible

18 Management Patient education Dietary manipulation Avoid straining Avoid reading on the loo!
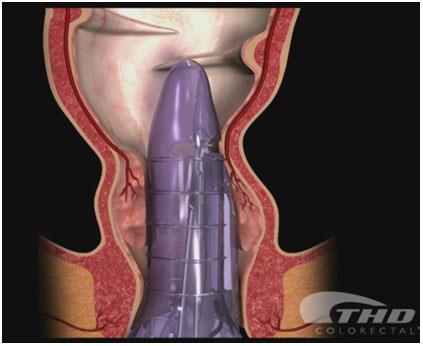
19 Treatment Sclerotherapy Banding Haemorrhoidectomy Stapled haemorrhoidectomy (PPH) THD / HALO
 Only for small piles")
20 OPD management: Sclerotherapy Oily Phenol 5% Nut allergy avoid anterior injection in males (prostatitis) Only for small piles


21 OPD management: Banding More effective than sclerotherapy Discomfort 20 mins after procedure Lifts piles
22 Haemorrhoidectomy Conventional Milligan Morgan Stapled haemorrhoidectomy Haemorrhoidal artery ligation (HALO)

23 Haemorrhoidectomy consent Pain Open wounds Flatus incontinence Anal stenosis Post op laxatives & Metronidazole

24
25 A common question... When do I refer PR bleeding and piles? Don t assume PR bleeding is piles esp in over 40 s Have a low threshold for endoscopic examination Piles are completely benign and don t need treatment unless patients quality of life is affected
26 A plee... No FOB s No CEA

27 Fistula in ano

28


29
30 Treatment options Conservative Lay open: the only cure for a fistula Seton Fibrin glue Advancement flap LIFT

31


32

33


34


35 Diagnosis...??
36 Pilonidal sinus Hair within perinatal cleft Umbilicus Webshaft of finger spaces Hirsuit
37 Presentation Asymptomatic Recurrent discharge and pain Abscess
38 Management Minimalistic approach Regular shaving Acute drainage Lateral approach (away from midline) Karydakis / Bascombe Rhomboid flap

39 Rhomboid flap


40 Pruritus ani Benign: piles, fistulae, polyp Dermatological Infection Neoplasia
41 Management Attempt to identify precipitating cause Avoid scratching Avoid excessive cleaning (bidet ideal) Avoid perfumed soap Avoid toilet paper
42 Management Barrier creams in combination with temporary steroid use Epaderm & Betnovate (max use 10 days) EUA


43 Rectal prolapse
44 Management Conservative (not a good option usually) Abdominal approach (rectopexy + resection) Laparotomy Constipation Low recurrence Laparoscopic rectopexy Perineal approach (Delormes / Altmeier) Reduced morbidity Increased recurrence rate (30 %)



45
46 Faecal Incontinence Distressing & socially incapacitating condition True prevalence remains unknown 3 8% of the population increasing in the elderly
47 Continence mechanisms Anatomy Resting tone: 55% IAS 30% EAS 15% haemorrhoidal plexuses
48 Frequency (%) Faecal Incontinence: Referral pattern n = 629 Ratio F:M = 3: Female Male
49 FI: Symptoms Urge Incontinence occurring with the patient s awareness, against their will because of lack of voluntary control two-minute warning Passive Without the patient s knowledge Post-defaecation leakage
50 FI: aetiology Trauma Obstetric injury Surgery Accidental Colorectal disease Rectal prolapse IBD Tumours Neurological Cerebral/spinal/peripheral Congenital Spina bifida Miscellaneous Behavioural, impaction
51 Frequency (%) n = 439 Obstetric Factors Overall Tear Episiotomy Forceps Ventouse Hysterectomy
52 Frequency (%) n = 154 Anal Surgery (Males) Overall Piles Banding Fistula -otomy Stretch
53 Treatment Exclude serious pathology Multimodal investigation if severe U/S Pressure testing Evacuation Proctography
54 Treatment Avoid caffeine/spicy foods Imodium / Codeine Pads Anal plug (Peristeen) Biofeedback Surgical repair Artificial sphincter Stoma SNS/PNS

 2 stage procedure Trial period")
55 Sacral Nerve Stimulation Matzel in 1995 for FI. Stimulation of S3 neuromodulation effect on ascending pathways, local autonomic system Locally (sphincter pressures, rectal sensation) Distant (gut motility, sensory cortex) 2 stage procedure Trial period 3 weeks Permanent implant
56 Indications Faecal Incontinence NICE approved % virtually continent, 30% of the rest will have a sig reduction in FI No trial yet comparing to sphincter repair
57 Expensive SNS: Problems Test box 200, Lead 2000, Battery 8000 Post operative problems Infection, nerve damage, battery lasts 6-8 years Loss of efficacy over time Requires regular re-programming Pregnancy Must be switched off during pregnancy c-section to avoid lead displacement


58 Posterior Tibial Nerve Stimulation 2003 used for FI Remote neuromodulation of sacral plexus via the posterior tibial nerve Achieved by Percutaneous transcutaneous
59 PTNS- Indications Just FI, so far 11 studies, most demonstrated sig improvement Given as a 1-2 month course Percutaneous more efficacious than transcutaneous Therapeutic effect that can persist for several months after treatment Large multicenter study under way comparing PTNS with SNS
60 PTNS- Problems Cheap equipment costs Needles 200 Pads 3 Stimulator boxes 80 Labour intensive Percutaneous PTNS requires practitioner support But transcutaneous can be self-administered
61 The past 45 mins Proctology Demonstrated array of pathologies seen Highlighted areas where primary care can take a bigger role

62 Questions?
63 Diverticular Disease Lee Dvorkin

64 Right sided in Orient Left sided in West 75% of over 70 yrs Only 10-30% cause symptoms Dilemma comes as to when, how and who to operate on
65 Don t assume change in bowel habit is diverticular disease


66 Aetiology Poor dietary fibre Hyperelasytosis and altered collagen structure with ageing Narrow sigmoid leads to high intraluminal pressures with mucosa protrusion at anatomical weak points
67 Complications Pain Diverticultis Fistula Bleeding Stricture Perforation
68 Presentation Elective Lower abdo pain Altered bowel habit distension Treatment Exclude cancer Reassure Increase fibre Surgery: beware concurrent IBS
69 Emergency Acute diverticulitis Fistula LIF pain Change in bowel habit Peritonism Sepsis Any adjacent organ Colovesical & colovaginal most common ddx: Crohn s, cancer


70 Emergency Abscess Bleeding Lower abdo pain/mass Systemic sepsis Painless & profuse Colour depends on site and speed


71 Emergency Obstruction Fibrosis stricture from longstanding sigmoid diverticular disease Presents exactly as LBO due to cancer Often cant tell until after resection

72 Investigation Depends on clinical presentation Most managed as outpatient with colonoscopy to confirm diagnosis Inpatients have variety of investigations CT Contrast enema Angiogram
73 Management Elective Recurrent persistent symptoms Development of a complication Evidence suggests that first attack often the worst and only a minority continue with problems Fistulae often too morbid to treat conservatively Emergency Severe sepsis not controlled with antibiotics Generalised peritonitis that fails to respond to treatment Torrential bleeding
74 Surgical issues in acute setting..? When to operate? ongoing clinical assessment When to resect bowel? lavage?? When to anastamose? avoiding anastamosis not always the easy option

75 Subsequent elective surgery Limited evidence to inform practice Ambrosetti et al... 14% recurrence after mild first attack 39% after a severe attack Higher chance recurrence in young 1 admission with severe attack in young 2 admissions Suspicion of malignancy
76 Summary Sigmoid diverticular disease is common Admission is uncommon CT best investigation Urgent surgery needed in <20% Laparoscopic lavage should be considered as should primary anastamosis Offer elective surgery to young symptomatic patients
Pelvic Floor Disorders. Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon
 Consultant Colorectal and General Surgeon") Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Treatment of haemorrhoids. Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland
 Treatment of haemorrhoids Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland Much overlap of haemorrhoidal symptoms with other conditions Is it just the haemorrhoids? what type of haemorrhoidal
Treatment of haemorrhoids Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland Much overlap of haemorrhoidal symptoms with other conditions Is it just the haemorrhoids? what type of haemorrhoidal
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT. Simon Radley Consultant Surgeon March 2013
 DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
Anterior anal fissure is much more common in women and may arise following vaginal delivery.
 ANAL FISSURE Definition An anal fissure (synonym: fissure-in-ano) is a longitudinal split in the anoderm of the distal anal canal which extends from the anal verge proximally towards, but not beyond, the
ANAL FISSURE Definition An anal fissure (synonym: fissure-in-ano) is a longitudinal split in the anoderm of the distal anal canal which extends from the anal verge proximally towards, but not beyond, the
Hemorrhoids. Carlos R. Alvarez-Allende PGY-III Colorectal Surgery
 Hemorrhoids Carlos R. Alvarez-Allende PGY-III Colorectal Surgery Overview Anatomy Classification Etiology Incidence Symptoms Differential Diagnosis Medical Management Surgical Management Anatomy Anal canal
Hemorrhoids Carlos R. Alvarez-Allende PGY-III Colorectal Surgery Overview Anatomy Classification Etiology Incidence Symptoms Differential Diagnosis Medical Management Surgical Management Anatomy Anal canal
Faecal Incontinence: Assessment and Management
 Mrs PK; 56 yrs; Married; 2 children Faecal Incontinence: Assessment and Management Professor Marc A Gladman MBBS DFFP PhD MRCOG FRCS (UK) FRACS Professor of Colorectal Surgery >10 years of incontinence
Mrs PK; 56 yrs; Married; 2 children Faecal Incontinence: Assessment and Management Professor Marc A Gladman MBBS DFFP PhD MRCOG FRCS (UK) FRACS Professor of Colorectal Surgery >10 years of incontinence
Conservative Management of Functional Bowel & Pelvic Floor Disorders
 Conservative Management of Functional Bowel & Pelvic Floor Disorders Kathy Davis PhD BSc(Hons)SRN Specialist Nurse Consultant Parkside Hospital & Minerva Medical Clinic Overview Burden of disease Aims
Conservative Management of Functional Bowel & Pelvic Floor Disorders Kathy Davis PhD BSc(Hons)SRN Specialist Nurse Consultant Parkside Hospital & Minerva Medical Clinic Overview Burden of disease Aims
Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland
 Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland 16:30-17:25 WS #168: Modern Treatment of Haemorrhoids 17:35-18:30 WS #180: Modern Treatment of Haemorrhoids (Repeated) BOTTOMS Science and
Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland 16:30-17:25 WS #168: Modern Treatment of Haemorrhoids 17:35-18:30 WS #180: Modern Treatment of Haemorrhoids (Repeated) BOTTOMS Science and
GI Physiology - Investigating and treating patients with pelvic floor dysfunction. Lynne Smith Department of GI Physiology NGH Sheffield
 GI Physiology - Investigating and treating patients with pelvic floor dysfunction Lynne Smith Department of GI Physiology NGH Sheffield Aims o o o To give an overview of lower GI investigations To demonstrate
GI Physiology - Investigating and treating patients with pelvic floor dysfunction Lynne Smith Department of GI Physiology NGH Sheffield Aims o o o To give an overview of lower GI investigations To demonstrate
Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee
 Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee MD, MMed (S'pore), FRCS (Edin) Associate Consultant Department of Surgery 9 January 2016 Incidence
Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee MD, MMed (S'pore), FRCS (Edin) Associate Consultant Department of Surgery 9 January 2016 Incidence
Guideline scope Diverticular disease: diagnosis and management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
Benign anorectal diseases
 Benign anorectal diseases Symptoms Bleeding Pruritus Discharge Fecal incontinence Diarrhea Constipation False need to defecate Examinations Clinical exam Anuscopy Rectosigmoidoscopy Endosonography MRI
Benign anorectal diseases Symptoms Bleeding Pruritus Discharge Fecal incontinence Diarrhea Constipation False need to defecate Examinations Clinical exam Anuscopy Rectosigmoidoscopy Endosonography MRI
Colorectal Problems In Primary Care
 Colorectal Problems In Primary Care Lincoln Israel General and Colorectal Surgeon Middlemore Hospital Middlemore Hospital Mercy Hospital Auckland Colorectal Centre (Gilgit Rd Specialist Centre) Manukau
Colorectal Problems In Primary Care Lincoln Israel General and Colorectal Surgeon Middlemore Hospital Middlemore Hospital Mercy Hospital Auckland Colorectal Centre (Gilgit Rd Specialist Centre) Manukau
, may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely,
 ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
Incidence of Colorectal Cancers- Australia. Anterior Resection 5/23/2018. What spurs us to investigate?
 Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Haemorrhoidectomy. Colorectal Surgery. Patient Information
 Haemorrhoidectomy Colorectal Surgery Patient Information What are haemorrhoids? Haemorrhoids, also know as piles, are soft fleshy lumps just inside the back passage (anus). They have a rich blood supply
Haemorrhoidectomy Colorectal Surgery Patient Information What are haemorrhoids? Haemorrhoids, also know as piles, are soft fleshy lumps just inside the back passage (anus). They have a rich blood supply
Office Management of Anorectal Disease. Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas
 Office Management of Anorectal Disease Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas Commonly seen Anorectal Disease Hemorrhoids Anal fissures Pruritus Abscesses
Office Management of Anorectal Disease Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas Commonly seen Anorectal Disease Hemorrhoids Anal fissures Pruritus Abscesses
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels.
 Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Perianal diseases. What causes pain in the bottom? What causes lumps around the bottom? What examination is likely?
 In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Perianal diseases www.corecharity.org.uk What are perianal diseases? What causes an itchy bottom? What causes pain in the
In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Perianal diseases www.corecharity.org.uk What are perianal diseases? What causes an itchy bottom? What causes pain in the
PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS. A08/S/d Colorectal: Faecal Incontinence (Adult)
") A08/S/d 2013/14 NHS STANDARD CONTRACT FOR COLORECTAL: FAECAL INCONTINENCE (ADULT) PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider
A08/S/d 2013/14 NHS STANDARD CONTRACT FOR COLORECTAL: FAECAL INCONTINENCE (ADULT) PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider
Bright-red bleeding: If you have piles, you might see bright-red bleeding on the toilet paper, in the toilet bowl or on the surface of the faeces.
 What are haemorrhoids/piles? In the inner lining of the anus there are three haemorrhoidal cushions of tissue, which help to seal the anus and contribute to the control of the bowels (continence). Often,
What are haemorrhoids/piles? In the inner lining of the anus there are three haemorrhoidal cushions of tissue, which help to seal the anus and contribute to the control of the bowels (continence). Often,
Small Bowel and Colon Surgery
 Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Constipation Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.uk
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Constipation Constipation is a symptom that can mean different things to different people but the usual
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Constipation Constipation is a symptom that can mean different things to different people but the usual
A Case of Fecal Incontinence: Medical and Interventional Treatment Options
 A Case of Fecal Incontinence: Medical and Interventional Treatment Options HPI JP is a 69 year-old F with a 12-month history of FI. Her symptoms began after a colonoscopy She has been experiencing passive
A Case of Fecal Incontinence: Medical and Interventional Treatment Options HPI JP is a 69 year-old F with a 12-month history of FI. Her symptoms began after a colonoscopy She has been experiencing passive
Fecal Incontinence. What is fecal incontinence?
 Scan for mobile link. Fecal Incontinence Fecal incontinence is the inability to control the passage of waste material from the body. It may be associated with constipation or diarrhea and typically occurs
Scan for mobile link. Fecal Incontinence Fecal incontinence is the inability to control the passage of waste material from the body. It may be associated with constipation or diarrhea and typically occurs
Tertiary, regional and local pelvic floor service providers: the future. model? Andrew Williams
 Tertiary, regional and local pelvic floor service providers: the future Andrew Williams model? Pelvic Floor Unit Guy s and St Thomas NHS Foundation Trust Background 23% women suffer at least one pelvic
Tertiary, regional and local pelvic floor service providers: the future Andrew Williams model? Pelvic Floor Unit Guy s and St Thomas NHS Foundation Trust Background 23% women suffer at least one pelvic
8/29/2016 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW. LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES
 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
Haemorrhoidal artery ligation
 Haemorrhoidal artery ligation Issued: May 2010 NICE interventional procedure guidance 342 www.nice.org.uk/ipg342 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme
Haemorrhoidal artery ligation Issued: May 2010 NICE interventional procedure guidance 342 www.nice.org.uk/ipg342 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme
Laparoscopic Ventral. Mesh Rectopexy (LVMR)
") Laparoscopic Ventral Mesh Rectopexy (LVMR) Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard
Laparoscopic Ventral Mesh Rectopexy (LVMR) Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Patient Information Leaflet
 Patient Information Leaflet Haemorrhoid Operation What are haemorrhoids? Everyone has swellings in the anal canal (back passage) called anal cushions. These bulges in the lining of the anal canal act like
Patient Information Leaflet Haemorrhoid Operation What are haemorrhoids? Everyone has swellings in the anal canal (back passage) called anal cushions. These bulges in the lining of the anal canal act like
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
RECTAL PROLAPSE objectives
 RECTAL PROLAPSE objectives 1.Classify rectal prolapse 2. Enumerate the causes of rectal prolapse 3. Differentiate between complete rectal prolapse and intussusception 4. List the modalities of treatment
RECTAL PROLAPSE objectives 1.Classify rectal prolapse 2. Enumerate the causes of rectal prolapse 3. Differentiate between complete rectal prolapse and intussusception 4. List the modalities of treatment
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Appendix B Protocol for management of obstetric anal sphincter injury THE MANAGEMENT OF THIRD- AND FOURTH-DEGREE PERINEAL TEARS
 Appendix B Protocol for management of obstetric anal sphincter injury Document Type: THE MANAGEMENT OF THIRD- AND FOURTH-DEGREE PERINEAL TEARS PURPOSE & SCOPE To provide a guideline that will assist in
Appendix B Protocol for management of obstetric anal sphincter injury Document Type: THE MANAGEMENT OF THIRD- AND FOURTH-DEGREE PERINEAL TEARS PURPOSE & SCOPE To provide a guideline that will assist in
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: COLORECTAL 5-May-2013 DEVELOPED BY: REVIEWED BY:
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: COLORECTAL 5-May-2013 DEVELOPED BY: REVIEWED BY:
Prolapse & Urogynaecology. Hester Mannion and Fabi Sica
 Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Faecal Incontinence Information Leaflet THE DIGESTIVE SYSTEM
 THE DIGESTIVE SYSTEM This factsheet is about faecal incontinence Faecal (or anal) incontinence is the loss of stool, liquid or gas from the bowel at an undesirable time. Males and females of any age may
THE DIGESTIVE SYSTEM This factsheet is about faecal incontinence Faecal (or anal) incontinence is the loss of stool, liquid or gas from the bowel at an undesirable time. Males and females of any age may
Landmarks in the History of Haemorrhoids
 Landmarks in the History of Haemorrhoids Charles V. Mann Date Comments c.2250 BC 1700 BC 1552 BC 460-375 BC Old Testament, Samuel 5:9 Old Testament Samuel 5:12 25 BC-AD 50 AD 130-200 Sometime between the
Landmarks in the History of Haemorrhoids Charles V. Mann Date Comments c.2250 BC 1700 BC 1552 BC 460-375 BC Old Testament, Samuel 5:9 Old Testament Samuel 5:12 25 BC-AD 50 AD 130-200 Sometime between the
Stapled transanal rectal resection for obstructed defaecation syndrome
 Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Peristeen and the Neurogenic Bowel Dysfunction Score (NBD) for pediatric patients with spina bifida
 for pediatric patients with spina bifida") Peristeen and the Neurogenic Bowel Dysfunction Score (NBD) for pediatric patients with spina bifida Coloplast develops products and services that make life easier for people with very personal and private
Peristeen and the Neurogenic Bowel Dysfunction Score (NBD) for pediatric patients with spina bifida Coloplast develops products and services that make life easier for people with very personal and private
TYPES OF RECTAL PROLAPSE
 RECTAL PROLPASE Rectal prolapse describes a condition where either the lining or entire wall of the rectum becomes loose and falls into, or even out of, the rectum through the anus. TYPES OF RECTAL PROLAPSE
RECTAL PROLPASE Rectal prolapse describes a condition where either the lining or entire wall of the rectum becomes loose and falls into, or even out of, the rectum through the anus. TYPES OF RECTAL PROLAPSE
Dr Nagham Al-Mozany. Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland
 Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 12:05-13:00 WS #33: Management of Benign Rectal Bleeding Management of Benign Rectal Bleeding
Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 12:05-13:00 WS #33: Management of Benign Rectal Bleeding Management of Benign Rectal Bleeding
A70.4 Insertion of neurostimulator electrodes into peripheral nerve Z12.2 Posterior tibial nerve R15.X Faecal incontinence
 The National Institute for Health and Clinical Excellence (NICE) has issued full guidance to the NHS in England, Wales, Scotland and Northern Ireland on Percutaneous tibial nerve stimulation (PTNS) for
The National Institute for Health and Clinical Excellence (NICE) has issued full guidance to the NHS in England, Wales, Scotland and Northern Ireland on Percutaneous tibial nerve stimulation (PTNS) for
Management of Neurogenic Bowel Dysfunction. Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders
 Management of Neurogenic Bowel Dysfunction Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders DEFECATION Delivery of colon contents to the rectum Rectal compliance
Management of Neurogenic Bowel Dysfunction Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders DEFECATION Delivery of colon contents to the rectum Rectal compliance
Lets talk about Faecal incontinence (FI) in Scleroderma
 in Scleroderma") Lets talk about Faecal incontinence (FI) in Scleroderma Dr. Shamaila Butt Gastroenterology Research Registrar GI Physiology unit University College Hospital London GI manifestations in Scleroderma Oesophagus
Lets talk about Faecal incontinence (FI) in Scleroderma Dr. Shamaila Butt Gastroenterology Research Registrar GI Physiology unit University College Hospital London GI manifestations in Scleroderma Oesophagus
When should we operate for recurrent diverticulitis. Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital
 When should we operate for recurrent diverticulitis Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital ASCRS Practice parameters for the Treatment of Acute Diverticulitis
When should we operate for recurrent diverticulitis Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital ASCRS Practice parameters for the Treatment of Acute Diverticulitis
Patient information leaflet. Royal Surrey County Hospital. NHS Foundation Trust. Haemorrhoids. Day Surgery Unit
 Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Haemorrhoids Day Surgery Unit What are haemorrhoids? The anal canal (back passage) contains cushions of tissue at the top of
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Haemorrhoids Day Surgery Unit What are haemorrhoids? The anal canal (back passage) contains cushions of tissue at the top of
Index of subjects. bilesalt, malabsorption, incontinence in 147
 Index of subjects alcoholism, neuronal damage in 118 Alzheimer dementia, faecal incontinence in 113 anal fissure, manometry in 5 anal retractor, reduction of resting pressure 128 Angelchick prosthesis,
Index of subjects alcoholism, neuronal damage in 118 Alzheimer dementia, faecal incontinence in 113 anal fissure, manometry in 5 anal retractor, reduction of resting pressure 128 Angelchick prosthesis,
Regaining Bowel Control. Yvette Perston Functional Bowel CNS Queen Elizabeth Hospital Birmingham
 Regaining Bowel Control Yvette Perston Functional Bowel CNS Queen Elizabeth Hospital Birmingham GI Tract Sigmoid Colon and Rectum Anterior Resection What is Anterior Resection Syndrome (LARS)? Disordered
Regaining Bowel Control Yvette Perston Functional Bowel CNS Queen Elizabeth Hospital Birmingham GI Tract Sigmoid Colon and Rectum Anterior Resection What is Anterior Resection Syndrome (LARS)? Disordered
DISEASES OF THE COLON, RECTUM, & ANUS
 DISEASES OF THE COLON, RECTUM, & ANUS Rocco Ricciardi, MD, MPH Chief, Section of Colon & Rectal Surgery Massachusetts General Hospital Associate Professor of Surgery Harvard Medical School CASE 1 Hemorrhoid
DISEASES OF THE COLON, RECTUM, & ANUS Rocco Ricciardi, MD, MPH Chief, Section of Colon & Rectal Surgery Massachusetts General Hospital Associate Professor of Surgery Harvard Medical School CASE 1 Hemorrhoid
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient Information Leaflet
 Patient Information Leaflet Your Haemorrhoid Operation What are haemorrhoids? Everyone has swellings in the anal canal (back passage) called anal cushions. These bulges in the lining of the anal canal
Patient Information Leaflet Your Haemorrhoid Operation What are haemorrhoids? Everyone has swellings in the anal canal (back passage) called anal cushions. These bulges in the lining of the anal canal
RUBBER BAND LIGATION OF HAEMORRHOIDS
 SINGAPORE MEDICAL JOURNAL Walter T. L. Tan K. T. Foo SYNOPSIS Haemorrhoids have been an affliction of mankind from the dawn of history. As much as 40-50% of the population will suffer from haemorrhoids
SINGAPORE MEDICAL JOURNAL Walter T. L. Tan K. T. Foo SYNOPSIS Haemorrhoids have been an affliction of mankind from the dawn of history. As much as 40-50% of the population will suffer from haemorrhoids
Surgical Therapies for the Treatment of IBD!
 Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Accidental Bowel Leakage (Fecal Incontinence)
") Accidental Bowel Leakage (Fecal Incontinence) What is Accidental Bowel Leakage (ABL)? Accidental bowel leakage is the inability to control solid or liquid stool. This is the inability to control gas and
Accidental Bowel Leakage (Fecal Incontinence) What is Accidental Bowel Leakage (ABL)? Accidental bowel leakage is the inability to control solid or liquid stool. This is the inability to control gas and
To inject, to band or to excise? These were the alternatives for a colorectal surgeon
 CHAPTER 2 Hemorrhoids To inject, to band or to excise? These were the alternatives for a colorectal surgeon some 50 years ago, when sclerosant injection, rubber band ligation and hemorrhoidectomy were
CHAPTER 2 Hemorrhoids To inject, to band or to excise? These were the alternatives for a colorectal surgeon some 50 years ago, when sclerosant injection, rubber band ligation and hemorrhoidectomy were
Randomised Mixed Methods Pilot Trial of Sacral and Percutaneous Tibial Nerve Stimulation for Faecal Incontinence
 Research for Patient Benefit Randomised Mixed Methods Pilot Trial of Sacral and Percutaneous Tibial Nerve Stimulation for Faecal Incontinence Thin NN 1, Taylor SJC 2, Bremner SA 2, Hounsome N 2, Alam A
Research for Patient Benefit Randomised Mixed Methods Pilot Trial of Sacral and Percutaneous Tibial Nerve Stimulation for Faecal Incontinence Thin NN 1, Taylor SJC 2, Bremner SA 2, Hounsome N 2, Alam A
Assessing rectal bleeding: A common symptom of haemorrhoids
 Assessing rectal bleeding: A common symptom of haemorrhoids Rectal bleeding is a red flag sign and one of the referral criteria for a 2-week wait to see a specialist. However, in most cases, it is commonly
Assessing rectal bleeding: A common symptom of haemorrhoids Rectal bleeding is a red flag sign and one of the referral criteria for a 2-week wait to see a specialist. However, in most cases, it is commonly
2/5/2016. Evolving Surgical Treatment Approaches for Fecal Incontinence in Women: An Evidence and Cased-Based Approach
 Evolving Surgical Treatment Approaches for Fecal Incontinence in Women: An Evidence and Cased-Based Approach Holly E Richter, PhD, MD, FACOG, FACS J Marion Sims Professor Obstetrics and Gynecology Professor
Evolving Surgical Treatment Approaches for Fecal Incontinence in Women: An Evidence and Cased-Based Approach Holly E Richter, PhD, MD, FACOG, FACS J Marion Sims Professor Obstetrics and Gynecology Professor
Summary and conclusion. Summary And Conclusion
 Summary And Conclusion Summary and conclusion Rectal prolapse remain a disorder for which no single ideal treatment was approved for all cases. Complete rectal prolapse (procidentia) is the circumferential
Summary And Conclusion Summary and conclusion Rectal prolapse remain a disorder for which no single ideal treatment was approved for all cases. Complete rectal prolapse (procidentia) is the circumferential
Although disparate topics, these two different pathologic
 34 H E M O R R H O I D S A N D R E C T A L P R O L A P S E CHARLES N. HEADRICK MICHAEL J. STAMOS Although disparate topics, these two different pathologic entities are commonly misdiagnosed by both layperson
34 H E M O R R H O I D S A N D R E C T A L P R O L A P S E CHARLES N. HEADRICK MICHAEL J. STAMOS Although disparate topics, these two different pathologic entities are commonly misdiagnosed by both layperson
Further information You can get more information and share your experience at
 CR08 Lateral Internal Sphincterotomy Further information You can get more information and share your experience at www.aboutmyhealth.org Local information You can get information locally from: Taunton
CR08 Lateral Internal Sphincterotomy Further information You can get more information and share your experience at www.aboutmyhealth.org Local information You can get information locally from: Taunton
EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May Dr. Annie Leong MBBS, FRANZCOG, CU
 EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May 2011 Dr. Annie Leong MBBS, FRANZCOG, CU Restore normal perineal anatomy Achieve good haemostasis Avoid infection and wound breakdown Avoid coital
EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May 2011 Dr. Annie Leong MBBS, FRANZCOG, CU Restore normal perineal anatomy Achieve good haemostasis Avoid infection and wound breakdown Avoid coital
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Anorectal Diagnostic Overview
 Anorectal Diagnostic Overview 11-25-09 3.11.2010 2009 2010 Anorectal Manometry Overview Measurement of pressures and the annotation of rectal sensation throughout the rectum and anal canal to determine:
Anorectal Diagnostic Overview 11-25-09 3.11.2010 2009 2010 Anorectal Manometry Overview Measurement of pressures and the annotation of rectal sensation throughout the rectum and anal canal to determine:
Management of Diverticulitis. Sanjay Adusumilli MBBS MS FRACS
 Management of Diverticulitis Sanjay Adusumilli MBBS MS FRACS 0411 051 281 Trained by CSSANZ in Oxford (UK) and Perth Appointments at BMDH, HSS, Norwest Private and SAN Hospital Surgery performed: Laparoscopic
Management of Diverticulitis Sanjay Adusumilli MBBS MS FRACS 0411 051 281 Trained by CSSANZ in Oxford (UK) and Perth Appointments at BMDH, HSS, Norwest Private and SAN Hospital Surgery performed: Laparoscopic
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE The management of faecal incontinence in adults 1.1 Short title Faecal incontinence 2 Background (a) (b) (c) The National Institute
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE The management of faecal incontinence in adults 1.1 Short title Faecal incontinence 2 Background (a) (b) (c) The National Institute
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
SACRAL NERVE STIMULATION FOR EXPERIENCE IN CHILDREN
 SACRAL NERVE STIMULATION FOR COLORECTAL DISEASES: EXPERIENCE IN CHILDREN C. LOUIS-BORRIONE - JM. GUYS TIMONE-ENFANTS MARSEILLE SACRAL NEUROMODULATION IN CHILDREN 26 : Humphreys et al - 23 children with
SACRAL NERVE STIMULATION FOR COLORECTAL DISEASES: EXPERIENCE IN CHILDREN C. LOUIS-BORRIONE - JM. GUYS TIMONE-ENFANTS MARSEILLE SACRAL NEUROMODULATION IN CHILDREN 26 : Humphreys et al - 23 children with
Anal Fissure: Finding the Root Cause
 Anal Fissure: Finding the Root Cause Michael A. Jobst, MD, FACS, FASCRS Surgical Associates, PC -- Lincoln, NE 27 th Annual Management of Colon and Rectal Diseases February 23, 2019 Objectives Differentiate
Anal Fissure: Finding the Root Cause Michael A. Jobst, MD, FACS, FASCRS Surgical Associates, PC -- Lincoln, NE 27 th Annual Management of Colon and Rectal Diseases February 23, 2019 Objectives Differentiate
Piles / Sclerosing. Endoscopy Department. Patient information leaflet
 Piles / Sclerosing Endoscopy Department Patient information leaflet You will only be given this leaflet if you have been diagnosed with piles / sclerosing. The information below outlines the condition,
Piles / Sclerosing Endoscopy Department Patient information leaflet You will only be given this leaflet if you have been diagnosed with piles / sclerosing. The information below outlines the condition,
Patient Information Leaflet
 Patient Information Leaflet Background Faecal incontinence is a common health problem, affecting over 1% of community-dwelling adults (1;2). Chronic constipation may affect 3-5% of the population depending
Patient Information Leaflet Background Faecal incontinence is a common health problem, affecting over 1% of community-dwelling adults (1;2). Chronic constipation may affect 3-5% of the population depending
Haemorrhoidal disorders -What is the optimal treatment?
 Haemorrhoidal disorders -What is the optimal treatment? Per-Olof Nyström, M.D., Ph.D. Professor of Surgery Karolinska Institutet and Karolinska University Hospital Huddinge Stockholm, Sweden The methods
Haemorrhoidal disorders -What is the optimal treatment? Per-Olof Nyström, M.D., Ph.D. Professor of Surgery Karolinska Institutet and Karolinska University Hospital Huddinge Stockholm, Sweden The methods
DIAGNOSIS AND MANAGEMENT OF COMMON ANORECTAL DISORDERS. Lisa Coleman, DO, FASCRS, FACS Center for Colorectal Surgery TPMG Retreat 2017
 DIAGNOSIS AND MANAGEMENT OF COMMON ANORECTAL DISORDERS Lisa Coleman, DO, FASCRS, FACS Center for Colorectal Surgery TPMG Retreat 2017 The Heinous Anus Anal Abscess Anal Cancer Anal Fissure Anal Warts Cancer
DIAGNOSIS AND MANAGEMENT OF COMMON ANORECTAL DISORDERS Lisa Coleman, DO, FASCRS, FACS Center for Colorectal Surgery TPMG Retreat 2017 The Heinous Anus Anal Abscess Anal Cancer Anal Fissure Anal Warts Cancer
Childbirth Trauma & Its Complications 23/ Mr Stergios K. Doumouchtsis
 Mr Stergios K. Doumouchtsis Consultant Obstetrician Gynaecologist & Urogynaecologist Childbirth Trauma & Its Complications Over eighty per cent of women sustain some degree of perineal trauma during childbirth.
Mr Stergios K. Doumouchtsis Consultant Obstetrician Gynaecologist & Urogynaecologist Childbirth Trauma & Its Complications Over eighty per cent of women sustain some degree of perineal trauma during childbirth.
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder).
.") An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder). Mederi Therapeutics has developed this kit to help you raise awareness of
An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder). Mederi Therapeutics has developed this kit to help you raise awareness of
DIVISION of COLOPRCTOLOGY
 DIVISION of COLOPRCTOLOGY Core Curriculum for the European Board of Surgery Qualification (EBSQ) in Coloproctology Goals, General Competencies and Specific Educational Objectives DEFINITION Coloproctology
DIVISION of COLOPRCTOLOGY Core Curriculum for the European Board of Surgery Qualification (EBSQ) in Coloproctology Goals, General Competencies and Specific Educational Objectives DEFINITION Coloproctology
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
A Nursing Assessment Tool for Adults With Fecal Incontinence
 Journal of Wound, Ostomy and Continence Nursing 2000, 279- A Nursing Assessment Tool for Adults With Fecal Incontinence Christine Norton, MA, RN, and Sonya Chelvanayagam, MSc, RN Abstract Fecal incontinence
Journal of Wound, Ostomy and Continence Nursing 2000, 279- A Nursing Assessment Tool for Adults With Fecal Incontinence Christine Norton, MA, RN, and Sonya Chelvanayagam, MSc, RN Abstract Fecal incontinence
COLORECTAL RESECTIONS
 COLORECTAL RESECTIONS What is a colorectal (bowel) resection? Surgery to remove a part of the large bowel is called a resection. Different parts of the colon require different operations and have different
COLORECTAL RESECTIONS What is a colorectal (bowel) resection? Surgery to remove a part of the large bowel is called a resection. Different parts of the colon require different operations and have different
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of endoscopic radiofrequency therapy of the anal sphincter for faecal incontinence
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of endoscopic radiofrequency therapy of the anal sphincter for faecal incontinence
A painful problem. Symptoms of haemorrhoids. Causes of haemorrhoids. Your evaluation
 A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn t be they re a very common problem that affects all kinds of people, including
A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn t be they re a very common problem that affects all kinds of people, including
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT
 STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
Inflammatory Bowel Disease and Surgery: What You Should Know
 Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
The Role of Surgery in Inflammatory Bowel Disease. Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health
 The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
Common Office Anorectal Problems
 Common Office Anorectal Problems Sandra J. Beck, M.D., FACS, FASCRS Associate Professor of Colon and Rectal Surgery University of Kentucky Medical Center l None Disclosures Benign Anal Rectal Disease l
Common Office Anorectal Problems Sandra J. Beck, M.D., FACS, FASCRS Associate Professor of Colon and Rectal Surgery University of Kentucky Medical Center l None Disclosures Benign Anal Rectal Disease l
Referral Criteria for Direct Access Outpatient Colonoscopy or Computed Tomography Colonography
 Referral Criteria for Direct Access Outpatient Colonoscopy or Computed Tomography Colonography 2019 Released 2019 health.govt.nz Citation: Ministry of Health. 2019. Referral Criteria for Direct Access
Referral Criteria for Direct Access Outpatient Colonoscopy or Computed Tomography Colonography 2019 Released 2019 health.govt.nz Citation: Ministry of Health. 2019. Referral Criteria for Direct Access
LONG TERM OUTCOME OF ELECTIVE SURGERY
 LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
2015 General Surgery Survival Guide
 2015 General Surgery Survival Guide Chapter 9: Hemorrhoids New codes in the block: 45350 & 45398 45350: Sigmoidoscopy, flexible; with band ligation(s) (eg, hemorrhoids) 45398: Colonoscopy, flexible; with
2015 General Surgery Survival Guide Chapter 9: Hemorrhoids New codes in the block: 45350 & 45398 45350: Sigmoidoscopy, flexible; with band ligation(s) (eg, hemorrhoids) 45398: Colonoscopy, flexible; with
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Northwest Rehabilitation Associates, Inc.
 Pelvic Health Patient Intake Form Name: Date: Please answer the following questions as honestly and thoroughly as you can. Your responses will help us better understand your condition and provide the best
Pelvic Health Patient Intake Form Name: Date: Please answer the following questions as honestly and thoroughly as you can. Your responses will help us better understand your condition and provide the best
ACG Clinical Guideline: Management of Benign Anorectal Disorders
 ACG Clinical Guideline: Management of Benign Anorectal Disorders Arnold Wald, MD, MACG 1, Adil E. Bharucha, MBBS, MD 2, Bard C. Cosman, MD, MPH, FASCRS 3 and William E. Whitehead, PhD, MACG 4 1 Division
ACG Clinical Guideline: Management of Benign Anorectal Disorders Arnold Wald, MD, MACG 1, Adil E. Bharucha, MBBS, MD 2, Bard C. Cosman, MD, MPH, FASCRS 3 and William E. Whitehead, PhD, MACG 4 1 Division
15. Prevention of UTI and lifestyle modifications
 15. Prevention of UTI and lifestyle modifications Key questions: Does improving poor voiding habits help prevent UTI recurrence? Does improving constipation help prevent UTI recurrence? Does increasing
15. Prevention of UTI and lifestyle modifications Key questions: Does improving poor voiding habits help prevent UTI recurrence? Does improving constipation help prevent UTI recurrence? Does increasing